Back to Journals » International Journal of Women's Health » Volume 18
Double-Balloon Catheter Alone or Combined with Oxytocin, Dinoprostone, or Misoprostol for Labor Induction in Late- and Post-Term Pregnancies: A Retrospective Cohort Study
Authors Kükrer S ![]() , Gülümser Ç, Arlıer S, Yücel N
, Gülümser Ç, Arlıer S, Yücel N
Received 2 February 2026
Accepted for publication 11 May 2026
Published 18 May 2026 Volume 2026:18 600653
DOI https://doi.org/10.2147/IJWH.S600653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Sadık Kükrer,1 Çağrı Gülümser,2 Sefa Arlıer,1 Neşe Yücel1
1Department of Obstetrics and Gynecology, University of Health Sciences, Adana City Training and Research Hospital, Adana, Turkey; 2Department of Obstetrics and Gynecology, Yuksek Ihtisas University, Ankara, Turkey
Correspondence: Sadık Kükrer, Email [email protected]
Purpose: To compare the effectiveness and safety of double-balloon catheter (DBC) alone or combined with oxytocin, dinoprostone, or misoprostol for labor induction in late- and post-term pregnancies with unfavorable cervices.
Patients and Methods: This single-center retrospective cohort study included 1022 women with singleton cephalic pregnancies at ≥ 41 weeks’ gestation and a Bishop score ≤ 6 who underwent induction between November 2017 and February 2025. Women were managed with DBC alone (n=234), DBC plus oxytocin (n=246), DBC plus dinoprostone (n=238), or DBC plus misoprostol (n=304). The primary outcomes were induction-to-delivery interval, vaginal delivery within 24 hours, and delivery mode; secondary outcomes included maternal and neonatal complications. Group comparisons, Kaplan-Meier analysis, and multivariable regression were performed.
Results: Induction outcomes differed significantly among protocols. Time-to-event analysis showed the shortest median time to vaginal delivery with DBC plus misoprostol (14.9 hours) and the longest with DBC plus dinoprostone (19.4 hours). Vaginal delivery within 24 hours was most frequent with DBC plus misoprostol and DBC alone. DBC plus dinoprostone had the highest cesarean delivery rate. Maternal complications were more frequent with DBC plus misoprostol, particularly uterine hyperstimulation, intrapartum fever/clinical chorioamnionitis, postpartum atony, and blood transfusion. Neonatal outcomes were largely comparable, although umbilical artery pH was slightly lower in the DBC plus misoprostol group. Estimated fetal weight was the only independent predictor of cesarean delivery.
Conclusion: Among DBC-based induction strategies, DBC plus misoprostol appeared most efficient but had a less favorable maternal safety profile. DBC plus oxytocin offered the most balanced effectiveness-safety profile, whereas DBC plus dinoprostone was associated with slower labor progression and less favorable operative outcomes. Protocol selection should be individualized according to maternal risk, urgency of delivery, and available intrapartum monitoring capacity.
Plain Language Summary: Why was this Study Done?
When pregnancy continues beyond 41 weeks, doctors often need to induce labor to reduce risks for the mother and baby. One common method uses a double-balloon catheter, which gently opens the cervix. This method can be used alone or together with medicines such as oxytocin, dinoprostone, or misoprostol. However, it is still unclear which approach gives the best balance between effectiveness and safety.
What did the Researchers Do?
We studied 1,022 women with pregnancies of 41 weeks or more who needed labor induction. We compared four approaches: double-balloon catheter alone, double-balloon catheter with oxytocin, double-balloon catheter with dinoprostone, and double-balloon catheter with misoprostol. We examined delivery timing, vaginal birth within 24 hours, cesarean delivery, and complications in mothers and neonates.
What did the Researchers Find?
The double-balloon catheter with misoprostol was linked with the shortest median time to vaginal birth and a high rate of vaginal birth within 24 hours. However, this group also had more maternal complications, including abnormal uterine contractions, fever or infection during labor, poor uterine contraction after birth, and blood transfusion. The double-balloon catheter with oxytocin showed the most balanced pattern between effectiveness and safety. The double-balloon catheter with dinoprostone was linked with slower labor progress and more cesarean deliveries.
What do these Results Mean?
For women needing labor induction after 41 weeks, the best method may depend on maternal risk, urgency of delivery, and the hospital’s ability to monitor labor closely. Infographic on late-term pregnancy induction: efficiency, morbidity and cesarean predictors.The infographic presents a study on induction protocols for late- and post-term singleton cephalic pregnancies with a Bishop score of 6 or less, involving 1,022 cases in a retrospective cohort study. Four induction protocols are compared: DBC alone (234 cases), DBC plus oxytocin (246 cases), DBC plus dinoprostone (238 cases) and DBC plus misoprostol (304 cases). Comparative findings show DBC plus misoprostol has the greatest efficiency but highest maternal morbidity. DBC plus oxytocin is effective with a balanced profile. DBC plus dinoprostone is a pharmacomechanical option. Clinical messages highlight misoprostol’s efficiency and oxytocin’s balanced profile. Protocol choice should balance efficiency, safety and monitoring. Higher estimated fetal weight is the only independent predictor of cesarean delivery.
Keywords: labor induction, prolonged pregnancy, balloon catheter, misoprostol, dinoprostone, oxytocin
Introduction
Induction of labor (IOL) is one of the most common obstetric interventions, performed in approximately 10% of births worldwide and nearly one in four births in high-income countries.1–3 Its use has steadily increased over the past few decades, driven by broader maternal–fetal indications and greater acceptance among patients and clinicians.2–5 Clinical guidelines recommend IOL when the risks of continuing pregnancy exceed those of delivery, particularly in conditions such as hypertensive disorders, diabetes, fetal growth restriction, and pregnancies that reach or surpass the term.6
Late-term (41+0 to 41+6 weeks) and post-term (≥42 weeks) pregnancies are the primary indications for IOL because of their association with adverse outcomes including macrosomia, shoulder dystocia, oligohydramnios, meconium aspiration, and increased perinatal mortality.7–9 Timely induction in these scenarios is essential to reduce morbidity while minimizing unnecessary cesarean deliveries.10
Cervical favorability, most often assessed using the Bishop score, is a key determinant of IOL success.7,8,11 An unfavorable cervix, present in up to half of the women, is associated with prolonged labor, failed induction, and higher rates of cesarean delivery.12 Cervical ripening can be achieved through pharmacological methods, such as dinoprostone (PGE2) and misoprostol (a PGE1 analog), or mechanical approaches, most commonly transcervical balloon catheters.2,13,14
Pharmacological and mechanical ripening methods differ not only in their mechanisms of action but also in their clinical balance between effectiveness and safety. Prostaglandins such as dinoprostone and misoprostol may accelerate cervical ripening and increase uterine activity, thereby shortening the induction-to-delivery interval and increasing the likelihood of vaginal delivery within 24 hours. However, this greater pharmacologic potency may be accompanied by higher rates of uterine tachysystole, non-reassuring fetal heart rate patterns, intrapartum fever, and postpartum uterine atony.13,15 In contrast, mechanical methods, particularly the double-balloon catheter (DBC), are generally associated with lower rates of uterine hyperstimulation but may require additional oxytocin augmentation and longer labor monitoring.16–18 Therefore, the choice of induction protocol should not be based solely on delivery speed, but should also account for maternal safety, fetal surveillance capacity, and the clinical urgency of delivery.
Current international guidelines support an individualized approach to labor induction that accounts for cervical favorability, maternal and fetal risk, prior uterine surgery, resource availability, and monitoring capacity. The World Health Organization has issued updated recommendations on mechanical methods for inducing labor, including balloon catheter-based approaches, and emphasizes their role in developing national and local protocols.19 NICE recommends dinoprostone or low-dose oral misoprostol for women with a Bishop score of 6 or less, while also advising that mechanical methods, including balloon catheters, should be considered when pharmacological methods are unsuitable, when the risk of hyperstimulation is clinically relevant, or when the woman prefers a mechanical method.20 NICE further notes that pharmacological induction requires regular assessment of uterine activity and fetal condition, that both dinoprostone and misoprostol may cause hyperstimulation, and that mechanical methods are less likely to cause hyperstimulation than pharmacological methods.20 ACOG likewise recognizes cervical ripening with prostaglandins or balloon catheter devices when the cervix is unfavorable and recommends oxytocin and amniotomy as evidence-based strategies during induction or augmentation when clinically appropriate.10,16 These recommendations support the clinical relevance of comparing DBC alone and DBC combined with oxytocin, dinoprostone, or misoprostol in late- and post-term pregnancies with unfavorable cervices.
Recent studies have explored combination regimens that leverage the complementary effects of mechanical dilation and pharmacological stimulation.9,15,16 Combining balloon catheters with oxytocin or prostaglandins can shorten labor and increase the likelihood of vaginal delivery within 24 hours.12,18 However, most evidence comes from heterogeneous study populations and indirect network meta-analyses, with limited head-to-head data specifically focusing on late- and post-term pregnancies with unfavorable cervices. In particular, misoprostol-based regimens have been linked to higher maternal morbidity, especially tachysystole and fever.9,21,22
Given these uncertainties, the optimal induction strategy for late- and post-term pregnancy remains unclear.1,3,23,24 We conducted a retrospective cohort study to compare the efficacy and safety of four DBC-based protocols: DBC alone, DBC with oxytocin, DBC with dinoprostone, and DBC with misoprostol. We hypothesized that DBC combined with misoprostol would be associated with the greatest induction efficiency but a less favorable maternal safety profile, whereas DBC alone and DBC combined with oxytocin would show a more balanced effectiveness-safety profile.
Materials and Methods
Study Design
This was a single-center retrospective cohort study. This retrospective cohort study was conducted to evaluate the efficacy and safety of labor induction methods in real-world clinical settings. The study was conducted between November 1, 2017, and February 15, 2025, at the obstetrics and gynecology clinic of a university hospital with a tertiary reference perinatology unit. This retrospective design enabled a large sample size and multivariate analyses, providing an appropriate methodological framework for evaluating the comparative effectiveness of different induction protocols.
