Back to Journals » Orthopedic Research and Reviews » Volume 14
Distal and/or Proximal Joint Stiffness Among Post-Fracture Patients Treated in University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia
Authors Gashaw M ![]() , Aragaw FM
, Aragaw FM ![]() , Zemed A
, Zemed A ![]() , Endalew M, Tsega NT
, Endalew M, Tsega NT ![]() , Asratie MH
, Asratie MH ![]() , Belay DG
, Belay DG ![]()
Received 4 March 2022
Accepted for publication 26 April 2022
Published 12 May 2022 Volume 2022:14 Pages 157—167
DOI https://doi.org/10.2147/ORR.S365011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Moges Gashaw,1 Fantu Mamo Aragaw,2 Ashenafi Zemed,1 Mastewal Endalew,3 Nuhamin Tesfa Tsega,4 Melaku Hunie Asratie,4 Daniel Gashaneh Belay2,5
1Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia; 2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Women’s and Family Health, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 5Department of Human Anatomy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Moges Gashaw, Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar Comprehensive Specialized Hospital, PO Box 196, Gondar, Ethiopia, Email [email protected]
Background: Stiffness, or more precisely, a restriction in the range of motion, is a potential complication following any intra- or extra-articular injury. The passive or active range of motion of the physiological joint is an important factor in determining the significance of joint stiffness. The goals of this study were to assess the incidence of joint stiffness following a fracture, using a standard goniometer, and to identify potential predictors of joint stiffness among post-fracture patients.
Methods: A prospective hospital-based cross-sectional study was conducted from July 1, 2021 to September 13, 2021, at University of Gondar Comprehensive Specialized Hospital. A total of 230 study participants participated in the study, and systematic sampling methods were used to recruit the study participants. Bivariate and multivariable binary logistic regression model analyses were conducted, with SPSS version 23, to identify factors associated with post-fracture joint stiffness.
Results: The overall prevalence of post-fracture stiffness was 25.7% (n=59). Having a left-side fracture (AOR=10.83; 95% CI 1.71– 17.74), patients having no physiotherapy follow-up (AOR=6.72; 95% CI 1.79– 25.13), and patients using assistive devices (AOR=11.95; 95% CI 3.63– 39.35) were significantly associated with post-fracture stiffness, with p-values of less than 0.05.
Conclusion: The study found that one-quarter of the study participants experienced post-fracture joint stiffness. A fracture on the left side, individuals with no physiotherapy follow-up, and the use of assistive devices were found to be independent predictors of joint stiffness. Early referral of fracture patients to the rehabilitation center is recommended to prevent post-fracture complications and joint stiffness.
Keywords: physiotherapy, fracture, joint, stiffness, range of motion
Introduction
Restriction of joint mobility is a common problem that is seen in post-fracture management.1 More than 90% of traumatic morbidity, mortality, and associated disability related to fracture occurs in low and middle-income countries. Road traffic accidents (RTAs), personal conflict, interpersonal violence, and work-related accidents are the most common causes of fractures.2,3 The upper extremity, head and hand, multiple parts, and lower extremity were the most commonly reported types of fractures based on the body parts involved.4
Stiffness after joint fracture and bone fixation is a very big challenge.5,6 Post-fracture stiffness and loss of range of motion (ROM) in the adjacent joint are a common complication of fracture. Stiffness, or more accurately, a limitation in the ROM, is a potential complication after any intra-articular or extra-articular injury.1 Most fractures and dislocations require a period of immobilization for proper healing. The cause of post-fracture stiffness could be contractures, the presence of dense intra-articular adhesions, fibrotic transformation of peri-articular structures, immobilization, pain, muscle guarding, or reduced joint function.7 The inevitable immobilization for several weeks leads to a reduction in the ROM, deterioration of muscle strength, malfunction of fine motor and gross motor skills, and changes in motor and sensory representations in the brain. Joint stiffness affects the essential function of movable joints by limiting movement and mobility, resulting in a negative impact on essential daily activity and a healthy lifestyle.8,9
The burden of stiffness ranges between 3% and 54–60%.10,11 The prevalence of limitations in joint ROM in Morocco was found to be 21.4%.12 The site of injury in which the initial injury occurred, purely intra-articular or extra-articular fracture, or both; the type of fracture, closed or open; the duration of the fracture; the type of fracture management; and accessing early rehabilitation services were independent predictors for the incidence of post-fracture stiffness identified by previous studies.13–15
ROM is the parameter used to define joint stiffness. The measure of the passive or active ROM of the physiological joint is a key component in assessing the importance of joint stiffness. A goniometer quantitatively measures the angular distance of the joint motion, and the loss of ROM in a contracture is usually recorded through comparison with the contralateral joint or normative values.16 The decrease in the ROM of an immobilized joint as a result of fracture before intervention with physiotherapy is a critical issue because of the unavoidable time lag from the immobilization to the rehabilitation phase.17
Even though numerous studies have reported the cause, burden, pattern of fracture, and outcome of treatment, occurrences of post-fracture stiffness are frequently seen in clinical practice set-ups. Despite this, there is a lack of evidence on the assessment and burden of post-fracture joint stiffness. The aims of this study were to assess the incidence of joint stiffness following a fracture, using a standard goniometer, and to identify the possible predictors of joint stiffness among post-fracture patients.
