Back to Journals » Vascular Health and Risk Management » Volume 13
DPP-4 inhibitor treatment: β-cell response but not HbA1c reduction is dependent on the duration of diabetes
Authors Kozlovski P, Bhosekar V, Foley JE ![]()
Received 27 October 2016
Accepted for publication 20 January 2017
Published 31 March 2017 Volume 2017:13 Pages 123—126
DOI https://doi.org/10.2147/VHRM.S125850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Video abstract presented by Plamen Kozlovski
Views: 592
Plamen Kozlovski,1 Vaishali Bhosekar,2 James E Foley3
1Novartis Pharma AG, Basel, Switzerland; 2Novartis Healthcare Private Limited, Hyderabad, India; 3Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA
Introduction: Dipeptidyl peptidase-4 (DPP-4) inhibitors reduce hyperglycemia in patients with type 2 diabetes mellitus (T2DM) by enhancing insulin and suppressing glucagon secretion. Since T2DM is associated with progressive loss of β-cell function, we hypothesized that the DPP-4 inhibitor action to improve β-cell function would be attenuated with longer duration of T2DM.
Methods: Data from six randomized, placebo-controlled trials of 24 weeks duration, where β-cell response to vildagliptin 50 mg twice daily was assessed, were pooled. In each study, the insulin secretory rate relative to glucose (ISR/G 0–2h) during glucose load (standard meal or oral glucose tolerance test) was assessed at baseline and end of study. The mean placebo-subtracted difference (PSD) in the change in ISR/G 0–2h from baseline for each study was evaluated as a function of age, duration of T2DM, baseline ISR/G 0–2h, glycated hemoglobin (HbA1c), fasting plasma glucose, body mass index, and mean PSD in the change in HbA1c from baseline, using univariate model.
Results: There was a strong negative association between the PSD in the change from baseline in ISR/G 0–2h and duration of T2DM (r= −0.89, p<0.02). However, there was no association between the PSD in the change from baseline in ISR/G 0–2h and the PSD in the change from baseline in HbA1c (r=0.33, p=0.52). None of the other characteristics were significantly associated with mean PSD change in ISR/G 0–2h.
Conclusion: These findings indicate that the response of the β-cell, but not the HbA1c reduction, with vildagliptin is dependent on duration of T2DM. Further, it can be speculated that glucagon suppression may become the predominant mechanism via which glycemic control is improved when treatment with a DPP-4 inhibitor, such as vildagliptin, is initiated late in the natural course of T2DM.
Keywords: insulin, insulin secretion rate, glucagon, α-cell, β-cell, glucagon-like peptide 1, gastric inhibitory polypeptide
Introduction
Progressive deterioration of pancreatic β-cell function contributes to the worsening of hyperglycemia in patients with type 2 diabetes mellitus (T2DM). In the UKPDS1 and ADOPT2 studies, increasing hyperglycemia with time was associated with decrease in β-cell function despite therapy with a sulfonylurea and/or metformin. Dipeptidyl peptidase-4 (DPP-4) inhibitors are a new class of oral antidiabetic drugs for treatment of T2DM.3 Physiologically, DPP-4 inhibitors increase the availability of active glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) in plasma, which in turn, improves the sensitivity of pancreatic β- and α-cells to glucose.3,4
Although DPP-4 inhibitors have been used extensively in a variety of clinical settings, the optimal stage for their use in T2DM treatment is still not well understood. It has been previously shown that there was no association between duration of diabetes and reduction in glycated hemoglobin (HbA1c) with DPP-4 inhibitor treatment.5 However, the effect of DPP-4 inhibitors on β-cell response during the treatment journey of patients with T2DM is unclear. Therefore, we evaluated the effect of vildagliptin on β-cell response (assessed as insulin secretory rate relative to glucose [ISR/G 0–2h]) and its association with factors such as disease duration, baseline ISR/G, HbA1c, age, and placebo-subtracted difference (PSD) in HbA1c change from baseline to end of study.