Ethical Approval
The study protocol was approved by the Institutional Ethics Committee of the Health Sciences University, Adana Faculty of Medicine (approval date: March 6, 2025; Decision no. 422). All procedures followed the principles of the Declaration of Helsinki and the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. At our institution, written informed consent for medical treatment, surgical intervention, and the use of anonymized clinical data for research was routinely obtained from all patients or their legally authorized representatives at the time of hospitalization.
Participants
The inclusion criteria were maternal age 20–40 years, gestational age ≥41 weeks (including both late-term pregnancies, defined as 41 weeks and 0–6 days, and post-term pregnancies, defined as 42 weeks and beyond), singleton pregnancy with a live fetus in cephalic presentation, a Bishop score ≤6, and a documented indication for induction of labor. The exclusion criteria included planned elective cesarean section, cervical insufficiency, a history of previous uterine surgery (including cesarean section or myomectomy), multiple pregnancy, major fetal anomaly, contraindications to prostaglandins or oxytocin, active vaginal bleeding or placenta previa, incomplete medical records, maternal body mass index (BMI) less than 18.5 kg/m² (underweight) or ≥40.0 kg/m² (class III obesity), maternal hemoglobin level <10 g/dL, and estimated fetal birth weight >4000 g.
The Bishop score was assessed at admission using five standard parameters: cervical dilatation, effacement, position, consistency, and fetal head station.25,26 Gestational age was calculated from the last menstrual period and was confirmed by ultrasonography during the first trimester.15,27
Data Collection Process
Data were retrospectively extracted from the hospital’s electronic medical records system using a standardized data collection form. The recorded variables included maternal demographics (age, height, weight, and body mass index), obstetric history (gravidity, parity, and prior delivery mode), pregnancy characteristics (gestational age, initial Bishop score, and estimated fetal weight), indications and methods of induction, labor parameters (time to active phase, total labor duration, and stage duration), maternal complications (tachysystole, intrapartum fever, chorioamnionitis, postpartum hemorrhage, and uterine atony), and neonatal outcomes (Apgar score, umbilical arterial pH, and NICU admission).
In total, 1,088 women were initially evaluated for eligibility. However, 66 patients were excluded owing to incomplete medical records, leaving 1,022 patients for the final analysis. Women were allocated to four induction protocol groups: double-balloon catheter (DBC) alone (n = 234), DBC plus oxytocin (n = 246), DBC plus dinoprostone (n = 238), and DBC plus misoprostol (n = 304). Figure 1 illustrates the flow of the participants from the initial assessment to the final analysis.
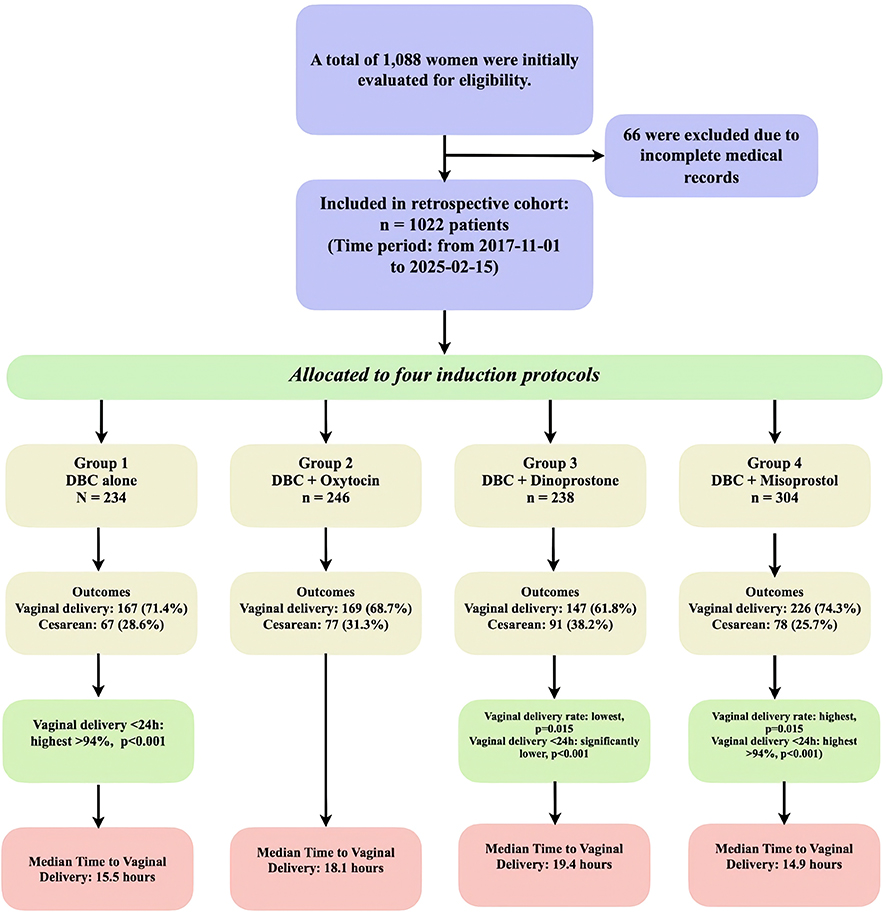 |
Figure 1 Flow diagram of participant enrollment, eligibility assessment, exclusions, allocation to induction protocols, and delivery outcomes. The diagram shows the number of women initially assessed for eligibility, excluded due to incomplete medical records, and included in the final analysis according to the induction protocol. |
Relationship to Prior Published Analysis
A related analysis from the same institutional induction database has been published previously.28 That study focused on women who achieved vaginal delivery after DBC-based induction and evaluated predictors of prolonged labor and timely vaginal delivery. The present study addresses a distinct comparative effectiveness and safety question by including the full eligible induction cohort, including cesarean deliveries, and by comparing DBC alone and DBC combined with oxytocin, dinoprostone, or misoprostol with respect to labor efficiency, delivery mode, maternal morbidity, and neonatal outcomes.
Classification According to Induction Protocol
Because of the retrospective cohort design, participants were not randomly assigned to induction protocols. The four study groups were defined according to the induction regimen documented in the electronic medical records: DBC alone, DBC plus oxytocin, DBC plus dinoprostone, or DBC plus misoprostol. Protocol selection was performed as part of routine clinical care and reflected institutional practice, cervical status at admission, maternal and fetal clinical characteristics, contraindications to pharmacological agents, urgency of delivery, intrapartum monitoring capacity, and the attending obstetrician’s clinical judgment. No intervention was assigned for research purposes. To reduce selection bias, uniform eligibility and exclusion criteria were applied across all groups; baseline maternal, obstetric, cervical, and fetal characteristics were compared across the four protocols; and multivariable models were adjusted for clinically relevant covariates. Nevertheless, because treatment selection was non-randomized, residual confounding and confounding by indication cannot be excluded.
A Cook Medical (Bloomington, IN, USA) double-balloon catheter was transcervically inserted in all the groups. The uterine balloon was inflated with 40 mL of sterile saline, and the vaginal balloon was inflated with 20 mL of sterile saline, in accordance with our institutional protocol, to reduce patient discomfort and minimize the risk of premature expulsion. Although the Cook double-balloon catheter allows inflation of up to 80 mL per balloon, our institution routinely uses a lower initial volume. The catheter was left in place for up to 12 h or until spontaneous expulsion.3,11
In the DBC + oxytocin group, intravenous oxytocin was initiated after catheter removal or expulsion if uterine activity was inadequate (defined as <3 contractions per 10 min for 30–60 min). A low-dose titration protocol was used, in which the infusion was started at 1–2 mU/min and increased by 1–2 mU/min at 15–30-minute intervals, up to a maximum of 20 mU/min.18,29 The infusion was adjusted to maintain 3–5 contractions per 10 min and was reduced or discontinued in the presence of tachysystole or non-reassuring fetal heart rate patterns.18,29
In the DBC + Dinoprostone group, a 10 mg controlled-release vaginal insert (Propess®, Ferring Pharmaceuticals) was placed immediately after catheter insertion.6,8 In the DBC + Misoprostol group, 25–50 µg of vaginal misoprostol was administered every 4–6 h during catheter placement, for a maximum of four doses (total cumulative dose ≤200 µg), or until the catheter was expelled or active labor was established, whichever occurred first.6
Timing of Measurements and Follow-Up
All women underwent continuous electronic fetal monitoring (c-EFM) from the start of induction until delivery. Uterine activity was assessed using external tocodynamometry, and an intrauterine pressure catheter was used at the clinician’s discretion when external tracing quality was inadequate. Amniotomy was performed when clinically appropriate, defined as cervical dilatation ≥3 cm with reassuring fetal status and engaging in a cephalic presentation.30 Intrauterine pressure catheters were used when external tocodynamometry tracings were inadequate for evaluating uterine activity or when oxytocin titration required precise monitoring of uterine contractions.
Operational Definitions
In our unit, the active phase of labor was defined as cervical dilation of ≥4 cm with regular contractions, consistent with several earlier studies on induced labor.11,31 Active phase arrest was defined as a lack of cervical dilation progress for ≥4 hours despite adequate uterine activity.17,29,32 Several contemporary guidelines recommend a threshold ≥6 cm to define the active phase.29,33,34 This difference represents a methodological limitation that may affect the comparability of our results with those of other studies and should be considered when interpreting our time-to-delivery results.
