Back to Journals » International Journal of Women's Health » Volume 17
Do Human Papilloma Virus and Cytological Testing Results Before Colposcopy Alter the Pathological Grading of Colposcopy Acetic Acid Visual Examination?: A Retrospective Study
Authors Gao S ![]() , Qian B
, Qian B ![]() , Wang T
, Wang T ![]() , Wang J
, Wang J
Received 7 August 2024
Accepted for publication 24 January 2025
Published 30 January 2025 Volume 2025:17 Pages 201—209
DOI https://doi.org/10.2147/IJWH.S490355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Songkun Gao,1 Boyang Qian,2 Tong Wang,1 Jiandong Wang1
1Gynecologic Oncology Department,Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, 100026, People’s Republic of China; 2Nantong University, Nantong, Jiangsu, 226019, People’s Republic of China
Correspondence: Tong Wang; Jiandong Wang, Gynecologic Oncology Department,Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, 100026, People’s Republic of China, Email [email protected]; [email protected]
Objective: To understand whether human papillomavirus (HPV) and cytological testing (TCT [ie, “thinprep” cytological testing]) results can provide more information beyond visual information for vaginal colposcopy examinations to upgrade or downgrade the visual diagnosis of vaginal colposcopy.
Patients and Methods: Data from 519 patients, who underwent vaginal colposcopy at the Beijing Obstetrics and Gynecology Hospital (Beijing, China) between January and June 2020, were included. Preoperative HPV and TCT results were statistically analyzed, and were divided into 3 groups according to postoperative cervical tissue pathological diagnosis: negative; low-grade squamous intraepithelial (LSIL); and high-grade squamous intraepithelial lesion (HSIL). Positive and negative predictive values for cervical inflammation, LSIL, and HSIL in patients diagnosed using vaginal colposcopy, based on cervical pathological grouping, and differences in HPV and TCT results among patients who underwent vaginal colposcopy, were analyzed.
Results: The age of patients diagnosed with cervicitis, LSIL, and HSIL using colposcopy gradually decreased, and the proportion of HPV16/18 infection in the HSIL group was significantly higher than the other 2 groups. There were significant differences in TCT results among the groups. According to pathological results from cervical tissue specimens, among all groups diagnosed using colposcopy, the age of the HSIL group was significantly younger than that of the other groups, and the proportion of patients with a TCT greater than LSIL was significantly higher than that of the other groups.
Conclusion: HPV did not provide additional information for vaginal colposcopy. Young(er) patients and those with a TCT greater than LSIL may consider upgrading the vaginal colposcopy diagnosis based on imaging information.
Keywords: vaginal colposcopy acetic acid visual diagnosis, cervical precancer, HPV, TCT
Introduction
Cervical cancer is the fourth most common cancer worldwide, accounting for 6.5% of all malignant tumors among women worldwide.1 Approximately 100,000 patients undergo treatment for precancerous cervical lesions annually.2 Cytological testing (TCT [ie, “thinprep” cytology testing]), visual inspection with acetic acid (VIA), and human papilloma virus (HPV) testing are the main screening methods for colposcopy.3 Digital colposcopy uses microscopy to examine the cervix and vagina, and can, to a certain extent, magnify and finely identify the junctions of scales and blood vessels. VIA during colposcopy is a simple, safe, and effective diagnostic method.4 However, it requires a specific level of physician skill/experience.5 Currently, the positive predictive rate of colposcopy is approximately 50%. Preoperative HPV and TCT results can provide additional textual information to supplement colposcopy imaging data, which can provide a basis for upgrading or downgrading colposcopy diagnosis. However, there is currently a lack of relevant research investigating the relationship between HPV and TCT results and colposcopy diagnosis results. As such, this study collected data from patients who underwent vaginal colposcopy examination in our hospital and their preoperative HPV and TCT results, to clarify whether preoperative examination can provide specific reference information for vaginal colposcopy visual diagnosis.
Materials and Method
This retrospective study included data from 933 patients who underwent vaginal colposcopy at Beijing Obstetrics and Gynecology Hospital (Beijing, China) between January and June 2020. The inclusion criteria were as follows: underwent vaginal colposcopy and multipoint cervical biopsy during surgery; pathology confirmed grading of cervical precancerous lesions; and underwent preoperative HPV and TCT examinations, with relevant results recorded in the medical record system. Patients who underwent surgery, including cervical resection (such as Manchurian surgery or total hysterectomy for various reasons), before undergoing colposcopy, and pregnant women were excluded from the study.
The ages of patients who underwent vaginal colposcopy and cervical biopsy, as well of HPV and TCT test results before the examination, were collected. All colposcopy examinations and cervical biopsies were performed by approved colposcopy examining physicians. Results of vaginal colposcopy examination and pathological diagnosis of postoperative multipoint cervical biopsy specimens were collected. Pathological results were obtained by 2 qualified pathologists. Based on the results of the vaginal colposcopy examination, patients were divided into 3 groups: normal; low-grade squamous intraepithelial (LSIL); and high-grade squamous intraepithelial lesion (HSIL). Based on pathological diagnosis of cervical biopsy specimens, patients in each group were further divided into negative (including inflammation and visible foam cells), LSIL, and HSIL groups. The vaginal colposcopy and cervical specimen pathological diagnoses of patients at different stages of cervical precancerous lesions, screened patients with different vaginal colposcopy and cervical specimen pathological diagnoses, were compared. The relationship between preoperative HPV test and TCT results, and differences in visual and pathological diagnosis, were analyzed.
