Back to Journals » Risk Management and Healthcare Policy » Volume 16
Does Unified Pool Arrangement Trigger Healthcare Corruption? Evidence from China’s Public Health Insurance Reform
Authors Wu J ![]()
Received 18 September 2023
Accepted for publication 28 October 2023
Published 3 November 2023 Volume 2023:16 Pages 2259—2261
DOI https://doi.org/10.2147/RMHP.S435404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jing Wu
School of Public Administration, Yanshan University, Qinhuangdao, Hebei Province, People’s Republic of China
Correspondence: Jing Wu, School of Public Administration, Yanshan University, West Section of Hebei Street No. 483, Qinhuangdao, Hebei Province, People’s Republic of China, Email [email protected]
The healthcare corruption has aroused heated discussions in China recently. From the beginning of 2023 to the present, at least 155 hospital directors have been investigated that the number is more than twice that of last year. The healthcare corruption was not only a matter of physician morality but also reflected the defects of China’s medical system.1
Since the establishment of China’s Urban Employee Basic Medical Insurance (UEBMI) in 1998, China has formed a fragmented health insurance system in urban areas. Fragmentation hindered the mutual aid function of health insurance. Therefore, from 2009 to 2020, China carried out the health financing reform of UEBMI which adjusted the pooling level from the county to the municipal level. However, the increasing financialization of the healthcare system would result in physicians weakening accountability to the public.2 Horizontal integration and vertical management of fiscal power enabled the municipal governments to concentrate and allocate health funding, but the administrative decentralization led to laxity of spending supervision by county governments. This flawed system was a tough test for physicians. Without supervision, physicians might induce patients to increase healthcare services for the purpose of maximizing income.3 Figure 1 was the framework of Unified Pool arrangement in China.
 |
Figure 1 Framework of Unified Pool Arrangement. |
The paper aimed to discuss whether the unified pool reform would trigger healthcare corruption. Treating the pooling level adjustment reform of UEBMI as a quasi-experiment, the study tried to interpret the empirical results based on Chinese health insurance regulations, and explored the reasons for the high incidence of healthcare corruption in China.
Instead of focusing solely on patients’ utilization of healthcare services, the paper considered the behaviors of healthcare provider (eg, hospitals, physicians) and healthcare policy executor (eg, county governments, medical insurance bureau) by a quasi-experiment. The effects of the unified pool reform on outpatient expenditure were examined by using the staggered DID model, and the moderating effects of physician density were examined by using DDD model. The micro data in the study were from the China Health and Retirement Longitudinal Study (CHARLS) in 2011, 2013, 2015, and 2018。The macro data were from China City Statistical Yearbook. The documents were from on the official websites of the municipal-level governments, the Medical Insurance Bureau, and the Human Resources and Social Security Bureau. After excluding the samples with missing information and the samples of municipalities directly under the central government, this paper finally obtained panel data for 4 periods, 573 respondents who were continuously tracked, and a total of 2292 observations.
Table 1 showed that the treatment effects on outpatient reimbursement expenditure were significant at a 5% significance level, no matter whether control variables were added. The implementation of unified pool reform would lead to a significant increase in outpatient reimbursement expenditure, rather than copayment expenditure. The treatment effects on outpatient expenses were also mainly caused by the increase in outpatient reimbursement expenditure. We utilized the parallel trend test to test the robustness of the empirical results and the results of the robustness test methods were consistent with the benchmark regression results. Table 2 showed that the physician density interaction coefficients were positively significant in the 5% significance level. In the pilot cities, increasing physician density would have a positive moderating effect on outpatient reimbursement expenditure. The pooling level reform would make the county governments loosen the supervision of funds spending.