Materials and Methods
Study Design, Period, and Setting
From July 1, 2021 to September 13, 2021, a hospital-based cross-sectional study was carried out at the University of Gondar, a comprehensive specialized hospital in Amhara regional state, Northwest Ethiopia, 742 km from Addis Ababa. The hospital is a tertiary level teaching and comprehensive hospital with over 700 inpatient beds and referral health services for more than 5 million people in Northwest Ethiopia. A large number of people from the surrounding zones and surrounding regions visit the hospital for various medical services.18 The hospital has a rehabilitation center, an operating room, an intensive care unit (ICU), a fistula center, and over 13 different wards and outpatient departments (OPDs).19 This comprehensive hospital has three inpatient wards for traumatic and orthopedic conditions, with 39 beds in the orthopedic ward, 36 beds in the surgical ward, and 13 beds in the trauma units. It has an OPD for evaluation and follow-up after discharge. The orthopedic OPD is open twice a week and an average of 40–60 post-hospitalization trauma patients attend appointments each week.
Study Participants, Inclusion and Exclusion Criteria, and Sample Size
The source population of this study was individuals who had fractures visiting the orthopedics department. The study population was all individuals who had sustained a fracture who visited University of Gondar Referral Hospital Orthopedic and/or Physiotherapy OPD during the study period. All post-fracture individuals with upper and lower limb fracture, aged 18 years old and above, who visited the Orthopedics and Physiotherapy OPD for follow-up, evaluation, and rehabilitation with a post-fracture duration of ≥3 months were included in this study. Individuals who had an open wound on the joint, patients with deep vein thrombosis (DVT), patients with a post-fracture duration of <3 months, patients who were under plaster of Paris during the data collection period, and those managed with external fixation were excluded from the study.
The sample size was calculated using EpiInfo 7. A total of 230 study participants participated in the study, using a single population proportion formula20 based on the assumptions of 95% confidence interval (CI), 50% proportion, 5% precision, 10% non-response, and contingencies. Systematic sampling methods was used to recruit the study participants.
Study Variables
The dependent variable of post-fracture stiffness (ROM limitation) was categorized as (Yes/No), and the ROM was measured using a widely used standard goniometer. ROM is defined as the degree of mobility of the proximal and distal joint of the affected extremity, and interpreted as: 1=full range of movement (categorized as No); 0.75=shows decrease by one-quarter, 0.5=half of normal ROM, and 0.25=only one-quarter is preserved (categorized as Yes).21,22
Independent variables were as follows. Sociodemographic variables: age, sex, marital status, handedness, residence, educational level, occupation, body mass index (BMI), and religion; behavioral characteristics: physical activity, smoking and drinking habits; clinical and medical characteristics: pain, associated comorbidity, type of fracture, cause of fracture, site of fracture, and type of fracture management.
Severity of Pain
The severity of pain was described on a 10 cm visual analogue scale: 0–3 cm, no pain to mild pain; 4–6 cm, moderate pain; 7–10 cm, severe pain.23,24
Data Collection Tools and Procedures
Data were gathered through interviews, patient record reviews, and examinations using a structured questionnaire. Data were collected by BSc physiotherapists working on the orthopedics and trauma units. The principal investigator provided intensive training to the data collectors on how to approach study participants, use the questionnaire, and recap the measurement techniques. The investigators closely monitored the data collection process, ensuring the accuracy, completeness, and consistency of the questionnaires, which were collected on a daily basis. The ROM of the proximal and distal joints, measured using a universal plastic goniometer,25 and the severity of pain, on the VAS, were assessed by BSc physiotherapists. The questionnaire was initially prepared in English by language experts and authors at University of Gondar and checked for the consistency of the questions. The English version of the questionnaire was translated into the local language (Amharic) and then translated back to English by language experts. The original and translated questionnaires were compared and any discrepancies were reviewed and corrections were made accordingly.
Data Processing and Analysis
Data were entered into EpiInfo version 7.1 before being exported to IBM SPSS version 23 statistical software for coding, recoding, storing, and further analysis. Descriptive statistics such as frequencies, percentages, means, and standard deviations were used for all participant characteristics and stiffness-related factors. Binary logistic regression was used to select variables and calculate the crude odds ratio (COR). Multivariable logistic regression included variables with a p-value of less than 0.2. To identify factors that influence post-fracture stiffness, the adjusted odds ratio (AOR) with 95% CIs for variables with a p-value of less than 0.05 was calculated.
Results
Sociodemographic Characteristics of the Study Participants
A total of 230 post-fracture patients participated in the study, with an age range from 18 to 79 years. The mean age of the participants was 35.98 years (±14.1). Nearly three-quarters (74.3%) of the participants were males, half of the participants (49.6%) were urban dwellers, and more than three-quarters (76.5%) of the participants were Orthodox Christians. The sociodemographic details of the participants are provided in Table 1.
