Back to Journals » Risk Management and Healthcare Policy » Volume 19
Does Long-Term Care Insurance Improve Health and Shift Healthcare Utilization? Evidence from China’s Pilot Program
Received 28 February 2026
Accepted for publication 24 June 2026
Published 29 June 2026 Volume 2026:19 605993
DOI https://doi.org/10.2147/RMHP.S605993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Xinfang Li,1 Mingqiang Li,2 Zhihui Li3
1Dong Fureng Institute of Economic and Social Development, Wuhan University, Wuhan, People’s Republic of China; 2Taikang Era of Longevity Institute, Taikang Insurance Group Co., Ltd., Beijing, People’s Republic of China; 3Vanke School of Public Health, Tsinghua University, Beijing, People’s Republic of China
Correspondence: Xinfang Li, Email [email protected]
Background: China introduced long-term care insurance (LTCI) pilot programs in 2016 to address the growing care needs of an aging population and the increasing number of disabled older adults. While LTCI is expected to improve health and reduce the financial burden of care, its broader impacts on healthcare utilization remain unclear.
Methods: Using four waves of the China Health and Retirement Longitudinal Study (CHARLS) from 2011 to 2018, this study examines the health and economic effects of LTCI using a difference-in-differences approach. The analysis focuses on middle-aged and older adults with functional disabilities in 15 pilot cities that implemented LTCI between 2016 and 2017, compared with individuals in non-pilot cities.
Results: The results show that LTCI is associated with improvements in self-reported health and memory function. In addition, LTCI is associated with reductions in inpatient visits and associated medical expenditures and an increase in outpatient visits, suggesting a shift in healthcare utilization from inpatient to outpatient services.
Conclusion: These findings from pilot cities and observational longitudinal survey data suggest that LTCI may contribute to improved health outcomes. The results provide new empirical evidence on the broader impacts of LTCI and offer policy implications for countries facing rapid population aging.
Keywords: long-term care insurance, health status, healthcare utilization, medical expenses, difference-in-differences model
Introduction
According to the United Nations World Population Prospects 2022, the global population aged 65 and older is projected to rise from 10% in 2022 to 16% by 2050, intensifying the worldwide demand for long-term care. This challenge is particularly acute in China. Data from the Seventh National Population Census reveals that by the end of 2020, China’s population aged 60 and above had reached 260 million (18.7% of the total), with 190 million aged 65 or older—accounting for roughly one-fifth of the global elderly population.1 The burden is further amplified by the growing number of disabled older adults. According to China’s Fifth National Sample Survey on the Living Conditions of the Elderly, approximately 35 million disabled older adults live in the country, accounting for 11.6% of the total elderly population. Projections suggest this number will rise to 46 million by 2035 and approximately 58 million by 2050. With the increasing proportion of the aging population and the growing number of disabled older adults, the traditional family-based informal care system is under unprecedented pressure. Shifting family structures, characterized by smaller household sizes, declining intergenerational co-residence, and increasing female labor force participation, have significantly weakened the caregiving capacity of younger generations. Urbanization and socioeconomic transformation have further weakened familial care norms.2 Against this backdrop, the development and implementation of LTCI policies have become increasingly critical for addressing the dual challenges of population aging and disability care.
Since the mid-20th century, several countries have established LTCI systems in response to population aging and its associated health and social care challenges. European nations such as the Netherlands and Germany, along with Asian countries including Japan and South Korea, were early adopters of comprehensive LTCI frameworks.3–6 Inspired by these international experiences, China has gradually developed its own LTCI system. In response to the urgent need for care services for disabled older adults, the Ministry of Human Resources and Social Security issued the “Guiding Opinions on the Pilot Implementation of Long-Term Care Insurance” in 2016. We examined 15 pilot cities that launched LTCI in 2016 and 2017.
There is an intrinsic and inseparable relationship between individual health status and socioeconomic development.7 Social security is often considered an important factor influencing the health of middle-aged and older adults,8 and LTCI constitutes a key institutional arrangement for a comprehensive social security system.9 China has acknowledged the necessity of developing a resilient and sustainable healthcare and insurance framework to adequately address the changing requirements of its aging demographic and the associated growing need for long-term care services.10 In this context, it is essential to empirically assess the health and economic effects of LTCI in China, to provide evidence for policymaking and improve the well-being of the aging population. This study aims to provide rigorous empirical evidence on the impact of LTCI on health outcomes and medical expenditures among middle-aged and older adults. Specifically, this study aims to answer the following questions: (1) Does LTCI participation improve health outcomes among disabled middle-aged and older adults? (2) How does LTCI affect healthcare utilization patterns and medical expenditures? (3) Are these effects heterogeneous across different subgroups? By doing so, it contributes to the refinement of China’s LTCI policy framework and offers valuable insights for other countries navigating similar demographic transitions.
Literature Review
In recent years, many countries have established LTCI systems, and both domestic and international scholars have conducted extensive research on their institutional design and policy development. Nevertheless, studies specifically examining the health and economic effects of LTCI remain relatively limited, and the available evidence is often mixed. In this context, this review draws on existing literature from two principal perspectives, health effects and economic effects, to develop a comprehensive understanding of the current state of knowledge and to identify important gaps that this study aims to address.
Health Effects of LTCI
Research on the health effects of LTCI remains relatively scarce, and findings on specific outcomes are often inconclusive. Existing studies can be broadly categorized into two strands. The first strand suggests positive effects of LTCI on health. For example, evidence from China indicates that LTCI participation improves self-reported health, enhances functional ability, and reduces depressive symptoms among older adults.11–17 Studies from South Korea also demonstrate that LTCI not only improves self-reported health and cognitive function but also is associated with lower mortality risk among beneficiaries compared to non-beneficiaries.18–20 The second strand of research reports that LTCI has not produced favorable impacts on health. Tamiya et al21 found that LTCI did not significantly improve subjective health status or activities of daily living (ADL) among older care recipients. These findings are similar to those of another study of the effect of LTCI,22 indicating that for frail older adults, the preservation of health and functional status may represent a more attainable objective than their improvement.
Economic Effects of LTCI
In addition to its health implications, a growing body of research has examined the economic effects of LTCI, particularly with respect to medical expenditures and healthcare utilization. The introduction of LTCI is generally expected to alleviate the financial burden of long-term care, reduce medical expenditures, and improve the efficiency of healthcare utilization. However, there is no consensus in the existing body of research. Some studies have found that LTCI significantly reduces medical expenditures and the frequency of medical visits.23,24 Chen and Ning25 examined the treatment effect of the LTCI policy on healthcare utilization and out-of-pocket (OOP) health expenditures in China. Regarding healthcare utilization, the implementation of LTCI led to a marked decline in outpatient visits, hospital admissions, and the duration of hospital stays over the past year. In terms of OOP, they found that LTCI lowers both inpatient and total OOP expenditures. International evidence also supports the economic benefits of LTCI. Research from South Korea indicates that the introduction of LTCI program has contributed to shorter hospital stays among older adults.26 Similarly, studies in Spain have shown that LTCI reduces hospital admissions and length of stay.27 Nevertheless, the economic effects of LTCI are not uniformly positive. For example, evidence from England finds that reductions in public long-term care spending had no impact on the use of more costly health care services, resulting in little impact on overall hospital costs.28 Some studies have found mixed effects of LTCI on medical expenditures.25,29
Given the universal challenge of population aging and the increasing strain on healthcare systems worldwide, evaluating the effectiveness of LTCI is critical for sustainable policy development. Building on this global imperative, this study makes several important contributions to the growing literature on LTCI. First, while existing studies often rely on broad population samples or self-reported disability status, we enhance identification accuracy by defining the treatment group more rigorously, specifically focusing on individuals with functional disabilities as measured by standardized ADL scores. By restricting the analysis to those with moderate to severe functional limitations, our estimates better reflect the true policy impact on the intended target population, thereby reducing selection bias and improving causal inference. Second, we provide a comprehensive assessment of LTCI’s effects across multiple dimensions, including both health outcomes and healthcare costs. Rather than focusing solely on self-reported health or utilization frequency, we examine a multidimensional set of outcomes: physical health (self-reported health), cognitive function (memory score), mental health (CES-D), healthcare utilization (inpatient and outpatient visits), and medical expenditures (inpatient and outpatient costs). This holistic approach allows for a more comprehensive understanding of how LTCI influences both individual well-being and system-level efficiency. Third, beyond simply documenting average treatment effects, we conduct detailed heterogeneity analyses across key demographic and socioeconomic subgroups by urban/rural residence, gender, and age group, shedding light on which subpopulations benefit most from the program—a critical consideration for designing equitable LTCI policies in both China and other countries facing rapid demographic transitions. Together, these methodological and analytical advancements allow us to not only generate more precise and policy-relevant estimates of LTCI’s impacts but also to identify which subpopulations benefit most and which may be left behind. By addressing these critical gaps, this study strengthens the empirical foundation for refining China’s LTCI policy and offers transferable insights for other aging societies seeking equitable and sustainable long-term care solutions.
