Back to Journals » Nature and Science of Sleep » Volume 12
Does Nasal Obstruction Induce Obstructive Sleep Apnea in Healthy Women?
Authors Pittaway I, Ishkova A, Bean H, McCarthy S, Lay I, Avraam J, Dawson A, Thornton T ![]() , Nicholas CL, Trinder J, O'Donoghue FJ, Jackson ML
, Nicholas CL, Trinder J, O'Donoghue FJ, Jackson ML ![]() , Jordan AS
, Jordan AS ![]()
Received 18 March 2020
Accepted for publication 11 May 2020
Published 22 June 2020 Volume 2020:12 Pages 347—355
DOI https://doi.org/10.2147/NSS.S254473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sutapa Mukherjee
Islay Pittaway,1 Anna Ishkova,1 Helena Bean,1 Stephanie McCarthy,1 Isabella Lay,1 Joanne Avraam,1 Andrew Dawson,1 Therese Thornton,1 Christian L Nicholas,1,2 John Trinder,1 Fergal J O’Donoghue,2,3 Melinda L Jackson,2,4 Amy S Jordan1,2
1Melbourne School of Psychological Sciences, The University of Melbourne, Parkville, VIC 3010, Australia; 2Institute for Breathing and Sleep, Austin Health, Heidelberg, VIC 3084, Australia; 3Department of Medicine, The University of Melbourne, Austin Hospital, Heidelberg, VIC 3084, Australia; 4Turner Institute for Brain and Mental Health, School of Psychological Sciences, Monash University, Clayton, VIC 3164, Australia
Correspondence: Amy S Jordan Tel +61 3 8344 6357
Email [email protected]
Purpose: Obstructive sleep apnea (OSA) is less prevalent among women and is associated with different symptoms and consequences to OSA in men. The reasons for these differences are unknown and difficult to tease apart in clinical populations. If OSA could be temporarily induced in healthy men and women, the causes of some of these differences could be investigated. Nasal blocking has been used to induce OSA in healthy men but its effect in women has not been reported.
Patients and Methods: A total of 14 healthy individuals (10 women) underwent in-laboratory diagnostic sleep studies on two occasions separated by a week. On one occasion, the nasal passages were blocked, whereas on the other occasion, participants slept naturally. In both conditions, a full-face mask was used to monitor respiratory events. Participants’ self-reported sleepiness, mood and performance on a motor learning task were assessed in the evening and morning of both sleep studies. Furthermore, endothelial function and self-reported sleep quality were assessed in the morning following each study.
Results: Nasal blockage induced OSA in healthy young (age=22± 3 years) and slim (BMI=22.2± 3.2 kg/m2) women (control AHI=2.0± 2.6, blocked AHI=33.1± 36.7 events/hr, p=0.02). One night of OSA was associated with poorer self-reported sleep quality (p< 0.001) and increased self-reported snoring (p< 0.04), choking and gasping during sleep (p< 0.001) but was not associated with alterations in mood, neurocognitive or endothelial function on the following morning.
Conclusion: Nasal blockage induces OSA in healthy, young, and normal weight women. However, whether the induced OSA is representative of naturally occurring OSA and the technique useful for future studies is unclear.
Keywords: pathophysiology, upper airway collapse, sex, breathing route, obstructive sleep apnea, nasal blockage, female
Plain Language Summary
Obstructive sleep apnea (OSA) is more common and associated with different symptoms and consequences in men as compared to women. The reasons for these differences are unknown and difficult to tease apart in clinic populations. Blocking the nose during sleep has been shown to induce OSA in otherwise healthy men, but no studies of nasal occlusion have been conducted in women to date. This study demonstrates that nasal occlusion induces OSA in otherwise healthy young women raising the possibility that nasal blockage may be useful technique for investigating sex differences in OSA.
Introduction
Obstructive sleep apnea (OSA) is approximately half as prevalent in women as it is in men.1 The reasons for the lower prevalence of OSA in women are not entirely clear. The pathogenesis of OSA is considered to be multifactorial, with elements of airway anatomy, dilator muscle responsiveness, respiratory system instability and the threshold for arousal from sleep all implicated.2 Women have been shown to have a less collapsible airway for any given body mass index,3,4 which may at least in part explain the lower prevalence of OSA. However, other aspects of the pathogenesis including respiratory control stability and airway dilator muscle responsiveness do not appear to differ between the sexes.3,5,6 Further, it is unclear whether the respiratory arousal threshold differs between sexes,7 although it should be noted that there is substantial within-subject variability in respiratory arousal threshold across the night.8 Thus, the causes of the sex difference in OSA prevalence are incompletely understood.
