Back to Journals » International Journal of General Medicine » Volume 15
Does Serum Osteocalcin Level Affect Carotid Atherosclerosis in Post-Menopausal Diabetic Females? A Case-Control Study
Authors Naguib M ![]() , Ali N, ElSaraf N, Rashed L, Azzam H
, Ali N, ElSaraf N, Rashed L, Azzam H
Received 10 December 2021
Accepted for publication 11 April 2022
Published 28 April 2022 Volume 2022:15 Pages 4513—4523
DOI https://doi.org/10.2147/IJGM.S353492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mervat Naguib,1 Nadia Ali,2 Nashwa ElSaraf,3 Lila Rashed,4 Hebatoallah Azzam5
1Diabetes and Endocrinology Unite, Internal Medicine Department, Faculty of Medicine Kasr Al-Ainy Hospital Cairo University, Cairo, Egypt; 2Internal Medicine Department, Ahmed Maher Hospital, Cairo, Egypt; 3Internal Medicine Department, Faculty of Medicine Kasr Al-Ainy Hospital Cairo University, Cairo, Egypt; 4Department of Biochemistry, Faculty of Medicine Cairo University, Cairo, Egypt; 5Radiology Department, Faculty of Medicine Kasr Al-Ainy Hospital Cairo University, Cairo, Egypt
Correspondence: Mervat Naguib, Diabetes and Endocrinology Unite, Internal Medicine Department, Kasr Al-Ainy Hospital Cairo University, 41 Manial Street, Cairo, 11451, Egypt, Tel +202/23641088, Email [email protected]
Purpose: To determine the association between serum osteocalcin and carotid intima media thickness (CIMT) in a group of post-menopausal females with type 2 diabetes (T2DM).
Patients and Methods: This cross-sectional study enrolled 75 postmenopausal women with T2DM and 40 age matched postmenopausal healthy females. Age, body mass index, blood pressure were recorded for all subjects. Laboratory tests including fasting blood glucose (FBG), glycated hemoglobin (HbA1c) and lipid profile were measured. Serum osteocalcin was measured using ELISA. Bone mineral density (BMD) was measured by DEXA scan. CIMT was assessed with B-mode ultrasonography.
Results: Patients with T2DM had significantly lower serum osteocalcin compared to control (63.73± 27.20 vs 136.16± 21.96 pg/mL, P< 0.001). Patients with osteoporosis had significantly lower osteocalcin level compared to those with normal BMD. Patients with T2DM had a significant negative correlation between serum osteocalcin and CIMT (r= − 0.332; P=0.003), FBG (r= − 0.732; P< 0.001), HbA1c (r=− 0.672; P< 0.001), and HOMA-IR (r= − 0.672; P< 0.001). However, multiple linear regression analysis revealed that CIMT in patients with diabetes was only significantly associated with age (P= 0.001), duration of diabetes (P< 0.001), SBP (P< 0.001), HOMA-IR (P=0.033), LDL (P=0.005), and HDL (P< 0.001). Furthermore, serum insulin (β= − 0.183, P=0.033), FBG (β= − 0.604, P< 0.001) and LDL (β= − 0.195, P= 0.02) were independently negatively correlated with serum osteocalcin.
Conclusion: In this study, Postmenopausal women with diabetes had significantly lower osteocalcin compared to non-diabetic women. Although serum osteocalcin was negatively correlated with CIMT, multivariate regression analysis revealed that osteocalcin level was only independently related to worse glycemic parameters in postmenopausal women with T2DM.
Keywords: osteocalcin, diabetes, atherosclerosis, glycated hemoglobin, lipid
Introduction
Diabetes is a major risk factor for atherosclerosis. Postmenopausal females with diabetes have triple the risk of developing cardiovascular (CVD) or cerebrovascular disease than healthy women.1 In addition, women with diabetes have a fourfold rise in the risk of death from acute coronary syndrome than diabetic men.2 The etiology of this excess cardiovascular morbidity and mortality is not completely clear. Although hyperglycemia has a major role in the development of atherosclerosis, there are other contributors involved in the pathogenesis of the cardiovascular diseases in patients with diabetes.3 The population-based studies showed that inflammation, oxidative stress and impaired antioxidant levels are major factors involved in atherosclerosis development in elderly patients with metabolic syndrome or any of its component.4
Osteoporosis is the second world wide health problem after CVD, and it is expected to increase as there is increase in the number of the elderly population.5 Relationship between type 2 diabetes mellitus (T2DM) and bone mineral density (BMD) has been debatable. While some studies showed reduced BMD others reported unchanged or increased BMD in patients with diabetes.6–8 In spite of higher BMD in patients with T2DM, they have increased susceptibility to fracture caused by increased risk of falls associated with the presence of neurovascular complications and the changes in their bone quality.9
Many previous studies have demonstrated that patients with osteoporosis are at significantly greater risk of developing CVD and more severe atherosclerosis and vascular calcification.10 The association between these two diseases could be related to the common risk factors involved in osteoporosis and vascular diseases, such as dyslipidemia, hypertension, and diabetes mellitus.11 However, the studies investigated the pathophysiologic relationship between cardiovascular risk factors and bone metabolism, bone mass have shown inconclusive and contradictory results. Bone is a highly vascular structure and there is molecular interaction between endothelial cells and bone cells.10,11 Angiogenesis plays a major role in bone fracture healing and repair and changes in the local vasculature are associated with the progression of osteoporosis.12,13 Also, there is increasing number of bone secreted osteokines that influence energy balance and glucose metabolism that could be involved in the pathogenesis of CVD.14
Osteocalcin (OCN) an osteoblast secreted protein is made up of 49 amino acids.15 Previous animal studies found that there is association between OCN and metabolic functions, including glucose and lipid metabolism via stimulation of beta cell proliferation and induction of adiponectin secretion.15 However, human studies from different populations revealed conflicting results. One study of patients with uncontrolled T2DM found that patients with T2DM had significantly lower levels of OCN compared to age-matched subjects without diabetes.16 However; another study revealed no association between serum OCN and the risk of development of diabetes among both women and men.17 So, the relationship of serum OCN and glucose homeostasis in patients with T2DM needs further evaluation in different populations.
