Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Down Syndrome-Associated Arthritis (DA): Diagnostic and Management Challenges
Authors Jones JT ![]() , Kitchen J, Talib N
, Kitchen J, Talib N
Received 15 December 2021
Accepted for publication 7 March 2022
Published 14 March 2022 Volume 2022:13 Pages 53—62
DOI https://doi.org/10.2147/PHMT.S282646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Jordan T Jones,1– 4 Jacqueline Kitchen,2,3 Nasreen Talib2,3
1Division of Rheumatology, Children’s Mercy Kansas City, Kansas City, MO, USA; 2Division of Pediatrics, Children’s Mercy Kansas City, Kansas City, MO, USA; 3University of Missouri-Kansas City School of Medicine, Kansas City, MO, USA; 4Division of Pediatrics, University of Kansas School of Medicine, Kansas City, KS, USA
Correspondence: Jordan T Jones, Division of Rheumatology, Children’s Mercy Kansas City, 2401 Gillham Road, Kansas City, MO, 64108, USA, Tel +1 816-234-3686, Email [email protected]
Abstract: Down syndrome (DS) is one of the most common birth defects in the United States, the most common genomic disorder of intellectual disability, and results from trisomy 21. This chromosome disorder causes an extensive, heterogenous phenotype that results in a broad presentation of symptoms that includes atlantoaxial instability, congenital heart defects, muscle hypotonia, hypothyroidism, hematologic disorders, recurrent infections, and autoimmune diseases. The autoimmune diseases are caused by immune system dysregulation that results in increased pro-inflammatory cytokines, along with other innate and adaptive immune system dysregulation. This is the likely cause of the increased risk of inflammatory arthritis or Down syndrome-associated arthritis (DA) seen in individuals with DS. Most individuals with DA present with polyarticular (five or more joints with arthritis at presentation of disease), rheumatoid factor and anti-nuclear antibody negative disease that is aggressive with bone and joint damage at presentation. There is notable delay in diagnosis of DA as there are no formal guidelines on screening or monitoring for inflammatory arthritis in individuals with DS. Once diagnosed, and despite aggressive therapy with disease modifying antirheumatic drugs, disease burden is high for those with DA. Therapy can also be challenging for those with DA as many require second and third-line disease modifying therapies. Many also struggle with medication toxicity and ineffectiveness that further causes challenges with management and outcomes. The purpose of this current review is to provide an up-to-date summary of the literature related to DA in children and adolescents with focus on presentation, diagnosis, and management considerations, along with current barriers that inhibit optimal care.
Keywords: Down syndrome, Down syndrome-associated arthritis, diagnosis, management, outcomes
Introduction
Down syndrome (DS) is one of the most common birth defects in the United States with an estimated birth prevalence of 12.6 per 10,000 live births.1 DS is also the most common genomic disorder of intellectual disability and results from a trisomy of human chromosome 21.2 This chromosomal disorder results from meiotic nondisjunction most commonly, but may also result from translocation. Mosaicism and partial trisomy 21 can also occur, and these are usually associated with fewer clinical features compared with nondisjunction and translocation.3 Trisomy 21 can present with extensive, heterogenous phenotype that can affect many bodily systems and results from a dosage imbalance of genes located on human chromosome 21.4 Due to the heterogenous phenotype, a broad presentation of symptoms may occur. Individuals with DS commonly present with obstructive sleep apnea, congenital heart defects, intellectual disability, atlantoaxial instability, muscle hypotonia (possibly caused by the reduced neuronal density and cerebellar hypoplasia), and short stature. They are also at increased risk to develop anxiety disorders, epilepsy, hypothyroidism, hearing and vision problems, hematologic disorders, and recurrent infections.2 Autoimmune diseases have also been reported at an increased incidence,5,6 which poses a unique medical challenge for individuals with DS and their medical care providers. Inflammatory arthritis in children with DS was first described in 1984 and was termed Down syndrome arthropathy,7 however, the term Down syndrome-associated arthritis (DA) has been proposed to better describe the inflammatory nature of the disease.8 Since 1984, studies have shown that DA is under-recognized with a delay in diagnosis of up to three years between symptoms onset and diagnosis.9–11 Most individuals with DA present with polyarticular (five or more joints with arthritis at presentation of disease), rheumatoid factor (RF) and anti-nuclear antibody (ANA) negative disease.8–11 There are reports that DA is more prevalent than juvenile idiopathic arthritis (JIA),7,8,10,11 which is the most common pediatric rheumatologic disease.12 DA appears more aggressive than JIA with more bone and joint damage at presentation,9,11 and despite aggressive therapy with disease modifying antirheumatic drugs (DMARDs) and biologic therapy, disease burden is higher for those with DA compared to those with JIA.10,13 Therapy can also be challenging for those with DA as many require second-line disease modifying therapies,9,10 but also struggle with medication toxicity and ineffectiveness.9,10,13
The purpose of this current review is to provide an up-to-date summary of the literature related to DA in children and adolescents with focus on presentation, diagnosis, and management considerations, along with current barriers that inhibit optimal care. Additionally, goals are outlined to optimize outcomes through earlier diagnosis and monitoring of disease, with considerations for therapy management.
