Back to Journals » Clinical Interventions in Aging » Volume 17
Dose Selection of Ropivacaine for Spinal Anesthesia in Elderly Patients with Hip Fracture: An Up-Down Sequential Allocation Study
Authors Wang Y ![]() , Zha H, Fang X, Shen T, Pan K, Zhang J, He K, Wang S
, Zha H, Fang X, Shen T, Pan K, Zhang J, He K, Wang S ![]() , Hu L
, Hu L
Received 18 April 2022
Accepted for publication 2 August 2022
Published 11 August 2022 Volume 2022:17 Pages 1217—1226
DOI https://doi.org/10.2147/CIA.S371219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Yu Wang,1,* Hanning Zha,1,* Xiang Fang,2 Tianjiao Shen,1 Kunyun Pan,1 Jianping Zhang,1 Keqiang He,1 Sheng Wang,1 Liguo Hu1
1Department of Anesthesiology, The First Affiliated Hospital of USTC (Anhui Provincial Hospital), Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China; 2Department of Anesthesiology, Hefei BOE Hospital, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Sheng Wang; Liguo Hu, Email [email protected]; [email protected]
Objective: The dose selection of ropivacaine for spinal anesthesia in clinical work mainly depends on the experience of the anesthesiologist. In this study, a prospective and modified up-down sequential allocation design was used to provide the optimal dose selection of ropivacaine for spinal anesthesia.
Patients and methods: This study was divided into two stages, and a total of 164 elderly patients with elective hip fractures were included. In stage I, the dose of ropivacaine was selected using the up-down sequential method of height correction, and the 50% effective dose (ED50) and 95% effective dose (ED95) were obtained. A nomogram for predicting satisfactory anesthesia and a formula for predicting the optimal dose was also given in this stage. In stage II, the dose of ropivacaine was calculated by using the optimal dose prediction formula, so as to evaluate the efficacy and safety of the model.
Results: The ED50 and ED95 of the stage I were 7.036 mg (95%CI 6.549– 7.585 mg) and 8.709 mg (95%CI 7.902– 14.275 mg), respectively. And provided a nomogram predicting satisfactory anesthesia with a C-index of 0.847 (95%CI 0.774– 0.92). The optimal dose prediction formula of ropivacaine was calculated, including variables for age, gender, height, and weight. This formula was found to be 90% efficient. It is worth mentioning that the incidence of direct transfer to the ward in the two stages was as high as 86.84% and 93.33%, respectively, and no patients were transferred to the ICU in stage II.
Conclusion: The ED50 and ED95 of ropivacaine were 7.036 mg and 8.709 mg, respectively, and the nomograms are sufficiently accurate to predict satisfactory anesthesia. Beyond that, the dose prediction equation provided in this study has high efficacy and safety, and can guide the dose selection of spinal anesthesia in elderly patients with hip fracture in clinical practice.
Clinical trials registration: ChiCTR2100046982
Keywords: ropivacaine, dose selection, elder, spinal anesthesia, Hip fracture, sequential design
Introduction
According to data from China’s seventh census in 2020, the 60-year-old population has reached 264 million, accounting for 18.7% of the total population; of which 190 million are 65-year-old, accounting for 13.5% of the total population, and have begun to enter the “aging society”. Concomitantly, the periarticular fragility fracture of the hip, a common serious injury, has significantly increased in incidence.1 Hip fractures are recognized as a major threat to older adults, with nearly one-third of patients dying within a year of a hip fracture, and about 50% of survivors unable to return to their pre-fracture functional status.1,2 Patients with hip fractures experience a variety of complications, including frailty.3 And frailty is a predisposing factor for falls and other adverse events, including organ decline, emergency hospitalization, nursing home admission, and death.4 Moreover, frail patients who are already in poor health will become even frailer due to pain, mobility problems and inability to take care of themselves.5 This creates a bad vicious circle.
Regaining mobility after surgery is a top priority in the treatment of hip fractures in elderly patients. However, the choice of anesthesia for elderly hip fracture surgery remains controversial.6 Previous studies have shown that spinal anesthesia does not provide better outcomes after surgery for elderly patients with hip fractures.7,8 Whereas, there are also many studies support spinal anesthesia as the advantages of shortened hospital stay, higher patient satisfaction, shorter anesthesia recovery time, and reduced postoperative opioid consumption.9–11 In addition, spinal anesthesia has the advantages of fast onset, complete block, and no impact on respiratory function,12 which can be widely used in elderly hip fracture surgery. In fact, with the development of ultrasound-guided intraspinal puncture technology, the success rate of intraspinal puncture including spinal anesthesia has significantly increased,13 which may further improve the satisfaction of spinal anesthesia.
At present, the medication and dosage of spinal anesthesia for elderly patients are basically determined by anesthesiologists based on experience, and the dosage of the medication directly affects the patient’s anesthesia effect, hemodynamics, and further affects the prognosis. In this study, 50% and 95% effective doses of ropivacaine in spinal anesthesia (ED50 and ED95) in elderly patients with hip fracture surgery were determined by a modified sequential design. At the same time, the prediction formula of the individual optimal dose is provided to guide the dose selection of ropivacaine in elderly patients with hip surgery and spinal anesthesia in clinical work.
