Back to Journals » International Journal of General Medicine » Volume 14
Does Red Cell Distribution Width Predict Hip Fracture Mortality Among the Arab Population? A Single-Center Retrospective Cohort Study
Authors Hamdan M ![]() , Haddad BI
, Haddad BI ![]() , Jabaiti M, Alryalat SA
, Jabaiti M, Alryalat SA ![]() , Abdulelah AA
, Abdulelah AA ![]() , Alabed SH, Alabdullah TF, Aouant AN, Shahein HE, Dweik HI, Matar K, Alisi MS
, Alabed SH, Alabdullah TF, Aouant AN, Shahein HE, Dweik HI, Matar K, Alisi MS ![]()
Received 9 October 2021
Accepted for publication 14 December 2021
Published 22 December 2021 Volume 2021:14 Pages 10195—10202
DOI https://doi.org/10.2147/IJGM.S343538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammad Hamdan,1 Bassem I Haddad,1 Mohammad Jabaiti,1 Saif Aldeen Alryalat,2 Ahmed A Abdulelah,3 Shahed H Alabed,3 Tamadur F Alabdullah,3 Alia N Aouant,3 Haneen E Shahein,3 Hadeel I Dweik,3 Khaled Matar,4 Mohammed S Alisi1,5
1Department of Special Surgery, Division of Orthopaedics, School of Medicine, The University of Jordan, Amman, Jordan; 2Department of Special Surgery, Division of Ophthalmology, School of Medicine, The University of Jordan, Amman, Jordan; 3School of Medicine, The University of Jordan, Amman, Jordan; 4School of Medicine, American University of the Caribbean, Cupecoy, Sint Maarten; 5Faculty of Medicine, Islamic University of Gaza, Gaza, Palestine
Correspondence: Mohammed S Alisi
School of Medicine, The University of Jordan, Queen Rania Al Abdullah St 266 Al Jubaiha, Amman, 11942, Jordan
Tel +962790983284
Email [email protected]
Background: Hip fractures impose significant morbidity and mortality. Red cell distribution width (RDW) appears to be an emerging tool in predicting mortality following hip fractures. Several factors can influence the RDW value including genetic factors and ethnicity. The purpose of the study was to assess the relation between RDW level at admission and hip fracture mortality within 6 months among Arab/Middle East populations.
Methods: We conducted a single-center retrospective cohort study including 549 patients (274 female and 275 male) diagnosed with a hip fracture undergoing surgery from February 2016 to December 2019. All included patients shared the same country of origin which is Arab Middle East country. Statistical analysis, including binary regression, was performed to assess the relationship between RDW and mortality within 6 months of admission. Other predictors of mortality following hip fracture surgery were also assessed.
Results: The mean age was 76.42 (± 9.19) years. Seventy (12.8%) of participants died within 6 months. No statistically significant association (P=0.053) between RDW level at admission and mortality within 6 months of surgery was found. Binary regression demonstrated that the only independent predictors of mortality were age (P= 0.003, odds ratio 1.048 with 95% CI 1.016 to 1.080) and male gender (P= 0.021, odds ratio 1.872 with 95% CI 1.100 to 3.185).
Conclusion: Although the previous studies reported that RDW is one of the predictors of mortality in hip fracture patients, our study found no relation in the Arab population. This finding may confirm the influence of genetic factors and ethnicity on RDW value. We recommend further large-scale multicenter studies to solidly establish the relationship between RDW and hip fracture mortality among the Arab/Middle East population.
