Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Disease Awareness, Care-Seeking Behavior, and Symptom Burden Among Japanese Patients with Generalized Anxiety Disorder: Results from a Web-Based Questionnaire of Clinical Trial Participants
Authors Nomoto K ![]() , Otsubo T, Misago R, Higa S
, Otsubo T, Misago R, Higa S ![]()
Received 9 December 2025
Accepted for publication 5 February 2026
Published 24 February 2026 Volume 2026:22 582812
DOI https://doi.org/10.2147/NDT.S582812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Keisuke Nomoto,1 Tempei Otsubo,2 Rikiya Misago,1 Shingo Higa1
1Medical Affairs, Viatris Pharmaceuticals Japan G.K., Tokyo, Japan; 2Department of Psychosomatic and Psychiatric Medicine, Tokyo Women’s Medical University Adachi Medical Center, Tokyo, Japan
Correspondence: Keisuke Nomoto, Medical Affairs, Viatris Pharmaceuticals Japan G.K., Azabudai Hills Mori JP Tower 1-3-1 Azabudai, Minato-ku, Tokyo, 106-0041, Japan, Tel +81 3 5656 0400, Email [email protected]
Purpose: This study was conducted among Japanese patients with generalized anxiety disorder (GAD) who had participated in a clinical trial to investigate their level of disease awareness, past medical care-seeking behavior and diagnoses, symptoms and impact on daily life, perceptions of diagnosis and clinical assessment, and changes after trial participation. The patients’ first-hand experiences related to symptoms and disease burden were collected through open-ended responses.
Patients and Methods: This was a quantitative (descriptive observational) study using a web-based questionnaire conducted from April 23 to May 25, 2025. Patients diagnosed with GAD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, and previously enrolled in Study B2411367, a clinical trial of venlafaxine, a serotonin-norepinephrine reuptake inhibitor, were eligible.
Results: Data from 98 respondents were analyzed. The most frequently reported GAD symptoms at trial entry included excessive anxiety or worry (99.0%), becoming fatigued easily (86.7%), and sleep problems (82.7%). Over half of respondents (53.1%) identified work or studying as the most affected area of daily life, describing impaired concentration, reduced efficiency, and physical strain. Regarding disease awareness, 72.4% of respondents had never heard of GAD and 71.4% attributed their anxiety to their personality. Only 11.2% had sought medical care before trial participation, with depression being the most frequent diagnosis (36.4%) and only 9.1% having been diagnosed with GAD.
Conclusion: Many patients with GAD were unaware of the disease name before trial entry and had symptoms that impacted daily life. The patients’ first-hand accounts provided deeper insight into their burden. The findings highlight the unmet needs among Japanese patients with GAD who participated in a clinical trial and the situation of low public disease awareness and limited recognition in clinical settings. Efforts to increase awareness of GAD may help facilitate earlier diagnosis and broaden access to appropriate treatment.
Clinical Trial Registration: UMIN000057689.
Keywords: generalized anxiety disorder, awareness, Japan, questionnaire, patient, burden
Introduction
Generalized anxiety disorder (GAD) is characterized by chronic, excessive, uncontrollable anxiety and worry about various aspects of daily life, such as finances, family, health, and the future.1 The disorder is often associated with nonspecific mental and physical symptoms,1 which impair the patient’s health-related quality of life (HRQoL) and daily functioning.2,3 GAD is primarily diagnosed according to the criteria provided in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), which specifies excessive anxiety and worry lasting ≥ 6 months, along with symptoms such as fatigue, difficulty concentrating, and sleep disturbance.1,4,5 The functional impact of these symptoms is a core feature of the disorder, as reflected in diagnostic criteria that specify significant difficulties in social activities, work, or other major areas of life.5 Previous studies have shown that individuals with GAD frequently experience reduced work productivity, impaired social functioning, and difficulties in daily life, even in the absence of overt psychiatric comorbidity.2,6,7
The lifetime prevalence of GAD is estimated to be 3.7% worldwide and 2.6% in Japan.6,8 According to a patient survey conducted by the Japanese Ministry of Health, Labour and Welfare, the number of Japanese patients being treated for GAD in 2023 was estimated to be 170,000.9 Considering that over 3,000,000 Japanese people may have GAD based on the prevalence in Japan (2.6%), the estimate provided by the Japanese Ministry of Health, Labour and Welfare suggests that only a very small percentage of Japanese patients with GAD are being diagnosed and treated for the disease.
Limited awareness of GAD is likely a factor in its under-diagnosis and low rates of care-seeking in Japan.2,7 A recent study of patients with probable GAD in Japan showed that many patients do not recognize that their condition constitutes an illness, and when they did seek medical care, the psychiatric diagnoses they had received were depression (26.9%), panic disorder (8.8%), and social anxiety disorder (5.4%), with only 4.0% being diagnosed with GAD.2 These data suggest limited awareness of GAD by Japanese patients and healthcare providers, which may limit opportunities for GAD patients to receive appropriate care.
Beyond awareness and diagnosis, relatively little is known about how Japanese patients with GAD perceive their symptoms, functional burden, and diagnostic experiences, particularly among patients participating in clinical trials. While symptom severity and treatment efficacy are commonly assessed in such trials, fewer studies have examined patients’ perspectives regarding symptom impact on daily functioning, motivations for participating in clinical research, or perceptions of diagnostic evaluation and clinical assessment. Similarly, patient-reported changes following trial participation, including symptoms, behaviors, and satisfaction with the trial, remain underexplored.
European guidelines and a US clinical review on the management of GAD recommend psychotherapy (eg, cognitive behavioral therapy) and pharmacological treatment with a selective serotonin reuptake inhibitor (SSRI) or serotonin-norepinephrine reuptake inhibitor (SNRI) as first-line treatment.10,11 Venlafaxine is an SNRI approved in Japan for the treatment of depression. To evaluate its efficacy and safety as a potential treatment for GAD, a multicenter, randomized, double-blind, placebo-controlled Phase 3 study (study identifier: B2411367; hereafter “Study B2411367”) of Japanese patients diagnosed with GAD according to the DSM-5 criteria was initiated in 2022. This trial was completed in 2024 after enrolling 357 Japanese patients treated at outpatient clinics.12
Study B2411367 demonstrated the efficacy and safety of venlafaxine, supporting its treatment potential in Japan. However, addressing the limited awareness of GAD in Japan would aid in expanding the real-world benefits of treatment. Gaining insight into how patients perceive their own symptoms, burden, and path to receiving treatment may help raise awareness among patients and healthcare providers by informing strategies to support earlier diagnosis and treatment. Furthermore, understanding patients’ medical care-seeking behavior could guide the establishment of support systems to help patients seek medical care and receive appropriate diagnosis and treatment.
