Back to Journals » Drug Design, Development and Therapy » Volume 19
Double Filtration Plasmapheresis Shows Superior Short-Term Efficacy to Intravenous Methylprednisolone in Acute Autoimmune Encephalitis: A Prospective Observational Study
Authors Li H, Ding J ![]() , Li Q, Pei X, Wang K, Peng J, Li W, Zhou X
, Li Q, Pei X, Wang K, Peng J, Li W, Zhou X ![]() , Zhu D
, Zhu D ![]() , Guan Y
, Guan Y
Received 2 October 2025
Accepted for publication 10 December 2025
Published 15 December 2025 Volume 2025:19 Pages 11163—11172
DOI https://doi.org/10.2147/DDDT.S565677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Hongyan Li,1,* Jie Ding,2,* Qiuju Li,1 Xuzhong Pei,1 Kan Wang,2 Jing Peng,2 Wanwan Li,2 Xiajun Zhou,2 Desheng Zhu,2 Yangtai Guan1
1Department of Neurology, Punan Branch of Renji Hospital, Shanghai Jiao Tong University School of Medicine (Punan Hospital in Pudong New District), Shanghai, 200125, People’s Republic of China; 2Department of Neurology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200127, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yangtai Guan, Department of Neurology, Punan Branch of Renji Hospital, Shanghai Jiao Tong University School of Medicine (Punan Hospital in Pudong New District), Shanghai, 200125, People’s Republic of China, Tel +86 13386271865, Fax +86 21 68383482, Email [email protected] Desheng Zhu, Department of Neurology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, No. 160, Pujian Road, Shanghai, 200127, People’s Republic of China, Tel +86 13564719779, Email [email protected]
Background: Autoimmune encephalitis (AE) is a severe neurological disorder, but limited evidence comparing the efficacy of double filtration plasmapheresis (DFPP) and intravenous methylprednisolone (IVMP) as first-line treatments in the acute phase. This study aimed to evaluate the clinical outcomes of DFPP versus IVMP in antibody-positive patients with AE.
Methods: A prospective observational cohort study was conducted at Renji Hospital from July 2018 to May 2024. Thirty-eight patients with antibody-confirmed AE in the acute phase who received either DFPP (n=22) or IVMP (n=16) as first-line therapy were included. The primary outcome was improvement in the Modified Rankin Scale (mRS), and the secondary outcome was improvement in the Clinical Assessment Scale for Autoimmune Encephalitis (CASE). Adverse events were recorded for safety assessment. Univariate and multivariate logistic regression analyses were performed.
Results: The DFPP group demonstrated significantly higher rates of functional improvement, with 68.2% (15/22) achieving mRS reduction compared to 31.3% (5/16) in the IVMP group (p=0.047). Similarly, symptomatic improvement (CASE score reduction) was observed in 72.7% (17/22) of DFPP patients versus 43.8% (7/16) with IVMP (p=0.099). Multivariate analysis identified DFPP as the sole independent predictor of better outcomes (OR: 5.234, 95% CI: 1.179– 23.235, p=0.030). Adverse events were limited to the DFPP group (3/22), including manageable deep venous thrombosis and hepatic impairment.
Conclusion: DFPP demonstrated superior short-term efficacy compared to IVMP in improving functional and symptomatic outcomes in acute-phase AE, suggesting its potential as a preferred first-line therapy. Further large-scale randomized trials are warranted to validate these findings.
Keywords: Autoimmune encephalitis, double filtration plasmapheresis, intravenous methylprednisolone, plasma exchange, immunotherapy, acute-phase
Introduction
Autoimmune encephalitis (AE) represents a group of immune-mediated disorders characterized by autoantibodies targeting neuronal surface or intracellular antigens, leading to diverse neuropsychiatric manifestations such as cognitive impairment, seizures, and movement disorders. With an estimated prevalence of 13.7/100000, AE poses significant diagnostic and therapeutic challenges due to its heterogeneous clinical presentation and severity, often necessitating intensive care in up to 70% of cases.1 Early intervention is critical, as prompt immunotherapy within four weeks of symptom onset has been associated with improved outcomes. Current first-line treatments include intravenous methylprednisolone (IVMP), intravenous immunoglobulin (IVIG), and therapeutic plasma exchange (TPE), which collectively aim to mitigate immune-mediated neuronal dysfunction.2,3 However, the comparative efficacy of these modalities, particularly novel TPE-derived techniques like double filtration plasmapheresis (DFPP), remains inadequately explored.
DFPP, a semi-selective apheresis technology, offers distinct advantages over conventional TPE by selectively removing pathogenic macromolecules (eg, autoantibodies, immune complexes) while retaining beneficial plasma components like albumin. Unlike TPE, DFPP eliminates the need for exogenous plasma replacement, thereby circumventing supply limitations and reducing transfusion-related risks.4 Preliminary studies in other autoimmune neurological conditions, such as myasthenia gravis and multiple sclerosis, suggest DFPP’s potential to enhance clinical outcomes when combined with immunosuppressants.5–8 For instance, DFPP combined with oral methylprednisolone demonstrated superior efficacy to oral methylprednisolone alone in myasthenia gravis.9 Improved symptoms of steroid-refractory multiple sclerosis were noted after DFPP.10 Despite these promising findings, robust evidence comparing DFPP directly with IVMP in acute-phase AE is scarce, highlighting a knowledge gap in clinical guidance for optimal first-line therapy selection.