Prevalence and Clinical Features of DA
There are no population-based prevalence studies of DA within the United States, but previous reports suggest an estimated prevalence of 8.7 to 12 per 1000 individuals with DS.7,11 In another study that used a novel screening tool to evaluate for inflammatory arthritis in children with DS there was one individual that was diagnosed with arthritis out of 91 screened,14 which would equate to one percent of the population screened or 10 per 1000 individuals with DS. For comparison, congenital heart disease occurs in 40% to 50% of individuals with DS, while thyroid disease is reported in 4% to 18%, Celiac disease in 5% and atlantoaxial instability in 1% to 2%.15 Additionally, in Ireland the estimated prevalence of DA is 20 per 1000 individuals with DS,8 however, the Irish incidence for DS is the highest in Europe at 1 in 547 births.16 The current proposed definition of DA is inflammatory arthritis in an individual with DS. The definition of inflammatory arthritis is adapted from JIA,17 and is defined as swelling within a joint, or limitation in the range-of-motion of joint movement with or without pain or tenderness that persists for at least 6 weeks duration, is observed by a physician and is not due to primary mechanical disorder or other identifiable cause outside of DS. The definition has raised debate among the rheumatology community as the majority feel DA is the same disease as JIA,18 and because of this, individuals with DA are commonly reported as part of JIA cohorts. This has provided a framework to compare differences in disease presentation, course, outcomes, and therapy between individuals with DA and JIA. The diagnosis of JIA is a clinical diagnosis based on the Edmonton 2001 International League of Associations for Rheumatology (ILAR) criteria.17 The definition for JIA includes the subtypes: oligoarticular (four or less joints with arthritis at diagnosis), polyarticular (five or more joints with arthritis at diagnosis and with either RF positive or negative), systemic-onset (arthritis with fever of at least 2 weeks duration noted to be daily, with quotidian pattern for at least 3 days, and accompanied by classic rash, lymphadenopathy, hepatosplenomegaly, or serositis), enthesitis-related arthritis (arthritis and enthesitis or arthritis or enthesitis with two or more of the following: sacroiliac joint tenderness, inflammatory low back symptoms, positive HLA-B27, family history of HLA-B27-associated disease, acute symptomatic anterior uveitis, arthritis in male after six years of age), and psoriatic arthritis (arthritis plus psoriasis or signs of psoriasis such as dactylitis, nail pitting, onycholysis or first degree relative with psoriasis).
Of the individuals with DA most present with a polyarticular course, with RF and ANA negative disease at presentation (Tables 1 and 2).7–11,13,19–24 The second most common presentation is oligoarticular course, however, of the studies that followed individuals with DA over time, almost 70% of those that presented with oligoarticular disease progressed to polyarticular disease,9,11,21 which makes psoriatic arthritis more likely the second most common presentation of inflammatory arthritis reported in DS. This is different compared to JIA where most individuals present with oligoarticular, ANA positive disease followed by polyarticular, RF negative disease.8,25 Additionally, most of those with oligoarticular and polyarticular JIA tend to be female, whereas those with DA have less discrepancy in sex predilection. The average age range at arthritis onset is also different between JIA and DA, with individuals with JIA presenting at an earlier age. This correlates with the most common JIA subtype of oligoarticular disease, which is mostly seen in toddlers. Polyarticular JIA has a biphasic trend with peaks between 1 and 3 years of age and 9 and 14 years of age.25 Reports of DA