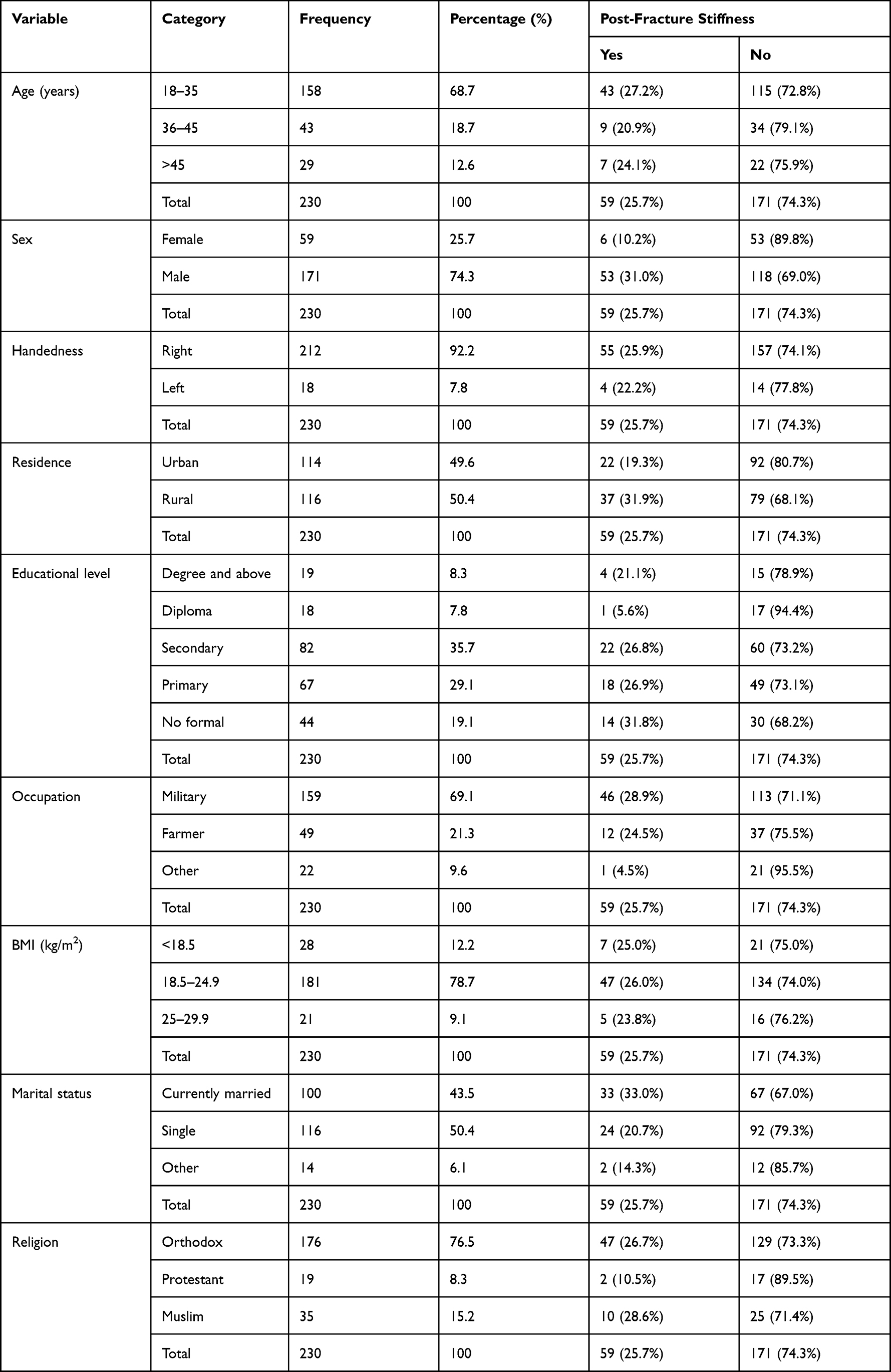 |
Table 1 Sociodemographic Characteristics of Post-Fracture Patients in Gondar, Ethiopia (n=230) |
Behavioral Characteristics of the Study Participants
More than half of post-fracture patients in this study were non-smokers (90%) and non-alcohol users (82.6%), and half of them took regular physical exercise (50.9%). Nearly one in ten fracture patients were active smokers (8.3%). Table 2 shows the behavioral characteristics of the study participants.