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by the Ethics Committees of Beijing Obstetrics and Gynecology Hospital, Capital Medical University (Beijing, China; No:2023-KY-021-01).
Test Methods
HPV Testing
Cervical scrape specimens were gently collected from the squamocolumnar junction of the cervix using a sampling brush. HPV genotypes were determined using a commercially available kit (23-HPV Genotyping Real-time PCR Kit, Hybribio, China), which detects 15 high-risk HPV types (HPV 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82), in accordance with manufacturer’s instructions.
Liquid-Based TCTs
Cells were collected from the ectocervix and cervical canal using a cervical canal brush. The cells attached to the small brush were then eluted into vials containing a cell preservation solution and sent to the pathology department (Beijing Obstetrics and Gynecology Hospital, Capital Medical University, China). The laboratory physician provided the final report.
Colposcopy
Colposcopic biopsy was performed according to operating procedures for colposcopy using a German Lescon photoelectric integrated electronic colposcopy system. Colposcopy was performed in accordance with the diagnostic criteria of the International Federation of Cervical Pathology and Colposcopy (IFPCC) and ASCCP.6,7 The colposcopy images were graded as normal, bend/low-grade lesions (LSIL), high-grade lesions (HSIL), and invasive cancer.
Detection of Pathology
Serial sections of cervical tissue specimens were prepared and histology was performed by 2 senior physicians from the pathology department of the authors’ hospital, who read the films and performed the examination, diagnosis, and treatment. The pathological classification was based on the 2014 World Health Organization Female Genitalia classification. According to the oncology classification criteria, LSIL included CIN1 and p16-negative CIN2, and HSIL included P16-positive CIN2 and CIN3.
Statistical Methods
All statistical analyses were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY, USA), Sigmastat version 3.5 (sigmastat.software.informer.com/) and spreadsheet software (Excel, Microsoft Corp., Redmond, WA, USA). Grading data are described using the frequency and composition ratio. Differently grouped data were compared using chi-squared analysis, while continuous data were analyzed using Kruskal–Wallis one-way analysis of variance (ie, “ANOVA”). Differences with p < 0.05 were considered to be statistically significant. According to the Bonferroni method, the p value was corrected to 0.017 for the 3 groups in each experiment.
Results
Data from 519 patients were included in this study, including 158 diagnosed with cervicitis by colposcopy, 256 with LSIL, 97 with HSIL, and 9 with cervical cancer (Table 1). If cervical cancer lesions could be directly observed during gynecological examinations without further HPV and TCT testing, most patients with cervical cancer were excluded from the study. Among the patients screened for vaginal colposcopy diagnosis of cancer in this study, 4 had cervical tissue pathology indicating cancer, 3 had HSIL, and 1 had LSIL. Due to the small number of patients who underwent HPV testing and TCT, patients with cervical cancer detected by colposcopy were not included in this study.
