Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Do Right, Be Bright: A Protocol on the Development of an Inter-Professional Health Intervention Model for Pre-School Children Through a Community-Based Service-Learning Initiative
Authors Bilal S, Misra S ![]() , Hussain S, Tan SS, Priya E
, Hussain S, Tan SS, Priya E
Received 16 January 2023
Accepted for publication 6 April 2023
Published 10 May 2023 Volume 2023:16 Pages 1301—1310
DOI https://doi.org/10.2147/JMDH.S405031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sobia Bilal,1 Snigdha Misra,2 Sumaira Hussain,3 Seok Shin Tan,2,4 Ekta Priya5
1Division of Prevention and Public Health Sciences, Pediatric Dentistry, College of Dentistry, University of Illinois Chicago, Chicago, IL, USA; 2Division of Nutrition and Dietetics, School of Health Sciences, International Medical University, Kuala Lumpur, Malaysia; 3Department of Community Medicine, School of Medicine, International Medical University, Kuala Lumpur, Malaysia; 4Jeffrey Cheah School of Medicine and Health Sciences, Monash University Malaysia, Bandar Sunway, Malaysia; 5MRC/CSO Social and Public Health Sciences Unit, School of Health and Wellbeing, University of Glasgow, Glasgow, Scotland
Correspondence: Snigdha Misra, Division of Nutrition and Dietetics, School of Health Sciences, International Medical University, Kuala Lumpur, Malaysia, Tel +603-2731 7608 ; +6016-617 9247, Fax +603-8656 7229, Email [email protected]
Abstract: An inter-professional project with a collaborative endeavor between the programs of Dentistry, Nutrition and Medicine was carried out with the aim to emphasise oral health maintenance, making the right nutritional choices and effective hand washing among pre-school children. The purpose of this paper is to share a detailed description of the design, development process, implementation, and planned evaluation of an interprofessional school-based health promotion intervention model “Do Right, Be Bright”. This model is part of a quasi-experimental study, targeting pre-school children as the “Targets of Change” through the empowerment of school teachers as the “Agents of Change”. The program design was based on Bartholomew’s Intervention Mapping Approach, which proposes a direction for developing a theory-based health promotion intervention and on the most extensively applied theories of health behavior, the Health Belief Model. Therefore, based on a thorough literature review and needs assessment, three key areas of needs were identified for the targeted preschool children: oral hygiene, hand hygiene and nutrition. The efficacy of this model will be pilot tested in a preschool in Kuala Lumpur Malaysia.
Keywords: oral hygiene, hand hygiene, nutrition, interprofessional education, health-promoting schools
Introduction
The Health Promoting School (HPS) initiative by the World Health Organization aims to attain organizational and structural change to create a supportive social and physical environment, improve its curricula, teaching and learning methods in schools and move beyond individual behavioral change. The six key features of HPS are (1) Healthy school policies, (2) Physical school environment, (3) Social school environment, (4) Health skills and education, (5) Links with parents and community, (6) Access to (school) health services.1 It is well established that health and education are intrinsically linked. Studies suggested that healthy children are more likely to learn effectively. Health promotion can help schools to meet their social aims and to improve educational attainment while young people that attend school have a better chance of good health.2,3 The focus should lay on child and adolescent public health for successfully achieving the universal establishment of health-promoting schools. This would subsequently improve health literacy and create a supportive environment for health.4 Healthy children and adolescents require appropriate measures from early childhood development and sustained throughout adolescence and adulthood. Early consideration of child and adolescent health by implementing interventions that reduce or eliminate risk exposure will contribute to the developmental phases and produce healthy active adults.4,5 Effective measures to protect and promote the health of children and adolescents involve equitable, sustainable and large numbers of the population.
