Back to Journals » Patient Preference and Adherence » Volume 17
Does Intradialytic Group Exercise Programme Influence Patient-Reported Outcomes, Laboratory Parameters, and Anthropometric Parameters in Maintenance Hemodialysis Patients? A Single-Group Repeated-Measures Trial
Authors Zhou L ![]() , Shi D
, Shi D ![]() , Zhang L, Wang Q, Chen L, Chen H
, Zhang L, Wang Q, Chen L, Chen H ![]()
Received 2 December 2022
Accepted for publication 10 February 2023
Published 21 February 2023 Volume 2023:17 Pages 491—501
DOI https://doi.org/10.2147/PPA.S400005
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Lijuan Zhou,1,2,* Dan Shi,2 Liyuan Zhang,2,* Qian Wang,2 Li Chen,2 Honglin Chen3
1Medical School, Nantong University, Nantong, People’s Republic of China; 2Nursing Department, Taizhou People’s Hospital, Taizhou, People’s Republic of China; 3School of Public Health, Nantong University, Nantong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Honglin Chen, Email [email protected]
Background: Maintenance hemodialysis(MHD) patients often suffer from fatigue and are recommended to undertake physical activities. The optimal format of exercise rehabilitation for MHD patients remains uncertain despite demonstrated health benefits. This study aimed to evaluate the effectiveness of an intradialytic group exercise programme for MHD patients.
Methods: This was a single-centre, single-group repeated-measures design study. The 12-week, three times per-week intradialytic group exercise programme was conducted for around 30 min during the first 2 hours of each dialysis session. Patient-reported outcomes including fatigue, anxiety, depression and health-related quality of life, laboratory parameters including haemoglobin, albumin, pre-albumin and hypersensitive C-reactive protein, and anthropometric parameters including triceps skinfold thickness, mid-upper arm circumference, mid-arm muscle circumference and handgrip strength, were measured at baseline, immediately post-intervention and 12-weeks post-intervention. The repeated-measures analysis of variance and Friedman test were used to compare the parametric and non‐parametric data across time points, respectively.
Results: Ninety patients were enrolled and 75 completed. Participants reported significant improvements across time points in fatigue (F = 10.19, p < 0.01), depression (F = 19.20, p < 0.001), health-related quality of life (F = 5.36, p = 0.006), haemoglobin (F = 3.43, p = 0.047), albumin (F = 4.42, p = 0.032), hypersensitive C-reactive protein (χ2 = 50.39, p < 0.001), pre-albumin (χ2 = 11.85, p = 0.003), triceps skinfold thickness (F = 25.03, p < 0.001), mid-upper arm circumference (F = 6.32, p = 0.005), mid-arm muscle circumference (F = 4.89, p = 0.02), and handgrip strength (F = 13.59, p < 0.001). Although the mean anxiety score tended to reduce, the difference across time points was nonsignificant (F = 1.33, p = 0.27).
Conclusion: The findings suggested that the intradialytic group exercise programme could improve MHD patients’ fatigue, depression, health-related quality of life, nutritional status, and inflammation.
Trial Registration: Chinese Clinical Trial Registry ChiCTR2000034394 (04/07/2020).
Keywords: maintenance hemodialysis, group exercise, aerobic exercise, resistance exercise nutrition, quality of life
Introduction
Chronic kidney disease (CKD) has become a leading public health problem in the past decade, especially in developing countries.1 End-stage renal disease (ESRD), a major lethal factor for CKD patients, is incurable unless renal transplantation is available. Given the limited access to renal grafts, lifelong dialysis has been the sub-optimal treatment for ESRD patients.2 In China, maintenance hemodialysis (MHD) is the most widely used therapeutic approach for ESRD treatment, with the number of MHD patients reaching 632 thousand in 2020.3 Significant progress has been made in hemodialysis technology and patient care; however, MHD patients still face various problems impairing their health-related quality of life (HRQOL).2,4
Physical inactivity is common among MHD patients5 and acts as one major modifiable risk factor for their poor HRQOL.6 The level of physical activity in MHD patients is strikingly reduced due to consequences of renal failure per se (eg, abnormal skeletal muscle metabolism and structure, mitochondrial dysfunction and electrolyte disturbance), anaemia and malnutrition;7,8 subsequently results in impaired exercise capacity, ultimately muscle wasting, poor HRQOL, and increased risks of hospitalization and mortality.8–11 Given the negative impacts caused by physical inactivity, MHD patients are recommended to undertake physical activities,6,12 and nephrology staff are encouraged to help patients engage in these activities.13
Exercise training is commonly used to improve MHD patients’ physical activity. Exercise training for MHD patients can be categorized as intradialytic and extradialytic exercise according to exercise time. Intradialytic exercise is preferred considering the lower physical activity level on dialysis days compared to nondialysis days;5,14 moreover, owing to the supervision of medical staff, intradialytic exercise is superior to interdialytic exercise in terms of patient adherence and safety.15,16 Being different from the exercise time, the optimal type of exercise training remains uncertain. Aerobic exercise increases endurance and resistance exercise increases muscle strength. A combination of these are commonly prescribed in exercise training and have shown benefits for MHD patients.17,18
Despite the beneficial effects of exercise training on MHD patients, it remains neglected in dialysis care because of various barriers,19 including the lack of motivation and resource restrictions.20,21 Further studies should tackle these barriers to promote physical exercise for MHD patients.
Group exercise, involving social interactions and providing a sense of belonging, positively affects participants’ motivation and keeps their adherence to the intervention.22,23 Besides, group exercise can provide a resource-saved way of exercise training because several patients can get together and exercise under the supervision of the same health professionals. Furthermore, maintenance hemodialysis is a regular and long-term treatment allowing MHD patients to get familiar with each other in the dialysis units, making it suitable for conducting group exercises. Thus, group exercise has potential promising results for MHD patients, considering the two-way benefits for patients and health professionals; however, the effects of intradialytic group exercise on MHD patients remain unclear.
