Back to Journals » Clinical Interventions in Aging » Volume 18
Does Hand Grip Strength (HGS) Predict Functional Independence Differently in Patients Post Hip Replacement Due to Osteoarthritis versus Patients Status Post Hip Replacement Due to a Fracture?
Authors Zasadzka E ![]() , Trzmiel T
, Trzmiel T ![]() , Kasior I, Hojan K
, Kasior I, Hojan K ![]()
Received 4 April 2023
Accepted for publication 27 June 2023
Published 24 July 2023 Volume 2023:18 Pages 1145—1154
DOI https://doi.org/10.2147/CIA.S415744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Ewa Zasadzka,1 Tomasz Trzmiel,1 Iwona Kasior,2 Katarzyna Hojan1
1Department of Occupational Therapy, Poznan University of Medical Sciences, Poznan, Poland; 2Department of Physical Therapy, College of Nursing and Allied Health Sciences, Howard University, Washington, DC, USA
Correspondence: Ewa Zasadzka, Email [email protected]
Purpose: The aim of the study was to determine whether hand grip strength (HGS) predicts functional independence in older patients who have undergone hip replacement due to osteoarthritis versus older patients who have undergone hip replacement surgery due to fracture.
Patients and Methods: The study included 239 patients aged 65 and over in the first weeks after total hip replacement during rehabilitation treatment. Multivariate linear regression was used to determine HGS as a predictor of activities of daily living (ADL) and instrumental activities of daily living (IADL) in both groups: patients post hip replacement due to osteoarthritis and patients post hip replacement due to a fracture.
Results: Analysis showed that pre-rehab HGS in the osteoarthritis group predicts improved activities of daily living after rehabilitation (ADL, OR = 1.098; CI 95% 1.052– 1.147 and IADL, OR = 1.182; CI 95% 1.103– 1.267) and 6 months after (ADL, OR = 1.191; CI 95% 1.066– 1.329 and IADL, OR = 1.096; CI 95% 1.012– 1.186). In the fracture group, HGS predicts the ADL (OR = 1.081; CI 95% 1.015– 1.152) after rehabilitation, and IADL after rehabilitation (OR = 1.122; CI 95% 1.046– 1.205) and 6 months after (OR = 1.090; 95% CI 1.021– 1.64).
Conclusion: HGS in patients after hip replacement surgery predicts functional independence in basic and complex activities of daily living. This can allow the identification of osteoarthritis patients with low hand grip - who can be considered as patients with a higher risk of an unsatisfying outcome of surgery. These patients should undergo pre-rehabilitation and should be monitored, and/or supported in terms of rehabilitation after discharge.
Keywords: hand grip strength, endoprosthesis, hip replacement, osteoarthritis, hip fracture
Introduction
Hip joint replacement has become one of the most frequent surgical interventions of the 20th century and the incidence of the procedure in people over 65 is significantly increasing.1 One of the main causes of hip replacement is osteoarthritis leading to hip joint damage and consequently to the deterioration of quality of life. Osteoarthritis of the hip joint affects about 7.5% of the population,2 and occurs more often in women than men.3 Hip replacement reduces pain and improves functional capacity in patients with osteoarthritis.4
However, falls are considered a major problem and the most common cause of injury in the elderly population.5 Hip fractures are an increasingly common consequence of falls in older people and involve a high risk of death and reduced function.6 It is estimated, that each year 1.6 milion cases of hip fracture occur worldwide.7 Hip replacement is considered the most common form of treatment in hip fractures among older patients.8
Many studies have shown that low HGS (hand grip strength) is associated with a greater likelihood of death,9 a risk of mobility decline, disability10 and hospitalization11 as well as an increased risk of complications or a longer hospital stay after surgery.12 It has also been demonstrated that HGS can not only be a determinant of upper limb strength but also that hand dynamometer measurements can show an older person’s overall strength.13,14
Previous studies15–18 documented numerous results using HGS after hip replacement in elderly people many months after surgery. Milman et al18 found that HGS predicts successful rehabilitation. In their retrospective study conducted on geriatric patients each kg of HGS increased the chance of successful rehabilitation by 6.8%. Savino et al conducted a study on 504 older patients. They found that the patients with the highest HGS are 4.07 times more likely to achieve walking recovery than patients with lowest HGS. Chang et al17 showed that HGS above 20.5 kg in males and above 11.5 kg in females predicts lower risk of complications (such as pneumonia, pressure ulcers, delirium, urinary tract infection, deep venous thrombosis) after surgery, and a higher chance for early walking recovery. Visser et al showed that loss of HGS can be associated with a lower chance of ambulation recovery after 12 months.