Materials and Methods
Study Design
This is a prospective, modified up-down sequential allocation study, which was conducted in the Department of Anesthesiology of the First Affiliated Hospital of the University of Science and Technology of China from June 2021 to March 2022, and passed the ethics review of the hospital ethics committee (2021KY113), and completed the registration in the China Clinical Trial Registration Center (ChiCTR2100046982). All study participants read and signed informed consent forms. This trial was conducted in accordance with the Declaration of Helsinki.
Eligibility Criteria
The inclusion criteria included (1) ASA classification II–IV; (2) Age ≥ 65 years old; (3) Elective hip fracture surgery (included femoral neck, femoral head, intertrochanteric or subtrochanteric fractures); (4) Sign the informed consent. Exclusion criteria included (1) Administered sedative and analgesic drugs within 3 hours before surgery; (2) Severe dementia; (3) Have uncontrolled neurological or psychiatric diseases; (4) Severe multiple injuries; (5) Contraindications to spinal anesthesia; (6) Participated in other drug trials within three months.
Anesthesia Procedures
Patients fasted for 8 hours before surgery. After entering the room, a “Venturi” mask with an oxygen flow of 2 L/min was used to inhale oxygen, open the venous access, connect the monitor, and continuously monitor the electrocardiogram (ECG), invasive blood pressure (IBP), pulse oxygen saturation (SpO2) and heart rate (HR). The anesthesia method is combined spinal-epidural anesthesia, the puncture is performed after ultrasound-guided positioning,14 the puncture point is L2-3, 2% lidocaine is selected as the local infiltration anesthesia, and 0.5% ropivacaine diluted with 10% glucose solution was used for spinal anesthesia. The patient is placed in a lateral recumbent position (the affected side is down), and spinal anesthesia is performed first. After the cerebrospinal fluid is confirmed to be smooth, 0.5% ropivacaine is given in about 30 seconds. Then an epidural catheter of 3–5 cm is indwelled in the epidural space. After ropivacaine injection, the lateral decubitus position was maintained for 15min to achieve unilateral block.15 Intraoperatively, additional 1% lidocaine should be added to the epidural space as needed, at the discretion of the anesthesiologist. The epidural catheter was removed after surgery.
Study Interventions
The dose of ropivacaine received by each patient in stage I was determined by a sequential method. Specifically, the initial dose was set at 7.5 mg. When the anesthesia effect of the previous patient was satisfactory, the dose of the next patient was reduced by 0.5 mg; when the anesthesia effect of the previous patient was unsatisfactory, the dose of the next patient was increased by 0.5 mg. In addition, considering the clear effect of height on the dose of spinal anesthesia, the dose should be further corrected by reference to height: for every 10cm increase or decrease in height, the dose should be increased or decreased by 0.5mg.
Definition of Satisfactory Anesthesia: (1) Anesthesia plane (assessed by acupuncture): higher than T10, lower than T6; (2) Pain-free operation within the first hour of surgery.
After the establishment of the optimal dose formula, the validation cohort was included in stage II. Spinal anesthesia was performed using the ropivacaine dose provided by the formula to evaluate the effectiveness of the formula to guide clinical ropivacaine dose selection and the success rate of meeting surgical needs.
Sample Size Calculation
The logistic regression model of this study plans to screen independent variables such as age, gender, height, weight, ASA classification, hemoglobin, white blood cells, red blood cells, and C-reactive protein. The calculation is based on the Events Per Variable principle,16 that is, the sample size is the independent Variable expected to be included multiplied by 10. Furthermore, considering the 20% dropout rate, 114 cases were finally included in the stage I of this study. In stage II, another 30 cases were included to verify the formula. A total of 144 patients.
Statistical Analysis
For numeric variables, the Shapiro-Wilk test was used to verify normality. Normally distributed variables are expressed as the mean (standard deviation), and abnormally distributed variables are expressed using the median (interquartile range). Categorical variables are expressed as numbers (percentages). Independent two-sample t-tests were used to compare normally distributed variables. Abnormally distributed variables were compared using the Mann-Whitney U test. Categorical variables were analyzed using the χ2 test or Fisher’s exact test. Probit regression was used to calculate ED50, ED95 and their 95% confidence interval (CI). Logistic regression was used to screen variables, and odds ratio (OR) was used to describe the variables included in univariate and multivariate regression models. Meanwhile, nomogram is established, and C-index evaluates its predictive ability. For patients who meet satisfactory anesthesia, a multiple linear regression model is used to establish a dose prediction equation. Data were analyzed using SPSS (version 24.0; SPSS Inc., IBM, Chicago, IL, USA). All statistical tests were two-tailed, and a P-value less than 0.05 was defined as statistically significant.
Results
Overall, a total of 180 patients were screened in this study between June 2021 and April 2022. Among them, in stage I, 15 patients refused to participate, 14 patients did not meet the criteria for admission, and 2 patients were unsuccessful in spinal anesthesia; In stage II, 1 patient refused to participate, and 4 patients did not meet the criteria for admission. A total of 144 patients completed the study, 114 in stage I and 30 in stage II. The complete selection flow chart of subjects in this study is shown in Figure 1. Baseline characteristics such as demographics and surgical information are shown in Table 1.