Thus, the present study was conducted as a quantitative assessment of Japanese patients with GAD enrolled in Study B2411367 to investigate their motivation for trial participation, awareness of GAD, medical care-seeking behavior and past diagnoses, symptoms present at trial entry and their impact on daily life, perceptions of diagnosis and assessment, changes after trial participation including their physical and mental symptoms, behavior, and challenges, and satisfaction with the clinical trial. This study has a robust scientific rationale in that it collected data directly from patients with a confirmed diagnosis of GAD based on DSM-5 criteria using a structured diagnostic interview, ensuring that the obtained insights are derived from well-characterized cases.
Materials and Methods
Study Design
This was a quantitative (descriptive observational) study using a web-based questionnaire. Participants were patients with GAD who had been enrolled through a clinical trial information website maintained by 3H Medi Solution Inc. (Seikatsu-Kojo WEB) in Study B2411367, a multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of venlafaxine conducted from August 2022 to July 2024. 3H Medi Solution Inc. recruited the participants for the present study, and consenting patients completed a web-based questionnaire online. The study period was from April 23 to May 25, 2025.
Study Population
Japanese patients with GAD who had participated in Study B2411367 and who voluntarily gave electronic informed consent were eligible for this study; no exclusion criteria were specified. To participate in Study B2411367, patients were required to have been diagnosed with GAD according to the DSM-5 diagnostic criteria and to have a Hamilton Anxiety Rating13 score of ≥ 20 and a Generalized Anxiety Disorder 7-Item (GAD-7) scale14 score of ≥ 10. Based on the number of patients with GAD who participated in Study B2411367 through a clinical trial information website, the maximum anticipated sample size was 219. Respondents in this study included those who completed treatment in Study B2411367 and rolled over to an open-label, long-term extension study lasting 52 weeks. Respondents were compensated for their participation in this study.
Study Variables
This study collected data on the following variables: patients’ awareness of GAD and medical care-seeking behavior before diagnosis (motivation for trial participation, awareness of GAD, awareness of symptoms, past medical care-seeking behavior and diagnoses), symptoms of GAD that were present at trial entry and their impacts on daily life, perceptions of diagnosis and assessment (feelings upon being diagnosed, burden of responding to the GAD-7), changes observed due to trial participation (degree of improvement in symptoms and their impacts on daily life, satisfaction with trial participation rated on a scale of 0 [poorly satisfied] to 10 [highly satisfied]), resistance to medical care and care experiences (resistance to visit/experiences visiting a psychiatric or psychosomatic medicine department), and perceived need for patient support groups.
Data Collection
Patients who wished to take part in this study were directed to a designated website and given an online explanation of the study to support their understanding prior to consent. The online explanation described the study objectives, procedures, expected time required to complete the questionnaire, and data handling. Those who gave voluntary consent on the electronic informed consent form proceeded to complete the web-based questionnaire. The questionnaire was developed by the researchers for this study and consisted of 44 single-choice, multiple-choice, or open-ended questions estimated to take between 30 and 40 minutes to complete; the questionnaire was self-completed by participants online using their own electronic devices. The questionnaire used in the study was written in Japanese; the English translation is provided in Supplementary Figure 1.
To support the accuracy and integrity of responses, participants completed the questionnaire independently and without interviewer involvement. Responses were submitted electronically and stored in a secure system managed by the survey administrator (3H Medi Solution Inc.). No personally identifiable information was included in the dataset used for analysis.
The web-based questionnaire was conducted after completion of Study B2411367. Survey responses were collected in a de-identified manner and could not be linked to treatment assignments in Study B2411367. Accordingly, analyses stratified by randomized treatment assignment were not performed. Due to the double-blind design, participants were not aware of their original treatment allocation in Study B2411367.
Statistical Analyses
Data from patients who completed the questionnaire were included in the analysis. Prespecified criteria for invalid responses were those with mutually contradictory answers to questionnaire items, nonsensical free text, or response patterns indicating non-engagement. Responses from patients whose total response time was less than 2 minutes were also regarded as invalid. The 2-minute threshold was prespecified as a quality-control criterion to flag potentially non-credible responses, such as rapid click-through behavior, based on internal completion time checks and prior experience of the survey administrator. Exclusions of invalid responses were adjudicated by the survey administrator. If a question was answered multiple times, the first response was used in the analysis. Data on categorical variables were summarized as the number and percentage of patients in each category. Data on continuous variables were summarized as descriptive statistics (number, mean, standard deviation [SD], minimum, median, quartiles, and maximum).
Results
Patient Characteristics
A total of 219 patients were eligible for this study, and the questionnaire was distributed to 215 patients after excluding 4 who could not be reached. Valid responses were obtained from 98 patients, all of whom were included in the analysis set (ie, no responses were excluded for inconsistency, lack of coherence, response time, or other quality-control reasons). The patients had a mean (SD) age of 44.5 (11.0) years, and 50 patients (51.0%) were male (Table 1). The most frequently observed duration from onset of GAD symptoms to trial entry was ≥ 5 years (34.7%), followed by ≥ 2 to < 5 years (31.6%) and ≥ 1 to < 2 years (21.4%).