In addition to the sex difference in the prevalence of OSA, the disease phenotype also differs between men and women.9 Women are more likely to demonstrate REM sleep predominant OSA,10 have shorter apneas11,12 with less blood oxygen desaturation,13 and have a smaller change in severity from supine to lateral body position14 than men. It is presently unclear whether these differences are related to women having lower severity of OSA than men in clinical samples,11,14 or if they occur irrespective of the severity of OSA. Alternatively, the differences may be influenced by sex differences in demographic factors, such as women with OSA being more likely to be older and have higher body mass indices than men with equally severe OSA.9,10
Finally, the symptoms and consequences of OSA also appear to differ between sexes,9,15 with women more likely to report insomnia, fatigue, headaches and depression, and to experience greater mood disturbance, impaired quality of life and altered metabolic consequences of OSA than men.9,16-18 There are also reports of improved mortality in women with OSA compared to men with OSA.19,20 Whether the different consequences of OSA relate to the altered characteristics of OSA mentioned above (shorter events with more sleep fragmentation and higher airway resistance but less desaturation) or reflect an underlying sex difference in susceptibility to OSA consequences is not known. It is difficult to tease apart these possibilities in clinical patients as either potentially biased samples of men and women who are matched on certain characteristics, or large numbers of subjects and statistical accounting for potentially confounding sex differences, are required.
An alternative way of investigating sex differences in OSA would be by temporarily inducing OSA in otherwise healthy individuals with and without the underlying confounding differences that exist in clinical samples. Numerous studies have demonstrated that blocking the nose of healthy men during sleep can induce OSA.21–25 However, none of these studies included any female participants. Thus, the primary aim of this study was to determine whether a single night of nasal blockage induces OSA in healthy young women. Although the primary aim of the study was to investigate the effect of nasal blockage in women, we also recruited approximately 1/3 men to ensure that the prior reported effects of nasal blockage were observed in our laboratory population (typically young, slim university students) using current OSA scoring rules.26 The secondary aim was to determine whether one night of nasal blocking was associated with negative consequences (sleepiness, memory impairment, impaired mood and/or cardiovascular function) in otherwise healthy young men and women.
Patients and Methods
Subjects
Healthy individuals aged between 18 and 65 years were recruited using flyers placed around the University of Melbourne Parkville campus. Individuals were excluded from participation if they were self-reported poor sleepers or were currently experiencing sleep disturbances, had recently travelled through more than 1 time-zone, were smokers, had been diagnosed with any sleep disorder, cardiorespiratory disease or diabetes, or were allergic to Amethocaine. The study was approved by the University of Melbourne Human Research Ethics Committee (1545303) and was performed in accordance with the Declaration of Helsinki. All participants gave informed written consent to participate.
Design
The present study utilised a crossover design, with each participant completing an experimental (nose blocked) and control night in the sleep laboratory, with the two nights separated by approximately 1 week. As the experimental intervention was self-evident, it was not possible to blind participants to experimental conditions. To prevent order effects, the experimental conditions were counterbalanced for every 10 participants, using a computer-generated pseudo-random sequence.
Procedures
Participants were asked to maintain their normal sleep schedule for the week leading up to the study and to refrain from ingesting caffeine or alcohol for 12 hours before attending the sleep laboratory. Participants arrived at the laboratory approximately three hours prior to their regular bedtime. Upon arrival, individuals had their age, sex, height, and weight recorded. They were then led into a quiet room where they completed the multivariable apnea risk index (MAPI, first night only),27 positive and negative affect schedule (PANAS),28 Karolinska Sleepiness Scale (KSS),29 and a motor learning task (motor sequence task: MST, details below) on a computer. Participants then prepared for bed, and were prepared for polysomnography. Specifically, participants were fitted with six EEG electrodes (F3, F4, C3, C4, O3, O4 referenced to the contralateral A1 or A2 electrode), left and right EOG, masseter EMG, oximeter, respiratory bands and leg sensors. On the experimental night participants then had their nose blocked (details below). On both nights a full-face mask (FreeMotion RT041, Fisher and Paykel, Auckland, NZ) was worn and was connected to a pitot flow sensor (Seleon GmbH, Heilbronn, Germany) to assess airflow. All signals were amplified and filtered using a Compumedics Grael (Abbotsford, VIC, Australia) unit and recorded using Profusion PSG 3 software (Compumedics, Abbotsford, VIC, Australia) in accordance with the AASM guidelines.26 Once the quality of the signals was confirmed, the lights were turned off and participants were allowed to sleep for at least 8 hours. If the nasal blockage became too bothersome during the night, participants could remove it for approximately 20 minutes, before it was re-inserted.
Following awakening, participants moved to a comfortable chair and 10 minutes elapsed before two blood pressure measurements (HEM 7130, Omron Healthcare, Singapore) were taken and endothelial function assessed (Endopat, Itamar Medical, Caesarea, Israel). Endopat measures of arterial stiffness (Augmentation index) and reactive hyperemia index (RHI) were automatically calculated. Participants then rated the quality of their sleep on a Likert scale ranging from 1 (very poor) to 10 (excellent), and reported how strongly they agreed with experiencing “Vivid dreams”, “Snoring”, “Gasping for air/feeling like I was choking” and “Feeling sweaty” (1 strongly disagree, 10 strongly agree). They were then provided with breakfast that did not include any caffeinated products after which they repeated the PANAS, KSS and MST. Subsequently, the electrodes and physiological sensors were removed and the participants were discharged from the laboratory.
Nasal Blockage: Nasal packing was employed to occlude the nares in accordance with prior studies.24 This involved inserting the ends of a petroleum jelly coated roll of gauze approximately 1.5 cm into each nostril until the participant was unable to breathe through their nose. The gauze was secured in place overnight using Sleek tape placed underneath the roll onto the nostrils and over the bridge of the nose.
