Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Disease Burden and Unmet Needs in Chinese Patients with Symptomatic and Exacerbating COPD While on Triple Inhaled Therapy: A Cross-Sectional Real-World Study
Authors Sun Y, Pennant T, Barrable FR
Received 11 November 2025
Accepted for publication 9 March 2026
Published 21 March 2026 Volume 2026:21 580726
DOI https://doi.org/10.2147/COPD.S580726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Yongchang Sun,1 Tia Pennant,2 Fraser R Barrable2
1Department of Respiratory and Critical Care Medicine, Peking University Third Hospital, Beijing, People’s Republic of China; 2Adelphi Real World, Bollington, UK
Correspondence: Yongchang Sun, Department of Respiratory and Critical Care Medicine, Peking University Third Hospital, 49 Huayuan North Road, Haidian District, Beijing, People’s Republic of China, Tel +86 15611963697, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a common respiratory disease and a major cause of mortality and morbidity in China. Global studies have revealed a subgroup of patients who had COPD symptoms and frequent exacerbations while receiving triple inhaled therapy. This study aimed to describe the clinical characteristics and disease burden of this patient population in China.
Methods: This cross-sectional, real-world study drew data from the Adelphi COPD Disease Specific Programme (DSP)™ from July to November 2022 in China. Adult patients with a diagnosis of COPD and receiving triple therapy at survey date were included; among them, patients who had frequent productive cough and sputum, a history of smoking, ≥ 2 moderate or ≥ 1 severe exacerbation(s) in the prior 12 months and were receiving triple therapy were identified as the symptomatic SET cohort; all other patients were categorized as the triple therapy cohort. Disease-related characteristics and perceptions of disease control were described for both cohorts.
Results: Of the 135 patients receiving triple therapy, 39 (28.9%) were categorized into the symptomatic SET cohort and 96 (71.1%) into the triple therapy cohort. In the triple therapy and symptomatic SET cohorts, mean (SD) age was 65.9 (9.0) and 69.2 (8.7), respectively; mean (SD) number of exacerbations during the last 12 months was 1.3 (1.4) and 2.3 (1.3), respectively; mean (SD) CAT score was 21.0 (8.3) and 25.7 (7.1), respectively. According to physicians’ perception, around 70% of patients in the symptomatic SET cohort had, at the minimum, somewhat controlled COPD (completely controlled: 2.6%; well controlled: 28.2%; somewhat controlled: 38.5%). Satisfactory COPD control was achieved in 33.3% and 38.5% of patients in the symptomatic SET cohort as perceived by physicians and patients, respectively.
Conclusion: Substantial disease burden and large unmet needs existed among patients with symptomatic and exacerbating COPD while receiving triple inhaled therapy in clinical settings in China. Novel therapeutic options and improved guideline-directed disease management are needed.
Keywords: exacerbations, triple inhaled therapy, physician survey, patient-reported outcomes, disease burden, China
Introduction
Chronic obstructive pulmonary disease (COPD) is a common respiratory disease and a major cause of mortality and morbidity.1,2 In China, the prevalence of COPD was 8.6% among adults aged 20 years or older in 2018, corresponding to nearly 100 million patients,3 and representing approximately 25% of all COPD cases globally.4 As of 2017, COPD ranked as the third leading cause of both death and disease burden measured by disability-adjusted life years in China.5 Common COPD symptoms include chronic dyspnea, cough and expectoration;6 an acute worsening of these symptoms defines an exacerbation and results in the need for additional therapy.7 Chinese patients with COPD are substantially impacted by exacerbations,8 which severely affect patients’ health status,9 and represent a major risk factor for mortality, poor health-related quality of life (HRQoL), frequent hospital admission and increased healthcare resource utilization (HCRU).9
Inhaled therapy is the cornerstone of COPD treatment, including bronchodilation with inhaled long-acting β2-agonists (LABA) and/or long-acting muscarinic antagonists (LAMA).7 Inhaled corticosteroids (ICS) are further added for patients with recurrent exacerbations to form triple therapy, the highest level of inhaled treatment for COPD.7 Global evidence has suggested that, while receiving the maximal triple inhaled therapy, some patients still experienced frequent exacerbations.10–12 For instance, an observational study from the UK reported that 14.8% of patients experienced frequent exacerbations despite receiving at least three months of maximal triple inhaled therapy.11 These patients presented with significantly higher risks of COPD-related death compared to the overall patients with maintenance-treated COPD, representing heavy disease burden and unmet need.11 Ongoing research into potential new treatment options for such patients includes randomized clinical trials (RCTs) evaluating biologics with inflammatory targets, such as anti-IL-5, anti-IL-5Rα, anti-IL-4Rα, anti-thymic stromal lymphopoietin (TSLP) and anti-IL-33.13,14
Although several studies have reported on the real-world effectiveness of triple therapy in Chinese patients with COPD,15,16 few have focused on patients who experienced symptoms and frequent exacerbations while on triple therapy, and little is known about the disease burden of these patients. A previous global study has revealed substantial clinical burden and extensive unmet needs in patients with COPD who experienced frequent symptoms and exacerbations while receiving triple inhaled therapy;17 here in the current study, we aimed to understand the disease burden and unmet needs in such patient population in China.
Methods
Study Design and Participants
This observational, real-world study utilized data from the Adelphi Real World COPD Disease Specific Programme (DSP)TM. The Adelphi Real World DSPs are impartial data sources independent of any specific study and are not intended for addressing any prespecified research questions or hypotheses. The DSP methodology has been validated and used in previously published studies.18–21 The Adelphi Real World COPD DSP was a cross-sectional linked physician- and patient- survey conducted in nine countries (France, Germany, Italy, Spain, UK, US, Canada, Japan and China) and has been used in the previous global study.17 DSP data collected in China from July to November 2022 were drawn and analyzed for the current study.
The eligibility of physicians and patients in the DSP has been described previously.17 Physicians meeting the following criteria were eligible for inclusion: hospital-based health care professionals (HCP), including primary care physicians (PCP) and respiratory specialists; personally responsible for managing patients with COPD; and attended to three or more patients with COPD in a typical month. There were no exclusion criteria for physicians. Patients meeting the following criteria were eligible for inclusion: aged 18 years or older; with a physician-confirmed diagnosis of COPD; and were not concurrently involved in a clinical trial at the time of data collection. Patients were excluded if they were younger than 18 years of age or if they were currently enrolled in a clinical trial. Each participating physician completed patient record forms for up to five consecutive eligible patients consulting for routine care. These patients were then invited to independently complete a voluntary patient self-completion survey and constituted the overall DSP population. From the overall DSP population, patients who were receiving triple therapy for COPD treatment were selected, among which a symptomatic SET cohort was established by identifying patients who had been reported by their physicians as having frequent productive cough and sputum in the four weeks preceding survey date and met the following criteria: 1) history of smoking (current or former smokers); 2) ≥2 moderate (defined as requiring treatment with antibiotic and/or oral corticosteroid without emergency room visit or overnight hospitalization) or ≥1 severe (defined as requiring emergency room visit or overnight hospitalization) exacerbation in the 12 months preceding the survey date; and 3) a prescription for triple inhaled therapy at the time of survey.17 All other patients receiving triple therapy (excluding patients in the symptomatic SET cohort) were categorized into the triple therapy cohort.
Ethics
Informed consent was obtained from all participating patients via a tick box in the patient self-completion survey. Data were deidentified and pseudo-anoymized to ensure confidentiality and were aggregated before sharing with the subscriber and/or for publication.