Materials and methods
Patients and study design
Data were pooled from six previously published, double-blind, randomized, placebo-controlled trials with 24 weeks study duration wherein β-cell response (ISR/G) to vildagliptin 50 mg twice daily or placebo was assessed at baseline and end of study (n=615).6–11
Assessments
In all the studies, β-cell response (ISR/G 0–2h) following a standard solid meal (breakfast) containing 500 kcal (60% carbohydrate, 30% fat and 10% protein), or oral glucose tolerance test (in one study),11 was assessed at baseline and at week 24.
Data analysis
The mean PSD (vildagliptin−placebo) in ISR/G 0–2h change from baseline in each study was evaluated as a function of mean age, disease duration, ISR/G 0–2h, HbA1c, fasting plasma glucose (FPG), body mass index (BMI) at baseline, and mean PSD (vildagliptin−placebo) in HbA1c change from baseline, using a univariate model.
Ethics and good clinical practice
All study participants provided written informed consent to participate in the respective clinical trials included in this pooled analysis. All protocols were approved by independent ethics committees/institutional review boards; individual study results have been reported as required by protocol and duly referenced in this article. All studies were conducted as per Good Clinical Practice and in accordance with the Declaration of Helsinki.
Results
The demographic and clinical characteristics of the participants by study and treatment group are presented in Table 1. The mean age, HbA1c, and T2DM duration of the study participants ranged from 50.2 to 59.3 years, 8.3% to 8.8%, and 1.6 to 13.2 years, respectively.
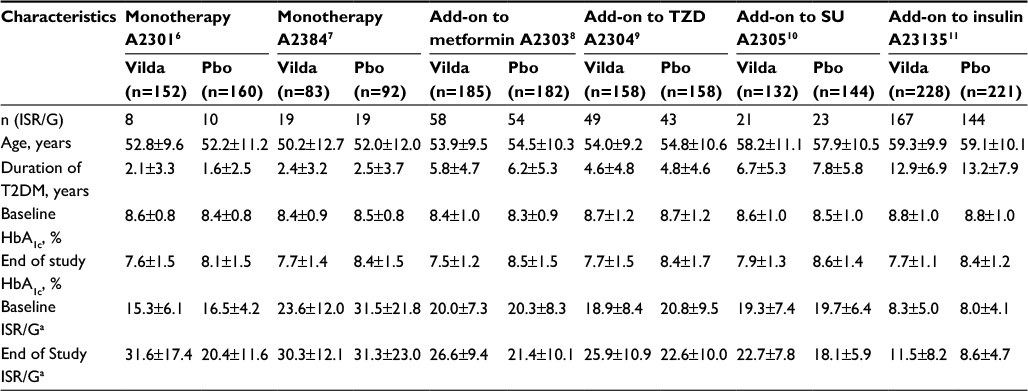 | Table 1 Demographic and clinical characteristics of the participants by study and treatment group Notes: apmol/min/m2/mmol/L. All values are mean ± SD unless specified. ‘n’ values denote the number of patients randomized to the respective treatment group. Abbreviations: HbA1c, glycated hemoglobin; ISR/G, insulin secretory rate relative to glucose; Pbo, placebo; SU, sulfonylurea; TZD, thiazolidinedione; T2DM, type 2 diabetes mellitus; Vilda, vildagliptin. |
There was a strong negative association between the mean PSD in ISR/G 0–2h change from baseline and mean baseline disease duration (r= −0.89, p<0.02) (Figure 1). However, no association was observed between the mean PSD in HbA1c change from baseline and mean baseline disease duration (r= −0.23, p=0.66) (Figure 1).
