Back to Journals » Journal of Pain Research » Volume 16
Does Percutaneous Endoscopic Lumbar Discectomy for Adolescent Posterior Ring Apophysis Fracture Accompanied with Lumbar Disc Herniation Have Better Outcome Than Lumbar Disc Herniation Alone?
Authors Wu H, Li T, Cao J, He D, Wu T, Liu J, Yuan J, Cheng X
Received 6 October 2022
Accepted for publication 7 March 2023
Published 16 March 2023 Volume 2023:16 Pages 911—919
DOI https://doi.org/10.2147/JPR.S380945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
Hui Wu, Tao Li, Jian Cao, Dingwen He, Tianlong Wu, Jiahao Liu, Jinghong Yuan, Xigao Cheng
Department of Orthopaedic Surgery, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China
Correspondence: Xigao Cheng, Department of Orthopaedics Surgery, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China, 330006, Email [email protected]
Objective: This study aims to compare the efficacy of percutaneous endoscopic lumbar discectomy (PELD) in treating adolescent posterior ring apophysis fracture (APRAF) accompanied by lumbar disc herniation (LDH) and lumbar disc herniation alone.
Methods: Herein we present a case series of adolescent patients who underwent PELD surgery from June 2017 to September 2021. All patients were divided into two distinct groups (ie Group A and B), based on their preoperative Computed tomography (CT) scans. Group A included patients with PRAF (type III) accompanied by LDH. Group B patients had LDH alone. The general clinical characteristics, clinical outcomes, and complications in patients from the two groups were assessed and compared.
Results: Compared to before surgery, the back and leg visual analog scores (VAS) and Oswestry Disability Index (ODI) were markedly improved in both groups’ patients at all follow-ups. Notably, no significant differences were observed in the back and leg VAS scores, and ODI values between the two groups at different time points after surgery. The mean intraoperative blood loss was significantly lower in Group B, relative to Group A. The mean operation time was significantly shorter in Group B, compared to Group A. There was no statistically significant difference in complication and recurrence rates between the two groups.
Conclusion: APRAF (type III) accompanied by LDH and LDH alone can obtain roughly equal surgical effects through PELD surgery and turns out to be a safe and effective surgical approach.
Keywords: adolescent, posterior ring apophysis fracture, percutaneous endoscopic lumbar discectomy, lumbar disc herniation
Introduction
Lumbar disc herniation (LDH) is relatively rare among the adolescent population but heavily contributes to low-back pain and lower-extremity radiculopathy.1 In some cases, small bone fragments are found near the posterior edge of the vertebral body, leading to a condition called posterior ring apophysis fracture (PRAF).2–4 PRAF is an extremely rare etiology of adolescent low back pain.2–5 Repeated microtrauma and physiological delay in posterior vertebral endplate ossification in adolescents and young adults are typically considered the main contributors to PRAF.2,4,6 Owing to the very low incidence rate of PRAF, clinicians often lack awareness of this condition, leading to a delayed or missed diagnosis.5 PRAF can be accurately diagnosed using computed tomography (CT) evaluation.5 Based on the CT scan fracture positioning, Takata et al classified PRAF into four categories.4,7–9 Type I represents the separation of the entire posterior margin; type II represents the partial vertebral separation fracture including the margin; type III represents laterally located fractures; type IV represents vertebral body edge fracture that spans the entire vertebral body.4,7–9 Due to continuous bone compression, conservative treatment is often ineffective, and thus, often requires surgical intervention.4,10 In recent years, percutaneous endoscopic lumbar discectomy (PELD) is widely used to correct adolescent LDH (ALDH),11 however, only limited studies have reported satisfactory results in the treatment of type III PRAF using PELD.9 Since a typical PRAF pathological feature is the displacement of the posterior vertebral body edge or the fracture entering into the spinal canal, some surgeons question the adequacy of nerve root decompression, in addition to the controversy regarding its efficacy in PRAF (type III) accompanied with LDH versus LDH alone. To the best of our knowledge, vertebral epiphyseal cartilage is usually completely fused to the vertebral body by 21 years of age.6 Therefore, in this study, we defined 21 years as the upper age limit of ALDH.6 This study aims to compare the efficacy of PELD in treating adolescent PRAF (APRAF, type III) accompanied by LDH versus LDH alone, which is not reported in prior investigations.