A study by Visser et al showed that decreased HGS is associated with low physical function in older participants.19 In their study, Beloosesky et al demonstrated significant correlations between HGS and the functioning of upper limbs (using DASH questionnaires) in elderly patients operated on after a hip fracture and their positive functional outcomes six months post surgery.20 Those authors suggested that additional interventions should be applied to increase muscle strength and thus improve the functional outcome.20 In another study, Visser et al showed that decreased HGS is associated with decreased recovery of mobility after hip surgery. They observed that a decrease in muscle strength, but not a loss of muscle mass after surgery, is a predictor of worse motor recovery from a hip fracture 12 months after hip fracture surgery.15 Savino et al found that grip strength in elderly people after hip fracture surgery correlates with strength of other muscle groups and that this measurement is highly predictive of functional deterioration, disability, hospitalization risk and mortality.16
However, despite numerous studies assessing the relation between HGS and different measures of physical function and recovery, there are no studies comparing the HGS predicting potential between osteoarthritis-caused and fracture-caused hip replacement patients. Therefore, the purpose of this study was to determine whether hand grip strength (HGS) predicts functional independence in older patients differently in these two groups.
Materials and Methods
Setting and Study Group
This was a prospective clinical study which was conducted with 239 patients aged 65 and over who had been admitted to the rehabilitation department after total hip replacement (Figure 1). The study observation was carried out from 2018 to 2021. Sample size was determined based on the formula from Green21 for the multiple correlation N ≥ 50 + 8m, where m is the number of predictors. The minimum sample size for this study is 180 persons.
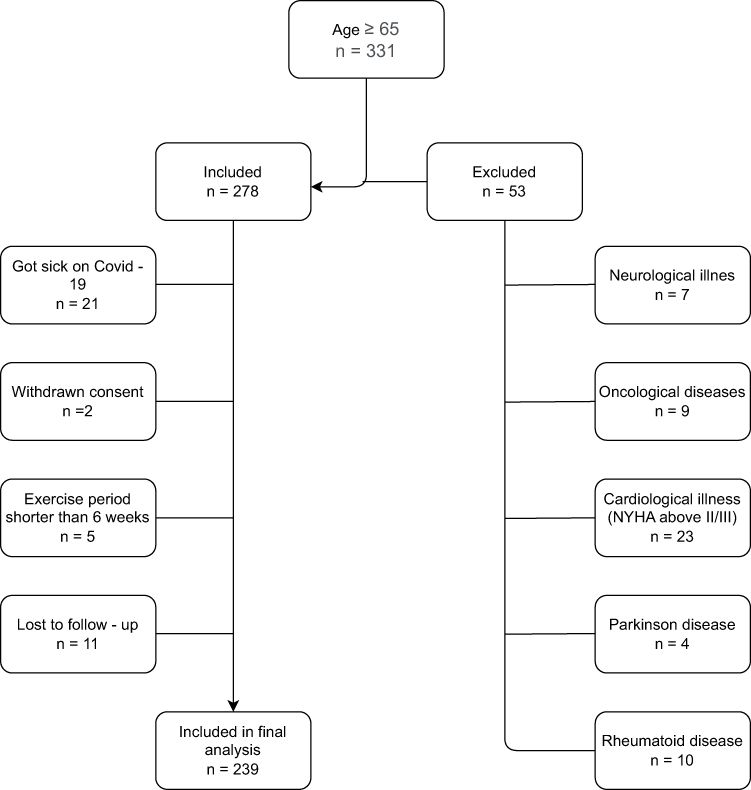 |
Figure 1 Criteria for including data for further analysis. |
All participants gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Poznan University of Medical Sciences (No. 995/18).