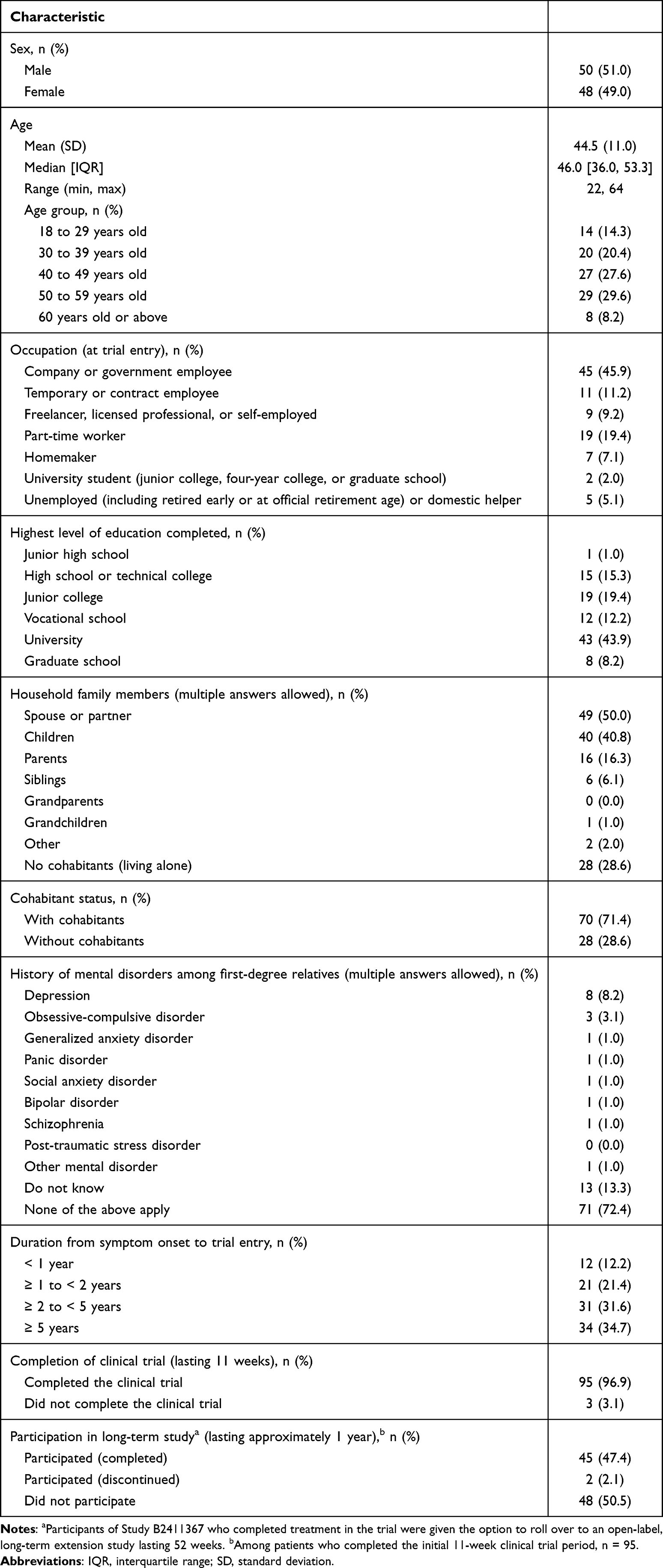 |
Table 1 Patient Characteristics (N = 98) |
Because survey responses were de-identified and could not be linked to randomized treatment assignment, analyses stratified by treatment group were not feasible, and reported post-trial changes reflect participants’ self-reported experiences rather than treatment effects.
Patients’ Awareness of GAD and Medical Care-Seeking Behavior Before Diagnosis
The greatest motivation to participate in the clinical trial was that patients identified with the eligibility criteria, such as “feeling anxious or worried about small things in daily life”, which was reported by 93.9% of patients (Table 2). Before trial entry, the majority of patients (72.4%) had never heard of GAD. Among those who had heard of it, 18.5% had detailed knowledge of the disease characteristics and treatment, 51.9% had a general understanding, and 29.6% had only heard the disease name. When asked whether they had perceived their anxiety as an illness or a personality trait, most patients (71.4%) had considered it a personality trait, while only 12.2% had regarded it as an illness.
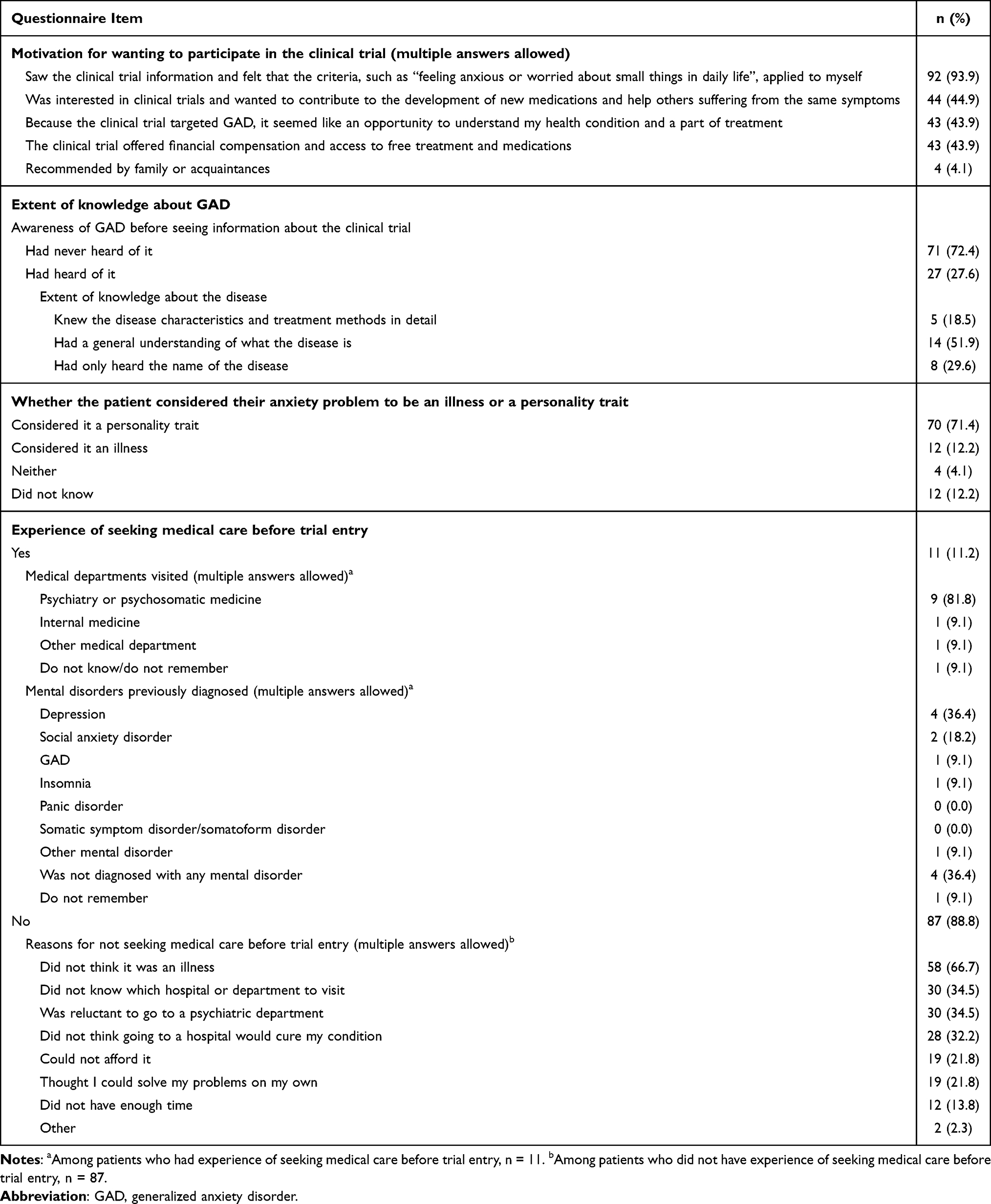 |
Table 2 Patients’ Awareness of GAD and Medical Care-Seeking Behavior Before Diagnosis (N = 98) |
Only 11 patients (11.2%) reported having sought medical care before trial entry, while the majority (88.8%) had not (Table 2). Among those who sought medical care, most had visited psychosomatic medicine or psychiatry departments (n=9; 81.8%). With respect to previous diagnoses of mental disorders, depression was the most frequent (36.4%), followed by social anxiety disorder (18.2%), GAD (9.1%), and insomnia (9.1%).