Methods
This study comprised a case series of adolescent patients who underwent PELD surgery in our department from June 2017 to September 2021. This study was approved by the Human Research Ethics Council at our hospital. All patients in this study provided written informed consent for treatment and to publish the data. The inclusion criteria for the patients were as follows:
- Age ≤21 years;
- Single-level PRAF (type III) accompanied by LDH or LDH alone confirmed by magnetic resonance imaging (MRI) and computed tomography (CT) scan, consistent with clinical symptoms;
- Poor response to conservative measures for a minimum of 3 months;
The exclusion criteria were as follows:
- Any previous history of spine surgery;
- Congenital spinal dysplasia, spinal tumor, and infection;
- Other types of PRAF.
All the patients were divided into two distinct groups based on their preoperative CT scan. Group A included patients with PRAF (type III) accompanied by LDH confirmed by preoperative CT scan. Group B included patients with LDH alone.
Surgical Technique
Since the clinical symptoms of PRAF accompanied with LDH are similar to those of lumbar disc herniation alone. Hence, the indications for percutaneous endoscopic interlaminar discectomy (PEID) and percutaneous endoscopic transforaminal discectomy (PETD) approach were consistent with previous principles.9,12 Therefore, in our case, PEID would be recommended for treating LDH especially at L5/S1 under certain conditions and PETD would be recommended for treating LDH especially at L3–4, L4–5.
PETD
All operations were performed under local anesthesia. Patients were placed in a lateral decubitus position on a radiolucent operating table Local anesthesia was performed at the entrance of the needle entry point, which was approximately 8–14 cm lateral to the spine midline. Next, an 18G needle was inserted, under fluoroscopic guidance. On the anteroposterior fluoroscopic view, the standard point of the initial needling is located on the medial pedicular line. On the lateral fluoroscopic view, the standard point of the initial needling, which was the surface of the superior articular process (SAP). Subsequently, detach the needle and replace it with a guidewire, and then a working channel is inserted, along with the guidewire. Under a continuous liquid flow of 0.9% saline solution, the unnecessary nucleus pulposus tissue was removed by bipolar radiofrequency and endoscopic forceps. As for patients with PRAF (type III) accompanied by LDH, the herniated disc should be removed first, which is conducive to leaving more space to treat apophysis fractures. We advocate that mobile fragment should be removed; however, the entire immobile bony fragment may not be resected if the nerve root has been sufficiently decompressed. The key of this surgery was to ensure that the nerve roots were fully exposed, and the pulsation was adequate.
PEID
In our study, all PEID operations were performed under local anesthesia. Patients were placed in prone position. The 18 G needle trajectory was introduced into the inferior margin of the articular surface. Subsequently, the needle was removed and replaced with a guidewire, and a working channel was inserted, according to the guidewire. Under a continuous liquid flow of 0.9% saline solution, the unnecessary nucleus pulposus tissue was removed by bipolar radiofrequency and endoscopic forceps. As for patients with PRAF (type III) accompanied by LDH, the soft herniated disc should be removed first, which is conducive to leaving more space to treat the apophysis fracture. We advocate that mobile fragment should be actively removed; however, the immobile fragment could be properly retained under the condition that the nerve root has been sufficiently decompressed.
Outcomes Measurements
Clinical Measurements
The general clinical parameters were analyzed and included age, gender, BMI, operative segment, duration of symptoms, straight-leg raising, mean operative time, mean blood loss, mean length of hospital stay, complications, and recurrence. Clinical outcomes were evaluated using VAS for low back and leg pain, the ODI score, and the modified MacNab criteria.
Statistical Analyses
Statistical analyses were performed using SPSS 26.0 software. The variables were presented as the mean ± standard deviation (SD). Paired t-test was used for intra-group comparison. Independent sample t-test and chi-square test were used to compare the differences in clinical outcomes between the two groups. P value <0.05 was defined as statistically significant.
Results
Demographics
In this study, 12 patients in group A and 31 patients in group B met our requirements of inclusion criteria. Patients’ baseline demographic characteristics were not significantly different between the two groups (Table 1).