This study was submitted to the Pearl Institutional Review Board (protocol number: #22-ADRW-147). Ethics approval was waived as this was a healthcare market research survey and data collection were in line with European Pharmaceutical Marketing Research Association guidelines.22 Each survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996.23
Measures
Data forms completed by physicians and patients were linked via a unique, pseudo-anonymized number. All information was recorded on the survey completion date from available medical records or designated recall periods for physicians and patients, with no follow-up data collected.
Physicians reported the level of disease burden and unmet needs including respiratory symptoms; exacerbation patterns; the level of COPD control based on physicians’ perception; their satisfaction with the current COPD control and whether they believed the best possible control was achieved; their perception of COPD severity (at initiation of current treatment and at the time of survey); and impact of COPD on daily lives. Additionally, physicians reported patients’ characteristics including demographics, comorbidities, asthma diagnosis, COPD-related characteristics and current treatment regimens. COPD-related characteristics included most recent blood eosinophil counts (BEC), lung function measured by post-bronchodilator (post-BD) forced expiratory volume in one second (FEV1) as a percentage of the predicted value (FEV1 [% predicted]), and Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification. Physicians also reported HCP involvement in the management of patients with COPD.
Patients self-reported the level of COPD control and impact of COPD on their daily lives using validated patient-reported outcome measures (PROMs), including the COPD Assessment Test (CAT; scores ranging from 0 to 40, with higher scores reflecting greater symptom severity), the European Quality of Life-5 Dimension-5 Level (EQ-5D-5L; Chinese-specific tariff; scores ranging from 0 to 1, with 0 representing worst imaginable health state and 1 representing best imaginable health state), the European Quality of Life-Visual Analogue Scale (EQ-VAS; scores ranging from 0 to 100, reflecting the worst to best imaginable health state), and work productivity and activity impairment (WPAI; four separate scores each ranging from 0 to 100, representing the percentage of work time missed or percentage impairment). Patients also reported their satisfaction with COPD control and their perception of disease control.
Data Analysis
Data were described using mean (standard deviation [SD]) or median (quartile [Q]1, Q3) for continuous variables and frequencies or percentages for categorical variables. Although this study was designed as a descriptive study, an exploratory bivariate analysis was performed to compare the outcomes between the two cohorts. Numerical variables were analyzed using Student’s t-test, categorical variables were analyzed using Fisher’s Exact test (Chi-squared test as an alternative when Fisher’s Exact could not be calculated) and ordered categorical variables were analyzed using Mann–Whitney U (non-parametric) test. A significance level of α = 0.05 was used, and all tests were two-sided. Missing data were handled as missing with no imputation performed. All analyses were conducted using Stata 19 (StataCorp. 2025. Stata Statistical Software: Release 19. College Station, TX, USA: StataCorp LLC).
Results
Patient Demographics and Clinical Characteristics
A total of 236 HCPs participated in the DSP and provided information on 844 patients with COPD. Among them, 135 patients received triple therapy for COPD treatment and were included in the current study, including 39 (28.9%) patients in the symptomatic SET cohort and 96 (71.1%) patients in the triple therapy cohort.
Patients in the triple therapy cohort had a mean (SD) age of 65.9 (9.0) years, with 61.5% being male. Patients in the symptomatic SET cohort had a mean (SD) age of 69.2 (8.7) years, with 94.9% being male. Former smokers were more prevalent in symptomatic SET cohort (triple therapy: 48.9%; symptomatic SET: 71.8%; p value <0.001). Hypertension was the most common cardiovascular comorbidity (triple therapy: 40.6%; symptomatic SET: 48.7%); diabetes without complications was found in 13.5% of patients in the triple therapy cohort and 25.6% of patients in the symptomatic SET cohort; diabetes with complications was found in 6.3% and 5.1% of patients in the two cohorts, respectively. Asthma-associated characteristics were present in 19.8% and 18.0% of patients in the triple therapy and symptomatic SET cohort, respectively. Results of BEC were available for 39 patients in the triple therapy cohort and 18 patients in the symptomatic SET cohort, of whom 23.1% in the triple therapy cohort and 27.8% in the symptomatic SET cohort had BEC ≥300 cells/μL (p = 0.777) (Table 1).
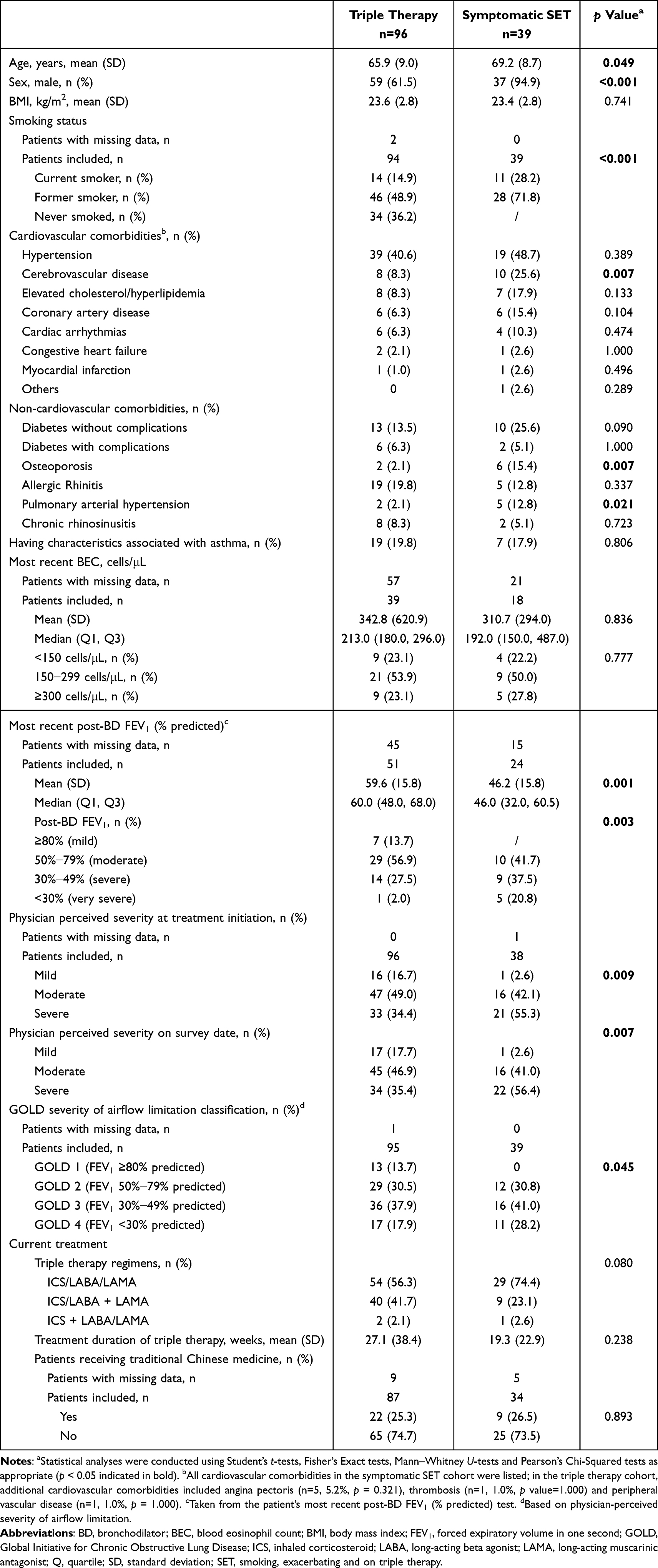 |
Table 1 Demographics and Clinical Characteristics |
Among the patients with lung function results available (triple therapy: n=51; symptomatic SET: n=24), median post-BD FEV1 (% predicted) was 60.0% in the triple therapy cohort and 46.0% in the symptomatic SET cohort (p = 0.001). In the triple therapy cohort, the percentages of patients with physician-perceived mild, moderate and severe COPD were 16.7%, 49.0% and 34.4%, respectively, at the time of current COPD treatment initiation and 17.7%, 46.9% and 35.4%, respectively, at the time of the survey date. In the symptomatic SET cohort, the percentages of physician-perceived mild, moderate and severe COPD were 2.6%, 42.1% and 55.3%, respectively, at the time of current COPD treatment initiation and 2.6%, 41.0% and 56.4%, respectively, at the time of the survey date. GOLD severity of airflow limitation (GOLD 1−4) based on physicians’ perception for both cohorts are also summarized in Table 1.
