Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Does Women’s Autonomy Matter on Attitude Towards Condom Use in Reducing Risk for HIV Infection Among Married Women in Ethiopia?
Received 2 September 2020
Accepted for publication 18 September 2020
Published 30 September 2020 Volume 2020:12 Pages 489—496
DOI https://doi.org/10.2147/HIV.S279609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Mohammed Ahmed,1 Abdu Seid2
1Department of Public Health, College of Health Science, Woldia University, Woldia, Ethiopia; 2Department of Midwifery, College of Health Science, Woldia University, Woldia, Ethiopia
Correspondence: Mohammed Ahmed Email [email protected]
Background: Condom utilization remains as the forefront guard to reduce the HIV/AIDS pandemic. However, evidence showed that the dynamics of gendered power, beliefs, and attitudes about condoms and sexuality retards condom use for a large proportion of Africa’s people. Therefore, this study aimed to assess the association between women’s autonomy in health decision making and attitude to condom use in reducing risk for HIV in Ethiopia using a nationally representative, population-based household survey data.
Methods: A cross-sectional study was carried out using 2016 nationally representative, population-based Ethiopia Demographic and Health Survey. SPSS version 21 was used to analyze the data. Multivariate logistic regression analysis was performed to assess the association between women’s autonomy in health decision making and attitude to condom use by controlling confounders. To declare statistically significant associations, adjusted odds ratios (AOR) with 95% confidence interval (CI) were used.
Results: The present study enrolled 6787 weighted samples of married women. The study showed that the odds of attitude toward condom use were 1.39 times (AOR: 1.39; 95% CI: 1.04– 1.85) higher among women who decide for their health care compared to its counterparts. Also, the odds of attitude toward condom use were positively associated among women who conquered higher education (AOR: 1.97; 95% CI: 1.17– 3.33), who had the richest wealth index quintile (AOR: 1.45; 95% CI: 1.01– 2.07), and who had ever been tested for HIV (AOR: 1.31; 95% CI: 1.09– 1.57). However, the odds of attitudes toward condom use were negatively associated among Muslims (AOR: 0.58; 95% CI: 0.46– 0.74) and Protestant religion (AOR: 0.69; 95% CI: 0.54– 0.88) followers.
Conclusion: The study culminates that women’s autonomy in health decision making improves attitudes toward condom use during sex for HIV prevention in Ethiopia. Besides, women’s higher education gets better wealth index, and HIV testing perks up the attitudes toward condom use; but religious affiliation deters it. Therefore, efforts need to be done in promoting women’s autonomy along with empowering women in education, economic as well as HIV detection. Furthermore, designing interventions that address primary prevention strategies like using condoms consistently along with addressing religious affiliation can have a significant effect on curtailing HIV/AIDS scourge.
Keywords: women, autonomy, attitude, condom, HIV, Ethiopia
Background
HIV and violence against women are recorded as twin epidemics that excessively affect women.1 Globally, in 2016, 51% of women were living with HIV.2 Contrasted to men, women living in Sub- Saharan Africa (SSA) are more affected by HIV, accounting for 59% of all infections in this region.3 In Ethiopia, in 2016, about 385,642 of females were infected with HIV compared to 285,263 of males.4 Besides, HIV prevalence varies notably by marital status and is 0.8% higher among women who report ever having been married compared with those who have never married (0.3%).5
The differences in the circulation of risk factors among women and men are attributable to the gender inequalities in HIV/AIDS. For example, in SSA, the risk of HIV infection is mainly due to the lower socioeconomic position of women.6–8 Besides economic differences, uneven power affiliations and the subordinate position of women relative to men also place women at higher risk for acquiring HIV.9,10 Currently, scholars have identified factors such as androcentricity and patriarchy as traditions that expose women to violence, exploitation, and exacerbate the spread of HIV.11
Women’s autonomy is defined as the ability the women to obtain information and make decisions about one’s concerns and is also a basis of reproductive rights.12
The link between women’s autonomy and HIV has been studied in different countries including in Northern Vietnam,13 India,14,15 Kenya,16 Nigeria,17 Malawi,18 Nepal,19 and South Africa.20 Besides, women’s autonomy has been positively associated with improved reproductive health, economic well-being, freedom from violence, and reduces women’s vulnerability to HIV/AIDS.14,19,21–27
Understanding the interconnection between women’s autonomy and HIV may explain why HIV prevalence is highest in particular cultures compared to others.20
To lessen the extent of HIV in SSA and other places, macro-level interventions through educational campaigns,28,29 and individual micro strategies that promote condom use30,31 were often applied since condom utilization remains as the forefront guard to reduce the HIV/AIDS pandemic.32 However, evidence showed that the dynamics of gendered power, beliefs, and attitudes about HIV, condoms, and sexuality retards condom use for a large proportion of Africa’s people.33–36
Also, women’s preferences, differences in sexual relationship power, and perceived exclusivity of the relationship with their sexual partners affect condom utilization.37,38 This underscores the call for a gender-specific analysis of the determinants of condom use that may be more suitable in a situation of gender power imbalance.39 There is an escalating recognition that tackling HIV must address gender inequalities.40 Besides, country-specific interventions are needed in Ethiopia since gender inequality in HIV/AIDS in SSA varies by country.41 Unfortunately, research assessing the association between women’s health decision making autonomy and attitude to condom use in reducing risk for HIV in Ethiopia has lagged. Therefore, the current study endeavors to bridge this gap by using the recent Ethiopian demographic and health survey data set.