Also, The association between serum OCN and atherosclerosis is conflicting and unclear.18 A study of Japanese men and postmenopausal women with T2DM reported significant negative correlation between serum OCN and carotid intima media thickness (CIMT) in men; on the other hand, there was no significant association between OCN and the atherosclerosis indices in postmenopausal women.19 However, a study of Chinese population found that serum OCN level in both men and post-menopausal women with T2DM was an independent risk factor for carotid atherosclerosis.20
Specific markers could be beneficial as indicators in the prevention and treatment approach of atherosclerosis in patients with diabetes. Based on the aforementioned observations, whether serum OCN could be a marker of atherosclerosis in different ethnic populations needs further evaluation. The aim of the current study was to investigate the association between serum levels of OCN and glycemic and lipid parameters and CIMT in a group of Egyptian post-menopausal females with T2DM.
Materials and Methods
Study Design
This study was a cross-sectional study performed in a tertiary care referral hospital between February 2019 and January 2020. We assigned 115 postmenopausal females included, 75 patients with T2DM and 40 healthy post-menopausal controls. Patients were recruited from the diabetic center, Kasr Al Ainy Hospital, Cairo, Egypt. The control subjects were collected from healthy postmenopausal volunteers. All subjects provided informed consent to participate in this study. The study protocol and procedures follow the ethical guidelines of the 1975 Declaration of Helsinki and has been approved by ethical committee of Kasr Al-Ainy Hospital, Faculty of Medicine, Cairo University (no.I-170316).
Patients with diagnosis of T2DM based on ADA criteria were eligible for inclusion in this study. Exclusion criteria included patients with 1) diabetes other than T2DM; 2) history of hepatic or renal diseases; 3) history of hyperparathyroidism; 4) therapy with corticosteroid, vitamin D supplementation, or antiresorptive agents. Clinical data obtained included age, body mass index (BMI) [weight (kg)/height (m2)], systolic blood pressure (SBP), diastolic blood pressure (DBP) and duration of diabetes. Blood samples were collected from each participant after a period of 10 hours fasting for measurement of fasting blood glucose (FBG), glycated hemoglobin (HbA1c), serum creatinine, total cholesterol (TC), high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides (TG), serum insulin, total serum calcium, phosphate and serum OCN. HOMA-IR was calculated according to the formula: [glucose (nmol/L) x insulin (µU/mL)/22.5], using fasting values.21
OCN Assay Principle
Serum OCN was measured using ELISA kit based on OCN antibody-OCN antigen interactions (immunosorbency) and a Horseradish Peroxidase (HRP) colorimetric detection system to detect OCN antigen targets in samples according to manufacturer’s instructions (Cusabio Biotech Co, Ltd, Houston, TX, USA). Samples were collected in EDTA tubes; centrifugation was performed for 15 minutes at 1000 × g at 2–8°C within 30 minutes of collection and samples stored at −80°C. Absorbance measurements were carried out in a microplate reader at 450 nm and the concentrations were calculated using a standard curve. The minimum detectable dose of human OCN is typically less than 7.8 pg/mL.
CIMT Measurement
To assess CIMT we used B-mode duplex ultrasound modality. Carotid examination was done using a high frequency 7.5 MHz linear probe of an ATL-HDL 5000 machine by two experienced physician blinded to the clinical condition of the participant. Linear scanning of the right and left carotid arteries was performed. CIMT was defined as the distance between intima-lumen line and media-adventitia border.Three dimensions were taken from the anterior and posterior walls of the common carotid artery, the carotid bifurcation, and the extracranial portion of the internal carotid artery. The average of both sides was calculated.22
BMD Measurement
We measured the BMD of the lumbar spine and the total hip using a Prodigy DEXA (GE Healthcare, Madison, WI, USA) calibrated daily using a standard phantom provided by the manufacturer. Patients were classified into 3 groups based on their BMD value: (1) patients with normal BMD if the T-score is equal to or greater than -1, (2) patients with osteoporosis if the T-score is equal to or below -2.5, and (3) patients with osteopenia if the T-score is below −1.0 and above −2.5.