Patients were included in the study according to the study criteria. Subjects from 4 to 6 weeks after surgery were selected to participate in the study. Additionally, the inclusion criteria were: age above 65 years old, good general health condition, no cognitive impairment (Mini–Mental State Examination, MMSE above 23),22 total hip replacement due to osteoarthritis or hip replacement s/p hip fracture after a fall.
Patients diagnosed with oncological diseases, cardiac illnesses resulting in insufficient circulation (NYHA above II/III), rheumatoid disease, neurological illness such as stroke, Parkinson's disease, MS, etc., were excluded from the study. Participants who dropped out of the study were also excluded.
Study Protocol
The first study measurement was conducted at the beginning of the rehabilitation process in the rehabilitation ward (the first two days after admission to the ward, between 4–6 weeks post discharge from the orthopedic ward). The second measurement was performed after six weeks of rehabilitation. Six months after the rehabilitation participants were contacted in their homes and a third measurement of functional independence and physical function scales was conducted.
The subjects were divided into two study groups depending on the cause of the orthopedic surgery:
- The osteoarthritis group (OAG) included subjects who underwent total hip replacement surgery due to joint osteoarthritis,
- The falls group (FG) included subjects who underwent total hip joint replacement due to the fracture of the femoral neck after a fall.
During their stay at the rehabilitation ward, each patient had followed a rehabilitation program consisting of passive and active exercises, strengthening exercises, and walking and balance training. Rehabilitation was adjusted individually depending of patient status and independence. Rehabilitation included 120 minutes of individual kinesiotherapy, additional physical therapy procedures (such as electrotherapy, pulsed magnetic field, laser, ultrasound, and/or cryotherapy), and prophylactic education with a physiotherapist.
Measurement
Patients functional independence was measured by Katz and Lawton scales. The activities of daily living (ADL) - Katz scale was used to analyze independence in basic activities of daily living such as: bathing, dressing, toileting, transferring, continence and feeding. One point means the person is independent; zero points means the person requires assistance or total care. A total score of 0–2 points is interpreted as a significant impairment in activities of daily living, 3–4 points as a moderate impairment and 5–6 points as a good performance of these activities.23,24
The instrumental activities of daily living (IADL) - Lawton scale was used to assess independence in terms of instrumental activities of daily living such as: using the telephone, shopping, preparing food, housekeeping, doing laundry, using transportation, handling medications and handling finances. Similarly, to the ADL scale, a rating of 0–1 is used. The maximum score is 8 points. An IADL assessment helps determine whether a patient may require further assistance or care, and lower scores indicate a higher level of dependence.25
Hand grip strength was measured using a hand dynamometer (JAMAR, Sammons Preston Rolyan, USA). The measurement was performed in the sitting position in an armless chair, with the forearm in a 90-degree flexed position. The average of the three measurements (in kilograms) was recorded for the dominant hand.26 Additionally, the subjects were assessed with the use of subjective and objective functional scores or questionnaires containing data characterizing the group based on selected elements of the comprehensive geriatric evaluation.
In addition to HGS two tests were used to assess the physical performance. The short physical performance battery (SPPB) test was used to assess physical performance. It analyzes lower limb function and consists of three parts:
- SPPB CHAIR STAND TEST - stand up from a chair without using your arms five times.
- SPPB BALANCE TESTS - evaluates balance in three positions side-by-side stand, semi-tandem stand and tandem stand.
- SPPB GAIT SPEED TEST - walk a short distance (3 m).