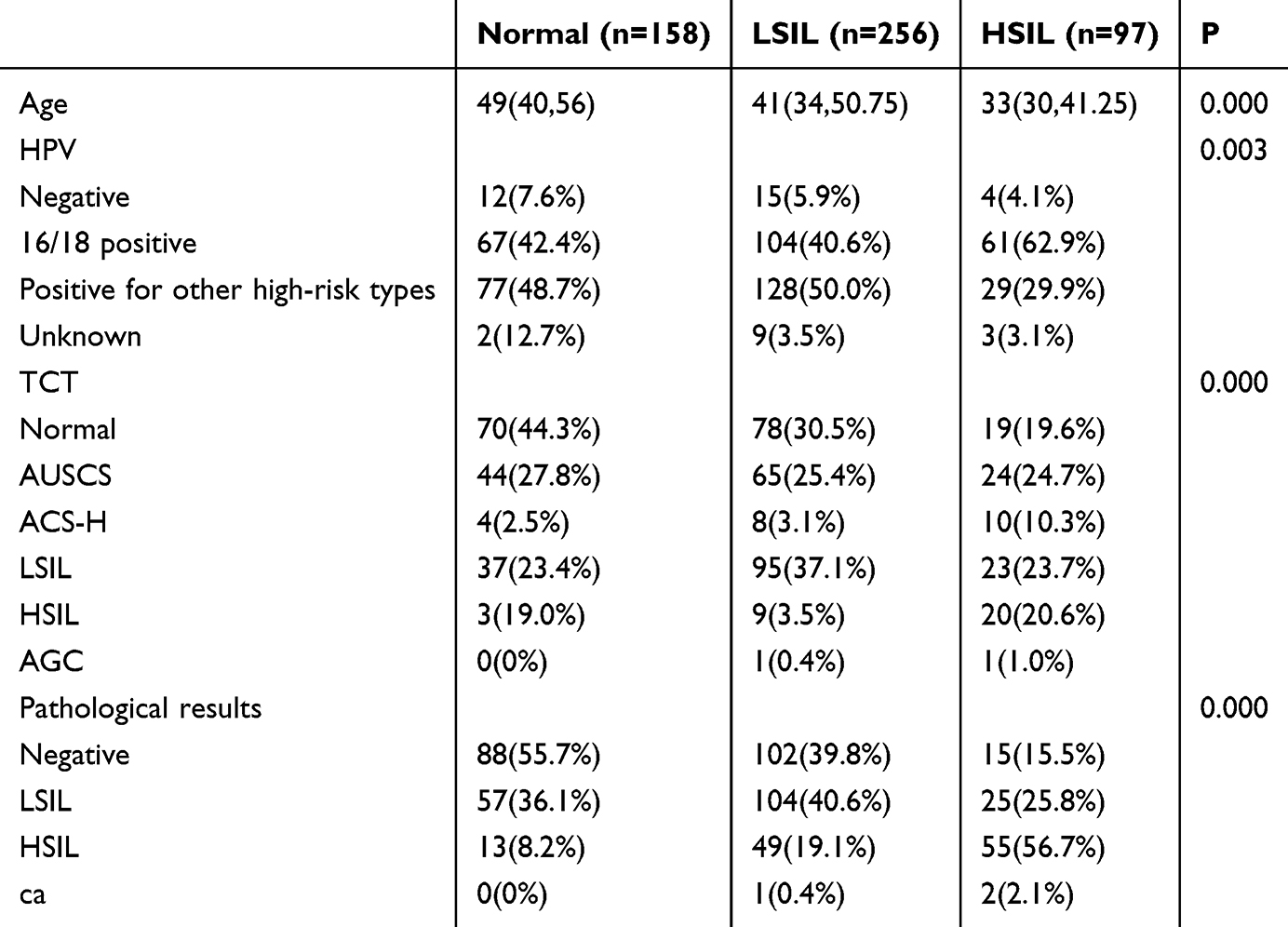 |
Table 1 Basic Information of Patients With Different Degrees of Cervical Lesions Diagnosed by Colposcopy |
Patients diagnosed with cervicitis according to colposcopy were significantly older than those diagnosed with LSIL (P=0.050), and both groups of patients were significantly older than those diagnosed with HSIL (normal: LSIL, P=0.017; LSIL, HSIL, P=0.025). The different subtypes of HPV infection in the normal group and LSIL group had no significant effect on vaginal colposcopy recognition (P=0.779), whereas the proportion of HPV16/18 in the HSIL group was significantly higher than that in the cervicitis and LSIL groups (P=0.003 and P=0.001, respectively).
In the TCT results, there were significant differences among the 3 groups (ie, normal, LSIL, and HSIL: normal versus [vs] LSIL [P=0.016];;normal vs HSIL [P=0.000]; LSIL vs HSIL [P=0.000]). There was consistency between TCT results and vaginal colposcopy diagnosis. The consistency between vaginal colposcopy diagnosis and postoperative cervical tissue biopsy was the lowest in the LSIL group, while that in the other two groups was > 55%.
The cervical inflammation, LSIL, and HSIL groups were analyzed based on pathological results after cervical biopsy as diagnostic criteria. Among the patients diagnosed as normal according to colposcopy, 70 had cervical tissue pathology indicating LSIL or higher (44.3%) (Table 2). For patients with normal pathological indications, the positive predictive value of colposcopy examination was 55.41% (95% confidence interval:47.55%–63.27%) and the negative predictive value was 67.50% (95% confidence interval:62.64%–72.36%). The analysis results indicated that age had no significant impact on the accuracy of vaginal colposcopy diagnosis in the normal group. HPV infection status had no significant impact on the accuracy of vaginal colposcopy diagnosis (Table 3). When the TCT results of patients indicated LSIL or above, the possibility of pathological upgrading significantly increased (P=0.024); however, the analysis of all TCT result types did not reveal significant differences among the 3 groups.
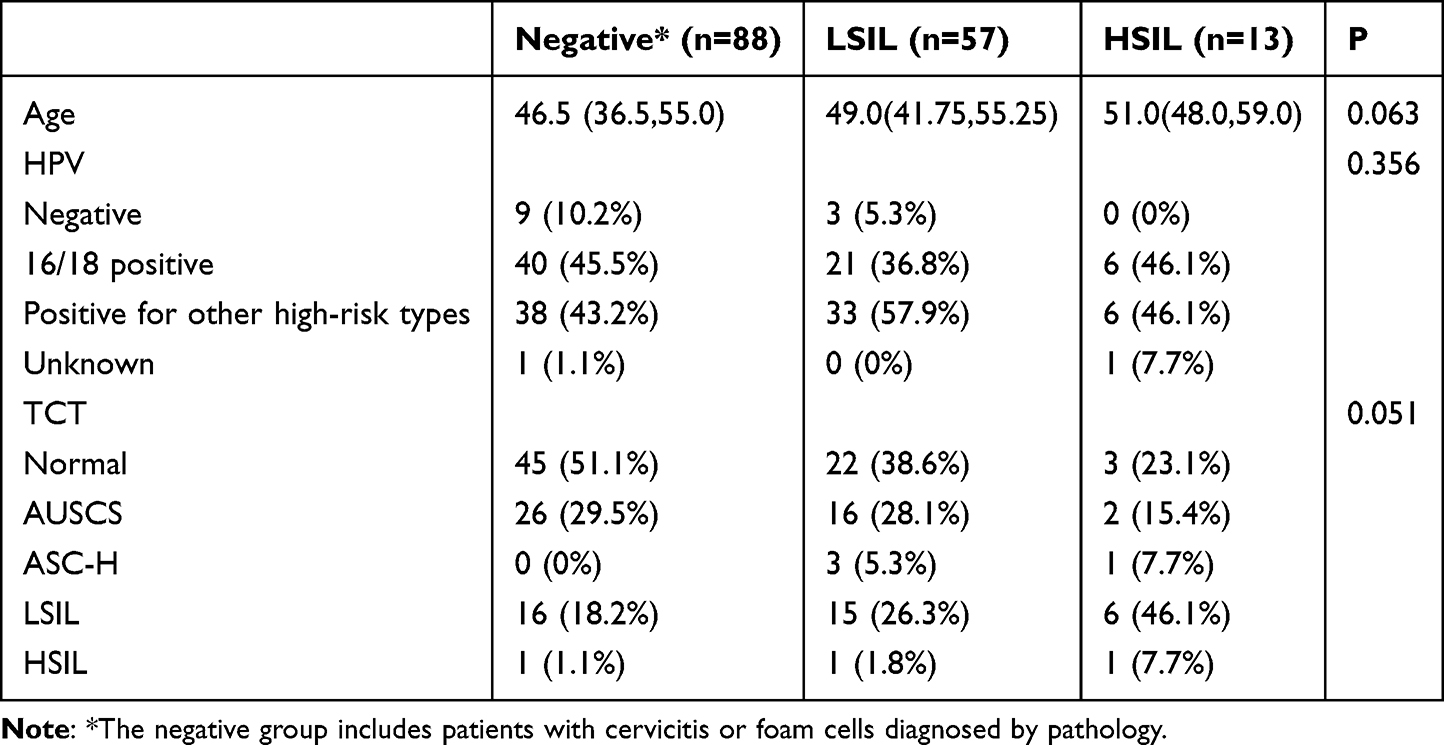 |
Table 2 General Information of Cervical Inflammation Group Patients Grouped According to Pathological Results of Cervical Biopsy Tissue |
 |
Table 3 P-values of HPV Infection in Different Pathological Groups of Normal Group |