Among the 87 patients who had not sought medical care prior to trial entry, the most frequently cited reason was the perception that their condition was not an illness (66.7%). Other frequently cited reasons included not knowing which hospital or department to visit (34.5%), reluctance to visit a psychiatric department (34.5%), the belief that seeking medical care would not cure their condition (32.2%), and thinking they could solve the problems on their own (21.8%). Practical barriers were also reported, including financial constraints (21.8%) and lack of time (13.8%).
Symptoms of GAD Present at Trial Entry and Impact on Daily Life
The symptoms of GAD present at trial entry, their impact on daily life, and summaries of representative patient comments illustrating their specific experiences are presented in Table 3. The original verbatim responses (in Japanese) of patients describing their experiences are presented in Supplementary Tables, along with the English translations (Supplementary Table 1, symptoms present at trial entry; Supplementary Table 2, impact on daily life).
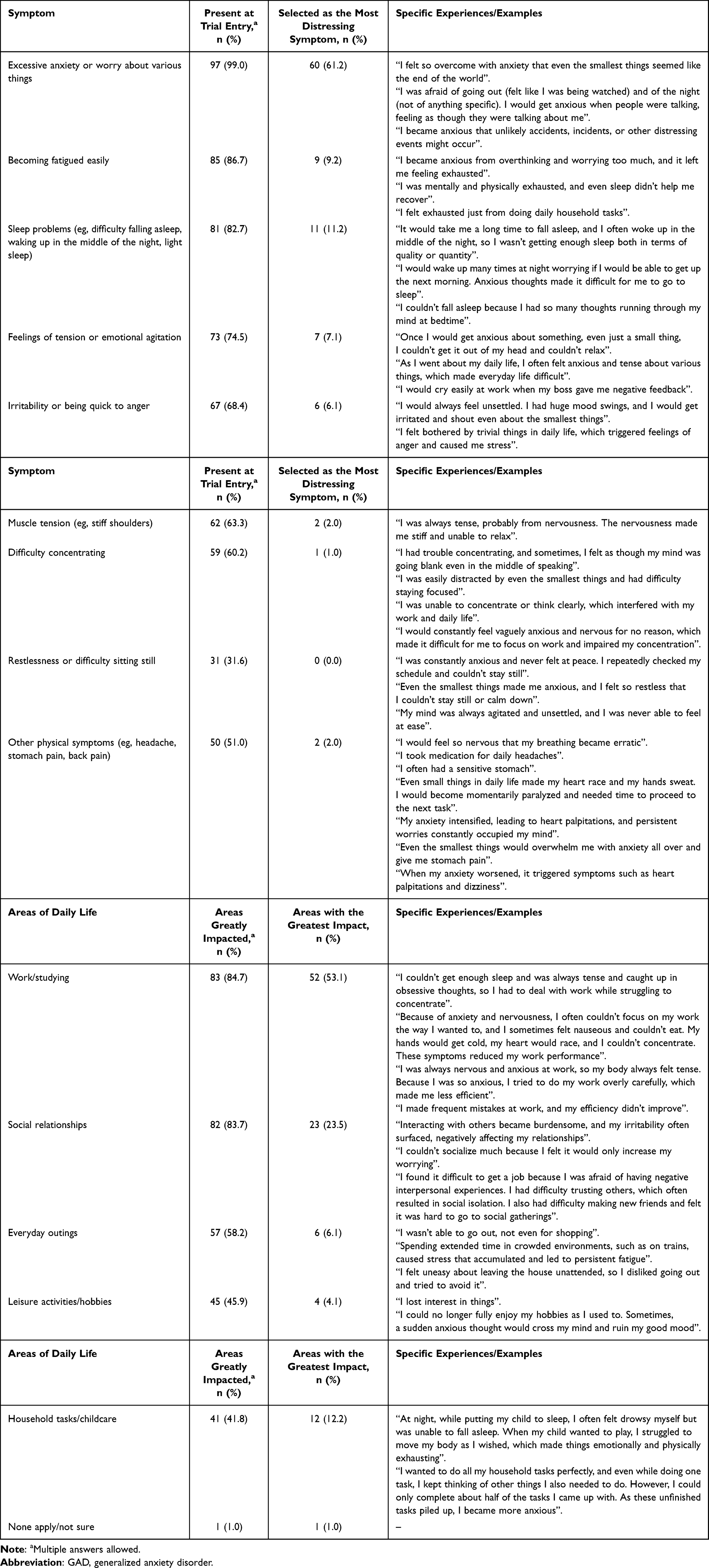 |
Table 3 Symptoms of GAD Present at Trial Entry and Impact on Daily Life (N = 98) |
At trial entry, nearly all patients (99.0%) reported experiencing excessive anxiety or worry. Becoming fatigued easily (86.7%) and sleep problems (82.7%) were also frequently reported. Other frequently reported symptoms included tension or agitation (74.5%), irritability (68.4%), muscle tension (63.3%), and difficulty concentrating (60.2%). The most distressing symptom among those present at trial entry was excessive anxiety or worry (61.2%), caused by constant anxious thoughts and fears about everyday situations. This was followed by sleep problems (11.2%) and fatigue (9.2%), with patients noting difficulty sleeping due to racing thoughts and exhaustion from overthinking.