Motor Sequence Task: The MST followed the protocol of Tucker et al.30 Specifically, the participant typed a 5-number sequence as many times and as accurately as they could for 30s using their non-dominant hand. Twelve trials were performed with 30s rest between each trial. On the first experimental session, participants used the sequence 41324, whereas on the second session participants used the sequence 23142.
Data Analysis
PSG data were visually scored for sleep stages and respiratory events in accordance with the recommended AASM (2012) guidelines26 by an expert technician who was blinded to the experimental night. Consistent with prior studies,30 the first 3 and last 3 trials of each MST session were averaged to monitor task performance. The positive affect questions were summed, as were the negative affect questions in order to generate a single value of positive and negative affect to compare between evening and morning, as well as between conditions.
Statistical Analysis
The primary aim was assessed with paired samples Student’s t-tests comparing the Apnea Hypopnea Index (AHI) between conditions in women only. This was repeated for the male subjects, although it should be noted this comparison was to ensure the previously reported effect in males was observed with our laboratory procedures. Subjective sleepiness and sleep quality as well as the other polysomnographic characteristics and secondary outcome variables were also compared between the experimental and control conditions using Student’s t-tests for all participants (men and women combined). Exploratory Pearson’s correlations were conducted to ascertain whether the overnight change in AHI was associated with baseline AHI or demographic characteristics (age, BMI, MAPI). In addition, preliminary insight into whether sex differences in OSA characteristics exist was determined by comparing sleep study variables between sexes. Due to only 4 men being studied, we have not reported p values but rather effect sizes, which were manually calculated (using the following equation: r= z ÷√n). Effect sizes were interpreted according to Cohen’s (1988) criteria, which defined small, medium and large effect sizes as being equivalent to 0.1, 0.3, and 0.5, respectively.31 All analyses were conducted using IBM SPSS Statistics 25 software (Armonk, NY). Mean±SD are presented and p<0.05 considered significant.
Results
Ten women and four men completed the protocol. The women were aged 22±3 years and had a mean BMI of 22.2±3.2 kg/m2. The men were aged 26±7 years and had a mean BMI of 22.6±3.7kg/m2. All participants had low probability of apnea based on the MAPI (range 0.01–0.19).