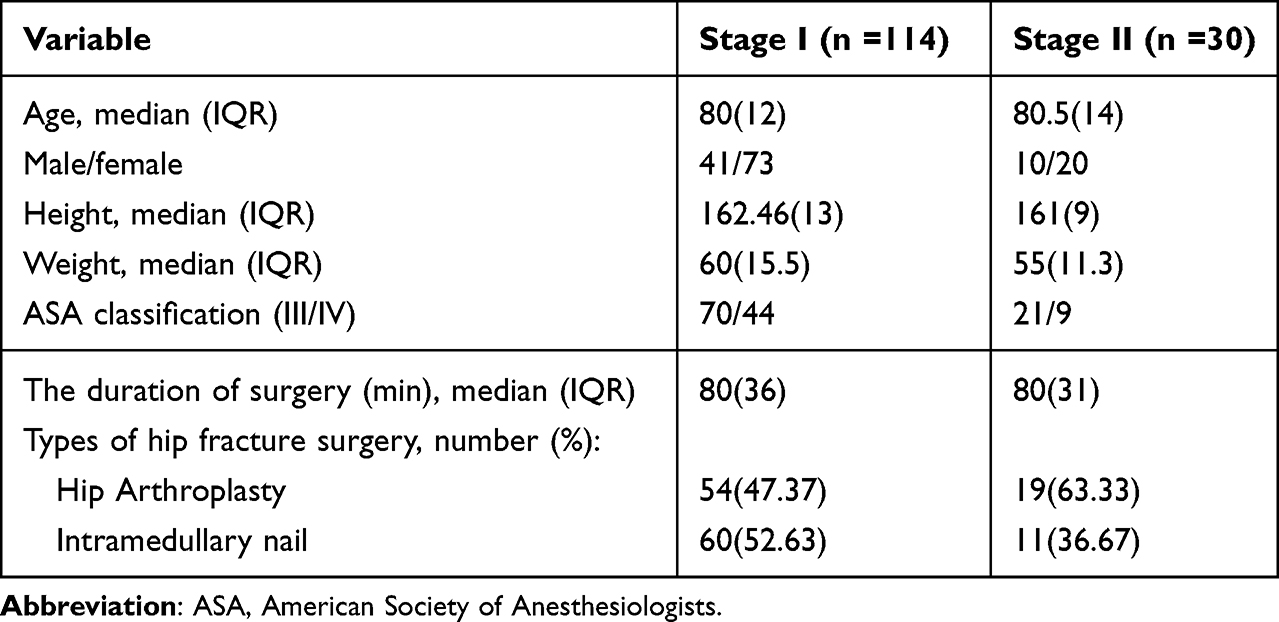 |
Table 1 Baseline Characteristics |
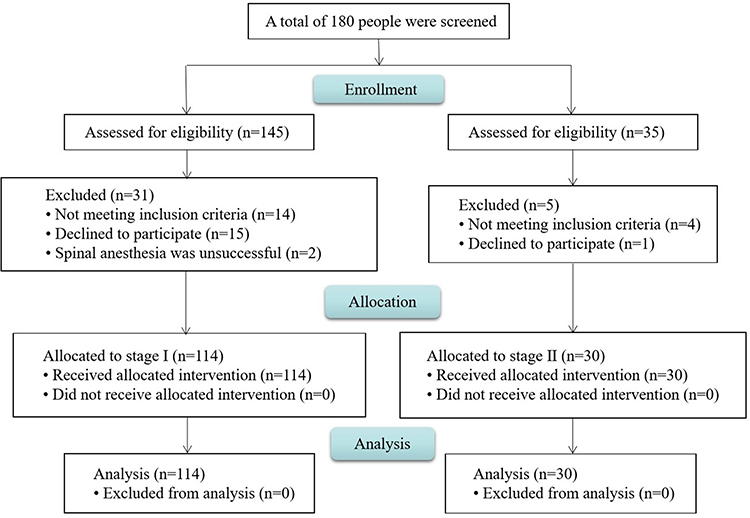 |
Figure 1 Flow chart of the study. |
ED50 (CI) and ED95 (CI)
According to the calculation results of Probit regression, the ED50 and ED95 of ropivacaine for spinal anesthesia of elderly hip fracture were 7.036 mg (95%CI 6.549–7.585 mg) and 8.709 mg (95%CI 7.902–14.275 mg), respectively. Goodness-of-fit test of the model P=0.108 > 0.05. The specific dose and the corresponding number of cases are shown in Table 2.