Methods
Data Source
The current study utilized the recent 2016 Ethiopia Demographic and Health Surveys (EDHS) data set. A two-stage stratified cluster sampling method was used. A detailed description of the study design and methodology of the survey were founded elsewhere.42 About 15,683 women (15–49 years) were interviewed in the 2016 EDHS, making up response rates of 95%. The analytic sample in this study included 6787 women currently married or in a relationship or living together between the ages of 15 and 49 years.
Study Variables
The main outcome variable of interest was the attitude to condom use for reducing risk for HIV/AIDS, which was measured by their response to the question of whether always using condoms during sex reduces their chance of getting AIDS. This variable had two responses either yes or no.
The main predictor variable was women’s autonomy over health care decision, which is an area that has received attention by researchers due to its growing importance from both a human rights and healthcare outcomes perspectives.43 This variable was obtained from the demographic and health survey variable “person who usually decides on the respondent’s health care (women)”. This variable had five responses: the respondent herself, the respondent, and her husband/partner, the husband/partner alone, someone else, and others. This variable was coded 1 (has autonomy over decision-making for her health), 2(a joint decision with her husband/partner), and 0 (does not have autonomy over decision-making for her health). Variables such as the age of the respondents, education status, type of residence, occupation, wealth index, access to media, and ever been tested for HIV were selected as covariates that affect attitude to condom use.
Statistical Analysis
SPSS version 21 was used to analyze the data. Frequencies and weighted percentages of study variables were reported. Bivariate analysis using Rao–Scott chi-square test was performed to examine the relationship between attitude to condom use and each of the independent variables and to select potential candidates for the multivariate model. A variable, which had a p-value of < 0.25 in bivariate analysis were entered into a multivariate binary logistic regression analysis to assess the association between women autonomy in health decision making and attitude to condom use by controlling confounders. To declare a statistically significant association, adjusted odds ratios (AOR) with 95% confidence interval (CI) were used. As recommended for complex survey design, sampling weights were applied for this study by dividing the individual women sample weight by 1000,000.
Ethics Approval and Consent to Participate
Since it is secondary data analysis from the 2016 EDHS database, ethical clearance for the study is not required. The researchers of this study have maintained the confidentiality of the data after received from the USAID–DHS program. Before the study commencement, the consent was obtained from the study participants.
Results
Descriptive Statistics of the Study Participants
About 6787 weighted samples were enrolled and analyzed. The majority age group was 20–29 years (42.4%), and the majority of the women resided in rural areas (79.9%). Most of the women did not attained education (53%), were unemployed (50.6%), and were from a middle wealth index category (19.8%). Only,15.5%, 10.7%, 17.9%, and 7.1% of women make decisions about their health care, on large household purchases, on visits to family or relatives, and what to do with money husband earns. Furthermore, 74.4% of the women responded that always using condoms during sex reduces their chance of getting AIDS (Table 1).