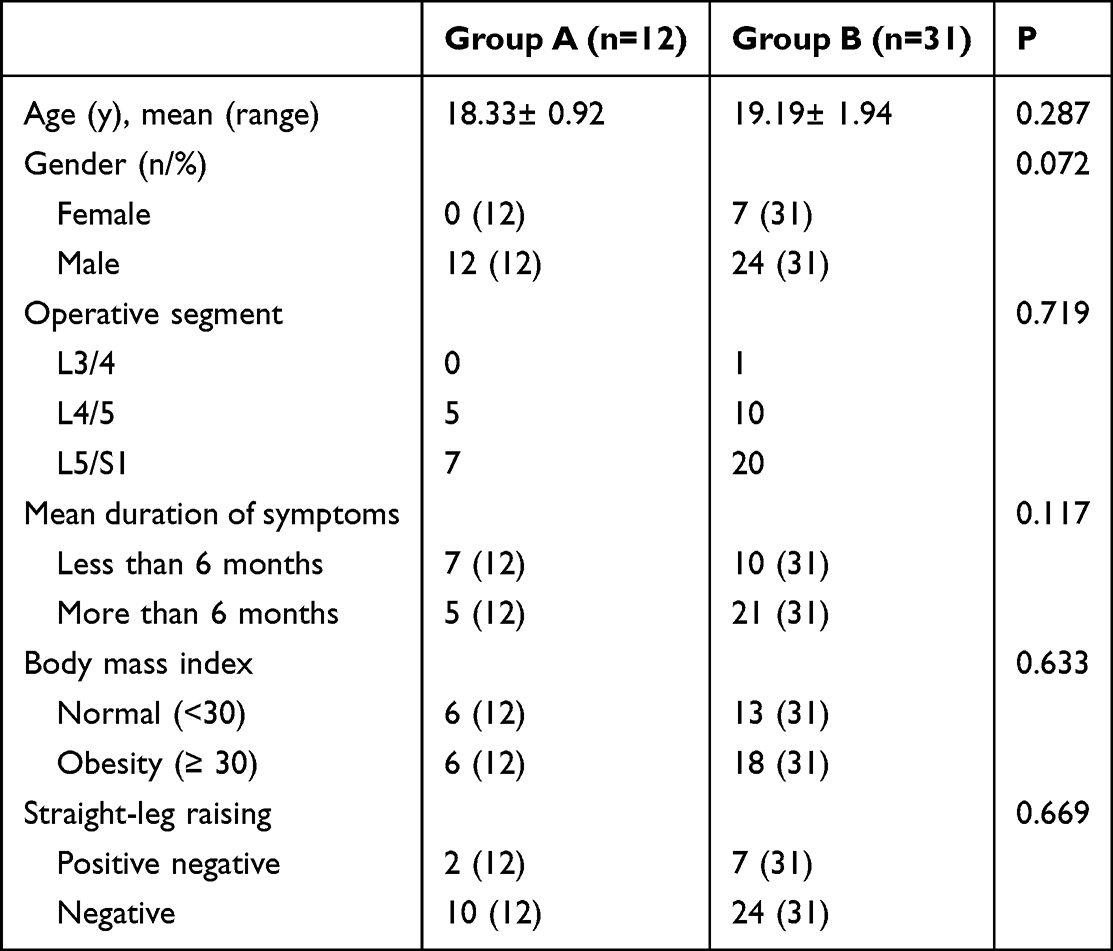 |
Table 1 Shows the Preoperative Baseline Data of the Two Groups of Patients |
Perioperative Outcomes
The mean hospital stay in group A (1.67±0.36 days) was nearly equal to the hospital stay of group B (1.97 ± 0.28 days) patients (P =0.553) (Table 2). The mean intraoperative blood loss was significantly lower in group B (51.77 ± 0.79 mL), relative to group A (63.75± 1.09 mL) (P <0.0001). The mean surgery time was significantly shorter for group B (47.74± 0.98 min) compared to group A (57.92± 1.56 min) patients (P < 0.0001) (Table 2).
