Back to Journals » International Journal of Women's Health » Volume 18
Discrimination, Stigma and Taboo Towards the Three Ms’ Working Body: A Systematic Review Around Menstruation, Maternity and Menopause
Authors Cicchetti M, Viotti S, Conforti A, Corrieri L, Converso D ![]() , Bacci G, Guidetti G
, Bacci G, Guidetti G
Received 2 July 2025
Accepted for publication 22 October 2025
Published 31 March 2026 Volume 2026:18 551155
DOI https://doi.org/10.2147/IJWH.S551155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Matteo Cicchetti,1 Sara Viotti,1,2 Alberto Conforti,1 Lia Corrieri,1 Daniela Converso,1 Giulia Bacci,1 Gloria Guidetti1
1Department of Psychology, University of Turin, Turin, Italy; 2Department of Psychology, CRISIS Center, University of Turin; Department of Economics; University of Ca’ Foscari, Venice, Italy
Correspondence: Sara Viotti, Email [email protected]
Abstract: Menstruation, maternity and menopause are three natural and everyday experiences in most women’s lives, but they often intersect in complex ways with career paths and workplace dynamics. In this study, the existing literature on these “three Ms” is systematically examined in relation to taboo, discrimination and stigma in work context, taking into account the PRISMA guidelines. A total of 84 articles from Pubmed, Scopus and Web of Science databases were analyzed. Most of the articles included refer to studies conducted in post-industrial, English-speaking countries, and only a few of them were conducted in non-post-industrial and low-income countries. The review is structured around the three key phases of the female reproductive life course: menstruation, maternity and menopause. These three Ms are examined using a tripartite framework: (1) the individual and subjective level, which focuses on personal experiences, identity, and psychological responses; (2) the organizational environment, which examines workplace policies, professional cultures, and institutional practices; and (3) attitudes and effects on well-being, including societal perceptions, stigma, and effects on psychological and overall health. This multi-level approach provides a comprehensive understanding of how these transitions are experienced, managed and interpreted both individually and in the socio-organizational environment. Despite the near parity in employment rates between men and women and the prevalence of the three Ms in post-industrial with high income countries, the literature is less extensive than expected, suggesting that there is limited academic engagement with the topic. The study highlights the reciprocal relationship between cultural beliefs and academic research. Increased academic attention to menstruation, maternity and menopause in relation to taboo, stigma and discrimination in the workplace could enhance public discourse and help improve the experiences of women at these life stages throughout their careers.
Keywords: menstruation, maternity, menopause, discrimination, stigma, taboo, workplace, systematic review, women’s health, organizational policy
Introduction
Over the last few decades, due to disappearance of physical and ideological barriers,1 the increasing participation of women in the workforce has led to a more balanced representation between genders. In western societies, the number of women in paid work has increased significantly and stands at 70.2% in Europe,2 exceeding by 10.2 percentage points men (80.4%), and 57.4% in the US, exceeding by 11.8 percentage point men (69.2%).3 Nevertheless, gender inequalities and disparities persist in organisations,4 reflecting stereotypical gender roles. We can state that organisational cultures are not gender-neutral, but instead are defined by specific gender expectations, which are ambivalent and contradictory especially for women working in male-dominated environments.1,5 Therefore, gender assumptions, beliefs and stereotypes can define settings, tasks and behaviours and can thus imply a set of pre-established hierarchical interactions based on the sexual division of labour and gender expectations that can be defined as gender segregation by occupational field.1,5,6 In this sense, organisations operate through what Acker7 calls “inequality regimes”, structural patterns that reproduce disparities, particularly along gender, but also in class and race, making inequality a structural in organisational life Acker.7 This condition seems to have roots in work-family stereotypes.6,8,
Regarding gender equality in the workplace, there is indeed a gap between policies and their practical implementation.9 This gap spans through various areas, such as gender diversity, equal access, and equal pay.8,10 In 2022, the difference between the employment rates of men and women aged 20–64 (gender employment gap) was 10.7%, only 0.2% less than in 2021.11 The situation is similar to the pay gap: on average, women earn less per hour than men.12 In 2023, the European Commission stated that this gap is still 13% on equal pay day and had changed only slightly over the last decade.4,13 As outlined by Musumeci and Solera,14 the different levels and types of women’s involvement in paid work are closely linked to the issue of the gendered division of family duties and responsibilities: in the EU-27, women with children have a lower employment rate than women without children. The gap is particularly wide in eastern countries, whereas it is smaller in northern countries. The negative effects of motherhood on employment are greater for the third child: the difference between the employment rates of women with three children and those of women with two children appears to be enormous in 12 countries. Moreover, the gender division of paid and unpaid work also becomes clear when comparing men’s employment rates and the impact of fatherhood: women, not men, tend to reduce their participation in the labour market when a child is born.14 We can consider this situation for women as a double bind, where they are expected to adopt male behaviours in the working context while also maintaining their distinctly female characteristics and stereotypes.1
This situation reflects what Acker15 theorized as the figure of the “ideal worker”, a model rooted in male experiences of full-time, continuous paid work, with all other responsibilities relegated to the private sphere. This image embodies male privileges and perspectives, thereby marginalizing women whose careers are often shaped by family duties and bodily transitions.
