Back to Journals » Journal of Pain Research » Volume 18
Dorsal Root Ganglion Pulsed Radiofrequency with Scar Radiofrequency Ablation Combined for Chronic Postoperative Abdominal Pain: A Retrospective Study
Authors Gu R ![]() , Huang Y, Li Y, Zhu T, Ma C, Tao G
, Huang Y, Li Y, Zhu T, Ma C, Tao G
Received 16 April 2025
Accepted for publication 28 July 2025
Published 7 August 2025 Volume 2025:18 Pages 3933—3942
DOI https://doi.org/10.2147/JPR.S532000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Ruxin Gu, Ying Huang, Yin Li, Tong Zhu, Chao Ma, Gaojian Tao
Department of Pain Medicine, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Gaojian Tao, Department of Pain Medicine, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210008, People’s Republic of China, Email [email protected]
Background: Chronic postoperative abdominal pain (CPAP) manifests as neuropathic or mixed pain, and conservative treatments often only provide temporary relief. This study evaluated the efficacy and safety of combining dorsal root ganglion pulsed radiofrequency (DRG-PRF) with scar radiofrequency ablation (RFA) for a better treatment.
Methods: A total of 48 CPAP patients were divided into the scar RFA group (RFA group, n = 25) and the combination of DRG-PRF and scar RFA group (RFA+PRF group, n = 23). The visual analogue scale (VAS) and Globe Pain Scale (GPS) questionnaires were used for pain intensity and its effects before and at intervals of 1, 7, 30, 90 and 180 days after the procedure.
Results: Baseline scores were comparable. The RFA+PRF group demonstrated significantly lower VAS scores at 1-day (1.2 ± 1.0 vs 1.6 ± 1.1, p = 0.040), 30-day (2.3 ± 1.1 vs 3.0 ± 0.9, p < 0.001), 90-day (2.7 ± 1.3 vs 3.7 ± 1.3, p < 0.001), 180-day of follow-up (2.7 ± 1.1 vs 3.5 ± 1.0, p = 0.002). GPS scores also showed significantly greater improvement in the RFA+PRF group at 30-day (51.2 ± 15.5 vs 62.2 ± 15.3, p = 0.028), 90-day (67.4 ± 16.3 vs 85.3 ± 14.7, p = 0.004), and 180-day (48.4 ± 13.3 vs 62.6 ± 10.9, p = 0.011) post-procedure. Additionally, a significantly higher proportion of patients in the RFA+PRF group achieved ≥ 50% pain relief at both 3 and 6 months (p < 0.05). No adverse reactions were observed in any participants.
Conclusion: The combination of DRG-PRF and scar RFA has demonstrated significant efficacy and high safety in the treatment of CPAP. Compared to scar RFA alone, the combined therapy provides more durable and significant long-term pain relief, making it a better choice for pain management in CPAP patients.
Keywords: chronic postoperative abdominal pain, dorsal root ganglion, pulsed radiofrequency
Introduction
Chronic post-surgical pain (CPSP) is a well-recognized complication of abdominal surgery, characterized by pain that develops or worsens in the surgical area and persists for more than three months after surgery, with other causes of pain excluded.1 Given the wide range of abdominal procedures performed, the incidence of chronic postoperative abdominal pain (CPAP) varies depending on the type of surgery. Previous studies have reported that CPAP occurs in up to 51.6% of patients following inguinal hernia repair,2 the prevalence of chronic pain after uterine and gastrointestinal surgeries ranges from 16.2% to 30.2% and 21.8% to 32.1%, respectively.3–5 The underlying mechanisms of CPAP, like other forms of CPSP, are not yet fully understood. However, contributing factors may include preoperative psychological conditions, surgical trauma, and perioperative pain management strategies. Neuropathic components are believed to play a critical role, potentially resulting from peripheral and central sensitization as well as direct nerve injury.6,7 Conventional treatments for CPAP include medication, physiotherapy, nerve blocks and surgical interventions. However, these approaches have limitations such as medication side effects,8 limited efficacy, short-lived effects,9 and great surgical trauma.10 As a result, many patients experience persistent functional impairment, psychological distress, and reduced overall quality of life.11
Radiofrequency-based interventions, including pulsed radiofrequency (PRF) and radiofrequency ablation (RFA), have emerged as effective minimally invasive techniques for managing chronic pain. These modalities have demonstrated long-term pain relief, reduced reliance on analgesics, and improved quality of life in patients with refractory chronic abdominal pain.12 PRF is believed to modulate neuronal excitability and inhibit pain signal transmission,13 whereas RFA directly ablates nerve endings within post-surgical scar tissue, alleviating pain by reducing nerve compression.14
From a pathophysiological perspective, the combination of dorsal root ganglion pulsed radiofrequency (DRG-PRF) and scar RFA may provide improved pain relief by simultaneously addressing neuropathic and mechanical components of CPAP. Notably, clinical evidence supporting the effectiveness of this synergistic approach in managing CPAP is still lacking. Therefore, this study aims aimed to evaluate the efficacy of scar RFA combined with dorsal root ganglion (DRG) PRF in the management of CPAP.
