Back to Journals » Clinical Ophthalmology » Volume 17
Does Surgical Resection of Horizontal Extraocular Muscles Disrupt Ocular Proprioceptors?
Authors Paduca A ![]() , Lundmark PO
, Lundmark PO ![]() , Bruenech JR
, Bruenech JR
Received 15 November 2022
Accepted for publication 6 April 2023
Published 15 May 2023 Volume 2023:17 Pages 1395—1405
DOI https://doi.org/10.2147/OPTH.S381247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ala Paduca,1 Per O Lundmark,2 J Richard Bruenech2
1Ophthalmology Department, State University of Medicine and Pharmacy Nicolae Testemitanu, Chisinau, Republic of Moldova; 2Department of Optometry, Radiography and Lighting Design, Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg, Norway
Correspondence: Ala Paduca, PhD Ophthalmology Department, State University of Medicine and Pharmacy Nicolae Testemitanu, bd Stefan cel Mare si Sfant 165, Chisinau, Republic of Moldova, Email [email protected]
Purpose: It has been promoted that disturbance of ocular proprioception may play a role in the pathogenesis of concomitant strabismus and other types of oculomotor anomalies. The aim of the study was to obtain knowledge about how surgical foreshortening of the myotendinous region potentially affects the proprioceptors that resides in this area of the muscles and to test the hypothesis that avoiding disruption of ocular proprioceptors result in a more favorable long term postoperative result.
Patients and Methods: The distal end of the lateral and medial rectus muscles from patients with manifest concomitant strabismus with a deviation of ≥ 15 prism diopters (PD) were collected during strabismus surgery and processed for light microscopy by standard histochemical techniques. Histological analysis served to differentiate between the tissue samples containing pure tendon, versus samples containing the myotendinous junction. Criteria for successful outcome was defined as a residual angle of deviation less than 10 PD. The binocular status of the patient was measured pre- and post-operatively at 6-months of follow-up.
Results: Tissue samples from 43 patients (median age 19 years old, range 3– 58 years) were collected during surgery. Twenty-six of the samples contained pure tendon, while 17 contained muscle fibres. The evolution of the post-operative result revealed a moderate reduction in the residual angle of deviation in patient-samples containing pure tendon. In contrast, the residual angle of deviation clearly increased in patient-samples containing muscle fibres. The difference between the two groups reached statistical significance after 6 months. Successful outcome was found to be more than three times more likely in cases where surgery was performed in pure tendon, compared to muscle fibres.
Conclusion: The current study supports the hypothesis that avoiding disruption of ocular proprioceptors, located in the distal myotendinous region, results in a more favorable postoperative result.
Keywords: strabismus, surgical outcome, proprioception
Corrigendum for this paper has been published.
Introduction
Proprioceptive input from the extraocular muscles is suggested to play an important role in the ocular alignment control, spatial orientation, postural control and in the development of binocular vision.1–8 There is a growing consensus in the recent literature that nerve terminals, located at the myotendinous junction, constitute one of the principal sources of ocular proprioception. Dogiel was the first to describe these structures and designated them palisade endings in his publication from 1906.9 His observations have been confirmed by other workers in a variety of other frontal eyed mammals.10–12 Palisade endings in more recent literature have been referred to as “innervated myotendinous cylinders (IMCs)” which describes how the innervated distal tip of some muscle fibers is encapsulated by a cylindrical fibrous sheet of collagen.13 The horizontal recti seem to contain larger numbers of these structures compared with the vertical recti and oblique muscles.12 The highest density is usually observed in the medial rectus, which arguably supports the notion that palisade endings play an important role for convergence eye movements in frontal-eyed species.14,15 There seem to be a modest number of IMCs in muscle samples obtained from infant subjects, compared to the number observed in adults, which indicate that there might be a postnatal development of these structures.16,17 The neural element, assumed to be sensory, is exclusively associated with the distal end of non-twitch multiply innervated muscle fibres.13,18,19 Most of the multiply innervated muscle fibres and their associated end organs are found in the global layer of the muscles.13 This layer constitutes muscle fibres that run adjacent to the eye, terminate on the scleral canopy, and participate in rotation of the globe.20 In contrast, the muscle fibres in the orbital layer insert in the fibroelastic Tenon’s capsule, forming a circular configuration of collagen, referred to as the pulley or pulley sleeve.21,22 The extraocular muscle direction of pull is believed to be influenced by the position of the pulley.20 Pulley activity may hence constitute yet another important parameter that could have implications for the outcome of eye muscle surgery. The orbital layer is richly endowed with muscle spindles, which puts them in a position to monitor pulley activity.23 Yet, the muscle spindle’s ability to provide such a function has been questioned by some authors.24,25
Accumulation of evidence from the research cited above supports the notion that the structural and functional organization of human extraocular muscles is complex, and that ocular proprioception may facilitate more aspects of ocular alignment and coordination than previously assumed. Several authors now believe that a disturbance of ocular proprioception in the myotendinous junction may play a role in the pathogenesis of a variety of oculomotor anomalies, including concomitant strabismus.26–28 Furthermore, disruption in the proprioceptive signal is also believed to potentially influence the strabismus surgery outcome.3,4
Yet, some uncertainty remains. Hence, the primary aim of the study was to obtain knowledge about how surgical foreshortening of the myotendinous region potentially affects the proprioceptors that reside in this area of the muscles. The secondary aim was to test the hypothesis that avoiding disruption of ocular proprioceptors result in a more favorable long-term postoperative result.