- For each part, the participant receives from 0 to 4 points. The maximum score for SPPB is 12 points.27
Timed up and go (TUG) test was used to assess the risk of falls. If the subject moves using a cane or crutch/crutches, they perform the test using them. It is assumed that if the time required to perform the test (distance 3 m) exceeds 13.5 seconds then the risk of falling is increased.28
Statistical Analysis
Statistical analysis was conducted using the Statistica 13.3 software (StatSoft. Poland). A Shapiro–Wilk’s test was used to test normal distribution. In the absence of normal distribution of the investigated variables, the Mann–Whitney U-test was used to compare the groups. Nominal variables were compared with the Pearson’s chi-squared test. The Wilcoxon signed-rank test was used to compare the results before and after rehabilitation. Correlation analysis was performed using the Spearman’s rank correlation. Multivariate linear regression was used to determine predictors of change in ADL and the IADL after rehabilitation, which were considered to be dependent variables. Baseline HGS as well as the results of SPPB, TUG, age, and BMI were considered as explanatory variables in the model. The p-value of <0.05 was considered statistically significant.
Results
Study Group
From the initial 385 we included 239 patients who had undergone total hip replacement surgery in the statistical analysis. Sample size was determined based on the formula from Green 21 for the multiple correlation N ≥ 50 + 8m, where m is the number of predictors. The minimum sample size for this study is 180 persons. The mean age of all subjects was 72.79 ± 6.51 years. There were 132 females and 107 males in the study group. The characteristics of the study groups are presented in Table 1. Groups did not differ in terms of age, however there were significant differences in terms of HGS, SPPB, and TUG at the baseline (Table 1).
 |
Table 1 Baseline Characteristics of Groups |
Comparison Before and After Rehabilitation
Analyzing the test results obtained by the respondents before and after rehabilitation treatment, a statistically significant improvement was noted in all scales. Significance of each improvement was <0.001 in both groups. However, comparison of results after rehabilitation and after a six-month follow-up period showed that further progress was present only in the fracture group and only in terms of ADL (p = 0.043), IADL (p < 0.001) and SPPB (p < 0.001). There were no significant changes between measures after rehabilitation and after follow-up in osteoarthritis group. Table 2 presents the results comparing the study groups after rehabilitation and after six-month follow-up. In both measures there were significant differences between the osteoarthritis group and fracture group in terms of TUG (in favor of osteoarthritis group) and ADL (in favor of the fracture group).
 |
Table 2 Comparison of the Results Between the Study Groups After Rehabilitation and After Six-Month Follow-Up |
HGS as Predictor of Activities of Daily Living and the Instrumental Activities of Daily Living
Multiple linear regression of predictors of ADL and IADL revealed that in the osteoarthritis group a higher HGS predicted better results of ADL and IADL in follow-up and after rehabilitation, while in the fracture group HGS was a predictor only in terms of the IADL (Table 3). It is worth mentioning that, among all analyzed predictors, the strongest was the HGS association with IADL in the osteoarthritis group (standardized coefficient b*= 0.721), while other significant associations were rather weak (standardized coefficient b* < 0.4).
 |
Table 3 Multiple Linear Regression of Predictors of ADL and IADL After Rehabilitation and After Follow-Up |
In the osteoarthritis group, an increase in strength by 1 kg increases the chances of being in the group that improved the ADL and IADL score both immediately after rehabilitation (ADL, OR = 1.098; CI 95% 1.052–1.147 and IADL, OR = 1.182; CI 95% 1.103–1.267) and 6 months after its completion. (ADL, OR = 1.191; CI 95% 1.066–1.329 and IADL, OR = 1.096; CI 95% 1.012–1.186).
In the fracture group, an increase in strength by 1 kg increases the chances of being in the group that improved the ADL (OR = 1.081; CI 95% 1.015–1.152) immediately after rehabilitation and IADL both immediately after rehabilitation (OR = 1.122; CI 95% 1.046–1.205) and 6 months after its completion (OR = 1.090; 95% CI 1.021–1.64).
