Back to Journals » Risk Management and Healthcare Policy » Volume 16
Dissecting WASH Assessment Tools and Recommending a Comprehensive Tool for Indian Healthcare Facilities
Authors Trivedi P, Bhavsar P ![]() , Kalpana P
, Kalpana P ![]() , Patel K
, Patel K ![]() , Das T, Yasobant S
, Das T, Yasobant S ![]() , Saxena D
, Saxena D ![]()
Received 29 May 2023
Accepted for publication 9 August 2023
Published 18 August 2023 Volume 2023:16 Pages 1593—1610
DOI https://doi.org/10.2147/RMHP.S376866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Poonam Trivedi,1 Priya Bhavsar,2 Pachillu Kalpana,2,3 Krupali Patel,4 Tanmoy Das,5 Sandul Yasobant,1,2,6 Deepak Saxena1,2,6
1Department of Public Health Science, Indian Institute of Public Health Gandhinagar (IIPHG), Gandhinagar, Gujarat, India; 2Centre for One Health Education, Research & Development (COHERD), Indian Institute of Public Health Gandhinagar (IIPHG), Gandhinagar, Gujarat, India; 3Centre for Development Research (ZEF), University of Bonn, Bonn, Germany; 4Parul Institute of Public Health, Parul University, Waghodia, Gujarat, India; 5Terre des hommes Foundation, Kolkata, West Bengal, India; 6School of Epidemiology & Public Health, Datta Meghe Institute of Medical Sciences (DMIMS), Wardha, Maharashtra, India
Correspondence: Deepak Saxena, Indian Institute of Public Health Gandhinagar, Opp. Air Force Head Quarters, Nr. Lekawada, Gandhinagar, Gujarat, 382042, India, Email [email protected]
Abstract: Providing adequate Water Sanitation and Hygiene (WASH) in Health Care Facilities (HCFs) has many benefits, including achieving Sustainable Development Goals (SDGs) and Universal Health Coverage (UHC). However, there is a significant shortage of statistics on the status of WASH in Healthcare Facilities (WinHCF), resulting in roadblocks in developing improvement strategies. Further, there is a lack of detailed comparison of WASH components covered in available tools against the standards. The present study aims to dissect the national and international tools for WASH assessment in HCFs to suggest comprehensive WASH indicators. The databases like PubMed, Scopus, ScopeMed, Cochrane and Google Scholar were used to extract the available tools. The assessment process, methodology, and components of national and various international tools were compared and synthesized. A total of seven tools, namely WASH FIT 2, Facet, SARA, SPA, TOOL BOX-II, CDC and Kayakalp, were compared on eight components: water, sanitation, hand hygiene, healthcare waste, environmental cleaning and hygiene, infrastructure, workforce management, policy and protocols. Although most tools have covered the same indicators, the methodology and definitions differ. Few of the tools fail to capture the basic indicators defined by Joint Monitoring Programme (JMP). The critical indicators of policy and protocols are only covered in WASH FIT 2, Kayakalp, and TOOL BOX-II. Likewise, most tools fail to capture the indicator of cleaning, IPC practices and climate resilience. The present review also highlighted the limitations of selected tools regarding definitions, methodology and implementation. Hence, based on the review findings, a comprehensive short tool has been developed to monitor WASH in HCF of India. It comprises all the essential fundamental indicators identified from various tools, and recommended by the JMP service ladder with proper definitions. This tool can be helpful for hospital staff and managers for the routine monitoring of WASH in HCFs and improve the quality of care and IPC practices in HCFs.
Keywords: WASH, IPC, SDGs, universal health coverage, assesment
Introduction
Water, sanitation and hygiene (WASH) in health care facilities (HCFs) is “the provision of water, sanitation, health care waste, hygiene, and environmental cleaning infrastructure, and services across all parts of a facility”.1 The WASH is crucial and has several benefits, including improving the quality of care and maternal, child and adolescent health, reducing antimicrobial resistance (AMR) and strengthening infection prevention and control (IPC) practices.1 The improved WASH also boosts the self-confidence and the performance of healthcare workers, reduces the national healthcare burden, and provides a platform to promote improved hygiene practices within the community. Further, there is also inequity in countries that lack essential WASH services, which has gained much attention after the COVID-19 pandemic. COVID-19 highlighted the lack of investment in WASH infrastructure, training, and commitment worldwide. Given several benefits and impacts of WASH in HCFs, universal access to water and sanitation has been recognized as key to achieving universal health coverage (UHC). The global goals for the 2030 Sustainable Development Goals (SDG) 6 also discussed ensuring all access to water and sanitation. The 2018 Declaration of Astana underpinned the country’s commitment to strengthen primary health care (PHC) for enhanced progress on UHC and the SDGs.2
With increased healthcare utilization in low/middle-income countries (LMICs), improving WASH services in HCFs is crucial to reduce the burden of hospital acquired infections (HAIs) and ensure patient safety. Hundreds of millions of patients annually are affected by HAIs; it is estimated that during the hospital stay, 15% of patients develop one or more infections, especially among women who come to the healthcare facility for delivery.3–6The evidence suggests that more than one million deaths yearly are associated with unclean births, while 26% of neonatal deaths and 11% of maternal mortality are due to infection.3,4 Most of these deaths are concentrated in LMICs, where HAI rates are twice that of high-income countries. In India, due to various initiatives like Janani Suraksha Yojana (JSY) and Kasturba Yojana, there is an increase in institutional delivery, which reflects a greater need to maintain WinHCFs. However, the WASH in maternity care units is scarce, with only 19.2% in labour rooms and 3.2% in post-natal care wards across three tiers of health facilities having functional toilets.5