This study addresses this gap by prospectively evaluating the efficacy and safety of DFPP versus IVMP in antibody-positive patients with acute-phase AE. While prior research has predominantly examined TPE as an adjunct to IVMP or IVIG,11,12 confounding the assessment of its standalone utility, our study design isolates the comparative effectiveness of DFPP monotherapy. Given the American Society for Apheresis’s endorsement of TPE for anti-NMDAR encephalitis,13 yet limited data on DFPP’s role, our findings aim to clarify whether DFPP’s mechanistic advantages translate into superior clinical outcomes. We hypothesized that DFPP, by rapidly removing pathogenic autoantibodies, would lead to superior short-term clinical improvement compared to IVMP in acute-phase AE. By analyzing functional improvement and symptom resolution, this study seeks to inform evidence-based therapeutic decisions and highlight potential avenues for optimizing AE management.
Methods
Ethics
This study was approved by the Ethics Committee of Renji Hospital, Shanghai Jiao Tong University School of Medicine (LY2024-031-B). All data were collected prospectively for the purpose of this study. Written informed consent was waived for the use of serum, cerebrospinal fluid (CSF), and clinical data, as this was a prospective observational study. The study was not registered as a clinical trial as it did not involve random assignment to interventions. All treatment decisions were made independently by clinicians based on disease severity, antibody profile, and patient-specific factors, in accordance with standard care guidelines. Patient data were anonymized to ensure confidentiality. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Study Design
A prospective observational cohort study was conducted at Renji Hospital from July 2018 to May 2024. The study aimed to compare the efficacy and safety of DFPP and IVMP as first-line immunotherapies for AE. The primary outcome was improvement in the mRS, and secondary outcomes included changes in the CASE and treatment-related adverse events.
Study Subjects
Inclusion Criteria: 1) Diagnosis of AE based on established consensus criteria; 2) Serum and/or CSF positivity for AE-related antibodies; and 3) Treatment with either IVMP or DFPP as initial monotherapy therapy during the acute phase of hospitalization. Exclusion Criteria: 1) Incomplete or uncertain clinical or treatment data; and 2) Receipt of other first-line immunosuppressive therapies (eg, IVIG) or second-line immunotherapy.
Definition of Acute Phase of AE and Treatment Window
The acute phase of AE was defined as the period within the first 4 weeks after symptom onset, characterized by active and progressive neuropsychiatric deficits requiring hospitalization and initiation of first-line immunotherapy. This definition aligns with established consensus guidelines emphasizing the critical importance of early intervention to mitigate neuronal injury and improve long-term outcomes.
The treatment window refers to the timeframe within which first-line immunotherapy (either DFPP or IVMP) was initiated. In this study, all treatments were started within the acute phase (ie, ≤4 weeks from symptom onset). This ensures that the comparative efficacy of the two interventions is evaluated during the period when immunotherapeutic agents are believed to have the greatest impact on disease activity and subsequent recovery.
Immunomodulatory agents such as mycophenolate mofetil (MMF) or azathioprine (AZA) were initiated only after completion of the acute-phase treatment and outcome assessment, and thus did not confound the short-term efficacy evaluation.
Treatment Allocation
Treatment allocation was based on clinical judgment and multidisciplinary team discussion, considering patient-specific factors such as antibody type, disease severity, comorbidities, and patient/family preferences. DFPP was typically considered for patients with moderate to severe disease or those with prominent antibody-mediated features, based on multidisciplinary discussion. Neither random assignment nor blinding was employed, in accordance with the observational design.
Treatment Protocols
DFPP Procedure: Patients underwent 3–5 sessions of DFPP, administered every other day. Plasmapheresis was performed using Plasauto Σ (Asahi Kasei Medical) or KM-9000 (Kawasumi) devices, with Plasmacure™ or Plasmaflo™ as plasma separators and Evaflux™ or Cascadeflo™ EC as component separators. The treated plasma volume was calculated using Nadler’s formula and hematocrit levels, targeting 1.3–1.5 times the total plasma volume. Anticoagulants included unfractionated heparin, low-molecular-weight heparin, or nafamostat mesilate.
IVMP Protocol: Patients received an initial IVMP dose of 480/500 mg/day, tapered by 50% every 3–5 days, followed by oral prednisone acetate (60 mg) with further adjustments based on clinical response.
Outcome Measures
Primary Outcome (Functional Assessment)
Proportion of patients with improved modified Rankin Scale (mRS) scores (ΔmRS = pre-treatment mRS-post-treatment mRS).
Secondary Outcomes (Symptomatic Assessment)
Proportion of patients with improved Clinical Assessment Scale for Autoimmune Encephalitis (CASE) scores (ΔCASE = pre-treatment CASE - post-treatment CASE), and incidence of treatment-related adverse events. Improvement was defined as ΔmRS> 0.