Discussion
The patients subjected to this study, underwent hip replacement surgery due to hip fractures or advanced osteoarthritis of the hip joint. Clinically useful scales were applied to aid in the analysis, such as Katz (ADL) and Lawton (IADL) scales, SPPB, and TUG, which are recommended by The National Institutes of Health (NIH).29–31 The main aim of the present study was to investigate HGS as a predictor of functional independence in older patients after total hip replacement and to asses potential differences in HGS's predicting ability between patients who had undergone surgery due to fractures and those who’s surgery was conducted due to osteoarthritis. Our research showed a statistically significant correlation between HGS and better functional independence measured by IADL and ADL in the osteoarthritis group while the correlation between HGS and better functional independence in the fracture group was observed only in regard to IADL. This research showed, that HGS predicts the ADL and IADL after hip replacement surgery and rehabilitation differently in patients operated on due to fractures and those who need to undergo surgery due to osteoarthritis.
Hershkovitz et al32 retrospectively studied data from 373 post-hip fracture patients. They found significant associations between HGS measured in admission to rehabilitation ward and functional outcomes measured by functional independence measure (FIM). Participants with higher HGS had greater chances of improvement in terms of functional independence. Selakovic et al33 conducted a study on patients after a hip fracture. The authors divided participants based on weak and strong hand grip groups, decided that a weak hand grip was defined by HGS <27 kg in males and < 16 kg in females according to revised cut-points for the diagnosis of sarcopenia formulated by the European Working Group on Sarcopenia in Older People (EWGSOP).34 Selakovic et al also found that patients with weak HGS had lower results in independence measures (Barthel Index) after a 3–6 month follow-up. The results obtained in our study are only partially consistent with results of above mentioned studies. In the present study HGS in the fracture group was associated only with IADL score after follow-up, and this association was low. These differences may be the result of using IADL and ADL as functional independence indicators. Due to different scoring scales between each scale, IADL and ADL are less capable of showing small changes in independence, while scales such as FIM are able to detect more precisely a patients state between full independence and full dependence.35
Studies assessing HGS as a predictor of functional independence after hip replacement surgery due to osteoarthritis are limited. Most of the studies are conducted without discrimination between an osteoarthritis group and a fracture group or are focused specifically on a fracture group. Therefore, it is hard to compare the results of the present study to the literature. Our results suggest that HGS is a more important prognostic factor in patients with osteoarthritis than in patients after a hip fracture. This can be a result of various negative consequences of osteoarthritis. Hip osteoarthritis causes a number of adverse outcomes, among them: pain, reduction of physical activity and lowered quality of life.36 Clynes et al37 showed that osteoarthritis can negatively impact patients’ functioning. Due to pain, swelling, inflammation patients with osteoarthritis suffer from reduced independence in activities of daily living.37 In Poland the waiting time for elective hip replacement surgery is often longer than one year.38 Waiting for the surgery that long can potentially aggravate negative symptoms and therefore lowering patients’ independence in activities of daily living.
Peng and Zeng argue that osteoarthritis and sarcopenia are related and could affect each other’s course.39 The authors claim that sarcopenia worsens rehabilitation effects and increases the risk of adverse outcomes after hip surgery. However not only osteoarthritis could be related with sarcopenia. Osteosarcopenia, a recently identified medical condition, encompasses the convergence of two age-related musculoskeletal disorders: sarcopenia and osteopenia or osteoporosis. The term “osteosarcopenia” has emerged to underscore the substantial overlap and interplay between these two conditions. Sarcopenia and osteoporosis share common risk factors and biological pathways including hormonal regulation. Individuals affected by osteosarcopenia face an escalated risk of experiencing detrimental outcomes, including falls, fractures, hospitalization, frailty, and even mortality.40,41 Osteosarcopenia is likely to have an impact on the outcome after replacement surgery.41 Regarding the present study, patients who constituted the osteoarthritis group and have a higher HGS are probably more active patients whose risk of sarcopenia is lower than in low HGS patients. This could be the explanation why in the osteoarthritis group patients’ independence was associated more with HGS than in the fracture group.
Numerous authors reported that high HGS is associated with better outcome after orthopedic surgery and especially hip replacement surgery.32,33,42–44 HGS measure is not only a useful indicator of a patient's overall condition but is also a predictor of short- and long-term surgery outcome. However, our study results suggest that predicting the value of HGS may differ between groups of patients with different causes of hip replacement surgery.
