Back to Journals » Drug Design, Development and Therapy » Volume 19
Dosing Optimization of Lamotrigine in Peripregnancy Epilepsy Through PopPK Modelling and Simulation
Authors Huo J ![]() , Liu Y, Yang J, Chen M, Yang L, Wang L, Zhang D, Liu T, Gao W, Dai H
, Liu Y, Yang J, Chen M, Yang L, Wang L, Zhang D, Liu T, Gao W, Dai H ![]() , Mei S
, Mei S ![]() , Zhao Z
, Zhao Z ![]()
Received 20 May 2025
Accepted for publication 3 November 2025
Published 20 November 2025 Volume 2025:19 Pages 10243—10258
DOI https://doi.org/10.2147/DDDT.S541597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Tamer Ibrahim
Jiping Huo,1,2,* Yilin Liu,3,* Jiayu Yang,1,2,* Meng Chen,4,* Li Yang,1 Lijun Wang,5 Dongjie Zhang,1 Tongtong Liu,1 Wanli Gao,5 Haibin Dai,4 Shenghui Mei,1,2 Zhigang Zhao1,2
1Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Clinical Pharmacology, College of Pharmaceutical Sciences, Capital Medical University, Beijing, 100045, People’s Republic of China; 3National Institute for Drug Clinical Trial, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China; 4Department of Pharmacy, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 5Department of Gynaecology and Obstetrics, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shenghui Mei, Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, 119 Nansihuan West Road, Fengtai District, Beijing, People’s Republic of China, Email [email protected] Zhigang Zhao, Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, 119 Nansihuan West Road, Fengtai District, Beijing, People’s Republic of China, Email [email protected]
Purpose: Lamotrigine demonstrates substantial interindividual pharmacokinetic variability during pregnancy, though the underlying mechanisms remain incompletely understood. The study aimed to develop a population pharmacokinetic model of lamotrigine in Chinese epileptic patients during the peripregnancy period, in order to identify the key influencing factors and thereby assist in providing a solution for the individualized administration of lamotrigine.
Methods: One hundred and twenty-eight perigestational epilepsy patients (293 plasma concentrations) from two Chinese hospitals between January 1, 2015 and May 31, 2024 were enrolled in the study. A nonlinear mixed-effects model was developed using Phoenix NLME™ (v8.3) with stepwise covariate selection. Model validation encompassed goodness-of-fit analysis, bootstrap analysis (n = 1000), prediction-corrected visual predictive checks, and normalized prediction distribution error evaluation. Optimal dosing regimens were derived through Monte Carlo simulations accounting for gestational/postpartum physiological changes.
Results: A one - compartment model combined with an additive and proportional error model was employed to characterize the pharmacokinetics of lamotrigine. Each factor’s impact on CL/F was systematically examined using a stepwise approach, resulting in the establishment of the final model: . CL/F was identified as the primary pharmacokinetic parameter, serving as the main outcome measure and foundational basis for dosing recommendations. The model demonstrated satisfactory accuracy and commendable predictability. LTG CL/F increased significantly from 5 weeks of gestation, with CL/F in stages 2, 3, and 4 being 131%, 193%, and 199% of stage 1 (< 5 weeks), respectively, and declining sharply to 68% of stage 1 postpartum.
Conclusion: The CL/F of lamotrigine was found to be increased significantly from 5 weeks of gestation and dropped sharply postpartum. Weight, pregnancy stage, and co-administration with valproic acid were identified as significant influencing factors. The internal verification results of the model were generally satisfactory, however, prospective multicenter cohorts incorporating larger-scale external datasets are imperative to establish robust generalizability, ultimately enabling precise personalized dose optimization strategies for peripregnancy epileptic patients.
Keywords: lamotrigine, peripregnancy, epilepsy, population pharmacokinetic model, nonlinear mixed effects modeling
Introduction
Epilepsy was a common neurological condition, affecting about 0.5–1% of the population.1 Approximately one-third of individuals with epilepsy were in their reproductive years, and 14–62% of women with epilepsy experienced increased seizures during pregnancy,2 which could negatively impact both maternal and fetal health, leading to complications such as fetal hypoxia, miscarriage, preterm birth, and preeclampsia.3,4 Antiseizure medications (ASMs) were the primary treatment, while their management during pregnancy presented a dual challenge: minimizing fetal exposure to ASMs while effectively preventing seizures.5
Lamotrigine (LTG), a second-generation antiepileptic drug, was recommended as the first-line treatment for women with epilepsy (WWE) during pregnancy due to its low risk of severe congenital malformations.5–10 It was the most commonly used ASMs for monotherapy in women of reproductive age and perinatal period.11 Despite its relative safety, LTG use during pregnancy carried some risk of teratogenicity, especially at maternal doses exceeding 300 mg/day, which significantly increased the risk of infant malformations.11–13 Some studies suggested that prenatal exposure to LTG might be associated with an increased risk of neurodevelopmental disorders, such as autism,12 impaired cognitive function,13 and attention deficits.11 However, the current evidence remained inconclusive and required validation from more extensive research. Given this uncertainty, it was critical to interpret these findings with caution within a personalized risk-benefit framework for each patient.
Significant individual variability was found in LTG metabolism during pregnancy,14 with inconsistent findings reported regarding changes and the extent of LTG clearance across different pregnancy stages. One study15 documented a 56.1% reduction in LTG concentration during pregnancy. Fotopoulou et al16 observed an increase in LTG clearance throughout all three trimesters, with the highest increase reaching 248% of pre-pregnancy levels in late pregnancy. Pennell et al reported that LTG clearance peaked at 32 weeks of gestation,16 while other studies indicated that LTG plasma concentration decreased most significantly in the second trimester.17
The pharmacokinetics of LTG underwent significant changes during the peripregnancy period. Factors such as maternal weight, plasma composition, hemodynamic fluctuations, hormonal effects, and the role of the fetal placenta in drug distribution and elimination were found to influence these alterations.18,19 However, the exact role of these factors remained unclear. A comprehensive understanding of LTG pharmacokinetics during the peripregnancy period was critical to ensure safe use and minimize risks to both mothers and fetuses.
Population pharmacokinetic (PopPK) approach could assess drug behavior within specific populations and help tailor individualized dosing regimens.20 Based on the largest cohort of Chinese pregnant and postpartum WWE assembled to date, the study aimed to establish a well-powered PopPK model that incorporated a novel gestational staging system to precisely quantify LTG CL/F during pregnancy and the postpartum stage. This robust and reliable model would establish evidence-based individualized drug administration regimens and provide valuable guidance for informed pharmacotherapeutic decisions for these patients.
Materials and Methods
Study Population
This multicenter retrospective cohort study consecutively enrolled perigestational epilepsy patients receiving LTG monotherapy at Beijing Tiantan Hospital (Capital Medical University) and The Second Affiliated Hospital (Zhejiang University School of Medicine) from January 2015 to May 2024.
Inclusion criteria comprised: (1) Diagnosis of epilepsy during pregnancy (any trimester) or within 6 months postpartum, confirmed by two board-certified neurologists according to the 2014 ILAE classification criteria; (2) Continuous LTG treatment for ≥7 days prior to plasma sampling to ensure pharmacokinetic steady-state (≥5 half-lives); (3) Availability of complete medical records including serial therapeutic drug monitoring data, obstetric outcomes, and neurological follow-up. Exclusion criteria included: (1) Age <18 years at conception; (2) Comorbid major psychiatric disorders (DSM-5 diagnosed depression, schizophrenia, or intellectual disability with IQ <70); (3) Documented poor medication adherence (modified Morisky scale score ≤ 2); (4) Missing critical clinical data (>20% variables incomplete).