Uterine tachysystole was defined as more than five contractions in 10 min, averaged over a 30-minute window.16 When associated with non-reassuring fetal heart rate (FHR) patterns, management includes reducing or ceasing oxytocin and implementing intrauterine resuscitation measures per unit protocol.32
Postpartum hemorrhage (PPH) was quantitatively measured in all vaginal and cesarean deliveries. Blood loss was recorded in milliliters and not visually estimated. PPH was defined as >500 mL after vaginal birth or >1000 mL after cesarean delivery.13 The blood transfusion requirements were documented as separate safety outcomes.13
Endpoints and Subgroup Analyses
The primary endpoints of the study were the rate of vaginal delivery within 24 hours of induction, induction-to-delivery interval (calculated from catheter insertion to delivery), and mode of delivery (vaginal or cesarean). The secondary end points encompassed a wide range of maternal and neonatal outcomes. Maternal process outcomes included the time from induction to the onset of active labor, duration of the first and second stages, changes in the Bishop score, and need for oxytocin augmentation after catheter removal or expulsion. Maternal safety outcomes included tachysystole with non-reassuring fetal heart rate changes, intrapartum fever, clinical chorioamnionitis, postpartum uterine atony, quantitative measurement of postpartum hemorrhage, need for blood transfusion, and length of hospitalization. Intrapartum fever was defined as a maternal temperature of ≥38.0 °C on two occasions at least 30 min apart or ≥39.0 °C on one occasion.1 Clinical chorioamnionitis was defined as intrapartum fever plus at least one of the following: uterine tenderness, maternal tachycardia (>100 beats/min), fetal tachycardia (>160 beats/min), or malodorous amniotic fluid.16,35 These standardized definitions were used to enhance the reproducibility and comparability of the studies. Neonatal outcomes included the 5-minute Apgar score (and the proportion with a score <7), presence of meconium-stained amniotic fluid, umbilical arterial pH, admission to the neonatal intensive care unit, and need for respiratory support, either continuous positive airway pressure or endotracheal intubation.
Subgroup analyses were performed for nulliparous versus multiparous women, and for patients with low (≤3) versus high (4–6) baseline Bishop scores. Maternal and neonatal complications were monitored for the first 24 h after delivery. The length of hospital stay was defined as the interval between delivery and discharge.
Statistical Analysis
All analyses were performed using Jamovi (version 2.6.44; The Jamovi Project, 2023) and JASP (version 0.19.3; JASP Team, 2024). Statistical significance was set at a two-sided p-value ≤0.05. Continuous variables were assessed for normality using the Shapiro–Wilk test and visual inspection of histograms. As most variables were non-normally distributed, they were reported as medians [minimum–maximum] and compared using the Kruskal–Wallis H-test. When overall differences were significant, the Dwass–Steel–Critchlow–Fligner post hoc test was applied. Categorical variables are summarized as frequencies (percentages) and analyzed using Pearson’s chi-square test or Fisher’s exact test (Fisher–Freeman–Halton test, where appropriate). Bonferroni correction was applied for pairwise post-hoc comparisons, and statistically different groups are indicated with superscript letters in the tables.
Changes in hemoglobin values (prepartum minus postpartum) and fetal arterial blood pH were compared across groups using non-parametric tests. Binary outcomes, such as vaginal delivery within 24 h, cesarean delivery, and maternal–neonatal complications, were compared using the Chi-square or Fisher’s exact test.
Four regression models were developed to identify the predictors of key labor outcomes. Logistic regression was used to determine the predictors of cesarean delivery, whereas linear regression was used to assess factors associated with the time from catheter insertion to the onset of active labor and the total induction-to-delivery interval. Additionally, logistic regression was performed to identify predictors of the need for oxytocin augmentation. These models were adjusted for potential confounders and the robustness of the associations was confirmed using sensitivity analyses.
The non-normally distributed dependent variables in Models 2 and 3 are log-transformed. Variables with p<0.10 in the univariable analysis and clinically relevant covariates were entered into multivariable models. Multicollinearity was assessed using Spearman correlation and the variance inflation factor (VIF). Because maternal age and BMI were highly correlated (Spearman’s r = 0.597, p < 0.001; VIF > 4), they were evaluated using separate models. Logistic regression models were fitted using either the enter method (Model 1) or backward stepwise likelihood ratio method (Model 4). Model fit was assessed using the Hosmer–Lemeshow test, and model performance was evaluated using Nagelkerke R² and classification accuracy. The linear regression assumptions of normality, homoscedasticity, and absence of autocorrelation were checked. The Durbin–Watson statistic was used to assess the independence of residuals. Multicollinearity was evaluated using correlation coefficients and variance inflation factors (VIF). Because of the high collinearity between maternal age and BMI, these variables were modeled separately. The analyses were based on complete cases as no missing data were present in the final cohort (n = 1,022). Statistical significance was set at p < 0.05. Although Bonferroni correction was applied to control for Type I error, the large sample size ensured >95% power, thereby minimizing the risk of Type II error.
Time-to-event outcomes were analyzed using the Kaplan–Meier method. The time of origin (t < ry >) was defined as the time of DBC insertion, and the event was described as vaginal delivery. Women who underwent cesarean delivery were right censored at the time of the procedure. Between-group comparisons were performed using the Log rank test, and post-hoc pairwise Log rank tests were conducted when the overall significance was observed. The median times, 95% confidence intervals, and numbers at risk are reported for each group.
Sample Size Calculation
Sample size estimation was based on the network meta-analysis by Orr et al36 reported reductions in induction-to-delivery time for combination therapies compared with the Foley catheter alone (−4.2 hours for Foley + oxytocin, −4.5 hours for Foley + misoprostol, and −2.1 hours for Foley + dinoprostone). Assuming an intergroup standard deviation of 1.8 h and within-group standard deviation of 6–15 h, the calculated Cohen’s f effect size ranged from 0.12 0.30. A one-way ANOVA power analysis (four groups, α = 0.05, power = 0.80) indicated that 31–188 participants were required per group. To account for the Kruskal–Wallis test’s lower relative efficiency compared with ANOVA (90%), the required sample size was increased by 10%, yielding a range of 35–209 participants per group (total: 140–836 participants). Assuming a moderate within-group standard deviation of 10 hours (Cohen’s f = 0.18), at least 94 patients per group (total n = 376) were required. With 1,022 women in the final cohort (the smallest group, comprising 234 patients), the study had more than 95% power to detect clinically meaningful differences of 2–4 h in the induction-to-delivery intervals.
Results
Maternal Characteristics
Among the 1,022 eligible women, 234 were managed with a double-balloon catheter (DBC) alone (group 1), 246 with DBC+oxytocin (group 2), 238 with DBC+dinoprostone (group 3), and 304 with DBC+misoprostol (group 4) (participant flow in Figure 1). Maternal age, weight, gravidity, and parity were similar between groups (Table 1). Maternal height and BMI differed significantly among the groups (p<0.001). Group 3 had a slightly higher median height (173 cm) and a correspondingly lower BMI (29.1 kg/m²). These differences, although statistically significant, were minor and may have limited clinical impact. Nulliparity was evenly distributed in groups 1 (41.0%, 96/234) in Group 1, 41.1% (101/246) in Group 2, 41.2% (98/238) in Group 3, and 41.1% (125/304) in Group 4 (p=0.999). Gestational age at delivery showed modest but statistically significant differences across the groups (p=0.044). (Table 1)
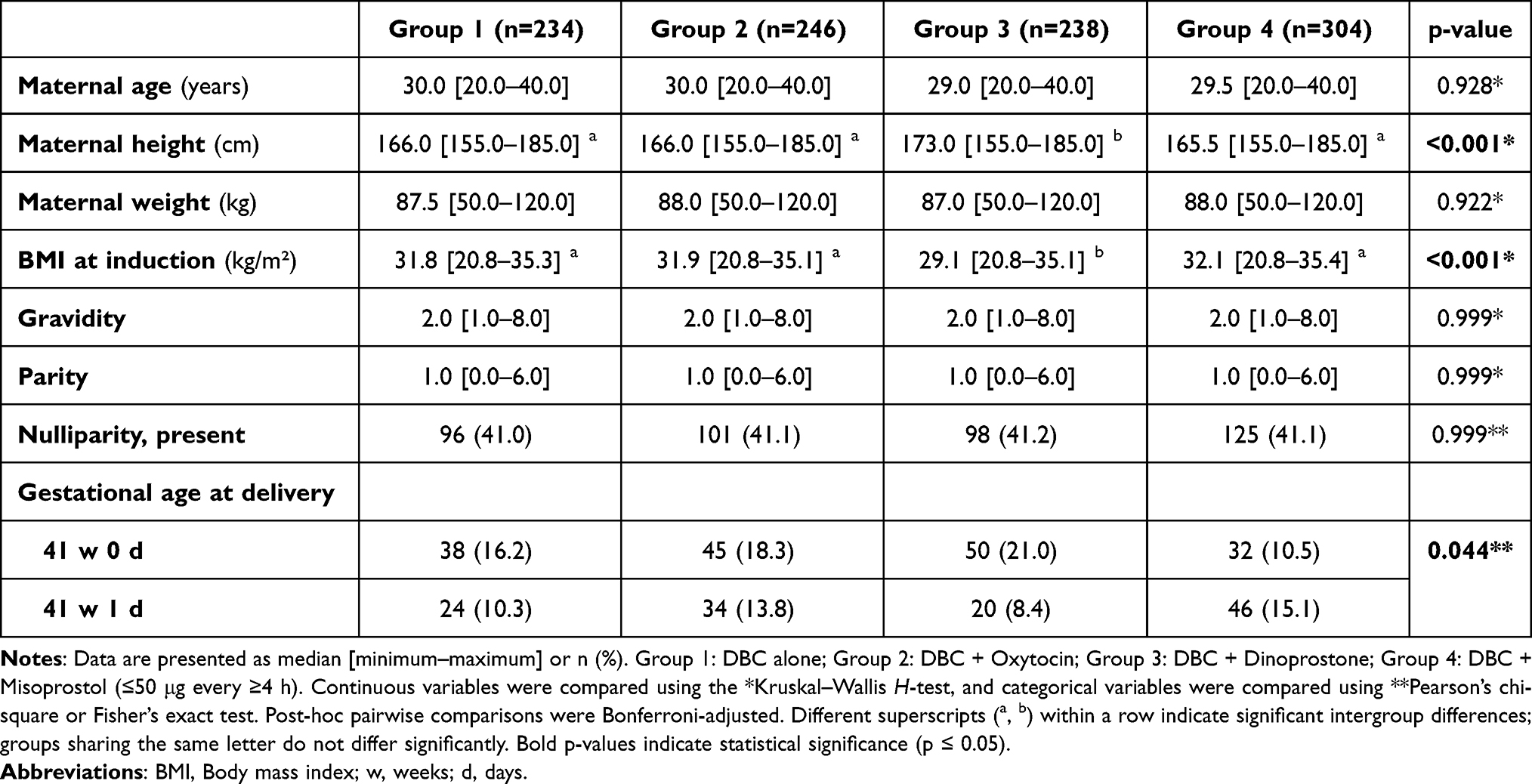 |
Table 1 Maternal Demographic Characteristics and Gestational Age Distribution Among Pregnant Women Undergoing Labor Induction: A Comparative Analysis of Study Groups |
Pre-Induction Obstetric Parameters and Bishop Components
The pre-induction obstetric characteristics were comparable between the groups (Table 2). The rate of post-term pregnancy was consistent, affecting approximately one-quarter of the participants in each group (p=0.999). Cervical dilatation at admission varied significantly (p=0.001), with 67.5% (166/246) of the women in the DBC+oxytocin group presenting with a closed cervix. The median initial Bishop score was the lowest in the DBC + misoprostol group (2.0, p=0.007). When categorized, a Bishop score ≤3 was most common in the DBC+oxytocin group (59.8%, 147/246) and least frequent in the DBC-alone group (44.4%, 104/234; p=0.002). In contrast, the change in the Bishop score after cervical ripening did not differ significantly among the groups (p=0.905).