Among patients diagnosed with LSIL using colposcopy, 105 had cervical tissue pathology confirmed as LSIL (41.0%) (Table 4). For patients with pathological indications of LSIL, the positive predictive value of colposcopy examination was 41.02% (95% confidence interval:34.95%–47.08%), and the negative predictive value was 68.44% (95% confidence interval:62.79%–74.09%). Results suggested that age was related to the degree of cervical lesions, and there were no significant differences in HPV types among the negative, LSIL, and HSIL groups. Similar to the normal group, HPV infection did not significantly affect the accuracy of vaginal colposcopy examination (Table 5). There was a significant difference in preoperative TCT results between patients with negative postoperative pathology and those with LSIL and HSIL (P=0.023), indicating that preoperative TCT examination of LSIL or higher suggests an increased possibility of upgrading vaginal colposcopy diagnosis results.
 |
Table 4 General Information of LSIL Group Patients Grouped According to the Pathological Results of Cervical Biopsy Tissue |
 |
Table 5 P-values of HPV Infection in Different Pathological Groups of LSIL Group |
Fifty-four individuals in the HSIL group were diagnosed with cervical tissue pathology of HSIL (56.8%) (Table 6), and there was no significant age difference among the 3 groups. For patients with pathological signs of HSIL, the positive predictive value of colposcopy examination was 55.67% (95% confidence interval:45.61%–65.73%), and the negative predictive value was 85.2% (81.92%–88.70%).
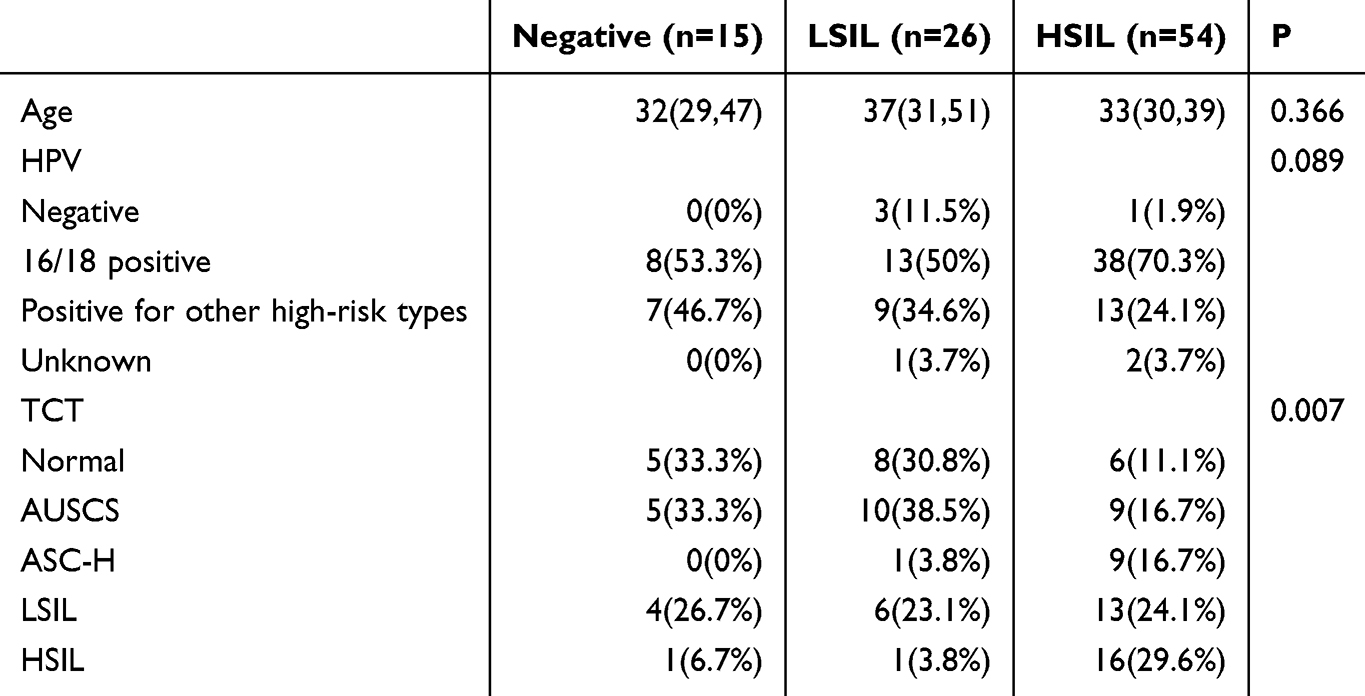 |
Table 6 General Information of Patients in the HSIL Group Grouped According to the Pathological Results of Cervical Biopsy Tissue |
Compared with the HSIL group, patients with a mild pathological degree diagnosed by colposcopy exhibited no significant changes in HPV typing (P=0.114). Pathological confirmation revealed that patients with HSIL had more severe TCT results (P=0.000) than those with pathological results, indicating a decrease in lesion severity and a certain degree of consistency between TCT and pathological biopsy results for vaginal colposcopy diagnosis of patients with HSIL.
Discussion
Screening methods for cervical cancer include HPV and cervical TCT, and the results of HPV and TCT are important factors in determining whether to perform vaginal colposcopy.8 If necessary, vaginal colposcopy and cervical tissue biopsy are necessary to detect precancerous lesions of the cervix early and ensure timely intervention and ensuing treatment.9 Physicians can make a visual diagnosis during vaginal colposcopy and acetic acid administration. Cervical tissue sampling should be performed if the physician deems it necessary to confirm the diagnosis via pathology. However, visual diagnosis relies on the sensitivity, specificity, and experience of the physician.10
Colposcopy is a highly subjective examination method, and different physicians may obtain different results when performing colposcopy on the same patient, mainly depending on their experience.11 In many countries and, especially, in primary hospitals, colposcopy physicians have poor abilities to identify, diagnose, and biopsy transitional bands.12,13