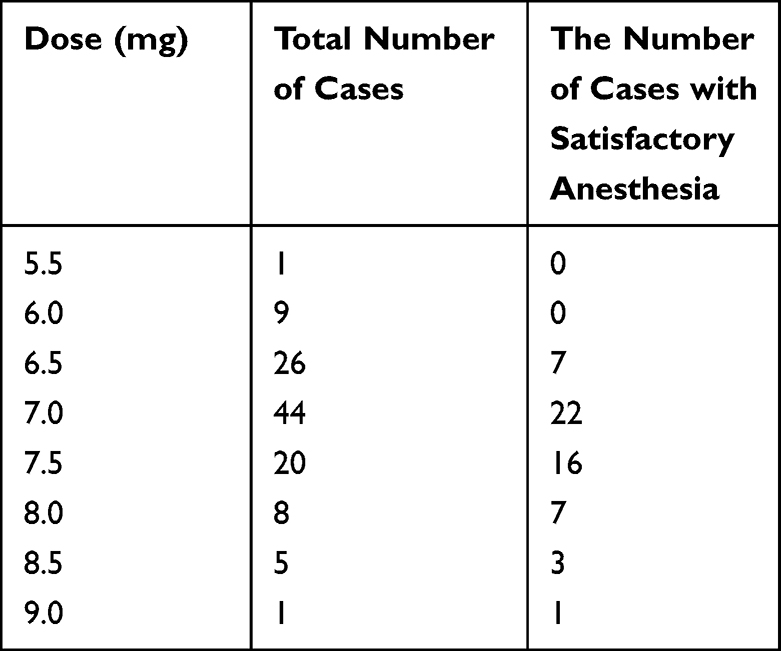 |
Table 2 Dose and Corresponding Number of Cases |
Variable Filtering and Nomogram
Nine independent variables were included in this study and entered into logistic regression, including age, gender, height, weight, ASA classification, hemoglobin, white blood cells, red blood cells, and C-reactive protein. Group comparisons are made according to whether satisfactory anesthesia is achieved. Comprehensive consideration of univariate analysis results and clinical practice, and finally screen out age, gender, height, and weight into the model. Crude and adjusted OR are shown in Table 3. It should be explained that the OR value failed to reflect the correlation between height and anesthesia effect because the sequential plan was modified by using height in this study.
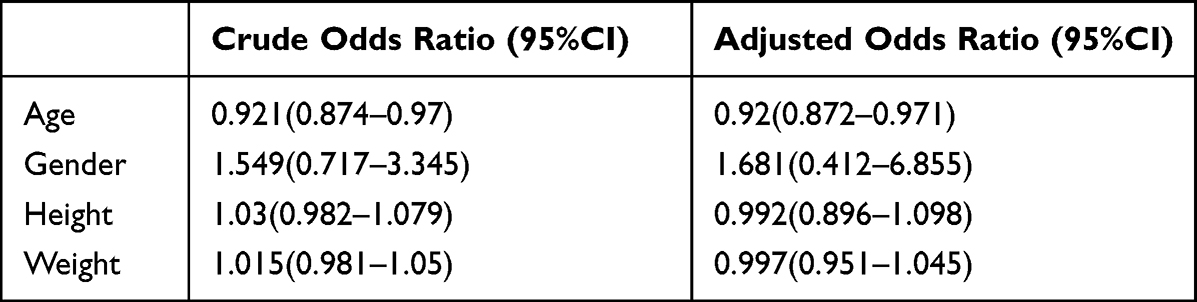 |
Table 3 Multivariate Logistic Regression Model |
Additionally to that, we visualized the logistic regression model using the nomogram constructed by the factors described above (Figure 2). Using C-index to evaluate the discrimination of the nomogram, C-index=0.847 (95%CI 0.774–0.92), suggesting good prediction accuracy. The nomogram model was internally verified by Bootstrap repeated 1000 times sampling method, and the calibration curve of the prediction model was obtained (Figure 3), which showed that the prediction model was in good consistency with the actual observed results.
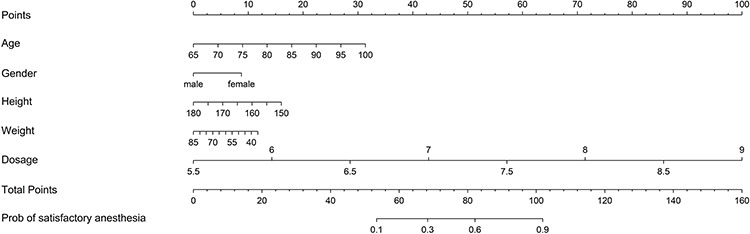 |
Figure 2 Nomogram to predict probability of satisfactory anesthesia. |
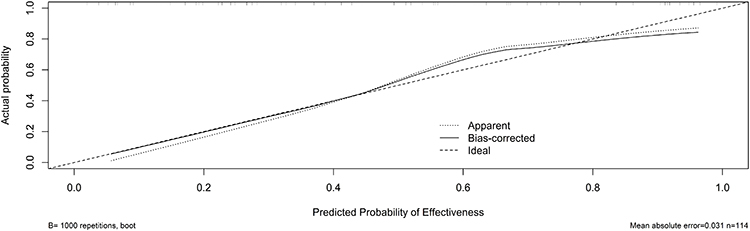 |
Figure 3 Calibration curve for nomogram. |
Formula for Predicting the Optimal Dose
According to the definition of satisfactory anesthesia in this study, there were 58 patients with appropriate anesthesia plane and satisfactory analgesic effect within the first hour of surgery. Based on this, the multiple linear regression model was used to incorporate age, gender, height and weight into the model as independent variables, and the following formula can be calculated: Dose(mg) = -1.39 + age(year)*0.011 - gender(male = 1; female = 0)*0.249 + height(cm)*0.047 + weight(kg)*0.005
This calculation equation has statistical significance, F=5.691, P=0.001<0.05, indicating that there is a linear correlation between the dependent variable and the independent variable. Correlation coefficient R=0.548, determination coefficient R2=0.3.