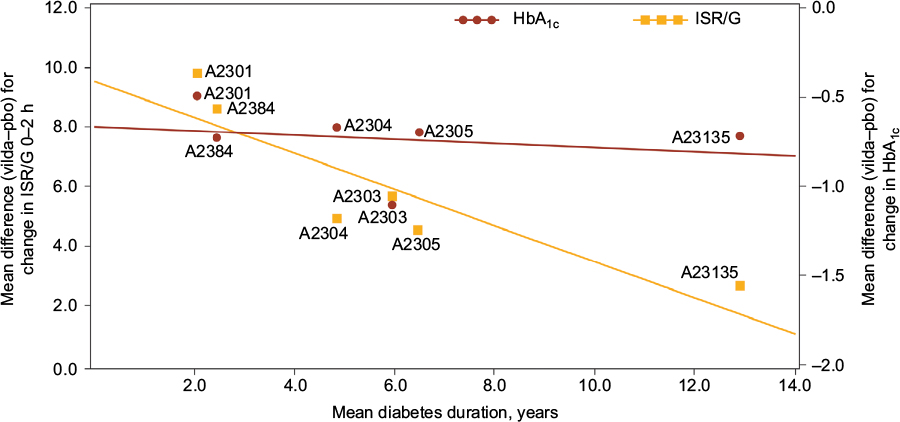 | Figure 1 Association between mean difference (vilda–pbo) in ISR/G change from baseline and mean difference (vilda–pbo) in HbA1c change from baseline vs mean duration of diabetes at baseline. Abbreviations: HbA1c, glycated hemoglobin; ISR/G, insulin secretory rate relative to glucose; pbo, placebo; vilda, vildagliptin. |
In addition, there was no association between the mean PSD in ISR/G 0–2h change from baseline and the mean PSD in HbA1c change from baseline (r=0.33, p=0.52), age (r= −0.81, p=0.05), baseline HbA1c (r= −0.59, p=0.11), ISR/G 0–2h (r=0.43, p=0.39), FPG (r=0.34, p=0.51), or BMI (r=0.70, p=0.12).
Discussion
The UKPDS demonstrated that glycemic control is progressively lost over time and that this loss is associated with a progressive loss of β-cell function.1 The ADOPT study showed that treatment with sulfonylurea, metformin, and pioglitazone demonstrates varying degrees of sustained durability, but eventually glycemic control is lost over time,12 and this loss is associated with a reduction in β-cell function.2 We hypothesized that this would translate into a reduction in β-cell response over time following vildagliptin therapy. The present analysis demonstrates that β-cell response (ISR/G) to vildagliptin treatment was indeed attenuated in patients with longer duration of diabetes.
The ISR/G depends on the sensitivity of β-cells to glucose and their maximum secretory capacity. β-cell function diminishes early in the disease progression due to decrease in the sensitivity of the β-cells to glucose and later due to a reduction in the maximum insulin-secretion capacity. DPP-4 inhibitors are known to improve the sensitivity of the β-cells to glucose, but they do not have a pronounced effect on the maximum secretory capacity which is largely determined by β-cell mass.13 We assume that early in the disease, vildagliptin mostly corrects the sensitivity defect, and continues to do so even later, while the overall effect on ISR/G is diminished by the progressive loss of the maximum capacity of insulin secretion.
We have previously shown with a larger pooled analysis of vildagliptin data that baseline-adjusted reduction in HbA1c is the same in drug-naïve patients with a short duration of diabetes and in patients with a long duration of diabetes on insulin therapy.5 In the current pooled analysis, which is a subset of the original pool, wherein β-cell function was assessed, we replicated this finding. This suggests that some element of vildagliptin action is progressively increasing to compensate for the reduced β-cell response in patients with T2DM.
Vildagliptin prolongs the meal induced increase in GLP-1 and GIP, which increases the sensitivity of the β-cells to glucose to increase insulin secretion during meals. The GLP-1 also increases the sensitivity of the α-cells to glucose to decrease glucagon secretion during meals. Physiologically, the reduction in glucagon secretion may be as important as the increase in insulin secretion in reducing hepatic glucose production.4 As the β-cell capacity declines, there is no known corresponding change in α-cell capacity. However, the diminished β-cell capacity could result in a reduced insulin paracrine inhibition of glucagon secretion, which is not mediated via GLP-1.14 The attenuated paracrine inhibition could lead to further increase in the already-increased glucagon level, which can, however, be suppressed by GLP-1 and its associated increase in α-cell sensitivity following DPP-4 inhibition. Thus, we speculate that glucagon suppression resulting from the enhanced GLP-1 levels following DPP-4 inhibition may be compensating the reduced β-cell function, leading to a similar baseline adjusted reduction in HbA1c.
Conclusion
The results indicate that the response of the β-cell, but not the HbA1c reduction, with vildagliptin is dependent on the duration of T2DM, and it can be speculated that glucagon suppression may become the predominant mechanism via which glycemic control is improved when treatment with a DPP-4 inhibitor such as vildagliptin is initiated late in the natural course of T2DM.