Improving the accuracy of visual diagnosis with colposcopy is beneficial for reducing the selection of subsequent cervical biopsy locations and providing timely disease information to physicians and patients.14 A Swedish study15 suggested that colposcopy has a weak ability to distinguish between normal and atypical lesions, and that simply increasing the number of times physicians perform colposcopy does not necessarily improve accuracy. Advances in technology have improved the accuracy of colposcopy, and Booth et al16 found that dynamic spectral imaging can help locate biopsy sites. Ferris et al17 suggested no significant difference in the area under the receiver operating characteristic curve (AUC) between polarized and unpolarized colposcopy. Patel et al18 used fluorescein sodium under a blue filter to assist in the observation of cervical lesions, which can effectively improve diagnostic accuracy. Tsampazis et al19 demonstrated that electrical impedance spectroscopy was effective in diagnosing CIN2+ and significantly increased the number of CIN2+ cases missed by vaginal colposcopy alone, especially in women referred for LSIL cytological examination. Artificial intelligence-based vaginal colposcopy image recognition systems are gradually being developed, with their sensitivity increasing from 70% in 2015 to > 90% currently.20
Reid and Scalzi proposed the Reid Colposcopic Index (RCI) in 1985 to ensure standardization and accuracy of colposcopy.21 New scoring systems for vaginal colposcopy results have been proposed, including the modified RCI22 and Swede Score.23 However, these scores have not been well correlated with pathology in some studies.24,25 Strander et al23 proposed the Swede score in 2005, which included acetouptake, margins and surface, vessels, locomotion size, and iodine staining. In a subsequent study by Alfonzo et al,26 this scoring criterion was able to distinguish patients with CIN2+ in clinical settings, with an AUC of 0.88 when combined with cytology and HPV diagnosis. In a study by Kushwah et al,27 Reid scores of 3–4 were mainly associated with CIN1-2; however, the management of these 2 grades was significantly different. Sweden scores ≥ 5 exhibited a sensitivity of 100% and specificity of 91.3% in distinguishing CIN2+ lesions. However, there is currently no consensus regarding the diagnosis of vaginal colposcopy.28 The International Federation of Cervical Pathology and Colposcopy (IFCPC), which is currently the authoritative international organization for cervical pathology and colposcopy, proposed 4 versions of vaginal terminology in 1975, 1990, 2002, and 2011, with the aim of promoting the harmonization of colposcopy terminology and practice. The American Society for Colposcopy and Cervical Pathology (ASCCP) proposed colposcopy standards in 2017 based on colposcopy practices in the United States; this terminology and evaluation method is commonly used in China for vaginal colposcopy image assessment.