 |
Table 2 Shows the Perioperative Characteristics of the Two Groups of Patients |
Clinical Evaluation
A total of 6 patients in Group A received bony fragment removal, including two cases at L4/5 level and four cases at L5/S1 level. Compared to before surgery, the back and leg VAS scores and ODI were markedly improved in both groups at all follow-up time points (Figure 1A–C). During the follow-up, an interesting phenomenon was noted. Although the VAS scores for the back and leg, and ODI were significantly improved at the 12-month follow-up, compared to before surgery, there were no significant differences in these parameters when compared to the 6-month follow-up (Figure 1A–C). Notably, no significant differences were observed in the back and leg VAS scores, and ODI values between the two groups at different time points after surgery (P > 0.05) (Table 3). However, patients in group A were more prone to transient sensory abnormalities than group B patients immediately after surgery. At the last follow-up, there were no significant differences in the overall excellent and good rates between the two groups (P > 0.05) (Table 3). The overall excellent and good rates of group A (12/12) were 100%, and in group B (30/31) were 96.77%. There were no serious complications in any of the two groups of patients.
 |
Table 3 Comparison of the Main Indicators of Clinical Outcomes Between the Two Groups |
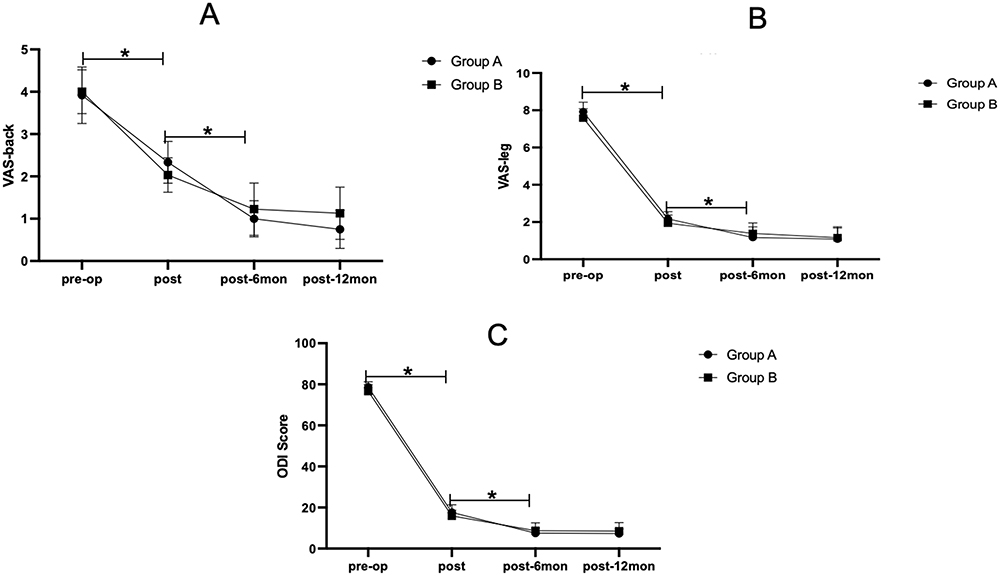 |
Figure 1 Show the VAS for back scores (A), VAS for leg scores (B) and ODI scores (C) were markedly improved in both groups at all follow-up time points. Abbreviations: VAS, the visual analogue scale; ODI, Oswestry disability index. Note: *p<0.05. |
Discussion
Being an essential and rare etiology of adolescent low back pain, posterior ring apophyseal fracture has not attracted enough attention.3,6 Owing to the relatively small sample sizes in various studies, the PRAF with LDH prevalence varies greatly among studies.2,9,13 It is reported that most patients experience delayed diagnosis spanning an average of over 1 year. 14 Because of poor response to conservative treatment, surgical intervention is always recommended.4,10 Many investigators suggested that centrally located lesions (ie, types I, II, and IV), which cause canal or foraminal stenosis, require bilateral laminectomy or total laminectomy to remove the large and extensive fragment(s).9,14 In type III cases where a unilateral lesion occurs, posterior discectomy with semilaminotomy or laminectomy without fusion is typically considered the gold standard surgical procedure.9 Children experience significant growth and a continuously changing skeletal structure. Therefore, minimally invasive surgery is optimal for their growing bodies. The typical pathological feature of ring apophysis fracture inducing the displacement of the posterior edge of the vertebral body or the fracture entering into the spinal canal makes nerve root decompression insufficient.5 Therefore, it is more meaningful to compare PELD efficacy in treating APRAF accompanied with LDH and LDH alone. It is reported that PELD achieved satisfactory results in treating PRAF (type III) accompanied by LDH, with an excellent and good rate of 93.4%. 