Materials and Methods
Data Source
This study utilizes data sourced from CHARLS, which is administered by the National School of Development at Peking University. Its baseline wave, conducted in 2011, encompassed 17,706 individuals from around 10,000 households, spanning 150 counties/districts and 450 villages/neighborhood communities throughout China. We selected CHARLS for three main reasons. First, LTCI primarily targets older adults at risk of functional disability, and CHARLS covers a nationally representative sample of individuals aged 45 and above, aligning closely with the policy’s target population. Second, the survey includes detailed data on self-reported health, cognitive and physical function, healthcare use, and healthcare expenditure, which allowed for a comprehensive assessment of both health and economic impacts. Third, CHARLS’s broad geographical coverage includes most LTCI pilot cities, enhancing the representativeness and validity of our sample. This study uses data from 2011, 2013, 2015, and 2018 waves of CHARLS. The pre-policy period is represented by pooled data from 2011, 2013, and 2015, while the post-policy period is based on the 2018 wave.
We included all individuals aged 45 and above in the CHARLS waves (2011–2018) who provided valid responses to our key variables—specifically, the outcome variables, disability status, and all essential control variables. No additional exclusion criteria for these core variables were applied. The treatment group included older adults with mild, moderate, or severe functional disabilities, defined using three criteria based on the six basic ADLs: (1) needing help with at least one ADL; (2) reporting difficulty in at least three ADLs; or (3) being unable to perform any of the six ADLs. These ADL items aligned with the Barthel Index used in most LTCI pilot cities. However, due to differences in response formats in CHARLS (Likert-scale items), our disability definition is broader than the official LTCI eligibility criteria. Robustness checks using stricter definitions confirmed that our results remain consistent.30 To minimize selection bias, we excluded cities that launched LTCI before 2016 or after 2018. The final sample included 15 pilot cities.
Variable Selection
Dependent Variables
This study examines outcomes across two main dimensions: health outcomes and economic outcomes. Health outcomes include self-reported health, memory and mental health, capturing both subjective and objective dimensions of health. Economic outcomes include healthcare utilization (outpatient visits and inpatient visits) and medical expenditures (outpatient and inpatient cost). Self-reported health is measured on a 5-point scale ranging from 1 (very poor) to 5 (very good), with higher scores indicating better health status. Memory function is assessed on a 10-point scale, where higher scores indicate better memory performance. The CES-D score ranges from 1 to 30, with higher scores indicating worse mental health. Memory function is included because cognitive decline often accompanies functional disability, and professional care services may alleviate cognitive burden. Depressive symptoms (CES-D) are included as mental health is a key dimension of well-being among disabled older adults, and LTCI may reduce care-related stress and social isolation. All monetary values, including inpatient and outpatient costs, household consumption, and other expenditure variables, were deflated to the 2015 price level using provincial level Consumer Price Indices (CPI) obtained from the China Statistical Yearbook. This adjustment ensured that our estimates reflect real changes in purchasing power rather than nominal inflation.
Independent Variables
The central explanatory variable examined in this research is the policy impact of LTCI, which was estimated through a difference-in-differences (DID) methodology. When evaluating the impact of the LTCI on the health status, healthcare utilization and medical expenditures of the disabled elderly people, cities where the LTCI pilot policy had been implemented were designated the experimental group. Eligibility for the treatment group was determined in two steps. First, an individual was considered potentially eligible if they resided in one of the 15 pilot cities listed in Table 1 and were covered by the relevant health insurance scheme according to that city’s policy – ie., Urban Employee Basic Medical Insurance (UEBMI) in cities where LTCI initially covered only employees, or UEBMI with Urban and Rural Resident Basic Medical Insurance (URRBMI) in cities with universal coverage. Second, among those insurance eligible individuals, we further restricted the sample to those with functional disabilities as measured by the six basic ADLs: bathing, dressing, toileting, transferring, continence, and feeding. Following the common practice in LTCI evaluation studies, a person was classified as having a disability if they met at least one of three criteria: (1) needing help with at least one ADL; (2) reporting difficulty in at least three ADLs; or (3) being unable to perform any of the six ADLs.
 |
Table 1 Key Characteristics of the 15 LTCI Pilot Cities Implemented in 2016 and 2017 |
Control Variables
To reduce potential confounding bias, we included a set of control variables in the analysis, categorized into three groups: (1) individual characteristics: age, marital status, education level, and household registration. These are standard demographic controls that are correlated with both health status and the likelihood of receiving care. We control them to reduce omitted variable bias; (2) social insurance coverage, such as social health insurance and social pension insurance. These are included to isolate the specific effect of LTCI from the general effects of having social insurance coverage. This ensured that the estimated impact is attributable to LTCI benefits rather than other forms of social protection; (3) household characteristics such as number of children and consumption level. These variables are included as controls to adjust for differences in family resources and informal care availability that may independently influence both LTCI participation and health-related outcomes, thereby reducing omitted variable bias. Following prior research, we used consumption rather than income as the measure of economic resources, as it is more stable and reliable in the context of developing countries.31
Baseline Regression
The DID model is widely applied in social sciences to evaluate policy effects. Its rationale lies in constructing a counterfactual framework that compares changes in the outcome variable under two scenarios: the presence and absence of a policy intervention. The underlying premise of the parallel trends assumption is that, without the policy intervention, the treatment and control groups would have exhibited comparable outcome trajectories over time. Under this assumption, the change in the outcome for the control group before and after the policy implementation serves as a counterfactual for what would have occurred in the treatment group without the intervention. The DID estimator is then calculated as the difference between the observed change in the treatment group (D1) and the change in the control group (D2), ie., D1 – D2. This double differencing isolates the net effect of the policy, controlling for time-invariant group differences and common time trends.32–34
Existing studies have employed the DID approach to assess the effects of LTCI on the health outcomes and health disparities of older adults.35 In addition, some studies have applied the DID method to examine the impact of LTCI implementation on disability among middle-aged and older adults in China, further exploring the heterogeneity of the policy effects.36 Although the 15 pilot cities all launched LTCI in 2016 or 2017, there is minor variation in the exact starting months. However, because the CHARLS survey was conducted in 2015 and 2018, with no survey in 2016 or 2017, we treated 2016–2017 as a uniform implementation window and employed a conventional two-period DID design. This approach is consistent with the LTCI literature that used CHARLS data. The DID model is specified as follows:

Where Yijt represents a comprehensive set of individual-level outcome variables for individual i in region j at time t, including health status, healthcare utilization and healthcare expenditures. The health status is measured by self-reported health status, mental health, and memory. The healthcare utilization is measured by the frequency of annual inpatient visits and monthly outpatient visit, while healthcare expenditure is captured by inpatient and outpatient costs.  is the treatment dummy (1 if in pilot city and functionally disabled).
is the treatment dummy (1 if in pilot city and functionally disabled).  is the time dummy (1 for 2018).
is the time dummy (1 for 2018).  represents the interaction term between the treatment group (as defined above) and a dummy variable before and after the implementation of the LTCI, where the interaction term coefficient β is the core coefficient of this paper. This variable captures the disparity in outcomes between pilot cities enacting the LTCI policy and non-participating regions, thereby enabling an assessment of the policy’s effectiveness. Because the fifteen selected pilot cities all started implementing the LTCI policy in 2016 and 2017, the years 2011, 2013, and 2015 were set as before the treatment for the city samples (Postt= 0), and 2018 is set as after treatment (Postt= 1). Xijt represents a set of individual-level control variables, including demographic characteristics and socioeconomic characteristics, including age, education, consumption level, insurance status and so on. τt represents year fixed effects; ωi represents individual fixed effects; and εijt represents the error term. To account for potential correlation of errors within the same geographical area and to ensure robust inference, we clustered the standard errors at the city level in all regression models reported in this study.
represents the interaction term between the treatment group (as defined above) and a dummy variable before and after the implementation of the LTCI, where the interaction term coefficient β is the core coefficient of this paper. This variable captures the disparity in outcomes between pilot cities enacting the LTCI policy and non-participating regions, thereby enabling an assessment of the policy’s effectiveness. Because the fifteen selected pilot cities all started implementing the LTCI policy in 2016 and 2017, the years 2011, 2013, and 2015 were set as before the treatment for the city samples (Postt= 0), and 2018 is set as after treatment (Postt= 1). Xijt represents a set of individual-level control variables, including demographic characteristics and socioeconomic characteristics, including age, education, consumption level, insurance status and so on. τt represents year fixed effects; ωi represents individual fixed effects; and εijt represents the error term. To account for potential correlation of errors within the same geographical area and to ensure robust inference, we clustered the standard errors at the city level in all regression models reported in this study.