All outcome assessments, including the mRS, CASE and relevant laboratory parameters, were conducted at admission (pre-treatment) and upon completion of the acute treatment phase (post-treatment, typically 7–10 days after treatment initiation). Although assessors were not blinded to treatment allocation, mRS and CASE scores were assessed using standardized criteria to minimize bias.
All unexpected medical events occurring during the treatment period and within 7 days post-treatment were recorded as adverse events. These events were monitored throughout hospitalization and graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. Infections were defined as clinical events necessitating antimicrobial therapy, corroborated by supporting laboratory or imaging findings. A serious adverse event was defined as any event that was fatal, life-threatening, resulted in prolonged hospitalization, or caused significant disability.
Statistical Analysis
Owing to the relative rarity of autoimmune encephalitis, the sample size (N = 38) was determined by the number of eligible cases available during the study period. A post-hoc power analysis confirmed that the sample provided adequate power for the primary comparisons. All statistical analyses were performed using SPSS version 22.0 (IBM Corporation, Armonk, NY). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed data were expressed as mean ± standard deviation (SD) and compared using Student’s t-test; non-normally distributed data were reported as median with interquartile range (IQR) and compared using the Mann–Whitney U-test. Categorical variables were summarized as frequencies and percentages, and group differences were examined using the chi-square test or Fisher’s exact test, as appropriate. For paired comparisons within groups (eg, pre- vs post-treatment), paired t-tests or Wilcoxon signed-rank tests were applied. A complete-case analysis strategy was adopted, whereby patients with missing primary outcome data (mRS at discharge) were excluded.
Multivariable logistic regression was employed to adjust for potential confounding variables, including age, sex, baseline mRS score, antibody type, and treatment group. Variables were included in the model based on clinical relevance and univariate associations (p < 0.1). To evaluate whether baseline disease severity influenced treatment response, an interaction term between treatment group and baseline mRS was incorporated into the regression model. A two-tailed p-value < 0.05 was considered statistically significant. Specific statistical tests used for each outcome are reported in the corresponding Results section. As the subgroup analyses were exploratory in nature, no correction for multiple comparisons was applied, and these findings should be interpreted with caution.
Results
Study Population and Baseline Characteristics
From July 2018 to May 2024, 41 consecutive patients with antibody-confirmed acute-phase AE were prospectively enrolled and allocated to first-line immunotherapy (DFPP: n=24; IVMP: n=17). Three participants discontinued treatment due to intolerance (DFPP: n=2; IVMP: n=1), yielding a final analytic cohort of 38 patients (DFPP: n=22; IVMP: n=16) who completed the therapeutic protocols and outcome assessments. A flowchart of the study is shown in Figure 1.
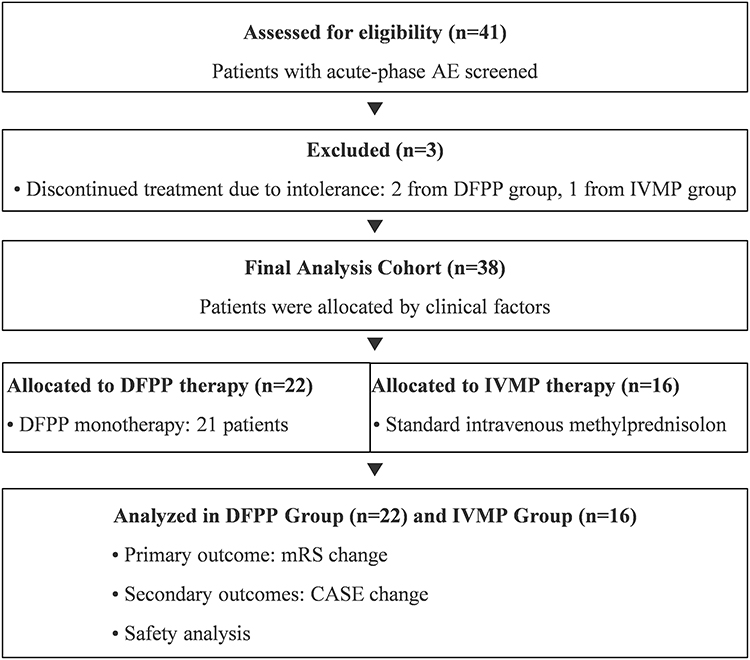 |
Figure 1 A flowchart of the study. |
The median age at onset was 46.00 years (IQR: 27.00–64.25), with 55.3% (21/38) being female. Two patients had coexisting autoimmune diseases (one had systemic lupus erythematosus and the other had autoimmune thyroiditis), and three had tumors. Baseline characteristics were comparable between groups, except for antibody profiles and hospitalization duration. Baseline characteristics and detailed antibody profiles of study participants were showed in Table 1. The IVMP group exhibited a balanced distribution of cell-surface (50%) and intracellular antigens (50%), while the DFPP group had a higher prevalence of cell-surface antibodies (68.2%, p=0.024), including anti-NMDAR encephalitis (40.91% vs 6.25%, p=0.025). Total hospitalization duration was longer in the DFPP group (18.23±0.96 vs 14.81±1.18 days, p=0.029), likely due to procedural requirements.