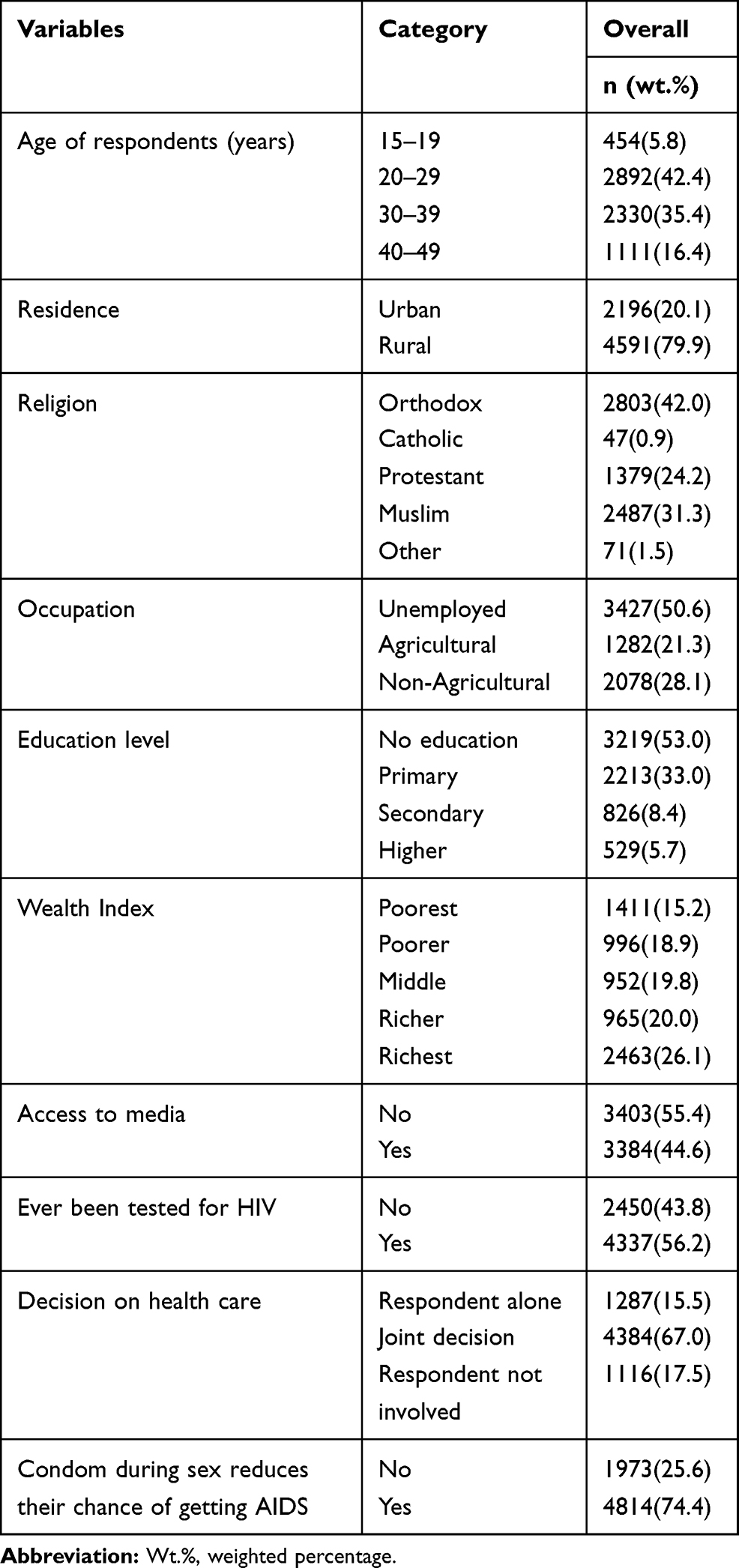 |
Table 1 Descriptive Statistics of the Sampled Women with the Study Variables in Ethiopia (N= 6787) |
Bivariate Analysis of Associations Between the Explanatory Variables and Attitude to Condom Use
In the bivariate analysis using Rao- Scott adjusted chi-square, attitude towards condom use is associated with residence, occupation, educational level, religion, wealth index, and women’s autonomy on health care decision at a p-value of < 0.001. Also, the age of the respondents was associated with the attitude towards using a condom during sex would reduce their chances of getting AIDS at p-value < 0.25 (Table 2).