In terms of the effects of exercise on MHD patients, current studies mainly focused on biochemical and physiological parameters,1,18,24,25 with limited attention on patient-reported outcomes, such as depression, anxiety, and fatigue. Considering the high prevalence and negative impacts of these patient-reported outcomes,26,27 it is necessary to comprehensively assess the effects of exercise training on patient-reported outcomes in addition to objective parameters.
Therefore, this study aimed to examine the effects of a 12-week intradialytic group exercise programme for MHD patients on patient-reported outcomes, laboratory parameters and anthropometric parameters.
Methods
The 12-week study applied a repeated measure research design (the Chinese Clinical Trial Registry: ChiCTR2000034394). The study was conducted according to the Declaration of Helsinki and approved by the Ethics Committee of Taizhou People’s Hospital, China (KY 202004001). All participants gave informed consent before participation.
Participants
Patients who took regular maintenance hemodialysis in the Hemopurification Center at the Taizhou People’s Hospital from September 2020 to April 2021 were available for enrollment. The study included participants who (1) aged ≥ 18 years, (2) took hemodialysis treatment for more than three months, (3) took hemodialysis four hours per time and three times per week (Monday-Wednesday-Friday or Tuesday-Thursday-Saturday), (4) had no physical disability and both upper and lower muscle strength were not less than grade III, and (5) gave informed consent. The exclusion criteria were as follows: (1) had serious complications such as uncontrolled cardiovascular disease, malignant tumours, severe infection, and active bleeding, (2) had aphasia or were deaf, and (3) had a doctor-diagnosed psychiatric illness.
Study Intervention
The Hemopurification Center has 10 wards, with 4 to 10 beds each. The research staff grouped participants with good relationships under the same purification time into the same ward. After then, the purification bed was fixed unless the patients wanted a change. The intradialytic group exercise programme was conducted during the first two hours of each hemodialysis session8,28,29 with a dose of 30 min per session, three sessions per week for 12 weeks. The exercise programme consisted of four parts: warm-up, aerobic, resistance, and cool-down (Table 1).
 |
Table 1 Components of the Intradialytic Group Exercise Programme |
Resistance loop bands (PROIRON®, SHANXI REGENT, China) were applied in the resistance exercise. These bands had five tension levels, including X-Light (5–10lbs), Light (15–20lbs), Medium (25–30lbs), Heavy (35–40lbs), and X-Heavy (45–50lbs). The tension levels were set according to the MHD patients’ tolerance every time before the session. During the resistance exercise, the patient could reduce the tension level by changing the resistance band or taking a rest if s/he reported the Rating of Perceived Exertion (RPE) was over 15 points.18,30
Actions were taken to guarantee the safety of MHD patients. Vital signs and weight would be measured when patients came to the centre; those with abnormal vital signs (blood pressure > 200/100 mmHg or < 110/50 mmHg, heart rate per minute< 60, or oxygen saturation < 80%) or having interdialytic weight gain (IDWG) > 5% would not take the current exercise session. Besides, during the exercise session, nurses in the centre performed continuous supervision, and patients should stop their exercise immediately when (1) their blood pressure was >200/100 mmHg or < 110/50 mmHg; (2) their heart rate were over 80% of the maximum heart rate (maximum heart rate = 220-age); or (3) they had hypoglycemia, dizziness, headache, pale complexion, chest pain, dyspnea, etc.
Data Collection and Outcomes
Data were collected by a research assistant (LC) at baseline (T0), immediately post-intervention (T1), and three months post-intervention (T2).
Patient-Reported Outcomes
Multidimensional fatigue inventory (MFI): Fatigue was measured by the MFI, which included five subscales of fatigue, namely general fatigue (4 items), physical fatigue (4 items), reduced activity (4 items), reduced motivation (4 items), and mental fatigue (4 items). Each item was scored using a Likert 5-point scale, with a total score ranging from 20 to 100.31 The higher the score, the patient had higher level of fatigue. The Chinese version of MFI had robust psychometric properties, with Cronbach’s alpha coefficient ranging from 0.83 to 0.92 and a contracts validity index of 0.93.32
Hospital anxiety and depression scale (HADS): Depression and anxiety were measured by the HADS, which consisted of 14 items and seven items for assessing anxiety (HADS-A) and depression (HADS-D), respectively.33 Each item was assessed as 0 to 3 points, with a total score of 21 for anxiety and depression, with higher scores indicating more severe psychological distress. The Cronbach’s alpha coefficient for the Chinese version of HADS-A was 0.78 and for the HADS-D was 0.76.34
Kidney disease quality of life-short form (KDQL-SF™, Version 1.3): The KDQL-SF consisted of a 36-item short-form health survey (SF-36) and a 12-filed survey in kidney disease-targeted areas (KDTA). The Chinese version of KDQL-SF™ demonstrated good reliability, with good internal consistency (Cronbach’s alpha ranging from 0.69–0.78) and test-retest reliability (ranging from 0.70 to 0.86).35 The scores ranged from 0 to 100, and the higher the KDQOL-36™ score, the better QOL the patients had.35
Laboratory Parameters
Blood sampling was analyzed after an overnight fast on dialysis-free days in the hospital’s laboratory. Haemoglobin (Hb) was analyzed on a haematology analyzer (XN-20, Sysmex®, Kobe-shi, Japan). Albumin (Alb), pre-albumin (pre-Alb) and hypersensitive C-reactive protein (hs-CRP) were analyzed on a bio-analysis machine (AU5800, Beckman Coulter, Shanghai, China).