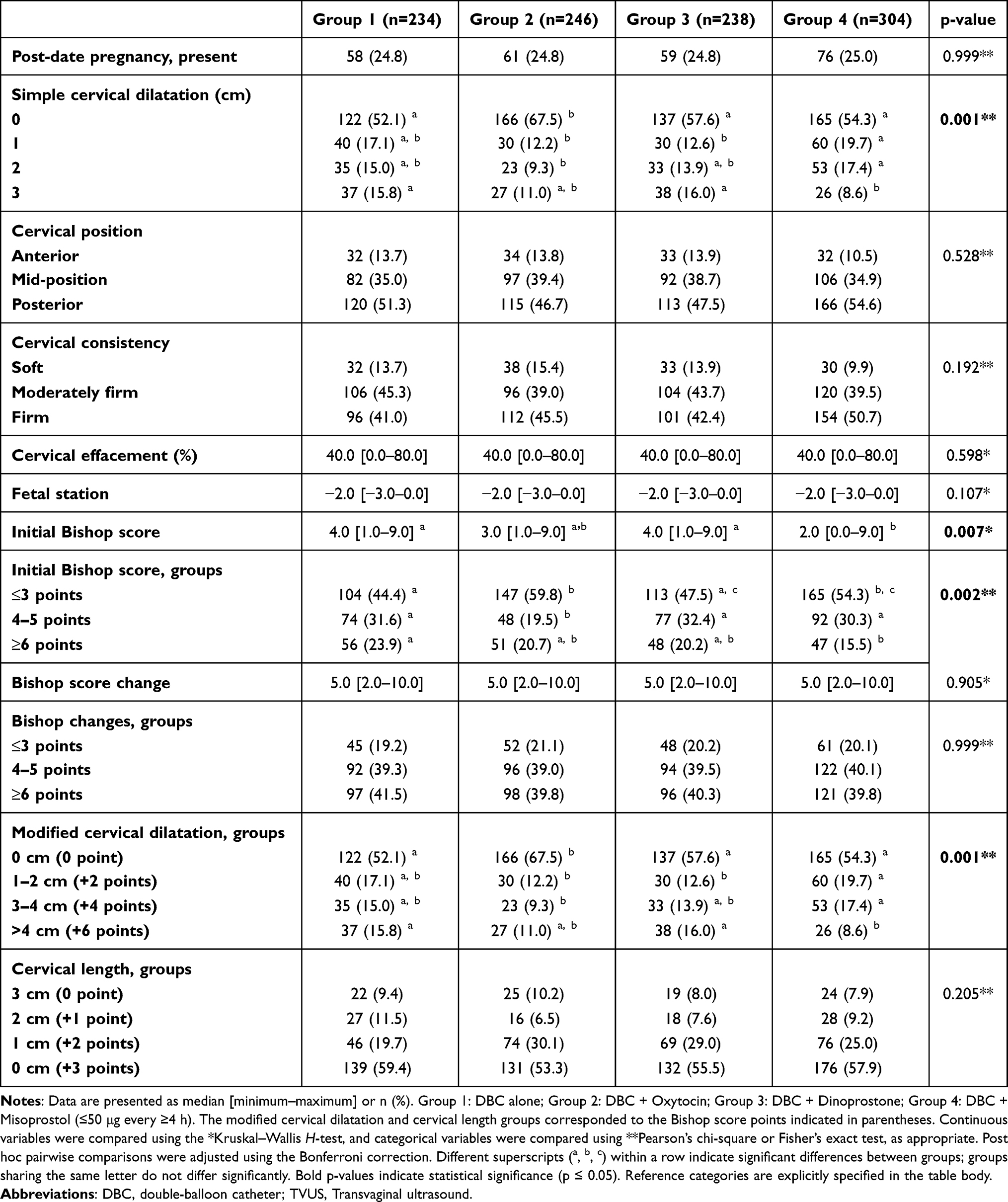 |
Table 2 Pre-Induction Obstetric Parameters and Bishop Components: A Cross-Group Evaluation of Baseline Characteristics |
Induction Process and Obstetric Outcomes
Labor progression parameters differed significantly between the groups (Table 3). The median time from insertion to active labor was 6.5 h in the DBC+misoprostol group and 9.7 h in the DBC + dinoprostone group (p<0.001). The total induction-to-delivery interval was 9.8 h in the DBC+misoprostol group and 14.9 h in the DBC+dinoprostone group (p<0.001). Pairwise post-hoc analyses (Bonferroni-adjusted) confirmed that the DBC+misoprostol group had a significantly shorter interval, whereas the DBC+dinoprostone group had the longest interval. The first and second stages also differed substantially between groups (both p<0.001). Vaginal delivery within 24 h occurred in 94.6% (DBC alone), 88.2% (DBC+oxytocin), 78.9% (DBC+dinoprostone), and 94.7% (DBC+misoprostol) (p<0.001).
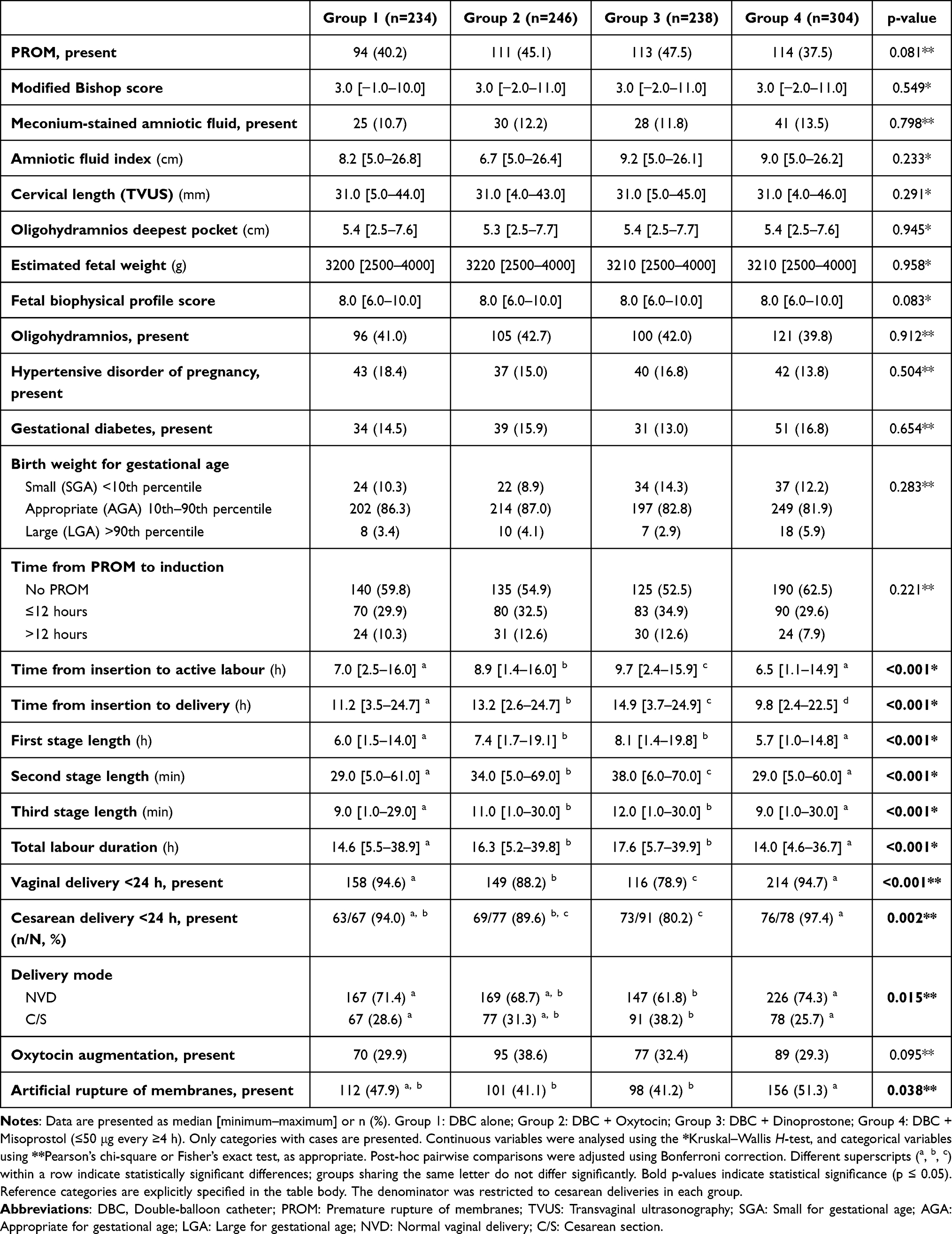 |
Table 3 Induction Process, Labor Progression, and Delivery Outcomes Across Study Groups: A Comprehensive Intergroup Analysis |
Maternal and Neonatal Complications
Maternal complications differed significantly between the groups (Table 4). Uterine hyperstimulation occurred in 22.7% of the DBC+misoprostol group and 5.7% of the DBC+oxytocin group (p<0.001). Intrapartum fever/clinical chorioamnionitis was 12.8% in the DBC+misoprostol group and ≤9% in the other groups (p=0.020). Postpartum uterine atony was 10.9% in the DBC+misoprostol group and 4.9% in the DBC+oxytocin group (p=0.041), and blood transfusions ranged from 3.7% (DBC+oxytocin) to 8.9% (DBC+misoprostol) (p=0.035). Prepartum hemoglobin values ranged from a median of 11.8 g/dL (DBC alone) to 12.1 g/dL (DBC+dinoprostone) (p=0.001), and postpartum hemoglobin ranged from 11.0 g/dL (DBC+misoprostol) to 11.3 g/dL (DBC+dinoprostone) (p<0.001), with minor absolute differences (<0.5 g/dL). The median maternal length of stay was 4.3 days in the DBC+misoprostol group and 3.4 days in the DBC+oxytocin group (p<0.001). Neonatal outcomes were broadly similar; umbilical arterial pH was lower in the DBC+misoprostol group (median 7.3; p<0.001), while the rates of 5-minute Apgar score <7, respiratory support, and NICU admission did not differ significantly (all p>0.3).