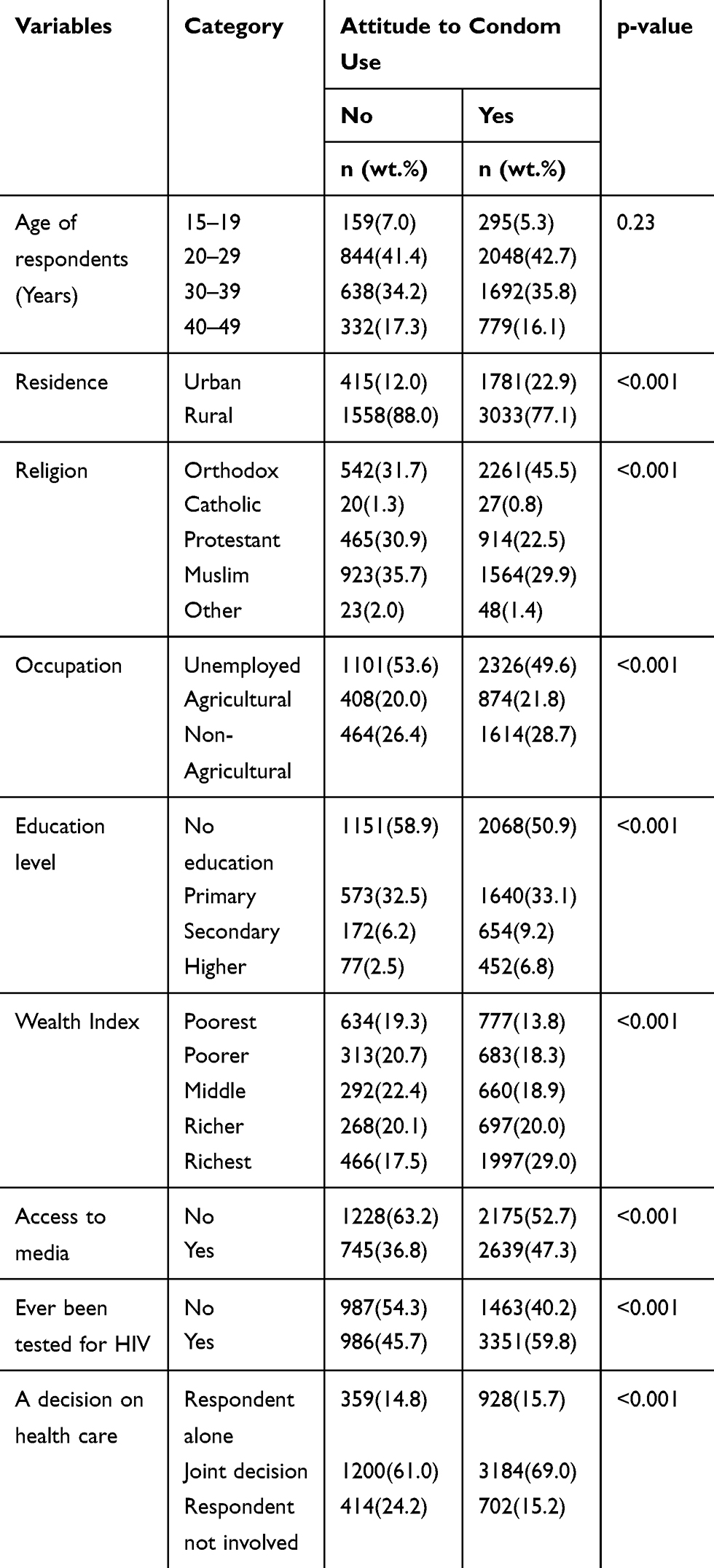 |
Table 2 Bivariate Analysis on Associations Between Outcome Variable, Attitudes Toward Condom Use, and Sociodemographic and Autonomy Indicators (n=6787) |
Multivariate Analysis Using Logistic Regression to Identify Predictors of Attitudes Towards Condom Use
All the variables were entered into multivariate logistic regression analysis since all the variables had a p-value of <0.25 in bivariate analysis. In the multivariate analysis, women’s her own decision on health care, religion, educational level, wealth index, and HIV testing was significantly associated with the attitudes towards always using a condom during sex would reduce the risk of HIV/AIDS. In this study, the odds of attitudes towards condom use were 1.39 times (AOR: 1.39; 95% CI: 1.04–1.85) higher among women who decide for their health care compared to its counterparts. The joint decision of the women for health care increased the odds of attitudes toward condom use by 1.59 times (AOR: 1.59; 95% CI: 1.25–2.02).
Regarding religion, Muslim and Protestant religion followers had lower odds of attitudes toward condom use by 42% (AOR: 0.58; 95% CI: 0.46–0.74), and 31% (AOR: 0.69; 95% CI: 0.54–0.88), respectively. Furthermore, attitudes towards condom use were 1.97 times (AOR: 1.97; 95% CI: 1.17–3.33) higher among women attained higher education. Besides, women in the richest wealth index quintile compared to the poorest increased the odds of attitudes toward condom use by 55% (AOR: 1.45; 95% CI: 1.01–2.07). Besides, women who ever tested for HIV were increased the odds of attitudes toward condom use by 1.31 times (AOR: 1.31; 95% CI: 1.09–1.57) (Table 3).