Fixed-dose ICS/LABA/LAMA was the most common regimen and was used in 56.3% of patients in the triple therapy cohort and 74.4% in the symptomatic SET cohort, followed by ICS/LABA plus a LAMA (triple therapy: 41.7%; symptomatic SET: 23.1%) and ICS plus LABA/LAMA (triple therapy: 2.1%; symptomatic SET: 2.6%). Mean (SD) duration of current triple therapy regimen was 27.1 (38.4) weeks for the triple therapy cohort and 19.3 (22.9) weeks for the symptomatic SET cohort. Additionally, traditional Chinese medicine was used in 25.3% and 26.5% of patients in the triple therapy and the symptomatic SET cohorts, respectively (Table 1). No significant differences between the two cohorts regarding the above treatment were observed (p ≥ 0.05).
COPD Symptoms Reported by Physicians and Exacerbations
According to physicians’ reports, the most frequent respiratory symptoms during the last four weeks prior to survey date and the most troublesome symptoms for both the triple therapy and the symptomatic SET cohorts are shown in Figure 1A and B. Wheezing (55.8%), shortness of breath during exertion/exercise (55.8%) and dry cough (44.2%) were the most frequently reported symptoms in the triple therapy cohort. In the symptomatic SET cohort, aside from productive cough/sputum (100%), wheezing (74.4%) and a tight feeling in the chest (51.3%) were the most frequently reported symptoms. Shortness of breath during exertion/exercise (19.2%) was reported as the most troublesome symptom in the triple therapy cohort and wheezing (43.6%) was reported as the most troublesome symptom in the symptomatic SET cohort. As shown in Figure 1C, 29.0% of patients in the symptomatic SET cohort and 7.7% of patients in the triple therapy cohort were reported to experience COPD symptoms every day during daytime hours (p < 0.001); symptom frequency was significantly higher in the symptomatic SET cohort compared to triple therapy cohort regardless of different observational period (p < 0.05 for all).
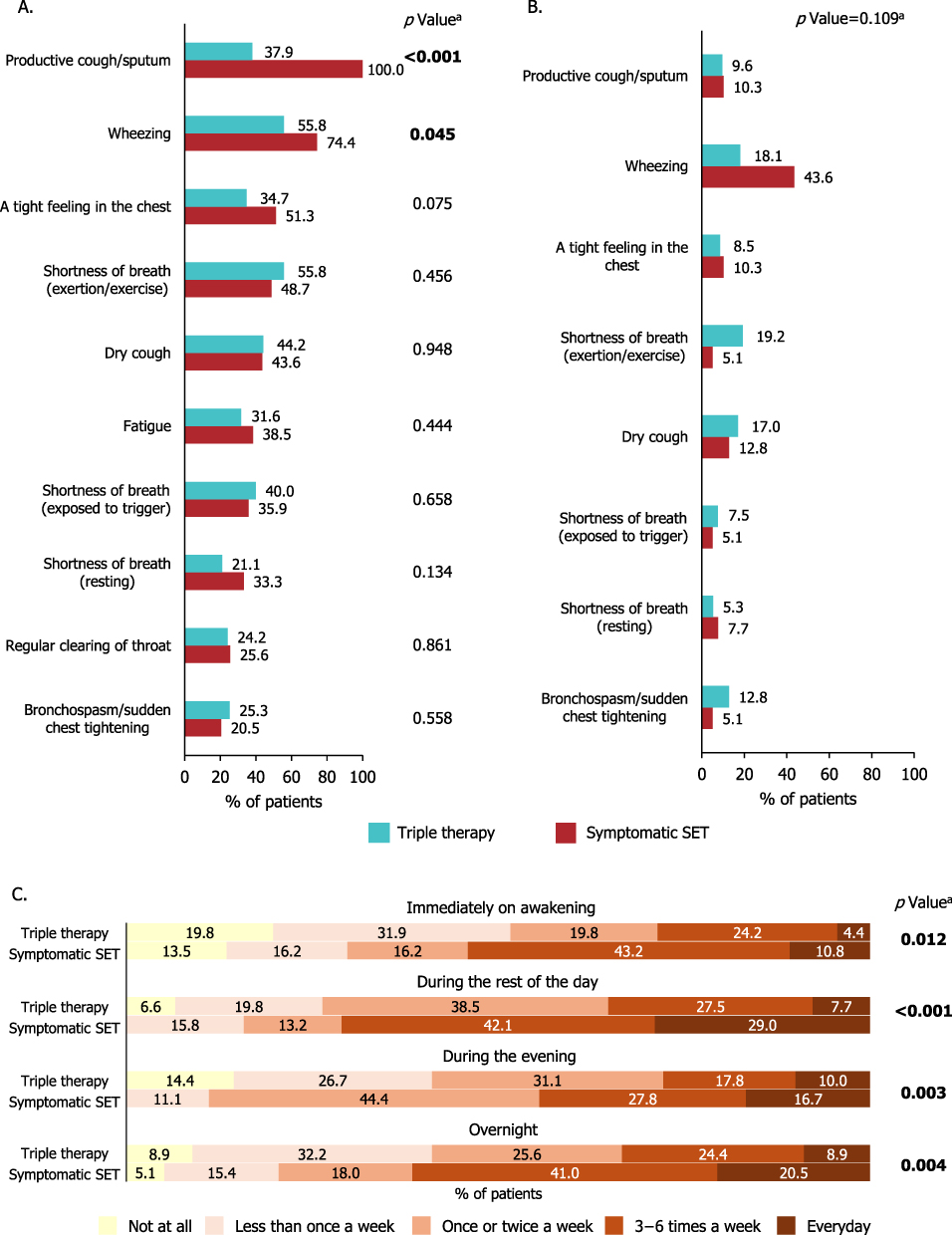 |
Figure 1 Respiratory symptoms reported by physicians for the patients in the triple therapy cohort and patients in the symptomatic SET cohort. (A) Frequently reported symptoms during the last four weeks prior to survey date; n=95 for triple therapy cohort and n=39 for symptomatic SET cohort. (B) Most troublesome symptoms; n=94 for triple therapy cohort and n=39 for symptomatic SET cohort. (C) Symptom frequency; immediately on awakening: n=91 for triple therapy cohort and n=37 for symptomatic SET cohort; during the rest of the day: n=91 for triple therapy cohort and n=38 for symptomatic SET cohort; during the evening: n=90 for triple therapy cohort and n=36 for symptomatic SET cohort; overnight: n=90 for triple therapy cohort and n=39 for symptomatic SET cohort. aStatistical analyses were conducted using Fisher’s Exact tests, Mann–Whitney U-tests and Pearson’s Chi-Squared tests as appropriate (p < 0.05 indicated in bold). Abbreviation: SET, smoking, exacerbating and on triple therapy. |
Table 2 summarizes key aspects of the patients’ exacerbation profiles during the last 12 months. In the triple therapy cohort, mean (SD) number of exacerbations in the last 12 months was 1.3 (1.4) and 35.4% of patients were free of exacerbation. In the symptomatic SET cohort, mean (SD) number of exacerbations during the last 12 months was 2.3 (1.3), with 30.8%, 33.3%, 17.9% and 17.9% of patients experiencing an exacerbation once, twice, three times and four or more times, respectively. The exacerbation profile was significantly different between the two cohorts (p <0.001). Changes in weather/climate were considered the most common exacerbation trigger for both cohorts. Physicians perceived that the significantly higher proportion of patients in the symptomatic SET cohort (87.2%) had high future exacerbation risks compared with patients in the triple therapy cohort (58.3%) (p = 0.001).
 |
Table 2 COPD Exacerbations |
COPD Control Status
According to physicians’ perception, 2.6%, 28.2% and 38.5% of patients had completely controlled, well controlled and somewhat controlled COPD in the symptomatic SET cohort, respectively, while the corresponding percentages were 7.3%, 50.0% and 27.1% in the triple therapy cohort. The proportions of patients perceived by physicians as having poorly controlled and uncontrolled COPD were 28.2% and 2.6%, respectively, in symptomatic SET cohort, and 13.5% and 2.1%, respectively, in the triple therapy cohort (Figure 2A). The physician perceived COPD control between the two cohorts was significantly different (p = 0.005).