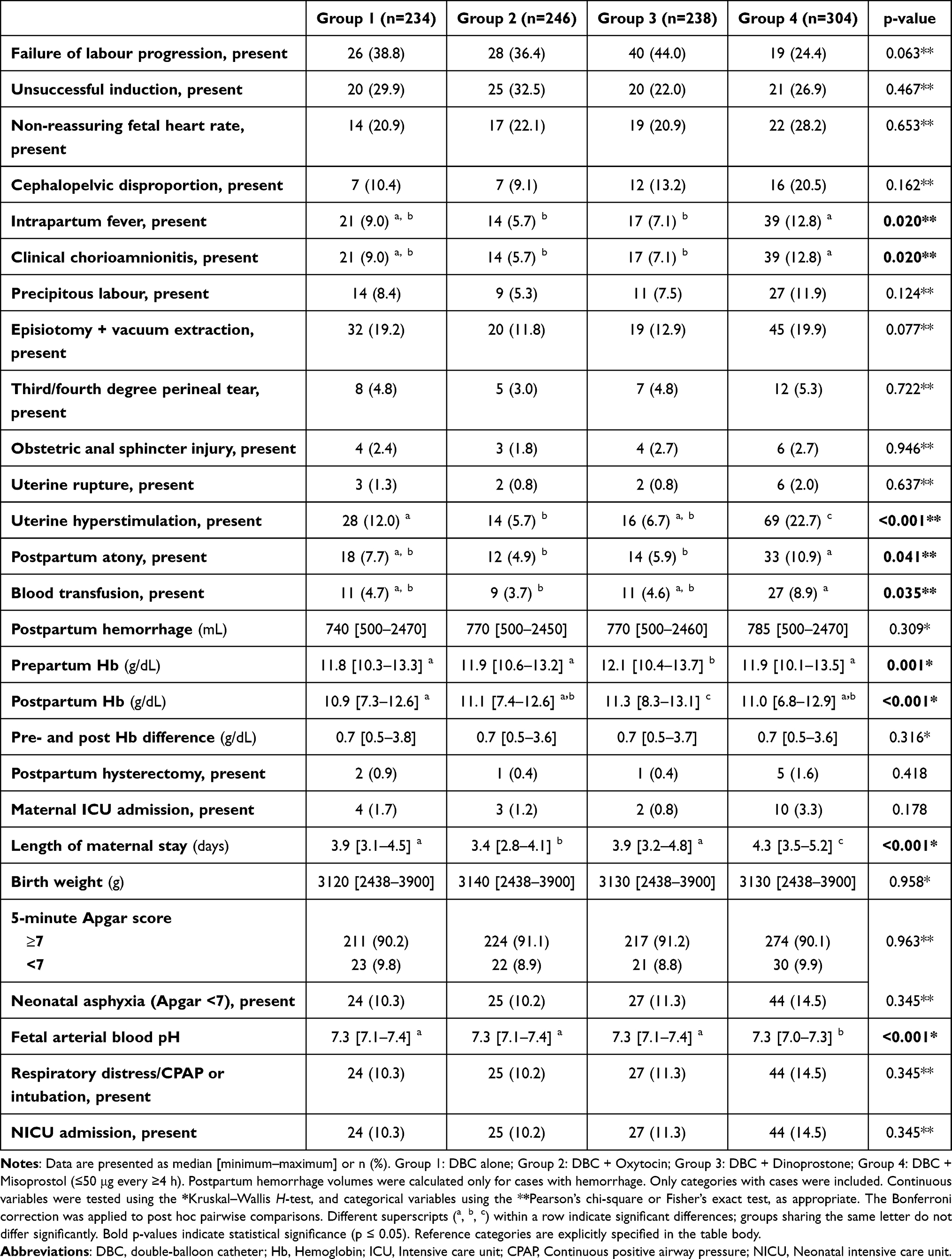 |
Table 4 Maternal Complications and Neonatal Outcomes in the Study Groups |
Predictors of Cesarean Delivery
Multivariable logistic regression identified estimated fetal weight (per 100 g increase) as the only independent predictor of cesarean delivery (Table 5; aOR, 1.01; 95% CI: 1.00–1.02; p<0.001). Maternal BMI, initial Bishop score, and parity were not significant factors after adjusting for the other variables.
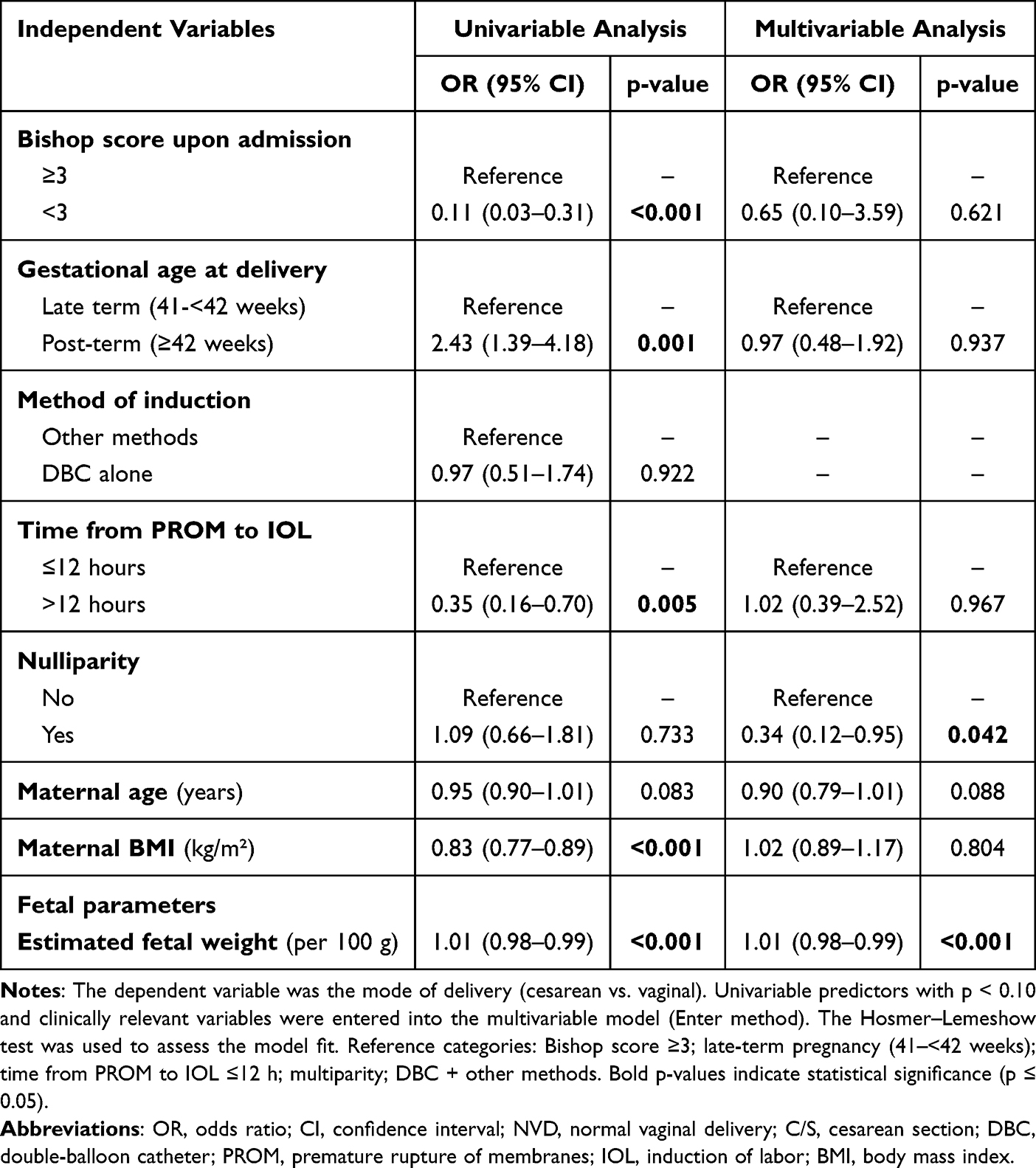 |
Table 5 Multivariable Logistic Regression Analysis of the Predictors of Cesarean Delivery |
Predictors of Total Induction-to-Delivery Time
In multivariate linear regression analysis, the induction method was the strongest determinant of the total induction-to-delivery interval (Table 6). Compared with DBC alone, DBC+misoprostol significantly shortened the interval (β = –0.11; 95% CI: –0.18 to –0.04; p = 0.002), whereas DBC+dinoprostone prolonged the interval (β = +0.09; 95% CI: 0.02–0.16; p=0.010). A higher baseline Bishop score independently predicted shorter induction-to-delivery time (p=0.004). Maternal BMI was significant in some models but remained inconsistent after adjusting for confounding factors.