Materials and Methods
A prospective study was conducted. The study population consisted of patients operated for strabismus at the Republican Clinical Hospital “Timofei Mosneaga” and Children Clinical Hospital “Emilian Cotaga”, Chisinau, Republic of Moldova, between January 2017 and June 2019. The inclusion criteria were manifest concomitant strabismus with a deviation of ≥15 prism diopters (PD), operated by muscle resection or combine surgery recession/resection. Patients with nystagmus, intermittent, paralytic or restrictive strabismus, neurological problems, cognitive problems, language barrier or mental conditions limiting the proper understanding of their role in the study were excluded.
Based on a reported postoperative residual angle of deviation of 6PD with SD 4.9,29 a sample size of 16 in each group was estimated as sufficient to unveil a large effect size (Cohen’s d >1.0) of measured differences between the groups, with a statistical power of 80%.
The research was conducted in compliance with recognized international standards and the principles of the Declaration of Helsinki. The study was approved by the Medical Ethics Board of the State University of Medicine and Pharmacy “Nicolae Testemitanu”, Chisinau, Republic of Moldova. A similar approval was obtained from the Norwegian Regional Ethical Committee for histochemical processing of the material in the biomedical research lab at the University of South-East Norway, Kongsberg, Norway.
Ophthalmological and Orthoptic Examinations
All patients underwent a full ophthalmological and orthoptic examination before and directly after surgery which was performed by main investigator. They were further examined after 10 days and at 1, 3 and 6-months of follow-up. The patients' best corrected visual acuity (BCVA) was assessed monocularly by using a Snellen chart at 6 m. Refractive errors were determined by retinoscopy 25 minutes after the instillation of 1 drop of 1% Tropicamide (Mydriacyl, Alcon Lab. Inc.) twice at 5 minute intervals.30,31 The angle of deviation was determined by prisms and alternating-cover test at distance (6 m) and near (33 cm) with accommodative target fixation both pre and postoperatively. An additional near measurement was obtained after 1 h mono-ocular occlusion of the non-dominant eye, or by habitually deviating the eye to measure the largest angle of deviation. Post-occlusion near measurement was obtained with an additional +3.00 D sphere over each eye before permitting the patient to regain binocular fusional ability. The angles of deviation when gazing above, below, left, and right were measured in all the patients. For uncooperative patients (2 patients aged 3 and 4 years old), a modified Krimsky method was used. Ocular motility examination was performed. Binocular sensory status was examined by means of the Bagolini test and classified as binocular single vision (BSV), monocular suppression or alternating suppression. Stereopsis was evaluated by Titmus stereo test (Stereo Optical Inc., Chicago, IL, USA) at 30 cm. In 2 cases, we were not able to appreciate the BV status due to the patients’ age. Post-operative result was defined as successful if the deviation was ≤10 PD, while a deviation of >10 PD was defined as unsuccessful.29,32,33
Surgery and Tissue Preparation
Strabismus correction by unilateral R&R procedure was done by the same surgeon (A.P.), under peribulbar block or general anesthesia, using standard procedure proposed by Parks et al.34 Surgical dosage was based on the maximal deviation angle. In our cases, we preferred to limit recessions and resections up to 8 mm. Large recessions or resections cause alteration in the palpebral aperture of the eyes and eye motility, including lateral incomitance.35 The full width strip of rectus muscles excised during strabismus were immediately immersed in a fixative solution of 2.5% glutaraldehyde and stored in a refrigerator at a temperature of 10 C in the Human tissue Bank in Chisinau, Moldova, for a minimum of 1 week before further preparation.
After washing, muscle samples were immersed in a 1% solution of unbuffered Osmium Tetroxide for 1 hr., then dehydrated in graded ethanol, cleared in Xylene, and embedded in Araldite. Serial transverse sections were cut on an ultramicrotome with a thickness of 0.75 µm, then mounted on glass slides and stained with Toluidine blue. The initial cut was obtained from the distal end of the tissue (containing pure tendon), and advanced towards the proximal end of the tissue (containing muscle fibres). Every 5 to 8 sections were examined until reaching the first evidence of muscle fibres and thereafter complete serial sections through all identified neuromuscular structures.
Histological Analysis
All tissue samples were examined under a light microscope (ZEISS Axio Lab.A1 with led illumination) with a magnification ranging from 200 to 1000x. Histological features and biometric characteristics were documented by a customized system for image analysis (global lab image and Imaris).