Statistical Analysis
Data were coded and entered using the statistical package (SPSS) version 23 (IBM Corp., Chicago, IL). Measurement data are presented as mean and standard deviation for quantitative variables and number and percentage for qualitative variables. Comparisons between groups were done using analysis of variance (ANOVA) with multiple comparisons post hoc test in normally distributed quantitative variables while non-parametric Kruskal–Wallis test and Mann–Whitney test were used for non-normally distributed quantitative variables. Correlations between quantitative variables were done using Pearson correlation coefficient. Data tested for normality and proved to be normally distributed. Then, stepwise regression for selection of independent determinants of OCN and CIMT in cases was performed. Potential confounding variables including age, duration of diabetes, SBP, DBP, BMI, creatinine, calcium, phosphate, CIMT, BMD, TC, TG, HDL, LDL, s.insulin, FBG, HBA1c, HOMA-IR were controlled in the regression models. The interaction of confounding variables was assessed. R-squared was measured to test how close the data are to the fitted regression line.
Results
Clinical, Laboratory, Imaging Measurements of the Study Subjects
This study enrolled 115 postmenopausal women (75 with diabetes and 40 without). Both women with and without diabetes had obesity-related BMIs of 32.18±4.1 and 32.46±6.02 kg/m2, respectively. The mean SBP was significantly higher in females with diabetes (138.4±17.6 mmHg) than control subjects (129.38±9.49 mmHg). In females with T2DM the mean duration of diabetes was 12.25±8.26 years and most of them had good glycemic control with the mean HbA1c was (6.4%; 46 mmol /mol). Patients with T2DM had diabetic dyslipidemia with significantly elevated TG and lower HDL than control subjects. Serum level of OCN was significantly lower in patients with diabetes compared to non-diabetic women (63.73±27.20 vs 136.16±21.96 pg/mL; P<0.001). There were no significant differences in serum calcium, serum phosphate, lumber BMD, and hip BMD between postmenopausal women with diabetes and controls (Table 1).
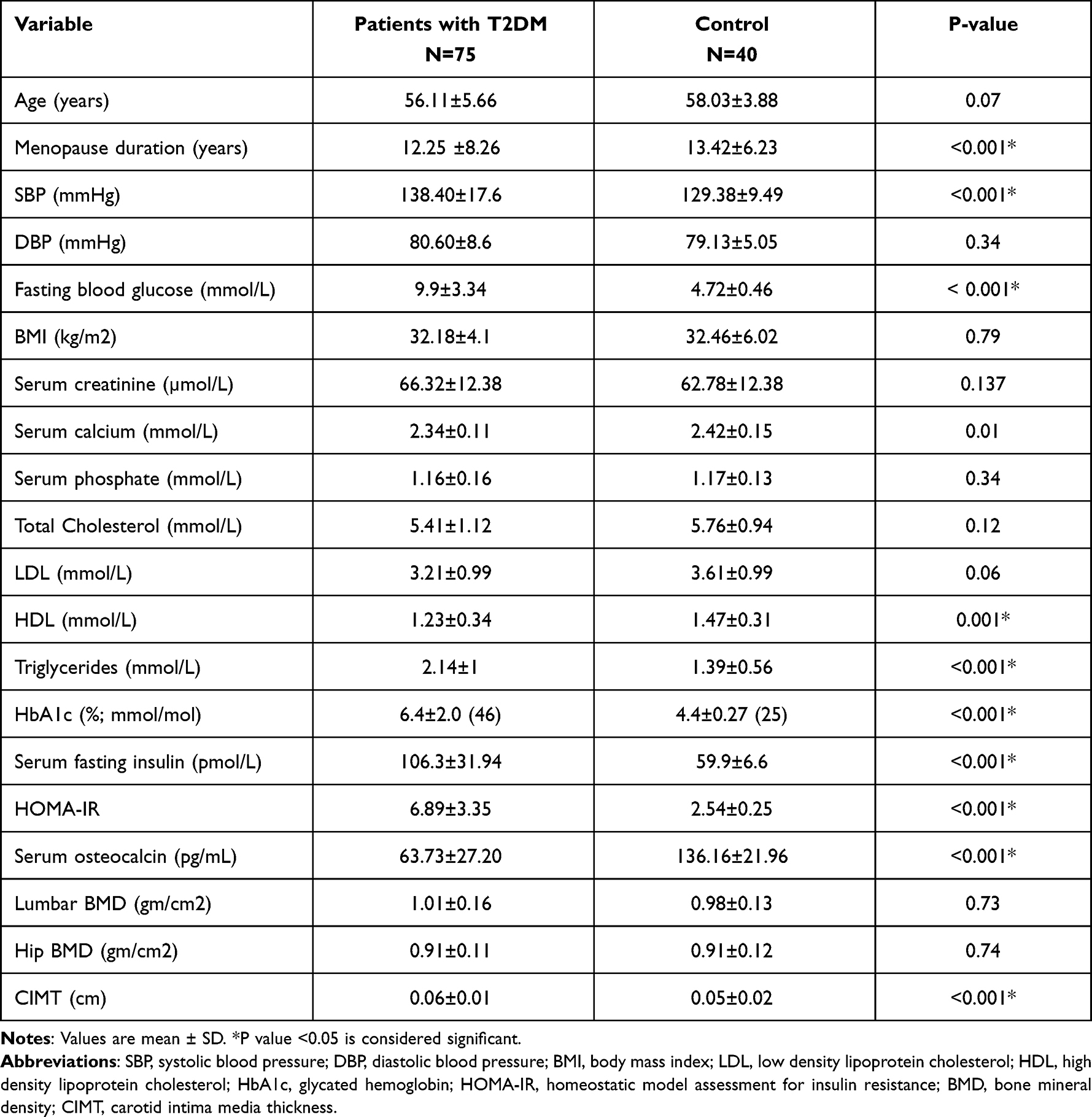 |
Table 1 Clinical, Laboratory, and Imaging Measurements of Postmenopausal Females with T2DM and Control Women |
Comparison of Clinical, Laboratory, Imaging Data of Diabetic Patients with Normal BMD, Osteopenia and Osteoporosis
Diabetic patients with osteoporosis had highest insulin resistance with mean HOMA-IR (9.01±3.35) compared to patients with normal BMD (4.96±2.80) and those with osteopenia (6.57±3.04) (P< 0.001). Also, patients with osteoporosis had significantly higher HbA1c and TG levels compared to those with osteopenia and normal BMD (P < 0.001 and P=0.006; respectively). Although, CIMT was higher in patients with osteoporosis (0.07±0.01 cm) compared to those with osteopenia (0.06±0.01 cm), the difference was not statistically significant (P=0.211). The lowest OCN level was found in women with osteoporosis (57.04±26.00 pg/mL), followed by patients with osteopenia (63.92±28.55 pg/mL), whereas patients with normal BMD had the highest OCN level (75.46±23.99 pg/mL) (P=0.048) (Table 2).