The study protocol received ethical approval from both institutional review boards (Tiantan IRB NO. KY2023-169-02; Zhejiang IRB NO. I2024714) with written informed consent obtained from all participants. All procedures complied with ICH-GCP guidelines and the Declaration of Helsinki (2013 revision).
Dosing Regimens and Concentration Measurement
All patients received LTG produced by The Wellcome Foundation Limited. LTG was administered in tablet form at daily doses ranging from 25 mg to 800 mg, typically given in one to two doses per day. Plasma concentrations of LTG were obtained from therapeutic drug monitoring data, with the majority of samples representing steady-state trough concentrations. Plasma concentrations of LTG were determined using a validated ultra-performance liquid chromatography-tandem mass spectrometry method. The analysis was performed on a Sciex Exion LC™ UHPLC tandem 6500 QTRAP mass system (AB SCIEX, CA, USA). Data acquisition and processing were conducted using Analyst software (version 1.7.2, AB SCIEX, CA, USA). Additionally, routine sample calibration and quality control measures were implemented in accordance with guidelines to ensure the accuracy and precision of the analysis. The calibration curve was linear from 1.37 to 20.9 mg/L (extendable to 209 mg/L with dilution; r > 0.999), with the lower limit of quantitation (LLOQ) of 1.37 mg/L.21 Method validation confirmed acceptable intra-day accuracy (bias: −4.00% to 2.00%) and precision (CV: 0.34–0.39%). Inter-day accuracy (bias: 0.22–0.53%) and precision (CV: 4.62–4.63%) also fell within the pre-defined acceptance criteria.
Data Collection
In the study, a comprehensive set of patients’ data was collected: (1) Demographic characteristics; (2) Biochemical indicators: laboratory test values including liver function and renal function; (3) LTG administration information; (4) Concomitant medications: enzyme inducers (Carbamazepine(CBZ), Oxcarbazepine(OXC), Phenobarbital), enzyme inhibitors (valproic acid(VPA)), other drugs that did not significantly affect LTG metabolism.
The collected patient information was compiled and verified by two individuals, following the data format requirements of Phoenix software.
Pharmacokinetic Analysis
The data was analyzed by nonlinear mixed-effects modeling method using the Phoenix NLME software (version 8.3, Certara, St. Louis, MO, USA) with the first-order conditional estimation with extended least square method (FOCE-ELS). Continuous data were presented as mean ± SD (range), while categorical data were presented as frequency (%). The objective function value (OFV), as well as the differences in Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC), were utilized to compare the models. Goodness-of-fit (GOF) plots, Bootstrap analysis, Visual Predictive Check (VPC), and Normalized Prediction Distribution Error (NPDE) were performed to evaluate the final model. The R package (v.4.1.2) was used for analysis and graphics output.
Base Model
A one-compartment model with first-order absorption and elimination was adopted as the structural model for LTG base model, as shown in Figure 1. The absence of both the absorption and distribution phases in the sampled data rendered the estimates of the absorption rate constant (Ka) and the apparent distribution volume (V/F) unreliable. Therefore, Ka and V/F were fixed at 1.93 h−1 and 68.8 L,19 respectively. Only CL/F was estimated during model development. While this approach improved model stability, fixing Ka and V/F entailed certain limitations: it restricted the assessment of interindividual variability in these parameters and potentially affected the precision of subsequent parameter estimations. These limitations should be acknowledged when interpreting the model’s results. The following equations were used to describe the model:



 |
Figure 1 Schematic diagram of a one-compartment model with first-order absorption and elimination for LTG. [Ka, absorption rate constant; CL/F, apparent clearance; Vc/F, apparentcentral volume of distribution]. |
Ka and Aa represented the absorption rate constant and the amount of LTG in the absorption site, respectively. CL and Ac represented the clearance of LTG and the amount of LTG in the central compartment, respectively. Cc represented the LTG concentration in the central compartment.
The inter-individual variability (η) and the residual variability (ε) were described by following models (4 and 5). η and ε were assumed to follow a normal distribution with a mean of zero and variances of ω2 and σ2, respectively. The index error model was employed to estimate the inter-individual variability of CL/F, while the combined additive and proportional error model was utilized to characterize the residual variability of LTG concentration.


θTV represented the population typical value of pharmacokinetic parameters, θi was the individual (ith) pharmacokinetic parameters. Cobs and Cpred represented the measured and predicted concentrations.
Covariate Model
Prior to covariate screening, correlation coefficients were calculated for all paired variables, with highly correlated covariates (correlation coefficient > 0.5) being excluded from the model simultaneously. In the PopPK model, various readily accessible indicators from routine clinical practice, such as peripregnancy stages, concomitant use of ASMs, body weight, liver and kidney function, were evaluated as potential covariates. The association between individual empirical Bayesian estimates of model parameters and patient covariates was assessed in a straightforward manner. Covariates were introduced or eliminated into the population model using a stepwise technique. In the forward addition approach, covariates were included in the base model if the difference in the objective function value (∆OFV) was greater than 3.84 (P < 0.05). In the backward elimination, covariates were retained in the model if ∆OFV was greater than 6.64 (P < 0.01). In previous PopPK studies, peripregnancy stages mostly followed the traditional gestational week classification standard, with the 14th and 28th weeks serving as key nodes. However, research had also shown that the LTG clearance increased as early as the 5th week of pregnancy.22 This discovery prompted us to reevaluate the classification of pregnancy stages when using LTG. Consequently, we innovatively adopted the 5th, 14th, and 28th weeks of pregnancy, as well as the delivery, as new key nodes to subdivide the peripregnancy stages. Detailed descriptions of the five classifications were presented in Table 1, aiming to delve deeper into the variation of LTG clearance across different pregnancy stages and their inherent connections with the progression of pregnancy.
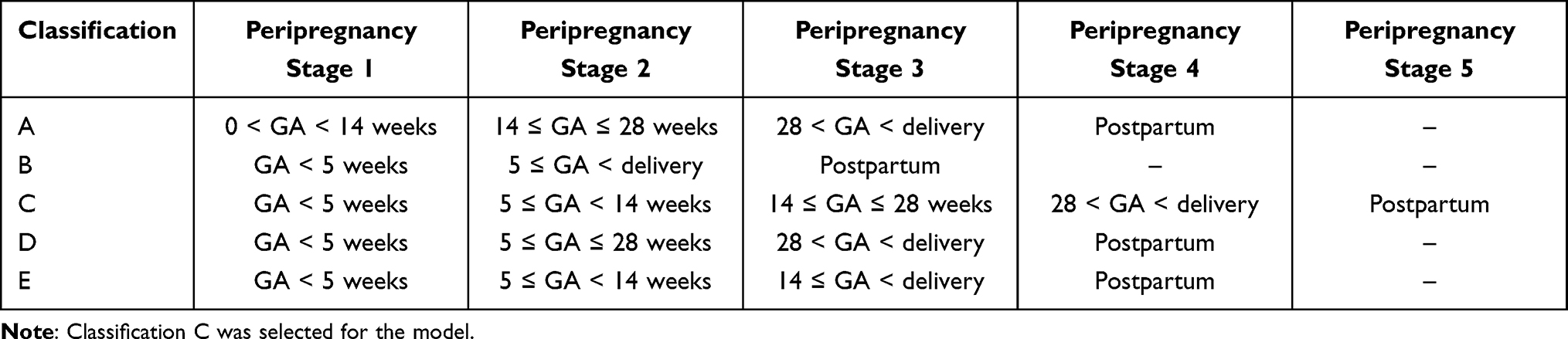 |
Table 1 Five Classification Methods for Peripregnancy Stages |
Model Evaluation
GOF plots were generated to assess the consistency between the base model and the final model against LTG concentration-time points. These plots included comparisons of observed concentrations versus individual population predicted concentrations (IPRED), population predicted concentrations (PRED), and conditional weighted residuals (CWRES) versus PRED. A non-parametric bootstrap method was employed to generate 1000 resampled datasets. Subsequently, a median estimate along with a 95% confidence interval (CI) was computed and compared to the final parameter estimates to evaluate the accuracy of the final model. The simulation based diagnostic performance of the final model was evaluated using the NPDE method (1000 runs). Additionally, 1000 data simulations were executed employing the VPC to evaluate the model’s predictive performance. The comparison between predicted and observed results was facilitated by calculating the 5th, 50th, and 95th percentiles, respectively.