Verification of Efficacy and Safety of the Formula
The stage II of this study included 30 patients, and the same anesthesia protocol was implemented as the stage I. The ropivacaine dose was provided by the prediction equation established in stage I. Finally, the anesthesia plane of 1 patient was below T10, 1 patient felt pain during skin incision, and the other 1 patient were satisfied with analgesia at the beginning of the operation, but the duration was less than 1 hour. The anesthesia plane of the 27 patients was suitable and could provide a completely satisfactory anesthesia effect within the first hour of surgery, indicating that the formula had an effective rate of 90%. Namely, this predictive formula can guide clinical ropivacaine dose selection to a considerable extent.
Perioperative Events
The perioperative-related adverse events in this study were mainly hemodynamic changes, including hypertension and hypotension after spinal anesthesia. In stage I, 20 patients had hypotension and 11 patients had hypertension. The cases of hypotension and hypertension in stage II were both 3. It should be noted that there was no significant and uncorrectable hypotension during the trial. The occurrence of hypertension may be related to the nervousness of patients during the operation. The number of patients with inappropriate anesthesia plane or insufficient analgesia within the first hour of surgery according to the definition of satisfactory anesthesia is shown in Table 4.
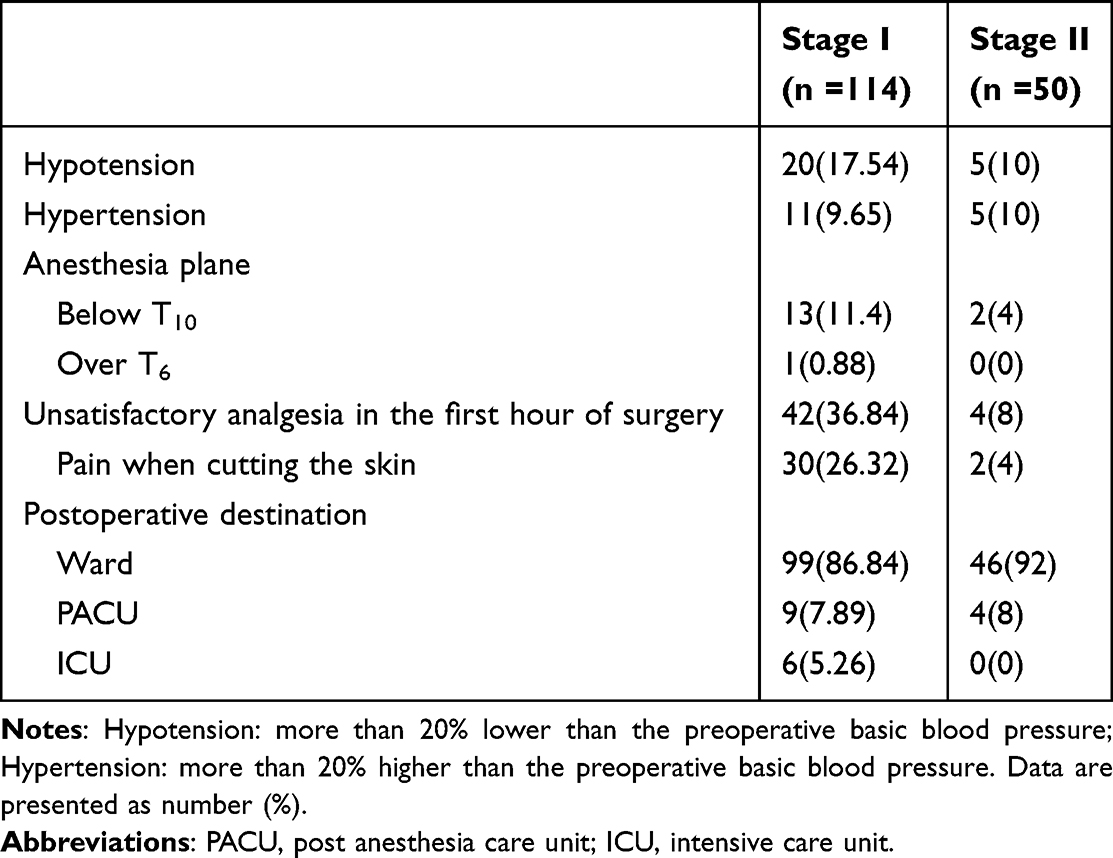 |
Table 4 Perioperative Events |
In stage I, after surgery, 99 patients (86.84%) were directly transferred to the ward, 9 (7.89%) were transferred to PACU, and 6 (5.26%) were transferred to ICU. In the stage II, after surgery, 28 patients (93.33%) were directly transferred to the ward, 2 (6.67%) were transferred to PACU, and none were transferred to the ICU.
Discussion
In this prospective, modified up-down sequential allocation study, we first calculated the ED50 and ED95 of ropivacaine for spinal anesthesia in the elderly with hip fractures, with specific values of 7.036 mg and 8.709 mg, respectively. After that, by screening the factors affecting the anesthetic effect, a more intuitive nomogram for predicting satisfactory anesthesia was established. The calculation formula for predicting the optimal dose of ropivacaine is then provided directly through the multiple linear regression model, and the factors included in the regression model included age, gender, height, and weight. After that, in stage II, the ropivacaine dose provided by the formula was used for spinal anesthesia, and the success rate was 90%. To our knowledge, this study is the first to provide a formula for calculating the optimal dose of ropivacaine for elderly hip fracture surgery.