At a global level, several school-based initiatives have been launched to promote the health of children and adolescents.6,7 There are several examples that illustrate the benefits of implementing school-based health interventions among children. These include handwashing, oral health, and nutrition programs.8–12 When implemented collectively in a school setting, this is known as a school health and nutrition program. Globally, this program has been found to be a cost-effective strategy for successfully improving children’s health, especially in low- and middle-income countries.13 School health and nutrition program capitalizes on using existing resources, through schools, a powerful setting, to provide timely support, and deliver preventive measures as well as safe and simple treatments. This is on top of providing health education and protective behavior change messaging to improve the health of school children.13,14 To be most effective, these programs can be customized to meet the needs of the targeted community. In areas where children are suffering from various conditions, converging multiple interventions onto a single platform allows for maximizing efficiency, the scale of impact and sustainability.15 The HPS framework has been employed to implement oral health interventions in several countries such as Taiwan,16 the United Kingdom,17 and Canada.18
In Malaysia, the school health program under the Ministry of Health is a comprehensive and systematic program carried out in government schools. For instance, this program provides oral healthcare to primary and secondary school children through a wide network of school dental clinics and mobile dental teams. It utilizes the outreach approach which has aided in increased coverage of oral health care to school children.19
School Health Service has three main components namely: School Health Service, School Dental Service and School Environmental Health Service. Priority is given to government-aided schools. Under this service school, children receive preventive health services, health screening, treatment of mild cases and referral to a health centre or hospital. Contrastingly, there is no structured program for school children in the private sector. Health services are provided based on the needs and demands of the community. A preliminary needs assessment carried out in the non-government schools reported that there is a lack of awareness and skills in terms of oral health, hygiene, and nutrition among the children. Therefore, an intersectoral and interprofessional collaboration was developed to promote more sustainable change by focusing on the prevention of oral health, nutrition and hygiene-related diseases and associated risks.
The aim of this paper is to share the development process, implementation, and evaluation plan of an interprofessional school-based health promotion intervention model “Do Right, Be Bright”. This model emphasizes oral health maintenance, correct nutritional choices and effective hand washing among preschool children through the empowerment of schoolteachers as “Agents of Change”.
Materials and Methods
This quasi-experimental study was approved by the International Medical University Institutional Joint Research and Ethics Committee (Ethic Approval Number: JCM-184/2019). This protocol complies with the Declaration of Helsinki. “Do Right, Be Bright” (DRBB) is an inter-professional school-based health promotion intervention model for preschool children, aged four to six years old, piloted in Malaysia. This intervention also targeted training the schoolteachers as “Agents of Change” (AOC) for a more sustainable health promotion initiative. Written consent was obtained from the school and from the parents of the preschool children, prior to the commencement of the study. Evidence suggests that the success of such training programs is dependent on the selection of a suitable behavior-changing model.20
This inter-professional project was a collaborative endeavor between the Dentistry, Nutrition and Medicine programs of the International Medical University, Kuala Lumpur, Malaysia. Multiple discussions were held with to obtain consensus on the approaches of each profession to design the model. This multidisciplinary approach was based on the understanding whereby individual health interventions would be more effective when packaged together. This intervention aspires to instill good health practices among preschool children and educate the teachers and parents on different health conditions, which may go unnoticed due to the lack of awareness.
It is evidenced that good practices during the early days of life translate into healthy behaviour in later years.21 Hence, this model is developed based on Bartholomew’s Intervention Mapping Approach, which proposes a direction for developing a theory-based health promotion intervention that includes six comprehensive steps as described below.22
Step 1: Needs Assessment
The community partner identified for this model was a private preschool, with a chain of branches across Kuala Lumpur, Malaysia. The preschool children (four-six years) were identified for piloting this model. A needs assessment was executed about oral health status, hand washing practices and food preferences of preschool children. Three key areas were identified from the needs assessment: oral hygiene, hand hygiene and nutrition.