Model-Informed LTG Dosing Regimens
Based on the final optimization model parameters, the Simulation module of Phoenix NLME (version 8.3) was utilized to predict the concentration of pregnant and postpartum WWE under various administration regimens. A validated virtual dataset was generated using the covariate distribution model. Subsequently, 50 kg, 65 kg, and 80 kg were chosen to represent patients with low, medium, and high body weights, respectively. Additionally, 18 drug administration regimens for pregnant and postpartum patients were simulated (50 kg group: 50, 100, 150, 200, 250, 300 mg/d; 65 kg group: 100, 150, 200, 250, 300, 350 mg/d; 80 kg group: 150, 200, 250, 300, 350, 400 mg/d). Due to the absence of an established effective concentration range for epilepsy treatment during pregnancy, the steady-state therapeutic concentration range of 2.5 to 15 mg/L23,24 for adult epilepsy patients was chosen as the reference standard in the study.
Results
Study Population
A total of 128 patients were enrolled in this study, from which 293 LTG plasma concentrations were obtained. The mean age of the participants was 28.24 years, with an age range spanning from 19 to 36 years. Additional demographic characteristics and co-medication details were provided in Table 2. The distribution of observations across the peripregnancy stages was as follows: 13 observations in Peripregnancy Stage 1, 63 in Stage 2, 111 in Stage 3, 84 in Stage 4, and 22 in the postpartum period. These data reflected the number of blood sampling points collected at each stage of pregnancy. Additional demographic characteristics and co-medication details were provided in Table 2.
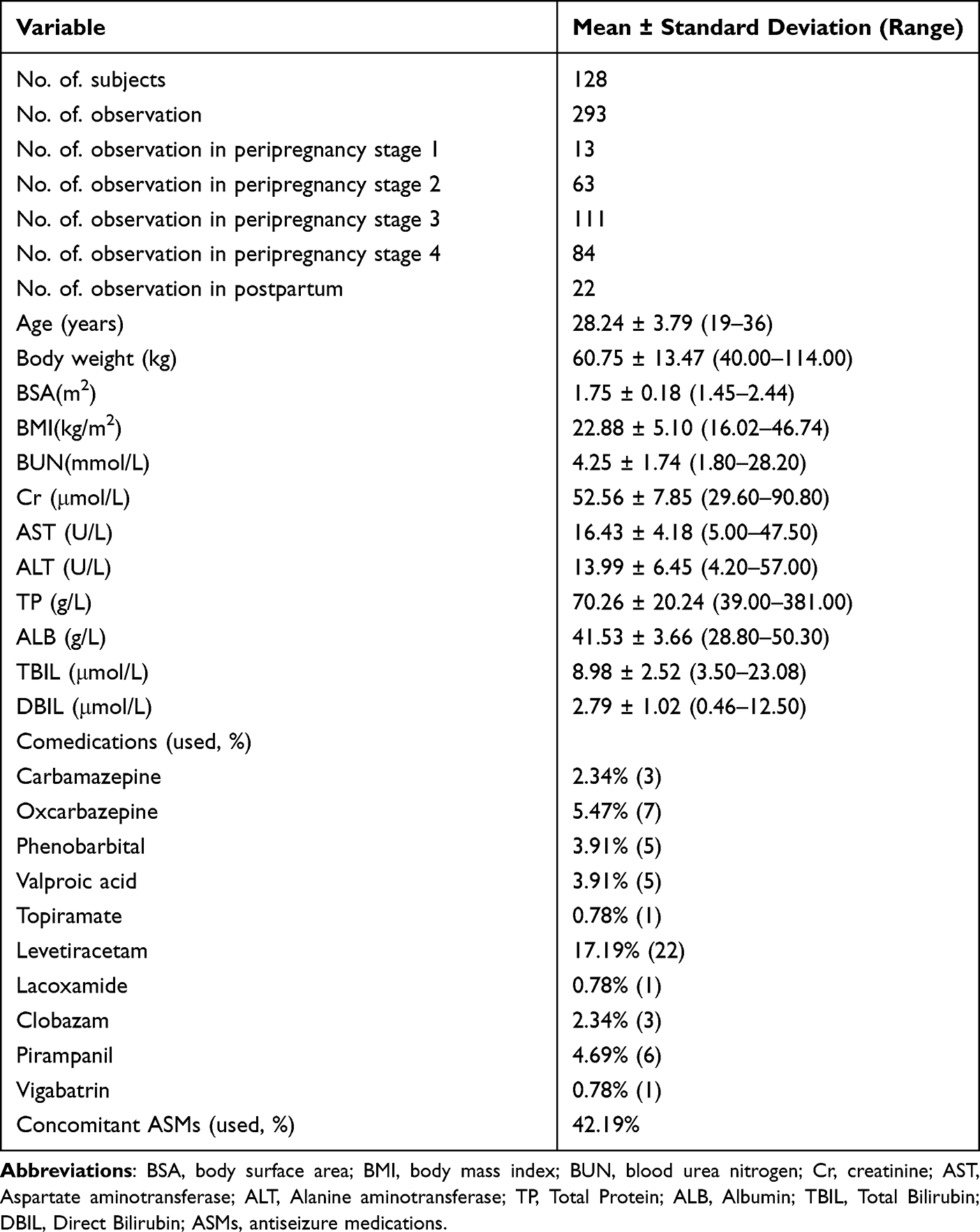 |
Table 2 Characteristics of Patients in the Population Pharmacokinetic Model |
Development of Population Pharmacokinetic Model
Figure S1 (Supplementary Material) displayed the correlation coefficients among potential covariables in the result matrix. Covariables were incrementally added to the basic model to construct a comprehensive model while ensuring avoidance of collinearity. Through the forward addition method, the impact of each covariable on pharmacokinetic parameters was examined, as detailed in Table S1 (Supplementary Material). Notably, the analysis revealed that defining the first 5 weeks of gestation as peripregnancy stage 1 (Classification C, as shown in Table 1) exerted a significantly greater impact on LTG CL/F compared to the other four classifications, with a substantial decrease in objective function value (Δ OFV = −181.38(C) vs −169.33(A), −125.60(D), −112.67(B), −49.17(E), P < 0.05). Table 3 presented the developmental procedures utilized in constructing the final model, which demonstrated that LTG CL/F was significantly affected by pregnancy, body weight, and enzyme inhibitors. The quantitative association between model parameters and covariables was detailed as follows:


 |
Table 3 Results in the Model Development Procedure of the Final Model |
inhibitor = −0.60, when comedicated with enzyme inhibitors, otherwise = 0
Peripregnancy stage = 0, when Peripregnancy stage = Peripregnancy stage 1
Peripregnancy stage = 0.28, when Peripregnancy stage = Peripregnancy stage 2
Peripregnancy stage = 0.59, when Peripregnancy stage = Peripregnancy stage 3
Peripregnancy stage = 0.57, when Peripregnancy stage = Peripregnancy stage 4
Peripregnancy stage = −0.33, when Peripregnancy stage = Peripregnancy stage 5
For Chinese pregnant and postpartum WWE, the CL/F typical value of LTG estimated by the final model was 2.42 L/h. The final model demonstrated a significant improvement in inter-individual variability of CL/F compared to the base model, with values of 50.76% versus 32.96% (final model). Detailed information on the model parameters and bootstrap results were presented in Table 4.