9 In our study, the excellent and good rate of PELD in treating epiphyseal ring disconnection was 100%, and that of LDH alone was 96.77%. This was mainly due to the relatively small number of cases in our study, along with a short follow-up time and adequate decompression of nerve roots. Most notably, at the last follow-up, there was no significant difference in the overall excellent and good rates between the two groups. Figures 2 and 3 depict two typical cases. Based on our analysis, the mean intraoperative blood loss was significantly lower in group B compared to group A. The mean surgery time was significantly shorter for group B patients compared to group A. The difference in the aforementioned results was primarily due to the removal of loose and mobile fragments during surgery. To better eliminate the hard- sharp-edged mobile bone fragments without causing nerve root injury and dural tears, the herniation disc must be removed first.9 Subsequently, bone fragments must be progressively removed under visual control using burrs and a rongeur.9 These procedures, unfortunately, enhanced surgery duration and bleeding in group A. In contrast, there was no significant difference in the average hospitalization time between groups A and B. This was likely due to the excellent care of the patients after surgery in our institution. We also speculated that the minimally invasive nature of PELD was another major factor.15 Our study demonstrated that both APRAF accompanied with LDH and LDH alone achieved good clinical outcomes following PELD treatment. During the follow-up period, the symptoms continued to improve at different time points following surgery in both groups’ patients. Although the VAS and ODI scores decreased at the 12-month follow-up, there were no significant differences in these scores compared to the 6-month follow-up. This phenomenon may have multiple explanations. For example, even if the materials compressing the nerve were removed, the critical recovery period for leg pain still fell within the 6-month time point following PELD.16 Moreover, the patient’s symptom duration was relatively short, and the distal deformation and demyelination of nerve fibers were mild.17 Although there was no significant difference in the VAS score of the lower extremity immediately after surgery, we observed that patients in group A were more prone to transient sensory abnormalities than in group B. This may be related to the excessive traction of the nerve root during surgery, especially in terms of the large mobile fragment.18 In addition, intraoperative bipolar electrocoagulation stimulation can also lead to