Anthropometric Parameters
The following five anthropometric parameters were measured. (1) Triceps Skinfold Thickness (TSF): TSF was measured using skinfold callipers, and the needle was read to the nearest 0.5mm. The measurement point was at the midpoint between the olecranon and the acromion tip of the nondialysis arm.36 The averages of two consecutive measurements were recorded; (2) Mid-Upper Arm Circumference (MUAC): MUAC was measured in the nondialysis side by a tape ruler at the midpoint of the upper arm, with the arm dropping naturally. Results were recorded to the nearest 0.1cm, and the averages of two consecutive measurements were recorded; (3) Mid-Arm Muscle Circumference (MAMC): the MAMC was calculated according to the formula MAMC(cm) = MUAC(cm) – 3.14*TSF(cm);37 (4) Handgrip Strength (HGS): The HGS of the nondialysis hand was measured by an electronic hand dynamometer (KYTO®, Dongguan, Guangdong, China) before the start of dialysis treatment. Results were recorded to the nearest 0.1kg, and the larger of two consecutive measurements were recorded.
Statistical Analysis
Data analysis was conducted using SPSS 22.0 (IBM, Armonk, NY, USA). The analysis was carried out on a per-protocol approach. The kurtosis and skewness tests were used to test the normal distribution of the data; data with normal distribution were described using means and standard deviation (SD); those without normal distribution were described using medians and quartiles [q25, q75]. The repeated-measures analysis of variance (rANOVA) and Friedman test were used to compare the parametric and non‐parametric data at three time points, respectively. All statistical tests were two-tailed, and p < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics
A total of 178 MHD patients were screened, among which 90 were recruited. Among the 90 recruited MHD patients, 75 (35 males) completed the 12-week intradialytic group exercise. The flow chart of patients during the study is shown in Figure 1. The mean age of the participants was 55.03 (10.69) years, ranging from 25 to 77 years. Most participants were married (92.0%) and had no religious beliefs (84.0%). More than half of people (68%) had a duration of dialysis longer than 36 months. The details of demographic and clinical characteristics are reported in Table 2.
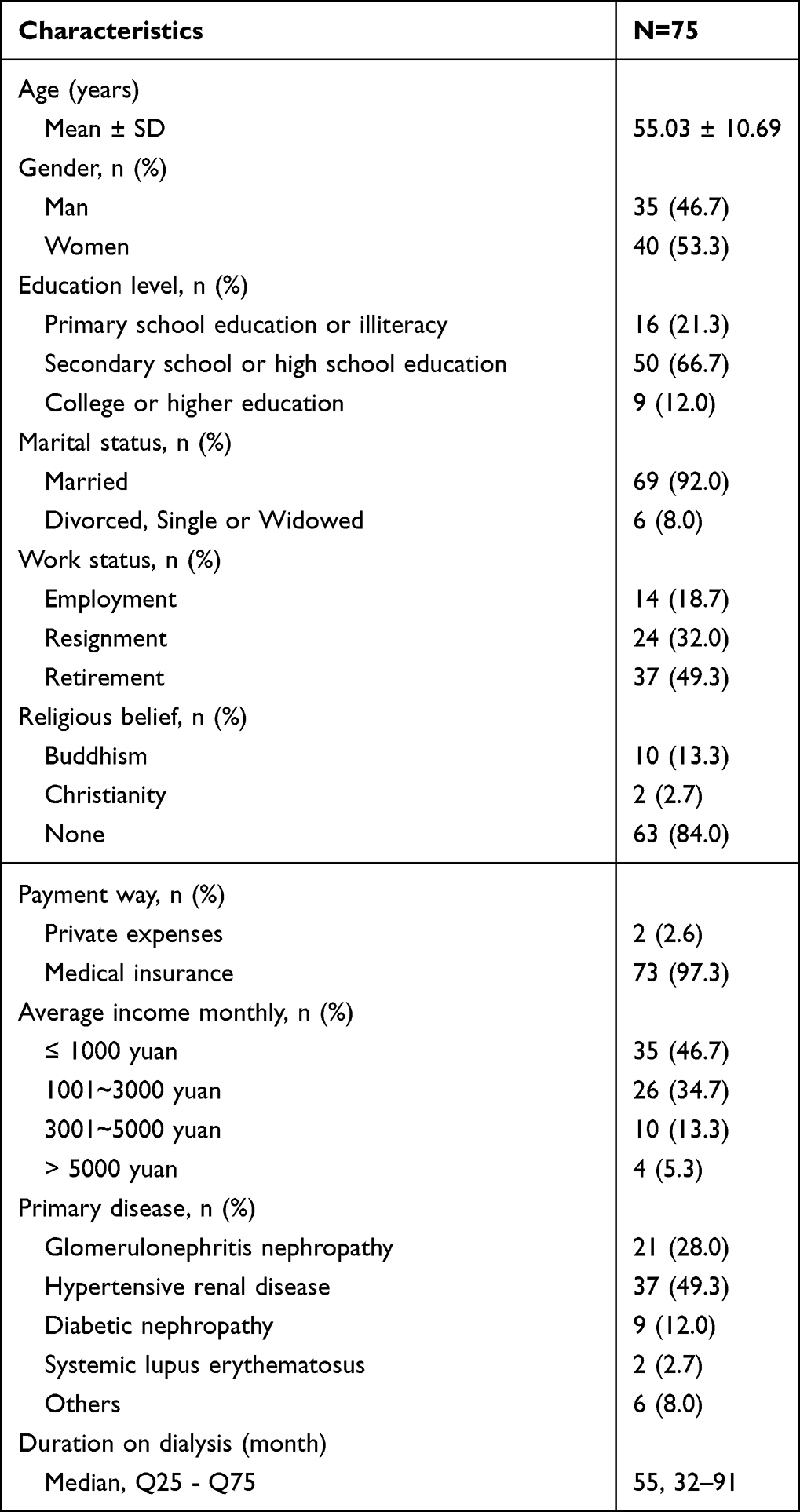 |
Table 2 Demographic and Clinical Characteristics |
 |
Figure 1 Flow chart of participants. |
Effects of the Intradialytic Group Exercise
Effects on Patient-Reported Outcomes
The results of rANOVA indicated significant improvements in fatigue (F = 10.19, p < 0.01), depression (F = 19.20, p < 0.001), and HRQOL (F = 5.36, p = 0.006) across time points. Although the mean anxiety score tended to reduce, the difference across time points was not significant (F = 1.33, p = 0.27).