Figure 1 shows the AHI on the two experimental nights in all participants. The AHI was significantly higher on the night when the nasal passages were blocked compared to the control night in women (AHI=33.1±36.7 versus 2.0±2.6 events/hr, respectively, p=0.02). Although the results appeared similar in the four men they were non-significant given the small sample size (AHI=19.3±36.7 versus 1.1±2.6 events/hr, respectively, p=0.12). Among all participants (men and women combined), the only significant predictor of the change in AHI between nights was the baseline AHI (p=0.006, r2=0.49). Other sleep characteristics on each night for both sexes are shown in Table 1.
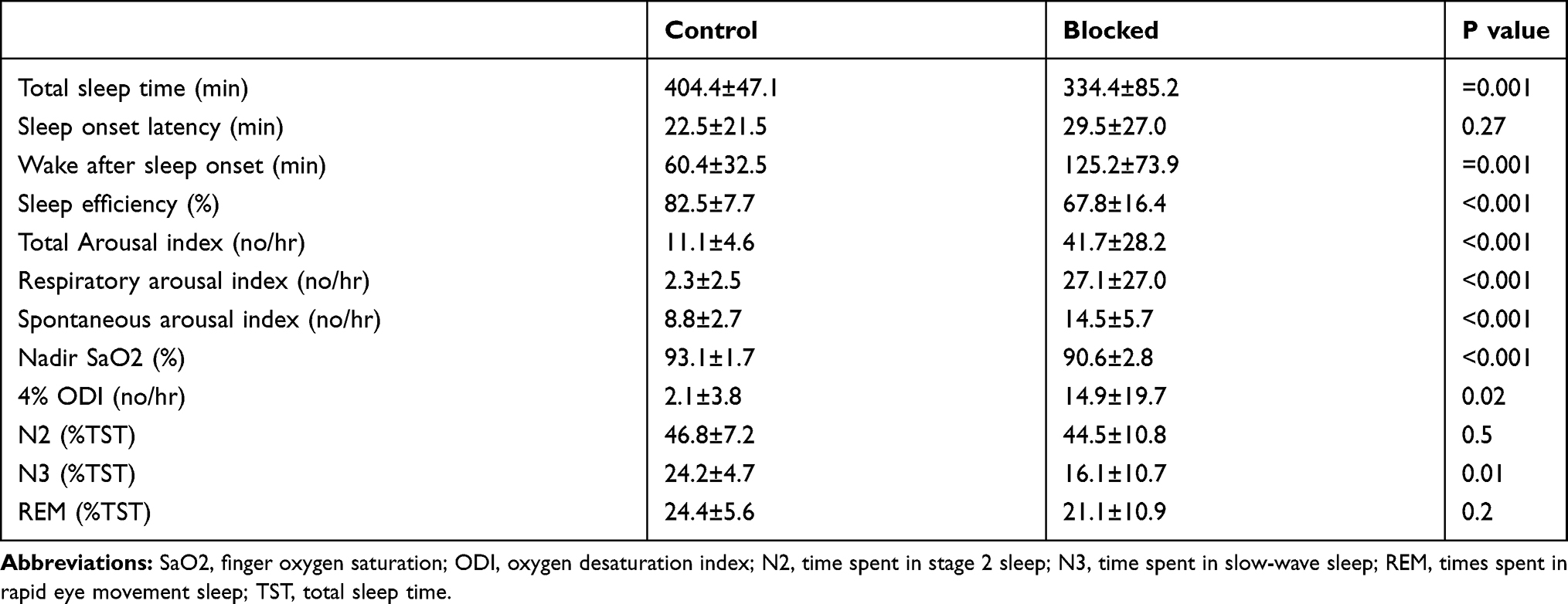 |
Table 1 Sleep Characteristics on the Control and Experimental (Blocked) Nights in All Participants (n=14) |
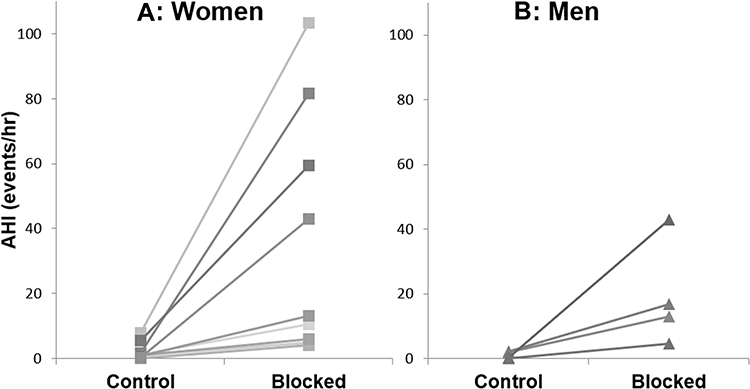 |
Figure 1 Individual Apnea-Hypopnea Indices (AHI) on the control and experimental (Blocked) nights in women ((A), squares, n=10) and men ((B), triangles, n=4) |
Four women developed severe OSA whereas the other 6 women studied developed no-mild OSA. The mean age (severe = 21.0±1.4 and no-mild = 22.7±4.8 years) and BMI (severe = 21.6±2.5 and no-mild = 22.7±3.8 kg/m2) were very similar between these sub-groups of women. Further, the AHI difference could be observed in both supine (severe = 71.4±27.3 and no-mild = 6.4±2.8 events/hr) and non-supine (severe = 55.6±8.6 and no-mild = 8.6±7.1 events/hr) positions. However, the four women who developed severe OSA appeared to have shorter sleep time (Total sleep time = 367±18.9 min and 438±24.2 min) and more disturbed sleep (Sleep efficiency = 76.2±5.2% and 87.7±4.5%) on the control night when compared to the women who went on to develop no-mild OSA. This was accompanied by a tendency for more REM-related respiratory events on the control night in the 4 women who went on to develop severe OSA (REM AHI severe 15.1±17.2 and no mild = 2.4±1.7 events/hr). The subjective reports of feeling like choking/gasping also tended to be higher in the 4 women who developed severe OSA as compared to those who developed no-mild OSA (7.3±1.5 and 5.2±3.2, respectively) whereas sleep quality tended to be lower in with severe OSA (2.3±1.3 and 3.8±2.4, respectively).
Table 2 summarises the effect of nasal blockage on subjective sleepiness, self-reported sleep quality and cardiovascular function. KSS ratings in the evening of the sleep study did not differ between conditions (5.0±1.9 prior to control night, 4.6±1.5 prior to blocked night, p=0.58). It did however differ between conditions on the morning following testing (Table 2). The subjective quality of sleep was poorer, and self-reported snoring and choking/gasping were increased, following the blocked night. Vivid dreams and self-reported sweatiness were not altered (Table 2). One male subject did not complete the cardiovascular testing due to missing equipment; hence, the cardiovascular data were obtained from 13 participants. Although there were trends towards differences in the arterial stiffness measure (AI) and heart rate, these were not significantly different between conditions (Table 2).
