Back to Journals » Infection and Drug Resistance » Volume 12
Disseminated Talaromyces marneffei And Mycobacterium avium Infection Accompanied Sweet’s Syndrome In A Patient With Anti-Interferon-γ Autoantibodies: A Case Report
Authors Su SS ![]() , Zhang SN, Ye JR, Xu LN, Lin PC
, Zhang SN, Ye JR, Xu LN, Lin PC ![]() , Xu HY, Wu Q, Li YP
, Xu HY, Wu Q, Li YP
Received 9 June 2019
Accepted for publication 18 September 2019
Published 10 October 2019 Volume 2019:12 Pages 3189—3195
DOI https://doi.org/10.2147/IDR.S218836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Shan-Shan Su,1,* Sheng-Nan Zhang,1,* Jun-Ru Ye,1 Ling-Na Xu,1 Peng-Cheng Lin,1 Han-Yan Xu,1 Qing Wu,2 Yu-Ping Li1
1Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325015, People’s Republic of China; 2The Center of Laboratory and Diagnosis, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325015, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu-Ping Li
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Wenzhou Medical University, South Baixiang, Ouhai District, Wenzhou, Zhejiang Province 325015, People’s Republic of China
Tel/fax +86 577 5557 9273
Email [email protected]
Background: Patients with high-titer anti-IFN-γ autoantibodies present disseminated non-tuberculous mycobacterial (NTM) and other opportunistic infections. Due to its rare occurrence and non-specific symptoms, this syndrome is difficult to diagnose during early disease stages. Here, we report a case with high-concentrations of serum anti-IFN-γ autoantibodies who presented with disseminated Talaromyces marneffei and NTM disease accompanied Sweet’s syndrome.
Case presentation: A 62-year-old Chinese woman with no previous history was admitted to our hospital in August 2016 due to intermittent fever for 2 years, left chest wall redness, and swelling for 3 months. During hospitalization, the patient was confirmed with disseminated T. marneffei and successfully treated with antifungal therapy. In July 2017, upon second admission, Mycobacterium avium intracellular (MAC) pulmonary infection was established after positive cultures from the right lung tissue. The patient failed treatment after 1 month of anti-NTM therapy due to side effects. In May 2018, she was confirmed as having disseminated MAC disease accompanied by hand rashes, which was considered as Sweet’s syndrome. High-level anti-IFN-γ antibodies in the patient serum were detected upon comparison with normal controls (2.85-fold increase). Following anti-NTM therapy, both symptoms and pulmonary infiltration gradually improved, and joint destruction and lymphadenitis remained.
Conclusions: Patients with anti-interferon-γ autoantibodies should be considered for severe, recurrent infections in adults in the absence of other known risk factors. Sweet’s syndrome is a common skin manifestation of the syndrome.
Keywords: Talaromyces marneffei, Mycobacterium avium, Sweet’s syndrome, autoantibodies, interferon-gamma
Introduction
Interferon-gamma (IFN-γ)/IL-12 pathways play a crucial role in the host defense to intracellular pathogens.1 Adult-onset immunodeficiency syndrome is characterized by defects in IFN-γ signaling caused by the generation of anti-IFN-γ autoantibodies (autoAbs) or inherited mutations in IFN-γ-signaling-associated factors. Immunocompromised patients are prone to a variety of bacterial infections, particularly disseminated non-tuberculous mycobacteriosis (NTM).2 High-concentrations of anti-IFN-γ autoAbs interfere with the natural inflammatory response to infection, including STAT1 phosphorylation, TNFα signaling, and IL-12 production.3 Patients with high-titers of IFN-γ autoAbs have mostly been reported in Asians, including Filipino, Thai, Vietnamese, Japanese, and Chinese residents from Hong Kong and Taiwan.4–10 Due to its rare occurrence, non-specific symptoms, and different manifestations, early diagnosis is challenging.