Keywords: RDW, hip fracture, mortality, Arab, red cell distribution width
Introduction
Hip fractures impose a global health burden, not only for being one of the most commonly encountered in acute orthopedic management but also for its associated morbidity and mortality.1 With the improvement in global life expectancy, hip fractures are estimated to increase in the upcoming years to 3.94 million and 6.26 million cases by 2025 and 2050, respectively, ranking hip fractures among the leading causes of morbidity worldwide.2 The Middle East is projected to account for 4.87% of global hip fractures in 2025, with a further increase to 6.96% by 2050.2 Hip fractures are associated with both, short-term and long-term mortality. Current estimates of mortality within the first postoperative month range between 5–10%, while the first-year mortality rate could approach as high as 36%.1,3
As a result of the significant association between hip fractures and mortality, several mortality predictive tools are utilized. Of significance, the American Society of Anesthesiologists (ASA) score and the Charlson Comorbidity Index (CCI).4,5 Specific prediction models with regard to hip fractures have been developed; they mainly encompass the Nottingham Hip Fracture Score (NHFS) and the Orthopedic version of the Physiologic and Operative Severity Score for the Enumeration of Mortality and Morbidity (O-POSSUM) as they enable preoperative risk stratification and accordingly aid in the management plan.6,7 Nonetheless, they have not been widely adopted due to the time-consuming process involved.8
The red cell distribution width (RDW) is a routine part of the complete blood count (CBC) and reflects the range of red blood cell (RBC) size and volume, where the higher the RDW, the greater the RBC heterogeneity. Although RDW is predominately used in the workup of anemia, it has been utilized as a predictive tool in a wide range of conditions among which are cardiovascular diseases, acute pancreatitis, diabetes, and colorectal cancer.9–13 As a result of the predictive value of RDW with various conditions, it is increasingly becoming an emerging tool in the prediction of mortality in hip fractures either solely, or in conjunction with other parameters.8,14–18
Since the RDW value may be influenced by genetic factors and different ethnicities or populations,19,20 we aimed to study the relation of RDW and mortality of hip fracture patients among the Middle East/Arab population sample. To the best of our knowledge, no previous studies from the Middle East reported this relationship.
Our study aimed to investigate the association of RDW value on admission with the short-term mortality (within 6 months of admission) in hip fracture patients. The results would either further reinforce or contradict the emerging use of RDW as an independent predictor of mortality in hip fractures.
Methods
A retrospective cohort study was conducted at a tertiary teaching hospital by retrieving and reviewing the records of patients who were admitted with a hip fracture during the period from February 2016 to December 2019. A total of 595 patients’ medical records were initially retrieved. Forty-six patients were excluded due to having missing information in medical records, being lost to follow-up, or being below the age of 50 years. Accordingly, 549 patients were included in the study and their medical records were reviewed. Of note, all included patients shared the same country of origin which is Arab Middle East country.
We collected the following data from the medical records: age, gender, comorbidities, type of fracture (femoral neck, intertrochanteric, or subtrochanteric), type of surgery (partial hip replacement, intramedullary nail, or dynamic hip screw), RDW upon admission, hemoglobin levels upon admission, and death up to 6 months after surgery.
Mortality was assessed collectively up to 6 months from the date of admission by either directly contacting the patients or their families by phone or by checking the date of the medical record for their latest visit to the clinic.
RDW is a measure of size variability of the erythrocytes and it is routinely done as part of CBC laboratory test at our institution. Our institution’s laboratory RDW reference limit is set at 15%. Accordingly, 2 RDW subcategories were set, normal RDW with value <15%, and elevated RDW with value ≥15%. The relationship between RDW at admission and all-cause mortality was subsequently investigated.
The study was conducted in accordance with ethical regulations of the Declaration of Helsinki. Ethical approval was obtained from the appropriate institutional review board (reference number 221000055).
Statistical Analysis
SPSS version 26.0 (Chicago, USA) was used in our analysis. Mean (± standard deviation) was used to describe continuous variables. Count (frequency) was used to describe other nominal variables. The independent sample t-test was performed to analyze the mean difference in mortality and each continuous measurement, and data were presented in mean difference and 95% confidence interval (CI). The Chi-square test was used to analyze the frequency difference between mortality and each categorical variable included in our analysis. Binary logistic regression was used to analyze the predictors of mortality. We adopted a model-building strategy to conduct binary logistic regression, where only variables that had a significant level (<0.1) at the univariate analysis were included in the regression model for multivariate analysis. The included variables were age, gender, RDW grouped values, type of fracture, and the presence of cardiovascular disease. All underlying assumptions were met. A P-value of 0.05 was adopted as a significant threshold.
Results
A total of 549 patients were included in this study, with a mean age of 76.42 (±9.19) years. They were 275 (50.1%) men and 274 (49.9%) women. Overall, seventy patients (12.8%) died within 6 months of admission (28 in hospital, 33 within 3 months, and 9 within 3–6 months). Table 1 details the characteristics of the included sample.