Symptoms that were present at trial entry substantially interfered with the daily lives of patients. The most frequently reported areas of impact were work or studying (84.7%) and social relationships (83.7%), followed by everyday outings (58.2%). When asked to identify the single most impacted domain of daily life, over half of patients (53.1%) reported work or studying, often describing impaired concentration, reduced efficiency, and physical strain. Social relationships (23.5%) were also frequently reported, with patients citing experiences of withdrawal, mistrust, and irritability, followed by household tasks/childcare (12.2%), caused by exhaustion and feeling overwhelmed.
Perceptions of Diagnosis and Assessment
More than half of patients reported feeling some relief upon receiving a GAD diagnosis, with a total of 54.1% feeling relieved or a little relieved (Table 4). A small proportion reported increased anxiety (12.2%). A majority of patients indicated having positive feelings after diagnosis, with 72.4% noting that they learned their symptoms could be treated, 48.0% that others shared the same symptoms, and 28.6% that treatment might restore their previous well-being. About a quarter (24.5%) felt reassured that the diagnosis was preferable to another disorder, such as depression. Negative reactions were also reported: 52.0% expressed resistance to taking medication, 32.7% felt treatment would be a hassle, 23.5% feared prejudice, and 21.4% felt depressed about having a disorder.
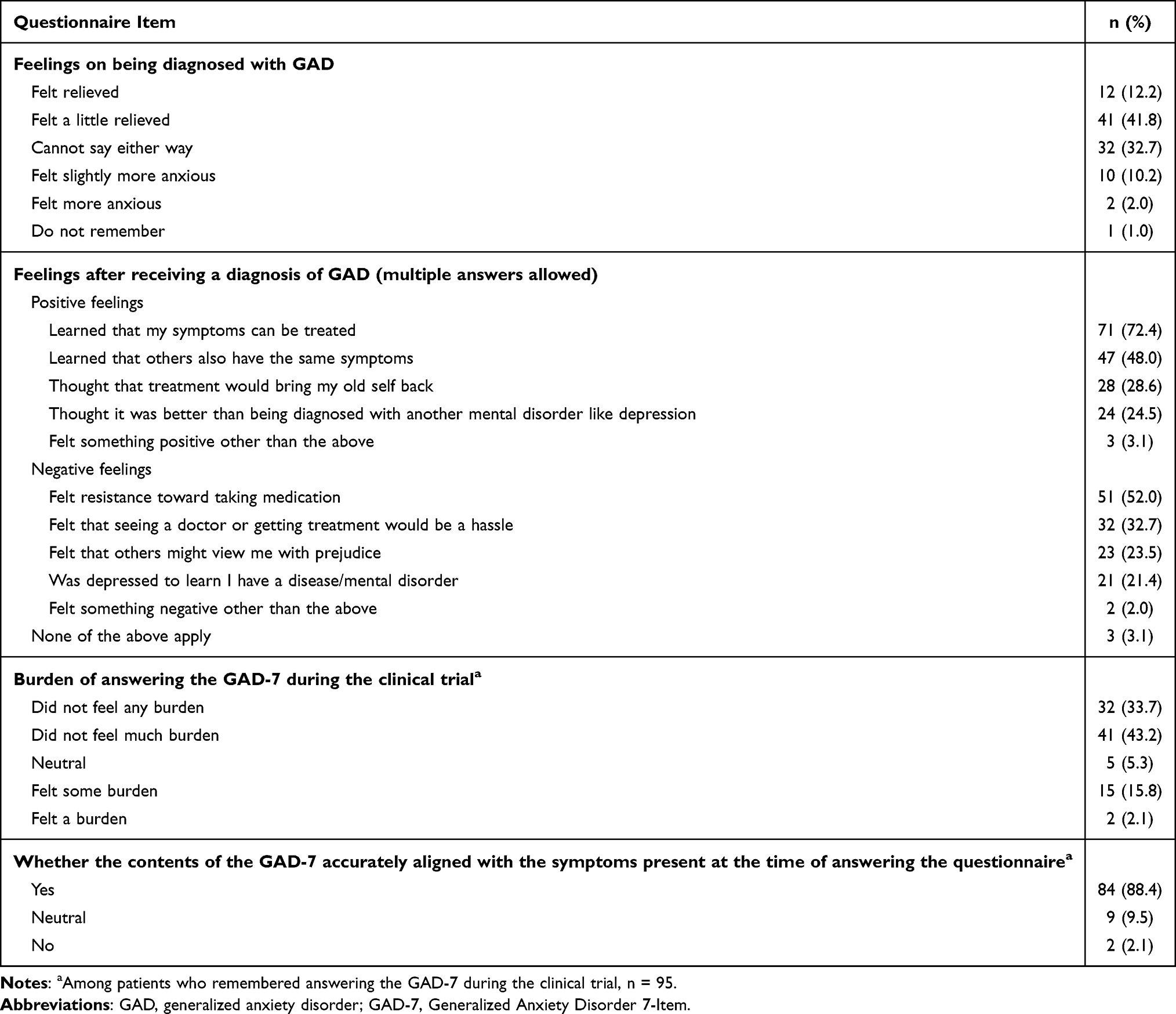 |
Table 4 Perceptions of Diagnosis and Assessment (N = 98) |
Regarding answering the GAD-7, most patients did not perceive it as burdensome, with 76.8% reporting little to no burden, while 17.9% experienced a greater degree of burden. The majority (88.4%) felt the GAD-7 accurately reflected their symptoms at the time of completing it.