A similar relationship was observed between age and the presence of cervical lesions is very close. A study from Brazil reported that women 25–29 years of age had the highest vaginal colposcopy referral rates after undergoing HPV testing and TCT. In terms of the diagnosis rate of cervical precancerous lesions, the odds ratio for CINII-III lesions diagnosed by HPV in the 25–29 years’ age group was 2.1–3.0 compared with the 30–64 years’ age group.29 In a big data study, among women 24–29 years of age who underwent HR-HPV testing, 26.9% tested positive, and 10.4% were directly transferred for colposcopy after cytological triage, with CIN2+ accounting for 47%. Among the population 50–64 years of age, these proportions were 5.3%, 1.2%, and 27%, respectively.30 Similar to previous studies, in our study, age was closely related to the severity of disease(s) diagnosed using colposcopy. Studies have suggested that females with CIN III < 50 years of age have a sensitivity of 85.9% in vaginal colposcopy, while women > 50 years of age have a slightly lower sensitivity (78%).31 Some researchers have suggested that this phenomenon is associated with age-related squamous epithelial regression.32 This study investigated the influence of age on the accuracy of vaginal colposcopy. In the normal and HSIL groups, our results indicated that age was not related to the results of colposcopy diagnosis. Younger patients have a higher probability of a pathological diagnosis corrected to HSIL only when they are diagnosed with LSIL using colposcopy. Based solely on the results of the vaginal colposcopy examination, young patients may have been missed or misdiagnosed.
In a previous prospective study, Petousis et al33 suggested that the positive predictive value of colposcopy was high, but the negative predictive value was low. Our results indicated that the negative predictive value was also low for patients with LSIL or cervicitis, suggesting that colposcopy cannot effectively distinguish between LSIL and cervicitis. However, the negative predictive value of the HSIL group was high, similar to that reported in previous studies, and colposcopy may be an effective diagnostic method for patients with HSIL.
The combination of HPV and TCT is considered to be a method for distinguishing between HSIL and non-HSIL.34 However, the diagnostic performance of colposcopy may be affected by the method and results selected during the initial screening. Compared with cytological abnormalities, cervical lesions with only HPV infection may be more difficult to identify because they are milder.12 A study by Liu et al35 found that vaginal colposcopy was more accurate in patients who were positive for HPV16/18 or had a high viral load. In the present study, we focused on patients classified as having other degrees of cervical lesions according to vaginal colposcopy. The results revealed no significant difference in HPV test results between the groups, indicating that it was not possible to correct the vaginal colposcopy results based on HPV results. However, the proportion of TCT results greater than or equal to LSIL was significantly different among the groups, suggesting that TCT results greater than or equal to LSIL can be used as a reference for upgrading vaginal colposcopy image diagnosis.
New detection indicators have also been used to triage patients with cervical intraepithelial neoplasia. Clarke et al36 used p16/Ki67 double staining to triage patients with HPVs other than those positive for HPV16/18. Stoler et al37 found that extended HPV genotyping (ie, “xGT”) is similar in efficacy to HPV combined screening and p16/Ki67 double staining for the detection of high-grade CIN. The detection of the HvvE7 protein and AX1/ZNF582 methylation is also considered to be a new diversion method applied in clinical studies.38
The present study aimed to provide information beyond imaging data for vaginal colposcopy diagnosis. One limitation of this study was the small number of participants and the large number of HPV subtypes; as such, quantitative analysis of TCT and HPV data was not performed, and inclusion factors were also limited. Due to the retrospective design of this study, the results of some patient examinations were unknown, which may have led to biased results. More targeted research is required to systematically develop relevant standards for upgrading or downgrading colposcopy.
Abbreviations
ASC-H, Atypical squamous cells: cannot exclude high-grade squamous intraepithelial lesion; ASC-US, Atypical Squamous Cells of Undetermined Significance; HR HPV, High-risk human papilloma virus; HPV, human papilloma virus; TCT, Thin prep cytologic test; LSIL, Low-grade Squamous Intraepithelial Lesion; HSIL, High-grade Squamous Intraepithelial Lesion.
Ethical Approval
The study was carried out in accordance with the ethical standards laid down in the Declaration of Helsinki, and was approved by the ethics committees of Beijing Obstetrics and Gynecology Hospital, Capital Medical University(No:2023-KY-021-01).As the experiment was a retrospective study and did not have any impact on patient treatment or prognosis, the ethics committee agreed to exempt informed consent from the patients. Patient data will be safeguarded and kept strictly confidential.
Acknowledgments
No contributors not mentioned in the text.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
Disclosure
All authors have no conflicts of interests to declare.