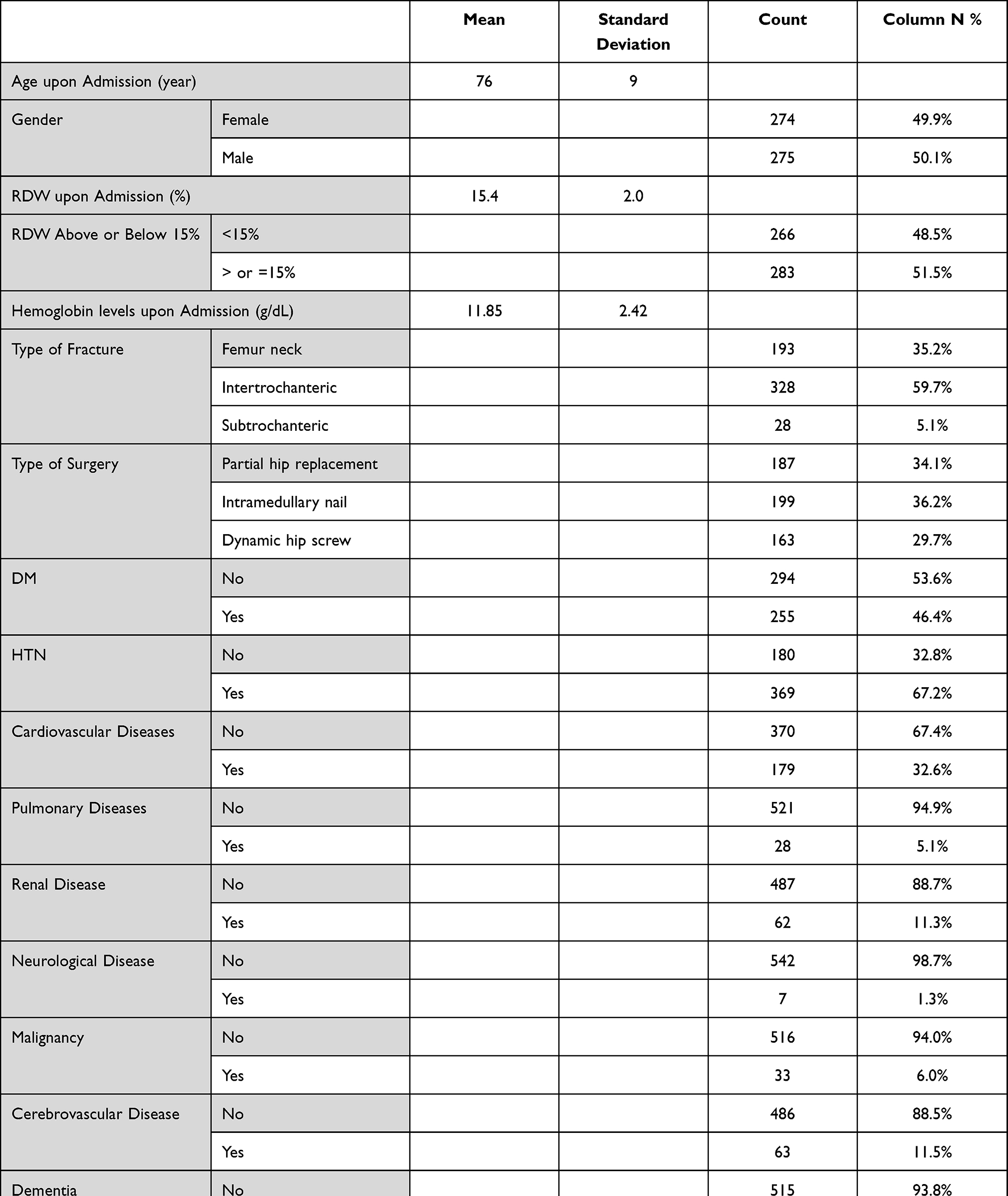 |
Table 1 Characteristics of Patients in the Included Sample |
Upon comparing the characteristics of patients who died within six months of admission and those who survived, the mean RDW was 15.85% (SD 1.96) and 15.36% (SD 1.96), respectively (P= 0.053; mean difference 0.486 with 95% CI between 0.01 to 0.98).