According to WHO, Collaborative practice happens when multiple health workers from different professional backgrounds work with patients, families, carers, and communities to deliver the highest quality of care across settings.23 The Interprofessional collaborative team involved three professions: dentistry, community medicine and nutrition. A thorough literature search was carried out by the team based on the identified areas. The researchers from each profession created an interprofessional DRBB model to address the needs identified. Subsequently, the team engaged with the school administration to establish a participatory approach. A briefing was also given to all the teachers on the proposed model to develop a sustainable teacher-centered school-based health promotion model and designated them as AOC. The AOC was empowered to sustain change as they were in constant touch with the preschool children. These preschool children are referred to as the “Targets of Change” (TOC).
Step 2: Specify the Objectives
In this step, the interprofessional collaborative team identified the specific programme outcomes based on the three health domains determined during the needs assessment.
Dental Health
- To screen the dental status of TOC.
- To assess the knowledge and practices of the TOC towards oral health.
- To enhance knowledge of TOC towards the significance of good oral hygiene.
- To promote good oral hygiene skills and practices among TOC.
- To empower the schoolteachers as AOC for tooth brushing drills in efforts to promote sustainable enforcement of oral health practices.
Nutrition
- To assess the nutritional status of the TOC.
- To assess the knowledge, practices and eating habits of the TOC.
- To enhance knowledge of TOC on healthy eating.
- To promote healthy eating practices among TOC.
- To empower the schoolteachers as AOC for healthy eating to promote good nutrition among the TOC.
Effective Hand Washing
- To assess the knowledge and practices of TOC towards hand washing.
- To enhance knowledge of TOC towards the significance of effective hand washing.
- To promote effective hand-washing skills and practices among TOC.
- To empower the schoolteachers as AOC for effective hand washing drills in efforts to promote hand hygiene.
Step 3: Strategy of “Do Right, Be Bright” Based on the “Health Belief Model”
The DRBB model is developed based on the most extensively applied theories of health behavior, the Health Belief Model (HBM). HBM is a psychological model which explains and predicts preventive health behavior. It consists of six domains that influence health behavior:24,25
- perceived susceptibility (possibility of facing disease)
- perceived severity (beliefs about the disease outcomes)
- self-efficacy (ability to successfully perform the recommended behavior)
- perceived benefits (understand the benefits of adopting a new behavior)
- perceived barriers (obstacles that prevent from performing a behavior)
- cues to action (internal and external stimuli)
The HBM model suggests individuals are more likely to act to prevent illness if they are provided with a particular course of action that promotes the change. The DRBB model is designed using six action-related factors of HBM:
- collecting information on the baseline health status with respect to dental health, nutrition, and handwashing practices of TOC.
- health education on disease and its consequences to training the AOC on how to recognize disease susceptibility and severity. (HBM domain: perceived susceptibility and severity)
- skill development on tooth brushing drills, making healthy food choices and effective handwashing are recommended actions. (HBM domain: perceived benefits and self-efficacy)
- recognizing and minimizing barriers to action through needs assessment and discussions with school management. (HBM domain: perceived barriers)
- development of a school environment that promotes action towards healthy behaviour through reinforcement of external stimuli (health education material and drills). (HBM domain: cues to action)
- exhibiting teacher-centered sustainable skill development activities to enhance self-efficacy and support the TOC for behaviour change. (HBM domain: self-efficacy and cues to action)
Step 4: Design of the “Do Right, Be Bright” Model
The framework of the DRBB is presented in Figure 1. This initiative was carried out in three Phases (Figure 2).