suggest an older average age at presentation of arthritis between 6.9 and 7.4 years,9,13 however, another report suggests that most of those with DA present in the 13 to 20 year age range.8 Despite the difference between these two studies of DA, both report differences compared to polyarticular JIA, and may represent a biphasic trend in DA that occurs later than the biphasic trend seen in JIA. Many studies report morning stiffness as a symptom in individuals with DA with most studies reporting greater than 50% of individuals endorsing morning stiffness, however, one study reported 38% of individuals with morning stiffness (Table 1).
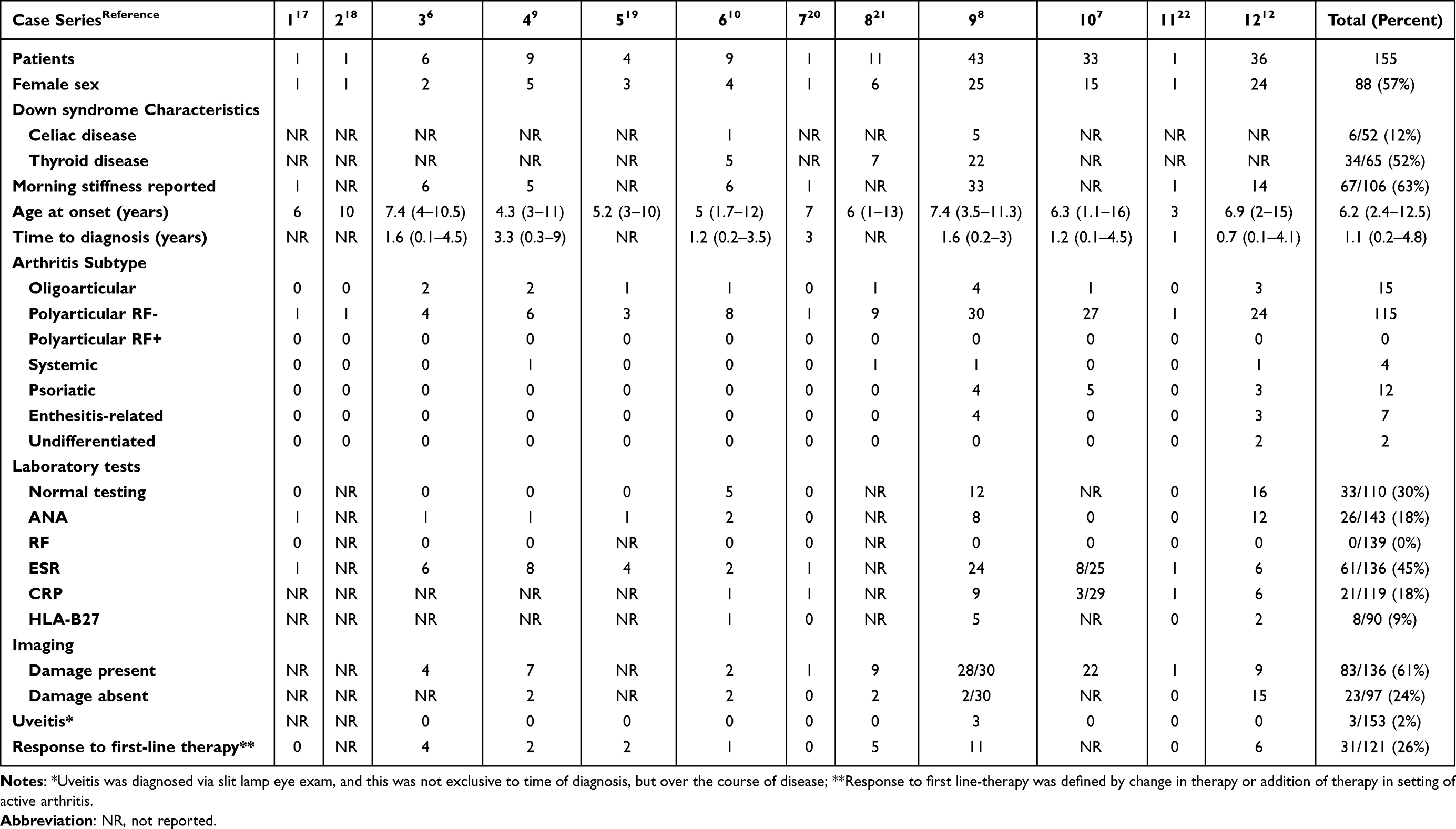 |
Table 1 Clinical Features of Down Syndrome-Associated Arthritis (at Diagnosis) |
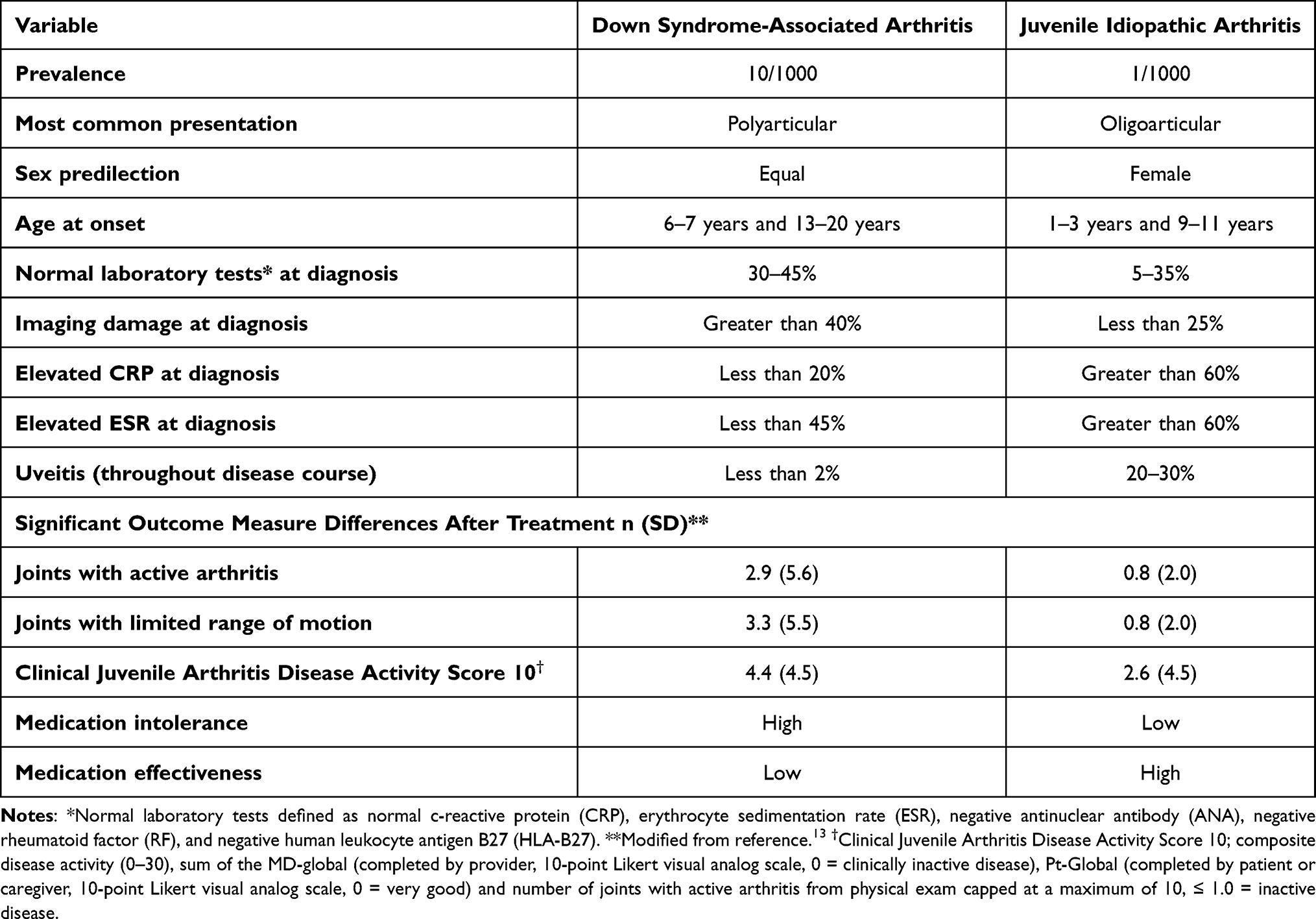 |
Table 2 Differences Between Down Syndrome-Associated Arthritis and Juvenile Idiopathic Arthritis |
Other differences exist between those with DA and JIA that include laboratory testing and imaging at disease presentation (Table 2). Earlier reports (prior to 2003) suggest the majority (88% to 100%) of those with DA present with elevated erythrocyte sedimentation rate (ESR),7,10,21 however, more recent reports (after 2009) suggest a lower percentage (17% to 56%) will have an elevated ESR at presentation.8,9,11,13 While the cause of this is not clear, it has been proposed that the more recent reports of DA were diagnosed earlier in the course of disease compared to the earlier reported cases,13 and when compared to JIA, significantly more individuals with DA had an elevation of ESR at diagnosis.8 There were also significantly more individuals with JIA that had a positive ANA compared to those with DA.8 Additionally, there are several reports of high positivity of anti-cyclic citrullinated peptide (CCP) antibody, RF, and other autoantibodies found in individuals with DS, however, these laboratory findings have not been correlated with presence of arthritis or rheumatic disease in those individuals.26–28 It is unclear what the significance of this is and likely indicates immune dysregulation in those with DS. It should be noted that anti-CCP and RF are rarely positive or elevated in those with DA. While many individuals with DA will present with abnormal laboratory tests at diagnosis, there is no consistently abnormal laboratory test seen across studies. Of the cases of DA reported, 28% to 44% of individuals presented with normal laboratory tests (normal ESR, CRP, and negative ANA, RF, CCP, and HLA-B27) at presentation of disease.9,13 Another difference between individuals with DA and JIA is imaging at diagnosis. For individuals with DA, imaging studies showed more joint abnormalities consistent with inflammatory disease such as osteopenia, bony erosions, joint space narrowing, effusion, synovitis, and tenosynovitis. When imaging studies at diagnosis of arthritis are compared between those with DA and JIA, the individuals with DA have significantly more joint damage present.8,9,13
Another difference noted between those with DA and JIA is the incidence of uveitis (Table 2), which is more prevalent in JIA, especially those with a positive ANA. There are only three patients reported in the literature with uveitis and DA,9 with two having HLA-B27 positive enthesitis-related arthritis with acute anterior uveitis and one having polyarticular RF, ANA, and HLA-B27 negative disease with chronic uveitis. While individuals with JIA are at increased risk of anterior uveitis, especially those with oligoarticular disease and ANA positivity,29 individuals with DA do not seem to have the same risk, even those with a positive ANA. For individuals with JIA, there is a known association between acute anterior uveitis and HLA-B27,30 and about 14% of those with polyarticular RF negative JIA develop chronic anterior uveitis.31 This may indicate that those with DA and HLA-B27 are at increased risk of acute uveitis, however, the numbers are too low to draw firm conclusions. More information is needed to further evaluate the risk of acute and chronic uveitis and determine if more frequent eye screening in patients with DA is necessary or if certain features increase the risk for inflammatory eye disease in this population.