postoperative sensory abnormalities.19 Fortunately, following several days of conservative treatment, such as dehydration and hormonal treatment, these symptoms were alleviated. At the last follow-up, most patients in both groups returned to their baseline functional status and were able to return to school or work without long-term recovery. During the follow-up period, no serious complications were observed in any of the two groups of patients.
 |
Figure 2 Case one. A 21-year-old male was admitted to our department for severe left leg radicular pain of nearly 6 months. The patient was diagnosed with L5/S1 posterior ring apophysis fracture accompanied with lumbar disc herniation (A–D). The soft herniated disc and mobile bony fragment were removed during the PEID surgery (E–G). The patient achieved immediate pain relief and was discharged from hospital within 4 days. The functional improvement was well at 6 months after PEID (H and I). Abbreviation: PEID, percutaneous endoscopic interlaminar discectomy. |
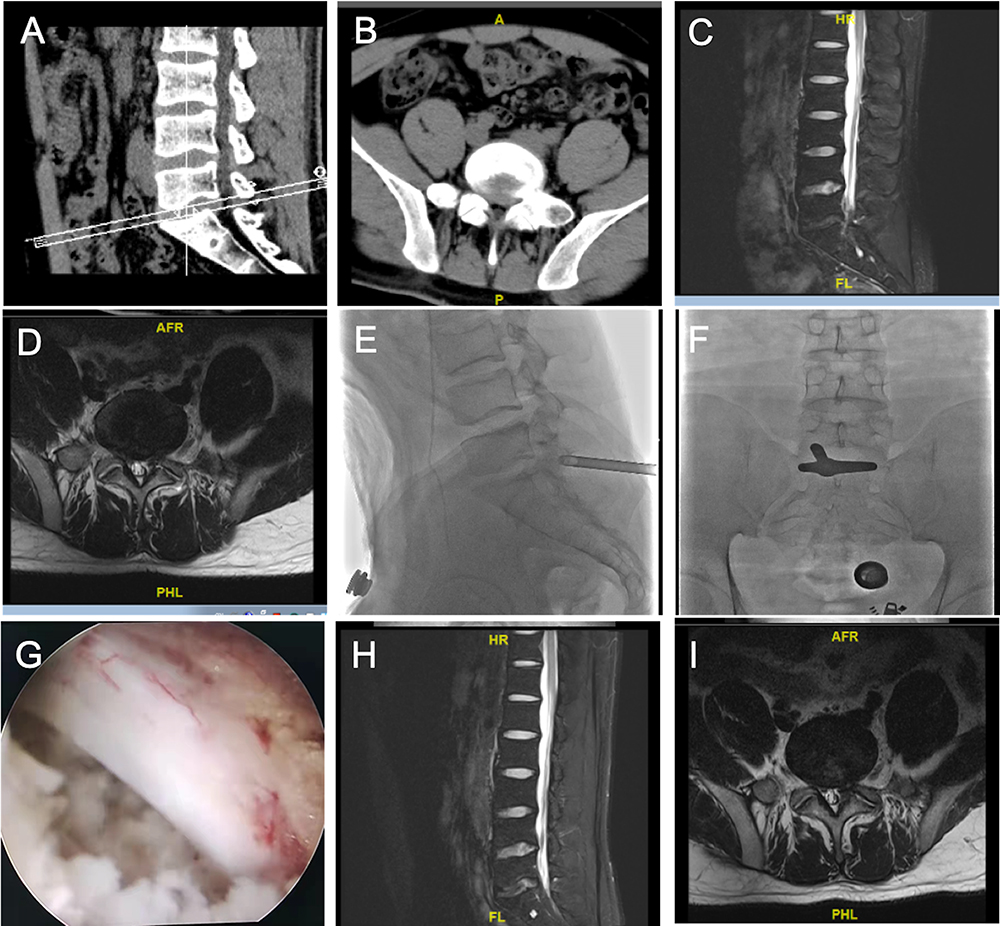 |
Figure 3 Case two. A 17-year-old male was admitted to our department for severe left low back pain and sciatica of nearly 10 months. The patient was diagnosed with L5/S1 lumbar disc herniation alone (A–D). The soft herniated disc was removed during the PEID surgery (E–G). The patient achieved immediate pain relief and was discharged from hospital within 24 hours. The functional improvement was well at 3 months after PEID (H and I). Abbreviation: PEID, percutaneous endoscopic interlaminar discectomy. |
Limitations
The present study had several limitations. First, the present study had a retrospective design with a small sample. Second, the follow-up period was short. Of course, high-quality research with sufficiently large sample sizes and longer follow-up period are necessary to further confirm these results. However, despite of these limitations, satisfactory short-term clinical results with PELD for both APRAF accompanied by LDH and LDH alone were confirmed.
Conclusion
Based on our analysis, PELD is a safe and effective approach for both APRAF accompanied with LDH and LDH alone. Furthermore, there are no significant differences in symptom relief and functional recovery.
Data Sharing Statement
The data of this study can be obtained by contacting the corresponding author, Xigao. Cheng, at [email protected].
Consent for Publication
Since the patients were minors, written informed consent was obtained from their parents for publication of this research and accompanying images and pictures.
Ethical Statement
This study was performed following the principles of the Declaration of Helsinki and was conducted according to the National Ethics Guidelines Statement. Informed consent was obtained from all participants or their parents. This study was supported by the ethics committee of the Second Affiliated Hospital of Nanchang University (No. Review [2014] No. (071).).