In India, the healthcare system has a mix of public and private HCFs. There are a total of 1,57,921 Sub Centres (SCs), 30,813 Primary Health Centres (PHCs), 5649 Community Health Centres (CHCs), 193 Sub-divisional Hospitals (SDHs) and 810 Districts Hospitals (DH) in the country7 and additionally a total of 43,486 private hospitals.8 In India, more than one in four HCFs lack basic water service (ie, a water source within 500 m of the facility). There is insufficient sanitation coverage, with only 55% of facilities having access to improved sanitation compared with the global average of 79% across LMICs.6 Moreover, even facilities with good infrastructure often face issues due to lack or unsuitable accessibility, quality and functionality. Due to the lack of access to water and sanitation, women are further discouraged from institutional delivery or delayed health-seeking advice.5
Given the several impacts of WASH, WinHCF received more attention. In 2019, the WHO/ Unicef Joint Monitoring Programme (JMP) published the first comprehensive global baseline report for water supply, sanitation and Hygiene.9 Although the data represents the first global estimates on WinHCFs and is an essential step toward monitoring progress towards the SDGs, there remain considerable gaps in data. Most countries fail to monitor their progress due to a lack of data, e.g. only 18 out of 200 countries have enough data to estimate the coverage of essential sanitation services in HCFs, and very few have data on medical waste management.9 There is also a significant shortage of national, regional and worldwide statistics on the status of WinHCF. Without reliable disaggregating data by location and type of facility causes difficulties in understanding and responding to needs and developing cost-improvement plans.9 The findings suggest a need for accelerated monitoring efforts at HCFs, sub-nationally and nationally, to strengthen international efforts toward SDG targets.3
Currently, in India, the only national initiative for WinHCFs is the Kayakalp programme launched in 2015 as an extension of Swachh Bharat Abhiyan (SBA), the nationwide campaign for universal sanitation coverage. The review of WASH assessment tools published in 2019 reported that although various tools are available for WASH assessment at the global level and in India, there is a lack of consensus between the different tools.10 However, there is still a lack of detailed comparison of WASH components and indicators covered in national and international tools. Therefore, this manuscript intends to conduct a review of national and international tools, which could potentially provide important lessons and an opportunity to develop a more comprehensive tool that can be adopted for routine monitoring of WinHCFs in India. Thus, this work is explicitly based on the review with a final recommendation of a comprehensive WinHCFs of India.
Materials
This study intends to recommend a comprehensive WASH assessment tool for HCFs of India by reviewing the national and international guidelines. The review used databases like PubMed, Scopus, ScopeMed, Cochrane and Google Scholar to extract available tools for the WASH assessment of HCFs. The assessment process, methodology, components, national (Kayakalp) indicators and various international tools were compared and synthesized. The information regarding the national tool Kayakalp were collected from the appropriate sources. The search terms like water, “sanitation”, ‘AND’ “hygiene” in combination with words like health care facilities’ AND’ “survey instruments”, “monitoring”, “evaluation”, “policy”, “guidelines”, and “best practice” ‘&’ “standards of care” were used.
Results
Seven WASH assessment tools were extracted based on search criteria. The tools included in the review were WASH FIT 2,11 FACET,12 SARA,13 SPA,14 CDC,15 TOOL BOX-II and Kayakalp.16 The description of each tool is presented below in Table 1.
 |
Table 1 Summary of Tools Included in the Review |
Overview of the WASH Indicators Across the Selected Tools
All the above tools were compared based on the eight components of WASH: water, sanitation, hand hygiene (and overall hygiene), waste management, environmental cleaning and hygiene, and other governance-associated indicators (infrastructure, management and workforce, policy and protocols). As presented in Table 2, the mode of data collection is common in all the tools. The information is collected through internal/external staff observation or staff interviews. However, in WASH FIT 2, Kayakalp and TOOL BOX-II, the information related to policy and protocols is also validated/ gathered from the record review. Although visual audit is covered in all the tools, its validation through microbiological surveillance is not covered in tools except Tool Box-II. While; in Kayakalp, only records of microbiological surveillance are observed. The determinants of WASH are only covered in the CDC tool.
 |
Table 2 Summary of Methodology and Components of WASH Assessment Tools |
Limitation of Tools
The present study also identified the limitation of various WASH tools. The Kayakalp is a lengthy tool lacking a specific focus on WASH that can be difficult to use for monitoring WinHCFs. Further, the various WASH components are not separate, making filling in the information and analyzing specific WASH components difficult. In most of the tools, there is a lack of focus on cleaning practices except for Kayakalp and TOOL BOX-II. Tools like SPA, SARA, and CDC fail to define the indicators. On the contrary, the indicators are defined correctly in WASH FIT 2, FACET and Kayakalp. Tools like CDC and SPA also capture the various determinants of the WinHCF by documenting the staff’s and patient’s satisfaction. In most tools, the information is collected through observation and staff interviews; but it is not validated by microbiological surveillance except in TOOL BOX-II and Kayakalp.