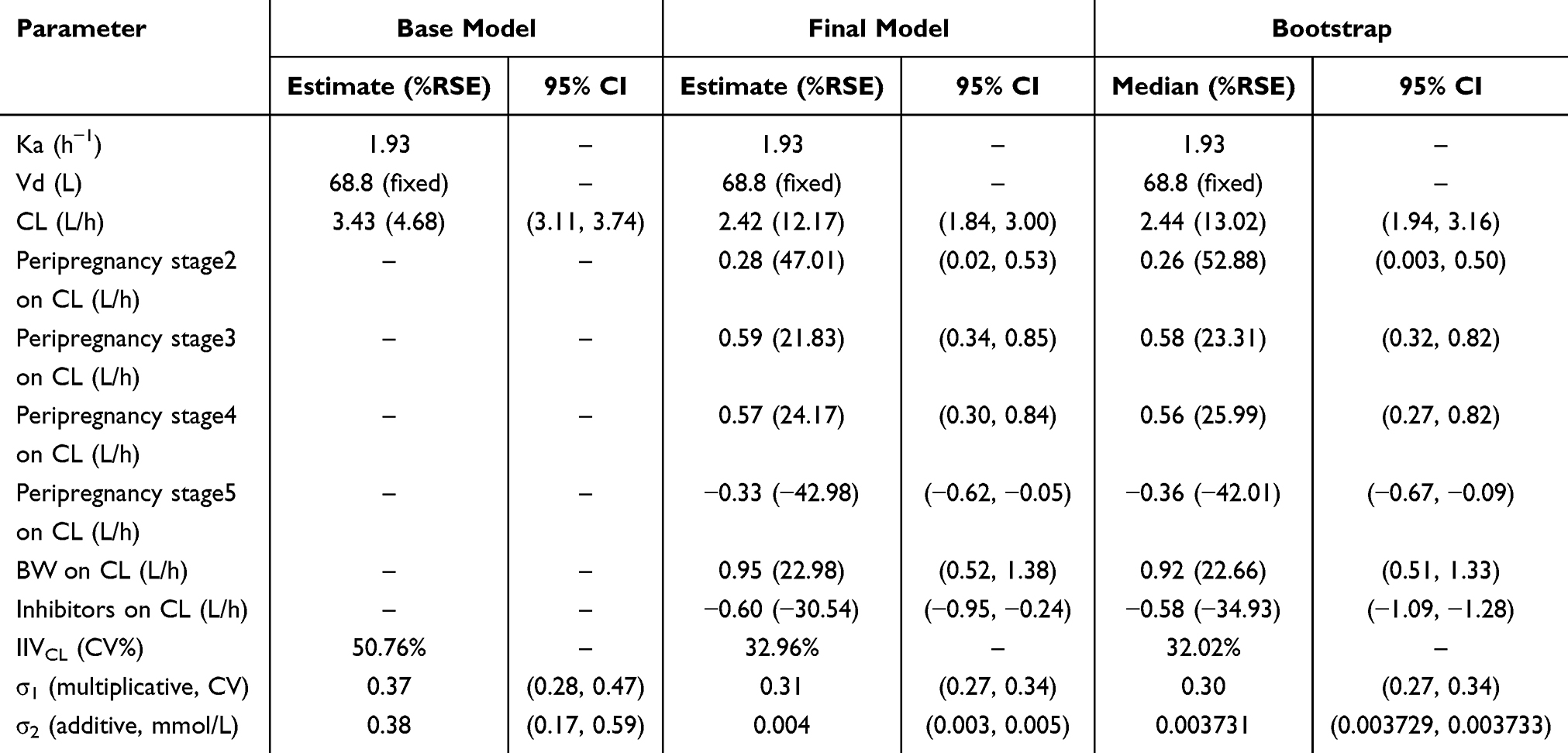 |
Table 4 Parameter Estimates and Bootstrap Results of Lamotrigine Population Pharmacokinetic Model |
Model Evaluation
As shown in Figure 2, the proximity of the observed values to the IPRED along the diagonal line (Y = X) indicated a closer alignment between the predicted and observed values, thereby reflecting a superior model fit. Furthermore, the CWRES of the refined model were randomly distributed around the zero line, with the majority of CWRES values falling within ±2. Overall, the GOF assessment of the final model demonstrated a strong concordance between the predicted and observed values.
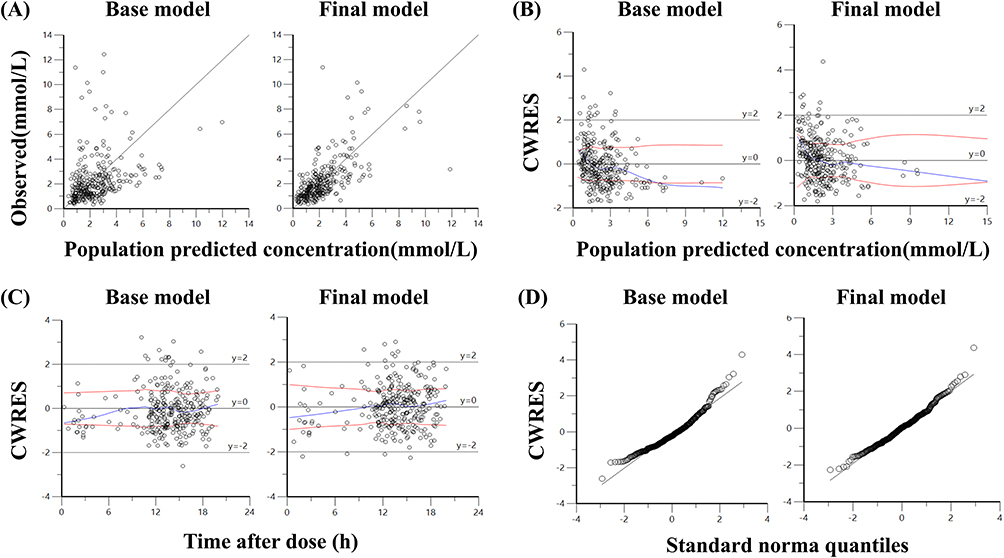 |
Figure 2 Diagnostic goodness-of fit plots of base model and final models: (A) Observed versus population predicted concentration (PRED); (B) Conditional weighted residual (CWRES) versus PRED; (C) Conditional weighted residual (CWRES) versus time after dose (TAD); (D) Quantile–quantile (QQ) plots of CWRES. |
As illustrated in Table 4, the Bootstrap program was configured to perform 1000 iterations of repeated sampling, and the model was successfully executed for all 1000 iterations. The point estimates of all PopPK parameters in the final model were consistent with the median values derived from the Bootstrap analysis, exhibiting a deviation of less than 1%. Furthermore, all parameter estimated fell within the 95% CI determined by the Bootstrap method.