Mei et al showed that the ED50 and ED95 of hyperbaric ropivacaine for cesarean section were 11mg and 15mg,17 and the sequential study of Lv et al showed that the ED50 of hyperbaric ropivacaine for cesarean section was 8.29mg.18 Practically, due to high abdominal pressure and distended intraspinal veins, the drug dose required for spinal anesthesia for puerperae is lower than that of non-puerperae women. However, the dose in the above study was still significantly higher than the ED50 and ED95 of 7.036 mg and 8.709 mg in this study. We believe that the main reason for the difference is that, in this study, after ropivacaine was injected into the subarachnoid space, the lateral decubitus position was maintained for 15 minutes, which enabled the realization of Unilateral spinal anesthesia. Secondly, the puncture point of L2-3 can also reduce the dosage of anesthetic drugs. Advanced age may be another reason.
There are many factors influencing the effect of spinal anesthesia. Age, height, weight, body position, drug specific gravity, liquid volume, concentration, injection speed, puncture point, patient position, abdominal circumference, and even lumbosacral cerebrospinal fluid volume can all affect the anesthesia block plane.19–24 In this trial, we controlled the controllable factors as much as possible, and the patient’s body position, puncture point, drug specific gravity, concentration, and injection speed were all kept consistent. On this basis, statistical analysis first found that age was a statistically significant influencing factor. Moreover, height, as part of the modified sequential protocol, also indisputably influenced the trial results. Furthermore, considering that elderly patients have large differences in body weight, and gender may affect patients’ perception of pain. Finally, four factors of age, gender, height, and weight are included in the statistical model. Then, we used these four factors to build a nomogram in order to more intuitively discover the impact of the inclusion factors on the probability of satisfactory anesthesia.
The dose of spinal anesthesia drugs significantly affect the anesthesia effect, including the analgesia plane, hemodynamics, and even long-term prognosis.25 The physiological homeostasis of the elderly is significantly more likely to be affected due to their weak vascular elasticity and poor nutritional status. At present, there is no unified plan for dose selection for elderly hip fracture surgery. Our study provides a formula for the dose selection of ropivacaine for spinal anesthesia, and the effective rate is 90%, which has high practical value. It is worth mentioning that the definition of satisfactory anesthesia in this study is that there is no pain within the first hour of the operation. Although the duration is not long, it can fully ensure that the dose is not excessive and the hemodynamics is stable. Furthermore, considering that surgically destructive stimulation, including skin incision and reamed intramedullary, occurs mainly within the first hour, the dose provided by the formula can be considered the lowest and optimal option.
Previous literature has suggested that appropriate spinal anesthesia has better perioperative hemodynamic stability than general anesthesia, and the need for intraoperative vasopressors is also significantly reduced.26 In elderly patients, the incidence of blood pressure drop after spinal anesthesia can be as high as 75%.27 In contrast, in this study, the incidence of hypotension after spinal anesthesia was only 20% in stage I and 10% in stage II. The main reason for this advantage is that unilateral anesthesia was well implemented in this trial, and only unilateral sympathetic nerves were blocked as much as possible. Moreover, the definition of satisfactory anesthesia in this study is relatively loose, and it is not mandatory that a single dose can meet the needs of the entire operation, resulting in a significant reduction in drug dosage. In addition to hemodynamics, the postoperative destination is also worthy of attention. In this study, the proportion of patients directly transferred to the general ward after surgery was as high as 86.84% and 93.33% respectively in the two trial stages, which may bring significant improvement in patient satisfaction and also help alleviate the shortage of anesthesia medical resources in China. It is worth noting that in stage II, when dose selection was guided by the calculation formula, the number of patients admitted to the ICU was 0, while the literature reported that the ICU transfer rate was about 7% in the elderly after surgery for hip fracture under general anesthesia.28 Given that the median age of patients in this study was as high as 80 years, the prognostic advantage of reducing the rate of ICU admission may have been greater than expected.
In addition to the above, there are some peculiarities in this study in terms of the trial protocol. First, the puncture site for spinal anesthesia was L2-3, considering that previous studies have provided some dosage options for L3-4.25,29 And due to factors such as hyperosteogenesis and ligament calcification in elderly patients,30 there are always some cases of failed puncture in the L3-4 space. At that time, L2-3 is a safe additional choice. Moreover, ultrasound-guided positioning can ensure the accuracy of puncture point. Second, we chose hyperbaric liquid in this trial, based on the fact that hyperbaric liquid can achieve anesthesia block effect more quickly than hypobaric and isobaric,31,32 and is more popular among surgeons.
There are also some limitations worth discussing in this study. First, this study did not set up a control group, but only a dose-finding test of ropivacaine in a single group. It is still necessary to compare with other commonly used drugs for spinal anesthesia such as bupivacaine in the future to determine the best choice of drug types. Second, this study paid relatively little attention to the prognosis of patients, mainly because we focused on the evaluation of intraoperative anesthesia effect, and the comparison of prognosis also needed to set up a control group. Last but not least, the calculation of the sample size of this study is based on the minimum sample size of logistic regression, which does not mean that the sample size is sufficient. In particular, the efficacy and safety of the calculation formula need to be confirmed by clinical trials with larger samples, or even randomized controlled trials.