Here, we report a patient from Wenzhou, mainland People’s Republic of China with high-concentrations of serum anti-IFN-γ autoantibodies who presented with disseminated Talaromyces marneffei (T. marneffei) after successfully antifungal treatment. The patient developed disseminated NTM disease accompanied by Sweet’s syndrome. Herein, we describe this case to help identify the syndrome and treatment in early. The study was approved by the Ethics Committee at the First Affiliated Hospital of Wenzhou Medical University, and complied with the Declaration of Helsinki.
Case Presentation
The patient was a 62-year-old Chinese woman with no previous disease history. She was admitted to our hospital in August 2016 due to intermittent fever with cough for 2 years, left chest wall redness, and swelling for 3 months. She presented with a fever and cough repeatedly from September 2014. Laboratory tests showed increased white cells and chest computed tomography (CT) suggested patchy infiltration in the left lower lobe, with mediastinal lymph node enlargement (Figure 1A–D). Empirical treatment with cephalosporin was partially effective, but the symptoms were recurrent. In May 2016, she developed redness and a swelling in the left front chest wall with pain and high fever. She was admitted to our hospital for incision and drainage of the disease site and antibiotic administration. At the time of admission, laboratory tests showed white blood cells counts of 20.61×109/L (3.5–9.5×109/L); neutral cell percentages of 0.744 (0.4–0.75); hemoglobin: 79 g/L (130–175g/L), platelets: 384×109/L (125–350×109/L), blood C-reactive protein (CRP): 43.6 mg/L (0–8 mg/L), high levels of Immunoglobin G (IgG): 50.5 g/L (7.51–15.6 g/L); blood (1, 3)-D glucan (G tests): 146.20 pg/mL (<100.5 pg/mL); and blood galactomannan test (GM) positivity (0.64) (<0.5). HIV serology tests were negative, and normal CD4+ T cell counts and serum globulins levels (including IgA, IgM, and total IgE) were within normal reference ranges. Serum cryptococcal capsular antigen tests and blood tuberculosis infection T cell spot tests (T-SPOT.TB) were negative. Chest CT (2016-8-27) showed alveolar consolidation in the anterior segment of the left upper lobe, and an anterior chest wall with rib destruction and multiple lymphadenopathies in the left axillary and mediastinum (Figure 1E–H). Fungal spores were detected in pus from the left chest wall and microbial cultures showed T. marneffei growth. Disseminated T. marneffei (lung, skin, and bone) were established and the patient was administered amphotericin B followed by itraconazole therapy. After 8 months of regular treatment, her condition improved and antifungal drugs were ceased. The patient was followed up regularly in the clinic (Figure 1I–L).
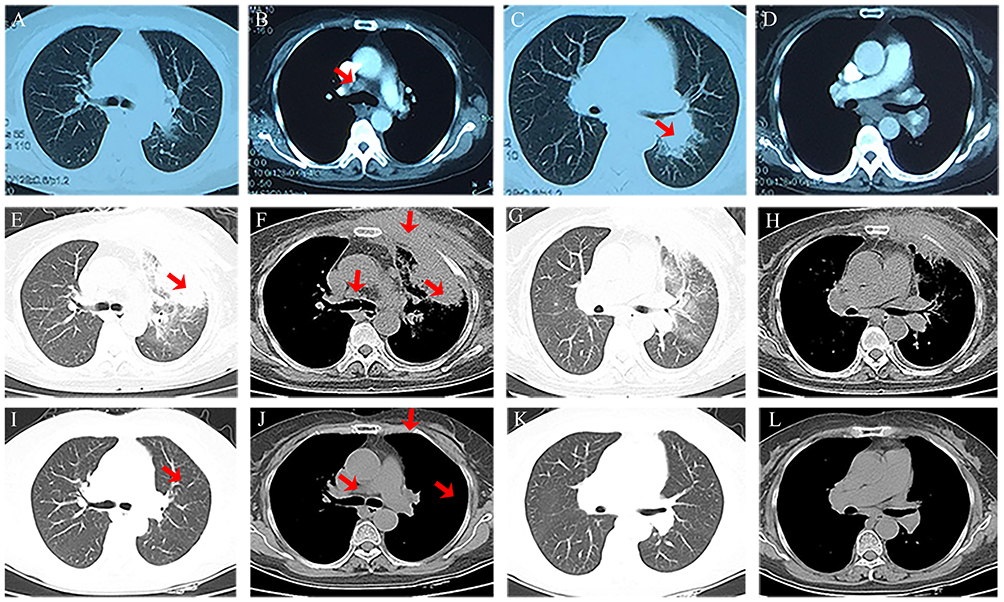 |
Figure 1 (A–D) 2014-9-9 chest CT showed patchy infiltration in the left lower lobe in lung window and lymph nodes enlargement in mediastinal window (arrows); (E–H) 2016-8-27 chest CT showed the alveolar consolidation in left upper lobe (arrows), the anterior chest wall with rib destruction (arrows); (I–L) 2017-5-8 chest CT showed improvement of pulmonary lesion and rib destruction after treatment (arrows). |