 |
Figure 1 Framework of DRBB. |
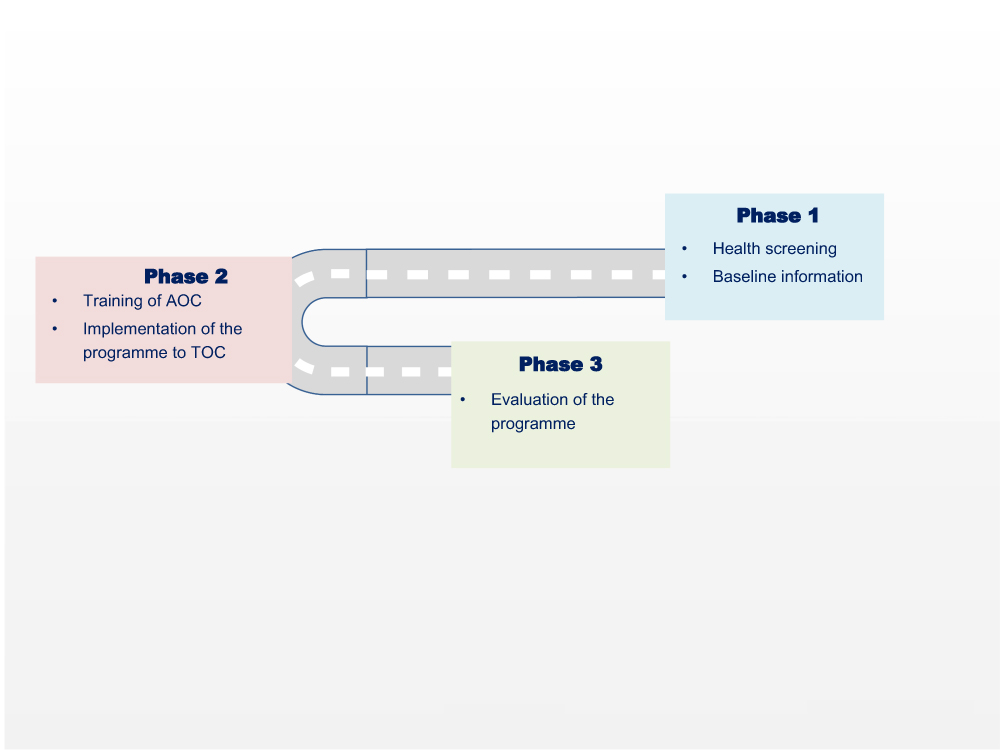 |
Figure 2 Phases of the DRBB program. |
Phase 1 DRBB Program
This phase focuses on health screening and the collection of baseline information.
Pre-school children (TOC):
- Parental consent was obtained for the TOC, enrolled in the project.
- They were screened for oral health and nutritional status.
- Information on oral health, eating habits and handwashing was collected using the knowledge, attitude, and practices (KAP) survey instrument.
Phase 2 DRBB Program
This phase focuses on the interventions of DRBB. It involves empowering the AOC for sustainable enforcement of health practices among the TOC. The following activities were carried out.
- Increase awareness of the importance of maintaining good hand and oral hygiene as well as healthy eating (through educational interactive games and role-play activities).
- increase awareness of the harmful effects of excessive sugar intake.
- Skill development through proper tooth brushing, effective hand washing drills and selection of healthy food choices.
Phase 3 DRBB Program
This phase focuses on the outcome evaluation of DRBB.
- Assessment of the effectiveness of maintaining good oral hygiene, handwashing, and making the right food choices was conducted using the post-intervention KAP survey.
- The sustainability and compliance of tooth brushing, hand washing drills and reinforcement of healthy eating practices by the AOC were also evaluated.
- The oral hygiene status, nutritional status and hand hygiene practices of the TOC were assessed after one year of the program.
Step 5: Implementation and Evaluation of Intervention
Phase 1
This phase focuses on the needs assessment of the TOC. The needs assessment was based on STEPS, which is the WHO’s recommended tool for the surveillance of non-communicable diseases (NCDs) and their risk factors.26 STEPS is a sequential process and starts with gathering key information on risk factors with a questionnaire; then moves to simple physical measurements, followed by a more complex collection of samples for biochemical analysis. This approach emphasizes that small amounts of good-quality data are more valuable than large amounts of poor data. Both STEP 1 and 2 have been adapted and incorporated into this study as reported in Table 1.
 |
Table 1 Adaptation of STEP 1 and 2 in DRBB Model |
Instruments Used in STEP 1
The instruments used for STEP 1 were to collect demographic Information.