The results of rANOVA showed significant improvements in laboratory parameters, including Hb (F = 3.43, p = 0.047) and Alb (F = 4.42, p = 0.032) across time points. The results of the Friedman test showed that MHD patients attain significant improvements in hs-CRP (χ2 = 50.39, p < 0.001) and pre-Alb (χ2 = 11.85, p = 0.003).
In terms of anthropometric parameters, significant improvements were obtained in TSF (F = 25.03, p < 0.001), MUAC (F = 6.32, p = 0.005), MAMC (F = 4.89, p = 0.02), and HGS (F = 13.59, p < 0.001). Comparisons of outcomes at different time points are reported in Table 3.
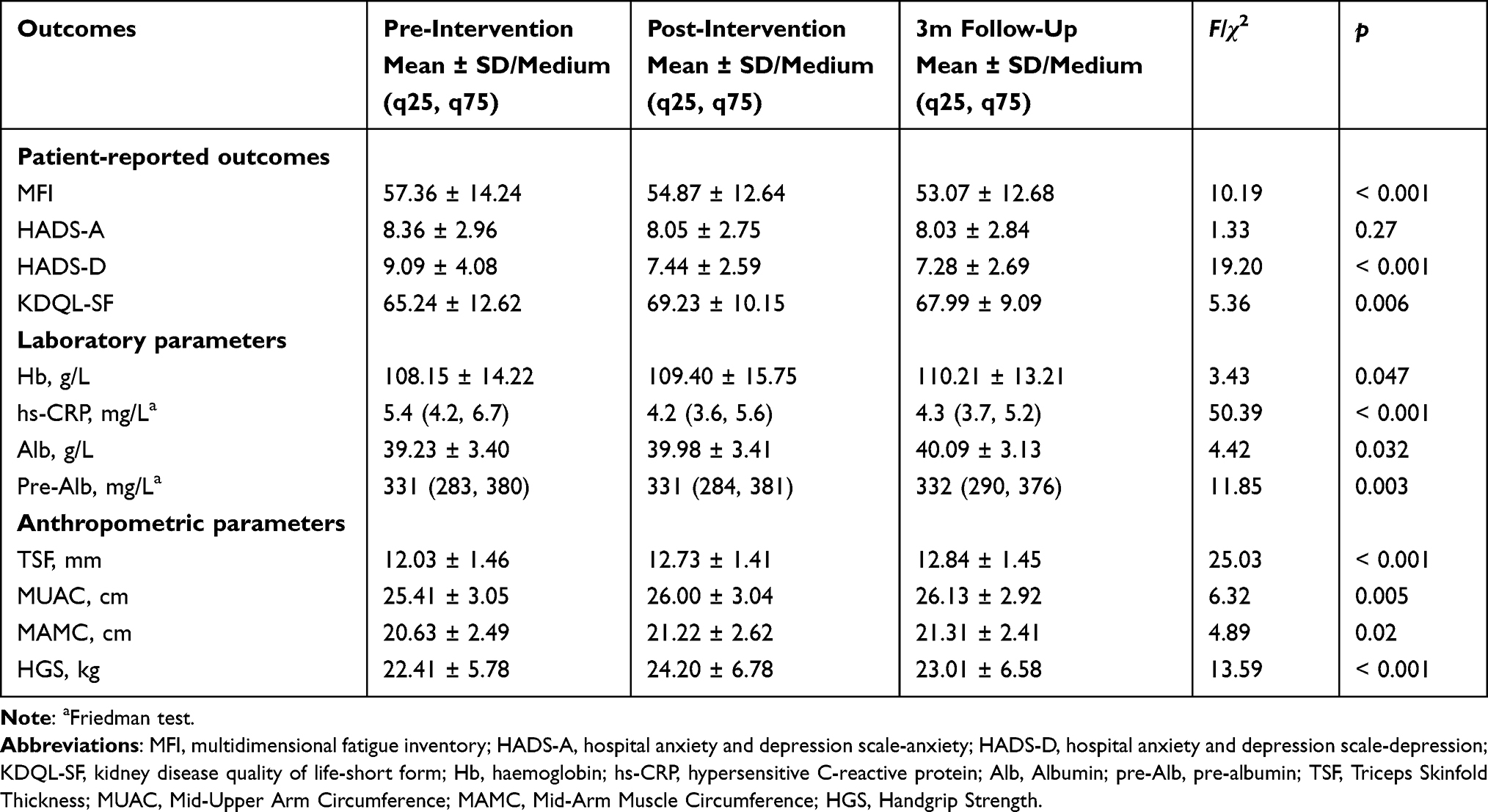 |
Table 3 Comparisons of Patient-Reported Outcomes at Different Time Points |
Discussion
Of the 90 MHD patients enrolled, 15 dropped out of the study. In addition to death, hospital transfer, hospitalization, surgery and other irresistible factors, 7 patients (7.7%) dropped out of the study due to loss of motivation, the proportion is lower than in previous studies.38,39 During the first data collection, 2 patients were unwilling to continue the study because data collection occupied too much of their time. During the intervention, 5 patients lost motivation and dropped out of the study. Among them, 3 patients thought the exercise was too much for their body to withstand, and 2 patients because they did not get along with other patients in the same group. In future studies, some time can be reserved for each group of patients before intervention to help a group of patients communicate effectively and adapt to the amount of exercise. In future studies, some time can be reserved for each group of patients before intervention, so as to help patients in a group to have effective communication and adapt to the amount of exercise. Make detailed explanations with the patient before intervention, including the amount of data to be collected. Ultimately, these controllable factors can avoid the loss of participants.