Water
Table 3 represents an overview of 17 water indicators and their consideration mode among the selected seven tools. The different tools have assessed the reported or observed indicators, also mentioned as superscript in the table. The source of water and accessibility is considered in all the tools except Kayakalp. Water availability is covered in all tools and documented through observation, while in Kayakalp, the information is collected from the patient and staff. The functionality of water points is only covered in WASH FIT 2 and TOOL BOX-II.
 |
Table 3 Mode of Documentation and Presence of Water Indicators Among the Selected Seven WASH Assessment Tools |
Similarly, the availability of sufficient water is covered only by four tools (WASH FIT 2, Kayakalp, Facet, and CDC). The indicators on water interruption and the alternate mechanism are only captured in three tools CDC, WASH FIT 2 and TOOL BOX-II. Similarly, the information on the alternate mechanism is captured in WASH FIT 2, CDC, FACET and TOOL BOX-II. In WASH FIT 2, the improved water source and accessibility are also included in addition to availability. The availability of drinking water is essential; however, SARA, SPA, and FACET fail to capture this indicator. In addition to that, the visual cleanliness of water points is also included in TOOL BOX-II. The availability of safe drinking water (presence of e-coli, chlorination) is captured in WASH FIT 2, FACETet, Kayakalp, and CDC. The information about arsenic testing is also gathered in FACET from the records. At the same time, the indicators of water treatment mechanisms are captured only in WASH FIT 2, Facet and CDC. None of the tools has covered the indicators of rainwater harvesting and conservation, except Kayakalp and WASH FIT 2.
Sanitation
Table 4 indicates that various tools have covered only the availability and type of toilets; however, the clear-cut definition of improved and sufficient toilets is unclear in tools except for WASH FIT 2 and Facet. The indicators on availability and type of toilets, whether improved or not, are captured in Kayakalp. All the tools have covered indicators on the separate toilet for people with limited mobility, except the SARA tool. Out of seven tools, the availability of separate toilets for menstrual management is covered only in the WASH FIT 2, FACET, CDC, and SPA tool. The visual cleanliness of the toilet is assessed only in FACET, Kayakalp, CDC, and TOOL BOX-II. The information on the drainage of toilets is only captured in WASH FIT 2, CDC and TOOL BOX-II. The hand washing facility for toilets is covered in all tools except Kayakalp and SARA. While most tools have captured the availability of a functional hand-washing facility for toilets, the cleanliness of the hand-washing facility is only captured in the TOOL BOX-II. The availability of showers is only covered by CDC and WASH FIT 2 tools. Most tools lack faecal sludge, storm, and wastewater management indicators except WASH FIT 2 and FACET tool. The information on IEC on the use of the toilet is only covered in Kayakalp. The open defecation around the facility is only covered in FACET and CDC.
 |
Table 4 Comparison of the Sanitation Indicators of Selected Tools |
Hand Hygiene
A total of nine indicators of hand hygiene were extracted from seven tools. The comparison of Tools based on each indicator is presented in Table 4. Although the functioning hand washing station is assessed with all the tools, the way of measurement and the definitions used for the assessment are different. In most of the tools, the functionality of the hand washing station is assessed through the availability of water and soap or alcohol hand rub. In TOOL BOX-II, the type of hand washing facility is also observed in addition to hand washing facilities. In TOOL BOX-II, accessibility and visual cleanliness of the hand washing station are also observed, which is not covered in any of the tools. Out of all seven tools, only half have the indicator on hand hygiene promotion, like WASH FIT 2, FACET, TOOL BOX-II and Kayakalp. Out of seven, the availability of hand hygiene compliance is only covered in SPA and WASH FIT 2. In WASH FIT 2, hand hygiene promotion, compliance, and hand hygiene audits for supply availability are also captured, which is not covered in other tools.
The availability of hand-drying material is only observed in the CDC tool. The availability of adequate personal protective equipment (PPE), mask, gloves, cap, boots, and goggles are covered in SARA, WASH FIT 2, TOOL BOX-II and Kayakalp. However, in the CDC tool, only the availability and type of gloves used in the facility are observed, and in FACET, the availability of PPE for waste handlers is assessed. The availability of alcohol hand rub is covered in all the tools. Surgical and nursing clothing use after proper sterilization is documented only in Kayakalp and TOOL BOX-II (Table 5).
 |
Table 5 Comparison of the Hygiene Indicators of Selected Tools |
The availability of functional sterilization apparatus (autoclave, sterilizer, chemical treatment) is covered in SARA, SPA, TOOL BOX-II and FACET. In Kayakalp and TOOL BOX-II, whether the autoclave is done correctly is documented through a signal lock for sterilization. The sterility of autoclaved packs maintained during storage is only covered in Kayakalp.