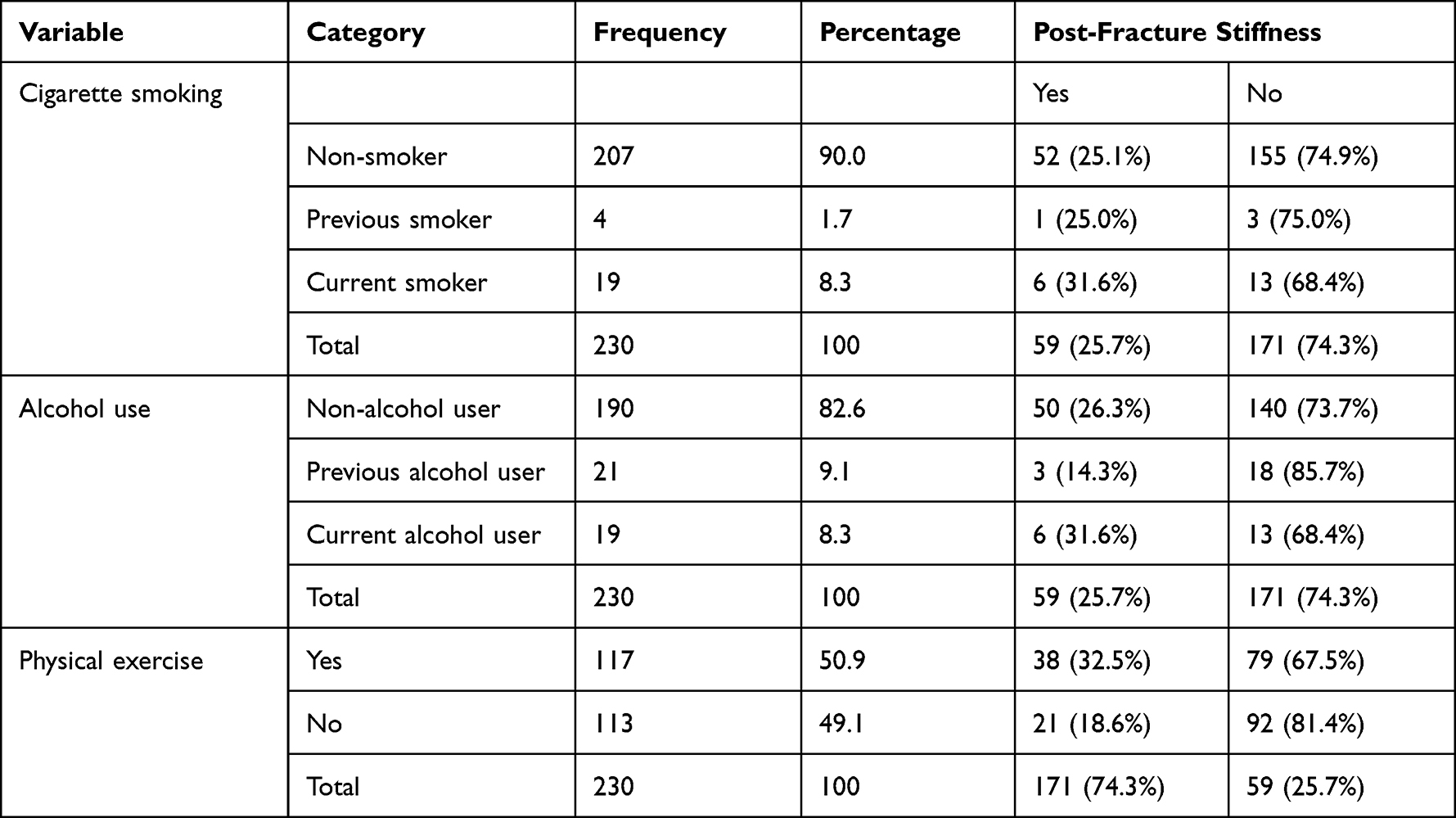 |
Table 2 Behavioral Characteristics of Post-Fracture Patients in Gondar, Ethiopia (n=230) |
Clinical and Medical Comorbidity Characteristics of the Study Participants
The most common cause of fracture was an RTA (62.2%), followed by a gunshot injury (20.0%). More than one-third (39.1%) of the study participants had musculoskeletal disorders and nearly three-quarters (73.9%) of participants had an open fracture. Nearly half of the participants (47%) reported mild pain and less than half of the study participants had a right-sided fracture (Table 3).