References
1. Jha AK, Mithun S, Sherkhane UB. et al. Systematic review and meta-analysis of prediction models used in cervical cancer. Artif Intell Med. 2023;139:102549. doi:10.1016/j.artmed.2023.102549
2. Perkins RB, Wentzensen N, Guido RS, Schiffman M. Cervical cancer screening: a review. JAMA. 2023;330(6):547–558. doi:10.1001/jama.2023.13174
3. Pariyar J. Update management of cervical precancer lesion. J Obstet Gynaecol Res. 2023;49(Suppl 1):191–202. doi:10.1111/jog.15604
4. Hayumbu V, Hangoma J, Hamooya BM, Malumani M, Masenga SK. Cervical cancer and precancerous cervical lesions detected using visual inspection with acetic acid at Livingstone Teaching Hospital. Pan Afr Med J. 2021;40:235. doi:10.11604/pamj.2021.40.235.32300
5. Ardahan M, Temel AB. Visual inspection with acetic acid in cervical cancer screening. Cancer Nurs. 2011;34(2):158–163. doi:10.1097/NCC.0b013e3181efe69f
6. Qin D, Bai A, Xue P, et al. Colposcopic accuracy in diagnosing squamous intraepithelial lesions: a systematic review and meta-analysis of the International federation of cervical pathology and colposcopy 2011 terminology. BMC Cancer. 2023;23(1):187. PMID: 36823557; PMCID: PMC9951444.doi:10.1186/s12885-023-10648-1
7. Wentzensen N, Massad LS, Mayeaux EJ Jr, et al. Evidence-based consensus recommendations for colposcopy practice for cervical cancer prevention in the United States. J Low Genit Tract Dis. 2017;21(4):216–222. PMID: 28953109.doi:10.1097/LGT.0000000000000322
8. McGee AE, Alibegashvili T, Elfgren K, et al. European federation for colposcopy and pathology of the lower genital Tract (EFC) and the European Society of Gynaecological Oncology (ESGO). European consensus statement on expert colposcopy. Eur J Obstet Gynecol Reprod Biol. 2023;290:27–37. PMID: 37716200.doi:10.1016/j.ejogrb.2023.08.369
9. Dai W, Wang T, Chen L, Qiu Z, Chen P, Chen D. Immediate risk of cervical intraepithelial neoplasia and diagnostic value of colposcopy among cytology-negative women with oncogenic HPV: a retrospective study. BMC Women's Health. 2024;24(1):419. doi:10.1186/s12905-024-03258-x
10. Panagakis GP, Machairiotis N, Tsiriva M, et al. A narrative review on the clinical utility of electrical impedance spectroscopy for diagnosing high-grade cervical intraepithelial neoplasia. Cureus. 2024;16(6):e61784. doi:10.7759/cureus.61784
11. Dorji N, Tshering S, Choden S, et al. Evaluation of the diagnostic performance of colposcopy in the diagnosis of histologic cervical intraepithelial neoplasia 2+(CIN2+. BMC Cancer. 2022;22(1):930. doi:10.1186/s12885-022-10030-7
12. Xue P, Ng MTA, Qiao Y. The challenges of colposcopy for cervical cancer screening in LMICs and solutions by artificial intelligence. BMC Med. 2020;18(1):169. PMID: 32493320; PMCID: PMC7271416.doi:10.1186/s12916-020-01613-x
13. Cui X, Wang H, Chen M, et al. Assessing colposcopy competencies in medically underserved communities: a multi-center study in China. BMC Cancer. 2024;24(1):349. PMID: 38504211; PMCID: PMC10949713.doi:10.1186/s12885-024-12106-y
14. Benites-Zapata VA, Hernandez-Bustamante EA, Acuña-Chávez LM, et al. Colposcopy in the Primary Health Care: a Scoping Review. J Prim Care Community Health. 2023;14:21501319231198942. PMID: 37740513; PMCID: PMC10517605.doi:10.1177/21501319231198942
15. Alfonzo E, Zhang C, Daneshpip F, Strander B. Accuracy of colposcopy in the Swedish screening program. Acta Obstet Gynecol Scand. 2023;102(5):549–555. PMID: 36879505; PMCID: PMC10072243.doi:10.1111/aogs.14538
16. Booth BB, Petersen LK, Blaakaer J, et al. Dynamic spectral imaging colposcopy versus regular colposcopy in women referred with high-grade cytology: a nonrandomized prospective study. J Low Genit Tract Dis. 2021;25(2):113–118. PMID: 33470739; PMCID: PMC7984761.doi:10.1097/LGT.0000000000000586
17. Ferris DG, Condorhuaman WS, Waller JL, Allmond L, Goebel A. Polarized light colposcopy compared with standard colposcopy. J Low Genit Tract Dis. 2015;19(3):234–238. PMID: 25943867; PMCID: PMC4482770.doi:10.1097/LGT.0000000000000111
18. Patel A, Suneja A, Malik R, Gupta B, Sharma S. Chromocolposcopy with fluorescein sodium for detection of premalignant and malignant lesions of the cervix: a cross-sectional study. Int J Gynaecol Obstet. 2024;165(1):169–175. PMID: 38071725.doi:10.1002/ijgo.15283
19. Tsampazis N, Vavoulidis E, Siarkou CM, et al. Diagnostic comparison of electrical impedance spectroscopy with colposcopy and HPV mRNA-testing in the prediction of CIN2+ women in Greece. J Obstet Gynaecol Res. 2023;49(4):1222–1229. PMID: 36658620.doi:10.1111/jog.15557
20. Vargas-Cardona HD, Rodriguez-Lopez M, Arrivillaga M, et al. Artificial intelligence for cervical cancer screening: scoping review, 2009-2022. Int J Gynaecol Obstet. 2024;165(2):566–578. PMID: 37811597.doi:10.1002/ijgo.15179
21. Reid R, Scalzi P. Genital warts and cervical cancer. VI. An improved colposcopic index for differentiating benign papillomaviral infections from high grade cervical intra epithelial neoplasia. Am J Obstet Gynecol. 1985;153(6):611–618. doi:10.1016/s0002-9378(85)80244-1
22. Ferris DG, Litaker MS. Prediction of cervical histologic results using an abbreviated Reid Colposcopic Index during ALTS. Am J Clin Exp Obstet Gynecol. 2006;194(3):704–710. doi:10.1016/j.ajog.2005.10.204
23. Strander B, Ellström-Andersson A, Franzén S, Milsom I, Rådberg T. The performance of a new scoring system for colposcopy in detecting high-grade dysplasia in the uterine cervix. Acta Obstetricia et Gynecologica Scandinavica. 2005;84(10):1013–1017. doi:10.1111/j.0001-6349.2005.00895.x
24. Apgar BS, Kaufman AJ, Bettcher C, Parker-Featherstone E. Gynecologic procedures: colposcopy, treatments for cervical intraepithelial neoplasia and endometrial assessment. Am Family Phys. 2013;87(12):836–843.