Environmental Cleaning
The cleanliness/ types and separate mops for critical areas are essential for the prevention of cross-infection. The cleaning policy and protocol review of HCFs is only covered in WASH FIT 2, Kayakalp, CDC and TOOL BOX-II (Table 6). The frequency of changing bed sheets and linen is also captured in the toolbox, CDC, and Kayakalp tool. However, it is covered only in TOOL BOX-II and Kayakalp. In TOOL BOX-II, in addition to availability, visual cleanliness of mops and buckets is also observed, and microbiological samples are taken to validate the cleanliness.
 |
Table 6 Comparison of the Environmental Cleaning Indicators of Selected Tools |
Mops type and its storage practices (laundered properly) are also covered in TOOL BOX-II; this information is not covered in the rest of the tools. The direction of mopping, disinfection and washing of mops are covered only in Kayakalp. The number of cleaning staff required is captured in WASH FIT 2, TOOL BOX-II and CDC, which is not captured in the rest of the tools. The dedicated person for monitoring housekeeping is only covered in CDC and Kayakalp tools. The training on cleaning protocols is essential to maintain cleanliness and prevent hospital-acquired infection. In most of the tools, this indicator is covered with different definitions. Awareness & demonstration of various cleaning procedures like the correct concentration of cleaning solution, Adherence to high-level disinfection, Chemical sterilization as per protocol, and decontamination process are only observed in Kayakalp. The availability of extra staff (e.g.a roster) and cleaning supplies in case of a high load are covered only in WASH FIT 2.
The availability of detergents/ mops and buckets is covered in the tools of WASH FIT 2, TOOL BOX-II, Kayakalp, and Facet. In Kayakalp, eco-friendly buckets and charts should be available for mopping in addition to materials not covered in any of the tools. Food hygiene is documented only in two tools WASH FIT and Kayakalp. While the laundry services management is only covered by WASH FIT 2 and TOOL BOX-II, the rest of the tools fail to capture this information. Like WASH FIT 2, the cleanliness and separation of clean and dirty linen are covered in TOOL BOX-II; however, whether the sufficient area is available is only covered in TOOL BOX-II. In contrast, the details about the availability and cleanliness of separate storage areas for dirty linen (till the collection for washing) are also covered in TOOL BOX-II, which is not covered in WASH FIT 2. In addition, whether the food is prepared safely with clean hands and utensils is also covered in WASH FIT 2.
Healthcare Waste
The availability of waste bins is covered in all the tools except Kayakalp. However, the categories are defined differently. In SPA, SARA, CDC and Tool BOX-II, only the availability of containers with liners is observed and reported; however, the number of bins is not captured. The disposal practices of syringes and the availability of hub cutters are covered only in two tools, Kayakalp and Tool BOX-II. In contrast, the availability of a sharp box is documented in all the tools. The availability of kits for waste transportation is not covered in any tools except FACET.
The availability of PPE for waste handlers is covered in FACET, CDC and WASH FIT 2. The availability of a hand hygiene facility for waste handlers is not covered in most tools except WASH FIT 2 and Kayakalp. The availability of a dedicated storage area is essential for IPC. This indicator is covered in the toolbox, Kayakalp, FACET, CDC, and WASH FIT 2. In Facet and CDC, the accessibility (fenced or locked storage facility) is also documented, whereas sufficient storage capacity is only reported in WASH FIT 2. The correct segregation is covered in all the tools except SARA and SPA.
Waste treatment technology for infectious and sharp waste is covered in all except Kayakalp. In TOOL BOX-II, there is no separate indicator for infectious and shape waste management; only how waste is managed in HCFs is documented. In WASH FIT 2, the infectious and sharp waste is combined into a single indicator. However, in other tools, the indicators related to the availability and functionality of the incinerator are given separately. The availability and functionality of the incinerator are captured in SARA, SPA and FACET with different methodologies. However, the availability of an ash pit for incinerators is only covered in WASH FIT 2. The availability of sufficient energy for incineration is covered in SPA, SARA, and WASH FIT 2. The functionality of the burial pit is covered only in WASH FIT 2 and Kayakalp.
TOOL BOX-II, Kayakalp, and WASH FIT 2 document the duration of storage of infectious waste. However, the definitions used in all are different. The segregation of anatomical waste is captured in TOOL BOX-II and WASH FIT 2; however, it is burned in a cremated or buried in a cemetery correctly is only covered in WASH FIT 2 (Table 7). Additionally, whether the burial pit withstands flooding is also captured in WASH FIT 2.