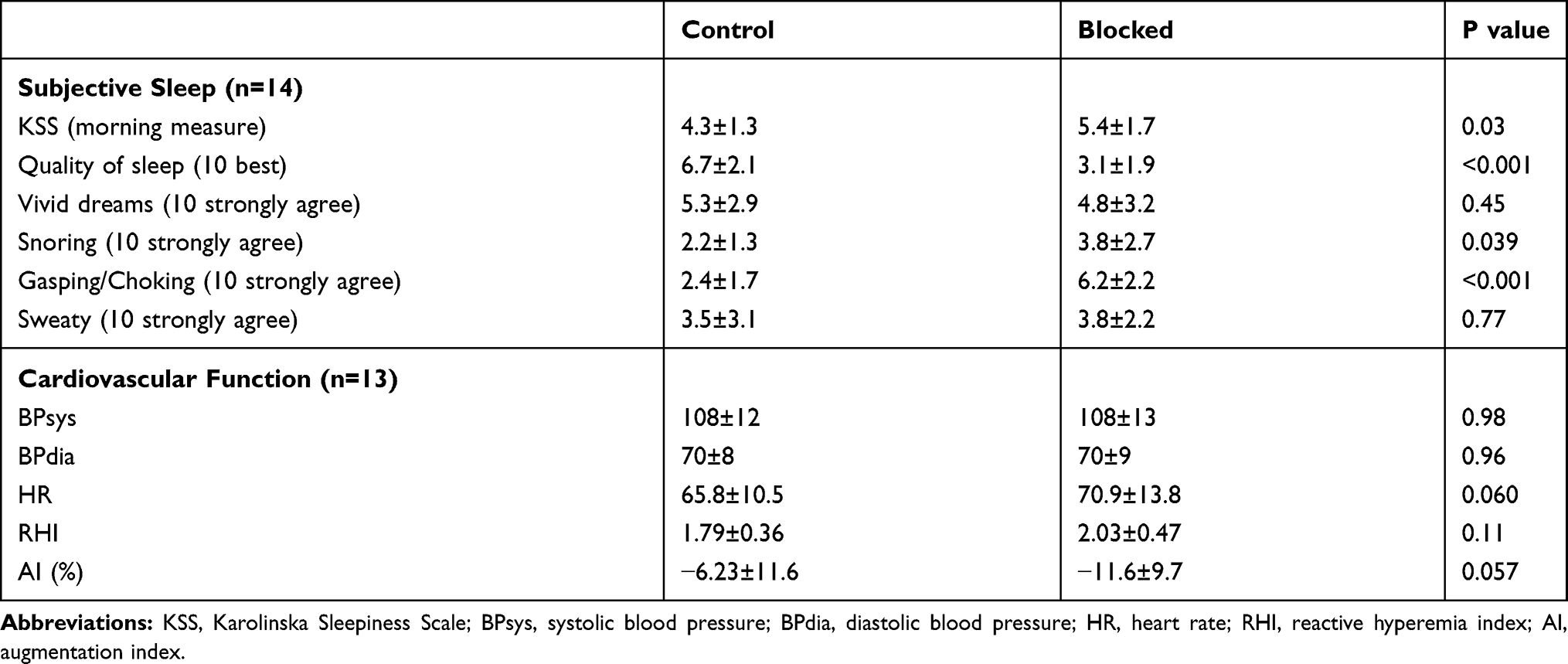 |
Table 2 Subjective Sleep and Cardiovascular Function on the Control and Experimental (Blocked Nose) Nights in All Participants |
Two participants were inadvertently given different test sequences (41324 vs 23142) from morning to evening on the first week of testing and therefore all MST data were excluded for both nights for these participants. The performance on the MST was slightly improved from the end of evening learning to the initial performance in the morning on both the control (23.4±4.5 and 25.5±6.5 correct trials, respectively, p=0.03) and blocked nose nights (22.1±6.2 and 25.9± 6.6 correct trials, respectively, p=0.004). However, the magnitude of the overnight improvement in MST performance did not differ between conditions (Figure 2, M1-M3 minus E10-E12, p=0.32).
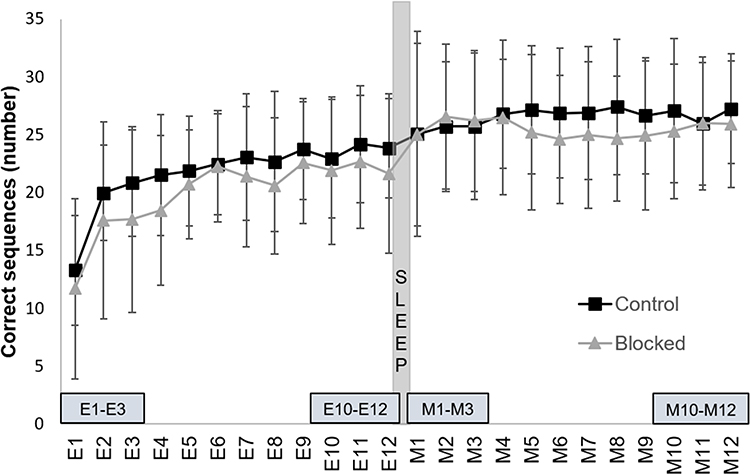 |
Figure 2 Motor sequence task performance in men and women with adequate data (n=12). The number of correct sequences typed during the motor sequence task over the twelve 30s trials conducted in the evening (E1–E12) and morning (M1–M12) on control (black square) and blocked nose (grey triangle) nights. The time points that were averaged for statistical comparisons are indicated in the horizontal bars at the bottom (E1–E3, E10–E12, M1–M3, M10–M12) and the time of the sleep period indicated by the grey vertical bar. |
Neither positive nor negative affect differed in the evening between study nights (Table 3). Likewise, neither positive nor negative affect differed between control and blocked nose nights in the morning (Table 3).