MHD patients tend to be sedentary,40 which can induce a catabolic state including reduced neuromuscular functioning, reduced exercise tolerance and reduced cardiorespiratory fitness.6,41 Over time, these catabolic adaptations may lead to functional limitations that interfere with activities of daily living and affect quality of life. Some studies29,39 suggest that exercise can change these conditions. Kidney Disease: Improving Global Outcomes (KDIGO) guidelines recommend that patients be physically active.42 Recent systematic reviews have shown that intradialytic exercise could improve the removal of solutes, systemic inflammation, exercise tolerance, walking ability, muscle strength, and QOL;43–47 however, limited attention has been put on patient-reported outcomes, and the optimal exercise type and format for MHD patients remains uncertain. This study applied the intradialytic group exercise programme for MHD patients; moreover, the study comprehensively examined the intervention effects on patient-reported outcomes, laboratory parameters and anthropometric parameters.
Aerobic exercise, using large muscle groups, primarily improves oxidative capacity and cardiovascular function, so as to improve endurance. Individual aerobic exercise in MHD patients is safe and has a significant effect on the control of hypertension, physical capacity, sleep quality and QOL.43,48 Resistance exercise can increase muscle size and strength, and it may help in reducing microinflammatory reactions and protein-energy wasting.18,29,49–52 In addition, the combination of aerobic exercise and resistance exercise is a common paradigm in exercise prescription, which embraces advantages of these two exercise ways. As a recent systematic review showed, differences between combined exercise and aerobic or resistance exercise alone did not reach statistical significance, however the combined one resulted in the largest effect sizes.53 Furthermore, given the social atmosphere in dialysis units and the benefits of group exercise concluded in available systematic reviews,54–56 group-based exercise may be suitable and beneficial for MHD patients. Therefore, this study applied an intradialytic group exercise programme consisted of both aerobic exercise and resistance exercise.
Results of the study showed that the intradialytic group exercise could improve patients’ fatigue, depression and HRQOL. The results were consistent with former studies.17,57,58 Although the anxiety score reduced over time, we found a nonsignificant improvement in patients’ anxiety. The finding was in line with the systematic review of Hargrove, El Tobgy, Zhou, Pinder, Plant, Askin, Bieber, Collister, Whitlock, Tangri, Bohm,59 which looked at the effectiveness of aerobic exercise on patients’ anxiety and demonstrated inconclusive results. Techniques such as deep breathing,60 guided imagery,61 and cognitive-behavioural interventions62 may be needed to reduce the level of anxiety. In addition to patient-reported outcomes, this study also used anthropometric and laboratory indicators to reflect MHD patients’ nutritional state and systemic inflammation. The findings suggested that the intradialytic group exercise positively affected malnutrition and systemic inflammation in MHD patients, which were consistent with previous studies.17,43 Furthermore, seven out of 90 patients dropped out for losing motivation, which was lower compared to former studies related to intradialytic exercise in MHD patients.8,18,29,63
Exercise training has been proven to be important to MHD patients, yet, it has received limited attention from both MHD patients and health providers for diverse reasons, among which the fear of injuries, the lack of motivation and resources restrictions are the common barriers.64 This study found that the intradialytic group exercise could benefit MHD patients with a low attrition rate. With the supervision of medical staff and peer support from other patients, intradialytic group exercise seems to provide a way for MHD patients to overcome the fear of injuries and sustain motivation. Healthcare providers and patients may treat exercise as the new “normal” in a physical and social environment, thus limiting opportunities for sedentary behaviours.21 Moreover, group exercise provides resource-saved exercise training because several patients can exercise under a health provider’s supervision. The exercise culture cultivated by fostering a common identity among participants and increasing social interaction during the group exercise may be the main reason for the low dropout rate.
Although the study generates some new knowledge in exercise rehabilitation in MHD patients, there are still some limitations. Firstly, this is a single-centre study, while results from a multicenter study enrolling more participants may be more reliable. Secondly, this is a single-group repeated-measures design study. Studies with a control group (such as randomized controlled trials) are needed to assess the effectiveness of the intradialytic group exercise. Thirdly, due to the sudden outbreak of COVID-19 in the city after the 3-month follow-up, thus, outcomes were not measured as scheduled at 6-month follow-up. A study with a more extended period is required to evaluate longer-term health impacts.
Conclusions
The findings of this study provided preliminary evidence that aerobic exercise combined with resistance exercise program could improve fatigue, depression, health-related quality of life, nutrition state and inflammation in patients undergoing maintenance hemodialysis. Further study using randomized controlled trials is needed to examine the effectiveness of the aerobic exercise combined with resistance exercise program for maintenance hemodialysis patients.
Abbreviations
CKD, Chronic kidney disease; ESRD, End-stage renal disease; MHD, maintenance hemodialysis; HRQOL, health-related quality of life; RPE, Rating of Perceived Exertion; IDEG, interdialytic weight gain; KDTA, kidney disease-targeted areas; MFI, Multidimensional fatigue inventory; HADS-A, Hospital anxiety and depression scale-anxiety; HADS-D, Hospital anxiety and depression scale-depression; KDQL-SF, Kidney disease quality of life-short form; Hb, Haemoglobin; hs-CRP, hypersensitive C-reactive protein; Alb, Albumin; pre-Alb, pre-albumin; TSF, Triceps Skinfold Thickness; MUAC, Mid-Upper Arm Circumference; MAMC, Mid-Arm Muscle Circumference; HGS, Handgrip Strength; SD, standard deviation; rANOVA, The repeated-measures analysis of variance.
Data Sharing Statement
The authors are willing to permanently share data supporting the results and analysis presented in the paper after publication. The data can be used for scientific research beneficial to human health. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The trial was conducted following the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of Taizhou People’s Hospital, China (NO. KY 202004001) and informed consent was taken from all individual participants.