This study has some limitations. The first limitation is a group selection. Due to the design of the study and tools selected to measure the outcomes, patients with possible cognitive dysfunction were excluded. Our decision to exclude patients with MMSE scores below 23 points, which suggested dementia symptoms, was also based on doubts about whether these individuals would remember the physiotherapist’s exercise recommendations.22,45 Following such recommendations is important for cooperation with the rehabilitation team and allows the patient to reach positive functional results. Our participants performed a 120 minute individually tailored rehabilitation treatment for six days per week during a six-week treatment. Using different physical therapy procedures (such as cryotherapy, laser therapy, etc.) was a result of the hospital's ability to conduct rehabilitation and respond to a participant's individual needs, but it can also be considered as a limitation of the study.
The second limitation is the fact that selected participants were somewhat independent in terms of ADL and IADL. A group with lower scores in ADL and IADL scales may vary more in the degree of improvement therefore, differences between these groups could potentially be more prominent. Another limitation was the application of ADL and IADL scales which (due to their scoring) are less able to show small differences than scales with more complex scoring, such as FIM. There were also no data available about participants physical activity, nutritional status, self-motivation, life satisfaction and depression. These factors may influence rehabilitation outcomes, therefore including these covariates in future investigations should be taken into consideration.
Conclusions
The study showed that HGS measurement after hip replacement surgery predicts functional independence in basic and complex activities of daily living differently in patients operated on due to a fracture versus osteoarthritis. This finding needs to be confirmed by other studies with more diversified groups of participants, involving patients with very low and very high baseline independence. Using different scales measuring independence in activities of daily living such as FIM should be implemented to improve the possibility to detect smaller changes. Clinicians should be encouraged to include HGS assessment in their evaluation of patients who plan to undergo total hip replacement, in order to optimize the treatment of high-risk older patients, and especially patients with osteoarthritis. This can allow for the identification of osteoarthritis patients with low hand grip strength - who can be considered as patients with a higher risk of unsatisfying outcomes of surgery. These patients should undergo pre-rehabilitation and should be monitored, and/or supported in terms of rehabilitation after discharge.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no conflicts of interest.
References
1. Learmonth ID, Young C, Rorabeck C. The operation of the century: total Hip replacement. Lancet. 2007;370(9597):1508–1519. doi:10.1016/S0140-6736(07)60457-7
2. Gabbert T, Filson R, Bodden J, Coppola C. Summary: NAON’s best practice guideline, total hip replacement (Arthroplasty). Orthop Nurs. 2019;38(1):4–5. doi:10.1097/NOR.0000000000000520
3. Ibrahim MS, Twaij H, Giebaly DE, Nizam I, Haddad FS. Enhanced recovery in total Hip replacement: a clinical review. Bone Joint J. 2013;95(12):1587–1594. doi:10.1302/0301-620X.95B12.31303
4. Bachmeier CJ, March LM, Cross MJ, et al. A comparison of outcomes in osteoarthritis patients undergoing total Hip and knee replacement surgery. Osteoarthritis Cartilage. 2001;9(2):137–146. doi:10.1053/joca.2000.0369
5. Magaziner J, Hawkes W, Hebel JR, et al. Recovery from Hip fracture in eight areas of function. J Gerontol a Biol Sci Med Sci. 2000;55(9):M498–507. doi:10.1093/gerona/55.9.m498
6. Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following Hip fracture. BMC Geriatr. 2016;16(1):158. doi:10.1186/s12877-016-0332-0
7. Irwin SC, Hughes AJ, Sheehan E, Merghani K. Trends in Irish Hip fracture surgery over a 7-year period and international registry comparison. Surgeon. 2022;20(2):94–102. doi:10.1016/j.surge.2021.03.002
8. Kang JS, Jeon YS, Ahn CH, Roh TH. Osteosynthesis versus endoprosthesis for the treatment of femoral neck fracture in Asian elderly patients. BMC Musculoskelet Disord. 2016;17:264. doi:10.1186/s12891-016-1123-7
9. Rantanen T, Volpato S, Ferrucci L, Heikkinen E, Fried LP, Guralnik JM. Handgrip strength and cause-specific and total mortality in older disabled women: exploring the mechanism. J Am Geriatr Soc. 2003;51(5):636–641. doi:10.1034/j.1600-0579.2003.00207.x
10. Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol a Biol Sci Med Sci. 2006;61(10):1059–1064. doi:10.1093/gerona/61.10.1059
11. Cawthon PM, Fox KM, Gandra SR, et al. Do muscle mass, muscle density, strength, and physical function similarly influence risk of hospitalization in older adults? J Am Geriatr Soc. 2009;57(8):1411–1419. doi:10.1111/j.1532-5415.2009.02366.x
12. Mendes J, Azevedo A, Amaral TF. Handgrip strength at admission and time to discharge in medical and surgical inpatients. JPEN J Parenter Enteral Nutr. 2014;38(4):481–488. doi:10.1177/0148607113486007
13. Strandkvist V, Larsson A, Pauelsen M, et al. Hand grip strength is strongly associated with lower limb strength but only weakly with postural control in community-dwelling older adults. Arch Gerontol Geriatr. 2021;94:104345. doi:10.1016/j.archger.2021.104345
14. Meessen JM, Fiocco M, Tordoir RL, et al. Association of handgrip strength with patient-reported outcome measures after total Hip and knee arthroplasty. Rheumatol Int. 2020;40(4):565–571. doi:10.1007/s00296-020-04532-5
15. Visser M, Harris TB, Fox KM, et al. Change in muscle mass and muscle strength after a Hip fracture: relationship to mobility recovery. J Gerontol a Biol Sci Med Sci. 2000;55(8):M434–40. doi:10.1093/gerona/55.8.m434
16. Savino E, Martini E, Lauretani F, et al. Handgrip strength predicts persistent walking recovery after Hip fracture surgery. Am J Med. 2013;126(12):1068–75.e1. doi:10.1016/j.amjmed.2013.04.017
17. Chang C-M, Lee C-H, Shih C-M, Wang S-P, Chiu Y-C, Hsu C-E. Handgrip strength: a reliable predictor of postoperative early ambulation capacity for the elderly with Hip fracture. BMC Musculoskelet Disord. 2021;22(1):103. doi:10.1186/s12891-021-03964-9
18. Milman R, Zikrin E, Shacham D, Freud T, Press Y. Handgrip strength as a predictor of successful rehabilitation after hip fracture in patients 65 years of age and above. Clin Interv Aging. 2022;17:1307–1317. doi:10.2147/CIA.S374366
19. Visser M, Deeg DJ, Lips P, Harris TB, Bouter LM. Skeletal muscle mass and muscle strength in relation to lower-extremity performance in older men and women. J Am Geriatr Soc. 2000;48(4):381–386. doi:10.1111/j.1532-5415.2000.tb04694.x
20. Beloosesky Y, Weiss A, Manasian M, Salai M. Handgrip strength of the elderly after Hip fracture repair correlates with functional outcome. Disabil Rehabil. 2010;32(5):367–373. doi:10.3109/09638280903168499
21. Green SB. How many subjects does it take to do a regression analysis. Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/s15327906mbr2603_7
22. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–935. doi:10.1111/j.1532-5415.1992.tb01992.x
23. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of adl: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914–919. doi:10.1001/jama.1963.03060120024016
24. Katz S, Downs TD, Cash HR, Grotz RC. Progress in development of the index of ADL. Gerontologist. 1970;10(1):20–30. doi:10.1093/geront/10.1_part_1.20
25. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(1):179–186. doi:10.1093/geront/9.3_Part_1.179
26. Lee SH, Gong HS. Measurement and interpretation of handgrip strength for research on sarcopenia and osteoporosis. J Bone Metab. 2020;27(2):85–96. doi:10.11005/jbm.2020.27.2.85
27. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556–561. doi:10.1056/NEJM199503023320902
28. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
29. Suzman R, Beard JR, Boerma T, Chatterji S. Health in an ageing world--what do we know? Lancet. 2015;385(9967):484–486. doi:10.1016/S0140-6736(14)61597-X
30. Rodin MB, Mohile SG. A practical approach to geriatric assessment in oncology. J Clin Oncol. 2007;25(14):1936–1944. doi:10.1200/JCO.2006.10.2954
31. Jiang S, Li P. Current development in elderly comprehensive assessment and research methods. Biomed Res Int. 2016;2016:3528248. doi:10.1155/2016/3528248
32. Hershkovitz A, Yichayaou B, Ronen A, et al. The association between hand grip strength and rehabilitation outcome in post-acute Hip fractured patients. Aging Clin Exp Res. 2019;31(10):1509–1516. doi:10.1007/s40520-019-01200-y
33. Selakovic I, Dubljanin-Raspopovic E, Markovic-Denic L, et al. Can early assessment of hand grip strength in older Hip fracture patients predict functional outcome? PLoS One. 2019;14(8):e0213223. doi:10.1371/journal.pone.0213223
34. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
35. Pashmdarfard M, Azad A. Assessment tools to evaluate activities of daily living (ADL) and Instrumental Activities of Daily Living (IADL) in older adults: a systematic review. Med J Islam Repub Iran. 2020;34:33. doi:10.34171/mjiri.34.33
36. Liu M, Jin F, Yao X, Zhu Z. Disease burden of osteoarthritis of the knee and Hip due to a high body mass index in China and the USA: 1990–2019 findings from the global burden of disease study 2019. BMC Musculoskelet Disord. 2022;23(1). doi:10.1186/s12891-022-05027-z
37. Clynes MA, Jameson KA, Edwards MH, Cooper C, Dennison EM. Impact of osteoarthritis on activities of daily living: does joint site matter? Aging Clin Exp Res. 2019;31(8):1049–1056. doi:10.1007/s40520-019-01163-0
38. Organisation for Economic Co-operation and Development. Health at a Glance 2021: OECD Indicators: waiting times for elective surgery. Available from: https://www.oecd-ilibrary.org/sites/507433b0-en/1/3/2/5/13/index.html?itemId=/content/publication/507433b0-en&_csp_=69a1197833db420974a2940c01518500&itemIGO=oecd&itemContentType=book#.
39. Peng H, Zeng Y. Research progress on the correlation between sarcopenia and osteoarthritis. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022;36(12):1549–1557. doi:10.7507/1002-1892.202209015
40. Hamad B, Basaran S, Coskun Benlidayi I. Osteosarcopenia among postmenopausal women and handgrip strength as a practical method for predicting the risk. Aging Clin Exp Res. 2020;32(10):1923–1930. doi:10.1007/s40520-019-01399-w
41. Yoo JI, Kim H, Ha YC, Kwon HB, Koo KH. Osteosarcopenia in patients with hip fracture is related with high mortality. J Korean Med Sci. 2018;33(4):e27. doi:10.3346/jkms.2018.33.e27
42. Long G, Chao C, Ming-Sheng T, Ping Y. Low grip strength associated with clinical outcomes after total hip arthroplasty - A prospective case-control study. Orthop Surg. 2021;13(5):1488–1495. doi:10.1111/os.13007
43. Hashimoto S, Hatayama K, Terauchi M, Saito K, Higuchi H, Chikuda H. Preoperative hand-grip strength can be a predictor of stair ascent and descent ability after total knee arthroplasty in female patients. J Orthop Sci. 2020;25(1):167–172. doi:10.1016/j.jos.2019.03.003
44. Shyam Kumar AJ, Beresford-Cleary N, Kumar P, et al. Preoperative grip strength measurement and duration of hospital stay in patients undergoing total Hip and knee arthroplasty. Eur J Orthop Surg Traumatol. 2013;23(5):553–556. doi:10.1007/s00590-012-1029-5
45. Shin C, Park MH, Lee S-H, et al. Usefulness of the 15-item geriatric depression scale (GDS-15) for classifying minor and major depressive disorders among community-dwelling elders. J Affect Disord. 2019;259:370–375. doi:10.1016/j.jad.2019.08.053
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024