Based on histological analysis, the tissue samples were identified as containing pure tendon (Figure 1), versus samples containing the myotendinous junction. The latter defined as the presence of muscle fibres (Figure 2) with positive identification of at least one myotendinous cylinder (Figure 3).
 |
Figure 1 Micrograph showing a transverse section of tendon obtained from a temporal rectus muscle, displaying an small artery enveloped by collagen and fibrocytes. No evidence of muscle fibres. Section stained with Toluidine blue. |
 |
Figure 2 Micrograph showing a transverse section of human extraocular muscles displaying the diversity in the fibre population. The light staining muscle fibres have large diameters and well-developed sarcoplasmic reticulum. The darker staining muscle fibres have smaller diameters and scares amounts of sarcoplasmic reticulum. Section stained with Toluidine blue. |
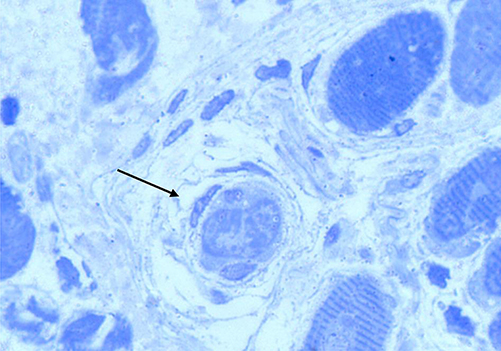 |
Figure 3 Micrograph showing a transverse section of human extraocular muscles displaying the preterminal distal end of a small dark staining muscle fibre where contractile elements are encapsulated by a few surrounding sheets of connective tissue (arrow). Section stained with Toluidine blue. |
The data obtained by this method was cross-referenced with muscle samples from non-strabismus subjects. The latter material, constituting full-length post-mortem material from 4 medial rectus muscles (range 4–74 years), was obtained from stock in the biobank in Norway. The material was used to observe potential histological dissimilarities between strabismus and non-strabismus muscle material. It also enabled histological examination of other type of receptors in a more proximal region of the muscle. This confirmed the location of muscle spindles and verified the absence of spindles in the resected material (Figure 4).
 |
Figure 4 Micrograph showing a transverse section of human extraocular muscles displaying a muscle spindle with 5 intrafusal fibres encapsulated by a capsule of perineural tissue. Stained with Toluidine blue. |