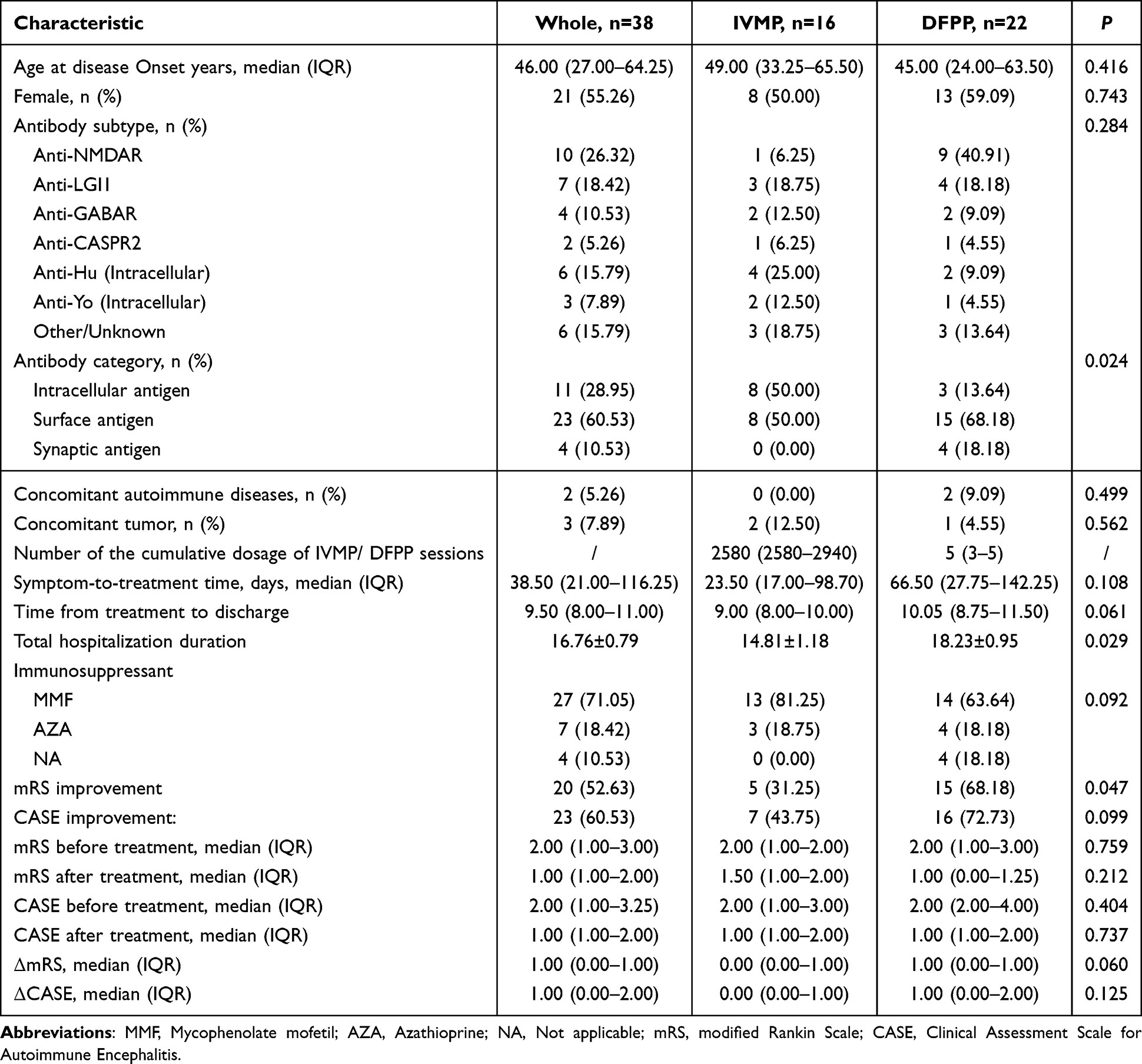 |
Table 1 Baseline Characteristics and Detailed Antibody Profiles of Study Participants |
Treatment Efficacy
Both therapies demonstrated clinical efficacy in the acute phase, with 52.6% (20/38) achieving mRS improvement and 60.5% (23/38) showing CASE score reduction. However, DFPP outperformed IVMP significantly. 1) Functional improvement (change in mRS) (Figure 2A): 68.2% (15/22) of DFPP patients exhibited mRS reduction versus 31.3% (5/16) with IVMP (p=0.047). The median ΔmRS was 1.00 (IQR: 0.00–1.00) for DFPP versus 0.00 (IQR: 0.00–1.00) for IVMP (p=0.060). 2) Symptomatic improvement (change in CASE) (Figure 2B): A trend favored DFPP [72.7% (17/22) vs 43.8% (7/16) p=0.099], with a median ΔCASE of 1.00 (IQR: 0.00–2.00) versus 0.00 (IQR: 0.00–1.00) for IVMP (p=0.125).