We also conducted the event study to test the parallel trends assumption:

Where k indexes the time relative to LTCI implementation, with k = −1 (year 2015) serving as the omitted reference period. Specifically, k = −3 corresponds to 2011 (three years before implementation), k = −2 corresponds to 2013 (two years before), k = 0 corresponds to the implementation period (2016–2017, when the 15 pilot cities launched LTCI), and k = 1 corresponds to the post-implementation period (2018). The coefficients βk capture the difference in outcomes between the treatment and control groups at each relative time k. The parallel trends assumption requires that the pre-policy coefficients (β-3 and β-2) are jointly and individually statistically indistinguishable from zero, indicating that the treatment and control groups followed similar trajectories before LTCI implementation. In contrast, significant post-policy coefficients (β1) would suggest that LTCI had a causal effect on the outcomes of interest. We clustered standard errors at the city level to account for within-city correlation of errors over time.
In summary, this research began by conducting descriptive statistics on the experimental group’s data to evaluate whether statistically significant differences exist in health status, healthcare utilization, and medical expenses between the treatment and control groups. Subsequently, we employed a DID approach to investigate the causal effect of the LTCI policy on health and economic outcomes among disabled older adults. To ensure the robustness of our findings, we conducted several robustness checks, including the parallel trends assumption and placebo tests. Ultimately, to examine whether the health and economic effects of LTCI differ consistently among the elderly, we conducted heterogeneity analysis across individual and regional dimensions.
Results
Descriptive Analysis
This study utilized data spanning four waves of the CHARLS (2011, 2013, 2015, and 2018), resulting in a final analytical sample of 102,436 observations from both pilot and non-pilot cities. Descriptive information on the variables is presented in Table 2. The year 2015 (t = 0) corresponded to the pre-treatment phase, prior to the rollout of the LTCI pilot in the treatment group, while 2018 (t = 1) represented the post-treatment period. First, at baseline (pre-policy period), respondents in pilot cities reported better health outcomes (self-reported health: 3.87 vs. 3.10; memory: 4.22 vs. 3.64; CES-D: 3.96 vs. 7.74) and lower healthcare utilization (inpatient visits: 0.057 vs. 0.16; outpatient visits: 0.11 vs. 0.42) compared to those in non-pilot cities. These baseline differences reflect the non-random selection of pilot cities. Importantly, the DID approach accounts for these time-invariant differences through city fixed effects, and our parallel trends tests (Figure 1) confirmed that both groups followed similar trajectories before policy implementation. Second, post-policy changes showed that pilot cities experienced improvements in health outcomes and reductions in inpatient utilization relative to their pre-policy levels, while non-pilot cities showed little change over the same period. This pattern is consistent with a policy effect, though causal interpretation requires the identifying assumptions discussed in Results.
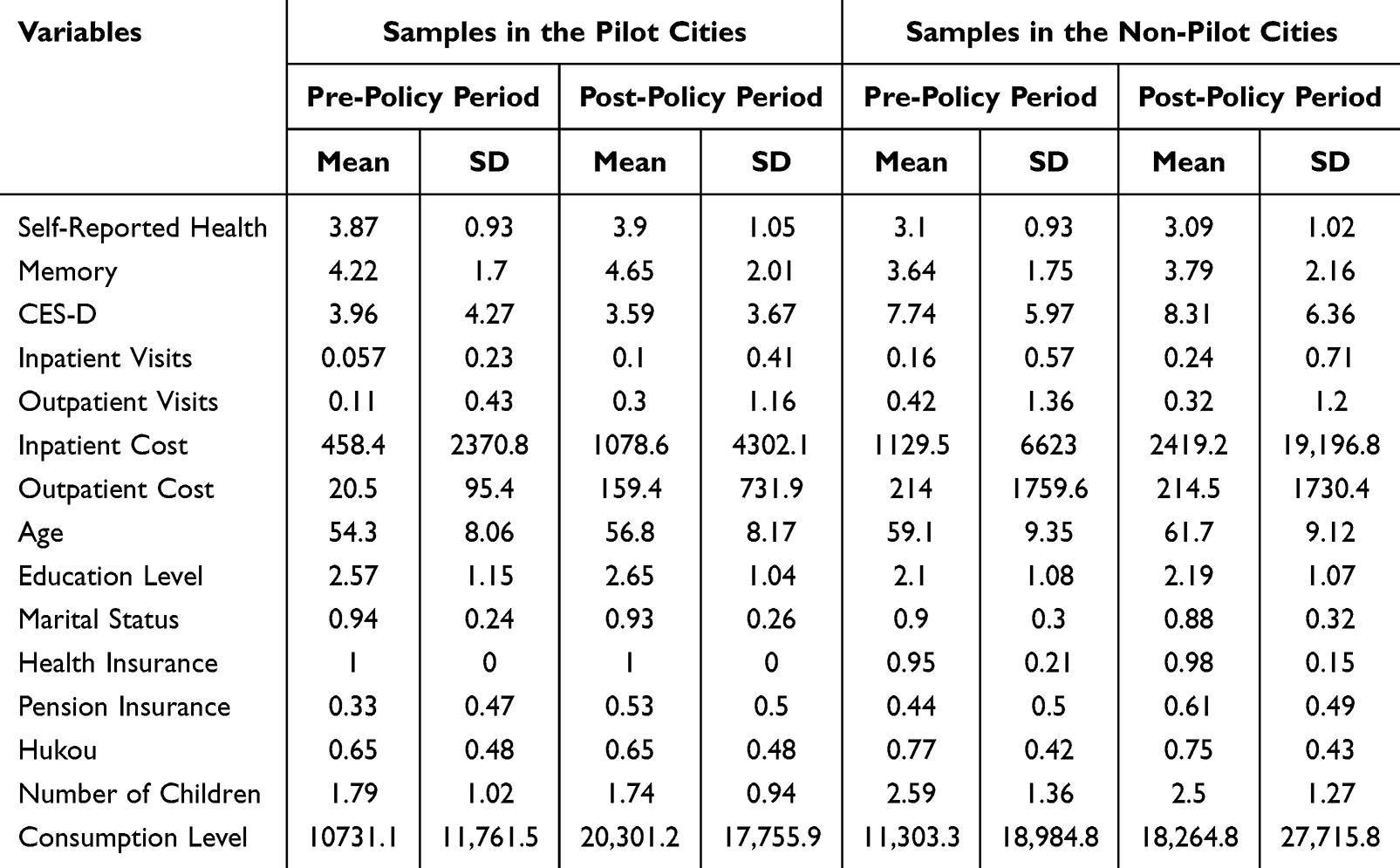 |
Table 2 Summary Statistics (CHARLS 2011–2018) |
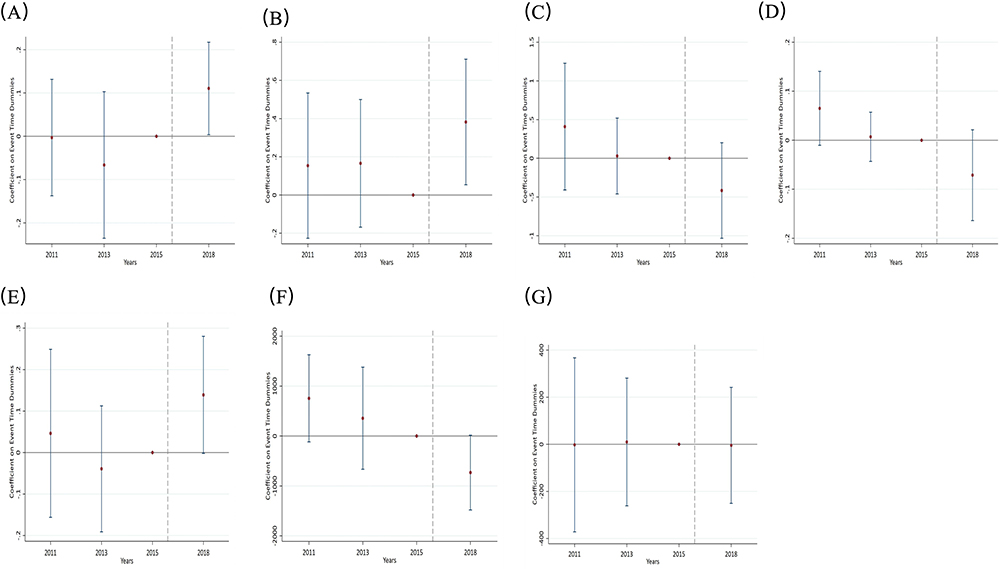 |
Figure 1 Test of the parallel trend assumption. (A) Parallel Trend Test for Self-Reported Health. (B) Parallel Trend Test for Memory. (C) Parallel Trend Test for CES-D. (D) Parallel Trend Test for Inpatient Visits. (E) Parallel Trend Test for Outpatient Visits. (F) Parallel Trend Test for Inpatient Cost. (G) Parallel Trend Test for Outpatient Cost. |
Benchmark Regression Results
Table 3 presented the benchmark regression results on the impact of LTCI on three key health outcomes: self-reported health, memory, and mental health. Mental health was assessed through the Center for Epidemiologic Studies Depression (CES-D) scale. Given the quasi-experimental nature of our DID design, we interpret the estimated coefficients as associations that are consistent with a causal interpretation under the parallel trends assumption, rather than as definitive causal claims. We found statistically significant positive effects of LTCI on both self-reported health and memory. The coefficient for the DID estimator is 0.1334 (p < 0.01) for self-reported health and 0.2988 (p < 0.05) for memory. The DID coefficient of 0.1334 represents a 0.133-point increase on a 5-point self-reported health scale (ranging from 1 = very poor to 5 = very good). Given the control group baseline mean of approximately 3.1, this corresponds to a 4.3% improvement relative to the baseline. The coefficient of 0.2988 on a 10-point memory scale (range 1–10) represents a 2.99% improvement relative to the control group baseline mean of 3.64. While modest in magnitude, this improvement is statistically significant and suggests that access to professional care may reduce cognitive burden and stress among care recipients. This indicates that, on average, the implementation of LTCI was associated with an improvement in these health dimensions among the treated population relative to the control group. The effect was particularly pronounced for memory, indicating that LTCI may reduce cognitive burden and stress for care recipients, likely by ensuring access to professional care services. However, we did not find a statistically significant average treatment effect of LTCI on mental health (CES-D score). Although the coefficient is negative, aligning with the hypothesized direction, it does not reach conventional levels of statistical significance (DID coefficient = −0.5079, p > 0.1). This suggests that while LTCI may have direct benefits on physical health and cognition, its impact on broader mental well-being might be more complex, attenuated, or require a longer time to materialize. Among the control variables, marital status emerged as a consistently significant predictor across all models. Being married was associated with better self-reported health, better memory, and better mental health, underscoring the importance of social support for the health of middle-aged and older adults.