The Predictive Check module was executed 1000 times, utilizing time after dose (TAD) as the horizontal axis and the observed values as the vertical axis. The model fitting was successful, and the results of the analysis were presented in Figure 3. The majority of the observed 5th, 50th, and 95th quantile lines fall within the corresponding simulated 5th, 50th, and 95th quantile ranges (represented by the shaded areas), indicating that the model demonstrated robust predictive capability across high, medium, and low concentration levels.
 |
Figure 3 Visual predictive check results of final model. Observed concentrations were depicted by dots. The 95th, 50th, and 5th percentiles of the predicted concentrations were represented by black dashed lines. The color shaded areas represented the 95% confidence intervals around the simulated 5th, 50th, and 95th percentiles. |
Figure 4 presented the NPDE diagnostic graph for the final model. The Q-Q plot and the histogram of the standard normal distribution indicated that the NPDE values of the final model approximately follow a standard normal distribution. Additionally, the predicted NPDE concentrations were randomly distributed around the reference line, with the majority falling within ±2. The statistical results of the NPDE for the final model were detailed in Table 5.
 |
Table 5 Statistic Test Results of NPDE in the Final Model |
 |
Figure 4 Normalized prediction distribution error (NPDE) plots of the models. (A) Histogram of the distribution of the NPDE against theoretical distribution (semitransparent blue fields); (B) Quantile–quantile plot of the distribution of the NPDE against theoretical distribution (semitransparent blue fields); (C) NPDE vs time after dose (h); (D) NPDE vs predicted concentrations. In plots (C and D), the three solid black lines represented the actual value of the NPDE at the 5th, 50th and 95th percentiles, the semitransparent red field represented a simulation-based 95% confidence interval for the median at 50th percentile, semitransparent blue fields represented a simulation-based 95% confidence interval for the corresponding model‐predicted 5th and 95th percentiles. The NPDE of the observations were represented by black dots. |
Monte Carlo Simulations
Figure 5 illustrated the increase in clearance rate beginning at 5 weeks of gestation, peaking during peripregnancy stages 3 and 4, and sharply declining postpartum, alongside Monte Carlo simulations of LTG steady-state trough concentrations under various dosing regimens. Compared with peripregnancy stage 1, the daily doses for peripregnancy stage 2 should be increased by 25–50%. For peripregnancy stages 3 and 4, the daily doses should be increased by approximately 67–100%. In the postpartum period, the daily dose of WWE should be reduced by 0–25%. Additionally, compared to the low weight group (50 kg), the daily dosage required an increase of 25–50% for the middle weight group (65 kg) and 33–67% for the high weight group (80 kg). Furthermore, when co-administered with VPA, the daily dose of LTG should be reduced by 33–67% compared to the dosage used without VPA.
 |
Figure 5 Boxplots of the distributions of simulated trough concentrations of LTG for 50 kg group, 65 kg group, 80 kg group under different dosing regimens at the peripregnancy stage 1, 2, 3, 4, 5. (A) Simulation of 50, 100, 150, 200, 250, 300 mg/d dose regimens in 50 kg group; (B) Simulation of 100, 150, 200, 250, 300 mg, 350 mg/d dose regimens in 65 kg group; (C) Simulation of 150, 200, 250, 300 mg, 350 mg, 400 mg/d dose regimens in 80 kg group. |
Table 6 summarized the recommended dosing regimens in detail.
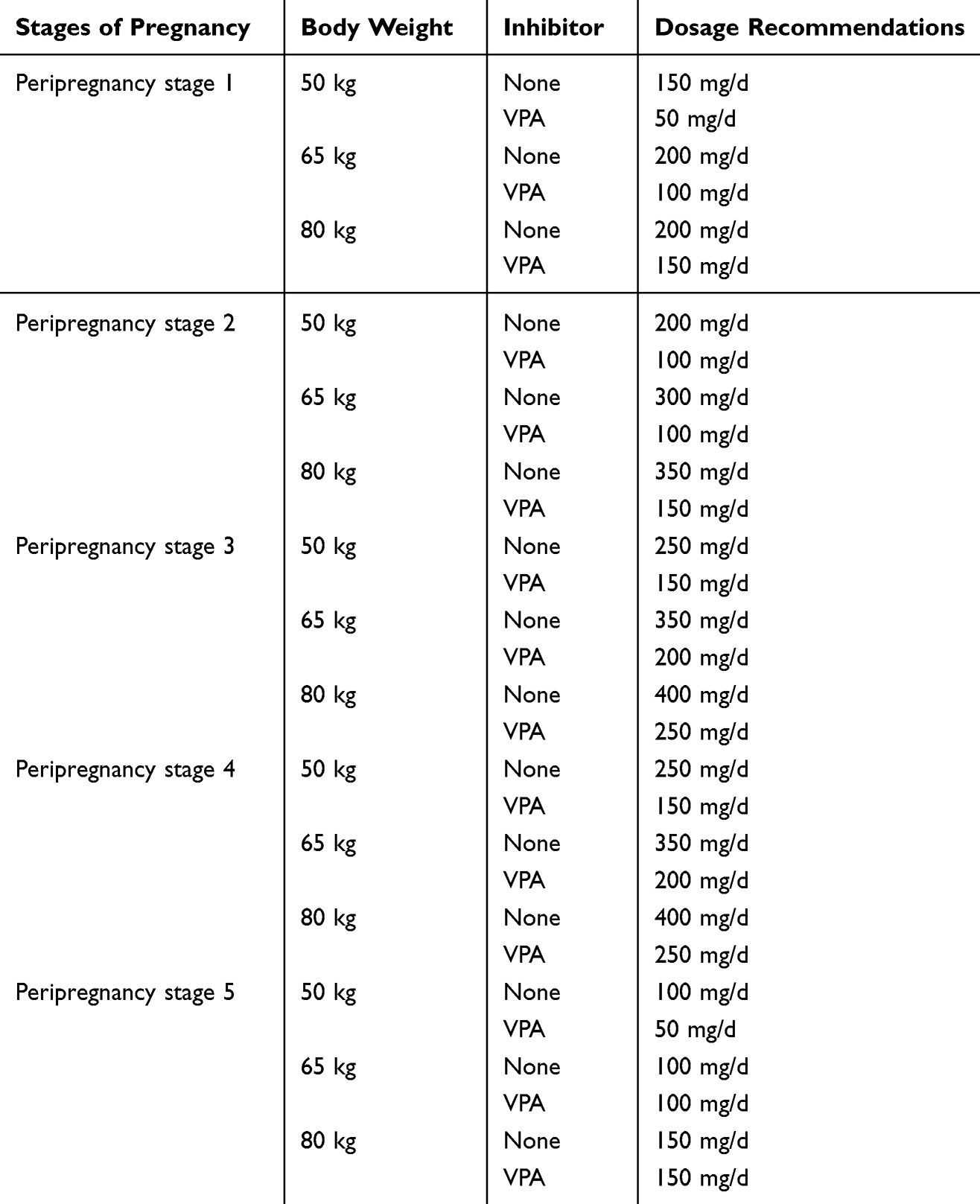 |
Table 6 Dosage Recommendations Based on the Final Model |
Discussion
This study developed and validated a PopPK model for LTG, and systematically evaluated the effects of demographic and clinical factors on the model parameters. Since most of the data were based on trough plasma concentrations, which could not provide sufficient insights into the absorption process, the values of Ka and V/F were fixed according to previous studies. The absorption of LTG was rapid, with Ka values in previous studies ranging from 1.09 to 3.18/h.25–28 In the study conducted by Wang et al,19 a meta-analysis of PopPK studies of LTG in WWE was performed to derive accurate historical Ka values. Consequently, the Ka value for the present study was established at 1.93/h and fixed during modeling. Previous PopPK studies conducted in adults with epilepsy reported Vd values ranging from 56.3 to 78.6 L,19,29,30 and this study set the Vd value as 59.8 L. The mean LTG CL/F value obtained in this study was 2.42 L/h, aligning with the estimated CL/F values (2.16–6.88 L/h)18,19,22 reported in pregnant patients with epilepsy.