 |
Table 2 Comparison of Clinical, Laboratory, and Imaging Parameter of Diabetic Patients with Normal BMD, Osteopenia and Osteoporosis |
Correlation Between Serum OCN Level and Different Variables in Patients with T2DM
OCN level was significantly negatively correlated with age (r = −0.314; P=0.005), FBG (r = −0.732; P< 0.001), HbA1c (r = −0.672; P< 0.001) (Figure 1), HOMA-IR (r = −0.611; P< 0.001) but positively correlated to hip BMD (r= 0.318; P=0.005) (Table 3). However, no statistically significant correlation was observed between the serum OCN and the duration of diabetes (r= −0.097; P=0.400), BMI (r= −0.051; P=0.659), LDL (r= −0.159; P= 0.164) HDL (r= 0.004; P=0.973), or TG (r= −0.131; P=0.252) (Table 3)
 |
Table 3 Correlation Analysis Between Serum Osteocalcin and Different Variables in Postmenopausal Females with Diabetes |
 |
Figure 1 Correlation analysis of serum osteocalcin level and glycated hemoglobin (HbA1c) in postmenopausal females with T2DM revealed significant negative correlation (r = −0.672; P<0.001). |
Multivariate Linear Regression to Detect Independent Parameters Associated with OCN Level in Postmenopausal Females with T2DM
To adjust the potential confounding factors, we incorporated these factors into multivariate regression analysis which revealed that osteocalcin level was only independently related to FBG (β= −0.604, 95% confidence interval [CI] −0.342 to −0.193; P< 0.001), s.insulin (β= −0.183, 95% CI −2.079 to −0.087; P=0.033) and LDL (β= −0.195, 95% CI −0.247 to −0.022; P=0.020).
CIMT in Postmenopausal Women with T2DM and Its Relation to Different Variables
CIMT was significantly higher in females with diabetes compared to control (0.06±0.01 vs 0.05±0.02 cm; P<0.001). CIMT was not significantly different in diabetic females with normal BMD (0.06±0.02 cm), osteopenia (0.06±0.01 cm) and osteoporosis (0.07±0.01) (P=0.211). In women with diabetes, CIMT was positively correlated to age (r= 0.455; P< 0.001), diabetes duration (r=0.370; P=0.001), SBP (r=0.559; P< 0.001), BMI (r=−0.239; P=0.035), LDL (r=0.389; P< 0.001), HbA1c (r= 0.334, P=0.003), HOMA-IR (r=0.422; P< 0.001) but negatively correlated to OCN level (r = −0.332; P=0.001) (Figure 2). However, Multiple linear regression analysis indicated that CIMT in patients with diabetes was only significantly associated with age (β= 0.264, 95% confidence interval [CI] 0.001 to 0.001; P= 0.001), duration of diabetes (β= 0.446, 95% CI 0.001 to 0.001; P< 0.001), SBP (β= 0.400, 95% CI 0.001 to 0.001; P< 0.001), HOMA-IR (β= 0.250, 95% CI 0.001 to 0.001; P=0.033), LDL (β= 0.194, 95% CI 0.001 to 0.001; P=0.005), and HDL (β= −0.282, 95% CI 0.001 to 0.001; P< 0.001).