Data analyses of the patients’ demographic data, clinical characteristics and surgery outcome were performed with commercial software, Statistical Package for Social Sciences (SPSS IBM SPSS Statistics for Windows, version 28.0. IBM Corp.). Descriptive statistics were expressed as mean and standard deviation (SD) or median, interquartile range (IQR); categorical data are presented as percentages. Mann Whitney U and t-test was used for comparing groups. Statistical significance was defined as p < 0.05 (two-sided).
Results
Forty-eight patients were initially enrolled into the study. Five of the patients were later excluded because the muscle samples obtained during surgery were found to be inadequate for histological analysis. Demographics and clinical characteristics are presented in Table 1.
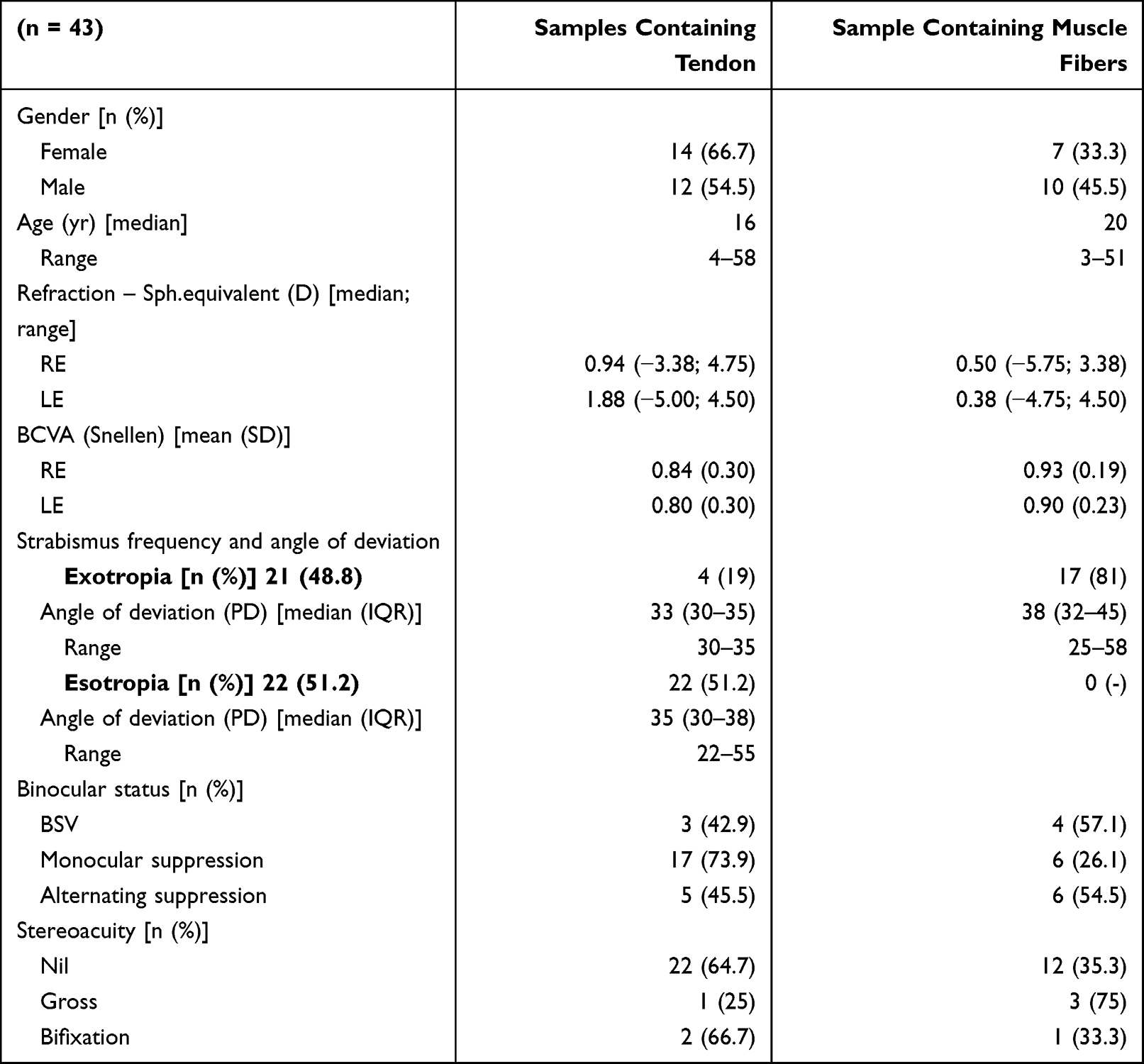 |
Table 1 General Demographics and Preoperative Clinical Characteristics of Subjects Included in the Study |
The post-surgical outcome measured after 6 months was found to be successful in 24 (55.8%) of the 43 resections performed on the horizontal rectus muscles. The remaining 19 (44.2%) was unsuccessful (based on the 10 PD criteria). Histological analysis revealed that 20 (76, 9%) out of the 26 samples containing pure tendon were clinically successful, while this was true for only 4 (23.5%) out of 17 of the samples containing muscle fibres. Hence, in the current study successful outcome was found to be 3.3 times more likely in cases where surgery was performed in pure tendon, compared to surgery performed in muscle fibres. The evolution of the surgical outcome is presented in Table 2 and Figure 5.
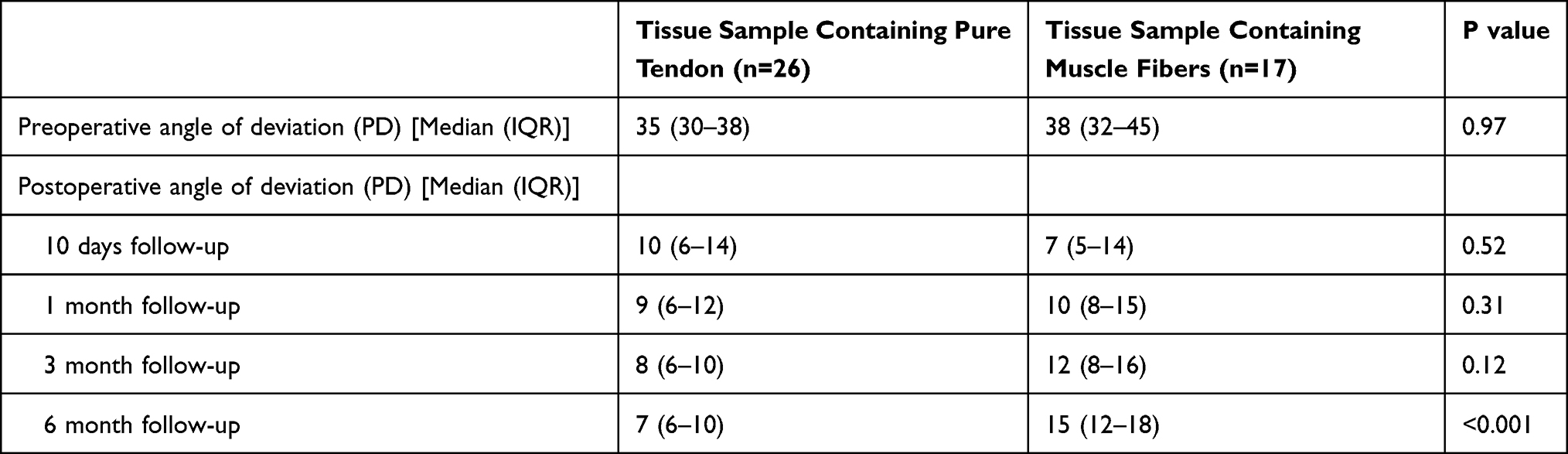 |
Table 2 Angle of Deviation Evolution According to Identified Type of Tissue Sample (Mann–Whitney U-Test) |
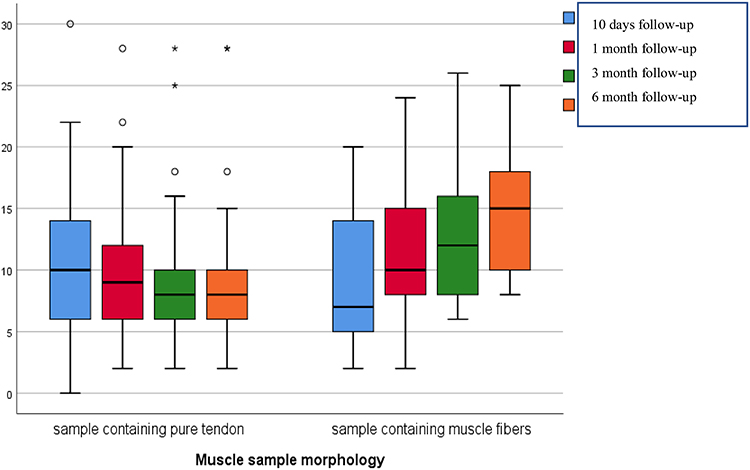 |
Figure 5 Angle of deviation evolution at 6 month follow-up. |
The evolution of the post-surgical deviation showed a mean reduction of 3 PD in the samples containing pure tendon. In contrast, the samples containing muscle fibres showed an increase in the post-surgical deviation by a mean of 8 PD. Comparison between the two groups showed an opposite and statistically significant difference at the 6-months follow-up (p < 0.001).