Materials and Methods
Patients
This retrospective study analyzed data from patients who underwent radiofrequency treatment for CPAP at the Pain Management Department of Nanjing Drum Tower Hospital between June 2020 and June 2024. All patients had previously undergone abdominal wall incision or hernia repair surgery, and met the diagnostic criteria of CPAP.1 The inclusion criteria were as follows: age of 18 years or older; visual analogue scale (VAS) score at least 3 (out of a maximum 10) persisting for more than three months; CPAP unresponsive to conservative treatment for at least one month or associated with intolerable side effects; undergoing scar RFA with or without DRG-PRF. Exclusion criteria were as follows: incomplete medical records or follow-up data; presence of other conditions causing abdominal pain, such as chronic gastritis, irritable bowel syndrome, etc.; severe bleeding disorders, coagulation dysfunction, or local skin infection at the surgical site; intellectual disabilities, communication disorders or poor cooperation; previous treatment involving visceral nerve destruction. A total of 48 patients were finally included and informed consent was obtained from all participants. The study complied with the principles outlined in the Declaration of Helsinki and was approved by the Medical Ethics Committee of Nanjing Drum Tower Hospital (No. 2024–515-01).
Techniques
Patients were divided into two groups which were the scar RFA group (RFA group) and the combination of DRG-PRF and scar RFA group (RFA+PRF group), all procedures were performed under standard monitoring and strict sterile technique.
The scar RFA operation process was as follows. The patients were placed on the operating table in a supine position. Following the delineation of the scar boundaries, the puncture site and needle trajectory were determined using the central portion of the scar as the anatomical reference. Local anesthesia was administered using 1 mL of 1% lidocaine. Under high-frequency ultrasound guidance, a 22-gauge radiofrequency cannula with a 10-mm active tip (Boston Scientific) was advanced into the core region of the scar tissue. Sensory stimulation was applied at 50 Hz and 0.4 V to confirm correct placement. The treatment was conducted at electrode tip temperatures of 60°C, 70°C, and 80°C, with each cycle lasting 60 seconds, repeated for three cycles. The electrode was repositioned at different angles to ensure complete coverage of the scar and its surrounding area within the high-echo vaporization zone.
For patients in the RFA+PRF group, PRF was performed immediately after scar RFA. The patient was repositioned to a prone position. With unenhanced thin-layer CT scan was used to identify the target DRG based on the primary pain region. A straight 22-gauge radiofrequency cannula with a 10-mm active tip was inserted at the target DRG (Figure 1). Sensory stimulation at 50 Hz and 0.4 V was used to confirm proper placement, followed by PRF treatment at 42°C for 5 minutes.
 |
Figure 1 Representative CT-guided images of positioning and placement during pulsed radiofrequency (PRF) treatment. (A) CT images of positioning before treatment. (B) CT images of placement during treatment. |
Questionnaires
The VAS (0–10, with 0 indicating no pain and 10 indicating the most severe pain) and Globe Pain Scale (GPS, 0–200, with higher scores indicating more severe pain effects) were used to provide a comprehensive and integrated assessment of the pain. In our study, the VAS and GPS were assessed at baseline (pre-treatment) and at 1, 7, 30, 90 and 180 days post-treatment. The number of patients with 50% pain reduction were evaluated after treatment. Additional data on rescue pain medication and complications were also collected and analyzed.