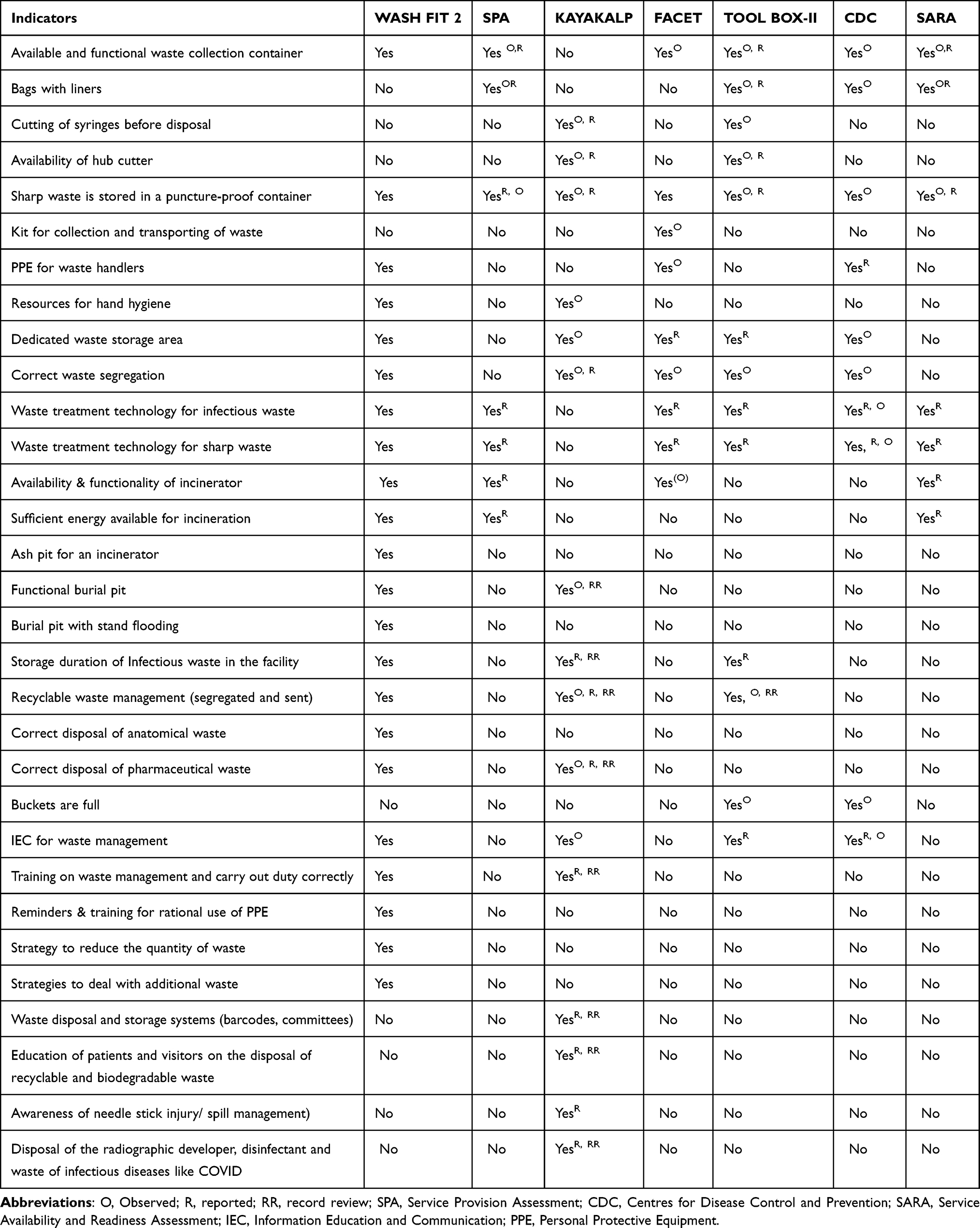 |
Table 7 Comparison of the Healthcare Waste Indicators of Selected Tools |
The indicator related to the treatment and disposal of pharmaceutical waste is covered only in WASH FIT 2 and Kayakalp. The removal of recyclable waste is documented in Kayakalp and WASH FIT 2. The quantity of waste is only documented in TOOL BOX-II and CDC. The reminder for bio medical waste (BMW) is captured in WASH FIT 2, Kayakalp, TOOL BOX-II and CDC. The indicators on the training of staff members on BMW are only captured in WASH FIT 2 and Kayakalp. Additional indicators like reminders and training on the rational use of PPE to reduce the quantity of waste and to deal with extra waste are only documented in WASH FIT 2. The indicator related to HCF is litter-free and is covered only in FACET and CDC.
Additional Blocks of WASH Assessment
Although most of the tools cover the source of electricity and functional backup system, Kayakalp and FACET fail to capture this indicator. WASH FIT 2 also captures the availability of sufficient energy, which is not covered in any of the tools. While the indicator on the primary source and backup is not covered in Kayakalp, the adequate lighting in the delivery room, indoors, and the hospital entrance is covered in Kayakalp, which is not covered in the rest of the tools except WASH FIT 2. The indicator on energy-efficient lighting is also covered in the latest Kayakalp tool and WASH FIT 2. The additional indicator on adequate lighting in showers and latrines, including at night, is covered in WASH FIT 2 and FACET, which is not covered in the rest of the tools.
The vector control measures are also assessed in tools like WASH FIT 2, Kayakalp, FACET and SPA. Sufficient functional environmental ventilation is captured only in WASH FIT 2 and Kayakalp. Similarly, the indicator of aesthetic appearance (painting, landscaping) is only covered in WASH FIT 2 and Kayakalp. FACET, the additional indicator on whether the HCFs are equipped with mosquito netting on doors and windows, is also included. It is captured through the availability of insecticide-treated nets for the beds (Table 8).
 |
Table 8 Comparison of the Infrastructure Indicators of Selected Tools |
Adequate and trained human resources must maintain WASH and IPC in HCFs. An up-to-date organogram is essential to understand the hierarchy in HCFs and supervision and monitoring mechanisms. However, it is not covered in most tools except WASH FIT and TOOL BOX-II (Table 9). Similarly, the indicator on the training of new staff, including waste handlers and cleaners, especially for IPC and WASH training, is only covered in WASH FIT 2 and TOOL BOX-II. The performance-based appraisal is not documented in most tools except TOOL BOX-II and WASH FIT 2. A clear written job description for staff, including cleaners, can improve staff accountability so that they can perform the task most effectively. However, WASH FIT 2 and Kayakalp have covered the clear-cut job responsibility indicator (including WASH & IPC) (Table 10).
 |
Table 9 Comparison of the Management of Workforce Indicators of Selected Tools |
 |
Table 10 Comparison of the Policy & Protocols Indicators of Selected Tools |
IPC committees are covered only by four tools: WASH FIT 2, Kayakalp, TOOL BOX-II, and SPA. In SPA, the quality management committee is documented instead of IPC. TOOL BOX-II and Kayakalp only cover the written protocol for BMW. However, the protocols for changing mops and buckets are only reported in TOOL BOX-II. A protocol for ongoing operation and maintenance of infrastructure and procurement is only covered in WASH FIT 2 and TOOL BOX-II. The existence and implementation of policies for cleaners’ occupational and patient safety are covered only by WASH FIT 2. Similarly, consultation with Women, disabled and indigenous groups, users, and staff about WASH needs and technology designs is only covered in WASH FIT 2.