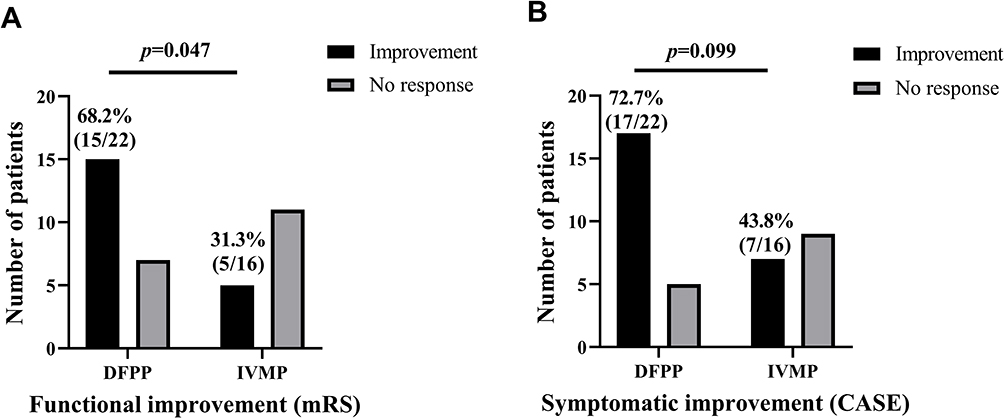 |
Figure 2 Clinical improvement rates. DFPP showed higher mRS improvement (68.2% vs 31.3%, p=0.047) (A) and CASE improvement (72.7% vs 43.8%, p=0.099) (B) than IVMP in the acute phase. Gray bars denote non-responders. |
In our study, univariate analysis was performed using a significance threshold of p < 0.1 to identify potential confounding factors, accounting for the limited sample size. This analysis indicated that baseline mRS (p = 0.056) and treatment type (p = 0.028) were potential determinants of the outcome. Gender and age were included as regular confounding factors in the multivariate analysis. Multivariate logistic regression (Tables 2 and 3) identified DFPP as the sole independent predictor of mRS improvement (OR: 5.234, 95% CI: 1.179–23.235, p=0.030), adjusting for sex, age, baseline mRS, and treatment type.
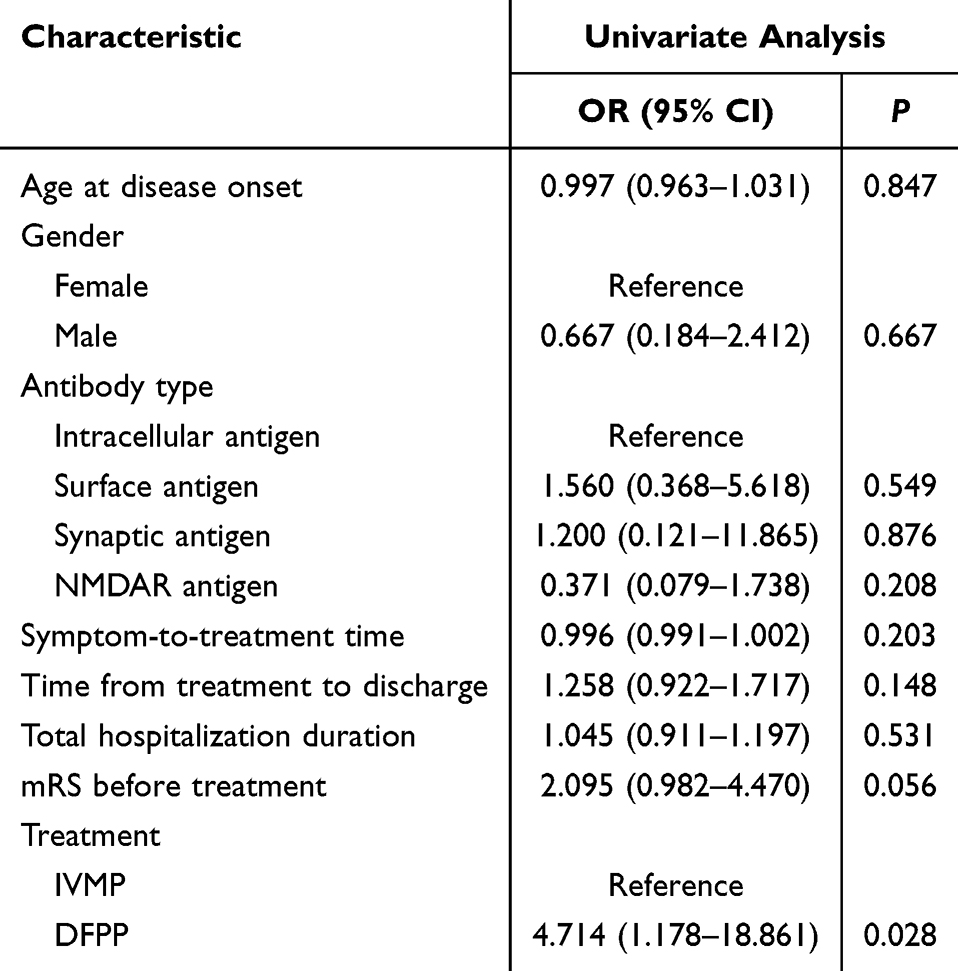 |
Table 2 Univariate Analysis of Treatment Efficacy |
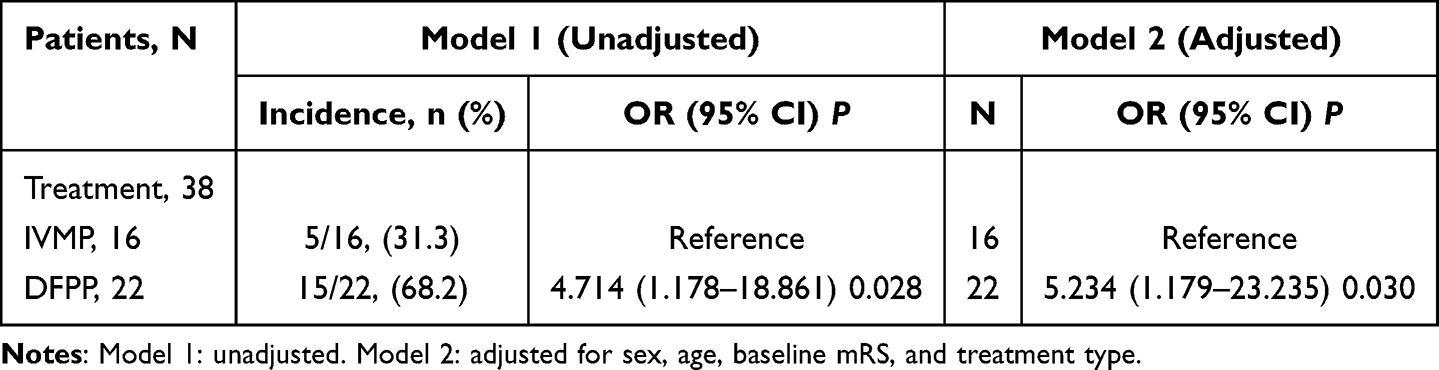 |
Table 3 Multivariate Regression Analysis for Effects of DFPP on Acute Autoimmune Encephalitis |
Subgroup Analysis
Subgroup analyses were performed to evaluate the consistency of treatment effects across different patient populations. Among patients with anti-NMDAR encephalitis—a subgroup of particular interest due to its predominance in the DFPP group—a higher rate of functional improvement (mRS reduction) was observed compared to the IVMP group, consistent with the overall cohort; however, formal statistical comparison was limited by the small sample size. Similarly, analyses based on other antibody subtypes (eg, LGI1, GABAR) suggested a trend toward better outcomes with DFPP, though these did not reach statistical significance. Sensitivity analysis including only patients receiving their first immunotherapy episode (n=32) also showed results aligned with the primary analysis, with DFPP remaining associated with greater improvement in mRS scores (68.2% vs 31.3%, p = 0.047).
Safety Outcomes
No adverse events occurred in the IVMP group. In the DFPP group, three events were reported (13.6% [3/22]), including two cases of deep venous thrombosis (9.09% [2/22]) and one heparin-induced hepatic impairment (4.55% [1/22]), all resolved with anticoagulation or heparin withdrawal. No cases resulted in bleeding, and no treatment discontinuations or serious adverse events occurred.