 |
Figure 2 Correlation analysis of serum osteocalcin level and carotid intima media thickness (CIMT) in postmenopausal females with T2DM showed significant negative correlation (r = −0.332; P=0.003). |
Discussion
This study showed that compared to postmenopausal women without diabetes, postmenopausal women with diabetes had significantly lower serum OCN levels. A recent study also demonstrated lower levels of OCN in T2DM patients than healthy subjects.23 Similar results have been observed in postmenopausal females with T2DM.24 Both in vivo and in vitro studies have indicated that OCN could have a role in lowering blood sugar, promoting insulin synthesis from pancreatic beta cells.24,25 Furthermore, OCN was found to promote energy expenditure and insulin sensitivity by increasing mitochondrial function in skeletal muscles and promoting adiponectin secretion from adipose tissue and decreasing lipid accumulation in the liver.26,27
In our study, serum OCN level had significant negative correlation with FBG, HbA1c and HOMA-IR in postmenopausal women with T2DM. Kanazawa et al reported the same results in post-menopausal women and men with T2DM.19 Moreover, Wang et al found that serum OCN levels were low in poorly controlled diabetic patients and became elevated after treatment.28 In our study, we found that patients without osteoporosis had better glycemic control than those with osteoporosis. It is possible that hyperglycemia might affect osteoblast maturation, which then results in a decrease in bone formation and OCN levels.29 Also, OCN could be glycated causing elevation of serum level of OCN in the presence of hyperglycemia.30 Lastly, hyperglycemia could suppress OCN gene expression in osteoblast leading to reduction of OCN level in patients with poor glycemic control.29 However, the results are not constant among different populations, while some studies in Caucasian and Asian populations showed that OCN level has a negative association with blood glucose, serum insulin, and HOMA-IR,31,32 studies in other populations found that OCN was not related to HOMA-IR.33,34 This difference could be related to the differences in age, gender, ethnicity, and genetic back ground of the studied populations.
Diabetes alters bone metabolism and BMD may differ in patients with diabetes and healthy subjects.6–8 Similar to our findings Asokan et al reported unaltered BMD in patients with T2DM.7 In contrast, Schwartz et al reported higher BMD in patients with diabetes with, paradoxically, higher increase in risk of fracture.35 Serum OCN reflects osteoblast function and it has been a good marker of bone formation for long time. Serum OCN levels were found to be significantly lower in patients with diabetes and osteoporosis, osteopenia, or normal bone density compared to healthy controls, furthermore, in all these groups, OCN levels were positively correlated with BMD.36 In the current study, OCN levels were significantly lower in patients with osteoporosis than in patients with normal BMD and were significantly associated with BMD in women with diabetes. However, when multiple linear regression was applied, serum OCN was only associated with blood glucose, and there was no significant association between OCN and BMD. This observation suggests that serum OCN may be influenced by blood glucose levels and may not be a good marker of bone formation in poorly controlled diabetic patients.
Previous studies showed that BMI had a positive correlation to insulin secretion in subjects with diabetes, which could reflect compensatory stimulation of insulin secretion associated with insulin resistance.37,38 Dumitru et al reported that serum OCN was lower in post-menopausal diabetic females compared to those without diabetes with no significant associations between OCN and BMI or any of metabolic parameters.39 Similar results were obtained in Japanese individuals with diabetes.40 Interestingly, in our study OCN was not correlated with BMI and multivariate regression showed that OCN was only significantly and negatively associated with FBG and s.insulin. These results suggest that OCN might have an important effect on insulin secretion than on insulin sensitivity in diabetic individuals.
One study reported significant negative correlation between LDL and TG and OCN level in patients with diabetes.20 However, another study failed to find any association between serum OCN and lipid profiles in Chinese patients with T2DM, although there was negative association between OCN and HbA1c.41 In our study, multivariate analysis showed significant negative correlation between serum OCN and LDL in diabetic patients.
The incidence of cardiovascular disease is higher in patients with osteoporosis.10 BMD and bone formation biomarkers were found to be low in patients with peripheral arterial atherosclerosis.42 Furthermore, in a recent meta-analysis including 10,300 patients the incidence of any atherosclerotic cardiovascular disease was significantly higher in individuals with osteoporosis compared to those without.43 Our results also showed a significant negative correlation between OCN, the bone formation biomarker, and CIMT in patients with diabetes. The pathophysiologic link between atherosclerosis and osteoporosis involves multiple mechanisms such as inflammatory factors, different adipokines such as adiponectin and resistin, and factors involved in bone metabolism.44 In agreement with our results, a study of a group of Chinese population revealed that serum OCN was significantly lower in patients with history of cardiovascular disease than those without CVD.45 Also, in a group of patients with metabolic syndrome with normal glucose tolerance serum OCN decreased significantly in patients with coronary artery disease compared to those without and showed an independent correlation with severity of coronary atherosclerosis.46 Recently, Riquelme-Gallego et al reported an inverse relationship between OCN levels and cardiovascular risk in patients with metabolic syndrome without T2DM.47
However, it’s not clear whether the relation of OCN level and atherosclerosis is a direct relationship or it’s associated with the impact of OCN on conventional cardiovascular risk factors. Whereas one study of patients with T2DM found that low serum OCN was a risk factor for carotid atherosclerosis independent of HbA1c, HOMA-IR and BMI,20 another study of Japanese population reported that OCN considerably and negatively correlate with CIMT once adjustment for different cardiovascular risk factors in men but not in women.19 Contrary to this data, a cross-sectional study of Korean subjects showed that increased level of serum OCN was related to coronary atherosclerosis.48
To find out the determinants of CIMT and serum OCN level we performed multivariate linear regression analysis and it showed that serum CIMT in patients with diabetes was only significantly associated with age, duration of diabetes, SBP, HOMA-IR and atherogenic lipid, but not associated OCN level. On the other hand, OCN was only significantly negatively associated with FBG, serum insulin and LDL. These findings suggest that, in menopausal women with diabetes, the blood glucose level is the most important determinant of OCN level, and that the inverse relationship between OCN and CIMT could be attributed to OCN and blood glucose interaction. Second, blood glucose levels can impact serum OCN, hence its use as a bone formation marker in diabetic individuals should be interpreted cautiously.