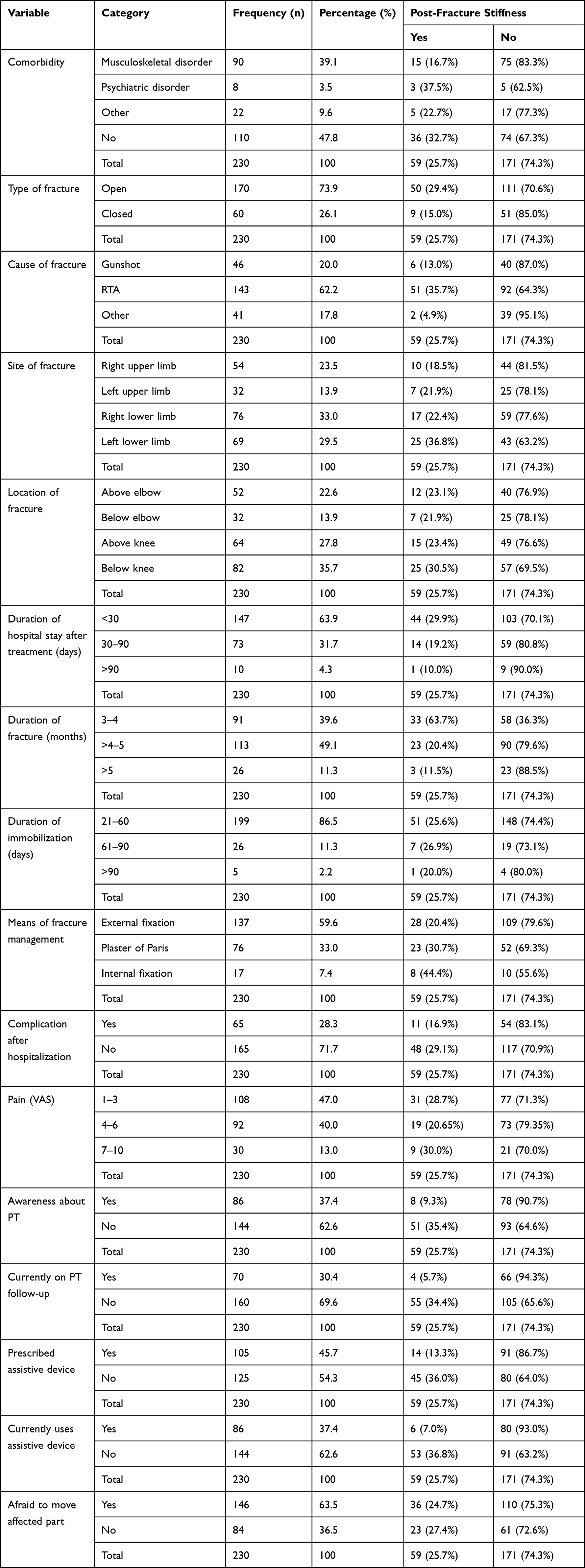 |
Table 3 Clinical and Medical Comorbidity Characteristics of Post-Fracture Patients in Gondar, Ethiopia (n=230) |
Magnitude of Post-Fracture Stiffness
The overall prevalence of post-fracture stiffness was 25.7% (n=59). The burden of post-fracture stiffness was significantly higher (89.8%, n=53) among men with fracture and in rural dwellers (62.7%, n=37). higher incidences of post-fracture stiffness were reported in young adults (n=43; 27.2%) and right dominant-handed individuals (n=55, 25.9%). Further description is provided in Tables 1, 2, and 3.
Regression Analysis
In the univariate regression analyses, post-fracture stiffness was significantly (p<0.20) associated with sex, residence, side of fracture, level of physical activity, good physiotherapy awareness, having physiotherapy follow-up, and using an assistive device. Multivariate regression showed that side of fracture, physiotherapy follow-up, and assistive device use were significantly associated when adjusting for the other included variables (p<0.05). Table 4 shows the associations between dependent and independent variables among the study participants. Having a left-sided fracture showed a statistically significant association with post-fracture stiffness as compared to right-sided fractures (AOR=10.83; 95% CI 1.71–17.74). A patient who had no physiotherapy follow-up was 6.72 times more likely to develop stiffness compared to a patient who had follow-up (AOR=6.72; 95% CI 1.79–25.13). Fracture patients who used an assistive device were 11.95 times more likely to develop stiffness compared to those without assistive devices (AOR=11.95; 95% CI 3.63–39.35).
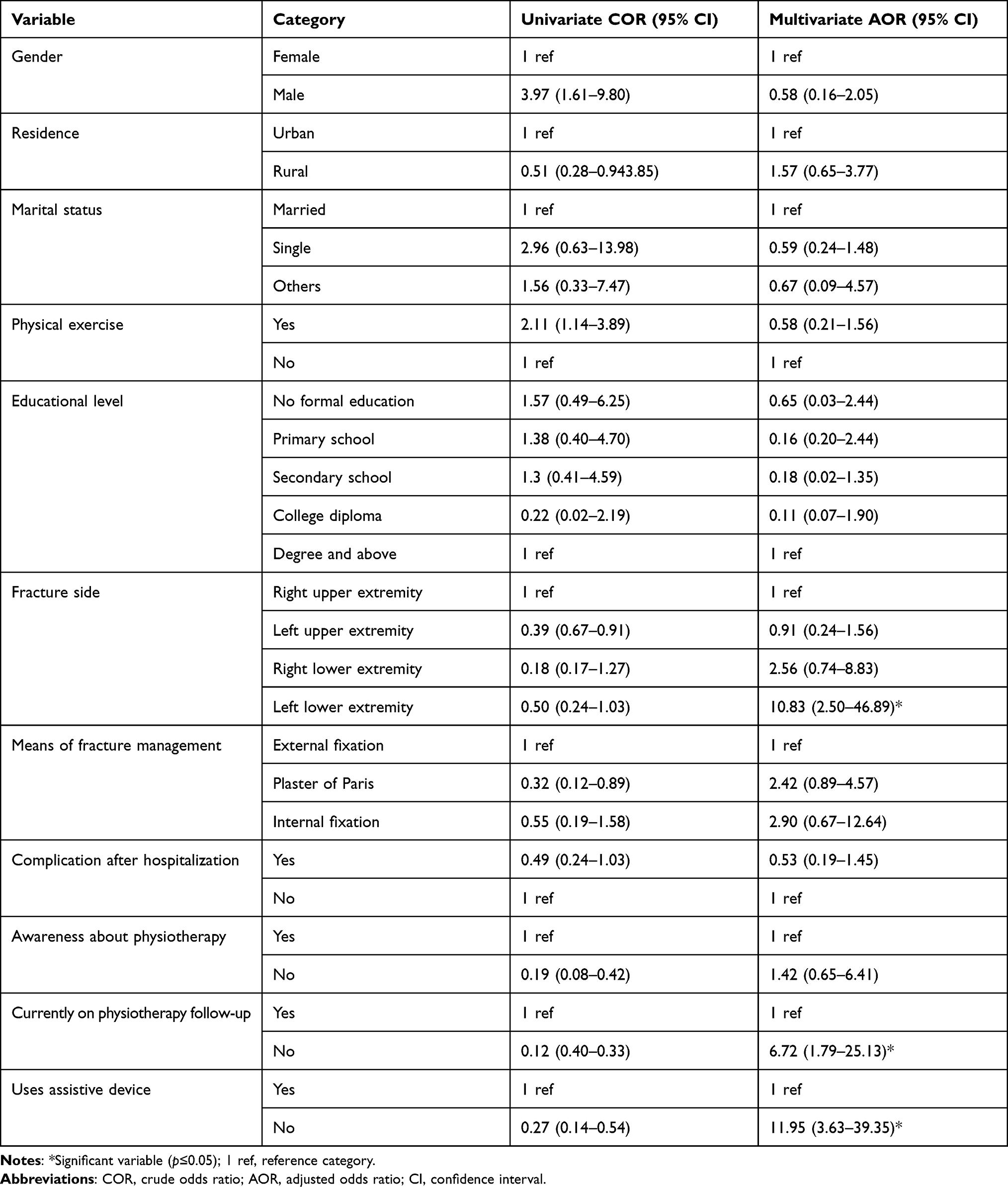 |
Table 4 Factors Associated with Post-Fracture Stiffness Among Post-Fracture Individuals at Gondar University, Ethiopia (n=230) |
Discussion
The main purpose of this study to determine the magnitude of post-fracture joint stiffness among individuals with fractures in Ethiopia, and to describe the associated factors. The findings of this study showed that the overall burden of joint stiffness followed by fracture was 25.7% (n=59); and site of fracture, individuals having physiotherapy follow-up, and the use of assistive devices were found to be independent factors for joint stiffness. In this study, post-fracture stiffness was highly reported by male participants (n=53; 89.8%), right-handed individuals (n=55; 93.2%), and rural dwellers (n=37; 62.7%).