Discussion
This prospective observational study provides compelling evidence that DFPP may offer superior clinical efficacy compared to IVMP as a first-line immunotherapy for antibody-positive acute-phase AE. Our findings demonstrate that DFPP was associated with significantly higher rates of functional improvement, and a strong trend toward greater symptomatic relief. These results contribute to the growing body of evidence supporting the use of DFPP in AE and highlight the need for further research to optimize treatment strategies.
The observed superiority of DFPP in rapidly removing pathogenic autoantibodies and inflammatory mediators. Unlike conventional TPE, DFPP selectively filters large molecular weight substances, including immunoglobulins and immune complexes, while preserving beneficial plasma components such as albumin.4 This targeted approach may explain the higher efficacy of DFPP in our study, particularly in patients with cell-surface antibody-mediated AE, who constituted the majority of the DFPP group. Previous studies have similarly reported favorable outcomes with TPE in anti-NMDAR encephalitis.14 However, many of these studies evaluated TPE in combination with steroids or IVIG,15–17 complicating the interpretation of its standalone efficacy. In addition, passively acquired autoantibodies may be detected after infusion of IVIG, which may mislead patients.18 Our work addresses this gap by directly comparing DFPP monotherapy with IVMP, thereby minimizing confounding effects from adjunctive treatments.
The differential response rates between DFPP and IVMP may also reflect the distinct pathophysiological mechanisms underlying AE. Cell-surface antibody-mediated AE, which predominated in the DFPP group, is thought to involve reversible neuronal dysfunction driven by humoral immunity, making it particularly amenable to antibody removal via apheresis. In contrast, intracellular antibody-associated AE, more common in the IVMP group, often involves T-cell-mediated cytotoxicity, which may respond better to broad immunosuppression with steroids.19 This hypothesis is supported by the significant intergroup differences in antibody profiles and the higher prevalence of anti-NMDAR encephalitis in the DFPP group. Nevertheless, the multivariate analysis adjusted for these baseline differences, reinforcing the robustness of our findings.