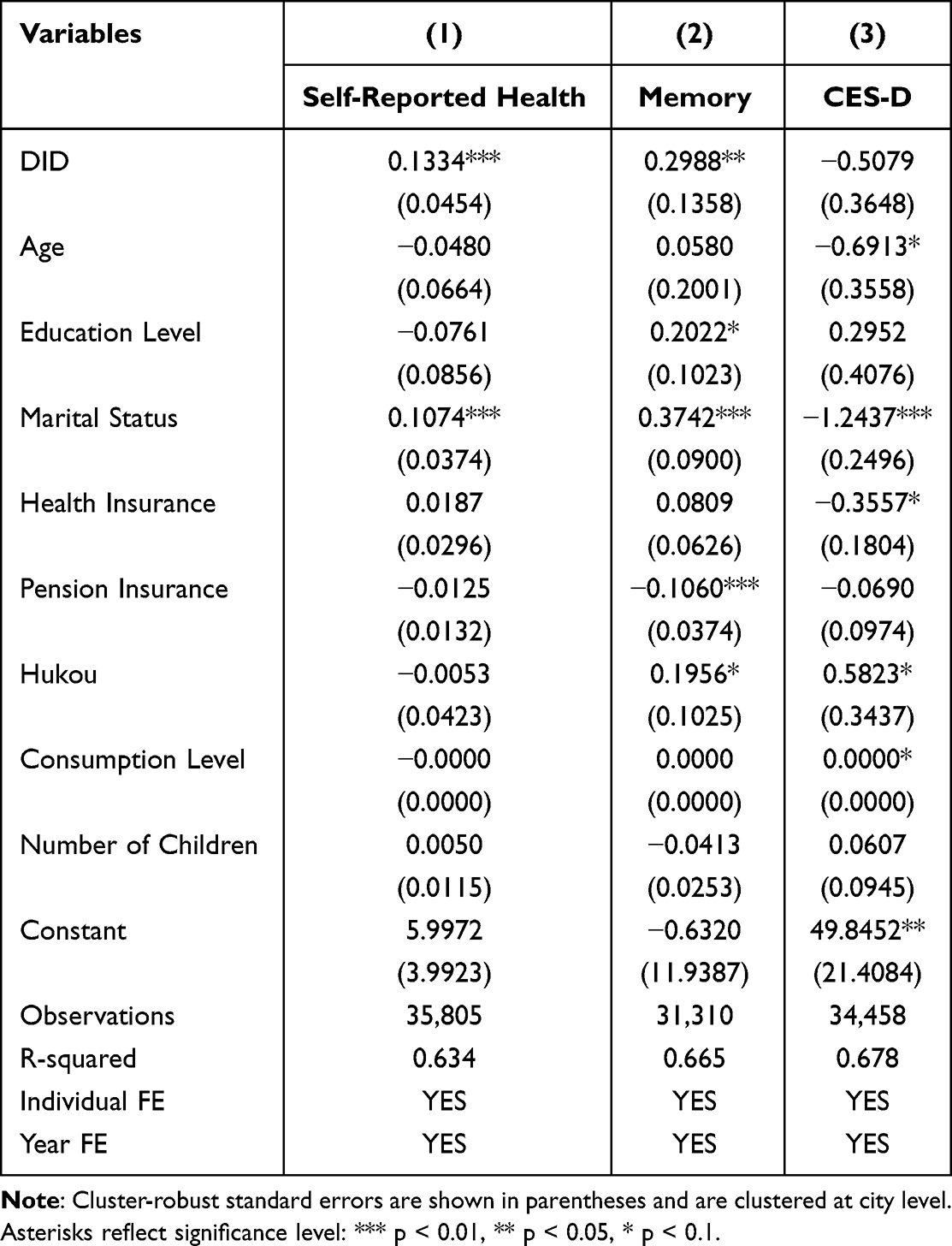 |
Table 3 The Impact of LTCI on Health Outcomes |
Table 4 presented the estimated effects of the LTCI on healthcare utilization and medical expenditures, capturing key economic dimensions of health service demand among middle-aged and older adults. The results indicated a statistically significant and economically meaningful impact of LTCI on healthcare utilization. The LTCI was associated with a reduction in the number of inpatient visits during last year by 0.0881 times (P < 0.05) and corresponds to an increase in the number of outpatient visits during last month by 0.142 times. The reduction of 0.0881 inpatient visits per year, relative to a control group baseline of 0.16 visits, represents a 55% decrease in the annual number of hospitalizations. The reduction of approximately 1,025 yuan in inpatient costs suggests a substantial decrease in inpatient healthcare expenditures among LTCI beneficiaries. This substitution effect suggested that a shift in healthcare utilization patterns following LTCI implementation, consistent with a quasi-experimental interpretation, likely by improving access to community-based and preventive care. From the perspective of medical expenditures, enrollment in the LTCI significantly reduced inpatient costs by approximately 1,024.67 yuan (p < 0.01). However, LTCI did not exhibit a significant effect on outpatient costs, suggesting that the increased utilization of outpatient services did not lead to a substantial rise in overall spending in this category.
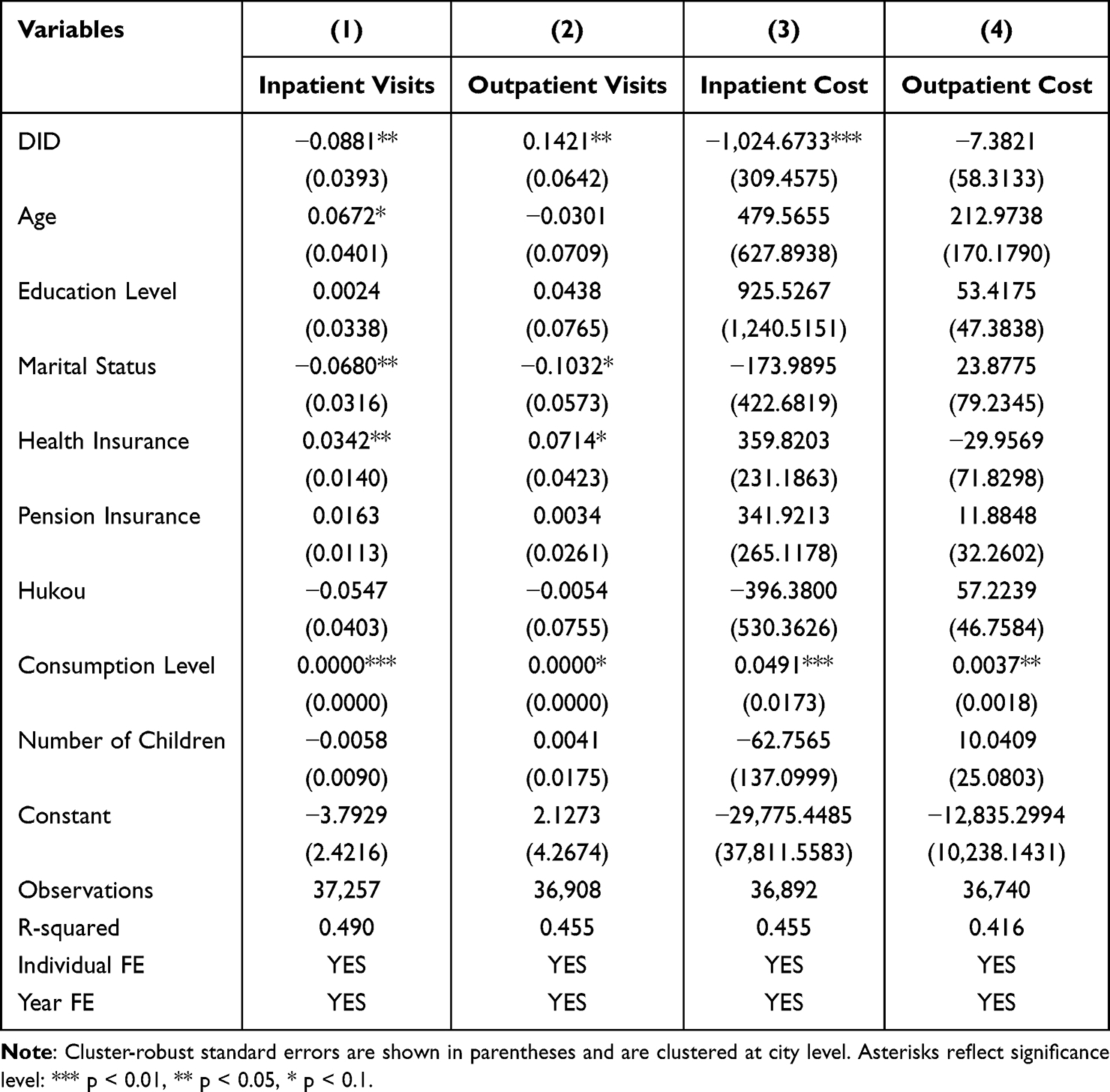 |
Table 4 The Impact of LTCI on Economic Outcomes |
Robustness Test
As evidenced by the preceding empirical analysis, the implementation of LTCI correlated with enhanced health outcomes and decreased inpatient service use and associated costs among middle-aged and older residents in the pilot cities. To verify the robustness of these findings, the fifteen pilot cities were included for further robustness testing of the empirical results.