When categorizing RDW to either less than 15% or more than or equal to 15% and using it as a categorical variable rather than a continuous variable, a more significant relationship was deduced with 62.9% of those who died within 6 months having an RDW value equal to or above 15%, compared to 49.9% of those who survived (P=0.028).
Table 2 compares the characteristics of patients who died within six months of admission and those who survived.
 |
Table 2 Comparison of the Characteristics of Patients Who Survived and Who Died Within 6 Months |
Upon performing a binary logistic regression to analyze the predictors of mortality, we included only variables that had a significant level (<0.1) at the univariate analysis (Table 2), including age, gender, RDW grouped values, type of fracture, and the presence of cardiovascular disease. Hemoglobin level was not included due to high collinearity with other variables. The resulted model was able to accurately predict 87.2% of the outcome and the omnibus test was significant at <0.001 level. The only variables that were found as significant predictors of mortality were age (P= 0.003, odds ratio 1.048 with 95% CI 1.016 to 1.080), and gender (P= 0.021, odds ratio 1.872 with 95% CI 1.100 to 3.185), as shown in Table 3.
 |
Table 3 Analysis of Predictors of Mortality |
Discussion
With the projected exponential increase in the prevalence of hip fractures in the upcoming years, the utilization of a readily accessible and rapidly assessed tool in predicting the significant associated mortality risk in patients is of significant value. Multiple tools, such as the Nottingham Hip Fracture Score (NHFS) and the Orthopedic version of the Physiologic and Operative Severity Score for the Enumeration of Mortality and Morbidity (O-POSSUM), have been developed and are currently utilized for the assessment of mortality risk in hip fracture patients.6,7 Nonetheless, currently available models are devoid of either, rapid assessment ability, ready accessibility, or both; thus limiting their clinical use.8 Accordingly, several studies investigated the use of RDW, a readily available and rapidly assessed hematological parameter, as a possible predictor of mortality in hip fracture patients.8,14–18
The exact explanation behind the link between elevated RDW level and increased mortality of variant illnesses (including hip fracture) is not well-understood.8 The main reported theory is that the anisocytosis of the erythrocytes is a result of chronic inflammatory status (higher level of inflammatory cytokines and oxidative stress).17,21 This state will lead to increased erythrocyte apoptosis, myelosuppression, and decreased erythropoietin production. The net result is a release of premature red cells into the circulation, hence, elevated RDW. Another theory postulated that the increased level of RDW may be resulted from huge disturbances in homeostasis due to underlying metabolic diseases such as hypertension, dyslipidemia, and malnutrition. Thus, increased the risk of mortality.15
Several reports documented that RDW may be influenced by genetic factors and different ethnic groups.19,20 Our study is unique as it studied the relation between RDW level and mortality of hip fracture in a Middle East/Arab population sample. To the best of our knowledge, no previous studies from our region confirmed or rejected that relation.
Our study failed to consider the RDW as one of the predictors of mortality in hip fracture patients as we did not find a statistically significant relation between RDW and mortality on binary regression.
Our findings are not consistent with the existing literature, where Garbharran et al17 reported a 1-year mortality rate of 36% among individuals with RDW level above 15.3% in comparison to a mortality rate ranging from 12% to 29% among participants with RDW level below 15.3% indicating a 3-fold increase in mortality risk. Similarly, Zehir et al14 demonstrated a 2.8-fold increase in mortality risk in patients older than 77 years with RDW level above 14.5% at presentation.
The only significant association between RDW and mortality in our study appeared when we grouped the RDW value into <15% and ≥15%. Among the deceased participants, 62.9% had an elevated RDW (RDW≥15%) on admission compared to only 49.9% of those who survived (P=0.028). Interestingly, this relation was not significant on binary logistic regression analysis.
Lv et al8 investigated the relation between RDW level and long-term mortality among hip fracture patients. They demonstrated a statistically significant and independent association between RDW level at admission (above 13.8%) and all-cause mortality risk at 2-year and 4-year in non-anemic hip fracture patients. We were satisfied by studying the same relation but at the short-term mortality (6 months) as there is evidence that the most critical time for an elderly patient with hip fracture is the first year after the fracture and specifically within the first 3 months. Furthermore, the hazards decreased substantially over the first 2 years after fracture.22,23 Interestingly, of 70 deceased patients in our study, 28 patients died while in hospital after surgery, 33 patients died within 3 months of surgery, and only 9 patients died after 3 months but less than 6 months of surgery.