Etiology and Pathogenesis.
The etiology and pathogenesis of DA has not been fully described, but since the 1970s there has been emerging evidence that individuals with DS have clear differences in their immune system compared to those without DS. This is supported by the increased incidence of autoimmune diseases such as Celiac and Diabetes mellitus type I, leukemia, and infections, especially pneumonia. Since that time work has been done that supports the idea that there is an intrinsic defect in the immune system of those with DS.32 Evidence has grown and reports show a diminished expansion of T and B lymphocytes, which strongly suggests a disturbance in the adaptive immune system in those with DS.33 Further, when those with DS were compared to healthy, neurotypical controls it was shown that those with DS have significantly higher percentages of interferon (IFN)-γ-producing CD4+ and CD8+ cells with higher Th1/Th2 ratio.34 There is also evidence to show that pro-inflammatory cytokines are dysregulated in individuals with DS. A study that compared healthy neurotypical children to healthy children with DS showed that those with DS had elevated IFN-γ, and tumor necrosis factor (TNF)-α, and decreased levels of interleukin (IL)-10.35 A meta-analysis from 2017 was performed looking at immune system differences between healthy individuals with DS and neurotypical healthy controls. The results showed that individuals with DS had significantly increased circulating levels of TNF-α, IL-1β, IFN-γ and neopterin when compared to neurotypical healthy controls. There were no differences seen in IL-4, IL-6, IL-8 and IL-10.36 It has been proposed that the additional interferon receptors encoded on chromosome 21 have created a gene dosage affect that has increased IFN pathway signaling that contributes to the elevated IFN expression in individuals with DS and likely contributes to chronic immune dysregulation that leads to an increased incidence of autoimmune and autoinflammatory diseases in individuals with DS.37–39 Based on these studies DS could be considered an interferonopathy. A study that compared the adaptive immune system of individuals with DA and JIA found noticeable differences between the two groups. There was expansion of IgM-only memory B cells in DA compared to JIA and decreased frequency of transitional B cells that may contribute to the immune dysregulation. Individuals with DA were also noted to have increased TNF and INF-γ responses by CD8− T cells and increased TNF and IL-17A responses by CD8+ T cells compared to individuals with JIA. There was also significant expansion of Th1/Th17 cells while Treg cells were reduced in DA. It was also noted that the increased proinflammatory cytokine response was associated with increased T cell plasticity. There were also cytokine differences noted in inflamed tissue between individuals with DA and JIA with increased synovial tissue inflammation that showed increased infiltration of T and B cells in those with DA compared to those with JIA.40 These findings suggest clear differences between those with DA and JIA and may indicate that DA and JIA are different diseases, however, it may also indicate that the differences in disease presentation between DA and JIA are a result of the immune dysregulation in those with DS. More studies are needed to determine biologic differences between DA and JIA and the extent that the immune dysregulation is involved in DA. This area of research could also identify novel biomarkers that could be used to aid with diagnosis and guide disease monitoring.