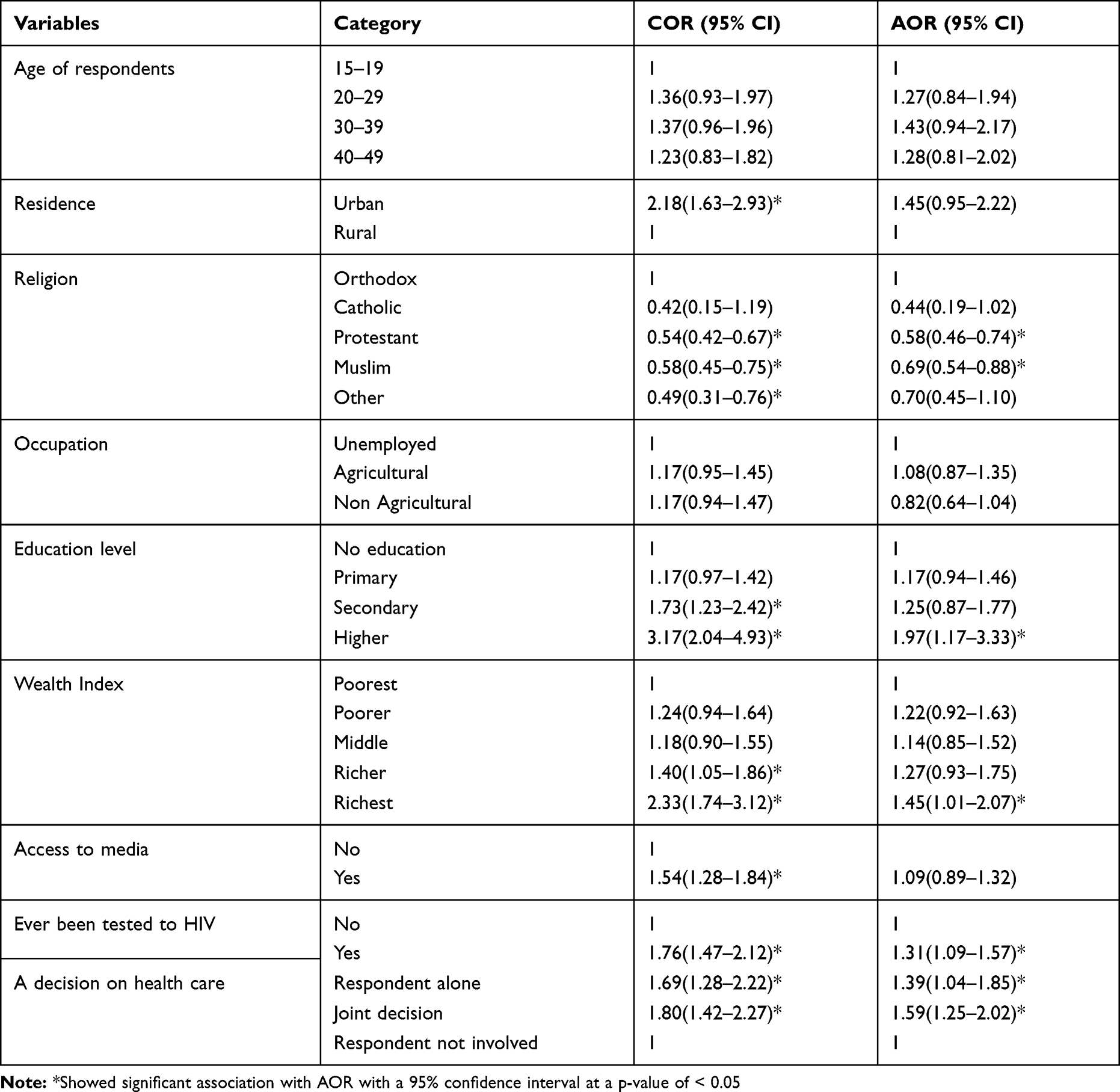 |
Table 3 Multivariate Analysis Table for Identifying Predictors of Attitudes Towards Condom Use Among Married Women in Ethiopia |
Discussion
To our knowledge, this is the first study to be conducted in Ethiopia to verify the relationship between women’s autonomy in health decision making and attitude to condom use in reducing the risk of HIV. This study found that women’s autonomy in health decision making power was positively associated with attitude to condom use. Also, joint health care decision power of the women with their husbands or partners increased their attitude to condom use. This finding is consistent with studies conducted in Philadelphia,37 India,14 Nigeria, and Kenya.38 This may be due to women who have greater autonomy are more likely to know about HIV/AIDS, and condoms.14,16,19 Also, women’s autonomy and the joint decision of the women with her husband/partner determines the nature of their sexual relationships, including attitude to condom use.44
Women who attended higher education had higher odds of attitude to condom use compared to their counterparts. This may be due to a positive effect of higher education levels on health-related outcomes including HIV knowledge and condom use.14,44,45 Moreover, education could modify some of the power dynamics within marriages so that more educated women believe more empowered to engage their husbands in discussions about condoms and their husbands are more unlock to these discussions. As a result, we would expect that these discussions would increase the likelihood of that couple’s attitudes to using condoms.16
Besides, Muslim and Protestant religious followers had less likely to have an attitude towards condom use. This may be due to religious ideology influencing condom use. The measure of religiosity (attendance at religious services, group affiliation, attitudes, perceptions of negative sanctions, and adherence to sanctions) was found to be associated with sexuality.46
Women in the highest wealth index quintile (richest) in Ethiopia were more likely to have positive attitudes toward condom use in reducing HIV risk compared to the poorest. This finding is consistent with multi-country studies, which were conducted in Nigeria, Kenya, and Nepal.38 This may be explained economically better off women increase the level of HIV/AIDS-related knowledge,47 higher opportunities for employment and education, which foster empowerment of women.48 Besides, women who ever tested for HIV have increased the attitude to condom use. This may be due to the effect of HIV testing on increasing the knowledge of HIV/AIDS transmission and its prevention.49,50
Strength and Limitation of the Study
Although findings in this study are useful for policy, there are some noteworthy limitations. For example, the data were collected from secondary data and our study may not be devoid of the shortcomings associated with this approach. Notwithstanding these limitations, our study is one of the few that have contributed in the context of women’s autonomy on health decision making and attitude to condom use in reducing risk for HIV, as no other studies done in the country using national representative data up to date.