In July 2017, she again developed a high fever. Laboratory examinations after hospital admission showed white blood cells counts of 11.66×109/L; neutral cell percentages of 0.647; hemoglobin: 80 g/L; platelets: 308×109/L; blood CRP: 53.9 mg/L; IgG: 30.2 g/L; erythrocyte sedimentation rates of 66 mm/h (0–20 mm/h); and CD4+ T lymphocyte ratios of 32.6% (34–52%). G-tests, GM, and pro-calcitonin were within the normal range. Repeat chest CT scans showed consolidation in the left and right upper lobes. Bronchoscopy examinations were pathogen negative. After 2 weeks of treatment with β-lactam antibiotics combined with oral antifungal drugs, no improvement in symptoms was observed and abnormal lung infiltration was observed in CT scans. CT-guided percutaneous right lung biopsy was performed. Pathological examinations demonstrated lung inflammation in the absence of granuloma formation. Mycobacterium avium (M. avium) was cultured and identified from mass spectrometry. Anti-NTM treatment included azithromycin, ethambutol, moxifloxacin, and rifabutin which were prescribed from August 2017. Due to adverse gastrointestinal and allergic reactions of the skin after 1 month of anti-NTM combination therapy, the patient refused treatment and was followed up in the clinic. No recurrence of the fever was observed.
In May 2018, the fever recurred with hand rashes, and the patient was admitted to the hospital a third time. Her body temperature peaked at 40°C with increased pulmonary infiltration accompanied by left sternoclavicular joint destruction (Figure 2A–C). Physical examinations revealed multiple palpable lymph nodes in the left neck, erythematous plaques, and nodules in both hands (Figure 3A). Blood tests were similar to previous examinations in which increased numbers of white blood cells, CRP, and high levels of serum IgG were observed. Immune electrophoresis revealed polyclonal gammopathy, and blood/bone marrow cultures were negative. After biopsy from the left cervical lymph node and left sternoclavicular joint, M. avium was cultured from both sites. Histopathology demonstrated inflammation from the lymph nodes, and small amounts of elastic fibers with small blood vessels. Histopathology of the hand skin showed neutrophil infiltration (Figure 3B and C). Microorganism cultures were negative. The patient was finally confirmed as disseminated NTM secondary to disseminated T. marneffei. In view of the negative microbial cultures in skin biopsy tissues, and the rapid resolution of hand rashes with steroid ointments, Sweet’s syndrome was diagnosed. Combination anti-NTM therapy was re-prescribed from June 2018. After 1 year of treatment, the patient’s symptoms and pulmonary consolidation improved. Bone destruction and lymphadenopathy, however, remained obvious (Figure 2D–F). Laboratory tests were in the normal range except for IgG (Figure 4). The patient presented multiple intracellular pathogen infections without HIV or immunodeficiency. Serum cytokines including IL-2, IL-4, IL-6, IL-10, TNF-α, and IFN-γ were within the normal range. Serum samples from both patients and controls (blood donors) including anti-IFN-γ autoantibodies, anti-IL-12 autoantibodies, anti-TNF-α, and IL-12 were assessed using ELISA kits (Cloud-Clone Corp). Patient serum was tested as four independent samples and statistical analysis were performed using unpaired t-tests (GraphPad Prism Software). The mean concentration of anti-IFN-γ antibodies in the serum samples of the patient (range: 33.13–47.06 ng/mL) was 2.85-fold higher than healthy subjects (range: 8.41–20.02 ng/mL) (P<0.01) (Figure 5). No statistically significant differences between patients and controls for TNF-α, IL-12, and anti- TNF-α were observed (data not shown).