Parallel Trend Test
The parallel trends test is an analytical approach used to assess whether the treatment and control groups followed similar trajectories over time before the implementation of the policy, thereby ensuring the validity of the DID framework.37,38 Figure 1 presented the event-study estimates for health status, healthcare utilization, and medical expenditures, with 2011 and 2013 representing pre-treatment periods and 2018 the post-treatment period. The coefficients for the pre-policy periods (2011 and 2013) were statistically insignificant (with confidence intervals containing zero), indicating no differential trends between the treatment and control groups prior to the policy implementation. In contrast, some coefficients for the post-policy period (2018) were statistically significant for key outcomes, confirming the policy’s impact. This pattern supports the parallel trends assumption required for DID estimation.
Based on these findings, we further examined the policy’s effects in the post-implementation period. The results indicated that the LTCI policy exerted significant impacts across multiple dimensions. In terms of health outcomes, the policy was associated with notable improvements in self-reported health and memory function. In the domain of healthcare utilization and expenditures, we observed a clear substitution effect: a statistically significant reduction in both the frequency and cost of inpatient services, accompanied by an increase in outpatient visits. Notably, total outpatient costs did not rise significantly. When combined with the considerable reduction in inpatient cost, these findings suggested that the policy was associated with not only an improvement in health outcomes but also in the overall efficiency of the healthcare system through better resource allocation. From the trend changes observed in Figure 1, the LTCI policy has exerted a significant influence on health status, healthcare utilization, and medical expenditures among middle-aged and older adults in the fifteen pilot cities, demonstrating its multifaceted impact on both individual well-being and the healthcare system.
Placebo Test
(Figure 2A–C) displayed the kernel density distributions of the DID coefficients obtained from random reassignment of treatment status. The red solid line indicated the true coefficient from the baseline regression, while the dashed line represented the mean of the 1,500 placebo coefficients. The placebo coefficients were tightly centered around zero, with the mean substantially deviating from the true estimate. This provided strong evidence that the observed effects are not attributable to coincidental patterns or unmeasured time-varying factors. Further supporting evidence was provided by the p-value scatter plots in (Figure 2B–D). Most p-values were concentrated near zero, with only a small fraction falling below the 10% significance threshold (dashed line). These results confirmed that the p-value plots offer more concise and informative validation of the robustness of our findings. Together, these placebo tests demonstrated that the estimated impacts of the LTCI pilot on health and economic outcomes are policy-driven and statistically distinct from noise. We also conducted robustness checks using confidence intervals and log-transformed cost to address the right-skewed nature of healthcare expenditure data, as reported in Appendix A (Tables A1 and A2).
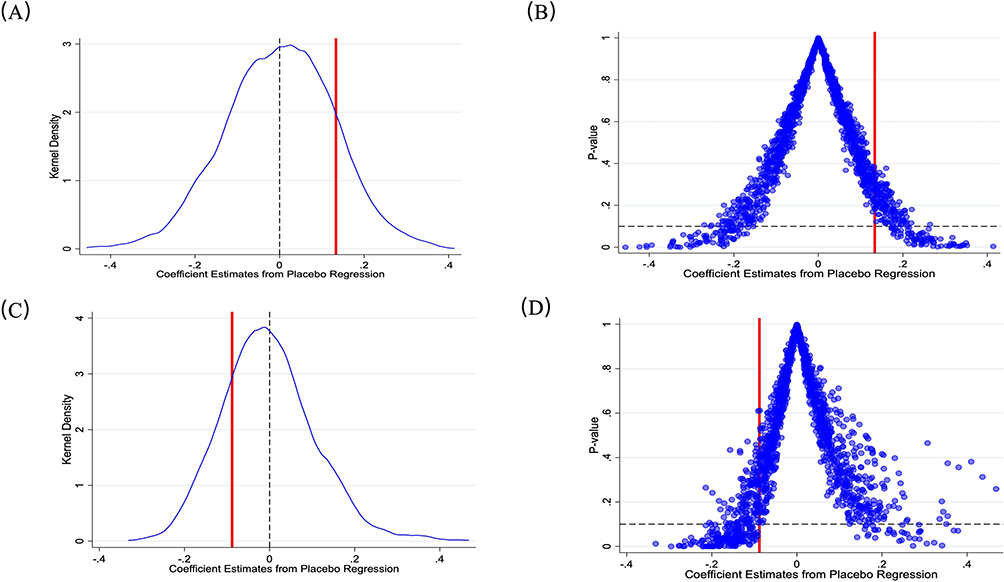 |
Figure 2 Placebo test for LTCI. (A) Coefficient Distribution of Self-Reported Health. (B) P-value Distribution of Self-Reported Health. (C) Coefficient Distribution of Inpatient Visits. (D) P-value Distribution of Inpatient Visits. |
Heterogeneity Analysis
Hukou Status Heterogeneity Analysis
We divided the sample by hukou status, distinguishing urban from rural residents, to examine whether the effects of LTCI vary across these institutional and socioeconomic groups. As shown in Table 5, the estimated effects of LTCI exhibited notable disparities between urban and rural residents.
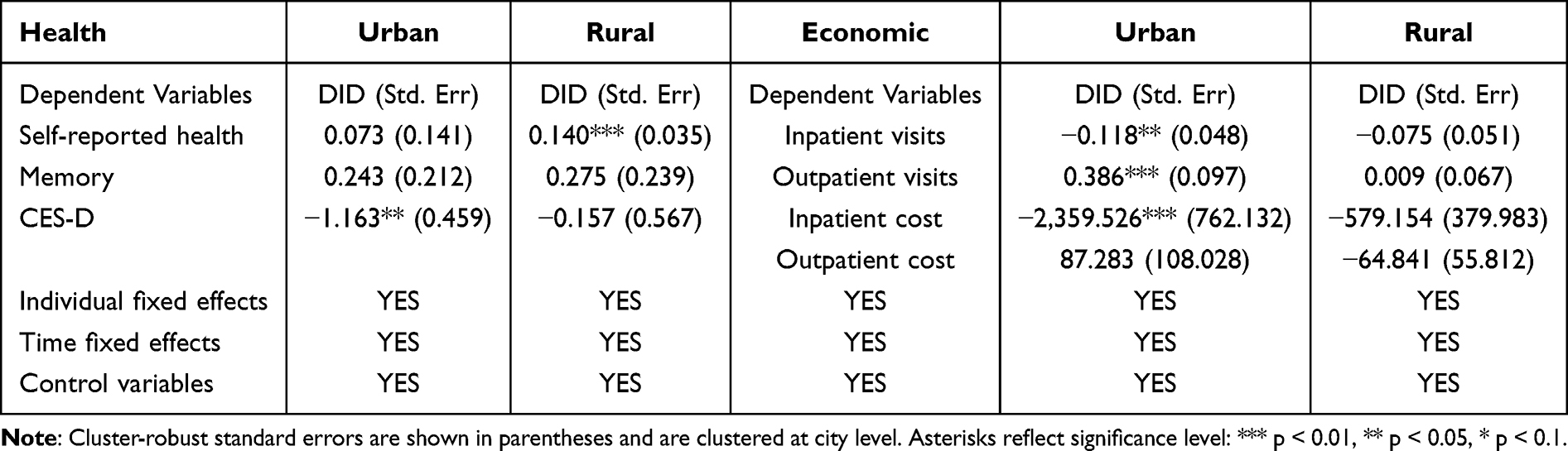 |
Table 5 Heterogeneous Results of Hukou Status |
In terms of health outcomes, LTCI was associated with improvement in self-reported health among rural residents (DID coefficient = 0.140, p < 0.01), whereas the effect for urban residents is positive but statistically insignificant. Memory function showed no significant improvement in either group. For mental health, LTCI significantly reduces depressive symptoms among urban residents (DID coefficient = –1.163, p < 0.05), but no such effect was observed in rural areas.