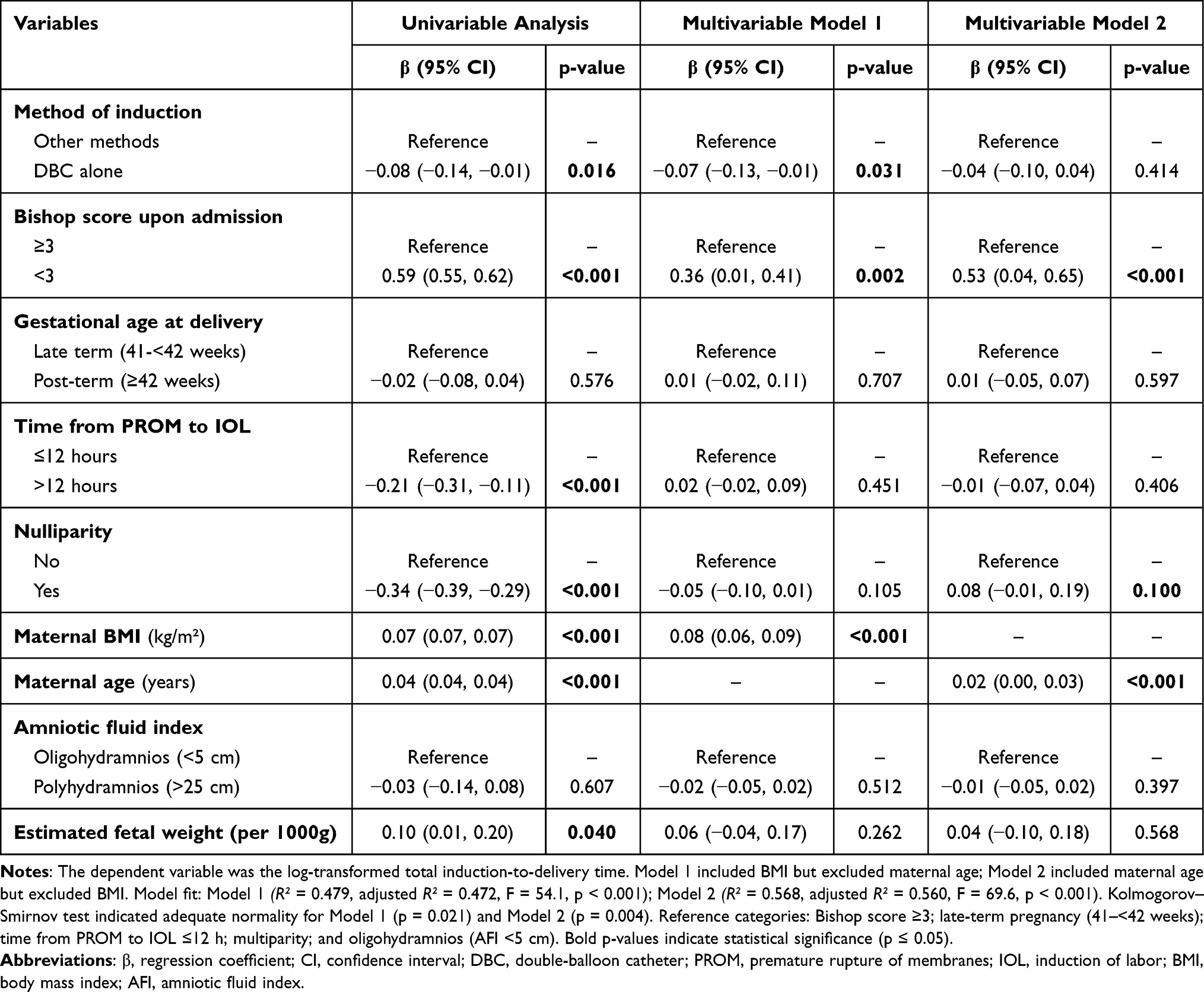 |
Table 6 Multivariable Linear Regression Analysis of the Predictors of Total Induction-to-Delivery Time |
In the supplementary analyses, the induction method and baseline Bishop score also emerged as key predictors of time to active labor, whereas maternal BMI and age showed model-dependent associations (Table S2). Nulliparity, higher maternal BMI, and polyhydramnios were independent predictors of oxytocin augmentation (Table S3). The predictors of time to active labor (Table S2) and oxytocin augmentation (Table S3) are provided in Supplementary Results 2 and 3, respectively.
Time-to-Event Analysis
Kaplan–Meier survival analysis demonstrated overall differences in the time to vaginal delivery among the four study groups (log-rank χ² = 94.7, df = 3, p<0.001; Figure 2). The shortest median time to vaginal delivery was observed in the DBC+misoprostol group (14.9 h, 95% CI: 14.4–15.6), whereas the DBC+dinoprostone group had the longest duration (19.4 h, 95% CI: 18.6–23.5). The DBC alone and DBC+oxytocin groups had intermediate median times of 15.5 h (95% CI: 15.0–16.4) and 18.1 h (95% CI: 17.1–18.6), respectively. Pairwise Log rank tests indicated that, while most intergroup differences were statistically significant (p<0.001), the comparison between DBC alone and DBC+misoprostol did not reach statistical significance (p=0.081). Overall, 709 women (69.4%) achieved vaginal delivery, and 313 (30.6%) were censored due to cesarean delivery. The DBC+dinoprostone group had the highest censoring rate (38.2%), whereas the DBC+misoprostol group had the lowest (25.7%). Detailed survival statistics are provided in Table S1 of the Supplementary Results 1.
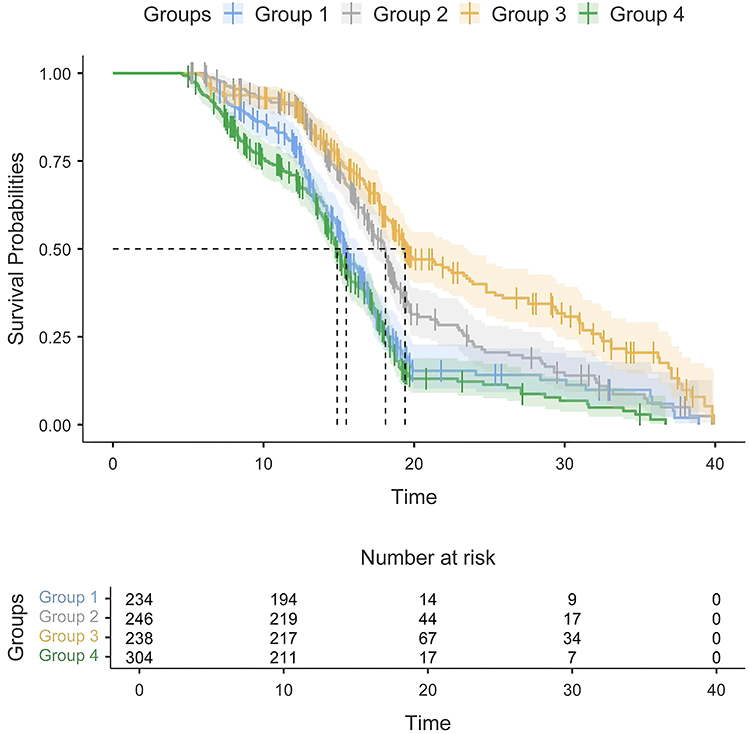 |
Figure 2 Kaplan–Meier curves for time to vaginal delivery by induction method. Kaplan-Meier curves compare time to vaginal delivery among women managed with DBC alone, DBC plus oxytocin, DBC plus dinoprostone, and DBC plus misoprostol. Cesarean deliveries were censored at the time of the surgery. The numbers at risk are shown below the x-axis. Abbreviation: DBC, double-balloon catheter. |
Discussion
Summary of Findings
In this large single-center cohort of late- and post-term pregnancies with unfavorable cervices, the DBC+misoprostol regimen was associated with a shorter induction-to-delivery interval and a higher rate of vaginal birth, whereas the DBC+dinoprostone regimen was associated with longer induction-to-delivery intervals and less favorable maternal outcomes than the other regimens. In the present study, DBC alone and DBC+oxytocin demonstrated intermediate effectiveness. Notably, the apparently greater efficiency of misoprostol was accompanied by higher maternal morbidity, whereas neonatal outcomes remained largely comparable across regimens. These observations highlight the need to balance efficacy and safety when selecting a DBC-based induction strategy, and should be interpreted cautiously, given the study’s retrospective, single-center design and restrictive eligibility criteria.
Interpretation in the Context of Current Literature
Our findings are consistent with recent network meta-analyses and Cochrane reviews, which have shown that DBC+misoprostol combinations accelerate cervical ripening, shorten the induction-to-delivery interval by approximately 3–5 h, and nearly double the likelihood of achieving vaginal birth within 24 h compared with either method alone.12,16,22 This effect likely reflects the synergistic action of mechanical dilation and potent uterotonic activity of misoprostol.
In contrast, DBC+dinoprostone appeared to be the least efficient, consistent with evidence3 that prostaglandin E2 induces more gradual cervical remodeling. In our cohort, the time to active labor and the total induction-to-delivery interval were approximately 3 and 5 h longer, respectively, compared with the DBC+misoprostol regimen. Prior large-scale analyses have also indicated broadly similar cesarean delivery rates across regimens but fewer hyperstimulation events with balloon-based approaches.1,16
Maternal complications were most frequent in the DBC+misoprostol group, consistent with the strong uterotonic activity of misoprostol.6 Although meta-analyses have generally reported comparable safety profiles for misoprostol and dinoprostone, these findings are limited by heterogeneity in dosing regimens, administration routes, and outcome definitions.6 In our cohort, the higher rates of fever, chorioamnionitis, atony, and transfusion may also reflect institutional protocols, such as diagnostic thresholds for intrapartum fever, criteria for clinical chorioamnionitis, and indications for blood transfusion, rather than the intrinsic pharmacological effects of misoprostol alone. Acknowledging the potential influence of local practices strengthens the validity of our interpretation and underscores the need for standardized outcome definitions in future multicenter studies.