In the recent literature, there is evidence that older age and male gender are predictors of increased mortality of hip fracture patients.23–26 After performing binary regression, our study revealed older age and male gender to be the only significant independent predictors of mortality; thus, supporting the preexisting reports.
The type of the presenting hip fracture could have a compelling predisposition to mortality where it has been reported that patients suffering from intertrochanteric fractures are at a higher risk of morbidity, and most importantly, mortality compared to the other types of hip fractures.27 In contrast, neither the type of hip fracture (P=0.084) nor the type of procedure performed (P=0.910) in our study demonstrated a statistically significant association with mortality. This finding is supported by the study of Zehir et al14 which reported similar findings to ours by demonstrating the absence of statistically significant association between the type of fracture or surgical approach and mortality among hip fracture patients. Due to the contradicting results in the literature, further investigations are recommended to establish the presence of a possible association between the type of fracture and mortality.
In terms of study limitations, our sample size, 549 participants, is rather small compared to some previous similar studies.8,15,17 More importantly, our study is limited by the relatively small number of deaths in our sample where only 70 out of 549 (12.8%) participants were deceased within 6 months of the date of admission that preventing the sub-categorization of our short-term mortality assessment into in-hospital mortality, 3-month mortality, and 6-month mortality. Furthermore, the study is also limited by its retrospective rather than prospective nature in a single institution.
We think that the conflicting results about the relation between RDW and mortality of hip fracture may be related to factors affecting the RDW such as lifestyle, genetic factors, and differences in ethnicity. We recommend the conduction of multicenter prospective cohort studies including Arab populations from multiple countries from the Middle East to further elaborate on the true relationship between RDW and hip fracture mortality.
Conclusion
Although the previous studies reported that RDW is one of the predictors of mortality in hip fracture patients, our study found no relation in the Arab population. This finding may confirm the influence of genetic factors and ethnicity on RDW value. Further large-scale multicenter studies are recommended to solidly establish the relationship between RDW and hip fracture mortality among the Arab/Middle East population.
Ethics Statements
The authors certify that this research was approved by institutional review board at Jordan University Hospital (ethical approval code: 221000055) and this study complied with the Declaration of Helsinki. As our study is a retrospective one that did not include patient identifying features, the institutional review board waived us from obtaining informed consent from the included participants.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Parker M, Johansen A. Hip fracture. BMJ. 2006;333(7557):27–30. doi:10.1136/bmj.333.7557.27
2. Cooper C, Campion G, Melton LJ
3. Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009;20(10):1633–1650. doi:10.1007/s00198-009-0920-3
4. Magi E. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1997;78(2):228. doi:10.1093/bja/78.2.228
5. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
6. Rushton PR, Reed MR, Pratt RK. Independent validation of the Nottingham Hip Fracture Score and identification of regional variation in patient risk within England. Bone Joint J. 2015;97-B(1):100–103. doi:10.1302/0301-620X.97B1.34670
7. van Zeeland ML, Genovesi IP, Mulder JW, Strating PR, Glas AS, Engel AF. POSSUM predicts hospital mortality and long-term survival in patients with hip fractures. J Trauma. 2011;70(4):E67–E72. doi:10.1097/TA.0b013e3181edbf7a
8. Lv H, Zhang L, Long A, et al. Red cell distribution width as an independent predictor of long-term mortality in hip fracture patients: a Prospective Cohort Study. J Bone Miner Res. 2016;31(1):223–233. doi:10.1002/jbmr.2597