Regarding healthcare utilization and expenditures, LTCI was associated with a reduction in inpatient visits among urban residents (DID coefficient = –0.118, p < 0.05). Moreover, outpatient visits increased significantly in urban areas (DID coefficient = 0.386, p < 0.01), suggesting a substitution from inpatient to outpatient care. Consistent with this pattern, inpatient costs declined significantly for urban residents, while no significant reduction was found for rural residents. Outpatient costs remained unchanged across both groups.
In summary, the results revealed clear heterogeneity in the impacts of LTCI by hukou status: rural residents benefited more in terms of physical health (self-reported health), while urban residents experienced greater improvements in mental health and reductions in inpatient care use and costs. These findings highlighted the differential access to and utilization of health and long-term care services across China’s urban–rural divide.
Gender Heterogeneity Analysis
To examine whether the effects of LTCI vary by gender, we divided the sample into male and female subgroups. This analysis aims to uncover potential differences in how men and women benefit from the program in terms of health outcomes and economic burdens. As shown in Table 6, the estimated impacts of LTCI differed meaningfully between genders.
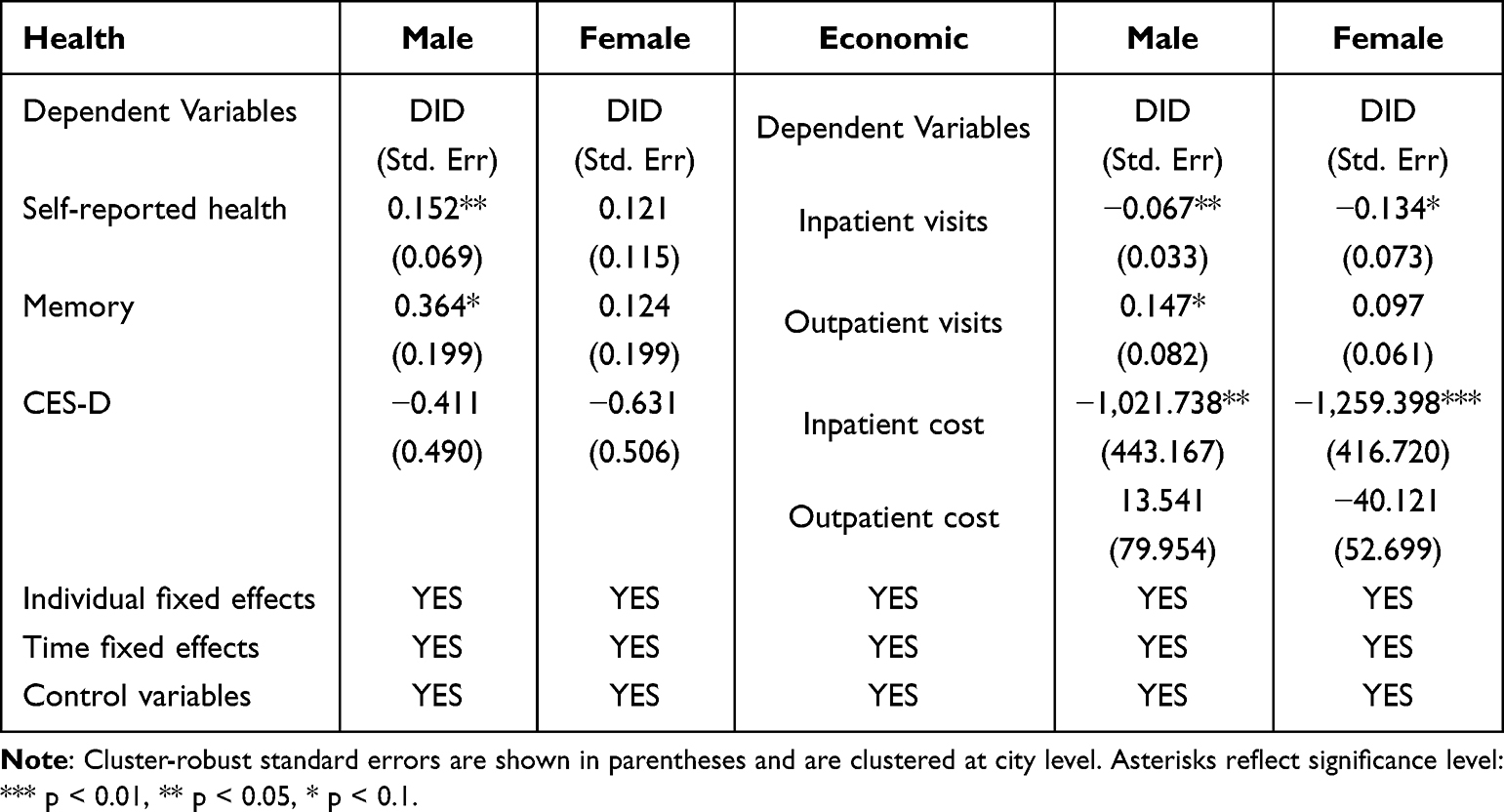 |
Table 6 Heterogeneous Results of Gender |
In terms of health outcomes, LTCI significantly improved self-reported health among males (DID coefficient = 0.152, p < 0.05), while the effect for females was positive but statistically insignificant. Similarly, memory function showed a marginally significant improvement among males (DID coefficient = 0.364, p < 0.10), whereas females exhibited a smaller, non-significant gain (DID coefficient = 0.124). No significant effects on depressive symptoms were observed for either gender.
Regarding healthcare utilization and expenditures, LTCI significantly reduced inpatient visits for both groups, with a larger reduction among males. Outpatient visits increased significantly for males (DID coefficient = 0.147, p < 0.10), indicating a shift from inpatient to outpatient care, especially among men. In line with these utilization patterns, inpatient costs declined significantly for both males and females, while outpatient costs remained unchanged across genders.
Overall, the health and economic effects of LTCI demonstrated notable gender heterogeneity. The policy benefited males more in terms of subjective health perceptions, such as self-reported health and memory function, whereas females experienced more pronounced advantages in the alleviation of objective economic burdens. Potential explanations for this disparity include, first, the fact that women often disproportionately assume the role of informal caregivers within families. By providing formal care services, LTCI significantly reduced caregivers’ burden and stress among females, which may directly translate into fewer health issues and lower medical expenditures. Second, as traditional care recipients, males showed more evident improvements in direct quality of life and health status after accessing formal care services, thereby exhibiting significant gains in self-reported health and cognitive function.
Age-Group Heterogeneity Analysis
The sample was stratified into two groups according to age, distinguishing younger elderly (<70 years) from older elderly (≥70 years). A comparative analysis was conducted to provide deeper insights into the role of LTCI. As presented in Table 7, a DID empirical analysis was performed across age groups to evaluate the impact of LTCI on health outcomes and medical expenditures. Overall, the results revealed notable heterogeneity, indicating that the effects of LTCI on health and medical spending varied substantially between different age groups.