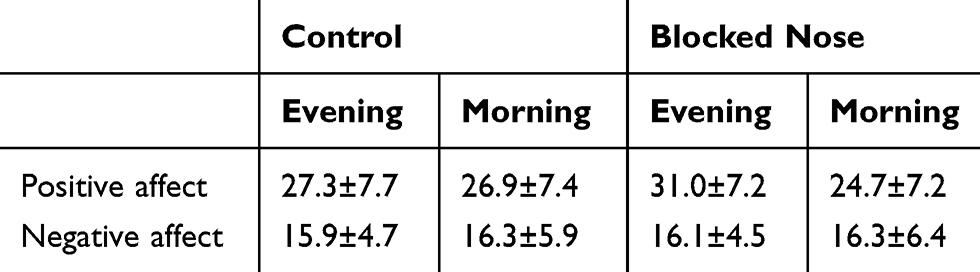 |
Table 3 Positive and Negative Affect Scores in the Morning and Evening of Control and Experimental (Blocked Nose) Nights in All Participants (n=14). No Significant Differences Between Evening-Morning or Between Conditions Were Observed |
The characteristics of OSA on the blocked nose night are shown separately for men and women in Table 4. This analysis should be considered in light of the fact that there are only 4 male participants. Given the low subject numbers, the effect sizes (a quantitative measure of the magnitude of the difference between the two groups31) are reported, and were quite small (in accordance with Cohen’s (1988) criteria, page 79–8031) for all comparisons except the obstructive apnea index which was moderately different between sexes (although still non-significant with p=0.21).
 |
Table 4 Obstructive Sleep Apnea Characteristics on the Blocked Nose Night in Men and Women. Due to the Small Number of Men Included the Effect Sizes are Reported (a Quantitative Measure of the Magnitude of the Difference Between the Two Groups) with Small, Medium and Large Effect Sizes Being Equivalent to 0.1, 0.3, and 0.5 (Pages 79–80).31 |
Discussion
The present study has demonstrated that blocking the nose of healthy, young women with normal body weight induces OSA in a similar fashion to what has been demonstrated in men.21–25 As per previous studies in men, there was a wide variability in the severity of OSA that was induced in women. The severity of OSA induced in these healthy individuals failed to correlate with the MAPI, BMI and age of participants. Only the AHI on the baseline night (which ranged from 0 to 7.9) was correlated with the magnitude of increase in AHI between conditions. Likewise, the four women who developed severe OSA on the blocked nose night appeared to have worse sleep quality and more REM-related events even on their control night perhaps indicating these individuals were lighter sleepers with a predisposition to airway collapse at least in REM. While blocking the nose clearly increased the AHI, it may have also independently disturbed sleep because the spontaneous arousal index and wake after sleep onset time were also increased on the blocked nose night while total sleep time was reduced in contrast to what is typically observed in at least chronic OSA.32 In addition, the OSA that was induced was associated with relatively mild blood oxygen desaturation (90% average, ODI = 15 events/hr) and was similar between body positions and NREM versus REM sleep. Finally, snoring was not commonly noted by the overnight staff. Thus, the OSA that was induced by blocking the nose appears to differ somewhat from spontaneously occurring OSA.
The mechanisms by which enforcing oral breathing induce OSA are uncertain. Upper airway resistance is similar when breathing through the oral as compared to nasal route while awake.33 However, even in the absence of respiratory events, airway resistance during sleep is actually higher during oral than nasal breathing.33 Elevated resistance during oral breathing while asleep may occur because of a relative reduction in upper airway dilator muscle activity due to reduced stimulation of upper airway negative pressure receptors during oral breathing,34 although not all studies demonstrate reduced dilator muscle activity during oral breathing.35 In addition, it is likely that participants adopted a more open jaw position on the blocked nose night which would predispose them to upper airway collapse36,37 and possibly shorten the transverse genioglossal fibers, thereby reducing the muscles mechanical efficacy.38 Another possibility is that during oral breathing the tongue is no longer restricted in its movement by the hard and soft palate and therefore is able to flop further back into the retroglossal space and therefore predispose to collapse. Finally, it is likely that the humidification of inspired air is reduced during oral breathing which may lead to a relative drying of the airway and increased surface tension forces as a result.39 Which, if any, of these mechanisms contributed to the increase in AHI observed in the current study during nasal occlusion is unknown.
Although there were very few men studied, the characteristics of the induced OSA appear similar between sexes. This contrasts with OSA in the sleep clinic and general populations in which men are typically reported to have longer respiratory events11 than women and a more even distribution of respiratory events between REM versus NREM as well as supine versus non-supine sleep positions.14 This may indicate that the cause of sex differences in OSA characteristics in clinical or general population samples are a result of comorbid conditions or anthropometric differences between sexes, such as higher body mass indices or older age in women with OSA. Alternatively, the similarity in OSA characteristics observed between sexes in this study may be related to the unique and un-natural cause of airway collapse (obligatory oral breathing) whereas the pathophysiology of naturally occurring airway collapse may cause the differences in OSA characteristic between sexes that are typically observed. For example, if the upper airway dilator muscles of women were more effective at holding open/re-opening the collapsible segment of the upper airway than the dilator muscles in men, it could explain why men get more OSA, have longer events (they are more reliant on arousal to re-open the airway) and why women would be relatively protected from events in NREM sleep compared to men but equally susceptible in REM (when the benefit of improved dilator muscle effectiveness would be reduced). Likewise, if sex differences in sleep-related breathing route preference exist then this advantage would have been removed in the current study. Further research with suitable numbers of men and women are required to assess such possibilities.