The indicators on the budget for cleaning/ IPC are captured only in WASH FIT 2 and TOOL BOX-II. Some indicators on protocols and monitoring mechanisms for infection are only covered in Kayakalp and TOOL BOX-II. As presented in Table 10, the indicators related to various protocols for IPC, like the restricted entry of visitors, regular monitoring of IPC practices, separate areas for infectious patients, measurement of device-related HAIs, etc., are only covered by Kayakalp. It includes the review of protocols for regular microbiological surveillance, measurement of HAIs, antibiotic policy, provision of Isolation ward, and protocol for autoclave. The provision of an isolation ward is also covered in the SPA tool. The dedicated person for maintaining IPC is not covered in most tools except WASH FIT 2 and TOOL BOX-II.
Similarly, a dedicated person for cleaning is covered in TOOL BOX-II, SPA, and CDC tools. The dedicated person for infectious disease surveillance is also covered in the SPA tool, which is not covered in the rest. The IPC staff training is covered in five tools while not in SARA and CDC. The indicator on staff vaccination for prevention of HAI (like Hep. B) is only covered in three tools: WASH FIT 2, TOOL BOX-II and Kayakalp. The various indicators of emergency response in case of pandemics/ epidemics are covered in WASH FIT, while the rest of the tools fail to capture this indicator. Emergency preparedness and response plans are not covered by any tools except WASH FIT 2 and SPA.
Discussion
The present review highlighted that although various tools have covered the WASH components, there is a lack of uniformity in definitions and methodology adopted for the assessment. E.g., In tools like SPA, TOOL BOX-II, and SARA, the information is collected through staff interview and observation, while in Kayakalp, the information is collected through various methods, e.g. indicator is assessed through patient and staff interviews and observation. However, how to score the data collected through different approaches is unclear. A few tools like Kayakalp are not specifically for WASH assessment; hence the various WASH components are not separate, making filling in the information and analyzing specific WASH components difficult.
Further, various tools like SARA, SPA, and TOOL BOX-II do not define the indicators. While in WASH FIT 2, each indicator is correctly defined in three scoring categories. The explanatory notes with the references are also given to ease the data collection process. Similarly, the indicators are also defined in the FACET tool for assessment. However, a few limitations of WASH FIT 2, the score assigned to selected individual indicators may be subjective, relying on observations that could vary from person to person.17 It is less focused on IPC and visual cleanliness practices. Most information in this tool is captured through observation and reported by the staff.
The present review also found that most tools fail to capture the indicators of the JMP WASH service ladders.2 The JMP classifies water supply, sanitation, hygiene, waste management, and environmental cleanliness as basic, limited and no service. It was formed by the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) with objective to generate the internationally comparable data to monitor progress towards the attainment of SDG targets related to WASH. JMP defines the basic water facility which includes the water availability from an improved source on-premises, an improved water source within 500 meters of the premises, but not all requirements for basic services are met.18 Although the other tools have covered this indicator, they have adopted different definitions e.g. In WASH FIT 2, FACET tool and TOOL BOX-II; the water source is defined as the availability of an improved source (defined as per the JMP criteria). Whereas the list of sources is provided in CDC, SPA, and SARA tools, the improved source is not defined. Staff reports the information on water sources in the TOOL BOX-II, SARA, FACET, and SPA.
Kayakalp fails to capture whether the water is from the improved source. In contrast, the reported data is verified through observation in the CDC tool. As per JMP, the accessibility of water is defined as water availability on the premises, within 500 meters, and more than 500 meters as basic, limited, and no service, respectively. FACET, CDC, and SPA tool have adopted the same definitions. However, in WASH FIT 2 and SARA, only water availability on the premises or outside is captured.
A sufficient water supply is essential to provide appropriate quality care and maintain WASH and IPC practices in HCFs. However, out of seven tools, only four covered this critical indicator. The definition of sufficient water differs in all four tools (WASH FIT 2, Kayakalp, FACET, and CDC). WASH FIT 2 has defined sufficient water quantity per the WHO guidelines on Essential environmental standards in health care. In contrast, FACET only captures the availability of enough water, which is not defined, and sufficient quantity means the water containers should have a capacity of 500 lit or more per the CDC tool. In Kayakalp, a sufficient amount is determined as at least 200 liters of water per bed per day is available (if municipal supply). Or the water is available on a 24×7 basis at all points of usage (for facilities having less than 100 beds, 350 litres per bed/day).