Evaluation of Down Syndrome-Associated Arthritis
Many challenges have been identified that contribute to a delayed or missed diagnosis of DA. One of those challenges is awareness about of the increased risk of inflammatory arthritis in individuals with DS among families and healthcare professionals. This has been proposed as part of the reason there is a delay in diagnosis of DA after long-standing inflammatory musculoskeletal symptoms occur.8–11 Additionally, when families and care providers of children with DS were surveyed 86% were unaware of their child’s increased risk to develop inflammatory arthritis.14 Others have also shown that families often are unaware that their child is displaying signs of arthritis,8 and many present to care several times with inflammatory arthritis symptoms prior to a diagnosis of DA.41 Even after diagnosis of DA, families report emotional, physical and financial challenges of being a parent and caregiver to an individual with intellectual disability and additional complex chronic disease42 that affects mobility and requires immunosuppressive therapy in the setting of increased risk of infection. Other challenges to diagnosis of DA include musculoskeletal findings specific to individuals with DS such as hypotonia, ligament laxity and delayed motor skills that may mask signs of inflammatory arthritis. Additionally, poor language skills or autism present in individuals with DS may prevent articulation of joint symptoms. In a national survey of DS clinic providers, 77% responded that they were aware of the risk for inflammatory arthritis in DS, however, less than half educated families about the risk, which is likely due to the lack of guidance around screening and evaluation for DA.43
There are currently no disease specific formal screening tools for DA, but the American Academy of Pediatrics (AAP) has published a clinical report for the health supervision of children with DS.15 The report discusses age-appropriate guidance on when to screen for specific conditions, when to refer to specialty care for evaluation, and anticipatory guidance for families as their child with DS ages, however, there is no discussion of increased risk for arthritis, formal guidance on screening or surveillance of DA. There have been two studies of novel musculoskeletal screening tools that have been developed and implemented for DA that have both successfully identified individuals with DA. One study was a tiered musculoskeletal screening clinic that children with DS attended where individuals with DS were screened with history and musculoskeletal exam, and then those with concern for inflammatory arthritis were referred for further evaluation by a pediatric rheumatologist to confirm the diagnosis of DA.8 Another study used a brief musculoskeletal screening questionnaire given to all families and patients seen in the DS clinic. All individuals with a positive screen had an ESR obtained, and had a musculoskeletal evaluation by a pediatric rheumatologist with additional laboratory and imaging tests performed if appropriate.14 Despite these two studies, there are currently no universally accepted DA screening tools that have been used more broadly. In a national survey of DS clinic providers and pediatric rheumatologists, most responded that they employ a combination of history, physical exam, laboratory tests, and imaging modalities to screen for DA,18,43 however, there were discrepancies in preferred laboratory tests and imaging modalities between the DS clinic providers and the pediatrics rheumatologists, and ultimately, there was no general consensus identified.
JIA is one of the most common causes of uveitis in childhood. It is predominantly anterior, nongranulomatous inflammation that affects the iris and ciliary body and has insidious onset. Due to this there are universal recommendations for screening for inflammatory eye disease.44 The lack of inflammatory eye disease noted in DA would suggest a low risk to develop uveitis. Further, most cases of uveitis seen in DA have a positive HLA-B27 and developed acute uveitis, while none of the individuals with a positive ANA developed uveitis. This may indicate less need for routine eye screening compared to those with JIA. An annual slit-lamp eye exam to evaluate for anterior uveitis is probably sufficient for those with DA unless specific eye issues are identified as about 60% of individuals with DS will have eye abnormalities that are more commonly seen in individuals with DS, and most of these are identified in the first year of life.15
Diagnostic Criteria of DA
There are currently no diagnostic criteria for DA, and it is generally agreed upon that DA is a diagnosis of inflammatory arthritis in an individual with DS. This has been challenged as most of the rheumatology community feels that DA is the same disease as JIA18 as there are many similarities between JIA and DA. Despite this, JIA is idiopathic in nature, and for it to occur in an individual with DS may contradict that idea. Additionally, there is emerging evidence that there are biologic differences between those with DA and JIA, which is likely caused by immune system dysregulation. Due to this we would propose DA as a separate disease entity when compared to JIA. The ILAR criteria used to define JIA has been used by default to classify DA as there are clinical similarities between these two diseases, and DA could be reclassified as another ILAR subtype of arthritis, as there is overlap between DA and several JIA subtypes. Work is needed to develop a disease specific diagnostic criterion for DA, which could be adapted from other types of inflammatory arthritis such as JIA or completely independent. This would increase disease awareness, education, and aid in development of surveillance and outcome measures for those with DA.
Treatment and Outcomes
Optimal treatment has proven complex as there is no current guidance on ideal therapy or approach to the treatment of DA. Because of the similarities between DA and JIA, therapies for JIA such as nonsteroidal anti-inflammatory drugs (NSAIDs), steroids (oral and intraarticular), disease modifying anti-rheumatic drugs (DMARDs) and biologic therapies have been utilized to treat DA. Many studies have shown that individuals with DA have more aggressive disease that requires second-line therapy such as DMARDs (Table 1).7,9–11,13,19,21–24 Of the second-line therapies, methotrexate is the most used DMARD therapy,9,13,18 but leflunomide, sulfasalazine, azathioprine, and hydroxychloroquine have also been employed to treat DA. In a survey of pediatric rheumatologists, methotrexate was mostly given via subcutaneous route at a dose of 15mg/m2 once weekly compared to oral formulation and dosages less than 15 mg/m2.18 Of those that report methotrexate use for individuals with DA, over half of all individuals had it discontinued due to intolerance.9,13 It is well documented that individuals with DS have intolerance to high dose methotrexate for treatment of leukemia, but also to low dose methotrexate for treatment of arthritis.9,45,46 Biologic therapies have reportedly been used in many (55% to 75%) individuals with DA, with TNF-inhibitors being the most common biologic agent used.9,13,18 Other biologic therapies used include: abatacept, tocilizumab, infliximab, anakinra and canakinumab.9,13 Of those with DA who were treated with biologic therapies, 40% to 60% had at least one change in biologic therapy due to ineffectiveness of the therapy.9,13 Additionally, when compared to those with JIA, those with DA had significantly more DMARD adverse events (93% versus 25%), and biologic therapy ineffectiveness (60% versus 17%).13 Steroids have been used as part of therapy too, but are the most avoided therapy due to the side effect profile related to weight gain, obesity, and comorbid issues related to DS.18,47
There are currently no validated arthritis disease measures for DA, and those developed and validated for JIA have been used as surrogates for disease activity with the caveat that measures for JIA were developed specifically for neurotypical individuals and may not be fully applicable to those with DA. The outcome measures commonly used for JIA include joints with active arthritis and limited range-of-motion (ROM), physician global assessment of disease activity (MD-global; 10-point Likert scale, 0 = clinically inactive disease), patient/parent assessment of overall well-being (Pt-global; 10-point Likert scale, 0 = very good), and Childhood Health Assessment Questionnaire (CHAQ), which is a disease-specific measure of functional status developed for JIA and used in clinical practice.48 A clinical Juvenile Arthritis Disease Activity Score (cJADAS)49 is a composite disease activity score for JIA, and is the sum of the MD-global, Pt-global and number of joints with active arthritis capped at a maximum score of 10 (cJADAS10). The cJADAS10 has cutoff values for defining states of disease activity. For oligoarticular disease, inactive disease is defined as cJADAS10 ≤ 1.0, low disease activity is >1.0 to ≤1.5, moderate disease activity is 1.51 to 4, and high disease activity is > 4. For polyarticular disease, inactive disease is defined as cJADAS10 ≤ 1.0, low disease activity is >1.0 to ≤ 2.5, moderate disease activity is 2.51 to 8.5, and > 8.5 is high disease activity.50 Cutoff values have not been established for other JIA subtypes.