Statistics
The Kolmogorov–Smirnov test was used to assess the normality of data distribution. Categorical data were compared using the chi-square test or Fisher exact test. Continuous data between groups were analyzed using either an unpaired t-test or the Mann–Whitney U-test, depending on data distribution. Generalized estimating equation (GEE) was used to evaluate differences in VAS and GPS scores between groups over time. All statistical analyses were performed using SPSS software (version 26.0, SPSS Inc., Chicago, IL). p <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 48 patients with CPAP were included in the study, with 25 patients in the RFA group and 23 in the RFA+PRF group (Figure 2). Patient characteristics were shown on Table 1. The mean age was 64.6 ± 7.2 years in the RFA group and 65.3 ± 6.9 years in the RFA+PRF group. Half of the patients were female. Approximately 2/3 patients suffered from moderate pain, with hernia surgery being the most common cause.
 |
Table 1 Demographic and Clinical Characteristics Data |
 |
Figure 2 Flow diagram for the study. |
There were no statistically significant differences between the two groups in terms of demographic and clinical characteristics. Additionally, no significant difference was observed in the type of rescue pain medication used between the groups. No adverse events, such as limb numbness, muscle weakness, hematoma, or neurological complications, were reported during the study.
Pain Assessment
Before treatment, the mean VAS scores were 6.1 ± 1.5 in the RFA group and 6.0 ± 1.5 in the RFA+PRF group, while the mean GPS scores were 136.8 ± 25.4 in the RFA group and 136.0 ± 29.9 in the RFA + PRF group, respectively. No significant differences were observed between the two groups at baseline. However, the VAS scores were significantly lower in the RFA+PRF group compared to the RFA group at multiple time points: 1-day (1.2 ± 1.0 vs 1.6 ± 1.1, p = 0.040), 30-day (2.3 ± 1.1 vs 3.0 ± 0.9, p < 0.001), 90-day (2.7 ± 1.3 vs 3.7 ± 1.3, p < 0.001), 180-day of follow-up (2.7 ± 1.1 vs 3.5 ± 1.0, p = 0.002) (Table 2 and Figure 3).
 |
Table 2 Comparison of VAS Scores Between Groups |
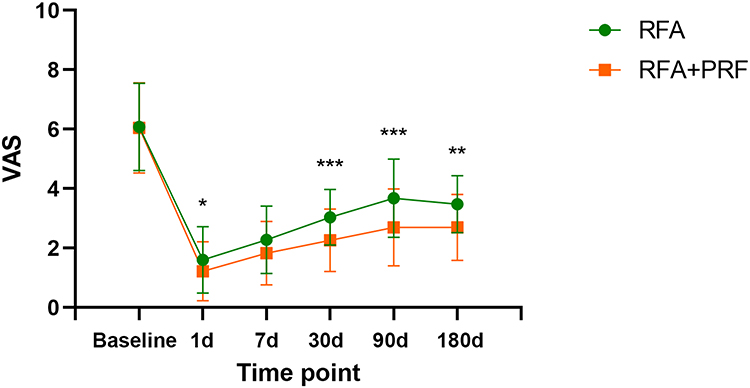 |
Figure 3 Evaluation of pain relief through VAS scores between groups. Statistical analysis using Generalized Estimating Equation (GEE). *The mean differences at 1-, 30-, 90- and 180-day after adjusting the baseline score were 0.4 (95% CI 0.0−0.7; p = 0.040), 0.8 (95% CI 0.4−1.1; p < 0.001), 0.9 (95% CI 0.5−1.4; p < 0.001) and 0.8 (95% CI 0.3−1.2; p = 0.002), respectively (*p < 0.05, **p < 0.01, ***p < 0.001). |
The GPS scores also demonstrated significantly greater improvement in the RFA+PRF group at the 30-day (51.2 ± 15.5 vs 62.2 ± 15.3, p = 0.028), 90-day (67.4 ± 16.3 vs 85.3 ± 14.7, p = 0.004), and 180-day (48.4 ± 13.3 vs 62.6 ± 10.9, p = 0.011) post-procedure compared to the RFA group (Table 3 and Figure 4). Furthermore, The GPS scale includes four components: pain, feelings, clinical outcomes and daily activities. Notably, with the exception of clinical outcomes, all other components demonstrated significant differences between the two groups at the 30-day, 90-day and 180-day postoperative follow-up (Table 4 and Figure 5).