25. Massad LS, Jeronimo J, Katki HA, et al. The accuracy of colposcopic grading for detection of high-grade cervical intraepithelial neoplasia. J Lower Genital Tract Dis. 2009;13(3):137–144. doi:10.1097/LGT.0b013e31819308d4
26. Alfonzo E, Holmberg E, Milsom I, Strander B. Colposcopic assessment by Swedescore, evaluation of effectiveness in the Swedish screening programme: a cross-sectional study. BJOG. 2022;129(8):1261–1267. PMID: 34894043.doi:10.1111/1471-0528.17054
27. Kushwah S, Kushwah B. Correlation of two colposcopic indices for predicting premalignant lesions of cervix. J Midlife Health. 2017;8(3):118–123. PMID: 28983158; PMCID: PMC5625575.doi:10.4103/jmh.JMH_22_17
28. Zhang B, Hong S, Zhang G, Rong F. Clinical application of the 2011 IFCPC colposcope terminology. BMC Women's Health. 2021;21(1):257. PMID: 34167543; PMCID: PMC8223298.doi:10.1186/s12905-021-01395-1
29. Teixeira JC, Vale DB, Discacciati MG, Campos CS, Bragança JF, Zeferino LC. Cervical cancer screening with DNA-HPV testing and precancerous lesions detection: a Brazilian population-based demonstration study. Rev Bras Ginecol Obstet. 2023;45(1):21–30. doi:10.1055/s-0043-1763493
30. Rebolj M, Mathews CS, Pesola F, et al. Age-specific outcomes from the first round of HPV screening in unvaccinated women: observational study from the English cervical screening pilot. BJOG. 2022;129(8):1278–1288. doi:10.1111/1471-0528.17058
31. Baena A, Mesher D, Salgado Y, et al. ESTAMPA study group. Performance of visual inspection of the cervix with acetic acid (VIA) for triage of HPV screen-positive women: results from the ESTAMPA study. Int, J, Cancer. 2023;152(8):1581–1592. doi:10.1002/ijc.34384
32. Wang S, Dang L, Liu S, et al. Cervical cancer screening via visual inspection with acetic acid and lugol iodine for triage of HPV-positive women. JAMA Network Open. 2024;7(3):e244090. doi:10.1001/jamanetworkopen.2024.4090
33. Petousis S, Christidis P, Margioula-Siarkou C, Sparangis N, Athanasiadis A, Kalogiannidis I. Discrepancy between colposcopy, punch biopsy and final histology of cone specimen: a prospective study. Arch Gynecol Obstet. 2018;297(5):1271–1275. doi:10.1007/s00404-018-4714-8
34. Akhter S, Bari A, Hayat Z. Variability study between pap smear, colposcopy and cervical histopathology findings. J Pak Med Assoc. 2015;65(12):1295–1299.
35. Liu Y, Liao J, Yi X, et al. Diagnostic value of colposcopy in patients with cytology-negative and HR-HPV-positive cervical lesions. Arch Gynecol Obstet. 2022;306(4):1161–1169. PMID: 35320389.doi:10.1007/s00404-022-06415-5
36. Clarke MA, Wentzensen N, Perkins RB, et al. Enduring consensus cervical cancer screening and management guidelines committee. recommendations for use of p16/Ki67 dual stain for management of individuals testing positive for human papillomavirus. J Low Genit Tract Dis. 2024;28(2):124–130. PMID: 38446575; PMCID: PMC11331430.doi:10.1097/LGT.0000000000000802
37. Stoler MH, Parvu V, Yanson K, Andrews J, Vaughan L. Risk stratification of HPV-positive results using extended genotyping and cytology: data from the baseline phase of the Onclarity trial. Gynecol Oncol. 2023;174:68–75. doi:10.1016/j.ygyno.2023.04.022
38. Agorastos T, Chatzistamatiou K, Moysiadis T, et al. Human papillomavirus E7 protein detection as a method of triage to colposcopy of HPV positive women, in comparison to genotyping and cytology. Final results of the PIPAVIR study. Int, J, Cancer. 2017;141(3):519–530. doi:10.1002/ijc.30761.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.