Acknowledgments
Special thanks go to the healthcare providers in the Hemopurification Center, the Taizhou People’s Hospital. We also appreciate all the participations who voluntarily took part in this study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Zhang L, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012;379(9818):815–822. doi:10.1016/S0140-6736(12)60033-6
2. Robinson BM, Akizawa T, Jager KJ, Kerr PG, Saran R, Pisoni RL. Factors affecting outcomes in patients reaching end-stage kidney disease worldwide: differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet. 2016;388(10041):294–306. doi:10.1016/S0140-6736(16)30448-2
3. National Kidney Disease Medical Quality Control Center. Chinese National Renal Data System; 2020. Available from: http://www.cnrds.net/TxLogin.
4. Shim HY, Cho MK. Factors influencing the quality of life of haemodialysis patients according to symptom cluster. J Clin Nurs. 2018;27(9–10):2132–2141. doi:10.1111/jocn.13904
5. Panaye M, Kolko-Labadens A, Lasseur C, et al. Phenotypes influencing low physical activity in maintenance dialysis. J Ren Nutr. 2015;25(1):31–39. doi:10.1053/j.jrn.2014.07.010
6. Zelle DM, Klaassen G, van Adrichem E, Bakker SJ, Corpeleijn E, Navis G. Physical inactivity: a risk factor and target for intervention in renal care. Nat Rev Nephrol. 2017;13(3):152–168. doi:10.1038/nrneph.2016.187
7. Kopple JD, Storer T, Casburi R. Impaired exercise capacity and exercise training in maintenance hemodialysis patients. J Ren Nutr. 2005;15(1):44–48. doi:10.1053/j.jrn.2004.09.022
8. Cho JH, Lee JY, Lee S, Park H, Choi SW, Kim JC. Effect of intradialytic exercise on daily physical activity and sleep quality in maintenance hemodialysis patients. Int Urol Nephrol. 2018;50(4):745–754. doi:10.1007/s11255-018-1796-y
9. Ortiz A, Covic A, Fliser D, et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet. 2014;383(9931):1831–1843. doi:10.1016/S0140-6736(14)60384-6
10. Peng YS, Chiang CK, Hung KY, et al. Are both psychological and physical dimensions in health-related quality of life associated with mortality in hemodialysis patients: a 7-Year Taiwan Cohort Study. Blood Purificat. 2010;30(2):98–105. doi:10.1159/000319002
11. Lopes AA, Lantz B, Morgenstern H, et al. Associations of self-reported physical activity types and levels with quality of life, depression symptoms, and mortality in hemodialysis patients: the DOPPS. Clin J Am Soc Nephrol. 2014;9(10):1702–1712. doi:10.2215/CJN.12371213
12. Parker K. Intradialytic exercise is medicine for hemodialysis patients. Curr Sports Med Rep. 2016;15(4):269–275. doi:10.1249/JSR.0000000000000280
13. Smith AC, Burton JO. Exercise in kidney disease and diabetes: time for action. J Ren Care. 2012;38 Suppl 1:52–58. doi:10.1111/j.1755-6686.2012.00279.x
14. Avesani CM, Trolonge S, Deleaval P, et al. Physical activity and energy expenditure in haemodialysis patients: an international survey. Nephrol Dial Transplant. 2012;27(6):2430–2434. doi:10.1093/ndt/gfr692
15. Pu J, Jiang Z, Wu W, et al. Efficacy and safety of intradialytic exercise in haemodialysis patients: a systematic review and meta-analysis. BMJ Open. 2019;9(1):e020633. doi:10.1136/bmjopen-2017-020633
16. Jung TD, Park SH. Intradialytic exercise programs for hemodialysis patients. Chonnam Med J. 2011;47(2):61–65. doi:10.4068/cmj.2011.47.2.61
17. Umami V, Tedjasukmana D, Setiati S. The effect of intradialytic exercise twice a week on the physical capacity, inflammation, and nutritional status of dialysis patients: a randomized controlled trial. Hemodial Int. 2019;23(4):486–493. doi:10.1111/hdi.12764
18. Dong ZJ, Zhang HL, Yin LX. Effects of intradialytic resistance exercise on systemic inflammation in maintenance hemodialysis patients with sarcopenia: a randomized controlled trial. Int Urol Nephrol. 2019;51(8):1415–1424. doi:10.1007/s11255-019-02200-7
19. Heiwe S, Jacobson SH. Exercise training in adults with CKD: a systematic review and meta-analysis. Am J Kidney Dis. 2014;64(3):383–393. doi:10.1053/j.ajkd.2014.03.020
20. Jhamb M, McNulty ML, Ingalsbe G, et al. Knowledge, barriers and facilitators of exercise in dialysis patients: a qualitative study of patients, staff and nephrologists. BMC Nephrol. 2016;17(1):192. doi:10.1186/s12882-016-0399-z
21. Clarke AL, Jhamb M, Bennett PN. Barriers and facilitators for engagement and implementation of exercise in end-stage kidney disease: future theory-based interventions using the Behavior Change Wheel. Semin Dialysis. 2019;32(4):308–319. doi:10.1111/sdi.12787
22. Tsutsumimoto K, Doi T, Shimada H, Makizako H, Suzuki T. Effects of group exercise programmes on quality of life in older adults with mild cognitive impairment: preliminary results from a randomized controlled trial. Psychogeriatrics. 2016;16(5):327–328. doi:10.1111/psyg.12165
23. Taraldsen K, Boulton E, Helbostad JL, Saltvedt I, Granbo R. Client, caregiver, volunteer, and therapist views on a voluntary supported group exercise programme for older adults with dementia. BMC Geriatr. 2020;20(1):235. doi:10.1186/s12877-020-01632-6