Changes Observed Due to Trial Participation
Overall, 70.4% of patients reported some degree of improvement in GAD symptoms following participation in the clinical trial, with 7.1% (n=7) improving and 63.3% (n=62) improving somewhat. In contrast, 26.5% (n=26) reported no change, 3.1% (n=3) experienced a slight worsening, and none reported worsening of symptoms.
The areas of daily life that improved after trial participation, along with summaries of representative patient comments illustrating their specific experiences, are presented in Table 5. The original Japanese verbatim responses and their English translations are shown in Supplementary Table 3. Treatment benefits were most often observed in work or studying (45.9%), with patients describing having better concentration, less fatigue, and greater emotional stability. Improvements were also noted in social relationships (35.7%), everyday outings (29.6%), leisure activities (24.5%), and household tasks or childcare (17.3%).
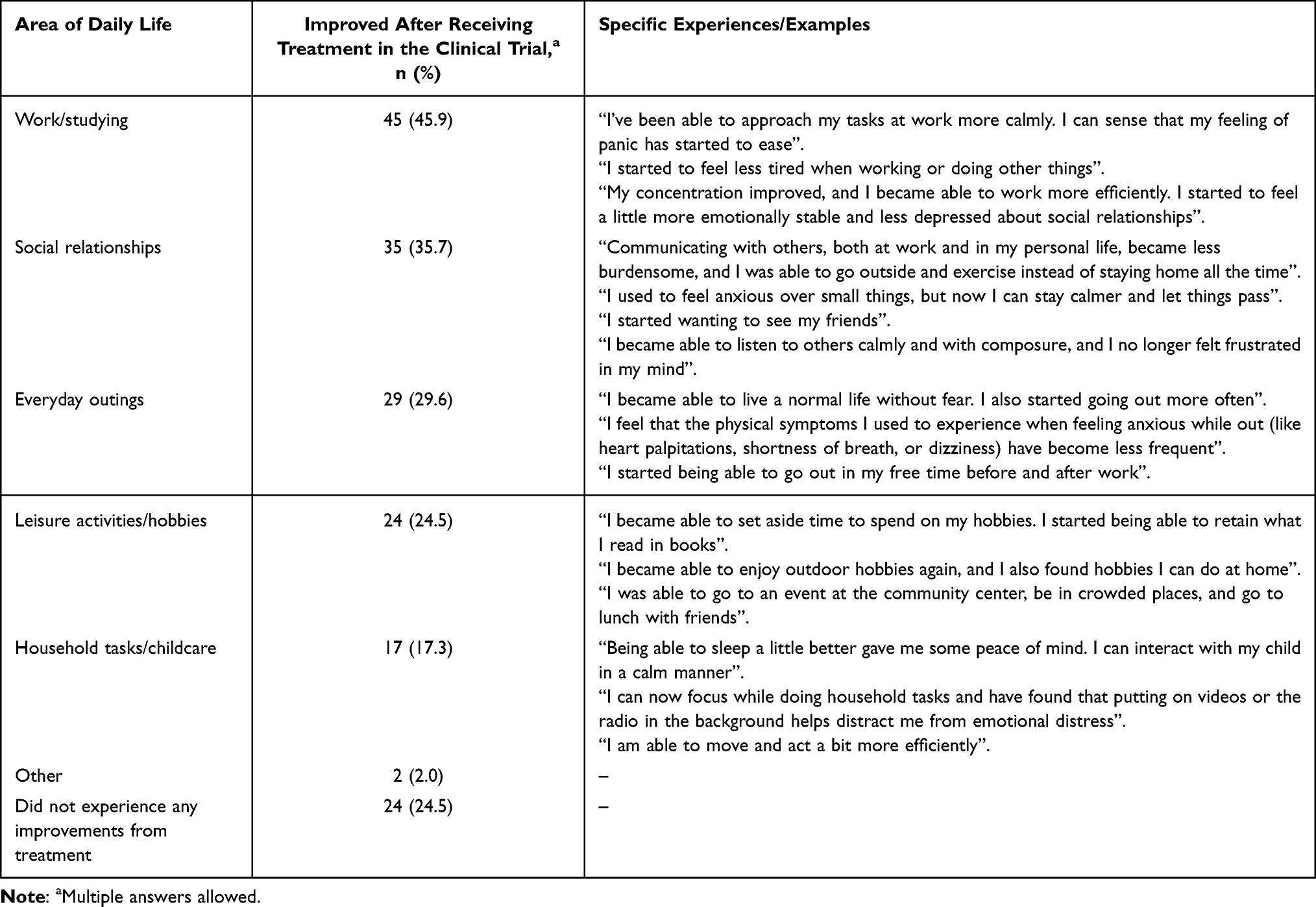 |
Table 5 Improvements in the Daily Life of Patients After Trial Participation (N = 98) |
Satisfaction with the clinical trial was high, with a mean (SD) score of 7.3 (2.0) and a median of 8.0 [interquartile range, 6.0–9.0] on a scale from 0 to 10. The number and percentage of patients who gave each score were as follows: 0, n=1 (1.0%); 1, n=1 (1.0%); 2, n=0 (0.0%); 3, n=1 (1.0%); 4, n=2 (2.0%); 5, n=11 (11.2%); 6, n=18 (18.4%); 7, n=11 (11.2%); 8, n=28 (28.6%); 9, n=8 (8.2%); and 10, n=17 (17.3%). Overall, most patients rated their satisfaction between 6 and 10.
Resistance to Medical Care, Care Experiences, and Need for Support Groups
Most patients reported feeling at least some resistance to visiting a psychiatric or psychosomatic medicine department for the clinical trial, with 53.1% (n=52) feeling some resistance and 19.4% (n=19) feeling resistance; 27.6% (n=27) reported feeling no resistance. For most patients, the clinical trial represented their first time receiving care at such a medical department (n=73, 74.5%), while one quarter (n=25, 25.5%) had previous experience.