In addition to disparities related to social gender roles, women’s careers and quality of working life can often be strongly influenced by their own bodily experiences and associated changes. Grandey et al16 highlights the taboo around the “three Ms” in organisational life, namely menstruation, maternity, and menopause. Despite their relevance to occupational health, these experiences are frequently marginalised or neglected in workplace discourse and policy. Throughout their careers, women encounter these changes presenting challenges from the merging of private bodily experiences with professional demands, highlighting the need to balance personal and professional spheres effectively.16 Since the three Ms are negatively regarded by society as taboos, meaning social prohibitions and shame around their discussion, they can present objective bodily changes and societal beliefs as factors that could explain gender disparities, inequities, and segregation in career outcomes.17–19 However, these phenomena are not only health issues, but are deeply embedded in broader socio-cultural work narratives and power structures, requiring a dedicated framework to understand how exclusion is perpetuated through silence and invisibility.
In this review, we adopted taboo, discrimination and stigma as conceptual lenses through which to interpret contemporary literature on how women experience these life transitions in the workplace.
Taboo refers to a form of social regulation that determines what is speakable and visible. Howson20 defines taboos as “beliefs and rules which societies develop (construct) to maintain dirt in its rightful place and which in turn, represent or symbolise the social order”. This perspective suggests that taboos function to preserve the symbolic integrity of social structures by categorizing certain topics or behaviors as “dirty” or inappropriate, thereby reinforcing societal norms and hierarchies. In the context of the workplace, particularly concerning the three Ms, these taboos can manifest as unspoken prohibitions that discourage open discussion or accommodation of these natural biological processes. Such taboos contribute to the marginalization of women’s experiences, perpetuating gender disparities and inhibiting the development of inclusive organizational policies.
As defined by the Stanford Encyclopedia of Philosophy, discrimination consists of “acts, practices, or policies that impose a relative disadvantage on persons based on their membership in a salient social group”.21 This definition draws attention to the structural and relational dimensions of discrimination, which go beyond individual bias to encompass how social norms and institutional arrangements differentially affect individuals based on gendered assumptions.
Goffman,22 in his seminal work on stigma, refers to it as “the situation of the individual who is disqualified from full social acceptance”. Consequently, the shame and stigma associated with these taboo subjects further compound the challenges that women encounter in the workplace,16 such as stereotypes and the associated discriminations. These dynamics resonate with the ideal worker expectation, rooted in the male breadwinner model,15,23 which requires complete commitment to work through long hours and prioritising employers’ interests above personal ones.24.
Stigma, as Link and Phelan25 elaborate, is a complex phenomenon that intersects with multiple disciplines, including psychology, sociology, and organisational studies and exists when “elements of labelling, stereotyping, separation, status loss and discrimination occur together in a power situation”. Referring to the first component “labelling”, it is pointed out how some human differences are ignored, meanwhile others are overlooked (eg, gender differences, sexual preferences, skin colour…) When labelled differences are linked to stereotypes refers to the second component, examples of this could be the male dominant workplaces and the continuative presence of control and humiliation in the workplace through humour, belittling conversations and the taboos associated with bodily changes during the three Ms5,8,26 The third feature, separation, arises when social labels signify a division between “us” and “them”, this can be traced back to gender segregation or experiences of exclusion.6 Finally, the fourth component concerns experiencing status loss and discrimination. Regarding gender differences, Correll & Benard27 emphasise that discrimination arises due to stereotypes about the performance of men and women that influence the evaluation of employees.
This conceptualization of stigma25 thus allows for a deeper understanding of how structural inequalities are maintained through individual and collective behaviours, policies, and cultural norms that support unequal treatment based on gender. Gender inequalities and disparities in organisations can manifest through various forms of social exclusion, such as aversion to interaction, avoidance, social rejection, discounting, discrediting, dehumanisation, and depersonalization of others into stereotypical caricatures.28 These behaviours not only reinforce discriminatory practices but also perpetuate gendered power imbalances causing a stigmatisation of gender differences within organisations.25,29–33 It pertains to a very complex model involving interactions among the stigmatizer, the stigmatised individual, and the community, all of whom contribute to the maintenance of stigma.25,32 Stigma can indeed be directed towards others or internalised personally.25 Internalised stigma (self-stigma) can contribute to a loss of self-efficacy, learned helplessness and lower psycho-physical health, greater psychological stress, and a higher likelihood of engaging in activities that harm the individual’s health, leading individuals to feel shame or self-loathing.