Binocular sensory status is displayed in Figure 6. The post-operative results showed an increase in frequency of BSV, by 38.5%, in the samples containing pure tendon. In contrast, the samples containing muscle fibres showed an increase of less than 11.8%. The difference between the two groups was statistically significant (p = 0.01).
 |
Figure 6 Preoperative (left) and postoperative (6 month follow-up) (right) binocular vision status according to muscle morphology. |
The associations between the type of deviation (convergent or divergent) and surgical interference with the myotendinous region is displayed in Figure 7. Seventeen out of 21 resection procedures performed on the medial rectus muscle to correct exotropia, implicated the myotendinous region. This stands in contrast to the resections on the lateral rectus muscle to correct convergent deviations, where none of the cases (22 lateral muscle) implicated the myotendinous region.
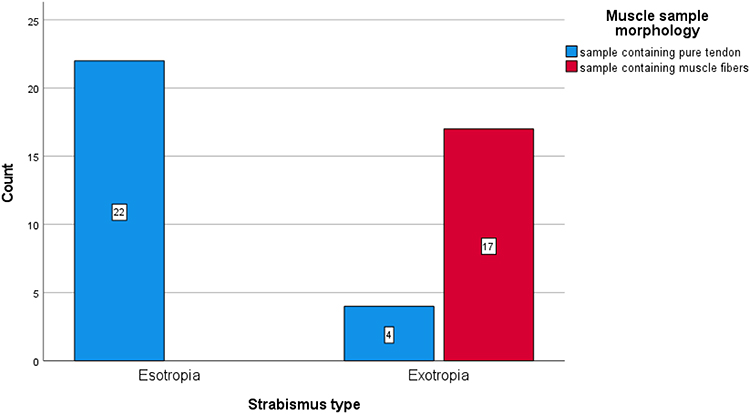 |
Figure 7 The associations between type of deviation (esotropia/exotropia) and surgical interference with the myotendinous region. |
Resections of the medial rectus muscle, beyond the length of 5.5 mm, increases the likelihood of disrupting the myotendinous region where the receptors reside. Whereas resections on the lateral rectus muscle can be performed up to 7mm without disruption of the myotendinous region (Figure 8).
 |
Figure 8 Muscle resection amount in relation to muscle morphology. Abbreviations: *LRM, lateral rectus muscle; MRM, medial rectus muscle. |
Discussion
Results from the current study revealed that successful outcome of strabismus surgery, according to 10 PD criteria, was 3.3 times more likely in those cases where resection was performed in pure tendon, compared to surgery performed involving muscle fibres. A similar ratio of likelihood of success was found for postoperative BSV, ie, an increase of 40% associated with resection performed in pure tendon vs 12.5% associated with resection performed in muscle fibres. However, it is important to mention that a large percentage of participants in both groups 48.8% still did not regain binocular single vision after strabismus surgery which can be due also to longstanding strabismus. Almost all of our patients were operated after vision maturation age (≥9 years old)36 (83.7%).
There are various options in the management of strabismus, and the procedures differ in how they affect the neuromuscular arrangement including Botulinum toxin injection37 and Bupivacaine.38 However, it has been suggested that botulinum toxin induce ultrastructural changes in the myotendinous nerve endings and that the toxin temporarily affects proprioceptive feedback from palisade endings.39,40 The effect of Bupivacaine on extraocular muscle proprioception remains unclear and further animal studies are required.