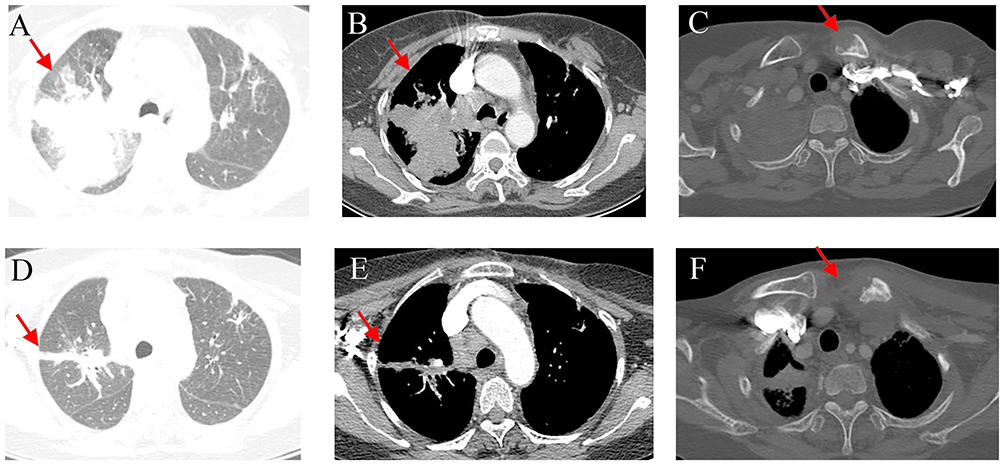 |
Figure 2 (A–C) 2018-5-8 chest CT showed right upper lobe consolidation and destruction of the left sternoclavicular joint (arrows); (D–F) 2019-06-04 chest CT showed gradually absorption of pulmonary consolidation but remains of bone destruction and lymphadenopathy after treatment (arrows). |
 |
Figure 3 (A) The erythematous painful papules in patient’s hands; (B, C) pathological examination of HE staining (HE×100; HE×400) from the hand skin lesion showed dermal florid full-thickness suppurative inflammation. |
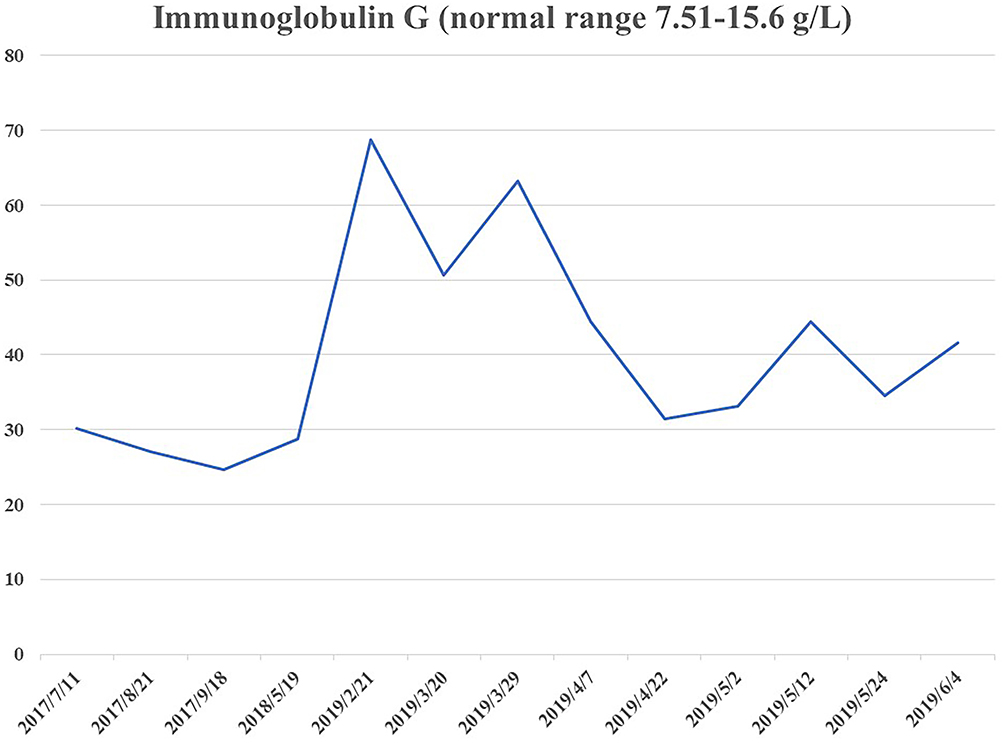 |
Figure 4 After treatment, level of Immunoglobin G remained high (normal range 7.51–15.6 g/L). |
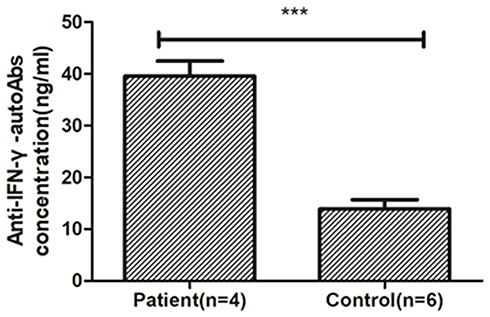 |
Figure 5 Anti-Interferon-γ autoantibodies concentration in serum, the patient (range: 33.13–47.06 ng/mL) was 2.85-fold to healthy subjects (anti-IFN-γ-autoAbs). ***P<0.001. |
Discussion And Conclusions
Immunodeficiency due to anti-IFN-γ autoantibodies was first described in 2004.11,12 Chan et al described the first laboratory confirmed case in an ethnic Chinese patient born in Xiamen in People’s Republic of China who resided in Hong Kong.13 Our case was born and resided in Wenzhou. Immunodeficiency can result from a genetic predisposition or environmental factors. Recent studies showed that the HLA class II alleles DRB and DQB confer a predisposition to anti-IFN-γ autoantibodies that are associated with immunodeficiency.14
Due to the rarity of the disease, the time from initial symptoms to a final diagnosis lasted for 4 years for this case. Broad-spectrum antibiotics were repeatedly prescribed with no improvements observed. The first episode of disseminated T. marneffei infection involving the lungs, lymph nodes, and chest wall was successfully treated with antifungal therapy. We failed to recognize the underlying immunocompromised factors until the patient developed disseminated NTM disease. Sweet’s syndrome was also established. In view of the repeated opportunistic infections with no underlying immunocompromised disease, we tested the patient for IFN-γ autoantibodies, with positive results observed. She was therefore considered as adult-onset immunodeficiency syndrome.