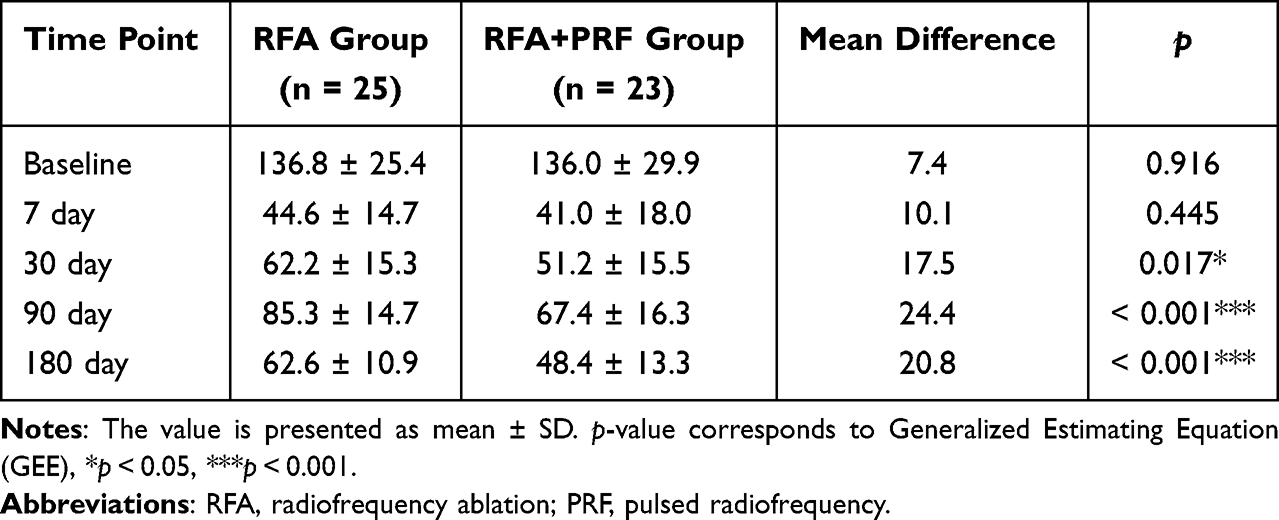 |
Table 3 Comparison of Global Pain Scale (GPS) Scores Between Groups |
 |
Table 4 Comparison of Each Part Scores of Global Pain Scale (GPS) |
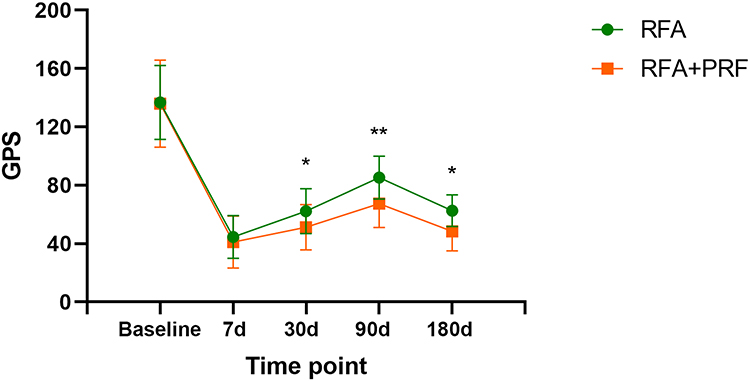 |
Figure 4 Comprehensive assessment of pain relief using Global Pain Scale (GPS) scores between groups. Statistical analysis using Generalized Estimating Equation (GEE). *The mean differences at 30-, 90- and 180-day after adjusting the baseline score were 17.5 (95% CI 1.9−33.1; p = 0.028), 24.4 (95% CI 8.0−40.8; p = 0.004) and 20.8 (95% CI 4.8−36.7; p = 0.011), respectively (*p < 0.05, **p < 0.01). |
 |
Figure 5 The graph showed each part scores of Global Pain Scale (GPS) between the study groups. Statistical analysis using Generalized Estimating Equation (GEE). (A) Evaluation of improvements in pain intensity. *The mean differences at 30-, 90- and 180-day after adjusting the baseline score were 2.6 (95% CI 0.5–4.8; p = 0.015), 4.2 (95% CI 2.3–6.2; p < 0.001) and 3.7 (95% CI 1.5–6.0; p = 0.001), respectively. (B) Evaluation of improvements in feelings. *The mean differences at 90- and 180-day after adjusting the baseline score were 5.0 (95% CI 2.5–7.5; p < 0.001) and 4.2 (95% CI 2.0–6.3; p < 0.001), respectively. (C) Evaluation of improvements in clinical outcomes. (D) Evaluation of improvements in daily activities. *The mean differences at 7-, 30-, 90- and 180-day after adjusting the baseline score were 1.9 (95% CI 0.0–3.9; p = 0.048), 2.3 (95% CI 0.2–4.4; p = 0.033), 5.2 (95% CI 3.0–7.4; p < 0.001) and 3.3 (95% CI 1.1–5.4; p = 0.003), respectively. (*p < 0.05, **p < 0.01, ***p < 0.001). |
Additionally, the proportion of patients achieving at least 50% pain relief was significantly higher in the RFA+PRF group than in the RFA group at both 3 months (69.6% vs 40.0%, p = 0.038) and 6 months (56.5% vs 24.0%, p = 0.020) post-procedure (Table 5).