Mechanisms of Body Weight, Gestational Age, and VPA on LTG Metabolism
The final PopPK model identified peripregnancy stage (ΔOFV = −38.2, p < 0.001), body weight (ΔOFV = −15.7, p = 0.002), and VPA coadministration (ΔOFV = −29.4, p < 0.001) as significant covariates influencing LTG CL/F. This peripregnancy staging system (including stages 1–4 and postpartum phases) demonstrated superior model fitness compared to traditional trimester classifications BIC: 412 vs 532). The PopPK analysis revealed that LTG CL/F levels varied across different stages of pregnancy, with levels in peripregnancy stages 2, 3, 4, and the postpartum stage representing 131%, 193%, 199%, and 68% of the levels observed in peripregnancy stage 1, respectively. These findings aligned with prior research on alterations in CL/F during pregnancy and the postpartum stage.18,19,31–33 It was proposed that circulating pregnancy hormones might compete with LTG, resulting in a reduction of LTG concentrations.18,19 Additionally, the plasma albumin level might be reduced due to the increased plasma volume associated with pregnancy. These pregnancy-related physiological changes could influence the CL/F of LTG. The elevated renal blood flow and glomerular filtration rate during pregnancy might increase renal excretion of LTG.34 The model confirmed that LTG clearance decreased sharply after delivery, returning to pre-pregnancy levels within 2–4 weeks. Failure to reduce the dosage promptly during this period might result in supratherapeutic plasma concentrations, thereby increasing the risk of LTG-related toxicities such as dizziness, ataxia, diplopia, nausea, and hypersensitivity reactions. Therefore, close therapeutic drug monitoring and timely dose reduction in the early postpartum period were crucial to minimize adverse events. Furthermore, the activities of the enzymes UGT1A4 and UGT2B7 were induced during pregnancy, potentially resulting in increased metabolism of LTG, which was predominantly metabolized by these isoenzymes.35
Body weight effects demonstrated a dose-dependent relationship (0.043 L/h/kg; r2 = 0.71), consistent with Young’s hepatic allometric scaling model (organ mass ∝ weight^0.74, p < 0.001).36,37 Patients ≥90 kg showed 2.3-fold higher CL/F than those ≤50 kg (p = 0.003).
Hepatic enzyme inhibitor could interfere with the breakdown of LTG, leading to a notable increase in plasma concentration when taken concurrently with VPA.38 Our study revealed that co-administration of VPA could decrease LTG CL/F by 46%. Similar findings had been reported by other researchers, with a 41% decrease in LTG CL/F observed in the Thai population,39 49% in the Spanish and German populations,36 and 46% in the Mexican population.40 VPA was a competing inhibitor of the UGT1A4, UGT1A4, and UGT2B7 enzymes responsible for LTG metabolism, leading to higher levels of LTG in the blood and a longer elimination time.41
Other Unexplored Covariates in LTG Metabolism
Several covariates, including demographic characteristics (age), hepatic function markers (AST, ALT, TP, ALB, TBIL/DBIL), renal function parameters (BUN, Cr), and enzyme-inducing medications, did not demonstrate statistically significant effects on LTG clearance in our final model. This lack of association could be explained by specific study population characteristics.
The absence of an observable impact of age on LTG CL/F in this research could potentially be attributed to the relatively limited age span (19–36 years), which could explain the non-existence of an age effect on LTG CL/F. Correspondingly, the majority of the participants in this study exhibited liver and kidney functions within the normal parameters. Only a single participant with WWE displayed a Cr below the standard range in at least two examinations. Consequently, this study did not identify a substantial impact of liver and kidney function on LTG CL/F.
Some studies included CBZ as a covariate in their final model,28,40 but this study failed to find its effect, because only 3 patients received CBZ in this study. Seven patients were co-administered OXC. Notably, OXC and its active metabolite, the monohydroxy derivative (MHD), had been shown to inhibit the CYP2C19 enzyme, induce the CYP3A4 and CYP3A5 enzymes, and exhibit only a slight induction of UDP-glucuronosyltransferase.42 Several studies had indicated that MHD functions as a relatively weak inducer of uridine diphosphate-glucuronyltransferase. Consequently, it was improbable that MHD significantly influences the pharmacokinetics of drugs predominantly metabolized via conjugation through UDPGT enzymes, such as LTG.42,43
Comparison with Previously Published PopPK Models in Epilepsy During Pregnancy
To date, only three studies have focused on the PopPK of LTG in patients with peripregnancy epilepsy. These investigations were characterized by notably small sample sizes and inconsistent findings across cohorts, as detailed in Table S2 (Supplementary Material). In contrast, the present study enrolled the largest patient cohort to date and established a relatively comprehensive PopPK model specific to pregnant and postpartum women with epilepsy, with key attributes including relevant covariates summarized in Table S3 (Supplementary Material).
Polepally et al18 first described pregnancy-related changes in LTG CL/F, but their model relied only on gestational age and overlooked body weight and co-medications, with limited data in early pregnancy. Karanam et al22 highlighted clearance changes as early as five weeks and proposed estradiol as a biomarker, yet the small sample size and variability in estradiol restricted clinical utility. Wang et al19 incorporated pharmacogenetics, improving explanation of inter-individual variability, but again sample size and limited early pregnancy data restricted generalizability. Tables S2 and S3 (Supplementary Material) respectively presented the basic characteristics of the study population and the model.
Compared to previous studies, our model offered several advancements. First, it incorporated a broader and more clinically relevant set of covariates, including body weight, gestational stage, and concomitant medications, which significantly enhanced its predictive accuracy and clinical applicability. Our study did not include estradiol levels as a covariate due to the lack of available data on estradiol levels, as well as its high inter-individual variability and limited feasibility for routine clinical application. Additionally, existing evidence highlighted the lower predictive reliability of estradiol compared to gestational age and body weight, further supporting our decision to prioritize more robust and clinically actionable predictors.22 Furthermore, this study was distinguished by its foundation on the largest cohort of pregnant and postpartum women with epilepsy reported to date, which ensured the robustness and generalizability of the findings. The substantial sample size enabled a comprehensive assessment of inter-individual variability across diverse patient subgroups and facilitated the development of practical, evidence-based dosage recommendations tailored to a range of clinical scenarios. Moreover, our model provided a detailed characterization of LTG CL/F changes as early as five weeks of gestation, addressing a critical gap in existing knowledge of early pregnancy pharmacokinetics. This comprehensive depiction supported timely therapeutic interventions and precise dosage adjustments during the critical early stages of pregnancy. Additionally, the model expanded its clinical utility by delivering individualized dosage recommendations stratified by body weight categories (low, medium, and high) and enzyme inhibitor use, offering comprehensive guidance across all stages of pregnancy and postpartum care.