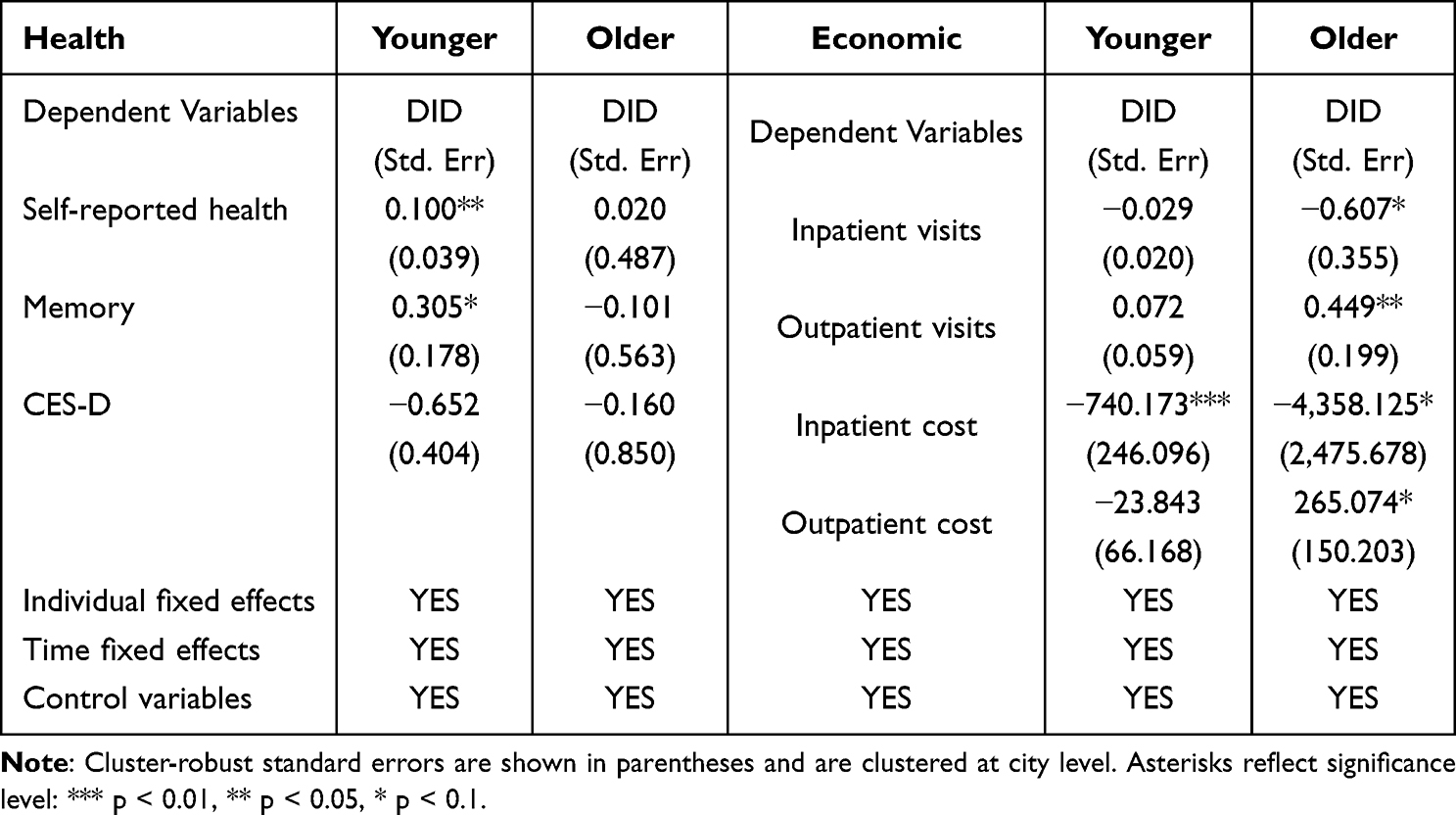 |
Table 7 Heterogeneous Results of Age Group |
In terms of health outcomes, LTCI significantly improved the self-reported health of younger elderly (DID coefficient = 0.100, p < 0.05), while the effect on older elderly was positive but statistically insignificant. Memory function also improved among the younger elderly (DID coefficient = 0.305, p < 0.1). LTCI showed no significant effect on depressive symptoms for either group.
Regarding healthcare utilization and expenditures, LTCI significantly reduced inpatient visits among older elderly (DID coefficient = –0.607, p < 0.1). Additionally, outpatient visits increased significantly among the older elderly (DID coefficient = 0.449, p < 0.05), suggesting a substitution effect between inpatient and outpatient care. Meanwhile, LTCI markedly reduced inpatient costs for both age groups. LTCI significantly increased outpatient costs among older elderly.
Overall, the younger elderly primarily gained health benefits, while the older elderly mainly obtained economic benefits. Several factors may explain this pattern. First, older elderly are typically high-frequency users of medical services, particularly inpatient care. The home-based and community care services provided by LTCI can effectively prevent or substitute for certain hospitalization needs, thereby significantly alleviating their financial burden. Second, LTCI serves as a policy tool that effectively reduced catastrophic health expenditure among older elderly, resulting in notable economic impacts.
Discussion
Several factors may explain the lack of a statistically significant average treatment effect on depressive symptoms (CES-D). First, mental health improvements may require longer exposure to LTCI than physical health outcomes. Our post-policy period was limited to 2018 (approximately 1–2 years after policy implementation), which may be too short for measurable changes in depressive symptoms to materialize. Psychological well-being often changes more slowly than self-reported physical health, as it depends on cumulative experiences of care quality, social engagement, and reduced caregiver stress over extended periods. Second, the CES-D measure captures a broad range of depressive symptoms such as depressed mood, loneliness, and sleep disturbance. LTCI may affect specific subdomains, including reducing worry about care needs or loneliness through regular social contact with caregivers, without shifting the overall composite score. Unfortunately, our data did not allow us to examine subdomain-specific effects. Third, our sample included both mild and severe functional limitations; the mental health benefits of LTCI may be concentrated among those with more severe disabilities who experience greater relief from care burden. Future research with longer follow-up periods, more diverse mental health measures, and larger samples to support subgroup analyses is needed to fully understand the relationship between LTCI and mental health.
The observed substitution from inpatient to outpatient care is a central finding of this study, and several mechanisms may explain this pattern. First, by providing home-based and community-based care services, LTCI may prevent or delay the onset of acute conditions that would otherwise require hospitalization. Regular monitoring by formal caregivers enables earlier detection of health deterioration, allowing timely outpatient intervention before conditions escalates to emergency or inpatient care. Second, from a health system perspective, LTCI may facilitate better care coordination between outpatient providers and long-term care services. When community health centers and LTCI providers share information and coordinate care plans, outpatient management becomes more effective, further reducing the need for inpatient care. Third, LTCI may improve medication adherence and chronic disease management. Professional caregivers can ensure that older adults take medications as prescribed, attend follow-up appointments, and follow treatment plans, which reduces the likelihood of complications requiring hospitalization. Fourth, the substitution effect may also reflect financial incentives. For older adults and their families, reduced out-of-pocket costs for outpatient services (through better insurance coverage or subsidies) may make outpatient care more affordable relative to inpatient care, shifting demand toward less intensive settings. While our data did not allow us to empirically distinguish these mechanisms, they provide a framework for future research.
The design of China’s LTCI pilots varies significantly across cities, particularly in benefit packages, financing, and eligibility (see Appendix A, Table A3). For instance, some cities offer only in-kind services while others include cash benefits; disability thresholds range from severe to moderate; and financing sources differ. These design choices likely influence health and utilization outcomes. Generous in-kind services may better support the shift from inpatient to outpatient care, whereas cash benefits could alter healthcare-seeking behavior differently. Because our main analysis pooled all pilot cities, these average effects might mask such underlying heterogeneity. Future studies with larger samples should formally test how specific design elements moderate LTCI’s impact.
Supply-side factors, especially regional healthcare infrastructure, also play a role. In cities with strong community health centers and ample outpatient capacity, LTCI’s focus on preventive care can more effectively reduce avoidable hospitalizations. Conversely, where outpatient access is limited by long waits or provider shortages, patients may still default to inpatient care, weakening this substitution effect. Thus, our interpretation of this shift as an efficiency gain should be viewed as suggestive rather than definitive.
Regarding generalizability, our findings stemmed from China’s unique institutional setting—social insurance tied to medical schemes, local policy discretion, and a strong family-care culture. While this differs from many other low- and middle-income countries (LMICs), the core link between LTCI, improved health, and a shift toward outpatient care offers useful lessons for aging LMICs. However, the actual impact will depend heavily on local infrastructure, labor markets, and cultural norms, so direct policy transfer requires caution and local piloting.
Finally, while our subgroup analyses revealed interesting gender patterns, we lacked direct data on caregiver burden or informal care hours. Therefore, our interpretations of these gender differences are exploratory. Without caregiver-level data, the link between LTCI and the hypothesized mechanism of caregiver relief remains theoretical. Future research needs detailed data on informal care and caregiver well-being to fully understand how LTCI operates at the household level.
Conclusion
Based on data from the CHARLS and employing a DID approach, our study found that the LTCI policy was associated with an improvement in the self-reported health and memory function of the enrolled population while optimizing healthcare resource allocation by substituting outpatient for inpatient care.
A key limitation of this study is that only one post policy wave (2018) was available, which prevents us from examining longer term effects or dynamic treatment patterns. While our event study design confirmed parallel pre trends and showed a significant immediate response, we could not assess whether the observed improvements are sustained, fade, or grow over time. To partially mitigate this concern, we conducted placebo tests using a falsified policy year (2015), which yielded null results, supporting that the 2018 changes were indeed associated with the actual policy rollout rather than pre-existing trends. Nonetheless, future research is needed to evaluate the persistence and long run evolution of LTCI effects.
Based on the empirical results, this study puts forward the following suggestions for consideration: First, where fiscally sustainable, extending the coverage of LTCI could be considered as one of the policy instruments to address the care needs of an aging population and mitigate household medical financial burdens. Second, equity and targeting remain critical. Our findings suggest that special attention could be directed toward strengthening long-term care service infrastructure in rural areas to reduce regional disparities in service accessibility. Finally, future policy design may benefit from incorporating a life-cycle perspective, such as exploring supportive measures for family caregivers alongside professional community-based care services to maximize the dual benefits of LTCI on health and economic efficiency.