Nonetheless, these results must be interpreted with caution and a number of limitations should be borne in mind. First, this study was a cross-sectional observational study. Prospective longitudinal studies are needed to ascertain causality between OCN and different parameters. Second, this study included patients on variable medications, requiring further studies to determine the effects of different medications. Third, the relatively small sample size because of financial issues that limits the generalization of these results. Fourth, we did not measure undercarboxylated osteocalcin (ucOC). Although, there are reports that ucOC, but not carboxylated osteocalcin, is responsible for the metabolic actions of osteocalcin,25,49 Hill et al assessed the direct effect of ucOC and carboxylated OCN in cell culture systems and found that both carboxylated and uncarboxylated osteocalcin directly increase glucose transport in adipocytes and myocytes, while suppressing proinflammatory cytokine secretion and stimulating interleukin 10 and adiponectin release.50
Conclusion
In menopausal women with diabetes we found that lower serum osteocalcin levels were associated mainly with higher blood glucose and higher insulin levels. Moreover, there was a negative correlation between OCN and CIMT, however CIMT was only independently associated with conventional cardiovascular risk factors.
Acknowledgments
All authors acknowledge their gratitude to the staff members of diabetes unite for their help and support. The abstract of this paper was presented as an oral presentation [AACE Communities MENA Conference] with interim findings. The oral presentation was published in “oral presentation” in [AACE Endocrine Practice: https://doi.org/10.1016/j.eprac.2021.11.075].
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Madonna R, Balistreri CR, De Rosa S, et al. Impact of sex differences and diabetes on coronary atherosclerosis and ischemic heart disease. J Clin Med. 2019;8(1):98. doi:10.3390/jcm8010098
2. Leon BM, Maddox TM. Diabetes and cardiovascular disease: epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015;6(13):1246–1258. doi:10.4239/wjd.v6.i13.1246
3. Muhlestein JB, Anderson JL, Horne BD, et al. Effect of fasting glucose levels on mortality rate in patients with and without diabetes mellitus and coronary artery disease undergoing percutaneous coronary intervention. Am Heart J. 2003;146(2):351–358. doi:10.1016/S0002-8703(03)00235-7
4. Dziegielewska-Gesiak S. Metabolic syndrome in an aging society - role of oxidant-antioxidant imbalance and inflammation markers in disentangling atherosclerosis. Clin Interv Aging. 2021;16:1057–1070. doi:10.2147/CIA.S306982
5. Stojanovic OI, Lazovic M, Lazovic M, Vuceljic M. Association between atherosclerosis and osteoporosis, the role of vitamin D. Arch Med Sci. 2011;7(2):179–188. doi:10.5114/aoms.2011.22066
6. Farhat GN, Cauley JA. The link between osteoporosis and cardiovascular disease. Clin Cases Miner Bone Metab. 2008;5(1):19–34.
7. Asokan AG, Jaganathan J, Philip R, Soman RR, Sebastian ST, Pullishery F. Evaluation of bone mineral density among type 2 diabetes mellitus patients in South Karnataka. J Nat Sci Biol Med. 2017;8(1):94–98. doi:10.4103/0976-9668.198363
8. Valderrábano RJ, Linares MI. Diabetes mellitus and bone health: epidemiology, etiology and implications for fracture risk stratification. Clin Diabetes Endocrinol. 2018;4:9. doi:10.1186/s40842-018-0060-9
9. Reyes RR, Moreno PR, Torres MM. Enfermedad cardiovascular, diabetes mellitus tipo 2 y osteoporosis. Rev Osteoporos Metab Miner. 2010;2(2):47–54.