Limitations
Due to the lack of pre-pregnancy therapeutic drug monitoring data for LTG, it was not feasible to accurately quantify the magnitude of change in LTG CL/F during pregnancy relative to pre-pregnancy baseline levels. The simulation of the postpartum period might also lack precision due to both the limited number of postpartum observations and the wide distribution of postpartum stage (1 to 84 days postpartum). Previous research indicated that LTG CL/F returned to pre-pregnancy levels within 2–4 weeks after delivery in WWE. Furthermore, this study did not incorporate genetic data to evaluate the influence of genotypes on LTG CL/F. Finally, as the study population consisted exclusively of Chinese pregnant and postpartum WWE, the generalizability of the model to other ethnic groups might be limited. Previous reports by Hussein et al25 and Grasela et al44 indicated that non-Caucasian populations exhibited 25% and 28.7% lower LTG CL/F compared to Caucasians, suggesting potential ethnic disparities in LTG pharmacokinetics. Thus, external validation is needed in other populations, including Caucasian, African, and multiethnic cohorts. Future multicenter studies with larger, diverse datasets and pharmacogenetic integration will be essential to confirm generalizability and refine individualized dosing strategies.
Conclusion
The PopPK model developed in this study could serve as a valuable tool for clinicians and pharmacists, facilitating personalized medication for patients with peripregnancy epilepsy. These findings could enhance the understanding of LTG therapy in pregnant women and support the development of improved clinical outcomes through more personalized treatment strategies. The model was rigorously validated using VPC, bootstrap analysis, and NPDE, all of which confirmed its high accuracy and precision. Simulations based on the model revealed a substantial increase in LTG CL/F during pregnancy, followed by a sharp decline after delivery. This robust PopPK model provided a valuable tool for designing personalized LTG dosing regimens in clinical practice. In future studies, it is necessary to include a larger sample size including different ethnic groups, investigate the effects of more covariates including pharmacogenomics on the pharmacokinetics of LTG in peripregnancy, and conduct model optimization and external validation of the model, which is of great clinical significance and will ultimately promote the clinical implementation of personalized medicine.
Abbreviations
ASMs, antiseizure medications; LTG, lamotrigine; VPA, valproic acid; OXC, oxcarbazepine; CBZ, carbamazepine; WWE, women with epilepsy; PopPK, population pharmacokinetic; LLOQ, the lower limit of quantitation; IND, enzyme inducer; BW, body weight; CL/F, clearance; Ka, the absorption rate constant; V/F, the apparent distribution volume; OFV, objective function value; AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; GOF, Goodness-of-fit; VPC, visual predictive check; NPDE, normalized prediction distribution errors; IPRED, individual population predicted concentrations; PRED, population predicted concentrations; CWRES, conditional weighted residuals; CI, confidence interval; MHD, monohydroxy derivative; TAD, time after dose.
Data Sharing Statement
The data and material are accessible upon reasonable request by contacting the corresponding author. The model code is accessible upon reasonable request by contacting the corresponding author.
Ethics Approval
The patients included in the study were from Beijing Tiantan Hospital of Capital Medical University and The Second Affiliated Hospital of Zhejiang University School of Medicine, and the study was approved by the Ethics Committee of the two hospitals (NO. KY2023-169-02; NO. I2024714).
Consent to Participate
Informed consent was acquired from each individual participant incorporated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Research Project on the Monitoring and Evaluation of Clinical Key Drug Utilization within the Chinese Research Hospital Society (2023). (grant number Y2023FH-YWPJ03-201).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gaus V, Ilyas-Feldmann M, Schmitz B. Epilepsie und Schwangerschaft. Der Nervenarzt. 2024;95:335–341. doi:10.1007/s00115-024-01626-4
2. Pennell PB, French JA, May RC, et al. Changes in seizure frequency and antiepileptic therapy during pregnancy. N Engl J Med. 2020;383:2547–2556. doi:10.1056/NEJMoa2008663
3. Decker BM, Thibault D, Davis KA, Willis AW. A nationwide analysis of maternal morbidity and acute postpartum readmissions in women with epilepsy. Epilepsy Behav. 2021;117:107874. doi:10.1016/j.yebeh.2021.107874
4. Dupont S, Vercueil L. Epilepsy and pregnancy: what should the neurologists do? Rev Neurol. 2021;177:168–179. doi:10.1016/j.neurol.2021.01.003
5. Meador KJ, Lindhout D. Epilepsy and unintended pregnancies. Neurology. 2017;88:724–725. doi:10.1212/WNL.0000000000003647
6. Harden CL, Pennell PB, Koppel BS, et al. Practice Parameter update: management issues for women with epilepsy—Focus on pregnancy (an evidence-based review): vitamin K, folic acid, blood levels, and breastfeeding. Neurology. 2009;73:142–149. doi:10.1212/WNL.0b013e3181a6b325
7. Tomson T, Marson A, Boon P, et al. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia. 2015;56:1006–1019. doi:10.1111/epi.13021
8. Jędrzejczak J, Bomba-Opoń D, Jakiel G, Kwaśniewska A, Mirowska-Guzel D. Managing epilepsy in women of childbearing age - Polish Society of Epileptology and Polish Gynecological Society Guidelines. Ginekol Pol. 2017;88:278–284. doi:10.5603/GP.a2017.0053
9. Llerda JAM, Marti AS, De la peña mayor P, et al. The Spanish Society of Neurology’s official clinical practice guidelines for epilepsy. Special considerations in epilepsy: comorbidities, women of childbearing age, and elderly patients. Neurologia. 2015;30:510–517. doi:10.1016/j.nrl.2014.08.002
10. Chang RSK, Lui KHK, Ip W, et al. Update to the Hong Kong Epilepsy Guideline: evidence-based recommendations for clinical management of women with epilepsy throughout the reproductive cycle. Hong Kong Med J. 2020;26:421–431. doi:10.12809/hkmj198367
11. Huber-Mollema Y, Oort FJ, Lindhout D, Rodenburg R. Behavioral problems in children of mothers with epilepsy prenatally exposed to valproate, carbamazepine, lamotrigine, or levetiracetam monotherapy. Epilepsia. 2019;60:1069–1082. doi:10.1111/epi.15968
12. Veroniki AA, Rios P, Cogo E, et al. Comparative safety of antiepileptic drugs for neurological development in children exposed during pregnancy and breast feeding: a systematic review and network meta-analysis. BMJ Open. 2017;7:e017248. doi:10.1136/bmjopen-2017-017248