The results showed that one-quarter of individuals with a fracture developed post-fracture stiffness in either the proximal or distal joint adjacent to the fractured bone. The observed frequencies of male and right-handed study participants were higher than those of female and left-handed individuals. The difference between urban and rural dwellers could be explained by urban fracture patients having better awareness and access to healthcare than rural dwellers. Furthermore, patients with open and below-knee fractures had a higher incidence of post-fracture stiffness than those with closed fractures and other fracture sites. This could be due to the fact that the majority of the study participants had open fractures, and patients with open fractures should be considered to have a soft-tissue wound with an underlying bone injury. The prevalence of post-fracture joint stiffness found in the current study is comparable with the findings of a study carried out in Morocco (21.4%)12 and in line with the previous evidence which reported that the burden of joint stiffness ranged between 3.0% and 60%.10,11
Patients with a left-sided fracture were 10.83 times more likely to have joint stiffness than those with a right-sided fracture. This could be related to most of the people using their right side for all activities of daily living. On the other hand, patients who had no physiotherapy follow-up were 6.72 times more likely to develop stiffness than those who had physiotherapy follow-up. This finding is supported by a previous study conducted on physiotherapy assessment and treatment of stiffness, and how it influences management. This is because physiotherapists will start by evaluating the condition carefully, with an examination of the overall health, daily activities, and the nature of the symptoms. Evaluation of the joint itself and the ability to move it will also be a crucial part of the physiotherapy evaluation, as it can reveal exactly what the underlying problem is. This will lead toward the recommendation of specific types of therapy and reduce the development of joint stiffness and prevent the underlying cause of stiffness.26 Those individuals with physiotherapy follow-up are given an appropriate and regular exercise program, which can help reduce stiffness and pain, increase flexibility, improve endurance, develop muscle strength, improve sleep, and keep bone and cartilage healthy.27
Fracture patients who used assistive devices were 11.95 times more likely to develop joint stiffness compared to those not using assistive devices. This may be because the use of assistive devices before and after discharge may increase functional dependence. Conversely, many assistive devices can help patients recover from an injury.