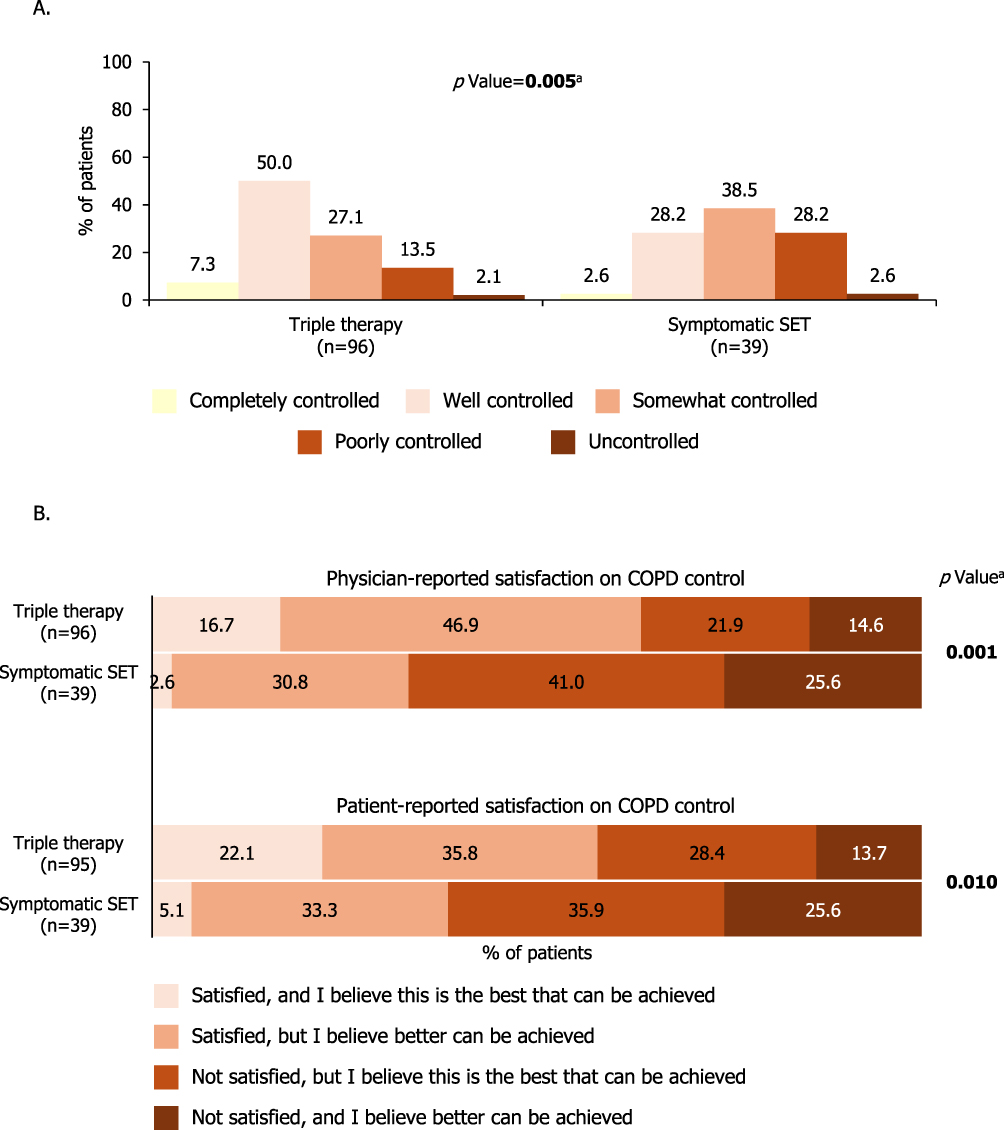 |
Figure 2 Physician perceived COPD control and physician- and patient-reported satisfaction with COPD control. (A) Physician perceived COPD control during the last four weeks prior to survey date. (B) Physician- and patient-reported satisfaction on COPD control. aStatistical analyses were conducted using Mann–Whitney U-tests (p < 0.05 indicated in bold). Abbreviations: COPD, chronic obstructive pulmonary disease; SET, smoking, exacerbating and on triple therapy. |
Physicians’ and patients’ satisfaction with the level of COPD control are reported for both cohorts in Figure 2B. Physicians and patients were more unsatisfied with COPD control in the symptomatic SET cohort compared to the triple therapy cohort. For instance, physicians were not satisfied with the level of COPD control and believed that better control could be achieved for 25.6% of patients in the symptomatic SET cohort and 17.8% of patients in the triple therapy cohort; and physicians were not satisfied but believed that the best possible control was achieved for 41.0% of patients in the symptomatic SET cohort and 27.4% of patients in the triple therapy cohort (p = 0.001). Patients’ satisfaction with COPD control showed a similar pattern with those of physicians and there was significant difference between the two cohorts (p = 0.010).
Impact of COPD on Daily Lives and HRQoL
Physician-reported impact of COPD on patients’ daily lives is shown in Figure 3. Large proportions of patients in the symptomatic SET cohort frequently or constantly experienced impacts of COPD on their daily lives compared to patients in the triple therapy cohort; exercise, mood and sleep were the most frequently impacted domains.