Muscle fibres in human extraocular muscles are highly specialized, innervated by different pools of motor neurons and arranged in layers with different physiological functions.41 Furthermore, it has recently been promoted that there is a compartmental innervation of extraocular muscles which suggests that segment of both the orbital and global layer can contract, on an individual basis.22,42 Such a structural organization indicates a wider division of labor between muscle segments than previously assumed, which in turn should require a highly structured and specific neural feedback. This imposes a variety of challenges for the surgeon because it is difficult to alter the strength of a muscle, or its direction of pull, without interfering with the proprioceptive signal. There is a certain consensus in the ophthalmic literature regarding the potential sources of proprioception. In contrast to extraocular muscles in other mammals, human extraocular muscles do not contain Golgi tendon organs therefore the only remaining reputable sources are muscle spindles and palisade endings/myotendinous cylinders.16 Their different locations, in the orbital and global layers, respectively, and their structural organization indicate that they provide different types of afferent information. The muscle fibres in the orbital layer, constituting nearly half the total, insert onto the orbital side of the fibroelastic Tenon’s capsule, while circling each muscle to form a pulley or pulley sleeve.21,43,44 Contraction of orbital fibres will hence affect the position and activity of the pulleys, which in turn will influence the muscle’s direction of pull.21 However, histological analysis of the material put to use in the current study clearly indicates that even the longest resections did not interfere with the region of the muscle containing muscle spindles. Spindles were only identified in the post-mortem material and, consistent with previous observation, had a remote location in relation to the distal myotendinous junction.5,16,24,25 The global fibres, on the other hand, insert onto the globe and provide the contractile force required to perform ocular rotations. Many of the multiply innervated muscle fibres in this layer were associated with structures with proprioceptive features (the IMCs). The potential proprioceptive capacity of these structures is not fully resolved, yet the results from the current study indicate that the best post-operative result was obtained in those patients where the surgical procedures did not interfere with the myotendinous region (where the structures reside). Furthermore, the oculomotor status of these patients improved gradually during the 6 months follow-up period. It seems legitimate to argue that this was caused by the oculomotor system's ability to restore ocular alignment through tuning of the efferent signal, a function that arguably relies on proprioceptive feedback from the extraocular muscles about eye position. It is of interest that all patients with undisrupted receptors seemed to have the ability to gradually reduce their postoperative deviation during the follow-up period, regardless of their numerical age. This indicates that there is a certain plasticity and ability to restore binocular functions throughout the various stages of life. This seems to apply even in mature patients, where the extraocular muscles are known to contain various signs of age-related degenerative changes.16
In the current study, the resection performed on the lateral rectus muscles was approximately equal to the resections performed on medial rectus muscles. Yet, histological analyses revealed that muscle fibres were only observed in the tissue obtained from medial rectus muscles. This reflects the difference between the short tendon of the medial rectus muscles compared to the long aponeurosis of the lateral rectus muscle. The latter muscle approaches the posterior aspect of the globe from an angle and must follow an arcuate path for some distance before it terminates, which is why the length of the lateral rectus tendon is claimed to be the double of that of the medial rectus.45 The rough estimate by these workers is consistent with our findings. Resections up to 7 mm of the temporal rectus could be performed without implicating the myotendinous junction, while resections of more than 5.5 mm on the medial rectus did so.
The patients with undisrupted myotendinous junction had a better successful motor outcome at 6 months follow-up, compared to patients where the muscle resection implicated muscle fibres. These results indicate that the evolution of the post-operative residual angle of deviation is highly influenced by the quality of the proprioceptive signal. It seems legitimate to argue that proprioception is an influencing factor of the surgical success. Proprioception may arguably also be implicated in the difference of surgical outcomes between manifest exotropia and esotropia. Resection of the medial rectus muscles, which contains the highest number of receptors, will arguably disrupt the proprioceptive signal more than a resection on the lateral rectus. Furthermore, proprioception is also believed to arise from receptors in the smooth muscle of the ciliary body, which arguably facilitate the required co-contraction of smooth and cross striated muscles during accommodation.46 Disruption of receptors in the medial rectus muscles may arguably interfere with this relationship.
Based on the current results, it seems advantageous to perform binocular surgeries in cases with large angles of deviations instead of large monocular muscle resection. Reducing the amount of resection in one extraocular muscle, by performing recession on the antagonist, may preserve the myotendinous area where the IMCs reside. However, further studies comparing surgical procedures are warranted.
The current study has some limitations related to sample size, as including more tissue samples in the study would have strengthened the statistical analysis. Another limitation is associated to the quality and the size of the tissue samples. The histological analysis was primarily based on observations of resected material which could not provide information about the full complement or distribution of receptors. Furthermore, it is difficult to obtain the same quality when processing tissue obtained through surgical procedures compared to tissue obtained through post-mortem dissection. However, the notion that histological details have been missed or misinterpreted due to low resolution seems unlikely and does not undermine the value of the following conclusion.
Conclusions
The current study supports the hypothesis that avoiding disruption of ocular proprioceptors, located in the distal myotendinous region, results in a more favorable postoperative result, both regarding the angle of deviation and binocular vision.
Abbreviations
EOM, extraocular muscle; LRM, lateral rectus muscle; MRM, medial rectus muscle; ET, esotropia; XT, exotropia; IMCs, innervated myotendinous cylinders; BSV, binocular single vision; PD, prism diopter; BCVA, best corrected visual acuity; D, diopters; R&R, recession–resection.
Data Sharing Statement
The dataset generated and analyzed in this study is not publicly available yet because it is a part of the PhD work in progress. Data information is available from the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted following the Declaration of Helsinki and was approved by the Ethics Committee of the State University of Medicine and Pharmacy Nicolae Testemitanu (No.36/76 (2016)). Written informed consent was approved by the EC SUMP and obtained before the patients’ participation in the survey and from the parents or guardians for patients under 18 years old.
Patient and Public Involvement Statement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding to declare.
Disclosure
The authors declare that they have no competing interests.