T. marneffei infection is frequently reported in HIV patients in Southern China and South-East Asia, in which opportunistic infections are endemic.15 Diagnosis is often delayed in non-HIV patients and non-endemic regions due to non-specific symptoms and the range of afflicted organs. Jasper et al reviewed the clinical characteristics and underlying immunological basis of T. marneffei infections in non-HIV infected patients.16 The diagnosis was dependent on the histopathological findings combined with fungal growth in the culture specimens. Tang et al described the clinical characteristics of T. marneffei co-infections with disseminated NTM in a case with high-titer anti-IFN-γ autoAbs.4 T. marneffei infection typically presents as a chronic disseminated infection involving pulmonary lymphadenopathy. The occurrence of NTM disease in People’s Republic of China has become more frequent in recent years.17 The clinical disease caused by NTM infections includes lymphadenitis, skin and soft tissue infections, pulmonary disease, and disseminated infections. Disseminated NTM infections are the most significant phenotype associated with anti-IFN-γ autoAbs. It is reported that ~81% of disseminated NTM subjects with normal CD4 lymphocyte counts and no obvious immunodeficiency have positive anti-IFN-γ autoAbs.6 Pulmonary NTM disease is most common, followed by lymph node, bones/joints, and skin involvement.18 The radiological manifestations of NTM pulmonary disease often showed consolidation without cavity and pleural thickening, which is partially resolved with empirical antibiotic treatment. Lung tissue culture showed NTM growth and MAC was one of the most isolated NTM species. Studies have reported that MAC accounts for 97.8% of IFN-γ autoAbs in patients with disseminated NTM infection.19 Skin manifestations have been reported in 49–57% of IFN-γ autoAbs syndromes.20,21 NTM skin manifestations can be divided into skin infections with NTM and reactive dermatitis. Recently, Jutivorakool et al reported that ~80% of adult-onset immunodeficiency cases with anti-IFN-γ autoAbs show skin involvement, ~82% have reactive skin disorders and 45% show skin infections.22 Sweet’s syndrome is most commonly observed in reactive dermatitis and often manifests as erythematous plaques and nodules. Histopathology revealed neutrophilic dermatoses with negative microbial cultures. More importantly, the presence of neutrophilic dermatoses warrants the clinical assessment of systemic opportunistic infections. The manifestation of skin infections with NTM also presents as nodules, subcutaneous abscesses, and ulcers,23 and the diagnosis is dependent on positive NTM growth from the cultures of infected tissues.
The trigger for the production of anti-IFN-γ autoAbs remains unknown. Strong endemic HLA DRB and DQB are known to be associated with the disease. The proteins encoded by these genes are expressed on the surface of antigen-presenting cells (APCs) and recognized by the receptors of Th cells. Interactions between APCs and Th cells may encourage the development of anti-IFN-autoAbs.24 Additionally, environmental stimuli may trigger disease induction, including infections and toxins.6 High-titer anti–IFN-γ autoAbs against IFN-γ are thus the major cause of disseminated NTM infections.6
In this case, multiple laboratory tests revealed elevated levels of IgG, and multiple myeloma and lymphoma were excluded upon thorough examinations. The clinical value of these tests was therefore highlighted. Although functional assessments of IFN-γ autoantibodies were not performed in this study, the repeated infections were suggestive of adult-onset immunodeficiency syndrome.
The rationale treatment of disseminated NTM patients with anti-IFN-γ autoantibodies is important, but the duration is unknown. Relapse can occur during short-term therapy and rituximab, an anti-CD20 monoclonal antibody, was administered in 6% of cases.25 Other methods include a combination of plasmapheresis and pulsed cyclophosphamide or cyclophosphamide in addition to antimicrobial treatment in refractory patients.26,27 The mortality rates were 3.2% in disseminated NTM patients with anti-IFN-γ autoantibodies.28
In summary, patients with high levels of anti-IFN-γ autoantibodies should be considered with severe, recurrent infections in adults in the absence of other known risk factors. Disseminated NTM is the most significant phenotype associated with the disease. Sweet’s syndrome represents a common form of reactive dermatitis that frequently occurs with this syndrome.
Abbreviations
NTM, non-tuberculous mycobacteriosis; IFN-γ, interferon-gamma; CT, computed tomography; CRP, C-reactive protein; Ig G, Immunoglobin G; G test, (1, 3)-D glucan; GM, galactomannan test; T-SPOT.TB, tuberculosis infection T cell spot test; PCT, pro-calcitonin; ESR, erythrocyte sedimentation rate; MAC, Mycobacterium avium intracellular; APCs, antigen-presenting cells.
Availability of Data And Material
All the information supporting our conclusions and relevant references are included in the manuscript. There are no datasets related to this case report.