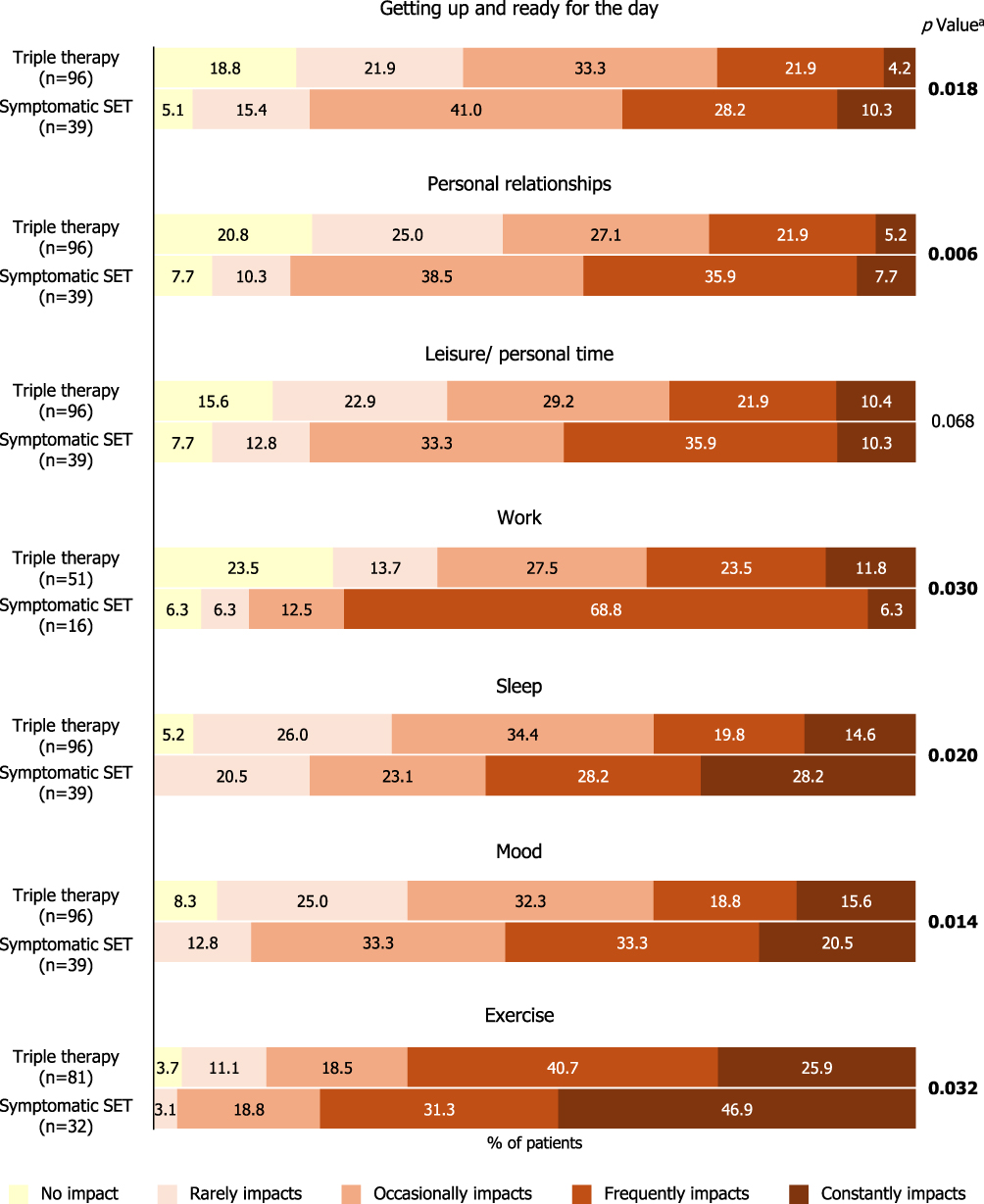 |
Figure 3 Impact of COPD on daily lives during the last four weeks. aStatistical analyses were conducted using Mann–Whitney U-tests (p < 0.05 indicated in bold). Abbreviations: COPD, chronic obstructive pulmonary disease; SET, smoking, exacerbating and on triple therapy. |
Patient-reported outcomes of HRQoL (CAT, EQ-5D-VAS, EQ-5D-5L and WPAI scores) in the triple therapy and symptomatic SET cohorts are summarized in Table 3. Among patients with data available (triple therapy: n=95; symptomatic SET: n=39), mean (SD) CAT score was 25.7 (7.1) in the symptomatic SET cohort and 21.0 (8.3) in the triple therapy cohort. For the CAT cough domain, 94.9% of patients in the symptomatic SET cohort and 93.7% of patients in the triple therapy cohort reported a score ≥2. For the CAT phlegm/sputum domain, 92.3% in the symptomatic SET cohort and 82.1% of patients in the triple therapy cohort reported a score ≥2. Mean (SD) EQ-5D-VAS and EQ-5D-5L scores were 57.1 (15.8) and 0.6 (0.3), respectively, in the symptomatic SET cohort, and 61.9 (17.0) and 0.7 (0.2) in the triple therapy cohort. Among the limited patients with WPAI data available, work impact was notably severe in patients in the symptomatic SET cohort.
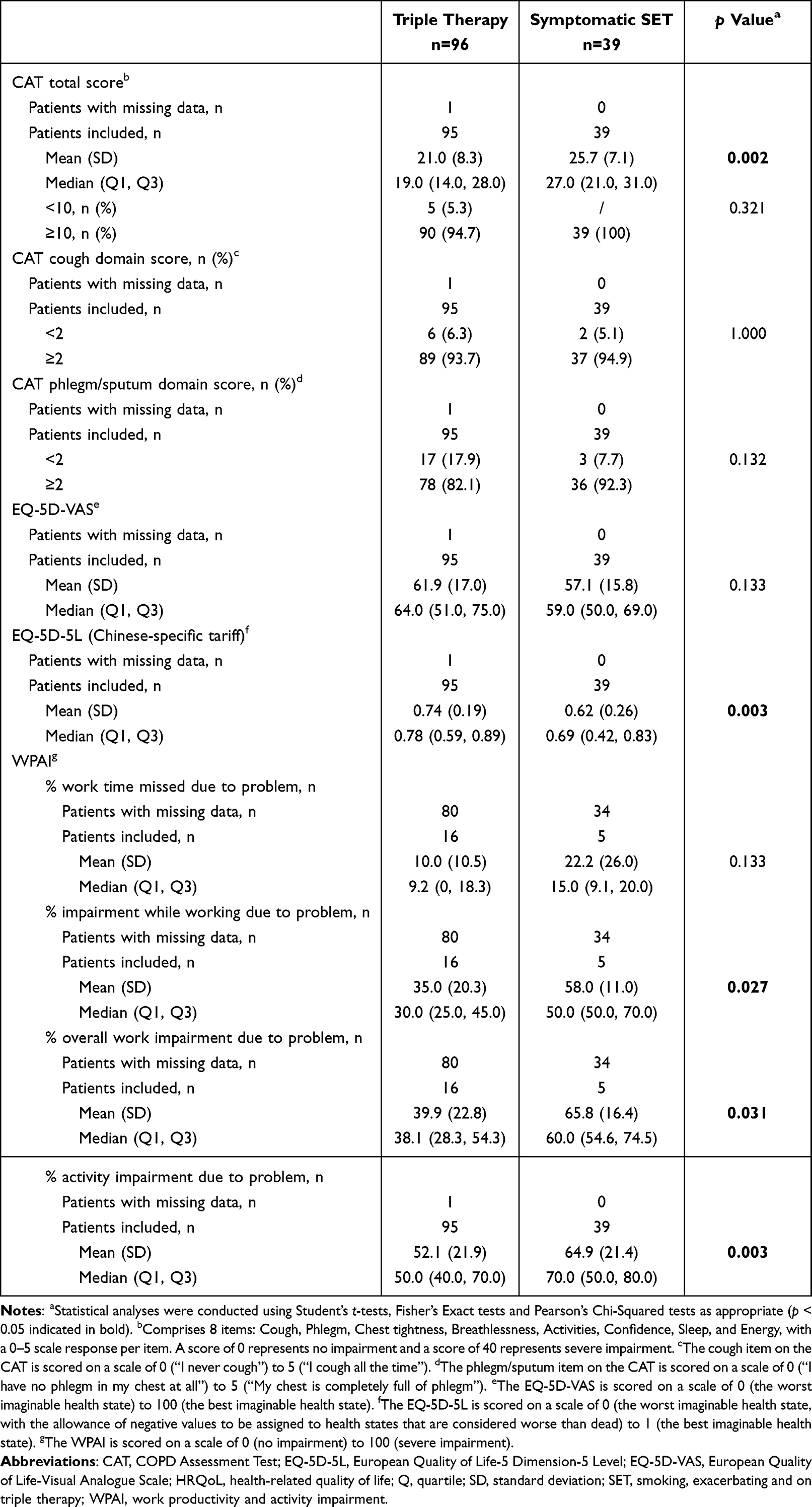 |
Table 3 Patient-Reported HRQoL |
Physician Involvement and HCRU
Mean (SD) number of patient visits to HCPs during the last 12 months was 6.5 (3.6) in the triple therapy cohort and 7.1 (3.8) in the symptomatic SET cohort. In both cohorts, respiratory specialists were the most common HCPs visited by patients for initial consultation, diagnosis of COPD, maintenance treatment initiation and current treatment decision (Table 4).