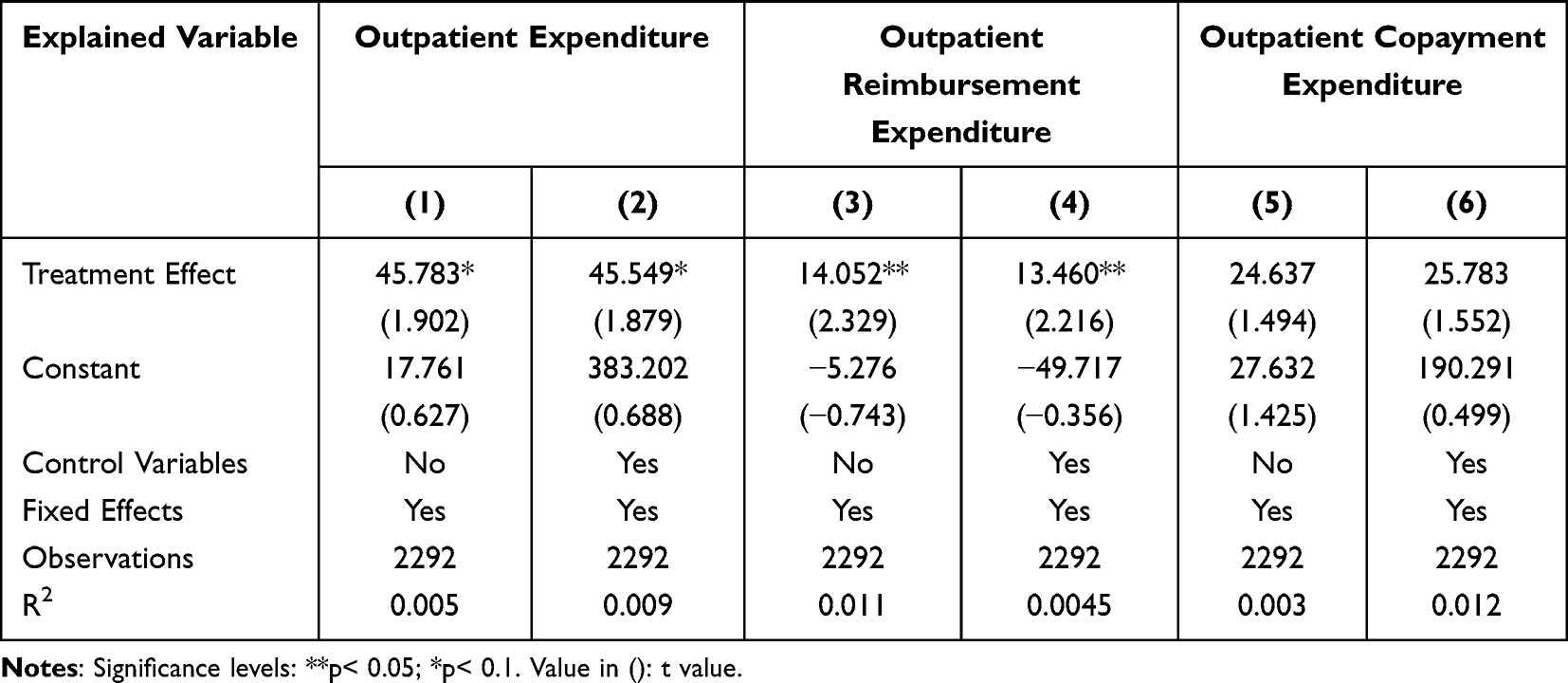 |
Table 1 Effects of Unified Pool Reform on Outpatient Expenditure |
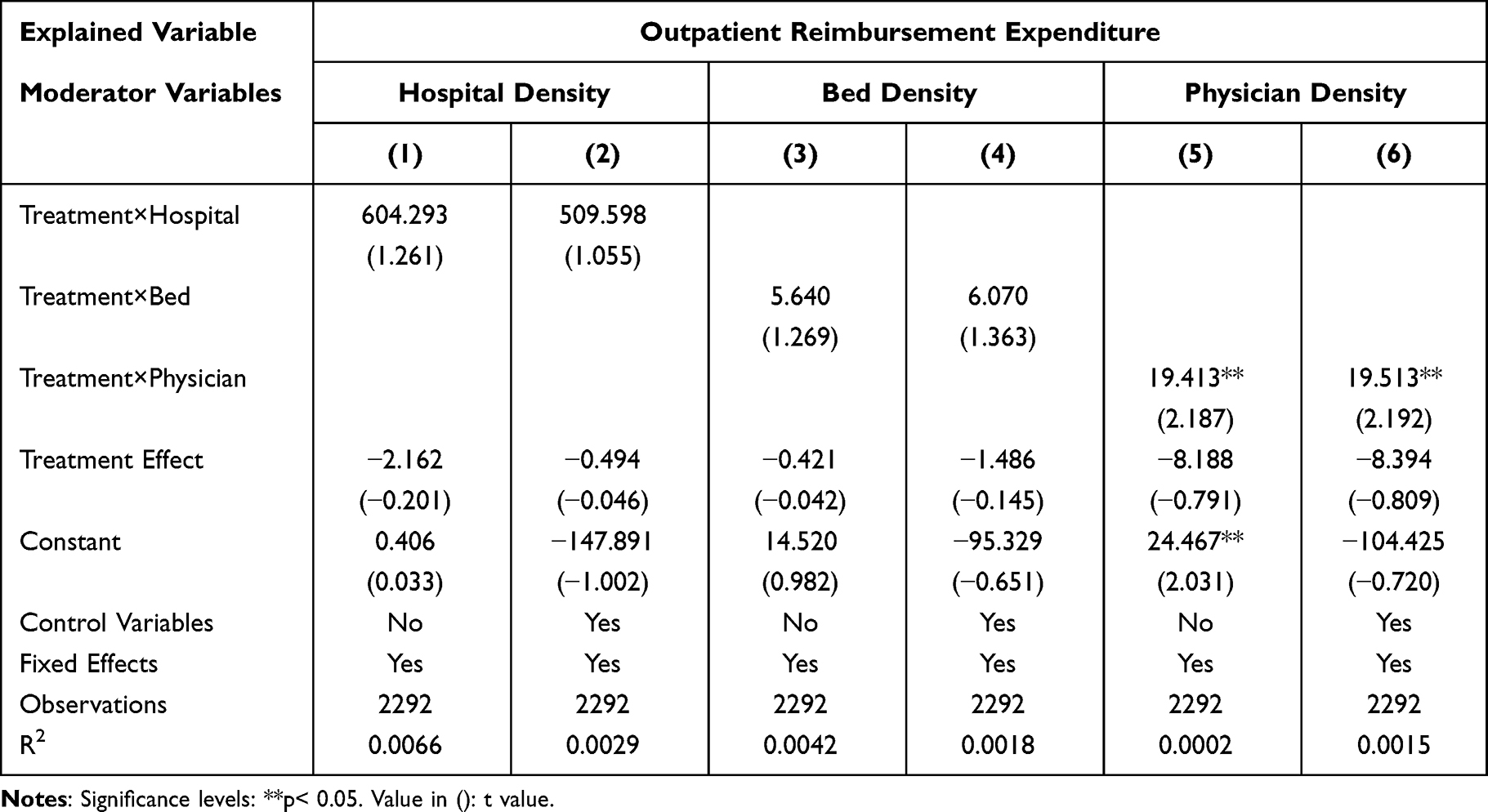 |
Table 2 Moderating Effects of Medical Resources Density |
According to the theory of demand inducement, an increase in physician density would lead to an increase in the quantity of inducement. The positive coefficient of the empirical results proved that the induced demand caused by the increase in physician density would increase the expenditure after the unified pool reform. In the system of fiscal concentration and administrative decentralization, the county governments would relax the supervision of healthcare providers, and the physicians would induce patients to increase their consumption of health services. Therefore, the county governments’ moral hazard caused by the pooling level reform would trigger healthcare corruption. Nonetheless, this letter emphasized that demand inducement does not equal healthcare corruption, but I cannot directly obtain data on the behavior of hospital leaders. Due to data limitations, physician density is adopted to examine healthcare corruption, which is also a shortcoming of this research.
Data Sharing Statement
The data of China Health and Retirement Longitudinal Survey (CHARLS) database are openly available at: http://charls.pku.edu.cn/.
Ethical Approval
Ethical approval for all the CHARLS waves was granted from the Institutional Review Board at Peking University. The IRB approval numbers are IRB00001052-11015 and IRB00001052-11014. As the datasets of CHARLS are publicly available, ethical approval was not needed for this study.
Disclosure
The author declares no conflict of interest.
References
1. Zhang P. Analysis of the public health functions of the Chinese government in the prevention and control of COVID-19. Risk Manag Healthc Policy. 2021;14:237–246. doi:10.2147/RMHP.S284251
2. Simonet D. Health care reforms, power concentration, and receding citizen participation. Risk Manag Healthc Policy. 2023;16:1359–1364. doi:10.2147/RMHP.S421397
3. Kilgore M, K PH, Kielhorn A, et al. Economic burden of hospitalizations of medicare beneficiaries with heart failure. Risk Manag Healthc Policy. 2017;10:63–70. doi:10.2147/RMHP.S130341
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.