Readers should note that these findings are based on LTCI pilot cities with heterogeneous implementation designs and observational data; therefore, the results should be interpreted with caution and may not be directly generalizable without considering local contextual factors and policy design specifics. Given China’s unique institutional features, direct generalizability to other countries is limited. However, for other middle-income nations experiencing rapid demographic aging and a high reliance on hospital-based care, the Chinese experience provides a valuable reference for how public insurance can catalyze the transition toward more efficient, home- and community-based care models.
Ethics Approval and Consent to Participate
All CHARLS surveys were approved by the Institutional Review Board (IRB) of Peking University (approval number: IRB00001052-11015), and written informed consent was obtained from all participants at the time of data collection. This study is a secondary analysis of publicly available, de-identified data from the CHARLS. In accordance with Article 32, Items 1 and 2 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023), research using de-identified, publicly available data without identifiable personal information meets the criteria for ethical review exemption. Therefore, additional ethical approval from the authors’ institutional review board was not required for this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Chen L, Zhang L, Xu X. Review of evolution of the public long-term care insurance (LTCI) system in different countries: influence and challenge. BMC Health Serv Res. 2020;20:1057. doi:10.1186/s12913-020-05878-z
2. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174. doi:10.1016/j.arr.2020.101174
3. Maarse JA, Jeurissen PP. The policy and politics of the 2015 long-term care reform in the Netherlands. Health Policy. 2016;120:241–16. doi:10.1016/j.healthpol.2016.01.014
4. Nadash P, Doty P, von Schwanenflugel M. The german long-term care insurance program: evolution and recent developments. Gerontologist. 2018;58:588–597. doi:10.1093/geront/gnx018
5. Iwagami M, Tamiya N. The long-term care insurance system in japan: past, present, and future. JMA J. 2019;2:67–69. doi:10.31662/jmaj.2018-0015
6. Kim H, Kwon S. A decade of public long-term care insurance in South Korea: policy lessons for aging countries. Health Policy. 2021;125:22–26. doi:10.1016/j.healthpol.2020.11.003
7. Wang Y, Feng X, Chai Y, et al. Coupling coordination relationship between health resource allocation and regional economic development: an empirical study based on five provinces in eastern China. Front Public Health. 2024;12:1513188. doi:10.3389/fpubh.2024.1513188
8. Liu J, Rozelle S, Xu Q, Yu N, Zhou T. Social engagement and elderly health in China: evidence from the China Health and Retirement Longitudinal Survey (CHARLS). Int J Environ Res Public Health. 2019;16. doi:10.3390/ijerph16020278
9. Wang Q, Abiiro GA, Yang J, Li P, De Allegri M. Preferences for long-term care insurance in China: results from a discrete choice experiment. Soc Sci Med. 2021;281:114104. doi:10.1016/j.socscimed.2021.114104
10. Chen S, Li L, Jiao L, et al. Long-term care insurance in China: current challenges and recommendations. J Glob Health. 2024;14:03015. doi:10.7189/jogh.14.03015
11. An R, Xiu S, Yang X, Wang S. The impact of long-term care insurance on the health status and healthcare expenditure of older adults in China. Front Psychiatry. 2024;15:1514603. doi:10.3389/fpsyt.2024.1514603
12. He W, Liu H. The system effect and group benefit equity of long-term care insurance from the perspective of short-term policy pilot. Front Public Health. 2025;13:1580349. doi:10.3389/fpubh.2025.1580349
13. Chen Q, Ma S, Lyu X. Effects of long-term care insurance on health: a study of the middle-aged and older adult in pilot cities in China. Front Public Health. 2025;13:1498105. doi:10.3389/fpubh.2025.1498105
14. Chen Y, Zhao H. Long-term care insurance, mental health of the elderly and its spillovers. Front Public Health. 2023;11:982656. doi:10.3389/fpubh.2023.982656
15. Tang Y, Chen T, Zhao Y, Taghizadeh-Hesary F. The impact of the long-term care insurance on the medical expenses and health status in China. Front Public Health. 2022;10:847822. doi:10.3389/fpubh.2022.847822
16. Chen L, Xu X. Effect evaluation of the Long-Term Care Insurance (LTCI) system on the health care of the elderly: a review. J Multidiscip Healthc. 2020;13:863–875. doi:10.2147/JMDH.S270454
17. Lei X, Bai C, Hong J, Liu H. Long-term care insurance and the well-being of older adults and their families: evidence from China. Soc Sci Med. 2022;296:114745. doi:10.1016/j.socscimed.2022.114745
18. Kim H, Mitra S. The economic and health effects of long-term care insurance: new evidence from Korea. J Econo Ageing. 2022;23:100412. doi:10.1016/j.jeoa.2022.100412
19. Choi JK, Joung E. The association between the utilization of long-term care services and mortality in elderly Koreans. Arch Gerontol Geriatr. 2016;65:122–127. doi:10.1016/j.archger.2016.03.013
20. Ju YJ, Nam CM, Lee SG, Park S, Hahm MI, Park EC. Evaluation of the South Korean national long-term care insurance-funded cognitive function training programme for older people with mild dementia. Age Ageing. 2019;48:636–642. doi:10.1093/ageing/afz067
21. Tamiya N, Noguchi H, Nishi A, et al. Population ageing and wellbeing: lessons from Japan’s long-term care insurance policy. Lancet. 2011;378:1183–1192. doi:10.1016/S0140-6736(11)61176-8
22. Takahashi M. Insurance coverage, long-term care utilization, and health outcomes. Eur J Health Econ. 2023;24:1383–1397. doi:10.1007/s10198-022-01550-x
23. Che T, Li J, Li J, Chen X, Liao Z. Long-term care needs and hospitalization costs with long-term care insurance: a mixed-sectional study. Front Public Health. 2024;12:1226884. doi:10.3389/fpubh.2024.1226884
24. Feng J, Wang Z, Yu Y. Does long-term care insurance reduce hospital utilization and medical expenditures? Evidence from China. Soc Sci Med. 2020;258:113081. doi:10.1016/j.socscimed.2020.113081
25. Chen H, Ning J. The impacts of long-term care insurance on health care utilization and expenditure: evidence from China. Health Policy Plan. 2022;37:717–727. doi:10.1093/heapol/czac003
26. Kim JH, Lee Y. Implementation of long-term care and hospital utilization: results of segmented regression analysis of interrupted time series study. Arch Gerontol Geriatr. 2018;78:221–226. doi:10.1016/j.archger.2018.07.007
27. Costa-Font J, Jimenez-Martin S, Vilaplana C. Does long-term care subsidization reduce hospital admissions and utilization? J Health Econ. 2018;58:43–66. doi:10.1016/j.jhealeco.2018.01.002
28. Crawford R, Stoye G, Zaranko B. Long-term care spending and hospital use among the older population in England. J Health Econ. 2021;78:102477. doi:10.1016/j.jhealeco.2021.102477
29. Dong J, Smieliauskas F, Konetzka RT. Effects of long-term care insurance on financial well-being. Geneva Pap Risk Insur Issues Pract. 2019;44:277–302. doi:10.1057/s41288-018-00113-7
30. Liu H, Ma J, Zhao L. Public long-term care insurance and consumption of elderly households: evidence from China. J Health Econ. 2023;90:102759. doi:10.1016/j.jhealeco.2023.102759
31. Strauss J, Lei X, Park A, et al. Health Outcomes and Socio-Economic Status Among the Elderly in Gansu and Zhejiang Provinces, China: evidence from the CHARLS Pilot. J Popul Ageing. 2010;3:111–142. doi:10.1007/s12062-011-9033-9
32. Lechner M. The estimation of causal effects by difference-in-difference methodsestimation of spatial panels. Foundations Trends® Econometrics. 2010;4:165–224. doi:10.1561/0800000014
33. Goodman-Bacon A. Difference-in-differences with variation in treatment timing. J Econom. 2021;225:254–277. doi:10.1016/j.jeconom.2021.03.014
34. Athey S, Imbens GW. Identification and inference in nonlinear difference-in-differences models. Econometrica. 2006;74:431–497. doi:10.1111/j.1468-0262.2006.00668.x
35. Tian Y, Fan L, Zhou M, Du W. Impact of long-term care insurance on health inequality in older adults in China based on the concentration index approach. Int Health. 2024;16:83–90. doi:10.1093/inthealth/ihad025
36. Cao N, Shi T, Pan C. Does long-term care insurance reduce the disability among middle-aged and older adults? Evidence from China. BMC Public Health. 2023;23:1138. doi:10.1186/s12889-023-16057-0
37. Baker AC, Larcker DF, Wang CCY. How much should we trust staggered difference-in-differences estimates? J Financial Econo. 2022;144:370–395. doi:10.1016/j.jfineco.2022.01.004
38. Callaway B, Sant’Anna PHC. Difference-in-Differences with multiple time periods. J Econometrics. 2021;225:200–230. doi:10.1016/j.jeconom.2020.12.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.