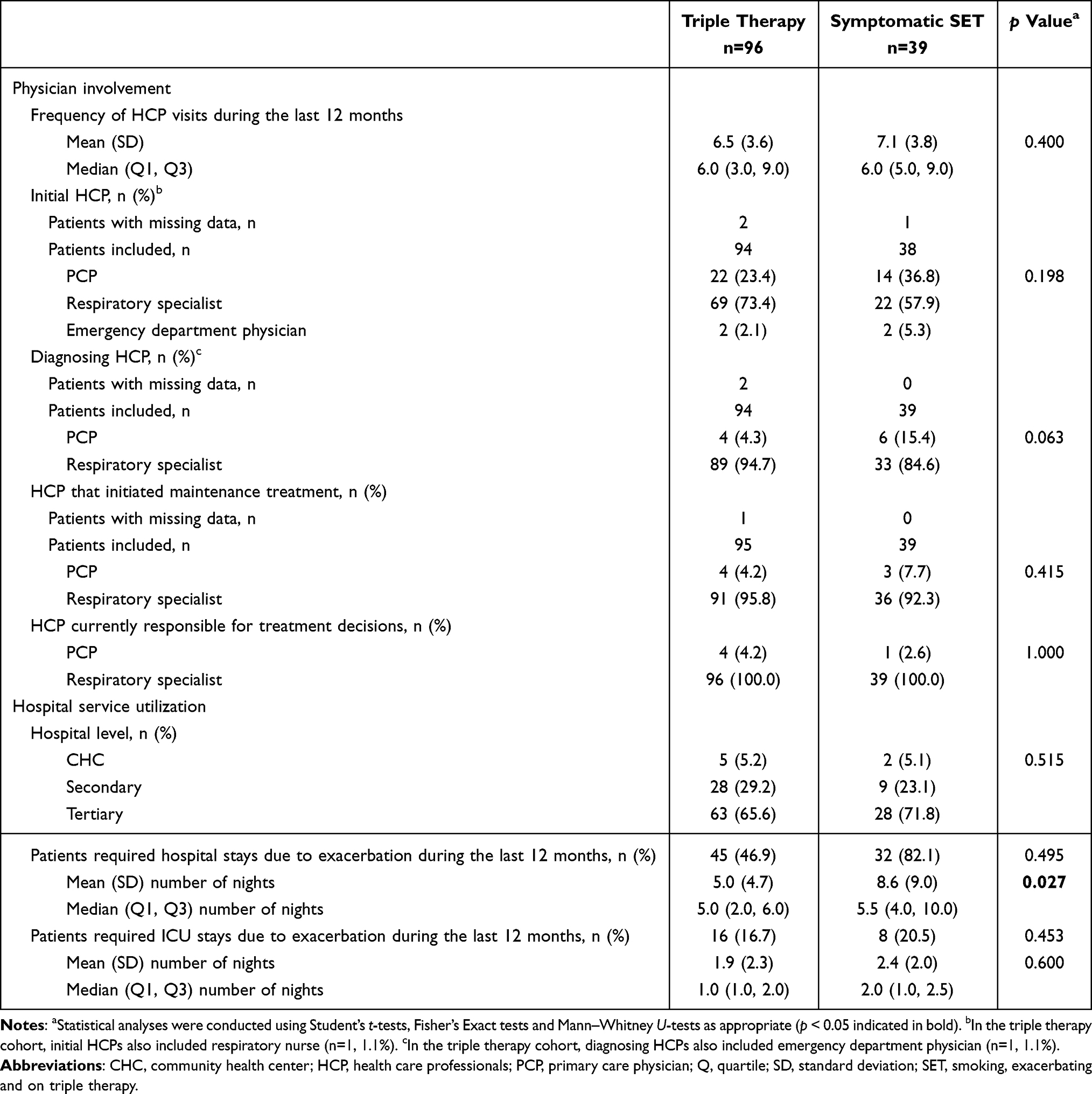 |
Table 4 Physician Involvement and Health Care Resource Utilization |
Tertiary hospitals were the most frequently visited hospitals for both the triple therapy (65.6%) and symptomatic SET (71.8%) cohorts, followed by secondary hospitals (triple therapy: 29.2%; symptomatic SET: 23.1%) and community health centers (CHCs, triple therapy: 5.2%; symptomatic SET: 5.1%). In the triple therapy cohort (n = 96), 45 (46.9%) patients required hospital stays and 16 (16.7%) patients required intensive care unit (ICU) stays as a result of COPD exacerbations during the last 12 months; mean (SD) numbers of nights spent in hospital and ICU due to exacerbations were 5.0 (4.7) and 1.9 (2.3), respectively. In the symptomatic SET cohort (n = 39), 32 (82.1%) and 8 (20.5%) patients required hospital and ICU stays, respectively, due to COPD exacerbations during the last 12 months; mean (SD) numbers of nights spent in hospital and ICU due to exacerbations were 8.6 (9.0) and 2.4 (2.0), respectively (Table 4).
Discussion
This cross-sectional real-world study identified and characterized a subpopulation of patients in China who had a history of smoking and experienced COPD symptoms and exacerbations while receiving triple inhaled therapy. Results of this study revealed that even with the highest-level inhaled treatment of triple therapy, these patients were still suffering from substantial disease burden from COPD, as reflected by the heavy symptom burden and high exacerbation frequencies. Considerable unmet needs concerning suboptimal disease control were revealed, as both physicians and patients reported low levels of satisfaction with COPD control. Poor HRQoL and detrimental impact on daily lives and work productivity were observed. These patients also experienced high numbers of HCRU events, indicating a high economic burden.
This study identified that among all patients with COPD receiving triple therapy, 28.9% (39/135) had a history of smoking and experienced COPD symptoms and exacerbations. This percentage is numerically comparable to the 33.1% (399/1205) in the global cohort of this DSP.17 However, it has to be pointed out that only 16.0% (135/844) of patients in the current study were receiving triple therapy, numerically lower than the 27.6% in the global DSP cohort and the 43.0% reported in a similar study conducted in the UK.11,17 The relative low usage of triple therapy among all patients with COPD in China was further supported by a recent multicentre, observational study (17.7%, 417/2358).8 Such low usage of triple therapy might reflect poor implementation of guideline-directed medical therapy (GDMT) and suboptimal disease management within the country.8 Considering that triple therapy is primarily used as an escalation treatment instead of initial treatment in real-world clinical settings in China,24 patients who are not adequately treated with dual therapies might not be accurately identified by physicians during their routine clinical visits, which requires a careful assessment of exacerbation histories as well as blood eosinophil levels, and thus not receiving triple therapy. Indeed, only 40.6% (39/96) of patients in the triple therapy cohort had BEC results available; the suboptimal testing rate of BEC may potentially limit the number of patients who are being escalated to triple therapy. Medication accessibility may also be an underlying reason, while triple therapy is increasingly available in tertiary hospitals, its access in community health center or secondary hospitals might still be limited. Economic considerations may also play a role in the low usage of triple therapy, as patients may opt for lower-cost therapies instead of triple therapy to reduce financial burden.