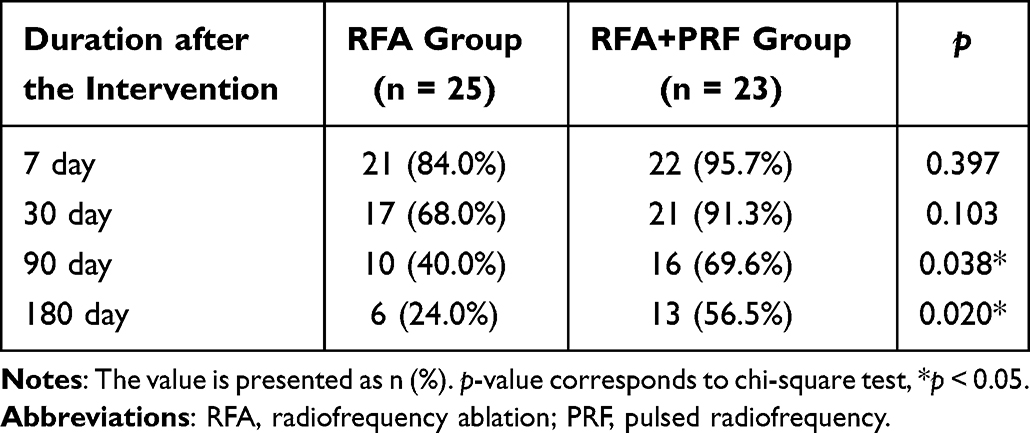 |
Table 5 Comparison of the Number of Patients with 50% Pain Reduction |
Discussion
CPAP is recognized as neuropathic or mixed pain associated with the surgical area, often manifesting as stabbing, lancinating, or burning sensations, which may be accompanied by symptoms such as numbness, swelling, or tenderness.4,15 Currently, there are no definitive preventive measures for CPAP. In addition to surgical factors, its development is linked to postoperative nerve damage, tissue inflammation and adhesion, postoperative analgesia, and preexisting conditions such as psychosocial factors and preoperative pain.6,12 Among these, preoperative pain is a major risk factor for CPAP and is commonly observed in patients undergoing hernia and gastrointestinal surgeries. Persistent pain can induce neuroplastic changes, increasing nerve sensitivity to pain, while intraoperative nerve damage may further contribute to its progression into chronic pain.3,5,16
Nerve damage plays a crucial role in the development of chronic pain, not only as a direct consequence of surgery but also as a result of excessive fibrosis and scar formation at the incision site. Studies have shown a strong correlation between scar size and the possibility of developing CPSP.17 In post-inguinal hernia surgery, pain is attributed to nerve compression by surgical meshes and scars, leading to the formation of neuromas and subsequently neuropathic pain, which is a key underlying mechanism of CPAP.2
CPAP significantly affects patients’ daily life and work activities, often leading to psychological distress and imposing a considerable economic burden.15 Traditional pharmacological treatments generally provide limited and temporary relief, while nerve blocks, although effective, offer only short-term pain reduction. When conservative treatments fail to alleviate patients’ pain, more invasive therapies such as radiofrequency-based interventions have been increasingly explored and applied. Alaa A et al retrospectively analyzed 30 patients with CPAP who underwent transversus abdominis plane nerve block therapy and reported an average pain relief duration of 84 days.18 In contrast, a retrospective study by Kastler et al on chronic inguinal neuralgia found that local nerve blocks only provided symptom relief for an average of 1.6 months, whereas radiofrequency treatment extended this relief to 12.5 months, indicating its significant longer-lasting efficacy.19
Our study demonstrated that combining DRG-PRF with scar RFA provided superior and sustained pain control compared to scar RFA alone in patients with CPAP. This synergistic effect manifested not only in accelerated pain intensity reduction (Table 2 and Figure 3), but also in multifaceted functional recovery, as shown by improvements in pain, feelings, and daily activities lasting through 6-month follow-up (Table 4 and Figure 5). Importantly, the combined therapy doubled the chances of achieving clinically significant pain relief (≥50% reduction) at both the 3-month (69.6% vs 40.0%) and 6-month endpoints (56.5% vs 24.0%), demonstrating its clear therapeutic advantage over standard ablation techniques.