When individuals with DA are evaluated, many have a substantial number of joints with active arthritis and limited ROM that mostly involves small and medium joints, with high disease activity and elevated MD-global, Pt-global, and CHAQ scores.9 In a study of individuals with DA that were matched to those with JIA, it was found that those with DA had less disease burden at diagnosis, were identified sooner compared to those with JIA and were treated aggressively with early imitation of DMARD and biologic therapy that was not significantly different from those with JIA. Additionally, there were no significant differences between those with JIA and DA for MD-global, joints with active arthritis, or JADAS10, but worse Pt-global and CHAQ scores for those with DA compared to those with JIA. At the end of the study there were noted improvements in all outcome measures, however, when compared to those with JIA, there were significantly worse outcomes for all domains (Pt-global, joints with active arthritis and limited ROM, CHAQ, cJADAS10) except for MD-global, which suggest greater disease burden and worse response to therapy for those with DA compared to those with JIA.13
For those with systemic-onset JIA (arthritis with fever of at least 2 weeks duration noted to be daily, with quotidian pattern for at least 3 days, and accompanied by classic rash, lymphadenopathy, hepatosplenomegaly, or serositis) there has been an increase in parenchymal inflammatory lung disease that appears to be associated with elevated serum level of IL-18, IFN-γ activation and activated T cell function.51 Of interest, there was an increased prevalence of systemic-onset JIA-related inflammatory lung disease in those with DS and the disease was more aggressive and burdensome for those with DS compared to those without DS.52 While the cause of this is unclear there is concern for immune dysregulation in those with DS that leads to worse outcomes.
Future Research
Evidence supporting proper identification and treatment of DA has been increasing in the past decade, however, there are still gaps in knowledge that exist. With the increased incidence of DA in those with DS, screening tools are needed to identify individuals earlier so appropriate therapies can be initiated to improve disease progression and outcomes. Routine musculoskeletal screening with questionnaires, physical exam, laboratory testing and imaging could be implemented as part of the AAP’s clinical report for the health supervision of children with DS15 to give guidance on when to screen and when to refer to specialty care. Novel biomarkers could be instrumental as part of a screening tool to support a diagnosis of DA and to monitor progress and response to therapy as diagnosis of DA can be challenging due to the unique traits seen in individuals with DS such as ligament laxity, hypotonia, intellectual disability, and delayed developmental milestones. A better approach to therapy is needed as the current therapies used to treat DA are associated with increased toxicity and ineffectiveness. A therapy approach specific for those with DA is warranted with medications that are better tolerated and more effective. With IFN hyperactivation and downstream Janus kinase (JAK) signaling there have been reports of JAK inhibition as a therapeutic option for those with DS and inflammatory arthritis.53,54 To determine changes in disease status DA-specific outcome measures are needed, like those with JIA and other rheumatic disease, to evaluate change and therapy effectiveness over time. In recognition of the of the critical health and quality-of-life needs for individuals with DS, the INCLUDE (Investigation of Co-occurring conditions across the Lifespan to Understand Down Syndrome) project (nih.gov/include-project) was launched in 2018 by the National Institutes of Health to investigate conditions that affect individuals with DS. Increased focus on DA research will undoubtedly lead to better screening, categorization of the disease, improved approach to therapy and better outcomes.