Conclusions
The present study revealed that women’s autonomy in health decision making improves attitudes toward condom use during sex for HIV prevention in Ethiopia. Besides, women’s higher education, get better wealth index, and HIV testing perks up the attitudes toward condom use; but religious affiliation deter it. Therefore, an all-inclusive strategy is needed to be implemented by the governments, policymakers, and intervention programmers to empower women to have full control of their healthcare decisions. Moreover, women should be mobilized, encouraged to pursue higher education, enabled to access economic resources, and provided with support to undergo HIV testing. Furthermore, designing interventions that address primary prevention strategies like using a condom consistently along with addressing religious affiliation can have a significant effect on curtailing HIV/AIDS scourge.
Data Sharing Statement
We used the USAID–DHS program 2016 Ethiopian demographic and health survey data set for this analysis. To request the same or different data for another purpose, a new research project request should be submitted to the DHS program here: https://dhsprogram.com/data/Access-Instructions.cfm. After receiving permission, the researcher can log in and select the specific data in the format they prefer.
Acknowledgments
We would like to express gratitude to the USAID–DHS program for offering the 2016 Ethiopia Demographic and Health Survey data set.
Author Contributions
All authors made a significant contribution to the work reported in all areas; took part in drafting, revising, or extremely reviewing the article; gave a final endorsement of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be responsible for all aspects of the work.
Funding
There is no funding to report.
Disclosure
We confirm that this research is our original paper. The authors report no conflicts of interest for this work.
References
1. Ghanotakis E, Mayhew S, Watts C. Tackling HIV and gender-based violence in South Africa: how has PEPFAR responded and what are the implications for implementing organizations? Health Policy Plan. 2009;24(5):357–366. doi:10.1093/heapol/czp024
2. Ghosn J, Taiwo B, Seedat S, Autran B, Katlama C. HIV. Lancet. 2018;392(10148):685–697. doi:10.1016/S0140-6736(18)31311-4
3. Magadi MA. Understanding the gender disparity in HIV infection across countries in sub-Saharan Africa: evidence from the demographic and health surveys. Sociol Health Illn. 2011;33(4):522–539. doi:10.1111/j.1467-9566.2010.01304.x
4. Deribew A, Biadgilign S, Deribe K, et al. The Burden of HIV/AIDS in Ethiopia from 1990 to 2016: evidence from the global burden of diseases 2016 study. Ethiop J Health Sci. 2019;29(1):859–868.
5. Central Statistical Agency (CSA) and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia;Rockville, Maryland,; 2018.
6. Gillespie S. Poverty, food insecurity, HIV vulnerability and the impacts of AIDS in sub? Saharan Africa. 2008.
7. Beegle K, Ozler B. Young Women, Rich (Er) Men and the Spread of HIV. Washington, DC Mimeo: The World Bank; 2006.
8. Njue C, Voeten HA, Remes P. Porn video shows, local brew, and transactional sex: HIV risk among youth in Kisumu, Kenya. BMC Public Health. 2011;11(1):635. doi:10.1186/1471-2458-11-635
9. Bouare O. Modeling contextual determinants of HIV/AIDS prevalence in South Africa to inform policy. Afr J Reprod Health. 2009;13:3.