Despite quite notable group changes in the AHI and subjective reports of increased sleepiness on the morning following the blocked nose condition, the self-reported mood and performance on the motor sequence task were not altered between conditions. This may relate to the fact that sleep was relatively well preserved (N2 and REM were unchanged between conditions and N3 was reduced from 24% to 16% of total sleep time). Alternatively, these analyses may have been underpowered. However, it is also possible that one night of OSA is insufficient to elicit these consequences of OSA, particularly in this young cohort. Similarly, cardiovascular function may only be altered by events associated with more severe hypoxemia or exposure to respiratory events over more than one night. Future research studies employing multiple nights sleeping with the nasal passages blocked in a larger sample may be required to separate these possibilities.
The study is limited by several factors, including the different cause of OSA compared to the natural situation, possible additional sleep disturbance from the intervention itself, and small number of men included in this study. A further limitation was the fact that it was not possible to blind participants as to the experimental condition. This was particularly problematic as, for safety reasons, participants were warned during the initial screening session that they may experience poorer sleep during the experimental condition and therefore should not schedule it before important activities the next day such as exams or long drives. It is therefore plausible that morning performance following the experimental intervention may have been influenced by participant expectation.
Conclusion
This study has shown that OSA can be induced in otherwise healthy, young normal weight women by blocking the nasal passages for a single night. However, the induced OSA appeared to differ somewhat from naturally occurring OSA. Therefore, whether blocking the nose to induce OSA will be useful for future research studies will depend on the question being asked. It is possible that more than one night is required to more adequately represent OSA and its consequences. We would advise anyone attempting such research to try to recruit individuals who report snoring or who have baseline AHIs in the high normal range (AHI 3–5) in order to maximise the chances of inducing significant OSA during nasal blockage.
Ethics Approval and Informed Consent
All procedures performed in this study were in accordance with the ethical standards of the University of Melbourne and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Disclosure
All authors declare they have no conflicts of interest in this work.
References
1. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81. doi:10.1016/j.smrv.2016.07.002
2. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med. 2013;188(8):996–1004. doi:10.1164/rccm.201303-0448OC
3. Jordan AS, Wellman A, Edwards JK, et al. Respiratory control stability and upper airway collapsibility in men and women with obstructive sleep apnea. J Appl Physiol. 2005;99(5):2020–2027. doi:10.1152/japplphysiol.00410.2004
4. Kirkness JP, Schwartz AR, Schneider H, et al. Contribution of male sex, age, and obesity to mechanical instability of the upper airway during sleep. J Appl Physiol (1985). 2008;104(6):1618–1624. doi:10.1152/japplphysiol.00045.2008
5. Eckert DJ, Malhotra A, Lo YL, White DP, Jordan AS. The influence of obstructive sleep apnea and gender on genioglossus activity during rapid eye movement sleep. Chest. 2009;135(4):957–964. doi:10.1378/chest.08-2292
6. Pillar G, Malhotra A, Fogel R, Beauregard J, Schnall R, White DP. Airway mechanics and ventilation in response to resistive loading during sleep: influence of gender. Am J Respir Crit Care Med. 2000;162(5):1627–1632. doi:10.1164/ajrccm.162.5.2003131
7. Eckert DJ, Younes MK. Arousal from sleep: implications for obstructive sleep apnea pathogenesis and treatment. J Appl Physiol. 2014;116(3):302–313. doi:10.1152/japplphysiol.00649.2013
8. Li Y, Orr J, Jen R, et al. Is there a threshold that triggers cortical arousals in obstructive sleep apnea. Sleep. 2019;42:zsz047.
9. Theorell-Haglow J, Miller CB, Bartlett DJ, Yee BJ, Openshaw HD, Grunstein RR. Gender differences in obstructive sleep apnoea, insomnia and restless legs syndrome in adults - What do we know? A clinical update. Sleep Med Rev. 2018;38:28–38. doi:10.1016/j.smrv.2017.03.003
10. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women. Effects of gender. Am J Respir Crit Care Med. 2001;163(3):608–613. doi:10.1164/ajrccm.163.3.9911064
11. Ware JC, McBrayer RH, Scott JA. Influence of sex and age on duration and frequency of sleep apnea events. Sleep. 2000;23(2):165–170. doi:10.1093/sleep/23.2.1c
12. Butler MP, Emch JT, Rueschman M, et al. Apnea-hypopnea event duration predicts mortality in men and women in the sleep heart health study. Am J Respir Crit Care Med. 2019;199(7):903–912. doi:10.1164/rccm.201804-0758OC