24. Palar R, Lobo D. Impact of intradialytic exercise on fatigue, biochemical and physiological parameters in patients on maintenance hemodialysis - A pilot study - Part 1. Clin Epidemiol Glob Health. 2022;15:101064. doi:10.1016/j.cegh.2022.101064
25. Arazi H, Mohabbat M, Saidie P, Falahati A, Suzuki K. Effects of different types of exercise on kidney diseases. Sports (Basel). 2022;10(3). doi:10.3390/sports10030042
26. Cheng J, Yang D, Zuo Q, Peng W, Zhu L, Jiang X. Correlations between uncertainty in illness and anxiety, depression and quality of life in patients receiving maintenance haemodialysis: a cross-sectional study. Nurs Open. 2022;9(2):1322–1331. doi:10.1002/nop2.1177
27. Bossola M, Marzetti E, Di Stasio E, et al. Prevalence and associated variables of post-dialysis fatigue: results of a prospective multicentre study. Nephrology (Carlton). 2018;23(6):552–558. doi:10.1111/nep.13059
28. Assawasaksakul N, Sirichana W, Joosri W, et al. Effects of intradialytic cycling exercise on daily physical activity, physical fitness, body composition, and clinical parameters in high-volume online hemodiafiltration patients: a pilot randomized-controlled trial. Int Urol Nephrol. 2021;53(2):359–371. doi:10.1007/s11255-020-02677-7
29. Martins Do Valle F, Valle Pinheiro B, Almeida Barros AA, et al. Effects of intradialytic resistance training on physical activity in daily life, muscle strength, physical capacity and quality of life in hemodialysis patients: a randomized clinical trial. Disabil Rehabil. 2020;42(25):3638–3644. doi:10.1080/09638288.2019.1606857
30. Arney BE, de Koning JJ, Foster C, et al. Comparison of rating of perceived exertion scales during incremental and interval exercise. Kinesiology. 2019;51(2):150–157. doi:10.26582/k.51.2.1
31. Smets EMA, Garssen B, Bonke B, De Haes JCJM. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39(3):315–325. doi:10.1016/0022-3999(94)00125-O
32. Pien LC, Chu H, Chen WC, et al. Reliability and validity of a Chinese version of the Multidimensional Fatigue Symptom Inventory-Short Form (MFSI-SF-C). J Clin Nurs. 2011;20(15–16):2224–2232. doi:10.1111/j.1365-2702.2010.03691.x
33. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
34. Wang SY, Zang XY, Liu JD, Cheng M, Shi YX, Zhao Y. Indicators and correlates of psychological disturbance in Chinese patients receiving maintenance hemodialysis: a cross-sectional study. Int Urol Nephrol. 2015;47(4):679–689. doi:10.1007/s11255-015-0910-7
35. Tao X, Chow SK, Wong FK. Determining the validity and reliability of the Chinese version of the Kidney Disease Quality of Life Questionnaire (KDQOL-36). BMC Nephrol. 2014;15:115. doi:10.1186/1471-2369-15-115
36. He L, Yang N, Wang J, et al. Mid-arm muscle and subcutaneous fat associated with all-cause mortality independent of BMI: a Prospective Cohort Study. Obesity (Silver Spring). 2021;29(7):1203–1214. doi:10.1002/oby.23179
37. Huang CX, Tighiouart H, Beddhu S, et al. Both low muscle mass and low fat are associated with higher all-cause mortality in hemodialysis patients. Kidney Int. 2010;77(7):624–629. doi:10.1038/ki.2009.524
38. Yabe H, Kono K, Yamaguchi T, Ishikawa Y, Yamaguchi Y, Azekura H. Effects of intradialytic exercise for advanced-age patients undergoing hemodialysis: a randomized controlled trial. PLoS One. 2021;16(10):e0257918. doi:10.1371/journal.pone.0257918
39. Perez-Dominguez B, Casana-Granell J, Garcia-Maset R, Garcia-Testal A, Melendez-Oliva E, Segura-Orti E. Effects of exercise programs on physical function and activity levels in patients undergoing hemodialysis: a randomized controlled trial. Eur J Phys Rehabil Med. 2021;57(6):994–1001. doi:10.23736/S1973-9087.21.06694-6
40. Yuenyongchaiwat K, Jongritthiporn S, Somsamarn K, Sukkho O, Pairojkittrakul S, Traitanon O. Depression and low physical activity are related to sarcopenia in hemodialysis: a single-center study. PeerJ. 2021;9:e11695. doi:10.7717/peerj.11695
41. Sabatino A, Cuppari L, Stenvinkel P, Lindholm B, Avesani CM. Sarcopenia in chronic kidney disease: what have we learned so far? J Nephrol. 2021;34(4):1347–1372. doi:10.1007/s40620-020-00840-y
42. Kidney Disease: Improving Global Outcomes Blood Pressure Work G. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3S):S1–S87. doi:10.1016/j.kint.2020.11.003
43. Salhab N, Karavetian M, Kooman J, Fiaccadori E, El Khoury CF. Effects of intradialytic aerobic exercise on hemodialysis patients: a systematic review and meta-analysis. J Nephrol. 2019;32(4):549–566. doi:10.1007/s40620-018-00565-z
44. Melendez Oliva E, Villafane JH, Alonso Perez JL, et al. Effect of exercise on inflammation in hemodialysis patients: a Systematic Review. J Pers Med. 2022;12(7):1188. doi:10.3390/jpm12071188
45. Ferreira GD, Bohlke M, Correa CM, Dias EC, Orcy RB. Does intradialytic exercise improve removal of solutes by hemodialysis? A Systematic Review and Meta-analysis. Arch Phys Med Rehabil. 2019;100(12):2371–2380. doi:10.1016/j.apmr.2019.02.009