At present, the debate on the pros and cons of different anesthesia options for elderly hip fractures is still ongoing. This study starts with spinal anesthesia, focuses on the dose selection of ropivacaine, and gives a specific calculation formula, which meets the requirements of precise anesthesia. Subsequent research can further compare the different densities of drugs and different types of drugs in spinal anesthesia, and screen the optimal general anesthesia scheme at the same time. Finally, comparing the optimal spinal anesthesia scheme with the optimal general anesthesia scheme is the future direction to explore the choice of anesthesia for elderly hip fracture surgery.
Conclusion
In conclusion, this study explored the optimal dose of ropivacaine for spinal anesthesia in elderly hip surgery. The ED50 and ED95 were 7.036 mg and 8.709 mg respectively. A nomogram for predicting satisfactory anesthesia was established with high accuracy. In addition, this study also provides a dose prediction equation of ropivacaine, which has high efficacy and safety, and can guide anesthesiologists in the choice of dose in clinical practice.
Data Sharing Statement
Six months after the main results are published, the individual participant data of this research report can be accessed with the permission of the corresponding authors. The study protocol, statistical analysis plan, and clinical study report will also be available.
Acknowledgments
Appreciate for the support from the Orthopedist and nursing teams of the First Affiliated Hospital of USTC.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was not funded by any source in the public, commercial, or nonprofit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bellelli G, Morandi A, Trabucchi M., et al. Italian intersociety consensus on prevention, diagnosis, and treatment of delirium in hospitalized older persons. Intern Emerg Med. 2018;13(1):113–121. doi:10.1007/s11739-017-1705-x
2. Bellelli G, Mazzola P, Corsi M, et al. The combined effect of ADL impairment and delay in time from fracture to surgery on 12-month mortality: an observational study in orthogeriatric patients. J Am Med Dir Assoc. 2012;13(7):
3. Inoue T, Maeda K, Nagano A, et al. Undernutrition, sarcopenia, and frailty in fragility hip fracture: advanced strategies for improving clinical outcomes. Nutrients. 2020;12(12):3743. doi:10.3390/nu12123743
4. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
5. Bergström U, Jonsson H, Gustafson Y, et al. The Hip fracture incidence curve is shifting to the right. Acta Orthop. 2009;80(5):520–524. doi:10.3109/17453670903278282
6. Griffiths R, Babu S, Dixon P, et al. Guideline for the management of hip fractures 2020: guideline by the association of anaesthetists. Anaesthesia. 2021;76(2):225–237. doi:10.1111/anae.15291
7. Du YT, Li YW, Zhao BJ, et al; Peking University Clinical Research Program Study Group. Long-term survival after combined epidural-general anesthesia or general anesthesia alone: follow-up of a randomized trial. Anesthesiology. 2021;135(2):233–245. doi:10.1097/ALN.0000000000003835
8. Kowark A, Adam C, Ahrens J, et al.; iHOPE study group. Improve Hip fracture outcome in the elderly patient (iHOPE): a study protocol for a pragmatic, multicentre randomised controlled trial to test the efficacy of spinal versus general anaesthesia. BMJ Open. 2018;8(10):e023609. doi:10.1136/bmjopen-2018-023609
9. Neuman MD, Rosenbaum PR, Ludwig JM, Zubizarreta JR, Silber JH. Anesthesia technique, mortality, and length of stay after Hip fracture surgery. JAMA. 2014;311(24):2508–2517. doi:10.1001/jama.2014.6499
10. Capdevila X, Aveline C, Delaunay L, et al. Factors determining the choice of spinal versus general anesthesia in patients undergoing ambulatory surgery: results of a multicenter observational study. Adv Ther. 2020;37(1):527–540. doi:10.1007/s12325-019-01171-6
11. Turner EHG, Whalen CJ, Beilfuss MA, Hetzel SJ, Schroeder KM, Spiker AM. Neuraxial anesthesia is associated with decreased pain scores and post-anesthesia care unit opioid requirement compared with general anesthesia in hip arthroscopy. Arthroscopy. 2021;37(1):139–146. doi:10.1016/j.arthro.2020.08.032
12. Stewart J, Gasanova I, Joshi GP. Spinal anesthesia for ambulatory surgery: current controversies and concerns. Curr Opin Anaesthesiol. 2020;33(6):746–752. doi:10.1097/ACO.0000000000000924
13. Chin KJ, Perlas A, Chan V, Brown-Shreves D, Koshkin A, Vaishnav V. Ultrasound imaging facilitates spinal anesthesia in adults with difficult surface anatomic landmarks. Anesthesiology. 2011;115(1):94–101. doi:10.1097/ALN.0b013e31821a8ad4