13. Kulkas A, Duce B, Leppanen T, Hukins C, Toyras J. Gender differences in severity of desaturation events following hypopnea and obstructive apnea events in adults during sleep. Physiol Meas. 2017;38(8):1490–1502. doi:10.1088/1361-6579/aa7b6f
14. O’Connor C, Thornley KS, Hanly PJ. Gender differences in the polysomnographic features of obstructive sleep apnea. Am J Respir Crit Care Med. 2000;161(5):1465–1472. doi:10.1164/ajrccm.161.5.9904121
15. Lozo T, Komnenov D, Badr MS, Mateika JH. Sex differences in sleep disordered breathing in adults. Respir Physiol Neurobiol. 2017;245:65–75. doi:10.1016/j.resp.2016.11.001
16. Valipour A, Lothaller H, Rauscher H, Zwick H, Burghuber OC, Lavie P. Gender-related differences in symptoms of patients with suspected breathing disorders in sleep: a clinical population study using the sleep disorders questionnaire. Sleep. 2007;30(3):312–319. doi:10.1093/sleep/30.3.312
17. Temple KA, Leproult R, Morselli L, Ehrmann DA, Van Cauter E, Mokhlesi B. Sex differences in the impact of obstructive sleep apnea on glucose metabolism. Front Endocrinol (Lausanne). 2018;9:376. doi:10.3389/fendo.2018.00376
18. Hirotsu C, Albuquerque RG, Nogueira H, et al. The relationship between sleep apnea, metabolic dysfunction and inflammation: the gender influence. Brain Behav Immun. 2017;59:211–218. doi:10.1016/j.bbi.2016.09.005
19. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8):e1000132. doi:10.1371/journal.pmed.1000132
20. Yeboah J, Redline S, Johnson C, et al. Association between sleep apnea, snoring, incident cardiovascular events and all-cause mortality in an adult population: MESA. Atherosclerosis. 2011;219(2):963–968. doi:10.1016/j.atherosclerosis.2011.08.021
21. Zwillich CW, Pickett C, Hanson FN, Weil JV. Disturbed sleep and prolonged apnea during nasal obstruction in normal men. Am Rev Respir Dis. 1981;124(2):158–160. doi:10.1164/arrd.1981.124.2.158
22. Olsen KD, Kern EB, Westbrook PR. Sleep and breathing disturbance secondary to nasal obstruction. Otolaryngol Head Neck Surg. 1981;89(5):804–810. doi:10.1177/019459988108900522
23. Taasan V, Wynne JW, Cassisi N, Block AJ. The effect of nasal packing on sleep-disordered breathing and nocturnal oxygen desaturation. Laryngoscope. 1981;91(7):1163–1172. doi:10.1288/00005537-198107000-00015
24. Suratt PM, Turner BL, Wilhoit SC. Effect of intranasal obstruction on breathing during sleep. Chest. 1986;90(3):324–329. doi:10.1378/chest.90.3.324
25. Wilhoit SC, Suratt PM. Effect of nasal obstruction on upper airway muscle activation in normal subjects. Chest. 1987;92(6):1053–1055. doi:10.1378/chest.92.6.1053
26. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the american academy of sleep medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
27. Maislin G, Pack AI, Kribbs NB, et al. A survey screen for prediction of apnea. Sleep. 1995;18(3):158–166. doi:10.1093/sleep/18.3.158
28. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037/0022-3514.54.6.1063
29. Akerstedt T, Gillberg M. Subjective and objective sleepiness in the active individual. Int J Neurosci. 1990;52(1–2):29–37. doi:10.3109/00207459008994241
30. Tucker M, McKinley S, Stickgold R. Sleep optimizes motor skill in older adults. J Am Geriatr Soc. 2011;59(4):603–609. doi:10.1111/j.1532-5415.2011.03324.x
31. Cohen J. Statistical Power Analysis for the Behavioural Sciences.
32. Shahveisi K, Jalali A, Moloudi MR, Moradi S, Maroufi A, Khazaie H. Sleep architecture in patients with primary snoring and obstructive sleep apnea. Basic Clin Neurosci. 2018;9(2):147–156. doi:10.29252/nirp.bcn.9.2.147
33. Fitzpatrick MF, McLean H, Urton AM, Tan A, O’Donnell D, Driver HS. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur Respir J. 2003;22(5):827–832. doi:10.1183/09031936.03.00047903
34. Basner RC, Simon PM, Schwartzstein RM, Weinberger SE, Weiss JW. Breathing route influences upper airway muscle activity in awake normal adults. J Appl Physiol. 1989;66(4):1766–1771. doi:10.1152/jappl.1989.66.4.1766
35. Doherty LS, Cullen JP, Nolan P, McNicholas WT. The human genioglossus response to negative airway pressure: stimulus timing and route of delivery. Exp Physiol. 2008;93(2):288–295. doi:10.1113/expphysiol.2007.039677
36. Ayuse T, Inazawa T, Kurata S, et al. Mouth-opening increases upper-airway collapsibility without changing resistance during midazolam sedation. J Dent Res. 2004;83(9):718–722. doi:10.1177/154405910408300912
37. Isono S, Tanaka A, Tagaito Y, Ishikawa T, Nishino T. Influences of head positions and bite opening on collapsibility of the passive pharynx. J Appl Physiol (1985). 2004;97(1):339–346. doi:10.1152/japplphysiol.00907.2003
38. Oliven A, Odeh M. Effect of positional changes of anatomic structures on upper airway dilating muscle shortening during electro- and chemostimulation. J Appl Physiol. 2006;101(3):745–751. doi:10.1152/japplphysiol.01462.2005
39. Verma M, Seto-Poon M, Wheatley JR, Amis TC, Kirkness JP. Influence of breathing route on upper airway lining liquid surface tension in humans. J Physiol. 2006;574(Pt 3):859–866. doi:10.1113/jphysiol.2005.102129
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.