High symptom frequency was observed, with 29.0% of patients in the symptomatic SET cohort and 7.7% of patients in the triple therapy cohort experiencing COPD symptoms during the day every day. Symptomatic SET patients in the current study had 2.3 exacerbations on average in the 12 months prior to survey date, significantly higher than that in the triple therapy cohort (averaged 1.3 exacerbations) in the same time frame. Although RCTs such as IMPACT and ETHOS have reported the efficacy of triple inhaled therapy in reducing exacerbations,25,26 physicians still perceived 87.2% of patients in the symptomatic SET cohort as having high future exacerbation risks, significantly higher than that perceived in the triple therapy cohort. This result suggests that triple therapy may be either ineffective or at least inadequate for preventing future exacerbations in patients in the symptomatic SET cohort. It was noteworthy that, despite the fact that all patients in the symptomatic SET cohort were symptomatic and experienced exacerbations, physicians considered that almost 70% of patients had at least somewhat controlled COPD (completely controlled: 2.6%; well controlled: 28.2%; somewhat controlled: 38.5%); this overestimation of COPD control may hinder the treatment escalation in these patients, resulting in under-treatment that in turn adds to the overall disease burden. Taken together, these results indicate notably heavy disease burden and substantial unmet needs among the patients in the symptomatic SET cohort in China, mirroring the findings from the global cohort of this DSP.17
Several real-world studies have reported significant improvement in PROMs, including CAT scores and measurements of HRQoL, after the treatment with triple therapy among patients with COPD.27–30 However, few studies have examined these PROMs specifically among patients who experienced symptoms and frequent exacerbations while receiving triple therapy,12,17 especially in China. In the current study, all patients in the symptomatic SET cohort had CAT scores ≥10 with a mean (SD) score of 25.7 (7.1), and these patients exhibited poor HRQoL including impairment in work and activity, with numerous aspects of daily lives such as sleep, mood and exercise all affected. These results are consistent with prior research, which has revealed elevated CAT scores in patients with frequent exacerbations31 and has highlighted the significant, deleterious effects that COPD exacerbations have on HRQoL, particularly with regard to activity impairment and mental health.32 As such, results from the current study comprehensively demonstrate the impairment of COPD on health status from the patients’ perspective, highlighting the unmet need for improvement in the wellbeing of those experiencing symptoms and exacerbations while receiving triple therapy in China.
Heavy disease burdens of COPD represent a large component of socioeconomic burden.9 In the current study, the incidence of HCRU events was notably high for patients in the symptomatic SET cohort: 82.1% and 20.5% of patients required hospital and ICU stays due to exacerbations, respectively. In line with these findings, an observational study in the UK reported a substantially higher number of HCRU events in patients who experienced exacerbations despite receiving maximal triple inhaled therapy compared to the overall patients with COPD.11 Considering the large number of patients with COPD in China, the overall costs associated with HCRU among these symptomatic SET patients is expected to be significantly high.
Findings from our study reinforce the notion that triple inhaled therapy may not provide adequate treatment for patients who experience symptoms and exacerbations while on triple therapy, highlighting the urgent need for novel therapeutic options.11,33 Previous studies have proposed that eosinophil-targeting biologics may be a promising treatment option, as eosinophilic inflammation might be associated with inadequate responses to triple therapy.11,33 However, it should be pointed out that in the current study, only 27.8% of patients in the symptomatic SET cohort had BEC ≥300 cells/μL, statistically comparable with the 23.1% reported in the triple therapy cohort. The relatively small number of patients with BEC results available may have limited the interpretation of this result in our study. Interestingly, a previous global study also reported similar results: among patients receiving triple therapy and had historical moderate/severe exacerbations during past one year, 33.5% of them had BEC ≥300 cells/μL.33 While patients with high BEC may be good candidates for eosinophil-targeting biologics, it remains unknown whether such biologics represent the best treatment option for those without elevated BEC. Epithelial-derived alarmins, on the other hand, are upstream regulators of both type 2 (T2)-high and T2-low immune responses in airway inflammation.14 Biologics targeting alarmins (including TSLP and IL-33) might serve as an alternative treatment option,14 facilitating a more tailored therapeutic strategy based on eosinophilic phenotypes.13
While awaiting the advent of more efficacious treatment options, there are other aspects in the comprehensive management of COPD that can be enhanced. For example, non-pharmacological treatment as outlined in the GOLD recommendations is a key part of COPD management and needs to be strengthened:7 In the current study, 28.2% of the symptomatic SET patients were current smokers, highlighting a need for patient education and assistance in smoking cessation. Viral infection was one of the most common exacerbation triggers, reported in 52.6% of the symptomatic SET patients in this study; vaccination against common respiratory viruses should therefore be offered as part of COPD management. Moreover, multidisciplinary management and multiple treatment modalities on both symptoms and emotions together with holistic assessment are also recommended.34 Also noteworthy is the deviation from GDMT observed in the current study, as around one-fourth of patients received traditional Chinese medicine. In fact, discrepancies between the real-world treatment patterns and the GDMT were also reported in a recent nationwide, multicentre study in China, highlighting a need for improvement in standardization of disease management.8
This study had several limitations. Firstly, participation of Adelphi COPD DSP surveys was influenced by physicians’ willingness to complete the surveys and minimum physician exclusion criteria were employed, resulting in potential physician selection bias. Patient selection bias was also possible, as patient enrolment relied on physicians’ subjective judgement and clinical perception rather than standardized diagnostic codes. To mitigate the patient selection bias, each physician was required to enrol their next five consecutively consulting eligible patients; however, this non-random sampling method limits the broader generalizability of the findings. Secondly, the retrospective nature of this study may have introduced recall bias from the patient. In order to minimize the recall bias, data were collected at the time of each patient’s consultation and physicians were able to refer to patients’ medical records while completing the patient record forms. Thirdly, missing data were not imputed, resulting in varying patient numbers in some analyses. For example, the numbers of patients with available spirometry or BEC results were small, and results of these outcomes should be considered exploratory and warrant further investigation in larger clinical studies. Fourthly, the symptoms required for inclusion in the symptomatic SET cohort, namely frequent productive cough and sputum (in the four weeks preceding survey date), were physician-reported and based on medical records instead of objective measures such as modified Medical Research Council (mMRC) Dyspnea Scale. Similarly, several outcomes in the current study (the assessment of COPD control, COPD symptoms and impact of COPD on patients’ daily activity during the last four weeks) were determined by physician’s clinical understanding of the patient’s condition. Consequently, these results may be influenced by physician’s subjectivity. Nevertheless, these subjective judgements by physicians served as the primary driver for treatment adjustment and reflected the real-world clinical decision-making. Lastly, comorbid bronchiectasis was not assessed. Despite the above-mentioned limitations, real-world studies are pivotal in highlighting areas of concern that are not addressed in clinical trials. Patients included in clinical trials represent a small proportion of the consulting population due to age restrictions and failure to meet stringent eligibility criteria. In contrast, patients treated in the real-world setting encompassing a more heterogeneous spectrum of patients and as a result, data from real-world studies serve as a vital complement to clinical trials and provide insight into the effectiveness of interventions in a broad patient population in routine clinical practice.
Conclusions
This study demonstrated the presence of a subpopulation of patients in China who experienced COPD symptoms and frequent exacerbations while receiving the highest level of inhaled treatment with triple therapy. These patients had heavy disease and socioeconomic burden and large unmet needs, highlighting a need for more effective treatment options. These patients may benefit from novel biologics based on tailored therapeutic strategies, together with an improvement in guideline-directed disease management approaches.
Data Sharing Statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://www.astrazenecaclinicaltrials.com/our-transparency-commitments/.
Data for studies directly listed on Vivli can be requested through Vivli at www.vivli.org. Data for studies not listed on Vivli could be requested through Vivli at https://vivli.org/members/enquiries-about-studies-not-listed-on-the-vivli-platform/. AstraZeneca Vivli member page is also available outlining further details: https://vivli.org/ourmember/astrazeneca/.