Acknowledgments
The authors acknowledge the patients, investigators, and staff at participating sites of all the studies. The authors also thank Sashi Kiran Goteti Novartis Healthcare Pvt. Ltd., Hyderabad, India, for editorial assistance.
Author contributions
All authors participated in the design, data review, data interpretation, and critically revised the manuscript. PK and JEF wrote the manuscript, and VB carried out the statistical analyses. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure
PK and JEF are employed by and own stocks in Novartis. VB is employed by Novartis. The study was funded by Novartis Pharma AG. Part of this data was presented as a poster (1093-P) at the 76th Scientific Sessions of the American Diabetes Association, June 10–14, 2016, New Orleans, LA, USA. The authors report no other conflicts of interest in this work.
References
No authors listed. U.K. prospective diabetes study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. U.K. Prospective Diabetes Study Group. Diabetes. 1995;44(11):1249–1258. | ||
Kahn SE, Lachin JM, Zinman B, et al. Effects of rosiglitazone, glyburide, and metformin on β-cell function and insulin sensitivity in ADOPT. Diabetes. 2011;60(5):1552–1560. | ||
Ahrén B, Schweizer A, Dejager S, Villhauer EB, Dunning BE, Foley JE. Mechanisms of action of the dipeptidyl peptidase-4 inhibitor vildagliptin in humans. Diabetes Obes Metab. 2011;13(9):775–783. | ||
Ahrén B, Foley JE. Improved glucose regulation in type 2 diabetic patients with DPP-4 inhibitors: focus on alpha and beta cell function and lipid metabolism. Diabetologia. 2016;59(5):907–917. | ||
Schweizer A, Dejager S, Foley JE. Impact of insulin resistance, body mass index, disease duration, and duration of metformin use on the efficacy of vildagliptin. Diabetes Ther. 2012;3(1):8. | ||
Dejager S, Razac S, Foley JE, Schweizer A. Vildagliptin in drug-naïve patients with type 2 diabetes: a 24-week, double-blind, randomized, placebo-controlled, multiple-dose study. Horm Metab Res. 2007;39(3):218–223. | ||
Pi-Sunyer FX, Schweizer A, Mills D, Dejager S. Efficacy and tolerability of vildagliptin monotherapy in drug-naïve patients with type 2 diabetes. Diabetes Res Clin Pract. 2007;76(1):132–138. | ||
Bosi E, Camisasca RP, Collober C, Rochotte E, Garber AJ. Effects of vildagliptin on glucose control over 24 weeks in patients with type 2 diabetes inadequately controlled with metformin. Diabetes Care. 2007;30(4):890–895. | ||
Garber AJ, Schweizer A, Baron MA, Rochotte E, Dejager S. Vildagliptin in combination with pioglitazone improves glycaemic control in patients with type 2 diabetes failing thiazolidinedione monotherapy: a randomized, placebo-controlled study. Diabetes Obes Metab. 2007;9(2):166–174. | ||
Garber AJ, Foley JE, Banerji MA, et al. Effects of vildagliptin on glucose control in patients with type 2 diabetes inadequately controlled with a sulfonylurea. Diabetes Obes Metab. 2008;10(11):1047–1056. | ||
Kothny W, Foley J, Kozlovski P, Shao Q, Gallwitz B, Lukashevich V. Improved glycemic control with vildagliptin added to insulin, with or without metformin, in patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2013;15(3):252–257. | ||
Kahn SE, Haffner SM, Heise MA, et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006;355(23):2427–2443. | ||
Foley JE, Bunck MC, Poelma M, et al. Beta cell function following 1 year vildagliptin or placebo treatment and after 12 week washout in drug-naive patients with type 2 diabetes and mild hyperglycaemia: a randomized controlled trial. Diabetologia. 2011;54(8):1985–1991. | ||
Foley JE, Liqueros-Saylan M, He YL, et al. Effect of vildagliptin on glucagon secretion during meals in patients with type 1 diabetes. Horm Metab Res. 2008;40(10):727–730. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.