As per the JMP criteria, the facility should have at least one toilet for people with limited disabilities. All the tools have covered this indicator except the SARA tool. Although various tools have captured the availability of toilets for limited disabilities, the definitions and options are different. In the Kayakalp and TOOL BOX-II, only the availability of toilets for people with limited mobility is captured, which is not adequately defined. In WASH FIT 2, the requirement for limited mobility is defined as accessible without stairs or steps; handrails for support are attached either to the floor or sidewalls; the door is at least 80 cm wide; the toilet has a raised seat (between 40–48 cm from the floor), a backrest and the cubicle has space for circulation/ manoeuvring. Similarly, FACET, CDC and SPA tools also used the same criteria; however, unlike WASH FIT 2 and FACET, the option to check functionality is not covered in the rest of the tools.
A separate improved toilet for staff and separates for males and females is needed to meet the requirement for basic sanitation, as per JMP guidelines. As per WASH FIT 2, a separate improved toilet should exist and be labelled appropriately for males and females. In CDC and TOOL BOX-II tools, the availability of separate toilets for males and females is captured only through reported information. In contrast, in the SPA tool, the availability of separate toilets is documented through observation.
The indicators of climate resilience, like faecal sludge, storm, and wastewater management, are not covered in most tools except for WASH FIT 2 and Facet tool. Further, The cleanliness/ types and separate mops for critical areas are essential for the prevention of cross-infection. However, this indicator is not covered in the five tools included in this review. It is covered only in TOOL BOX-II and Kayakalp. The cleaning policy and protocol review of HCFs is only covered in three tools WASH FIT 2, Kayakalp, and TOOL BOX-II.
The present review highlighted the need for a comprehensive, easily adaptable tool for the routine monitoring of WinHCF comparable to international standards of JMP. Based on the present review, a comprehensive tool for WASH assessment has been developed, which can be used by an internal team of HCFs for routine monitoring of WASH practices. Although this comprehensive tool was recommended keeping a view on Indian HCFs, it is very much likable that other settings having similar context to India like country can easily adopt this tool with a validation. This tool has a potential to be implemented in the HCFs of various levels including public and private, thus the scalability of this tool is highly recommended to any other similar settings.
Recommended WASH Assessment Components
Based on the review findings, Table 11 indicates the essential components that must be considered for the WASH assessment. The recommended comprehensive WASH assessment tool for HCFs of India has both the observed and reported components within the components of water, sanitation, hand hygiene, environmental hygiene, biomedical waste management, governance. Although most of the components could be assessed through both observation and reported method except governance can only be reported; however, it depends which assessment mode to accept based on the factors like, who is the assessor, time for the assessment, resources for the assessment. In ideal scenario, it is recommended to assess the indicators through both the observation and reported method for better accuracy. Additionally, this tool has a great advantage by combining most of the indicators from various existing tools. Earlier any of the single existing tool was not having all the proposed indicators of the comprehensive tools. Therefore, it is highly recommended to conduct the WASH assessment more comprehensively.
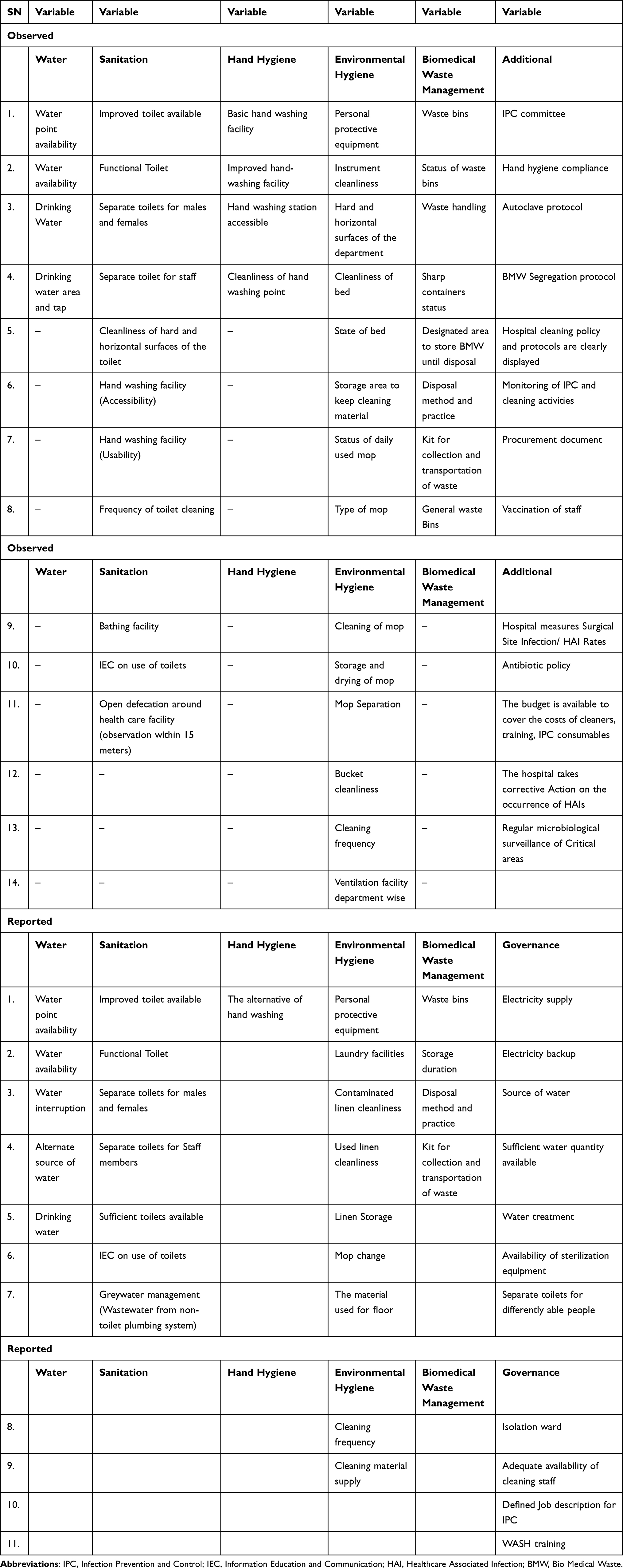 |
Table 11 Recommended WASH Assessment Components |
Conclusions
Although various tools are available for WASH assessment, no tool covers all essential indicators and is comparable to international standards. The present review provides the basic WASH assessment tool with a standard definition developed based on the review of national and international WASH tools. The tool aims to help the healthcare staff with routine monitoring of HCFs and gap assessment, which can be used to develop improvement plans and quality improvement of the HCFs, improving the IPC practices, and staff and patient satisfaction.5
Acknowledgments
We extend our gratitude to the Health and Family Welfare and the Government of Kolkata for their kind support during the project activities. We thank the WASH experts for providing the necessary guidance for this study. We are also thankful to the research team of the Indian Institute of Public Health Gandhinagar (IIPHG) for their extended support during the review. We would like to thank the Terre des hommes (TdH) for their continuous project support.