Oral Hygiene
- Parents of TOC and AOC: The oral hygiene questionnaires sought information on socio-demographics, knowledge, attitude, and oral health practices. The questionnaires were adapted from previous studies.27–30
Snacking habits of the children
- Children’s dietary intake and snacking habits were assessed using the Child Diet Questionnaire, 2-day 24-hour dietary recall and Food Preference Questionnaire for Children by the parents.31
Food Parenting Practices
- Child feeding questionnaire (CFQ) was used to assess child feeding in aspects related to parents’ beliefs, attitudes, and practices. There are seven domains in CFQ which include parental perception of feeding responsibility, parental perception of own overweight, parental perception of their child’s overweight, concern about child weight, parental monitoring of child eating habit, parental restriction of food intake and parental pressure to eat.32 A 5-point Likert scale from 1 (never) to 5 (always) will be used to capture the responses. A higher mean score in each domain indicates higher levels of parental concern and control in child feeding (restriction, pressure to eat and monitoring) respectively.
Handwashing status of the children
- Knowledge, attitude, and practices (KAP) survey was conducted at baseline to assess existing knowledge about handwashing. Leave record was obtained from the year before to make comparisons of absenteeism pre/post-intervention.
Instruments Used in STEP 2
The instruments used for STEP 2 were to collect physical measurements of TOC.
Clinical examination form:
- DMFT/dmft: For dmft, the teeth not counted are unerupted and congenitally missing teeth and supernumerary teeth. The rules for recording d, m, and f are the same as for DMFT. The total count is 20 teeth. For dmfs, the teeth not counted are the same as for dmft. As with DMFS, there are five surfaces on the posterior teeth and four surfaces on the anterior teeth. The total count is 88 surfaces.33
- Visible plaque index (VPI): The VPI is recorded as follows: after drying the teeth with an air syringe, visible microbial deposits will be assessed with the naked eye in the cervical third and, with the use of a dental explorer, on the four surfaces (mesial, distal, facial, or buccal, and lingual) of all the existing teeth. Code zero is assigned when there is no visible plaque, and code one is assigned when a visible plaque is present.34
Nutritional status of the children
- Weight and height of the children were measured using TANITA digital weighing scale and SECA collapsible stadiometer, respectively. WHO growth charts (weight-for-age, height-for-age, weight-for-height, and BMI-for-age) were used to determine the nutritional status of the children.
Phase 2: Intervention Phase
Nutbeam’s outcome model for health promotion intervention was used in this study.35 This model complements both Phase 2 and 3 (Figure 3). This phase focused on educating and training the AOC and TOC on oral health practices, hand washing, and healthy eating.
 |
Figure 3 Intervention Phase based on Nutbeam’s Outcome model. |
Phase 3: Evaluation of the Program
This phase evaluated the effectiveness of the DRBB model. Oral hygiene status and caries increment of the TOC were assessed. Their knowledge, attitude, and practice were also reassessed to compare pre-and post-intervention. Clinical examination was carried out after twelve months to evaluate the plaque scores, gingival status, and dental caries increment. The effectiveness of the handwashing intervention was assessed through a post-intervention KAP survey along with the assessment of TOC’s absenteeism due to illness. The nutritional status of the TOC was assessed after twelve months. Pre- and post-intervention data were compared.
Step 6: Long-Term Sustainable Integration: Empowering the AOC
A successful health-promoting school initiative greatly relies on personnel, resources, funding, and policy. DRBB model focuses on training the AOC, as an initiative to achieve long-term sustainable integration. There are multiple benefits of implementing school-based health interventions among children. These include handwashing, oral health, and nutrition programs. A training module encompassing health promotion for oral health, nutrition and hygiene was developed for the AOC. The AOCs were trained to carry out periodic interventions in all the three areas identified. The module also had different activities to engage the TOC while educating them on the health parameters.