Consent For Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Acknowledgments
We thank the patients and their families and all staff in the department for their support. This study was supported by the Wenzhou Municipal Science and Technology Bureau (CN) (ZH2017001).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sexton P, Harrison AC. Susceptibility to nontuberculous mycobacterial lung disease. Eur Respir J. 2008;31(6):1322–1333. doi:10.1183/09031936.00140007
2. Nekooie-Marnany N, Deswarte C, Ostadi V, et al. Impaired IL-12- and IL-23-mediated immunity due to IL-12Rbeta1 deficiency in Iranian patients with mendelian susceptibility to mycobacterial disease. J Clin Immunol. 2018;38(7):787–793. doi:10.1007/s10875-018-0548-1
3. Browne SK, Holland SM. Anticytokine autoantibodies in infectious diseases: pathogenesis and mechanisms. Lancet Infect Dis. 2010;10(12):875–885. doi:10.1016/S1473-3099(10)70196-1
4. Tang BS, Chan JF, Chen M, et al. Disseminated penicilliosis, recurrent bacteremic nontyphoidal salmonellosis, and burkholderiosis associated with acquired immunodeficiency due to autoantibody against gamma interferon. Clin Vaccine Immunol. 2010;17(7):1132–1138. doi:10.1128/CVI.00053-10
5. Lee WI, Huang JL, Wu TS, et al. Patients with inhibitory and neutralizing auto-antibodies to interferon-gamma resemble the sporadic adult-onset phenotype of Mendelian Susceptibility to Mycobacterial Disease (MSMD) lacking Bacille Calmette-Guerin (BCG)-induced diseases. Immunobiology. 2013;218(5):762–771. doi:10.1016/j.imbio.2012.08.281
6. Browne SK, Burbelo PD, Chetchotisakd P, et al. Adult-onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367(8):725–734. doi:10.1056/NEJMoa1111160
7. Tanaka Y, Hori T, Ito K, Fujita T, Ishikawa T, Uchiyama T. Disseminated Mycobacterium avium complex infection in a patient with autoantibody to interferon-gamma. Intern Med. 2007;46(13):1005–1009. doi:10.2169/internalmedicine.46.6452
8. Koya T, Tsubata C, Kagamu H, et al. Anti-interferon-gamma autoantibody in a patient with disseminated Mycobacterium avium complex. J Infect Chemother. 2009;15(2):118–122. doi:10.1007/s10156-008-0662-8
9. Patel SY, Ding L, Brown MR, et al. Anti-IFN-gamma autoantibodies in disseminated nontuberculous mycobacterial infections. J Immunol. 2005;175(7):4769–4776. doi:10.4049/jimmunol.175.7.4769
10. O’Connell E, Rosen LB, LaRue RW, et al. The first US domestic report of disseminated Mycobacterium avium complex and anti-interferon-gamma autoantibodies. J Clin Immunol. 2014;34(8):928–932. doi:10.1007/s10875-014-0073-9
11. Hoflich C, Sabat R, Rosseau S, et al. Naturally occurring anti-IFN-gamma autoantibody and severe infections with Mycobacterium cheloneae and Burkholderia cocovenenans. Blood. 2004;103(2):673–675. doi:10.1182/blood-2003-04-1065
12. Doffinger R, Helbert MR, Barcenas-Morales G, et al. Autoantibodies to interferon-gamma in a patient with selective susceptibility to mycobacterial infection and organ-specific autoimmunity. Clin Infect Dis. 2004;38(1):e10–e14. doi:10.1086/380453
13. Chan JF, Yee KS, Tang BS, Cheng VC, Hung IF, Yuen KY. Adult-onset immunodeficiency due to anti-interferon-gamma autoantibody in mainland Chinese. Chin Med J (Engl). 2014;127(6):1189–1190.