RFA achieves analgesia by releasing radiofrequency energy within scar tissue, generating high temperatures, and precisely destroying pain nerve endings that may have formed within the scar tissue after surgery.20 In contrast, PRF is a neuromodulatory technique that causes minimal damage to nerve tissue. By releasing pulsed electric currents near the target nerves, PRF modulates sensory nerve ion channels, disrupting pain signal transmission and providing pain relief.21 A study comparing the efficacy of pharmacological treatment, DRG-PRF, and intercostal nerve PRF for post-thoracotomy pain syndrome found that that DRG-PRF was superior to the other two treatments in terms of both pain relief rate and duration.22 These results are similar to those reported by Huang et al in a study on postherpetic neuralgia.23 Unlike thermal RFA, PRF modulates the electrophysiological activity of nerve fibers without causing direct nerve destruction, reducing the risk of complications such as neuritis, paresthesia, and motor dysfunction.13
In this study, pain relief was achieved in both treatment groups, but the combined therapy doubled the chances of achieving clinically significant pain relief (≥50% reduction) at both the 3-month (69.6% vs 40.0%) and 6-month endpoints (56.5% vs 24.0%), demonstrating its clear advantages in terms of long-term pain symptom relief. Clinically, there are three possible mechanisms that could explain the observed advantages. (1) Scar RFA disrupts nerve endings within scar tissue, reducing pain signal transmission and alleviating nerve compression. Meanwhile, DRG-PRF modulates the excitability of spinal nerves, further decreasing pain perception. The combined application of these two techniques achieves multi-target and multi-level intervention in pain treatment, prolonging the analgesic effect. (2) Multiple studies have shown that PRF can modulate glial cells in the spinal dorsal horn, reducing local neuroinflammatory responses and inhibiting central sensitization.24–26 This suppresses the production and release of inflammatory mediators and pain-inducing substances, contributing to long-term pain relief. (3) The principle of neuro-radiofrequency thermocoagulation is to destroy specific nerve fibers, especially the unmyelinated fine fibers that transmit pain. Exposure to high temperatures induces fiber degeneration, blocking pain signal transmission to the brain. However, nerves often have a certain degree of self-repair capability, pain may return over time, the long-term effectiveness of peripheral nerve RFA alone may be limited.
During data collection, one case of inguinal pain associated with prostatitis was misdiagnosed (excluded from the analysis), which alerts us to the possibility that some refractory CPAP cases may involve undetected visceral-somatic pain.27 To ensure specificity of treatment outcomes, our study implemented rigorous exclusion criteria for visceral comorbidities (chronic gastritis, irritable bowel syndrome, prostatitis, etc). Patients receiving visceral nerve modulation therapy were excluded to isolate the effects of combined DRG-PRF and scar RFA on abdominal wall neuropathology. This approach ensures that the observed treatment effects directly reflect targeted interventions for abdominal wall neuropathology rather than unrelated pain sources. Clinically, these findings underscore the importance of multidisciplinary collaboration to confirm the etiology of pain before initiating invasive procedures like radiofrequency treatment.