10. Danilevicius CF, Lopes JB, Pereira RM. Bone metabolism and vascular calcification. Braz J Med Biol Res. 2007;40(4):435–442. doi:10.1590/s0100-879x2007000400001
11. Xu H, Wang Z, Li X, et al. Osteoporosis and osteopenia among patients with type 2 diabetes aged ≥50: role of sex and clinical characteristics. J Clin Densitom. 2020;23(1):29–36. doi:10.1016/j.jocd.2019.04.004
12. Beamer B, Hettrich C, Lane J. Vascular endothelial growth factor: an essential component of angiogenesis and fracture healing. HSS J. 2010;6(1):85–94. doi:10.1007/s11420-009-9129-4
13. Carulli C, Innocenti M, Brandi ML. Bone vascularization in normal and disease conditions. Front Endocrinol (Lausanne). 2013;4:106. doi:10.3389/fendo.2013.00106
14. Liu DM, Mosialou I, Liu JM. Bone: another potential target to treat, prevent and predict diabetes. Diabetes Obes Metab. 2018;20(8):1817–1828. doi:10.1111/dom.13330
15. Lee NK, Sowa H, Hinoi E, et al. Endocrine regulation of energy metabolism by the skeleton. Cell. 2007;130(3):456–469. doi:10.1016/j.cell.2007.05.047
16. Achemlal L, Tellal S, Rkiouak F, et al. Bone metabolism in male patients with type 2 diabetes. Clin Rheumatol. 2005;24(5):493–496. doi:10.1007/s10067-004-1070-9
17. Zwakenberg SR, Gundberg CM, Spijkerman AM, van der A DL, van der Schouw YT, Beulens JW. Osteocalcin is not associated with the risk of type 2 diabetes: findings from the EPIC-NL Study. PLoS One. 2015;10(9):e0138693. doi:10.1371/journal.pone.0138693
18. Tacey A, Qaradakhi T, Brennan-Speranza T, Hayes A, Zulli A, Levinger I. Potential role for osteocalcin in the development of atherosclerosis and blood vessel disease. Nutrients. 2018;10(10):1426. doi:10.3390/nu10101426
19. Kanazawa I, Yamaguchi T, Yamamoto M, et al. Serum osteocalcin level is associated with glucose metabolism and atherosclerosis parameters in type 2 diabetes mellitus. J Clin Endocrinol Metab. 2009;94(1):45–49. doi:10.1210/jc.2008-1455
20. Sheng L, Cao W, Cha B, Chen Z, Wang F, Liu J. Serum osteocalcin level and its association with carotid atherosclerosis in patients with type 2 diabetes. Cardiovasc Diabetol. 2013;12:22. doi:10.1186/1475-2840-12-22
21. Salgado AL, Carvalho L, Oliveira AC, Santos VN, Vieira JG, Parise ER. Insulin resistance index (HOMA-IR) in the differentiation of patients with non-alcoholic fatty liver disease and healthy individuals. Arq Gastroenterol. 2010;47(2):165–169. doi:10.1590/s0004-28032010000200009
22. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim. Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011). Cerebrovasc Dis. 2012;34:290–296. doi:10.1159/000343145
23. Sanchez-Enriquez S, Ballesteros-Gonzalez IT, Villafán-Bernal JR, et al. Serum levels of undercarboxylated osteocalcin are related to cardiovascular risk factors in patients with type 2 diabetes mellitus and healthy subjects. World J Diabetes. 2017;8(1):11–17. doi:10.4239/wjd.v8.i1.11
24. Im JA, Yu BP, Jeon JY, Kim SH. Relationship between osteocalcin and glucose metabolism in postmenopausal women. Clin Chim Acta. 2008;396(1–2):66–69. doi:10.1016/j.cca.2008.07.001
25. Ferron M, Hinoi E, Karsenty G, Ducy P. Osteocalcin differentially regulates beta cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc Natl Acad Sci U S A. 2008;105(13):5266–5270. doi:10.1073/pnas.0711119105
26. Fernandes TAP, Gonçalves LML, Brito JAA. Relationships between bone turnover and energy metabolism. J Diabetes Res. 2017;2017:9021314. doi:10.1155/2017/9021314
27. Han Y, You X, Xing W, Zhang Z, Zou W. Paracrine and endocrine actions of bone-the functions of secretory proteins from osteoblasts, osteocytes, and osteoclasts. Bone Res. 2018;6:16. doi:10.1038/s41413-018-0019-6
28. Wang Q, Zhang B, Xu Y, Xu H, Zhang N. The relationship between serum osteocalcin concentration and glucose metabolism in patients with type 2 diabetes mellitus. Int J Endocrinol. 2013;2013:842598. doi:10.1155/2013/842598
29. Riddle RC, Clemens TL. Insulin, osteoblasts, and energy metabolism: why bone counts calories. J Clin Invest. 2014;124(4):1465–1467. doi:10.1172/JCI75554
30. Maddaloni E, D’Onofrio L, Lauria A, et al. Osteocalcin levels are inversely associated with Hba1c and BMI in adult subjects with long-standing type 1 diabetes. J Endocrinol Invest. 2014;37(7):661–666. doi:10.1007/s40618-014-0092-7
31. Pacicca DM, Brown T, Watkins D, et al. Elevated glucose acts directly on osteocytes to increase sclerostin expression in diabetes. Sci Rep. 2019;9(1):17353. doi:10.1038/s41598-019-52224-3