Current evidence on the assessment of outcomes in proximal or distal joint stiffness in intra-articular non-union fractures, treated with open reduction and internal fixation augmented with artificial bone, shows good outcomes in terms of muscle strength, rate of return to work, and function, as assessed by the Mayo Elbow Performance Score and Oxford Elbow Score.28,29 In addition, studies have reported that surgical treatment can restore the structural stability of the joint and soft-tissue structure in an injury with dislocation or subluxation.29–32
Strengths and Limitations of the Study
This is the first study of its kind in the study area, as well as the first in Ethiopia, to assess joint stiffness and fracture with a representative sample size, and perhaps the first to measure the joint range of motion with a standard plastic goniometer. Some significant limitations should be addressed in future research. Comparisons in the Discussion section are problematic owing to a lack of literature in this field and the absence of previously published studies similar to the study findings.
Conclusion
According to the study findings, one-quarter of the study participants experienced post-fracture joint stiffness in the proximal and/or distal joint. Having a left-sided fracture, individuals who did not receive physiotherapy, and the use of assistive devices were discovered to be independent predictors of joint stiffness. It is recommended that fracture patients be referred to a rehabilitation center as soon as possible to avoid post-fracture complications and joint stiffness.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; COR, crude odds ratio; OPD, outpatient department; PT, physiotherapy; ROM, range of motion; RTA, road traffic accident; VAS, visual analogue scale.
Data Sharing Statement and Availability
The manuscript contains all data relevant to our findings. Requests for additional information about the dataset and questions about data sharing should be directed to the corresponding author at: [email protected].
Ethical Approval and Consent to Participate
This research was conducted in accordance with the Declaration of Helsinki. The Ethical Review Committee of the Physiotherapy Department, University of Gondar (ref. no. Physio256/2021) granted ethical approval to carry out this study. All participants were informed about the purpose of the study and each study participant provided written consent.
Acknowledgments
First and foremost, we would like to express our heartfelt gratitude to the University of Gondar, Department of Physiotherapy, for providing ethical approval and material support. Our thanks and appreciation go to the data collectors, supervisors, and study participants, without whom this study would not have been possible.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding from any government, commercial, or non-profit organization.
Disclosure
All authors declare that they have no financial or personal conflicts of interest as a result of this work.
References
1. Müller AM, Sadoghi P, Lucas R, et al. Effectiveness of bracing in the treatment of nonosseous restriction of elbow mobility: a systematic review and meta-analysis of 13 studies. J Shoulder Elbow Surg. 2013;22(8):1146–1152. doi:10.1016/j.jse.2013.04.003
2. Tegegne KT Assessment of the prevalence of trauma cases visited at emergency OPD in Dilla university referral hospital from April 20, 2008–May 20, 2008; 2019.
3. Shavaleh R, Motevalian SA, Mahdavi N, Haddadi M, Mohaghegh MR, Hamedi Z. Epidemiological study of hospitalized road traffic injuries in Iran 2011. Med J Islam Repub Iran. 2018;32(1):50. doi:10.14196/mjiri.32.50
4. Asefa A, Seyoum G, Wamisho B. Common types and pattern of bone fractures among road traffic injury victims seen In Addis Ababa piblic hospitals. Ethiop Med J. 2019;57(2):149–156.
5. Rollo G, Falzarano G, Ronga M, et al. Challenges in the management of floating knee injuries: results of treatment and outcomes of 224 consecutive cases in 10 years. Injury. 2019;50:S30–S8. doi:10.1016/j.injury.2019.03.016
6. Rollo G, Prkić A, Pichierri P, et al. Plate-and-bone-strut fixation of distal third humeral shaft aseptic non-unions: a consecutive case series. J Clin Orthop Trauma. 2019;10:S127–S32. doi:10.1016/j.jcot.2019.05.004
7. Parmar S, Shyam A, Sabnis S, Sancheti P. The effect of isolytic contraction and passive manual stretching on pain and knee range of motion after hip surgery: a prospective, double-blinded, randomized study. Hong Kong Physiother J. 2011;29(1):25–30. doi:10.1016/j.hkpj.2011.02.004
8. Peeters CM, Visser E, Van de Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after hip fracture in the elderly: a systematic literature review. Injury. 2016;47(7):1369–1382. doi:10.1016/j.injury.2016.04.018
9. Yıldırım N, Filiz Ulusoy M, Bodur H. The effect of heat application on pain, stiffness, physical function and quality of life in patients with knee osteoarthritis. J Clin Nurs. 2010;19(7‐8):1113–1120. doi:10.1111/j.1365-2702.2009.03070.x
10. Maloney WJ. The stiff total knee arthroplasty: evaluation and management. J Arthroplasty. 2002;17(4):71–73. doi:10.1054/arth.2002.32450
11. Christensen CP, Crawford JJ, Olin MD, Vail TP. Revision of the stiff total knee arthroplasty. J Arthroplasty. 2002;17(4):409–415. doi:10.1054/arth.2002.32105
12. Hajjioui A, Fourtassi M, Nejjari C. Prevalence of disability and rehabilitation needs amongst adult hospitalized patients in a Moroccan university hospital. J Rehabil Med. 2015;47(7):593–598. doi:10.2340/16501977-1979
13. Pujol N, Boisrenoult P, Beaufils P. Post-traumatic knee stiffness: surgical techniques. Orthop Traumatol Surg Res. 2015;101(1):S179–S86.