Ethics Approval and Informed Consent
This study was submitted to the Pearl Institutional Review Board (protocol number: #22-ADRW-147). Ethics approval was waived as this was a healthcare market research survey. Written informed consent was obtained from all participating patients during the survey.
Acknowledgments
The authors thank Shuyi Wang, PhD, from Costello Medical (Shanghai) and Bo Lyu, PhD, from Costello Medical (Singapore) for medical writing support and editorial assistance, funded by AstraZeneca China, and complied with international guidelines for Good Publication Practice (GPP 2022).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by AstraZeneca China. AstraZeneca China was involved in the study design, data collection, data analysis, and preparation of the manuscript.
Disclosure
TP and FB are employees of Adelphi Real World.
The abstract of this paper was presented at the 2025 European Respiratory Society Congress as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in European Respiratory Journal: https://doi.org/10.1183/13993003.congress-2025.PA2555.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–17. doi:10.1016/S0140-6736(22)00470-6
2. Soriano JB, Kendrick PJ, Paulson KR; Collaborators GBDCRD. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China pulmonary health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Advancing COPD care in China through a comprehensive approach. Available from: https://www.who.int/news-room/feature-stories/detail/advancing-copd-care-in-china-through-a-comprehensive-approach.
5. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
6. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
7. Global strategy for prevention, diagnosis and management of COPD: 2024 report. Available from: https://goldcopd.org/wp-content/uploads/2024/02/GOLD-2024_v1.2-11Jan24_WMV.pdf.
8. Yang T, Cai B, Cao B, et al. REALizing and improving management of stable COPD in China: results of a multicentre, prospective, observational study (REAL). Ther Adv Respir Dis. 2023;17:17534666231178692. doi:10.1177/17534666231178692
9. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
10. Alcazar-Navarrete B, Garcia-Rio F, Sanchez G, et al. Burden of disease among exacerbating patients with COPD treated with triple therapy in Spain. Int J Chron Obstruct Pulmon Dis. 2021;16:2149–2161. doi:10.2147/COPD.S310319
11. Chen S, Miravitlles M, Rhee CK, et al. Patients with chronic obstructive pulmonary disease and evidence of eosinophilic inflammation experience exacerbations despite receiving maximal inhaled maintenance therapy. Int J Chron Obstruct Pulmon Dis. 2022;17:2187–2200. doi:10.2147/COPD.S378649
12. Chen S, Small M, Lindner L, Xu X. Symptomatic burden of COPD for patients receiving dual or triple therapy. Int J Chron Obstruct Pulmon Dis. 2018;13:1365–1376. doi:10.2147/COPD.S163717
13. Appleton LK, Hanania NA, Adrish M. Personalized COPD Care: the Future of Precision-Based Therapies. J Clin Med. 2024;13(21):6339. doi:10.3390/jcm13216339
14. Varricchi G, Poto R. Towards precision medicine in COPD: targeting type 2 cytokines and alarmins. Eur J Intern Med. 2024;125:28–31. doi:10.1016/j.ejim.2024.05.011
15. Huang WC, Chen CY, Liao WC, et al. A real world study to assess the effectiveness of switching to once daily closed triple therapy from Mono/Dual combination or open triple therapy in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1555–1568. doi:10.2147/COPD.S308911
16. Lin L, Song Q, Cheng W, et al. Impact of exacerbation history on future risk and treatment outcomes in chronic obstructive pulmonary disease patients: a prospective cohort study based on global initiative for chronic obstructive lung disease (GOLD) A and B classifications. J Glob Health. 2024;14:04202. doi:10.7189/jogh.14.04202
17. De Soyza A, Nordon C, Coak E, et al. Clinical burden of people with symptomatic and exacerbating COPD while on triple inhaled therapy. J Clin Med. 2025;14(18):6488. doi:10.3390/jcm14186488
18. Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes - a means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. doi:10.1185/03007990802457040
19. Anderson P, Higgins V, Courcy J, et al. Real-world evidence generation from patients, their caregivers and physicians supporting clinical, regulatory and guideline decisions: an update on disease specific programmes. Curr Med Res Opin. 2023;39(12):1707–1715. doi:10.1080/03007995.2023.2279679
20. Babineaux SM, Curtis BH, Holbrook T, Liu L, Colclough H, Piercy J. Evidence for validity of a national physician and patient-reported survey in China and United Kingdom: the disease specific programme. Value Health. 2014;17(7):A728. doi:10.1016/j.jval.2014.08.065
21. Higgins V, Piercy J, Roughley A, et al. Trends in medication use in patients with type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab Syndr Obes. 2016;9:371–380. doi:10.2147/DMSO.S120101
22. European Pharmaceutical Market Research Association. Code of Conduct 2022. Available from: https://www.ephmra.org/sites/default/files/2022-08/EPHMRA%202022%20Code%20of%20Conduct.pdf.
23. US Department of Health and Human Services. Summary of the HIPAA privacy rule. Available from: https://www.hhs.gov/sites/default/files/privacysummary.pdf.
24. Chen Y, Li X, Hou D, et al. Treatment patterns and triple therapy utilization in Chinese patients with chronic obstructive pulmonary disease: an analysis of real-world data from the Yinzhou database. Int J Chron Obstruct Pulmon Dis. 2025;20:2659–2670. doi:10.2147/COPD.S499783
25. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
26. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
27. Tabberer M, Jones CE, Kilbride S, et al. Single-inhaler triple therapy and health-related quality of life in COPD: the IMPACT study. Adv Ther. 2020;37(9):3775–3790. doi:10.1007/s12325-020-01409-8
28. Gessner C, Trinkmann F, Bahari Javan S, et al. Effectiveness of extrafine single inhaler triple therapy in chronic obstructive pulmonary disease (COPD) in Germany - the TriOptimize study. Int J Chron Obstruct Pulmon Dis. 2022;17:3019–3031. doi:10.2147/COPD.S382405
29. Richeldi L, Schino P, Bargagli E, et al. TRITRIAL: the impact of fixed triple therapy with Beclometasone/Formoterol/Glycopyrronium on health status and adherence in chronic obstructive pulmonary disease in an italian context of real life. Int J Chron Obstruct Pulmon Dis. 2024;19:475–487. doi:10.2147/COPD.S445858
30. Sudi A, Santa B, Horvath A, et al. The real-world efficacy of fixed triple inhalation therapy in the treatment of moderate COPD patients (RATIONALE study). Int J Chron Obstruct Pulmon Dis. 2024;19:1943–1955. doi:10.2147/COPD.S474354
31. Varol Y, Ozacar R, Balci G, Usta L, Taymaz Z. Assessing the effectiveness of the COPD Assessment Test (CAT) to evaluate COPD severity and exacerbation rates. COPD. 2014;11(2):221–225. doi:10.3109/15412555.2013.836169
32. Hurst JR, Skolnik N, Hansen GJ, et al. Understanding the impact of chronic obstructive pulmonary disease exacerbations on patient health and quality of life. Eur J Intern Med. 2020;73:1–6. doi:10.1016/j.ejim.2019.12.014
33. Benson VS, Pascoe KC, Siddall J, Small M, Mullerova H. Exacerbation frequency and eosinophil counts among patients with COPD currently prescribed triple therapy. Int J Chron Obstruct Pulmon Dis. 2019;14:2711–2723. doi:10.2147/COPD.S217503
34. Fu Y, Chapman EJ, Boland AC, Bennett MI. Evidence-based management approaches for patients with severe chronic obstructive pulmonary disease (COPD): a practice review. Palliat Med. 2022;36(5):770–782. doi:10.1177/02692163221079697
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.