Neonatal outcomes did not differ significantly across the groups, consistent with previous meta-analyses demonstrating that maternal complications associated with prostaglandins rarely translate into clinically meaningful neonatal compromise when adequate intrapartum monitoring is employed.1,6 The slightly lower umbilical artery pH observed in the misoprostol group was consistent with the low-certainty findings of previous systematic reviews. Importantly, although the incidence of uterine hyperstimulation was significantly higher in the DBC+misoprostol group (22.7%) than in the other regimens (5.7–12.0%), this increase did not result in adverse neonatal outcomes. This suggests that, although misoprostol may enhance uterine activity, its potential risks can be effectively mitigated through vigilant intrapartum surveillance and timely clinical interventions.
Predictors of Cesarean Delivery
Estimated fetal weight (EFW) emerged as the only independent predictor of cesarean delivery in our study, whereas maternal BMI, Bishop score, and parity were not significant after adjusting for other variables. Each 100 g increase in fetal weight was associated with an approximately 1% higher likelihood of cesarean delivery. This contrasts with the findings of large multicenter studies and systematic reviews that have consistently identified nulliparity, elevated BMI, poor Bishop scores, and advanced gestational age as independent predictors of failed induction.16 Our exclusion of women with macrosomia and extreme BMI likely reduced the confounding factors, making incremental increases in EFW within the non-macrosomic range more predictive of adverse outcomes. This finding highlights the importance of context-specific eligibility criteria when interpreting the prognostic factors.37
In exploratory analyses, polyhydramnios appeared to be associated with a lower risk of cesarean delivery; however, this association did not persist after adjusting for confounders and should not be interpreted as causal. The existing literature provides inconsistent evidence, and any apparent protective effect may be due to residual confounding or diagnostic variability rather than an actual biological effect.37 Notably, in the supplementary analyses, polyhydramnios emerged as a predictor of oxytocin augmentation (Table S3). This association should be regarded as hypothesis generating rather than confirmatory, given the retrospective design and potential confounding factors. Future prospective studies are warranted to clarify whether polyhydramnios influences labor outcomes including cesarean delivery and oxytocin requirement.
Strengths and Limitations
The strengths of this study include its large sample size, detailed subgroup analysis, and use of survival methods to model time-to-delivery, which provided a robust assessment of induction efficiency. Unlike many retrospective cohorts, we rigorously excluded women with extreme BMI and suspected macrosomia, thereby minimizing the major confounders and improving the internal validity of our prognostic analysis.
This study had several limitations. First, its retrospective, single-center design limits causal inference and leaves the possibility of residual confounding despite multivariate adjustment. Second, patient-centered outcomes such as maternal satisfaction, pain perception, and recovery experience, as well as provider-level factors including intrapartum management strategies, thresholds for amniotomy or intrauterine resuscitation, and adherence to dosing protocols were not recorded. These unmeasured variables may have influenced both the efficacy and safety. Third, although strict exclusion criteria (eg, suspected macrosomia and extreme BMI) strengthened the internal validity and reduced significant confounding factors, they also restricted the external applicability of the findings to more diverse obstetric populations and settings with variable monitoring capabilities. Finally, diagnostic variability in outcomes, such as intrapartum fever, tachysystole, and clinical chorioamnionitis, may have influenced the observed differences in maternal morbidity.
In this large retrospective cohort study, the DBC+misoprostol regimen was associated with the shortest induction-to-delivery interval but also with higher maternal morbidity. The DBC+oxytocin regimen provided a more balanced profile of efficacy and safety, whereas the DBC+dinoprostone regimen was the least favorable across all assessed outcomes. These results should be interpreted cautiously, considering the retrospective, single-center design and restrictive exclusion criteria, which may limit their generalizability.
Clinical and Public Health Implications
Our findings highlight a fundamental tradeoff between the efficiency and safety of DBC-based induction strategies. The DBC+misoprostol regimen was associated with the shortest induction-to-delivery interval and higher vaginal birth rates; however, the difference compared with that of DBC alone was not statistically significant (p=0.081). This finding suggests that the apparent advantages of misoprostol should be interpreted with caution, particularly because of its association with higher rates of maternal morbidity. In contrast, DBC+oxytocin combinations offered a more balanced profile between efficacy and safety, whereas DBC+dinoprostone protocols were slower and less favorable in terms of operative outcomes.
Clinically, DBC+misoprostol may be considered when rapid delivery is required, such as in post-term pregnancies or in cases of urgent maternal–fetal conditions that require immediate delivery. However, its use should be coupled with continuous intrapartum monitoring and preparedness to manage tachysystole, fever, and postpartum hemorrhage. For women at an increased risk of uterine hyperstimulation or hemorrhage or in healthcare environments where monitoring capacity is limited, DBC+oxytocin may be a safer option. In contrast, DBC+dinoprostone appears to be less favorable when prolonged latent phases or increased operative delivery risks are a concern. Although misoprostol is inexpensive, stable at room temperature, and widely accessible, its clinical use should be carefully aligned with institutional resources and the capacity to ensure adequate maternal and fetal monitoring.
At the population level, optimizing induction strategies is becoming increasingly crucial, as induction rates now exceed 30% in many high-income countries. Aligning protocol selection with local resources, patient risk profiles, and monitoring capabilities is essential to ensure maternal safety and timely delivery. These results underscore the need for context-specific guidelines that balance efficiency and safety to improve maternal and neonatal outcomes in diverse health care settings.
Future Research and Generalizability
Future research should focus on directly comparing the balloon-misoprostol and balloon–oxytocin regimens in multicenter randomized trials using standardized induction protocols. Such studies need to incorporate clinically relevant safety endpoints, including tachysystole with fetal compromise, postpartum atony, hemorrhage, and transfusion requirements, as well as patient-centered outcomes, such as satisfaction, pain perception, and recovery experience. Cost-effectiveness analyses are crucial for guiding practices in both high- and low-resource settings. Moreover, stratification by parity and baseline Bishop score is essential, given their continued clinical relevance, despite not emerging as independent predictors in our cohort. Reporting absolute risk differences and the numbers needed to treat or harm will further facilitate the translation of the findings into clinical decision-making. Finally, mechanistic studies are warranted to clarify how estimated fetal weight and amniotic fluid characteristics influence induction success, ideally using standardized definitions and core outcome sets to improve comparability across studies.
Conclusion
In this large single-center retrospective cohort study, the DBC + misoprostol regimen was associated with the greatest induction efficiency but also with the highest maternal morbidity, including uterine hyperstimulation, intrapartum fever or clinical chorioamnionitis, postpartum uterine atony, and blood transfusion requirement. The DBC + oxytocin regimen demonstrated the most balanced effectiveness-safety profile, whereas the DBC + dinoprostone regimen showed slower labor progression and a less favorable profile across all assessed outcomes. Because these findings derive from a non-randomized retrospective cohort, they should be interpreted as comparative associations rather than definitive evidence of superiority. In late- and post-term pregnancies with unfavorable cervices, induction protocol selection should be individualized according to maternal risk, urgency of delivery, and the capacity for continuous intrapartum monitoring, particularly when misoprostol-containing regimens are used.
Abbreviations
AGA, Appropriate for gestational age; AFI, Amniotic fluid index; ANOVA, Analysis of variance; BMI, Body mass index; CI, Confidence interval; CPAP, Continuous positive airway pressure; C/S, Cesarean section; DBC, Double-balloon catheter; EFM / c-EFM, (Continuous) electronic fetal monitoring; EFW, Estimated fetal weight; FHR, Fetal heart rate; Hb, Hemoglobin; ICU, Intensive care unit; IOL, Induction of labor; IQR, Interquartile range; LGA, Large for gestational age; NICU, Neonatal Intensive Care Unit; NVD, Normal vaginal delivery; OR, Odds ratio; PPH, Postpartum hemorrhage; PROM, Premature rupture of membranes; SD, Standard deviation; SGA, Small for gestational age; TVUS, Transvaginal ultrasonography; VIF, Variance inflation factor.
Data Sharing Statement
The de-identified patient data supporting this study were obtained from institutional electronic medical records. Owing to privacy and institutional restrictions, the datasets are not publicly accessible. However, they may be provided by the corresponding author upon reasonable request and with approval from the Ethics Committee.
Ethics Approval and Consent to Participate
All the participants provided written informed consent. The study protocol was approved by the Scientific Research Ethics Committee of the Adana City Training and Research Hospital (approval date: March 6, 2025; decision no. 422).
Consent for Publication
The data that support the findings of this study are not openly available owing to sensitivity reasons and are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Mr. Gökhan Karakoç and Mr. Ali Karakoç from Model Statistics CRO (Turkey) for their professional support in statistical planning and data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jones MN, Palmer KR, Pathirana MM, et al. Balloon catheters versus vaginal prostaglandins for labour induction (CPI Collaborative): an individual participant data meta-analysis of randomised controlled trials. Lancet. 2022;400(10364):1681–20. doi:10.1016/S0140-6736(22)01845-1
2. Patabendige M, Chan F, Vayssiere C, et al. Vaginal misoprostol versus vaginal dinoprostone for cervical ripening and induction of labour: an individual participant data meta-analysis of randomised controlled trials. BJOG. 2024;131(9):1167–1180. doi:10.1111/1471-0528.17794
3. Yuan L, Peng J, Yang L, Zhao Y. Efficacy and safety of double balloon catheter and dinoprostone for labor induction in multipara at term. Arch Gynecol Obstet. 2024;309(2):533–540. doi:10.1007/s00404-022-06891-9
4. Carvalho-Afonso M, Policiano C, Clode N, Ayres-de-Campos D. Cervical ripening with Foley catheter balloon: a prospective cohort of 320 women. Int J Gynaecol Obstet. 2025;170(2):768–773. doi:10.1002/ijgo.70088
5. Li S, He H, Zheng W, Liu J, Chen C. Comparison of outcomes of labor induction with dinoprostone vaginal insert (PROPESS) and double balloon cook catheter in term nulliparous pregnancies. J Obstet Gynaecol Res. 2025;51(1):e16107. doi:10.1111/jog.16107
6. Taliento C, Manservigi M, Tormen M, et al. Safety of misoprostol vs dinoprostone for induction of labor: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2023;289:108–128. doi:10.1016/j.ejogrb.2023.08.382
7. Chang TA, Li YR, Ding DC. Oxytocin and vaginal dinoprostone in labor induction: a systematic review and meta-analysis. Int J Gynaecol Obstet. 2024;166(2):626–638. doi:10.1002/ijgo.15443
8. Huang F, Chen H, Wu X, et al. A model to predict delivery time following induction of labor at term with a dinoprostone vaginal insert: a retrospective study. Ir J Med Sci. 2024;193(3):1343–1350. doi:10.1007/s11845-023-03568-3
9. Kruit H, Place K, Vayrynen K, et al. Comparison of balloon catheter, oral misoprostol, or combination of both for cervical ripening in late-term and post-term nulliparous women: a Finnish randomized controlled multicenter pilot trial. Acta Obstet Gynecol Scand. 2025;104(2):389–399. doi:10.1111/aogs.15034
10. Grobman WA. The role of labor induction in modern obstetrics. Am J Obstet Gynecol. 2024;230(3S):S662–S668. doi:10.1016/j.ajog.2022.03.019
11. Wang Y, Zhou X. Comparison of double balloon catheter and dinoprostone vaginal insert in induced labor: a meta-analysis of 2267 patients. Clin Exp Obstet Gynecol. 2025;52(2).