14. Yercan HS, Sugun TS, Bussiere C, Selmi TAS, Davies A, Neyret P. Stiffness after total knee arthroplasty: prevalence, management and outcomes. knee. 2006;13(2):111–117. doi:10.1016/j.knee.2005.10.001
15. Hulet C, Djian P. Stiffness of the knee joint–SFA 2002. Revue de chirurgie orthopedique et reparatrice de l’appareil moteur. 2007;93(8Suppl):5S14–5S5.
16. Gerhardt JJ, Rondinelli RD. Goniometric techniques for range-of-motion assessment. Phys Med Rehabil Clin N Am. 2001;12(3):507–528. doi:10.1016/S1047-9651(18)30047-0
17. Lin CWC, Donkers NA, Refshauge KM, Beckenkamp PR, Khera K, Moseley AM. Rehabilitation for ankle fractures in adults. Cochrane Database Syst Rev. 2012;1:11. doi:10.1186/2046-4053-1-11
18. Ayele TA, Zeleke BM, Tessema GA, Melak MF. Magnitude and patterns of injuries among patients in Gondar University Hospital, northwest Ethiopia: an institutional-based study. Open Access Surg. 2017;10:25–31. doi:10.2147/OAS.S126043
19. Mohammed A, Seid ME, Gebrecherkos T, Tiruneh M, Moges F. Bacterial isolates and their antimicrobial susceptibility patterns of wound infections among inpatients and outpatients attending the University of Gondar Referral Hospital, Northwest Ethiopia. Int J Microbiol. 2017;2017:2017.
20. Kasiulevičius V, Šapoka V, Filipavičiūtė R. Sample size calculation in epidemiological studies. Gerontologija. 2006;7(4):225–231.
21. Mangone PG. Posttraumatic knee stiffness: by identifying at-risk patients, can we prevent this in the future?: commentary on an article by Julius Bishop, MD, et al.:“predictive factors for knee stiffness after periarticular fracture. A case-control study”. JBJS. 2012;94(20):e154. doi:10.2106/JBJS.L.00998
22. Keogh JW, Cox A, Anderson S, et al. Reliability and validity of clinically accessible smartphone applications to measure joint range of motion: a systematic review. PLoS One. 2019;14(5):e0215806. doi:10.1371/journal.pone.0215806
23. Aicher B, Peil H, Peil B, Diener H. Pain measurement: Visual Analogue Scale (VAS) and Verbal Rating Scale (VRS) in clinical trials with OTC analgesics in headache. Cephalalgia. 2012;32(3):185–197. doi:10.1177/03331024111430856
24. Kane RL, Bershadsky B, Rockwood T, Saleh K, Islam NC. Visual analog scale pain reporting was standardized. J Clin Epidemiol. 2005;58(6):618–623. doi:10.1016/j.jclinepi.2004.11.017
25. Kim Y-W. Concurrent validity and clinical usefulness of universal plastic goniometer for hip internal and external rotation range measurement. J Korean Soc Phys Med. 2018;13(1):99–105. doi:10.13066/kspm.2018.13.1.99
26. Walton J, Russell S. Physiotherapy assessment of shoulder stiffness and how it influences management. Shoulder Elbow. 2015;7(3):205–213. doi:10.1177/1758573215586152
27. Bhave A, Corcoran J, Cherian JJ, Mont MA. Astym® therapy for the management of recalcitrant knee joint stiffness after total knee arthroplasty. J Long Term Eff Med Implants. 2016;26(2):151–159. doi:10.1615/JLongTermEffMedImplants.2016012530
28. Meccariello L, Prkić A, Campagna V, et al. Two-stage bone-and-strut technique in the treatment of septic non-unions in the upper limb. Med Glas. 2021;18(1). doi:10.17392/1306-21
29. Rollo G, Vicenti G, Rotini R, Prkic A, Eygendaal D, Meccariello L. Open reduction and internal fixation using double plating with biological and artificial bone grafting of aseptic non-unions of the distal humerus: clinical results. In: Strat Trauma Limb Reconstr 2021;16(3):144. doi:10.5005/jp-journals-10080-1533
30. Espinosa N, Maurer M. Peroneal tendon dislocation. Eur J Trauma Emerg Surg. 2015;41(6):631–637. doi:10.1007/s00068-015-0590-0
31. Rollo G, Luceri F, Pasquino A, et al. Bone grafiting combined with Sauvé-Kapandji Procedures for the treatment of aseptic distal radius non-union. In: Congress of the Italian Orthopaedic Research Society 2019 Guest Editors: F. Castoldi, GM Peretti, A. Marmotti, L. Mangiavini; Vol 34, No. 4 Supplement 3; July, 2020:213.
32. Rollo G, Luceri F, Bisaccia M, et al. Allograft versus autograft in forearm aseptic non-union treatment. J Biol Regul Homeost Agents. 2020;34(4Suppl. 3):207–212.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.