Both Indian Institute of Public Health Gandhinagar (IIPHG), India & Terre des hommes (TdH), India reserves the equal right for this work. No part of this publication is reproduced, stored, or distributed in any form or by any means, electronic or mechanical, including photocopying.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was made possible by the generous support of the Terre des hommes(TdH) Foundation, Kolkata, India. The work described in this article was conceptualized and developed by the Indian Institute of Public Health Gandhinagar. Staff of the funding agency critically reviewed the draft and offered comments to improve the paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Godfrey S, Keraita B, Fontana G, et al. WASH in health care facilities UNICEF scoping study in eastern and southern Africa united republic of Tanzania; 2019.
2. Joint Monitoring Program JMP, World Health Organization WHO, United Nations Children’s Fund UNICEF. Global progress report on wash in health care facilities; 2020.
3. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Heal. 2014;2(6):323–333. doi:10.1016/S2214-109X(14)70227-X
4. Lawn J, Graham W, Blencowe H. Evidence, experience, estimated lives saved and cost clean birth kits – potential To Deliver? Policy brief -purpose and process; 2010:1–16. Available from: https://www.healthynewbornnetwork.org/hnn-content/uploads/CBK_brief-LOW-RES.pdf.
5. UNICEF. WASH in health care facilities | UNICEF India. Available from: https://www.unicef.org/india/what-we-do/wash-facilities.
6. Tseng KK, Joshi J, Shrivastava S, Klein E. Estimating the cost of interventions to improve water, sanitation and hygiene in healthcare facilities across India. BMJ Glob Heal. 2020;5(12):1–11. doi:10.1136/bmjgh-2020-003045
7. National Health Mission. Infrastructure: national health mission. Available from: https://nhm.gov.in/index1.php?lang=1&level=2&sublinkid=1220&lid=190.
8. Jaffrelot C, Vihang J. Private healthcare in India: boons and banes. Institut Montaigne; 2020:1–6. Available from: https://www.institutmontaigne.org/en/blog/private-healthcare-india-boons-and-banes.
9. WHO; UNICEF; JMP. WASH in health care facilities, global baseline report 2019. 2019. Available from: https://www.unwater.org/publications/wash-in-health-care-facilities-global-baseline-report-2019/.
10. Patel K, Kalpana P, Trivedi P, Yasobant S, Saxena D. Assessment of water, sanitation and hygiene in HCFs: which tool to follow? Rev Environ Health. 2019;34(4):435–440. doi:10.1515/reveh-2019-0001
11. Water Health Organization U. Water and sanitation for health facility improvement tool (WASH FITT A practical guide for improving quality of care through water, sanitation and hygiene in health care facilities; 2018.
12. Terre des hommes, Eawag and CartONG, et al.The Facility Evaluation Tool for WASH in institutions (FACET). Available form: https://www.eawag.ch/en/department/sandec/projects/sesp/facet/
13. Republic of Zambia M of H. Zambia service availability and readiness assessment 2010, summary report; 2010. Available from: https://www.who.int/healthinfo/systems/zmb_sara_report_2010_web.pdf?ua=1.
14. The Demographic and Health Survey Program. Service provision assessment survey, Inventory Questionnaire the DHS Program; 2022.
15. CDC. Data collection tools and communication | the safe water system. CDC; 2020. Available from: https://www.cdc.gov/healthywater/global/healthcare-facilities/tools.html.
16. Ministry of Health And Family Welfare, Government of India, KAYAKALP; 2015. https://www.nhm.gov.in/images/pdf/in-focus/Implementation_Guidebook_for_Kayakalp.pdf.
17. Maina M, Tosas-Auguet O, McKnight J, et al. Extending the use of the world health organisations’ water sanitation and hygiene assessment tool for surveys in hospitals – from WASH-FIT to WASH-FAST. PLoS One. 2019;14(12):1–15. doi:10.1371/journal.pone.0226548
18. WHO; UNICEF; JMP. Core questions and indicators for monitoring WASH in health care facilities in the sustainable development goals; 2019.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.