References
1. Balslev D, Newman W, Knox PC. Extraocular muscle afferent signals modulate visual attention. Invest Ophthalmol Vis Sci. 2012;53(11):7004–7009. doi:10.1167/iovs.12-10249
2. Gauthier GM, Nommay D, Vercher JL. The role of ocular muscle proprioception in visual localization of targets. Science. 1990;249(4964):58–61. doi:10.1126/science.2367852
3. Steinbach MJ, Smith DR. Spatial localization after strabismus surgery: evidence for inflow. Science. 1981;213(4514):1407–1409. doi:10.1126/science.7268444
4. Weir CR, Knox PC, Dutton GN. Does extraocular muscle proprioception influence oculomotor control? Br J Ophthalmol. 2000;84(9):1071. doi:10.1136/bjo.84.9.1071
5. Lukas JR, Blumer R, Aigner M, Denk M, Baumgartner I, Mayr R. Propriozeption aus äusseren Augenmuskeln des Menschen: Zur Morphologie ihrer Muskelspindeln [Proprioception of extra-ocular muscles in the human: on the morphology of muscle spindles]. Klin Monbl Augenheilkd. 1997;211(3):183–187. German. doi:10.1055/s-2008-1035119
6. Donaldson IM. The functions of the proprioceptors of the eye muscles. Philos Trans R Soc Lond B Biol Sci. 2000;355(1404):1685–1754. doi:10.1098/rstb.2000.0732
7. Bucci MP, Soufi H, Villeneuve P, Colleville L, Bui-Quoc E, Lions C. Importance of proprioceptive information for postural control in children with strabismus before and after strabismus surgery. Front Syst Neurosci. 2016;10:67. doi:10.3389/fnsys.2016.00067
8. Buisseret P. Influence of extraocular muscle proprioception on vision. Physiol Rev. 1995;75(2):323–338. doi:10.1152/physrev.1995.75.2.323
9. Dogiel AS. Die Endigungen der sensiblen Nerven in den Augenmuskeln und deren Sehnen beim Menschen und den Säugetieren. Archiv für mikroskopische Anatomie. 1906;68(1):501–526. doi:10.1007/BF02979882
10. Blumer R, Lukas JR, Wasicky R, Mayr R. Presence and structure of innervated myotendinous cylinders in sheep extraocular muscle. Neurosci Lett. 1998;248(1):49–52. doi:10.1016/s0304-3940(98)00331-0
11. Richmond FJ, Johnston WS, Baker RS, Steinbach MJ. Palisade endings in human extraocular muscles. Invest Ophthalmol Vis Sci. 1984;25(4):471–476.
12. Ruskell GL. The fine structure of innervated myotendinous cylinders in extraocular muscles of rhesus monkeys. J Neurocytol. 1978;7(6):693–708. doi:10.1007/BF01205145
13. Lukas J-R, Blumer R, Denk M, Baumgartner I, Neuhuber W, Mayr R. Innervated myotendinous cylinders in human extraocular muscles. Invest Ophthalmol Vis Sci. 2000;41(9):2422–2431.
14. Land MF. Eye movements of vertebrates and their relation to eye form and function. J Comp Physiol A. 2015;201(2):195–214. doi:10.1007/s00359-014-0964-5
15. Blumer R, Maurer-Gesek B, Gesslbauer B, et al. Palisade endings are a constant feature in the extraocular muscles of frontal-eyed, but not lateral-eyed, animals. Invest Ophthalmol Vis Sci. 2016;57(2):320–331. doi:10.1167/iovs.15-18716
16. Bruenech R, Ruskell GL. Myotendinous nerve endings in human infant and adult extraocular muscles. Anat Rec. 2000;260(2):132–140. doi:10.1002/1097-0185(20001001)260:2<132::AID-AR30>3.0.CO;2-H
17. Blumer R, Streicher J, Davis-López de Carrizosa MA, de la Cruz RR, Pastor AM. Palisade endings of extraocular muscles develop postnatally following different time courses. Invest Ophthalmol Vis Sci. 2017;58(12):5105–5121. doi:10.1167/iovs.17-22643
18. Eberhorn AC, Horn AK, Eberhorn N, Fischer P, Boergen KP, Büttner-Ennever JA. Palisade endings in extraocular eye muscles revealed by SNAP-25 immunoreactivity. J Anat. 2005;206(3):307–315. doi:10.1111/j.1469-7580.2005.00378.x
19. Lienbacher K, Mustari M, Ying HS, Büttner-Ennever JA, Horn AKE. Do palisade endings in extraocular muscles arise from neurons in the motor nuclei? Invest Ophthalmol Vis Sci. 2011;52(5):2510–2519. doi:10.1167/iovs.10-6008
20. Demer JL. Current concepts of mechanical and neural factors in ocular motility. Curr Opin Neurol. 2006;19(1):4.
21. Demer JL, Oh SY, Poukens V. Evidence for active control of rectus extraocular muscle pulleys. Invest Ophthalmol Vis Sci. 2000;41(6):1280–1290.
22. Ruskell GL, Kjellevold Haugen I-B, Bruenech JR, Van Der Werf F. Double insertions of extraocular rectus muscles in humans and the pulley theory. J Anat. 2005;206(3):295–306. doi:10.1111/j.1469-7580.2005.00383.x
23. Büttner-Ennever JA, Eberhorn A, Horn AK. Motor and sensory innervation of extraocular eye muscles. Ann N Y Acad Sci. 2003;1004:40–49. doi:10.1111/j.1749-6632.2003.tb00240.x
24. Ruskell GL. The fine structure of human extraocular muscle spindles and their potential proprioceptive capacity. J Anat. 1989;167:199–214.