32. Kindblom JM, Ohlsson C, Ljunggren O, et al. Plasma osteocalcin is inversely related to fat mass and plasma glucose in elderly Swedish men [published correction appears in J Bone Miner Res. 2010 Dec;25(12):2527]. J Bone Miner Res. 2009;24(5):785–791. doi:10.1359/jbmr.081234
33. Yeap BB, Chubb SA, Flicker L, et al. Reduced serum total osteocalcin is associated with metabolic syndrome in older men via waist circumference, hyperglycemia, and triglyceride levels [published correction appears in Eur J Endocrinol. 2011 Feb;164(2):315]. Eur J Endocrinol. 2010;163(2):265–272. doi:10.1530/EJE-10-0414
34. Zhou M, Ma X, Li H, et al. Serum osteocalcin concentrations in relation to glucose and lipid metabolism in Chinese individuals. Eur J Endocrinol. 2009;161(5):723–729. doi:10.1530/EJE-09-0585
35. Schwartz AV, Vittinghoff E, Bauer DC, et al. Association of BMD and FRAX score with risk of fracture in older adults with type 2 diabetes. JAMA. 2011;305(21):2184–2192. doi:10.1001/jama.2011.715
36. Nareman YM, Seham EN, Gehan HE, Reem MA, Alzhraa AE, Mohsen ES. Serum osteocalcin level in type II diabetes mellitus as a marker for early detection of osteoporosis. Al-Azhar Med J. 2015;44(1):41–50. doi:10.12816/0015698
37. Fukuda-Akita E, Okita K, Okauchi Y, et al. Impaired early insulin secretion in Japanese type 2 diabetes with metabolic syndrome. Diabetes Res Clin Pract. 2008;79:482–489. doi:10.1016/j.diabres.2007.10.003
38. Funakoshi S, Fujimoto S, Hamasaki A, et al. Analysis of factors influencing pancreatic β-cell function in Japanese patients with type 2 diabetes: association with body mass index and duration of diabetic exposure. Diabetes Res Clin Pract. 2008;82:353–358. doi:10.1016/j.diabres.2008.09.010
39. Dumitru N, Carsote M, Cocolos A, et al. The link between bone osteocalcin and energy metabolism in a group of postmenopausal women. Curr Health Sci J. 2019;45(1):47–51. doi:10.12865/CHSJ.45.01.06
40. Funakoshi S, Yoshimura K, Hirano S, et al. Undercarboxylated osteocalcin correlates with insulin secretion in Japanese individuals with diabetes. Diabetol Metab Syndr. 2020;12:72. doi:10.1186/s13098-020-00579-3
41. Chen Y, Zhao Q, Du G, Xu Y. Association between serum osteocalcin and glucose/lipid metabolism in Chinese Han and Uygur populations with type 2 diabetes mellitus in Xinjiang: two cross-sectional studies. Lipids Health Dis. 2017;16(1):139. doi:10.1186/s12944-017-0512-8
42. Pennisi P, Signorelli SS, Riccobene S, et al. Low bone density and abnormal bone turnover in patients with atherosclerosis of peripheral vessels. Osteoporos Int. 2004;15(5):389–395. doi:10.1007/s00198-003-1550-9
43. Ye C, Xu M, Wang S, et al. Decreased bone mineral density is an independent predictor for the development of atherosclerosis: a systematic review and meta-analysis. PLoS One. 2016;11(5):e0154740. doi:10.1371/journal.pone.0154740
44. Szekanecz Z, Raterman HG, Pethő Z, Lems WF. Common mechanisms and holistic care in atherosclerosis and osteoporosis. Arthritis Res Ther. 2019;21(1):15. doi:10.1186/s13075-018-1805-7
45. Chen L, Li Q, Yang Z, et al. Osteocalcin, glucose metabolism, lipid profile and chronic low-grade inflammation in middle-aged and elderly Chinese. Diabet Med. 2013;30(3):309–317. doi:10.1111/j.1464-5491.2012.03769.x
46. Bao Y, Zhou M, Lu Z, et al. Serum levels of osteocalcin are inversely associated with the metabolic syndrome and the severity of coronary artery disease in Chinese men. Clin Endocrinol (Oxf). 2011;75(2):196–201. doi:10.1111/j.1365-2265.2011.04065.x
47. Riquelme-Gallego B, García-Molina L, Cano-Ibáñez N, et al. Circulating undercarboxylated osteocalcin as estimator of cardiovascular and type 2 diabetes risk in metabolic syndrome patients. Sci Rep. 2020;10(1):1840. doi:10.1038/s41598-020-58760-7
48. Prats-Puig A, Osiniri I, Soriano-Rodríguez P, et al. Undercarboxylated osteocalcin relates to cardiovascular risk markers in offspring of families with metabolic syndrome. Atherosclerosis. 2014;233(1):272–277. doi:10.1016/j.atherosclerosis.2014.01.00
49. Rached M-T, Kode A, Silva BC, et al. FoxO1 expression in osteoblasts regulates glucose homeostasis through regulation of osteocalcin in mice. J Clin Invest. 2010;120:357–368.
50. Hill HS, Grams J, Walton RG, Liu J, Moellering DR, Garvey WT. Carboxylated and uncarboxylated forms of osteocalcin directly modulate the glucose transport system and inflammation in adipocytes. Horm Metab Res. 2014;46(5):341–347. doi:10.1055/s-0034-1368709
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.