12. Sanchez-Ramos L, Lin L, Vilchez-Lagos G, et al. Single-balloon catheter with concomitant vaginal misoprostol is the most effective strategy for labor induction: a meta-review with network meta-analysis. Am J Obstet Gynecol. 2024;230(3S):S696–S715. doi:10.1016/j.ajog.2022.01.005
13. Diguisto C, Le Gouge A, Arthuis C, et al. Cervical ripening in prolonged pregnancies by silicone double balloon catheter versus vaginal dinoprostone slow release system: the MAGPOP randomised controlled trial. PLoS Med. 2021;18(2):e1003448. doi:10.1371/journal.pmed.1003448
14. Hostinska E, Lubusky M, Pilka R. Prospective comparison of cervical ripening with double balloon Cook catheter, misoprostol or dinoprostone in term singleton pregnancies. Ginekol Pol. 2022;94(3):221–228. doi:10.5603/GP.a2022.0023
15. Anjali, Jain S, Pasrija S, Kille HC. Labor induction with combined low-dose oral misoprostol and Foley catheter vs oral misoprostol alone at term gestation-a randomized study. AJOG Glob Rep. 2022;2(3):100060. doi:10.1016/j.xagr.2022.100060
16. de Vaan MD, Ten Eikelder ML, Jozwiak M, et al. Mechanical methods for induction of labour. Cochrane Database Syst Rev. 2023;3(3):CD001233. doi:10.1002/14651858.CD001233.pub4
17. Grace Ng YH, Aminuddin AA, Tan TL, Kuppusamy R, Tagore S, Yeo GSH. Multicentre randomised controlled trial comparing the safety in the first 12 h, efficacy and maternal satisfaction of a double balloon catheter and prostaglandin pessary for induction of labour. Arch Gynecol Obstet. 2022;305(1):11–18. doi:10.1007/s00404-021-06090-y
18. Sanchez-Ramos L, Levine LD, Sciscione AC, et al. Methods for the induction of labor: efficacy and safety. Am J Obstet Gynecol. 2024;230(3S):S669–S695. doi:10.1016/j.ajog.2023.02.009
19. Organization WH. WHO recommendations on induction of labour, at or beyond term; 2022.
20. Geneen LJ, Gilbert J, Reeves T, et al. Timing of induction of labour in the prevention of prolonged pregnancy: systematic review with meta‐analysis. Reproductive, Female and Child Health. 2022;1(1):69–79. doi:10.1002/rfc2.6
21. Chen Q, Zhou H, Hu Y, Xue J. Which approach is better for labor induction: simultaneous or sequential administration of oxytocin and intrauterine balloon-a systematic review and a meta-analysis. J Matern Fetal Neonatal Med. 2024;37(1):2395490. doi:10.1080/14767058.2024.2395490
22. Yin J, Li Y, Chen Y, Wang C, Song X. Intracervical Foley catheter plus intravaginal misoprostol compared to intravaginal misoprostol-only for cervical ripening: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2023;281:76–84. doi:10.1016/j.ejogrb.2022.12.022
23. Al-Hafez L, Khanuja K, Mendez-Figueroa H, et al. Misoprostol with balloon vs oxytocin with balloon in high-risk pregnancy induction: a randomized controlled trial. Am J Obstet Gynecol MFM. 2023;5(12):101175. doi:10.1016/j.ajogmf.2023.101175
24. Tang RJ, Bode LM, Baugh KM, et al. Duration of double balloon catheter for patients with prior cesarean: a before and after study. AJOG Glob Rep. 2024;4(3):100378. doi:10.1016/j.xagr.2024.100378
25. Abdullah ZHA, Chew KT, Velayudham VRV, et al. Pre-induction cervical assessment using transvaginal ultrasound versus Bishops cervical scoring as predictors of successful induction of labour in term pregnancies: a hospital-based comparative clinical trial. PLoS One. 2022;17(1):e0262387. doi:10.1371/journal.pone.0262387
26. Levine LD, Downes KL, Parry S, Elovitz MA, Sammel MD, Srinivas SK. A validated calculator to estimate risk of cesarean after an induction of labor with an unfavorable cervix. Am J Obstet Gynecol. 2018;218(2):254e251–254e257. doi:10.1016/j.ajog.2017.11.603
27. Dorwal M, Yadav G, Singh P, et al. Deriving a prediction model for emergency cesarean delivery following induction of labor in singleton term pregnancies. Int J Gynaecol Obstet. 2023;160(2):698–706. doi:10.1002/ijgo.14403
28. Kukrer S, Arlier S. Induction of labor in late-term and post-term pregnancies using double-balloon catheter for cervical ripening: predictors of prolonged labor across four combined augmentation protocols in a retrospective cohort study. J Clin Med. 2026;15(5):2011. doi:10.3390/jcm15052011
29. Kruit H, Nupponen I, Heinonen S, Rahkonen L. Comparison of delivery outcomes in low-dose and high-dose oxytocin regimens for induction of labor following cervical ripening with a balloon catheter: a retrospective observational cohort study. PLoS One. 2022;17(4):e0267400. doi:10.1371/journal.pone.0267400
30. Appadurai U, Gan F, Hong J, Hamdan M, Tan PC. Six compared with 12 hours of Foley balloon placement for labor induction in nulliparous women with unripe cervices: a randomized controlled trial. Am J Obstet Gynecol MFM. 2023;5(11):101157. doi:10.1016/j.ajogmf.2023.101157
31. Dasgupta S, Dasgupta J, Goswami B, Mondal J. Randomized controlled trial comparing efficacy of a combination regime containing two cervical sensitizers (mifepristone + Foley’s catheter) versus single agent mifepristone or Foley’s catheter for labor induction in women attempting TOLAC at late third trimester with a dead fetus in utero. J Obstet Gynaecol Res. 2023;49(11):2671–2679. doi:10.1111/jog.15772
32. Eser A, Ozkaya E, Abide CY, et al. Transcervical Foley balloon catheter and vaginal prostaglandin E2 insert combination vs. vaginal prostaglandin E2 insert only for induction of labor at term: a randomized clinical trial. Arch Gynecol Obstet. 2019;299(2):451–457. doi:10.1007/s00404-018-4998-8
33. Polonia-Valente R, Costa S, Coimbra C, et al. Labor induction with a combined method (pharmacologic and mechanical): a randomized controlled trial. J Gynecol Obstet Hum Reprod. 2023;52(9):102649. doi:10.1016/j.jogoh.2023.102649
34. Shalev-Ram H, Cirkin R, Cohen G, et al. Is there a difference in labor patterns after induction with prostaglandins and double-balloon catheters? AJOG Glob Rep. 2023;3(3):100198. doi:10.1016/j.xagr.2023.100198
35. Hamm RF, McCoy J, Oladuja A, et al. Maternal morbidity and birth satisfaction after implementation of a validated calculator to predict cesarean delivery during labor induction. JAMA Netw Open. 2020;3(11):e2025582. doi:10.1001/jamanetworkopen.2020.25582
36. Orr L, Reisinger-Kindle K, Roy A, et al. Combination of Foley and prostaglandins versus Foley and oxytocin for cervical ripening: a network meta-analysis. Am J Obstet Gynecol. 2020;223(5):743e741–743e717. doi:10.1016/j.ajog.2020.05.007
37. Yogamoorthy U, Saaid R, Gan F, Hong J, Hamdan M, Tan PC. Induction of labor via Foley balloon catheter placement for 6 vs 12 hours in women with 1 previous cesarean delivery and unfavorable cervices: a randomized controlled trial. Am J Obstet Gynecol MFM. 2023;5(11):101158. doi:10.1016/j.ajogmf.2023.101158
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Factors for the Success of Vaginal Dinoprostone for the Induction of Labour
Liu W, Guo L, Feng L, Wang J, Zhang M, Fan X
International Journal of Women's Health 2024, 16:1093-1101
Published Date: 13 June 2024
Double Balloon Combined with Oxytocin in Labor Induction: Analysis of Multivariate Factors Affecting the Efficacy of Cervical Ripening
Wu XL, Liu HY, Xiang QH, Yin Z, Zhou R, Wang YJ, Zhou BY, Wang F, Zhao M, Chen M
International Journal of Women's Health 2024, 16:1219-1227
Published Date: 5 July 2024
Uterine Reaction to Oxytocin and Maternal-Neonatal Outcomes in Inducing Labor: A Retrospective Cohort Study
Liu H, Fan Z, Wu F, Wang M, Yang Z, Zhang F
International Journal of Women's Health 2025, 17:2793-2803
Published Date: 30 August 2025