14. Chen L, Huang J, Zhang Y, et al. Real-time ultrasound-guided versus ultrasound-assisted spinal anesthesia in elderly patients with hip fractures: a randomized controlled trial. Anesth Analg. 2022;134(2):400–409. doi:10.1213/ANE.0000000000005778
15. Fanelli G, Borghi B, Casati A, Bertini L, Montebugnoli M, Torri G. Unilateral bupivacaine spinal anesthesia for outpatient knee arthroscopy. Italian Study Group on Unilateral Spinal Anesthesia. Can J Anaesth. 2000;47(8):746–751. doi:10.1007/BF03019476
16. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
17. Mei Z, Ngan Kee WD, Sheng ZM, et al. Comparative dose-response study of hyperbaric ropivacaine for spinal anesthesia for cesarean delivery in singleton versus twin pregnancies. J Clin Anesth. 2020;67:110068. doi:10.1016/j.jclinane.2020.110068
18. Lv M, Zhang P, Wang Z. ED50 of intrathecal ropivacaine for cesarean delivery with and without epidural volume extension with normal saline: a randomized controlled study. J Pain Res. 2018;11:2791–2796. doi:10.2147/JPR.S174176
19. Chen M, Chen C, Ke Q. The effect of age on the median effective dose (ED50) of intrathecally administered plain bupivacaine for motor block. Anesth Analg. 2014;118(4):863–868. doi:10.1213/ANE.0000000000000147
20. Harten JM, Boyne I, Hannah P, Varveris D, Brown A. Effects of a height and weight adjusted dose of local anaesthetic for spinal anaesthesia for elective Caesarean section. Anaesthesia. 2005;60(4):348–353. doi:10.1111/j.1365-2044.2005.04113.x
21. Fu F, Xiao F, Chen W, et al. A randomised double-blind dose-response study of weight-adjusted infusions of norepinephrine for preventing hypotension during combined spinal-epidural anaesthesia for Caesarean delivery. Br J Anaesth. 2020;124(3):e108–e114. doi:10.1016/j.bja.2019.12.019
22. Wei CN, Zhang YF, Xia F, Wang LZ, Zhou QH. Abdominal girth, vertebral column length and spread of intrathecal hyperbaric bupivacaine in the term parturient. Int J Obstet Anesth. 2017;31:63–67. doi:10.1016/j.ijoa.2017.02.002
23. Hocking G, Wildsmith JA. Intrathecal drug spread. Br J Anaesth. 2004;93(4):568–578. doi:10.1093/bja/aeh204
24. Higuchi H, Hirata J, Adachi Y, Kazama T. Influence of lumbosacral cerebrospinal fluid density, velocity, and volume on extent and duration of plain bupivacaine spinal anesthesia. Anesthesiology. 2004;100(1):106–114. doi:10.1097/00000542-200401000-00019
25. Lilot M, Meuret P, Bouvet L, et al. Hypobaric spinal anesthesia with ropivacaine plus sufentanil for traumatic femoral neck surgery in the elderly: a dose-response study. Anesth Analg. 2013;117(1):259–264. doi:10.1213/ANE.0b013e31828f29f8
26. Finsterwald M, Muster M, Farshad M, Saporito A, Brada M, Aguirre JA. Spinal versus general anesthesia for lumbar spine surgery in high risk patients: perioperative hemodynamic stability, complications and costs. J Clin Anesth. 2018;46:3–7. doi:10.1016/j.jclinane.2018.01.004
27. Graves CL, Underwood PS, Klein RL, Kim YI. Intravenous fluid administration as therapy for hypotension secondary to spinal anesthesia. Anesth Analg. 1968;47(5):548–556. doi:10.1213/00000539-196809000-00018
28. Gonçalves TJM, Gonçalves SE, Nava N, et al. Perioperative immunonutrition in elderly patients undergoing total hip and knee arthroplasty: impact on postoperative outcomes. JPEN J Parenter Enteral Nutr. 2021;45(7):1559–1566. doi:10.1002/jpen.2028
29. Wang W, Li Y, Sun A, Yu H, Dong J, Xu H. Determination of the median effective dose (ED50) of bupivacaine and ropivacaine unilateral spinal anesthesia: prospective, double blinded, randomized dose-response trial. Anaesthesist. 2017;66(12):936–943. doi:10.1007/s00101-017-0370-9
30. Tang Z, Zhang C, Xu Z, Jin F, Liang D. Observation of single spinal anesthesia by 25G needle puncture through a lateral crypt for Hip surgery in elderly patients. Medicine. 2019;98(27):e16334. doi:10.1097/MD.0000000000016334
31. Uppal V, Retter S, Shanthanna H, Prabhakar C, McKeen DM. Hyperbaric versus isobaric bupivacaine for spinal anesthesia: systematic review and meta-analysis for adult patients undergoing noncesarean delivery surgery. Anesth Analg. 2017;125(5):1627–1637. doi:10.1213/ANE.0000000000002254
32. Cantürk M, Kılcı O, Ornek D, Ozdogan L, Pala Y, Sen O. Ropivacaine for unilateral spinal anesthesia; hyperbaric or hypobaric? Rev Bras Anestesiol. 2012;62(3):298–311. doi:10.1016/S0034-7094(12)70131-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low-Dose Morphine Intrathecal Analgesia in Elderly Patients with Hip Fracture Undergoing Single Spinal Anesthesia: A Randomized Controlled Trial
Buršík D, Romanová T, Lečbychová K, Bílená M, Burda M, Ševčík P, Haiduk F, Frelich M, Káňová M, Máca J
Local and Regional Anesthesia 2026, 19:598583
Published Date: 12 May 2026