Importantly, no adverse reactions were observed in any participants. The safety of combination therapy further enhances its clinical benefits. Unlike neurectomy, which carries risks such as permanent hypoesthesia or motor deficits.10 Both radiofrequency methods are minimally invasive and can be precisely guided by imaging to minimize damage to surrounding tissues, ensuring a high safety profile and strong reliability for repeated procedures.
Several limitations should be considered in order to better evaluate our findings. First, the main limitation of our study was the retrospective nature and the patients were not randomized. Second, the study was conducted in a single medical center, the sample size was relatively small and the follow-up period was short, which may affect the generalizability of this study. Third, there are slight differences in techniques and performed procedures among different physicians. Finally, there are multiple etiologies for CPAP besides common neuropathic pain, such as myofascial pain and phantom pain. However, these different etiological types were not differentiated, and CPAP was directly treated uniformly as neuropathic pain, which may affect the reliability and accuracy of the results. Further large-sample randomized studies are required to confirm our results and identify the best candidates for PRF procedures.
Conclusion
The combination of DRG-PRF and scar RFA has demonstrated significant efficacy and high safety in the treatment of CPAP. Compared to scar RFA alone, the combined therapy provides more durable and significant long-term pain relief, making it a better choice for pain management in CPAP patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Jiangsu Province, China (BK20241718).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schug SA, Lavand’homme P, Barke A, et al. The IASP classification of chronic pain for ICD-11: chronic postsurgical or posttraumatic pain. Pain. 2019;160(1):45–52. doi:10.1097/j.pain.0000000000001413
2. Nikkolo C, Lepner U. Chronic pain after open inguinal hernia repair. Postgrad Med. 2016;128(1):69–75. doi:10.1080/00325481.2016.1121090
3. Grundström H, Fredrikson M, Alehagen S, et al. Incidence of self-reported pelvic pain and risk factors for pain 1 year after benign hysterectomy: a register study from the Swedish National Quality Registry for Gynecological Surgery. Acta Obstet Gynecol Scand. 2023;102(10):1359–1370. doi:10.1111/aogs.14455
4. Martinez V, Lehman T, Lavand’homme P, et al. Chronic postsurgical pain: a European survey. Eur J Anaesthesiol. 2024;41(5):351–362. doi:10.1097/EJA.0000000000001974
5. Jin J, Chen Q, Min S, et al. Prevalence and predictors of chronic postsurgical pain after colorectal surgery: a prospective study. Colorectal Dis. 2021;23(7):1878–1889. doi:10.1111/codi.15640
6. Thapa P, Euasobhon P. Chronic postsurgical pain: current evidence for prevention and management. Korean J Pain. 2018;31(3):155–173. doi:10.3344/kjp.2018.31.3.155
7. Gold MS, Gebhart GF. Nociceptor sensitization in pain pathogenesis. Nat Med. 2010;16(11):1248–1257. doi:10.1038/nm.2235
8. Vetter TR, Kain ZN. Role of the perioperative surgical home in optimizing the perioperative use of opioids. Anesth Analg. 2017;125(5):1653–1657. doi:10.1213/ANE.0000000000002280
9. Sahoo RK, Pradhan A, Samanta P, et al. Effect of ultrasound-guided ilioinguinal-iliohypogastric nerve block on chronic pain in patients undergoing open inguinal hernia surgery under spinal anesthesia: a randomized double-blind study. Korean J Pain. 2024;37(4):332–342. doi:10.3344/kjp.24172
10. Moore AM, Bjurstrom MF, Hiatt JR, et al. Efficacy of retroperitoneal triple neurectomy for refractory neuropathic inguinodynia. Am J Surg. 2016;212(6):1126–1132. doi:10.1016/j.amjsurg.2016.09.012
11. Fletcher D, Stamer UM, Pogatzki-Zahn E, et al. Chronic postsurgical pain in Europe: an observational study. Eur J Anaesthesiol. 2015;32(10):725–734. doi:10.1097/EJA.0000000000000319
12. Vachirakorntong B, Kawana E, Zhitny VP, et al. Radiofrequency Ablation’s effectiveness for treating abdominal and thoracic chronic pain syndromes: a systematic review of the current literature. Pain Physician. 2023;26(7):E737–e759. doi:10.36076/ppj.2023.26.E737
13. Sinha P, Sarkar B, Goswami S, et al. Effectiveness of combination of ultrasonography-guided pulsed radiofrequency neuromodulation with steroid at the suprascapular nerve in chronic shoulder pain. Pain Pract. 2020;20(1):16–23. doi:10.1111/papr.12820
14. Vatansever D, Tekin I, Tuglu I, et al. A comparison of the neuroablative effects of conventional and pulsed radiofrequency techniques. Clin J Pain. 2008;24(8):717–724. doi:10.1097/AJP.0b013e318173c27a
15. Sellam S, Nguyen AT, Pogu M, et al. Transversus abdominis plane block in the treatment of chronic postsurgical abdominal wall pain improves patient quality of life: a retrospective study and literature review. Pain Physician. 2023;26(2):E91–e100. doi:10.36076/ppj.2023.26.E91
16. Fregoso G, Wang A, Tseng K, et al. Transition from acute to chronic pain: evaluating risk for chronic postsurgical pain. Pain Physician. 2019;22(5):479–488.