10. Gupta GR. How men’s power over women fuels the HIV epidemic. BMJ. 2002;324(7331):183–184. doi:10.1136/bmj.324.7331.183
11. Bowman CG. Theories of domestic violence in the African context. Am UJ Gender Soc Pol’y & L. 2002;11:847.
12. Maimburg RD. Women’s autonomy - A cornerstone of reproductive rights. Sexual Reproductive Healthcare. 2019;22:100463. doi:10.1016/j.srhc.2019.100463
13. Chi BK, Rasch V, Thị Thúy Hạnh N, Gammeltoft T. Pregnancy decision-making among HIV positive women in Northern Vietnam: reconsidering reproductive choice. Anthropol Med. 2011;18(3):315–326. doi:10.1080/13648470.2011.615909
14. Bloom SS, Griffiths PL. Female autonomy as a contributing factor to women’s HIV-related knowledge and behaviour in three culturally contrasting States in India. J Biosoc Sci. 2007;39(4):557–573. doi:10.1017/S0021932006001623
15. Wayal S, Cowan F, Warner P, Copas A, Mabey D, Shahmanesh M. Contraceptive practices, sexual and reproductive health needs of HIV-positive and negative female sex workers in Goa, India. Sex Transm Infect. 2011;87(1):58–64. doi:10.1136/sti.2010.043158
16. Adamczyk A, Greif M. Education and risky sex in Africa: unraveling the link between women’s education and reproductive health behaviors in Kenya. Soc Sci Res. 2011;40(2):654–666. doi:10.1016/j.ssresearch.2010.12.003
17. Mbonu NC, Van den Borne B, De Vries NK. Gender-related power differences, beliefs and reactions towards people living with HIV/AIDS: an urban study in Nigeria. BMC Public Health. 2010;10:334. doi:10.1186/1471-2458-10-334
18. Durevall D, Lindskog A. Economic inequality and HIV in Malawi. World Dev. 2012;40(7):1435–1451. doi:10.1016/j.worlddev.2011.12.003
19. Atteraya MS, Kimm H, Song IH. Women’s autonomy in negotiating safer sex to prevent HIV: findings from the 2011 Nepal Demographic and Health Survey. AIDS Education Prevention. 2014;26(1):1–12. doi:10.1521/aeap.2014.26.1.1
20. Mashinini DP, Pelton-Cooper M. HIV risk in a group of educated urban Black African women in South Africa: private accounts of gendered power dynamics. Fem Psychol. 2012;22(2):204–219. doi:10.1177/0959353512439190
21. Jewkes RK, Dunkle K, Nduna M, Shai N. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet. 2010;376(9734):41–48. doi:10.1016/S0140-6736(10)60548-X
22. Chacham AS, Maia MB, Greco M, Silva AP, Greco DB. Autonomy and susceptibility to HIV/AIDS among young women living in a slum in Belo Horizonte, Brazil. AIDS Care. 2007;19(Suppl 1):S1222. doi:10.1080/09540120601114402
23. Darteh EKM, Dickson KS, Doku DT. Women’s reproductive health decision-making: A multi-country analysis of demographic and health surveys in sub-Saharan Africa. PLoS One. 2019;14(1):e0209985. doi:10.1371/journal.pone.0209985
24. Kc S, Neupane S. Women’s autonomy and skilled attendance during pregnancy and delivery in Nepal. Matern Child Health J. 2016;20(6):1222–1229. doi:10.1007/s10995-016-1923-2
25. Rahman M. Women’s autonomy and unintended pregnancy among currently pregnant women in Bangladesh. Matern Child Health J. 2012;16(6):1206–1214. doi:10.1007/s10995-011-0897-3
26. Rahman MM, Mostofa MG, Hoque MA. Women’s household decision-making autonomy and contraceptive behavior among Bangladeshi women. Sexual Reproductive Healthcare. 2014;5(1):9–15. doi:10.1016/j.srhc.2013.12.003
27. Sano Y, Sedziafa AP, Vercillo S, Antabe R, Luginaah I. Women’s household decision-making autonomy and safer sex negotiation in Nigeria: an analysis of the Nigeria demographic and health survey. AIDS Care. 2018;30(2):240–245. doi:10.1080/09540121.2017.1363363
28. Coates TJ, Richter L, Caceres C. Behavioural strategies to reduce HIV transmission: how to make them work better. Lancet. 2008;372(9639):669–684. doi:10.1016/S0140-6736(08)60886-7
29. Shelton JD, Cassell MM, Adetunji J. Is poverty or wealth at the root of HIV? Lancet. 2005;366(9491):1057–1058. doi:10.1016/S0140-6736(05)67401-6
30. Ajuwon AJ, McFarland W, Hudes ES, Adedapo S, Okikiolu T, Lurie P. HIV risk-related behavior, sexual coercion, and implications for prevention strategies among female apprentice tailors, Ibadan, Nigeria. AIDS Behav. 2002;6(3):229–235. doi:10.1023/A:1019839824312