Due to COVID-19, the face-to-face intervention was hampered. To ensure the sustainability of the DRBB program, technology was used to carry out the activities and reiterate the messages. The drill sessions of the AOC were conducted synchronously to engage with the TOC and follow up with the skills acquired by them. Barriers to non-compliance were identified and addressed, depending on their nature.
Conclusion
The DRBB health promotion model is an interprofessional initiative based on Bartholomew’s Intervention Mapping Approach and health belief model. The paper describes the robust design, development, implementation, and planned evaluation of this model among selected preschool children in Kuala Lumpur, Malaysia. The DRBB model can help health promoters to develop a theory and evidence-based programs through the identification of key modifiable determinants of health behaviors, the choice of intervention methods and applications and the development of implementation strategies.
Acknowledgments
This study was supported by The Beaconhouse School, Kuala Lumpur, Malaysia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Health-Promoting Schools Series 5: Regional Guidelines Development of Health-Promoting schools—a Framework for Action. WHO Regional Office for the Western Pacific; 1996.
2. Langford R, Bonell C, Jones H, et al. The World Health Organization’s Health Promoting Schools framework: a Cochrane systematic review and meta-analysis. BMC Public Health. 2015;15(1):1–5. doi:10.1186/s12889-015-1360-y
3. Lee A, Lo A, Li Q, Keung V, Kwong A. Health promoting schools: an update. Appl Health Econ Health Policy. 2020;18(5):605–623. doi:10.1007/s40258-020-00575-8
4. Barnekov V, Buijs G, Clift S, et al. The health promoting school: a resource for developing indicators. Int Planning Commit Eur Network Health Promoting Sch Task Force. 2006;1:53.
5. Laski L. Realising the health and wellbeing of adolescents. BMJ. 2015;14:351.
6. WHO and UNESCO. Making Every School a Health-Promoting School: Country Case Studies. WHO and UNESCO; 2021.
7. WHO and UNESCO. Global Standards for Health Promoting Schools and Their Implementation Guidance. WHO and UNESCO; 2018.
8. Bramantoro T, Santoso CM, Hariyani N, et al. Effectiveness of the school-based oral health promotion programmes from preschool to high school: a systematic review. PLoS One. 2021;16(8):e0256007. doi:10.1371/journal.pone.0256007
9. Tidwell JB, Gopalakrishnan A, Unni A, et al. Impact of a teacher-led school handwashing program on children’s handwashing with soap at school and home in Bihar, India. PLoS One. 2020;15(2):e0229655. doi:10.1371/journal.pone.0229655
10. McIsaac JL, Penney TL, Ata N, et al. Evaluation of a health promoting schools program in a school board in Nova Scotia, Canada. Prev Med Rep. 2017;5:279–284. doi:10.1016/j.pmedr.2017.01.008
11. Yusof ZY, Jaafar N. Health promoting schools and children’s oral health related quality of life. Health Qual Life Outcomes. 2013;11(1):1–9. doi:10.1186/1477-7525-11-205
12. Rana L, Alvaro R. Applying a Health Promoting Schools approach to nutrition interventions in schools: key factors for success. Health Promot J of Austr. 2010;21(2):106–113. doi:10.1071/HE10106
13. Shrestha RM, Ghimire M, Shakya P, Ayer R, Dhital R, Jimba M. School health and nutrition program implementation, impact, and challenges in schools of Nepal: stakeholders’ perceptions. Trop Med Health. 2019;47(1):1. doi:10.1186/s41182-019-0159-4
14. Turunen H, Sormunen M, Jourdan D, von Seelen J, Buijs G. Health promoting schools—a complex approach and a major means to health improvement. Health Promot Int. 2017;32(2):177–184. doi:10.1093/heapro/dax001
15. Allen G. Early Intervention: The Next Steps. An Independent Report to Her Majesty’s Government. London: HM Government; 2011.