17. Palabiyik O, Demir G. Chronic pain after open appendectomy and its effects on quality of life in children aged 8–18 years. Pain Res Manag. 2021;2021:6643714. doi:10.1155/2021/6643714
18. Abd-Elsayed A, Malyuk D. Efficacy of transversus abdominis plane steroid injection for treating chronic abdominal pain. Pain Pract. 2018;18(1):48–52. doi:10.1111/papr.12580
19. Kastler A, Aubry S, Piccand V, et al. Radiofrequency neurolysis versus local nerve infiltration in 42 patients with refractory chronic inguinal neuralgia. Pain Physician. 2012;15(3):237–244. doi:10.36076/ppj.2012/15/237
20. Tun K, Cemil B, Gurcay AG, et al. Ultrastructural evaluation of pulsed radiofrequency and conventional radiofrequency lesions in rat sciatic nerve. Surg Neurol. 2009;72(5):496–500;discussion501. doi:10.1016/j.surneu.2008.11.016
21. Usmani H, Dureja GP, Andleeb R, et al. Conventional radiofrequency thermocoagulation vs pulsed radiofrequency neuromodulation of ganglion impar in chronic perineal pain of nononcological origin. Pain Med. 2018;19(12):2348–2356. doi:10.1093/pm/pnx244
22. Cohen SP, Sireci A, Wu CL, et al. Pulsed radiofrequency of the dorsal root ganglia is superior to pharmacotherapy or pulsed radiofrequency of the intercostal nerves in the treatment of chronic postsurgical thoracic pain. Pain Physician. 2006;9(3):227–235.
23. Huang X, Ma Y, Wang W, et al. Efficacy and safety of pulsed radiofrequency modulation of thoracic dorsal root ganglion or intercostal nerve on postherpetic neuralgia in aged patients: a retrospective study. BMC Neurol. 2021;21(1):233. doi:10.1186/s12883-021-02286-6
24. Vallejo R, Tilley DM, Williams J, et al. Pulsed radiofrequency modulates pain regulatory gene expression along the nociceptive pathway. Pain Physician. 2013;16(5):E601–13. doi:10.36076/ppj.2013/16/E601
25. Lin ML, Lin W-T, Huang R-Y, et al. Pulsed radiofrequency inhibited activation of spinal mitogen-activated protein kinases and ameliorated early neuropathic pain in rats. Eur J Pain. 2014;18(5):659–670. doi:10.1002/j.1532-2149.2013.00419.x
26. Xu X, Fu S, Shi X, et al. Microglial BDNF, PI3K, and p-ERK in the spinal cord are suppressed by pulsed radiofrequency on dorsal root ganglion to ease SNI-induced neuropathic pain in rats. Pain Res Manag. 2019;2019:5948686. doi:10.1155/2019/5948686
27. Shian B, Larson ST. Abdominal wall pain: clinical evaluation, differential diagnosis, and treatment. Am Fam Physician. 2018;98(7):429–436.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of a Novel Ultrasound-Guided C8 Dorsal Root Ganglion Puncture Approach and Radiofrequency Treatment for Postherpetic Neuralgia
Yang L, Yang J, Zhang S, Lu G, Fang W, Bao Y, Meng C, Xiang Y
Journal of Pain Research 2026, 19:616718
Published Date: 10 July 2026