13. Blotière PO, Miranda S, Weill A, et al. Risk of early neurodevelopmental outcomes associated with prenatal exposure to the antiepileptic drugs most commonly used during pregnancy: a French nationwide population-based cohort study. BMJ Open. 2020;10:e034829. doi:10.1136/bmjopen-2019-034829
14. Kashif T, Fathima N, Usman N, Qaseem A, Jayaraj JS. Women with epilepsy: anti-epileptic drugs and perinatal outcomes. Cureus. 2019;11:e5642. doi:10.7759/cureus.5642
15. Pennell PB, Karanam A, Meador KJ, et al. Antiseizure medication concentrations during pregnancy: results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) Study. JAMA Neurol. 2022;79:370–379. doi:10.1001/jamaneurol.2021.5487
16. Clark CT, Klein AM, Perel JM, Helsel J, Wisner KL. Lamotrigine dosing for pregnant patients with bipolar disorder. Am J Psychiatry. 2013;170:1240–1247. doi:10.1176/appi.ajp.2013.13010006
17. Tomson T, Landmark CJ, Battino D. Antiepileptic drug treatment in pregnancy: changes in drug disposition and their clinical implications. Epilepsia. 2013;54:405–414. doi:10.1111/epi.12109
18. Polepally AR, Pennell PB, Brundage RC, et al. Model-based lamotrigine clearance changes during pregnancy: clinical implication. Ann Clin Transl Neurol. 2014;1:99–106. doi:10.1002/acn3.29
19. Wang ML, Tao YY, Sun XY, et al. Estrogen profile- and pharmacogenetics-based lamotrigine dosing regimen optimization: recommendations for pregnant women with epilepsy. Pharmacol Res. 2021;169:105610. doi:10.1016/j.phrs.2021.105610
20. Methaneethorn J, Leelakanok N. Sources of lamotrigine pharmacokinetic variability: a systematic review of population pharmacokinetic analyses. Seizure. 2020;82:133–147. doi:10.1016/j.seizure.2020.07.014
21. Jiang R, Zhang D, Zhao Z, Mei S. Simultaneous determination of 24 antiepileptic drugs and their active metabolites in human plasma by UHPLC-MS/MS. J Pharm Biomed Anal. 2023;232:115437. doi:10.1016/j.jpba.2023.115437
22. Karanam A, Pennell PB, French JA, et al. Lamotrigine clearance increases by 5 weeks gestational age: relationship to estradiol concentrations and gestational age. Ann Neurol. 2018;26:556–563. doi:10.1002/ana.25321
23. Patsalos PN, Spencer EP, Berry DJ. Therapeutic drug monitoring of antiepileptic drugs in epilepsy: a 2018 update. Ther Drug Monit. 2018;40:526–548. doi:10.1097/FTD.0000000000000546
24. Hiemke C, Bergemann N, Clement HW, et al. Consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology: update 2017. Pharmacopsychiatry. 2018;51:e1. doi:10.1055/s-0037-1600991
25. Hussein Z, Posner J. Population pharmacokinetics of lamotrigine monotherapy in patients with epilepsy: retrospective analysis of routine monitoring data. Br J Clin Pharmacol. 1997;43:457–465. doi:10.1046/j.1365-2125.1997.00594.x
26. Chen C. Validation of a population pharmacokinetic model for adjunctive lamotrigine therapy in children. Br J Clin Pharmacol. 2000;50:135–145. doi:10.1046/j.1365-2125.2000.00237.x
27. Brzaković B, Vučićević K, Kovačević SV, et al. Pharmacokinetics of lamotrigine in paediatric and young adult epileptic patients--nonlinear mixed effects modelling approach. Eur J Clin Pharmacol. 2014;70:179–185. doi:10.1007/s00228-013-1606-5
28. Mallaysamy S, Johnson MG, Rao PGM, et al. Population pharmacokinetics of lamotrigine in Indian epileptic patients. Eur J Clin Pharmacol. 2013;69:43–52. doi:10.1007/s00228-012-1311-9
29. Wegner I, Wilhelm AJ, Lambrechts DA, Sander JW, Lindhout D. Effect of oral contraceptives on lamotrigine levels depends on comedication. Acta Neurol Scand. 2014;129:393–398. doi:10.1111/ane.12197
30. Milovanovic JR, Jankovic SM. Population pharmacokinetics of lamotrigine in patients with epilepsy. Int J Clin Pharmacol Ther. 2009;47:752–760. doi:10.5414/cpp47752
31. Fotopoulou C, Kretz R, Bauer S, et al. Prospectively assessed changes in lamotrigine-concentration in women with epilepsy during pregnancy, lactation and the neonatal period. Epilepsy Res. 2009;85:60–64. doi:10.1016/j.eplepsyres.2009.02.011
32. Pennell PB, Peng L, Newport DJ, et al. Lamotrigine in pregnancy: clearance, therapeutic drug monitoring, and seizure frequency. Neurology. 2008;70:2130–2136. doi:10.1212/01.wnl.0000289511.20864.2a
33. Ohman I, Luef G, Tomson T. Effects of pregnancy and contraception on lamotrigine disposition: new insights through analysis of lamotrigine metabolites. Seizure. 2008;17:199–202. doi:10.1016/j.seizure.2007.11.017
34. Anderson GD. Pregnancy-induced changes in pharmacokinetics: a mechanistic-based approach. Clin Pharmacokinet. 2005;44:989–1008. doi:10.2165/00003088-200544100-00001
35. Arfman IJ, Wammes-van der Heijden EA, Ter Horst PGJ, et al. Therapeutic drug monitoring of antiepileptic drugs in women with epilepsy before, during, and after pregnancy. Clin Pharmacokinet. 2020;59:427–445. doi:10.1007/s40262-019-00845-2
36. Rivas N, Buelga DS, Elger CE, et al. Population pharmacokinetics of lamotrigine with data from therapeutic drug monitoring in German and Spanish patients with epilepsy. Ther Drug Monit. 2008;30:483–489. doi:10.1097/FTD.0b013e31817fd4d4
37. Young JF, Luecke RH, Pearce BA, et al. Human organ/tissue growth algorithms that include obese individuals and black/white population organ weight similarities from autopsy data. J Toxicol Env Health Part A. 2009;72:527–540. doi:10.1080/15287390802647203
38. Lalic M, Cvejic J, Popovic J, et al. Lamotrigine and valproate pharmacokinetics interactions in epileptic patients. Eur J Drug Metab Pharmacokinet. 2009;34:93–99. doi:10.1007/BF03191157
39. Singkham N, Towanabut S, Lertkachatarn S, Punyawudho B. Influence of the UGT2B7 −161C>T polymorphism on the population pharmacokinetics of lamotrigine in Thai patients. Eur J Clin Pharmacol. 2013;69:1285–1291. doi:10.1007/s00228-012-1449-5
40. Chávez-Castillo CE, Medellín-Garibay SE, Del Carmen Milán-Segovia R, Rodríguez-Leyva I, Romano-Moreno S. Dosing recommendations based on population pharmacokinetics of lamotrigine in Mexican adult patients with epilepsy. J Pharm Sci. 2020;109:2902–2908. doi:10.1016/j.xphs.2020.05.030
41. Rowland A, Elliot DJ, Williams JA, Mackenzie PI, Dickinson RG, Miners JO. In vitro characterization of lamotrigine N2-glucuronidation and the lamotrigine-valproic acid interaction. Drug Metab Dispos. 2006;34:1055–1062. doi:10.1124/dmd.106.009340
42. Han X, Huang J, Lv J, et al. The influence of concomitant antiepileptic drugs on lamotrigine serum concentrations in Northwest Chinese Han population with epilepsy. PLoS One. 2019;14:e0210600. doi:10.1371/journal.pone.0210600
43. Flesch G. Overview of the clinical pharmacokinetics of oxcarbazepine. Clin Drug Investig. 2004;24:185–203. doi:10.2165/00044011-200424040-00001
44. Grasela TH, Fiedler-Kelly J, Cox E, Womble GP, Risner ME, Chen C. Population pharmacokinetics of lamotrigine adjunctive therapy in adults with epilepsy. J Clin Pharmacol. 1999;39:373–384. doi:10.1177/00912709922007949
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.