31. Nuttall J, Romano J, Douville K, et al. The future of HIV prevention: prospects for an effective anti-HIV microbicide. Infect Dis Clin North Am. 2007;21(1):219–39, x. doi:10.1016/j.idc.2007.01.009
32. Crosby RA. State of condom use in HIV prevention science and practice. Curr HIV/AIDS Rep. 2013;10(1):59–64. doi:10.1007/s11904-012-0143-7
33. Leclerc‐Madlala S. Youth, HIV/AIDS and the importance of sexual culture and context. Soc Dyn. 2002;28(1):20–41. doi:10.1080/02533950208458721
34. Terry PE, Mhloyi M, Masvaure TB, Adlis SA. Gender equity and HIV/AIDS prevention: comparing gender differences in sexual practice and beliefs among Zimbabwe university students. Int Q Community Health Educ. 2004;24(1):29–43. doi:10.2190/F5VV-JPNE-71AT-8FUH
35. Tsai AC, Subramanian SV. Proximate context of gender-unequal norms and women’s HIV risk in sub-Saharan Africa. AIDS. 2012;26(3):381–386. doi:10.1097/QAD.0b013e32834e1ccb
36. Maticka-Tyndale E. Condoms in sub-Saharan Africa. Sex Health. 2012;9(1):59–72. doi:10.1071/SH11033
37. Bonacquisti A, Geller PA. Condom-use intentions and the influence of partner-related barriers among women at risk for HIV. J Clin Nurs. 2013;22(2324):3328–3336. doi:10.1111/jocn.12101
38. Sharma BB, Small E, Mengo C, Ude P. Women’s autonomy and attitudes toward condom use: a multicountry analysis. Soc Work Public Health. 2017;32(4):238–253. doi:10.1080/19371918.2016.1275073
39. Boer H, Mashamba MT. Gender power imbalance and differential psychosocial correlates of intended condom use among male and female adolescents from Venda, South Africa. Br J Health Psychol. 2007;12(Pt 1):51–63. doi:10.1348/135910706X102104
40. Carael M, Marais H, Polsky J, Mendoza A. Is there a gender gap in the HIV response? Evaluating national HIV responses from the United Nations General Assembly Special Session on HIV/AIDS country reports. JAIDS. 2009;52:S111S8. doi:10.1097/QAI.0b013e3181baeec2
41. Sia D, Onadja Y, Hajizadeh M, Heymann SJ, Brewer TF, Nandi A. What explains gender inequalities in HIV/AIDS prevalence in sub-Saharan Africa? Evidence from the demographic and health surveys. BMC Public Health. 2016;16(1):1136. doi:10.1186/s12889-016-3783-5
42. ICentral Statistical Agency and ICF. Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
43. Henry Ofori Duah I-A-A. Determinants of health care decision making autonomy among mothers of children under five years in ghana: analysis of 2014 ghana demographic and health survey. Int J Womens Health Wellness. 2017;3(4).
44. Mengo C, Small E, Sharma BB, Paula U. Risky sexual behavior of multiple partner relations and women’s autonomy in four countries. Sex Cult. 2016;20(3):535–554. doi:10.1007/s12119-016-9341-6
45. Snelling D, Rasugu ODW, Hong S, Georgiades K, Racine Y, Boyle MH. HIV/AIDS knowledge, women’s education, epidemic severity and protective sexual behaviour in low- and middle-income countries. J Biosoc Sci. 2007;39(3):421–442. doi:10.1017/S0021932006001465
46. Sarkar NN. Barriers to condom use. Eur j Contraception Reproductive Health Care. 2008;13(2):114–122. doi:10.1080/13625180802011302
47. Faust L, Yaya S, Ekholuenetale M. Wealth inequality as a predictor of HIV-related knowledge in Nigeria. BMJ Global Health. 2017;2(4):e000461. doi:10.1136/bmjgh-2017-000461
48. Rodrigo C, Rajapakse S. HIV, poverty and women. Int Health. 2010;2(1):9–16. doi:10.1016/j.inhe.2009.12.003
49. Hutchinson AB, Branson BM, Kim A, Farnham PG. A meta-analysis of the effectiveness of alternative HIV counseling and testing methods to increase knowledge of HIV status. AIDS. 2006;20(12):1597–1604. doi:10.1097/01.aids.0000238405.93249.16
50. Salway T, Thomson K, Taylor D, et al. Post-test comparison of HIV test knowledge and changes in sexual risk behaviour between clients accessing HIV testing online versus in-clinic. Sex Transm Infect. 2019;95(2):102–107. doi:10.1136/sextrans-2018-053652
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.