Regarding the need for patient groups, nearly half of the patients (n=48, 49.0%) thought such a group would be helpful and 26.5% (n=26) thought it would be very helpful, while a small proportion expressed negative views (“Do not think it would be very helpful”, n= 7, 7.1%; “Do not think it would be helpful at all”, n=0, 0.0%). Interest in participation was also high, with 64.3% (n=63) indicating they would be interested in participating, while 30.6% (n=30) indicated they would not be very interested and 5.1% (n=5) indicated no interest.
Discussion
This study of Japanese patients with GAD who had participated in a clinical trial for venlafaxine investigated patients’ disease awareness, past medical care-seeking behavior and diagnoses, symptoms and impact on daily life, perceptions of diagnosis and clinical assessment, and changes after trial participation.
This study found that most patients enrolled in the clinical trial had been experiencing anxiety symptoms for years that impaired their activities in areas of daily life such as work/studying and social relationships but had not sought medical care. This study also found that many of them were not aware of GAD and had construed their anxiety problems as personality traits, with only a small percentage considering their symptoms an illness. This finding is in line with the results of a previous study that investigated disease awareness in patients with probable GAD in Japan, in which a large proportion of participants also considered their symptoms to be personality-related; the authors of the study likewise reported that 76.5% of the study participants had no knowledge of GAD, and only 3.9% had detailed knowledge of it.2 These observations support the notion that limited disease awareness remains a major barrier to recognition and diagnosis of GAD in Japan. Furthermore, in the aforementioned study,2 over half of participants had never visited a medical institution for anxiety or other mental issues. These findings align with the results of our study, in which the majority of participants had never sought medical care. The findings from our study and previous literature indicate a very low level of public awareness of GAD in Japan and suggest that GAD may be highly underdiagnosed and undertreated in the Japanese population. Thus, raising public awareness of GAD and its treatability may help individuals with GAD receive appropriate diagnosis and treatment.
This study obtained first-hand accounts of the symptoms and burden on daily life of patients with GAD, which provide important insights for clinicians to better understand the patient experience. Patients frequently described difficulties in daily functioning due to anxiety, tension, and sleep problems, which affected their work, household responsibilities, and social relationships. These findings align with those of previous studies on the functional impact of GAD symptoms2,6,7 and help characterize the impact on daily life at the time of trial entry. Reported changes after trial participation included feeling calmer and more focused when working or doing household tasks, greater emotional stability and reduced distress in interpersonal relationships, and an increased ability to leave the house. These patient-reported changes contextualize participants’ experiences following trial participation and offer insights beyond traditional clinical endpoints. These findings suggest that appropriate diagnosis and treatment can be associated with improvements not only in symptoms but also in daily functioning among patients with GAD. In Study B2411367, treatment with venlafaxine led to significant improvements in both anxiety symptoms and functioning. Interpreted together with the present findings, these results highlight the clinical importance of diagnosing and treating GAD, underscoring the potential for meaningful improvements in patients’ daily lives.
The patients enrolled in the clinical trial generally reported a high level of satisfaction with their participation. Although this observation reflects participants’ experiences during trial participation, it does not imply treatment efficacy or causal mechanisms. Satisfaction with trial participation may have been influenced by multiple factors, including access to specialist care, structured follow-up, and increased attention to symptoms, and should therefore be interpreted cautiously.
Most patients reported little or no burden associated with completing the GAD-7 and felt that the questionnaire accurately reflected their symptoms. The GAD-7 is well known as a useful diagnostic tool for GAD, as it takes only a few minutes to complete and imposes a negligible burden upon patients.14,15 The Japanese version of the GAD-7 has been fully validated by Muramatsu et al.16 The results of this study suggest that the Japanese version of the GAD-7 may be useful not only for screening but also for measurement-based care.
Regarding patient groups, many patients expressed a favorable opinion for the availability of such groups, indicating a high level of need. Among the patients’ reflections on receiving a GAD diagnosis, close to half of patients felt encouraged to hear that others had the same symptoms, suggesting that patients with GAD may receive emotional support from the presence of other patients. Mutual support among patients with a mental health disorder, such as through communication in patient groups, has been shown to contribute to symptomatic recovery, empowerment, and coping with the disease.17,18 Given the low level of awareness of GAD in Japan, patient groups for GAD are expected to provide direct support to patients and foster understanding, hopefully contributing to improving public awareness of the disease.
This study has several limitations. First, the study relied on the patients’ recollections of their experiences at the time of trial participation (up to about 3 years before this study), and thus the possibility of recall bias cannot be excluded. Their current clinical state and overall trial experience may have influenced how they retrospectively reported their awareness of GAD, symptom severity, and disease burden at trial entry. Although participants were instructed to recall their experiences at the time of trial entry, the potential influence of active treatment effects, placebo response, and trial-related care or attention cannot be excluded. Second, because this study included patients who were previously enrolled in a clinical trial, there is a risk of selection bias, where patients with more severe symptoms or greater distress may have been overrepresented; thus, caution should be used when generalizing the findings. Third, the clinical trial involved compensation and a level of care that may have been more attentive than in routine practice, and these factors may have influenced patient satisfaction. The findings of this study should be interpreted in light of these limitations.
Conclusion
The present study showed that Japanese patients with GAD who had participated in Study B2411367 had limited awareness of GAD as a medical condition but experienced substantial disease burden. Patients reported mental and physical symptoms that impaired functioning in various areas of daily life. Despite this burden, most had never sought medical care before trial entry, and among those who did seek medical care, only a few were diagnosed with GAD.
The present findings should be interpreted in light of the study’s limitations, including its retrospective design and restriction to individuals who had participated in a clinical trial, which may limit generalizability. Nonetheless, the findings of this study highlight the unmet needs among Japanese patients with GAD who participated in a clinical trial, including low disease awareness and limited recognition in clinical settings. Efforts to increase awareness of GAD may help facilitate earlier diagnosis and broaden access to appropriate treatment.