Funding
This study was supported by the National Science Founding of China (No. 81860397 to Xigao Cheng).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lavelle WF, Bianco A, Mason R, et al. Pediatric disk herniation. J Am Acad Orthop Surg. 2011;19(11):649–656. doi:10.5435/00124635-201111000-00001
2. Akhaddar A, Belfquih H, Oukabli M, et al. Posterior ring apophysis separation combined with lumbar disc herniation in adults: a 10-year experience in the surgical management of 87 cases. J Neurosurg Spine. 2011;14(4):475–483. doi:10.3171/2010.11.SPINE10392
3. Epstein NE, Epstein JA. Limbus lumbar vertebral fractures in 27 adolescents and adults. Spine. 1991;16(8):962–966. doi:10.1097/00007632-199108000-00017
4. Wu H, Zheng S, He D, et al. Percutaneous endoscopic interlaminar discectomy for posterior ring apophyseal fracture accompanied with lumbar disc herniation in a 12-year pediatric diver: a case report. Childs Nerv Syst. 2023;39(1):275–278. doi:10.1007/s00381-022-05605-5
5. Conlee EM, Driscoll SW, Wood KC, et al. Posterior vertebral endplate fractures: a retrospective study on a rare etiology of back pain in youth and young adults. Pm&r. 2019;11:619–630. doi:10.1016/j.pmrj.2018.10.002
6. Kadam G, Narsinghpura K, Deshmukh S, et al. Traumatic lumbar vertebral ring apophysis fracture with disk herniation in an adolescent. Radiol Case Rep. 2017;12:427–430. doi:10.1016/j.radcr.2016.11.026
7. Takata K, Inoue SI, Takahashi K, et al. Fracture of the posterior margin of a lumbar vertebral body.. J Bone Joint Surg Am. 1988;70(4):589–594. doi:10.1055/s-2008-1040215
8. Epstein NE, Epstein JA, Thomas M. Treatment of fractures of the vertebral limbus and spinal stenosis in five adolescents and five adults. Neurosurgery. 1989;24(4):595. doi:10.1097/00006123-198904000-00019
9. Zheng ZZ, Tu Z, Li Y, et al. Full-endoscopic lumbar discectomy for lumbar disc herniation with posterior ring apophysis fracture: a retrospective study. World Neurosurg. 2018. doi:10.1016/j.wneu.2018.12.054
10. Wu X, Ma W, Du H, Gurung K. A review of current treatment of lumbar posterior ring apophysis fracture with lumbar disc herniation. Eur Spine J. 2013;22:475–488. doi:10.1007/s00586-012-2580-9
11. Zheng C, Fei W, Lin C. Transforaminal percutaneous endoscopic discectomy in the treatment of far-lateral lumbar disc herniations in children. Int Orthop. 2016;40(6):1099–1102. doi:10.1007/s00264-016-3155-x
12. Eggers C, Pedrosa DJ, Kahraman D, et al. A New full-endoscopic technique for the interlaminar operation of lumbar disc herniations using 6-mm endoscopes: prospective 2-year results of 331 patients. Minim Invasive Neuro. 2006;49(02):80–87. doi:10.1055/s-2006-932172
13. Martínez-Lage JF, Poza M, Arcas P. Avulsed lumbar vertebral rim plate in an adolescent: trauma or malformation? Childs Nerv Syst. 1998;14(3):131–134. doi:10.1007/s003810050195
14. Baba H, Uchida K, Furusawa N, et al. Posterior limbus vertebral lesions causing lumbosacral radiculopathy and the cauda equina syndrome. Spinal Cord. 1996;34(7):427–432. doi:10.1038/sc.1996.76
15. Cao J, Huang W, Wu T, Jia J, Cheng X. Percutaneous endoscopic lumbar discectomy for lumbar disc herniation as day surgery - short-term clinical results of 235 consecutive cases. Medicine. 2019;98(49):e18064. doi:10.1097/MD.0000000000018064
16. Basques BA, Haws BE, Khechen B, et al. The effect of preoperative symptom duration on postoperative outcomes after a tubular lumbar microdiscectomy. Clin Spine Surg. 2019;32(1):E27–E30. doi:10.1097/BSD.0000000000000711
17. Wang Y, Gao F, Zou H. Numbness and weakness recovered at a less extent in patients with lumbar disc herniation after percutaneous endoscopic lumbar discectomy. Pain Res Manag. 2019;2019:4642701. doi:10.1155/2019/4642701
18. Chen Z, Zhang L, Dong J, et al. Percutaneous transforaminal endoscopic discectomy compared with microendoscopic discectomy for lumbar disc herniation: 1-year results of an ongoing randomized controlled trial. J Neurosurg Spine. 2018:1–11. doi:10.3171/2017.7.SPINE161434
19. Phan K, Teng I, Schultz K, et al. Treatment of lumbar spinal stenosis by microscopic unilateral laminectomy for bilateral decompression: a technical note. Orthop Surg. 2017;9:241–246. doi:10.1111/os.12335
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Research Trends of Percutaneous Endoscopic Lumbar Discectomy in the Treatment of Lumbar Disc Herniation Over the Past Decade: A Bibliometric Analysis
Zhang Y, Chu J, Xia Y, Xie Y, Zhang R, Chen X, Chen Z, Yao X
Journal of Pain Research 2023, 16:3391-3404
Published Date: 4 October 2023