9. Ilhan E, Güvenç TS, Altay S, et al. Predictive value of red cell distribution width in intrahospital mortality and postintervention thrombolysis in myocardial infarction flow in patients with acute anterior myocardial infarction. Coron Artery Dis. 2012;23(7):450–454. doi:10.1097/MCA.0b013e3283587897
10. Al-Najjar Y, Goode KM, Zhang J, Cleland JG, Clark AL. Red cell distribution width: an inexpensive and powerful prognostic marker in heart failure. Eur J Heart Fail. 2009;11(12):1155–1162. doi:10.1093/eurjhf/hfp147
11. Yao J, Lv G. Association between red cell distribution width and acute pancreatitis: a cross-sectional study. BMJ Open. 2014;4(8):e004721. doi:10.1136/bmjopen-2013-004721
12. Gang L, Lifang W. Association of the elevated red blood cell distribution width with the risk of developing diabetes mellitus. Intern Med. 2016;55(15):1959–1965. doi:10.2169/internalmedicine.55.5956
13. Song Y, Huang Z, Kang Y, et al. Clinical usefulness and prognostic value of red cell distribution width in colorectal cancer. Biomed Res Int. 2018;2018:9858943. doi:10.1155/2018/9858943
14. Zehir S, Sipahioğlu S, Ozdemir G, Sahin E, Yar U, Akgül T. Red cell distribution width and mortality in patients with hip fracture treated with partial prosthesis. Acta Orthop Traumatol Turc. 2014;48(2):141–146. doi:10.3944/AOTT.2014.2859
15. Yin P, Lv H, Li Y, et al. Hip fracture patients who experience a greater fluctuation in RDW during hospital course are at heightened risk for all-cause mortality: a prospective study with 2-year follow-up. Osteoporos Int. 2018;29(7):1559–1567. doi:10.1007/s00198-018-4516-7
16. Yin P, Lv H, Zhang L, Long A, Zhang L, Tang P. Combination of red cell distribution width and American Society of Anesthesiologists score for hip fracture mortality prediction. Osteoporos Int. 2016;27(6):2077–2087. doi:10.1007/s00198-015-3357-x
17. Garbharran U, Chinthapalli S, Hopper I, George M, Back DL, Dockery F. Red cell distribution width is an independent predictor of mortality in hip fracture. Age Ageing. 2013;42(2):258–261. doi:10.1093/ageing/afs176
18. Ji HM, Han J, Bae HW, Won YY. Combination of measures of handgrip strength and red cell distribution width can predict in-hospital complications better than the ASA grade after hip fracture surgery in the elderly. BMC Musculoskelet Disord. 2017;18(1):375. doi:10.1186/s12891-017-1738-3
19. Zalawadiya SK, Veeranna V, Panaich SS, Afonso L, Ghali JK. Gender and ethnic differences in red cell distribution width and its association with mortality among low risk healthy United state adults. Am J Cardiol. 2012;109(11):1664–1670. doi:10.1016/j.amjcard.2012.01.396
20. Fava C, Cattazzo F, Hu ZD, Lippi G, Montagnana M. The role of red blood cell distribution width (RDW) in cardiovascular risk assessment: useful or hype? Ann Transl Med. 2019;7(20):581. doi:10.21037/atm.2019.09.58
21. Patel KV, Ferrucci L, Ershler WB, Longo DL, Guralnik JM. Red blood cell distribution width and the risk of death in middle-aged and older adults. Arch Intern Med. 2009;169(5):515–523. doi:10.1001/archinternmed.2009.11
22. Haentjens P, Magaziner J, Colón-Emeric CS, et al. Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390. doi:10.7326/0003-4819-152-6-201003160-00008
23. Schnell S, Friedman SM, Mendelson DA, Bingham KW, Kates SL. The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr Orthop Surg Rehabil. 2010;1(1):6–14. doi:10.1177/2151458510378105
24. Smith T, Pelpola K, Ball M, Ong A, Myint PK. Pre-operative indicators for mortality following hip fracture surgery: a systematic review and meta-analysis. Age Ageing. 2014;43(4):464–471. doi:10.1093/ageing/afu065
25. Morri M, Ambrosi E, Chiari P, et al. One-year mortality after hip fracture surgery and prognostic factors: a prospective cohort study. Sci Rep. 2019;9(1):18718. doi:10.1038/s41598-019-55196-6
26. Endo Y, Aharonoff GB, Zuckerman JD, Egol KA, Koval KJ. Gender differences in patients with hip fracture: a greater risk of morbidity and mortality in men. J Orthop Trauma. 2005;19(1):29–35. doi:10.1097/00005131-200501000-00006
27. Vaseenon T, Luevitoonvechkij S, Wongtriratanachai P, Rojanasthien S. Long-term mortality after osteoporotic hip fracture in Chiang Mai, Thailand. J Clin Densitom. 2010;13(1):63–67. doi:10.1016/j.jocd.2009.10.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.