Despite its efficacy in the acute phase, DFPP was associated with a longer total hospitalization duration and a higher incidence of adverse events, including deep venous thrombosis and heparin-induced hepatic impairment. These complications, though manageable, underscore the invasive nature of DFPP and the need for careful patient selection and monitoring.20 The extended hospitalization in the DFPP group likely reflects the logistical demands of apheresis, such as catheter placement and equipment availability, rather than inferior clinical outcomes.21 Future studies should explore strategies to streamline DFPP administration, such as early catheter placement or standardized protocols, to reduce hospitalization times and improve cost-effectiveness.
The discrepancy between mRS and CASE score improvements warrants further discussion. While both scales demonstrated a treatment advantage for DFPP, the effect was statistically significant only for mRS. This may reflect the broader symptom dimensions captured by the CASE score, which includes psychiatric, cognitive, and motor domains, compared to the mRS’s focus on global disability.22 Some patients may exhibit symptomatic improvements (CASE) without achieving a corresponding reduction in disability (mRS), particularly in milder cases. Alternatively, the smaller sample size may have limited the statistical power to detect significant differences in CASE scores. Larger studies with longer follow-up periods are needed to clarify this relationship and assess the durability of treatment effects.23
Our study has several limitations. First, the non-randomized, observational design introduces potential selection bias, as treatment allocation was based on clinical judgment rather than randomization. The predominance of cell-surface antibodies in the DFPP group suggests that clinicians may have favored apheresis for patients perceived to have a higher likelihood of response, potentially inflating the observed treatment effect. Second, the small sample size precluded subgroup analyses by specific antibody types or disease severity, limiting the generalizability of our findings. Third, the prolonged startup time from symptom onset to treatment—median 66.5 days—was influenced by referral delays, diagnostic confirmation, and multidisciplinary decision-making. This delay may have affected treatment outcomes and should be considered when interpreting the results. Fourth, the short-term follow-up period did not allow for assessment of long-term outcomes or relapse rates, which are critical for evaluating the sustained benefits of DFPP. Finally, the single-center design may limit the external validity of our results, particularly in settings with differing apheresis protocols or patient populations.
Despite these limitations, our study adds to the emerging literature supporting the use of DFPP in AE. The findings are consistent with prior reports of apheresis efficacy in refractory AE and extend these observations to first-line treatment. Future research should prioritize multicenter, randomized controlled trials to validate our results and address the limitations of the current study. Key areas for investigation include (1) standardized protocols for DFPP administration, (2) long-term outcomes and relapse rates, (3) cost-effectiveness analyses comparing DFPP with other immunotherapies, and (4) biomarker-driven approaches to predict treatment response. Additionally, studies exploring combination therapies, such as DFPP followed by IVMP or IVIG, may further optimize outcomes for severe or refractory cases.
In conclusion, our study suggests that DFPP is a promising first-line therapy for acute-phase AE, offering superior short-term efficacy compared to IVMP. These findings underscore the importance of early and targeted immunotherapy in AE and highlight the need for further research to refine treatment algorithms and improve patient outcomes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Dr. Yangtai Guan and Dr. Desheng Zhu) upon reasonable request.
Ethics Statement
This study was approved by the Ethics Committee of Renji Hospital, Shanghai Jiao Tong University School of Medicine (LY2024-031-B). Patient data were anonymized to ensure confidentiality. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
The authors thank the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Municipal Commission of Health and Family Planning Foundation of Shanghai Pudong New Area (No. PW2022E-01), the New Quality Clinical Specialties of High-end Medical Disciplinary Construction in Pudong New Area (No. 2024-PWXZ-16), the Interdisciplinary Program of Shanghai Jiao Tong University (No. YG2023LC04), and the Innovative Research Team of High-Level Local Universities in Shanghai [SHSMU- ZDCX20211901].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hiesgen J, Schutte C. Autoimmune encephalitis: part 1 (epidemiology, pathophysiology and clinical spectrum). S Afr Med J. 2023;113(3):116–121. doi:10.7196/SAMJ.2023.v113i3.780
2. Nissen MS, Ryding M, Meyer M, et al. Autoimmune encephalitis: current knowledge on subtypes, disease mechanisms and treatment. CNS Neurol Disord Drug Targets. 2020;19(8):584–598. doi:10.2174/1871527319666200708133103
3. Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165. doi:10.1016/S1474-4422(12)70310-1
4. Hirano R, Namazuda K, Hirata N. Double filtration plasmapheresis: review of current clinical applications. Ther Apher Dial. 2021;25(2):145–151. doi:10.1111/1744-9987.13548
5. Bennani HN, Lagrange E, Noble J, et al. Treatment of refractory myasthenia gravis by double-filtration plasmapheresis and rituximab: a case series of nine patients and literature review. J Clin Apher. 2021;36(3):348–363. doi:10.1002/jca.21868
6. Liu C, Liu P, Ma M, et al. Efficacy and safety of double-filtration plasmapheresis treatment of myasthenia gravis: a systematic review and meta-analysis. Medicine. 2021;100(17):e25622. doi:10.1097/MD.0000000000025622
7. Khatri BO, McQuillen MP, Harrington GJ, et al. Chronic progressive multiple sclerosis: double-blind controlled study of plasmapheresis in patients taking immunosuppressive drugs. Neurology. 1985;35(3):312–319. doi:10.1212/WNL.35.3.312
8. Lin Y, Zhou X, Wu J, et al. Effectiveness of double-filtration plasmapheresis in reducing immunoglobulin and culprit antibody levels in neuroimmune disorders: a single-center retrospective analysis from China. J Neuroimmunol. 2024;396:578463. doi:10.1016/j.jneuroim.2024.578463
9. Zhang L, Liu J, Wang H, et al. Double filtration plasmapheresis benefits myasthenia gravis patients through an immunomodulatory action. J Clin Neurosci. 2014;21(9):1570–1574. doi:10.1016/j.jocn.2013.11.046
10. Heigl F, Hettich R, Arendt R, et al. Immunoadsorption in steroid-refractory multiple sclerosis: clinical experience in 60 patients. Atheroscler Suppl. 2013;14(1):167–173. doi:10.1016/j.atherosclerosissup.2012.10.025
11. Zhang Y, Huang HJ, Chen WB, et al. Clinical efficacy of plasma exchange in patients with autoimmune encephalitis. Ann Clin Transl Neurol. 2021;8(4):763–773. doi:10.1002/acn3.51313
12. Moser T, Harutyunyan G, Karamyan A, et al. Therapeutic plasma exchange in multiple sclerosis and autoimmune encephalitis: a comparative study of indication, efficacy and safety. Brain Sci. 2019;9(10):267. doi:10.3390/brainsci9100267
13. Connelly-Smith L, Alquist CR, Aqui NA, et al. Guidelines on the use of therapeutic apheresis in clinical practice - evidence-based approach from the writing Committee of the American Society for Apheresis: the Ninth Special Issue. J Clin Apher. 2023;38(2):77–278. doi:10.1002/jca.22043
14. Zhang Y, Liu G, Jiang M, et al. Efficacy of therapeutic plasma exchange in patients with severe refractory anti-NMDA receptor encephalitis. Neurotherapeutics. 2019;16(3):828–837. doi:10.1007/s13311-019-00725-4
15. Zhang L, Wu MQ, Hao ZL, et al. Clinical characteristics, treatments, and outcomes of patients with anti-N-methyl-d-aspartate receptor encephalitis: a systematic review of reported cases. Epilepsy Behav. 2017;68:57–65. doi:10.1016/j.yebeh.2016.12.019
16. Suppiej A, Nosadini M, Zuliani L, et al. Plasma exchange in pediatric anti-NMDAR encephalitis: a systematic review. Brain Dev. 2016;38(7):613–622. doi:10.1016/j.braindev.2016.01.009
17. DeSena AD, Noland DK, Matevosyan K, et al. Intravenous methylprednisolone versus therapeutic plasma exchange for treatment of anti-N-methyl-D-aspartate receptor antibody encephalitis: a retrospective review. J Clin Apher. 2015;30(4):212–216. doi:10.1002/jca.21363
18. Uchida Y, Kato D, Adachi K, et al. Passively acquired thyroid autoantibodies from intravenous immunoglobulin in autoimmune encephalitis: two case reports. J Neurol Sci. 2017;383:116–117. doi:10.1016/j.jns.2017.11.002
19. Endres D, Leypoldt F, Bechter K, et al. Autoimmune encephalitis as a differential diagnosis of schizophreniform psychosis: clinical symptomatology, pathophysiology, diagnostic approach, and therapeutic considerations. Eur Arch Psychiatry Clin Neurosci. 2020;270(7):803–818. doi:10.1007/s00406-020-01113-2
20. Grupp C, Beckermann J, Köster E, et al. Relapsing and progressive complications of severe hypertriglyceridemia: effective long-term treatment with double filtration plasmapheresis. Blood Purif. 2020;49(4):457–467. doi:10.1159/000506506
21. Maxted AP, Connell R, Hussain F. Double filtration plasmapheresis - 10-year pediatric experience as an alternative to plasma exchange. Transfus Apher Sci. 2020;59(6):102928. doi:10.1016/j.transci.2020.102928
22. Soellradl E, von Oertzen TJ, Wagner JN. Evaluation of the clinical assessment scale for autoimmune encephalitis (CASE) in a retrospective cohort and a systematic review. Neurol Sci. 2024;45(11):5423–5428. doi:10.1007/s10072-024-07642-1
23. Brenner J, Ruhe CJ, Kulderij I, et al. Long-term cognitive, functional, and patient-reported outcomes in patients with anti-NMDAR encephalitis. Neurology. 2024;103(12):e210109. doi:10.1212/WNL.0000000000210109
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identifying Key Prognostic Indicators for Relapse and Chronic Epilepsy in Autoimmune Encephalitis: Insights from a Multicenter Retrospective Study
Lai Q, Chen Y, Wang W, Lian Z, Liu T, Wen C
Journal of Inflammation Research 2024, 17:11529-11543
Published Date: 24 December 2024