Conclusion
DA continues to be a significant cause of disability for children and adolescents with DS. Education is needed to raise awareness among families with a child or adolescent with DS and healthcare providers. Through education and routine screening more children with DA will get the appropriate care they need. Better medications and therapy approaches are needed for those with DA to mitigate adverse drug affects and drug ineffectiveness, which is problematic for those with DS. With improved awareness, better screening, and early effective therapy, the outcomes for those with DA should improve as long-term joint damage and disability are prevented.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. de Graaf G, Buckley F, Skotko BG. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States. Am J Med Genet A. 2015;167A(4):756–767. doi:10.1002/ajmg.a.37001
2. Antonarakis SE, Skotko BG, Rafii MS, et al. Down syndrome. Nat Rev Dis Primers. 2020;6(1):9. doi:10.1038/s41572-019-0143-7
3. Bull MJ. Down syndrome. N Engl J Med. 2020;382(24):2344–2352. doi:10.1056/NEJMra1706537
4. Asim A, Kumar A, Muthuswamy S, Jain S, Agarwal S. Down syndrome: an insight of the disease. J Biomed Sci. 2015;22:41. doi:10.1186/s12929-015-0138-y
5. Shin M, Siffel C, Correa A. Survival of children with mosaic Down syndrome. Am J Med Genet A. 2010;152A(3):800–801. doi:10.1002/ajmg.a.33295
6. Verstegen RHJ, Chang KJJ, Kusters MAA. Clinical implications of immune-mediated diseases in children with Down syndrome. Pediatr Allergy Immunol. 2020;31(2):117–123. doi:10.1111/pai.13133
7. Yancey CL, Zmijewski C, Athreya BH, Doughty RA. Arthropathy of Down’s syndrome. Arthritis Rheum. 1984;27(8):929–934. doi:10.1002/art.1780270813
8. Foley CM, Deely DA, MacDermott EJ, Killeen OG. Arthropathy of Down syndrome: an under-diagnosed inflammatory joint disease that warrants a name change. RMD Open. 2019;5(1):e000890. doi:10.1136/rmdopen-2018-000890
9. Jones JT, Talib N, Lovell D, Becker ML. Clinical features and treatment of Down syndrome arthropathy: experience from two US tertiary hospitals. Paediatr Drugs. 2019;21(1):33–39. doi:10.1007/s40272-018-0322-0
10. Olson JC, Bender JC, Levinson JE, Oestreich A, Lovell DJ. Arthropathy of Down syndrome. Pediatrics. 1990;86(6):931–936. doi:10.1542/peds.86.6.931
11. Juj H, Emery H. The arthropathy of Down syndrome: an underdiagnosed and under-recognized condition. J Pediatr. 2009;154(2):234–238. doi:10.1016/j.jpeds.2008.07.056
12. Woo P, Colbert RA. An overview of genetics of paediatric rheumatic diseases. Best Pract Res Clin Rheumatol. 2009;23(5):589–597. doi:10.1016/j.berh.2009.08.001
13. Jones JT, Smith C, Becker ML, Lovell D, Investigators CR. The Down syndrome-associated arthritis Cohort in the new Childhood Arthritis and Rheumatology Research Alliance (CARRA) Registry: clinical characteristics, treatment and outcomes. Arthritis Care Res. 2020. doi:10.1002/acr.24418
14. Jones JT, Smith C, Talib N. Brief musculoskeletal screen and patient education for Down syndrome-associated arthritis. Glob Pediatr Health. 2021;8:2333794X211045562. doi:10.1177/2333794X211045562
15. Bull MJ; Committee on G. Health supervision for children with Down syndrome. Pediatrics. 2011;128(2):393–406. doi:10.1542/peds.2011-1605
16. Johnson Z, Lillis D, Delany V, Hayes C, Dack P. The epidemiology of Down syndrome in four counties in Ireland 1981–1990. J Public Health Med. 1996;18(1):78–86. doi:10.1093/oxfordjournals.pubmed.a024466
17. Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392.
18. Nicek A, Talib N, Lovell D, Smith C, Becker ML, Jones JT. Assessment and treatment of Down syndrome-associated arthritis: a survey of pediatric rheumatologists. Pediatr Rheumatol Online J. 2020;18(1):57. doi:10.1186/s12969-020-00445-6
19. Sherk HH, Pasquariello PS, Watters WC. Multiple dislocations of the cervical spine in a patient with juvenile rheumatoid arthritis and Down’s syndrome. Clin Orthop Relat Res. 1982;162:37–40. doi:10.1097/00003086-198201000-00007
20. Herring JA. Cervical instability in Down’s syndrome and juvenile rheumatoid arthritis. J Pediatr Orthop. 1982;2(2):205–207. doi:10.1097/01241398-198202020-00017
21. Padmakumar B, Evans jones LG, Sills JA. Is arthritis more common in children with Down syndrome? Rheumatology. 2002;41(10):1191–1193. doi:10.1093/rheumatology/41.10.1191
22. Çubukçu D, Alkan H. Patient with arthritis and Down’s syndrome: a dilemma to distinguish, juvenile idiopathic arthritis or arthropathy of the syndrome?. J PMR Sci. 2014;18:36–39.
23. Krumrey-Langkammerer M, Hass JP. Trisomy 21 and juvenile idiopathic arthritis: relevance of chromosomal aberrations for the diagnostic assessment of arthritis. Akt Rheumatol. 2016;2016(41):390–395.
24. Mauro A, Zenzeri L, Rega R, Di Nardo G, Sottile R. Chronic arthropathy in Down’s syndrome: case report and literature review. Case Report. Int J Clin Rheumtol. 2019;14(5):213–215.