46. Matsuzawa R, Hoshi K, Yoneki K, et al. Exercise training in elderly people undergoing hemodialysis: a Systematic Review and Meta-analysis. Kidney Int Rep. 2017;2(6):1096–1110. doi:10.1016/j.ekir.2017.06.008
47. Song Y, Chen L, Wang M, He Q, Xue J, Jiang H. The optimal exercise modality and intensity for hemodialysis patients incorporating Bayesian network meta-analysis and systematic review. Front Physiol. 2022;13:945465. doi:10.3389/fphys.2022.945465
48. Henrique DM, Reboredo Mde M, Chaoubah A, Paula RB. [Aerobic exercise improves physical capacity in patients under chronic hemodialysis]. Arq Bras Cardiol. 2010;94(6):823–828. Portuguese. doi:10.1590/S0066-782X2010005000043
49. Bullani R, El-Housseini Y, Giordano F, et al. Effect of intradialytic resistance band exercise on physical function in patients on maintenance hemodialysis: a pilot study. J Ren Nutr. 2011;21(1):61–65. doi:10.1053/j.jrn.2010.10.011
50. Saitoh M, Ogawa M, Dos Santos MR, et al. Effects of intradialytic resistance exercise on protein energy wasting, physical performance and physical activity in ambulatory patients on dialysis: a Single-Center Preliminary Study in a Japanese Dialysis Facility. Ther Apher Dial. 2016;20(6):632–638. doi:10.1111/1744-9987.12447
51. Olvera-Soto MG, Valdez-Ortiz R, Lopez Alvarenga JC, Espinosa-Cuevas Mde L. Effect of resistance exercises on the indicators of muscle reserves and handgrip strength in adult patients on hemodialysis. J Ren Nutr. 2016;26(1):53–60. doi:10.1053/j.jrn.2015.06.006
52. Moriyama Y, Hara M, Aratani S, Ishikawa H, Kono K, Tamaki M. The association between six month intra-dialytic resistance training and muscle strength or physical performance in patients with maintenance hemodialysis: a multicenter retrospective observational study. BMC Nephrol. 2019;20(1):172. doi:10.1186/s12882-019-1375-1
53. Bogataj S, Pajek M, Pajek J, Buturovic Ponikvar J, Paravlic A. Exercise-based interventions in hemodialysis patients: a Systematic Review with a Meta-Analysis of Randomized Controlled Trials. J Clin Med. 2019;9(1):43. doi:10.3390/jcm9010043
54. Martin JT, Wolf A, Moore JL, Rolenz E, DiNinno A, Reneker JC. The effectiveness of physical therapist-administered group-based exercise on fall prevention: a systematic review of randomized controlled trials. J Geriatr Phys Ther. 2013;36(4):182–193. doi:10.1519/JPT.0b013e3182816045
55. Church G, Parker J, Powell L, Mawson S. The effectiveness of group exercise for improving activity and participation in adult stroke survivors: a systematic review. Physiotherapy. 2019;105(4):399–411. doi:10.1016/j.physio.2019.01.005
56. Liang H, Tian X, Liu XL, et al. The comparative efficacy of group- versus home-based exercise programs in patients with ankylosing spondylitis: protocol for a meta-analysis. Medicine (Baltimore). 2018;97(29):e11540. doi:10.1097/MD.0000000000011540
57. Mi Rye S, Hyuk Jung H, Bae Kim S, Sik Park J, Seok Yang W. Effects of regular exercise on anxiety, depression, and quality of life in maintenance hemodialysis patients. Ren Fail. 2009;24(3):337–345. doi:10.1081/JDI-120005367
58. Malini H, Forwaty E, Cleary M, Visentin D, Oktarina E, Lenggogeni DP. The effect of intradialytic range of motion exercise on dialysis adequacy and fatigue in hemodialysis patients. J Nurs Res. 2022;30(4):e221. doi:10.1097/jnr.0000000000000506
59. Hargrove N, El Tobgy N, Zhou O, et al. Effect of aerobic exercise on dialysis-related symptoms in individuals undergoing maintenance hemodialysis: a Systematic Review and Meta-Analysis of Clinical Trials. Clin J Am Soc Nephrol. 2021;16(4):560–574. doi:10.2215/CJN.15080920
60. Nipa N, Hapsah H, Majid A. Deep breathing relaxation exercise for reducing anxiety of patients under hemodialysis treatment. Enferm Clin. 2021;31:S793–S796. doi:10.1016/j.enfcli.2021.07.032
61. Beizaee Y, Rejeh N, Heravi-Karimooi M, Tadrisi SD, Griffiths P, Vaismoradi M. The effect of guided imagery on anxiety, depression and vital signs in patients on hemodialysis. Complement Ther Clin Pract. 2018;33:184–190. doi:10.1016/j.ctcp.2018.10.008
62. Saki M, Khoshnood S, Mohammadipour F, Ebrahimzadeh F, Rezaei F. The effect of cognitive–behavioral intervention on hope and death anxiety level in patients undergoing hemodialysis. J Ment Health Train Educ Pract. 2022;17(3):181–190. doi:10.1108/JMHTEP-08-2020-0059
63. Lopes LCC, Mota JF, Prestes J, et al. Intradialytic resistance training improves functional capacity and lean mass gain in individuals on hemodialysis: a Randomized Pilot Trial. Arch Phys Med Rehabil. 2019;100(11):2151–2158. doi:10.1016/j.apmr.2019.06.006
64. Tao X, Chow SK, Wong FK. A nurse-led case management program on home exercise training for hemodialysis patients: a randomized controlled trial. Int J Nurs Stud. 2015;52(6):1029–1041. doi:10.1016/j.ijnurstu.2015.03.013
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation Between the Frailty of Elderly Patients on Regular Haemodialysis and the Quality of Life of Their Family Caregivers: A Cross-Sectional Evaluation
Zhu Z, Li P, Chai D, Luan W
Journal of Multidisciplinary Healthcare 2022, 15:2321-2330
Published Date: 12 October 2022