25. Bruenech JR, Ruskell GL. Muscle spindles in extraocular muscles of human infants. Cells Tissues Organs. 2001;169(4):388–394. doi:10.1159/000047906
26. Corsi M, Sodi A, Salvi G, Faussone-Pellegrini MS. Morphological study of extraocular muscle proprioceptor alterations in congenital strabismus. Ophthalmologica. 1990;200(3):154–163. doi:10.1159/000310097
27. Li J, Shen C. Histological and ultrastructural studies of extraocular muscle proprioceptor in concomitant strabismus. Zhonghua Yan Ke Za Zhi. 2001;37(3):200–202.
28. Park S-E, Sa H-S, Oh S. Innervated myotendinous cylinders alterations in human extraocular muscles in patients with strabismus. Korean J Ophthalmol. 2009;23:93–99. doi:10.3341/kjo.2009.23.2.93
29. Kampanartsanyakorn S, Surachatkumtonekul T, Dulayajinda D, Jumroendararasmee M, Tongsae S. The outcomes of horizontal strabismus surgery and influencing factors of the surgical success. J Med Assoc Thai. 2005;88(Suppl 9):S94–S99.
30. Twelker JD, Mutti DO. Retinoscopy in infants using a near noncycloplegic technique, cycloplegia with tropicamide 1%, and cycloplegia with cyclopentolate 1%. Optom Vis Sci. 2001;78(4):215–222. doi:10.1097/00006324-200104000-00010
31. Yazdani N, Sadeghi R, Momeni-Moghaddam H, Zarifmahmoudi L, Ehsaei A. Comparison of cyclopentolate versus tropicamide cycloplegia: a systematic review and meta-analysis. J Optom. 2018;11(3):135–143. doi:10.1016/j.optom.2017.09.001
32. Wan MJ, Chiu H, Shah AS, Hunter DG. Long-term surgical outcomes for large-angle infantile esotropia. Am J Ophthalmol. 2018;189:155–159. doi:10.1016/j.ajo.2017.11.006
33. Chen Y-W, Lin S-A, Lin P-W, Huang H-M. The difference of surgical outcomes between manifest exotropia and esotropia. Int Ophthalmol. 2019;39(7):1427–1436. doi:10.1007/s10792-018-0956-5
34. Parks M, Mitchell P, Wheeler M, Tasman W, Jaeger E. Duane’s Foundations of Clinical Ophthalmology. Lippincott Williams & Wilkins; 2002.
35. ElFekih L, Lajmi H, Ben Yakhlef A. Indications and results of exotropia surgical management. Tunis Med. 2021;99(5):569–574.
36. Beauchamp GR, Black BC, Coats DK, et al. The management of strabismus in adults--I. Clinical characteristics and treatment. J Aapos. 2003;7(4):233–240. doi:10.1016/s1091-8531(03)00112-5
37. Kassem RR, Badr RAA, Al Zarea BKA, et al. Botulinum toxin injection in horizontal rectus muscles without electromyography using an open sky versus a closed sky technique. J Pediatr Ophthalmol Strabismus. 2022;59(6):388–395. doi:10.3928/01913913-20220210-03
38. Mohamed Abdel-Moneim El-Mofty R, Kassem RR, Abdel-Salam LO. Histopathological changes in extraocular muscles of rabbits following injection of bupivacaine 5mg/Ml versus 7.5mg/Ml. Cutan Ocul Toxicol. 2022;41(3):210–214. doi:10.1080/15569527.2022.2066113
39. Dengis CA, Steinbach MJ, Kraft SP. Registered eye position: short- and long-term effects of botulinum toxin injected into eye muscle. Exp Brain Res. 1998;119(4):475–482. doi:10.1007/s002210050363
40. Suh YW, Uhm CS, Cho YA. Ultrastructural changes in myotendinous nerve endings induced by injection of botulinum toxin into the extraocular muscle. Graefes Arch Clin Exp Ophthalmol. 2010;248(12):1795–1801. doi:10.1007/s00417-010-1513-8
41. Bohlen MO, Warren S, Mustari MJ, May PJ. Examination of feline extraocular motoneuron pools as a function of muscle fiber innervation type and muscle layer. J Comp Neurol. 2017;525(4):919–935. doi:10.1002/cne.24111
42. Demer JL. Compartmentalization of extraocular muscle function. Eye. 2015;29(2):157–162. doi:10.1038/eye.2014.246
43. Demer JL, Miller JM, Poukens V. Surgical implications of the rectus extraocular muscle pulleys. J Pediatr Ophthalmol Strabismus. 1996;33(4):208–218. doi:10.3928/0191-3913-19960701-03
44. Demer JL, Miller JM, Poukens V, Vinters HV, Glasgow BJ. Evidence for fibromuscular pulleys of the recti extraocular muscles. Invest Ophthalmol Vis Sci. 1995;36(6):1125–1136.
45. Athavale SA, Kotgirwar S, Lalwani R. Rectus and oblique muscles of eyeball: a morphometric study of Indian population. Anat Cell Biol. 2015;48:201–204. doi:10.5115/acb.2015.48.3.201
46. Flügel-Koch C, Neuhuber WL, Kaufman PL, Lütjen-Drecoll E. Morphologic indication for proprioception in the human ciliary muscle. Invest Ophthalmol Vis Sci. 2009;50(12):5529–5536. doi:10.1167/iovs.09-3783
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.