25. Petty RE, Laxer RM, Lindsley CB, Wedderburn L. Textbook of Pediatric Rheumatology.
26. Nisihara RM, Skare TL, Silva MBG, et al. High positivity of anti-CCP antibodies in patients with Down syndrome. Clin Rheumatol. 2007;26(12):2031–2035. doi:10.1007/s10067-007-0606-1
27. da Rosa Utiyama SR, Nisihara RM, Nass FR, Oliveira NP, Fiedler PT, de Messias-reason IT. Autoantibodies in patients with Down syndrome: early senescence of the immune system or precocious markers for immunological diseases? J Paediatr Child Health. 2008;44(4):182–186. doi:10.1111/j.1440-1754.2007.01229.x
28. Orro E, Alnek K, Reimand T, et al. Patients with down syndrome have increased prevalence of rheumatoid factor but not autoantibodies to anti-cyclic citrullinated peptide. Clin Chim Acta. 2019;495:40–42. doi:10.1016/j.cca.2019.03.1614
29. Heiligenhaus A, Heinz C, Edelsten C, Kotaniemi K, Minden K. Review for disease of the year: epidemiology of juvenile idiopathic arthritis and its associated uveitis: the probable risk factors. Ocul Immunol Inflamm. 2013;21(3):180–191. doi:10.3109/09273948.2013.791701
30. Martin TM, Rosenbaum JT. An update on the genetics of HLA B27-associated acute anterior uveitis. Ocul Immunol Inflamm. 2011;19(2):108–114. doi:10.3109/09273948.2011.559302
31. Saurenmann RK, Levin AV, Feldman BM, et al. Prevalence, risk factors, and outcome of uveitis in juvenile idiopathic arthritis: a long-term follow up study. Arthritis Rheum. 2007;56(2):647–657. doi:10.1002/art.22381
32. Kusters MA, Verstegen RH, Gemen EF, de Vries E. Intrinsic defect of the immune system in children with Down syndrome: a review. Clin Exp Immunol. 2009;156(2):189–193. doi:10.1111/j.1365-2249.2009.03890.x
33. de Hingh YC, van der Vossen PW, Gemen EF, et al. Intrinsic abnormalities of lymphocyte counts in children with down syndrome. J Pediatr. 2005;147(6):744–747. doi:10.1016/j.jpeds.2005.07.022
34. Franciotta D, Verri A, Zardini E, et al. Interferon-γ- and interleukin-4-producing T cells in Down’s syndrome. Neurosci Lett. 2006;395(1):67–70. doi:10.1016/j.neulet.2005.10.048
35. Nateghi Rostami M, Douraghi M, Miramin Mohammadi A, Nikmanesh B. Altered serum pro-inflammatory cytokines in children with Down’s syndrome. Eur Cytokine Netw. 2012;23(2):64–67. doi:10.1684/ecn.2012.0307
36. Zhang Y, Che M, Yuan J, et al. Aberrations in circulating inflammatory cytokine levels in patients with Down syndrome: a meta-analysis. Oncotarget. 2017;8(48):84489–84496. doi:10.18632/oncotarget.21060
37. Sullivan KD, Lewis HC, Hill AA, et al. Trisomy 21 consistently activates the interferon response. Elife. 2016;5. doi:10.7554/eLife.16220
38. Sullivan KD, Evans D, Pandey A, et al. Trisomy 21 causes changes in the circulating proteome indicative of chronic autoinflammation. Sci Rep. 2017;7(1):14818. doi:10.1038/s41598-017-13858-3
39. Waugh KA, Araya P, Pandey A, et al. Mass cytometry reveals global immune remodeling with multi-lineage hypersensitivity to type I interferon in Down syndrome. Cell Rep. 2019;29(7):1893–1908 e4. doi:10.1016/j.celrep.2019.10.038
40. Foley C, Floudas A, Canavan M, et al. Increased T cell plasticity with dysregulation of follicular helper T, peripheral helper T, and treg cell responses in children with juvenile idiopathic arthritis and Down syndrome-associated arthritis. Arthritis Rheumatol. 2020;72(4):677–686. doi:10.1002/art.41150
41. Cruikshank M, Tunc A, Walsh J, Galea P, Davidson J, Gardner-Medwin J. Arthritis in Down’s syndrome is still being missed. Pediatr Rheumatol Online J. 2008;6:P54. doi:10.1186/1546-0096-6-S1-P54
42. McDonagh K, McGuire BE, Durand H. Being a parent of a child with Down’s arthritis: an interpretative phenomenological analysis. Disabil Rehabil. 2021;1–9. doi:10.1080/09638288.2021.1979663
43. Jones JT, Smith C, Talib N. Assessment of Down syndrome-associated arthritis: a survey of Down syndrome clinic providers. Glob Pediatr Health. 2021;8:2333794X21999134. doi:10.1177/2333794X21999134
44. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
45. Peeters M, Poon A. Down syndrome and leukemia: unusual clinical aspects and unexpected methotrexate sensitivity. Eur J Pediatr. 1987;146(4):416–422. doi:10.1007/BF00444952
46. Buitenkamp TD, Mathot RA, de Haas V, Pieters R, Zwaan CM. Methotrexate-induced side effects are not due to differences in pharmacokinetics in children with Down syndrome and acute lymphoblastic leukemia. Haematologica. 2010;95(7):1106–1113. doi:10.3324/haematol.2009.019778
47. Bertapelli F, Pitetti K, Agiovlasitis S, Guerra-Junior G. Overweight and obesity in children and adolescents with Down syndrome-prevalence, determinants, consequences, and interventions: a literature review. Res Dev Disabil. 2016;57:181–192. doi:10.1016/j.ridd.2016.06.018
48. Singh G, Athreya BH, Fries JF, Goldsmith DP. Measurement of health status in children with juvenile rheumatoid arthritis. Arthritis Rheum. 1994;37(12):1761–1769. doi:10.1002/art.1780371209
49. McErlane F, Beresford MW, Baildam EM, et al. Validity of a three-variable Juvenile Arthritis Disease Activity Score in children with new-onset juvenile idiopathic arthritis. Ann Rheum Dis. 2013;72(12):1983–1988. doi:10.1136/annrheumdis-2012-202031
50. Consolaro A, Negro G, Chiara Gallo M, et al. Defining criteria for disease activity states in nonsystemic juvenile idiopathic arthritis based on a three-variable juvenile arthritis disease activity score. Arthritis Care Res. 2014;66(11):1703–1709. doi:10.1002/acr.22393
51. Schulert GS, Yasin S, Carey B, et al. Systemic juvenile idiopathic arthritis-associated lung disease: characterization and risk factors. Arthritis Rheumatol. 2019;71(11):1943–1954. doi:10.1002/art.41073
52. Saper VE, Chen G, Deutsch GH, et al. Emergent high fatality lung disease in systemic juvenile arthritis. Ann Rheum Dis. 2019;78(12):1722–1731. doi:10.1136/annrheumdis-2019-216040
53. Pham AT, Rachubinski AL, Enriquez-Estrada B, Worek K, Griffith M, Espinosa JM. JAK inhibition for treatment of psoriatic arthritis in Down syndrome. Rheumatology. 2021;60(9):e309–e311. doi:10.1093/rheumatology/keab203
54. Worley E, Li W, Jones JT. Atypical presentation of systemic arthritis in a Toddler with Down syndrome. Case Rep Pediatr. 2021;2021:6567770. doi:10.1155/2021/6567770
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.