16. Wei CT, Lo KY, Lin YC, Hu CY, Chen FL, Huang HL. Effects of health-promoting school strategy on dental plaque control and preventive behaviors in schoolchildren in high-caries, rural areas of Taiwan: a quasi-experimental design. BMC Oral Health. 2021;21:1. doi:10.1186/s12903-021-01927-z
17. Kwan SY, Petersen PE, Pine CM, Borutta A. Health-promoting schools: an opportunity for oral health promotion. Bull World Health Organ. 2005;83(9):677–685.
18. Macnab A, Kasangaki A. ‘Many voices, one song’: a model for an oral health programme as a first step in establishing a health promoting school. Health Promot Int. 2012;27(1):63–73. doi:10.1093/heapro/dar039
19. Ministry of Health. Oral Healthcare for Schoolchildren in Malaysia. Ministry of Health Malaysia; 2006.
20. Anstrom C, Kimberlin D, Sunnarborg K, et al. Parents and teachers acting as change agents: the influence of nutritional knowledge to support the development of healthy behaviors in children in rural Appalachia. J Acad Nutr Diet. 2017;117(9):A91. doi:10.1016/j.jand.2017.06.079
21. Frech A. Healthy behavior trajectories between adolescence and young adulthood. Adv Life Course Res. 2012;17(2):59–68. doi:10.1016/j.alcr.2012.01.003
22. Bartholomew Eldredge L, Markham C, Ruiter R, Fernandez M, Kok G, Parcel G. Planning Health Promotion Programs.
23. WHO. Framework for Action on Interprofessional Education and Collaborative Practice. World Health Organization; 2010.
24. Champion VL, Skinner CS. The health belief model. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior and Health Education: Theory, Research, and Practice. Jossey-Bass; 2008:45–65.
25. Maiman LA, Becker MH. The health belief model: origins and correlates in psychological theory. Health Educ Monogr. 1974;2(4):336–353. doi:10.1177/109019817400200404
26. WHO. STEPwise Approach to NCD Risk Factor Surveillance (STEPS). WHO; 2020. Available from: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps.
27. Singhal K, Prasanth MA, Singh V, Choudhary R. Knowledge, attitude & practice of parents about child oral health in Jodhpur city: a questionnaire survey. Int J Dent Med Res. 2015;1(6):37–41.
28. Ramroop V, Wright D, Naidu R. Dental health knowledge and attitudes of primary school teachers toward developing dental health education. West Indian Med J. 2011;60(5):576–580.
29. Lian CW, Phing TS, Chat CS, Shin BC, Baharuddin LH, Jalil ZB. Oral health knowledge, attitude and practice among secondary school students in Kuching, Sarawak. Archives of Orofacial Sciences. 2010;5(1):9–16.
30. Lang WP, Woolfolk MW, Faja BW. Dental health knowledge and attitudes of elementary school teachers in Scientifica Michigan. J Public Health Dent. 1989;49(1):44–50. doi:10.1111/j.1752-7325.1989.tb02020.x
31. Fildes A, van Jaarsveld CH, Llewellyn CH, Fisher A, Cooke L, Wardle J. Nature and nurture in children’s food preferences. Am J Clin Nutr. 2014;99(4):911–917. doi:10.3945/ajcn.113.077867
32. Birch LL, Fisher JO, Grimm-Thomas K, Markey CN, Sawyer R, Johnson SL. Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite. 2001;36(3):201–210. doi:10.1006/appe.2001.0398
33. Cappelli D, Mobley C. Prevention in Clinical Oral Health Care. Mosby Elsevier; 2008.
34. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque. Int Dent J. 1975;25(4):229–235.
35. Nutbeam D. Evaluating health promotion—progress, problems and solutions. Health Promot Int. 1998;13(1):27–44. doi:10.1093/heapro/13.1.27
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.