14. Ku CL, Lin CH, Chang SW, et al. Anti-IFN-gamma autoantibodies are strongly associated with HLA-DR*15:02/16:02 and HLA-DQ*05:01/05:02 across Southeast Asia. J Allergy Clin Immunol. 2016;137(3):945–948 e948. doi:10.1016/j.jaci.2015.09.018
15. Chitasombat M, Supparatpinyo K. Penicillium marneffei Infection in Immunocompromised Host. Curr Fungal Infect Rep. 2012;7(1):44–50. doi:10.1007/s12281-012-0119-5
16. Chan JF, Lau SK, Yuen KY, Woo PC. Talaromyces (Penicillium) marneffei infection in non-HIV-infected patients. Emerg Microbes Infect. 2016;5:e19. doi:10.1038/emi.2016.18
17. Yu X, Liu P, Liu G, et al. The prevalence of non-tuberculous mycobacterial infections in mainland China: systematic review and meta-analysis. J Infect. 2016;73(6):558–567. doi:10.1016/j.jinf.2016.08.020
18. Aoki A, Sakagami T, Yoshizawa K, et al. Clinical significance of interferon-gamma neutralizing autoantibodies against disseminated nontuberculous mycobacterial disease. Clin Infect Dis. 2018;66(8):1239–1245. doi:10.1093/cid/cix996
19. Chi CY, Lin CH, Ho MW, et al. Clinical manifestations, course, and outcome of patients with neutralizing anti-interferon- autoantibodies and disseminated nontuberculous mycobacterial infections. Medicine. 2016;95:25. doi:10.1097/MD.0000000000003927
20. Chetchotisakd P, Kiertiburanakul S, Mootsikapun P, Assanasen S, Chaiwarith R, Anunnatsiri S. Disseminated nontuberculous mycobacterial infection in patients who are not infected with HIV in Thailand. Clin Infect Dis. 2007;45(4):421–427. doi:10.1086/520030
21. Phoompoung P, Ankasekwinai N, Pithukpakorn M, et al. Factors associated with acquired anti IFN-gamma autoantibody in patients with nontuberculous mycobacterial infection. PLoS One. 2017;12:4. doi:10.1371/journal.pone.0176342
22. Jutivorakool K, Sittiwattanawong P, Kantikosum K, et al. Skin manifestations in patients with adult-onset immunodeficiency due to anti-interferon-gamma autoantibody: a relationship with systemic infections. Acta Derm Venereol. 2018;98(8):742–747. doi:10.2340/00015555-2959
23. Xu X, Lao X, Zhang C, et al. Chronic Mycobacterium avium skin and soft tissue infection complicated with scalp osteomyelitis possibly secondary to anti-interferon-gamma autoantibody formation. BMC Infect Dis. 2019;19(1):203. doi:10.1186/s12879-019-3771-3
24. Chi CY, Chu CC, Liu JP, et al. Anti-IFN-gamma autoantibodies in adults with disseminated nontuberculous mycobacterial infections are associated with HLA-DRB1*16:02 and HLA-DQB1*05:02 and the reactivation of latent varicella-zoster virus infection. Blood. 2013;121(8):1357–1366. doi:10.1182/blood-2012-08-452482
25. Cohen PR, Kurzrock R. Sweet’s syndrome revisited: a review of disease concepts. Int J Dermatol. 2003;42(10):761–778. doi:10.1046/j.1365-4362.2003.01891.x
26. Baerlecken N, Jacobs R, Stoll M, Schmidt RE, Witte T. Recurrent, multifocal Mycobacterium avium-intercellulare infection in a patient with interferon-gamma autoantibody. Clin Infect Dis. 2009;49(7):e76–e78. doi:10.1086/605581
27. Chetchotisakd P, Anunnatsiri S, Nanagara R, Nithichanon A, Lertmemongkolchai G. Intravenous cyclophosphamide therapy for anti-IFN-gamma autoantibody-associated mycobacterium abscessus infection. J Immunol Res. 2018;2018:6473629. doi:10.1155/2018/6473629
28. Pruetpongpun N, Khawcharoenporn T, Damronglerd P, et al. Disseminated talaromyces marneffei and mycobacterium abscessus in a patient with anti-interferon-gamma autoantibodies. Open Forum Infect Di. 2016;3:2.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.