Future research should extend these findings by examining broader populations, using prospective designs to reduce recall bias, and evaluating pathways that link symptom recognition to timely diagnosis and treatment. Studies assessing the impact of educational or awareness-based interventions on care-seeking behavior may further inform strategies to address unmet needs related to GAD in Japan.
Abbreviations
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; GAD, generalized anxiety disorder; GAD-7, Generalized Anxiety Disorder 7-Item Scale; HRQoL, health-related quality of life; IQR, interquartile range; SD, standard deviation; SNRI, serotonin-norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; UMIN-CTR, University Hospital Medical Information Network Clinical Trial Registry; US, United States.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and with the approval of Viatris Inc.
Ethics Approval and Informed Consent
This study was conducted in compliance with the Declaration of Helsinki and notifications related to the Ethical Guidelines for Medical and Biological Research Involving Human Subjects. The study protocol (protocol ID: VENL-CAZ-7f 002) was approved on April 16, 2025 (approval no. CRE10845), by the Medical Corporation TOUKEIKAI Kitamachi Clinic Ethics Review Board, an independent review board registered with the ethics review board reporting system of the Japanese Ministry of Health, Labour and Welfare (registration no. 11001110). Prior to initiation, this study was registered in the University Hospital Medical Information Network Clinical Trial Registry (identifier: UMIN000057689).
The Act on the Protection of Personal Information and applicable privacy guidelines in Japan were followed in handling the personal and sensitive personal information of patients in this study. After completion of the web-based questionnaire, all responses were anonymized and submitted for analysis as data that could not identify individual patients. All participants provided informed consent for the use of their questionnaire responses in the publication of study results in academic settings, including medical journals. Participants were anonymized (de-identified so that individuals could not be identified), and only de-identified data, including open-ended responses, were used for analysis and publication.
Acknowledgments
This work was sponsored and funded by Viatris Pharmaceuticals Japan G.K., Tokyo, Japan. 3H Medi Solution Inc. recruited participants and implemented the questionnaire for this research. Statistical analysis was performed by Satista, Inc., and medical writing and editorial assistance were provided by Yamada Translation Bureau, Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Viatris Pharmaceuticals Japan G.K.
Disclosure
Keisuke Nomoto, Rikiya Misago, and Shingo Higa are full-time employees of Viatris Pharmaceuticals Japan G.K. Tempei Otsubo has received lecture fees from Viatris Pharmaceuticals Japan G.K.; Takeda Pharmaceutical Co., Ltd.; Otsuka Pharmaceutical; Sumitomo Pharma Co., Ltd.; Meiji Seika Pharma Co., Ltd.; Kyowa Pharmaceutical; Lundbeck Japan; and IQVIA. The authors report no other conflicts of interest in this work.
References
1. Munir S, Takov V. Generalized Anxiety Disorder. StatPearls. StatPearls Publishing LLC.; 2025.
2. Matsuyama S, Otsubo T, Nomoto K, Higa S, Takashio O. Prevalence of generalized anxiety disorder in Japan: a general population survey. Neuropsychiatr Dis Treat. 2024;20:1355–14. doi:10.2147/ndt.S456272
3. Locke AB, Kirst N, Shultz CG. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2015;91(9):617–624.
4. Mishra AK, Varma AR. A comprehensive review of the generalized anxiety disorder. Cureus. 2023;15(9):e46115. doi:10.7759/cureus.46115
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR. American Psychiatric Association Publishing; 2022.
6. Ruscio AM, Hallion LS, Lim CCW, et al. Cross-sectional comparison of the epidemiology of DSM-5 generalized anxiety disorder across the globe. JAMA Psychiatry. 2017;74(5):465–475. doi:10.1001/jamapsychiatry.2017.0056
7. Keller MB. The long-term clinical course of generalized anxiety disorder. J Clin Psychiatry. 2002;63(Suppl 8):11–16.
8. Ishikawa H, Kawakami N, Kessler RC. Lifetime and 12-month prevalence, severity and unmet need for treatment of common mental disorders in Japan: results from the final dataset of World Mental Health Japan Survey. Epidemiol Psychiatr Sci. 2016;25(3):217–229. doi:10.1017/s2045796015000566
9. Portal Site of Official Statistics of Japan. e-Stat (Portal Site of Official Statistics of Japan). Available from: https://www.e-stat.go.jp/.
10. DeGeorge KC, Grover M, Streeter GS. Generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2022;106(2):157–164.
11. National Institute for Health and Care Excellence. Generalised anxiety disorder and panic disorder in adults: management. National Institute for Health and Care Excellence: guidelines. National Institute for Health and Care Excellence (NICE); 2019.
12. Otsubo T, Watanabe K, Inoue T, et al. A randomized, double-blinded, placebo-controlled study to evaluate the efficacy and safety of venlafaxine extended release in Japanese patients with generalized anxiety disorder. Psychiatry Clin Neurosci. 2025;79(12):849–858. doi:10.1111/pcn.13907
13. Matza LS, Morlock R, Sexton C, Malley K, Feltner D. Identifying HAM-A cutoffs for mild, moderate, and severe generalized anxiety disorder. Int J Methods Psychiatr Res. 2010;19(4):223–232. doi:10.1002/mpr.323
14. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
15. Mossman SA, Luft MJ, Schroeder HK, et al. The Generalized Anxiety Disorder 7-item scale in adolescents with generalized anxiety disorder: signal detection and validation. Ann Clin Psychiatry. 2017;29(4):227–234a. doi:10.1177/104012371702900404
16. Muramatsu K, Miyaoka H, Kamijima K, et al. [Validity and usefulness of the Japanese version of the Generalized Anxiety Disorder 7-Item (GAD-7) scale] (meeting proceedings). Jpn J Psychosom Med. 2010;50:592. (in Japanese).
17. Smit D, Miguel C, Vrijsen JN, Groeneweg B, Spijker J, Cuijpers P. The effectiveness of peer support for individuals with mental illness: systematic review and meta-analysis. Psychol Med. 2023;53(11):5332–5341. doi:10.1017/s0033291722002422
18. Fortuna KL, Solomon P, Rivera J. An update of peer support/peer provided services underlying processes, benefits, and critical ingredients. Psychiatr Q. 2022;93(2):571–586. doi:10.1007/s11126-022-09971-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.