Therefore, since menstruation, maternity and menopause represent bio-psycho-social conditions that require women only to attend to personal needs first, when they are brought into work they can generate incongruence with the ideal worker expectation Acker.15 Moreover, since stigma relates to the impact of a taboo, discrimination and the perception of the person affected and others, we can contend that the three Ms are particularly stigmatised in the workplace, where they are seen as indicators of weakness and incompetence.5,16
Thereby, taboo discrimination and stigma can have a negative impact on well-being and career trajectories of working women, as well as the broader life systems in which they are integrated, including the workplace. Moreover, the balance between work and biographical transitions for women is affected by stereotypical attitudes and behaviours related to the three Ms, potentially leading to discriminatory incidents. Discrimination and perceived discrimination can be seen as a type of stressor that has received increasing attention in the literature in recent years and they have been proved to be linked to depression, anxiety and poorer general health.34
Although previous reviews have addressed several topics regarding the three Ms, they have treated the issues of menstruation, maternity and menopause separately and in reference to single correlates of a physiological, psychological or social nature.17,35–37 For example, reviews have examined menstrual distress in reproductive-age women,36 psychosocial correlates of exclusive breastfeeding,17 or menopause at work,38 or organisational policies on menstruation and menopause.39
In the same vein, reviews have been provided concerning the three Ms with regard to working women’s lives with specific focuses on how to manage health related factors or psychosocial correlates in the working context that can affect the quality of life during such transitions.40–43 However, to this date, there is a lack of systematic literature reviews addressing the three Ms simultaneously in the workplace. Moreover, none has framed these issues through taboo, discrimination, and stigma, despite their relevance in explaining how such transitions become silenced and marginalised at work. The recent integrative review of Grandey et al16 tackled the taboo of the three Ms by reviewing the evidence for how menstruation, maternity, and menopause are each linked to hormonal and physiological changes, societal beliefs and stereotypes, work affect, cognition, and behaviour. The purpose of this systematic review is to examine how the three Ms are connected with stigma and discrimination in the workplace. The findings highlight how taboos surrounding menstruation, maternity, and menopause contribute to stereotyping and prejudices, shaping attitudes and behaviours that ultimately impact on women’s well-being and quality of life. By addressing these issues, our intent is to clarify how extensively these topics have been discussed in recent literature, providing insights for future research.
Materials and Methods
Search Strategy and Eligibility Criteria
The bibliographic search that led to this systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.44,45 The PRISMA checklist is described, in detail, in Table S1.
To guarantee a quality of the articles included in this systematic review the following electronic databases were used for the present study: PubMed; Scopus and Web Of Science. We used combinations of keywords related to the “Three Ms” biological transitions (menstruation, maternity, and menopause), the work context (eg, workplace, employment, working conditions), and concepts (discrimination, taboo, and stigma) Boolean operators and truncation were used to enhance sensitivity and comprehensiveness.
Some Examples of Search Strings Included:
- (“Menstruation” OR “menstrual pain” OR “Menstrual Cycle”) AND (“work*” OR “employment”) AND (“discrimination*” OR “taboo*” OR “stigma”)
- (“maternity” OR “pregnancy*” OR “mother*”) AND (“work*” OR “workplace”) AND (“social stigma” OR “discrimination exposure”)
- (“menopause” OR “climacteric*”) AND (“working condition*”) AND (“taboo*” OR “social discrimination”)
On PubMed, the search was adapted, adding MeSH terms to ensure alignment with database-specific indexing (eg, “Menstrual Cycle”[MeSH], “Menopause”[MeSH] “Workplace”[MeSH], “Social Discrimination”[MeSH], “Taboo”[MeSH])
The complete list of Boolean search strings used across all databases is provided in Appendix A.
To collect the most up-to-date data, the search was limited to journal articles published between January 2010 and September 2024, and further exclusions were made after reviewing title, abstract and full text.
The Inclusion Criteria Were as Follows:
- Articles that address menstrual discrimination, stigma and taboo in the workplace;
- Articles that address workplace discrimination, stigma and taboo related to maternity, pregnancy, return to work after maternity/parental leave and breastfeeding;
- The journal articles dealing with menopause discrimination, stigma and taboo in the workplace;
- Empirical studies using both qualitative and quantitative methodology.
The exclusion criteria were as follows:
1. The journal articles were not published between January 2010 and September 2024;
2. The articles were not published in English;
These exclusion criteria were chosen for the following reasons:
- We decided to include only the most recent literature in this systematic review. Therefore, only the last 14 years were considered. Moreover, only papers written in English were included, recognizing that this might lead to important results being overlooked and limited corroboration of reported data. On the other hand, this choice allows us to consider only research published in international journals.
Process
The article selection process was carried out by the first, third and fourth authors. The aforementioned process was conducted in different stages, described in the results. At first, the selection process was carried out separately and individually, with the review organised by topic. All subsequent exclusions and inclusions were proposed by one author and cross-checked by the others. The entire selection and exclusion process was overseen by the second and last authors. There were times when the authors confronted each other about whether to exclude or include some articles. In these cases, all these articles were read individually and each author selected the reasons why the article in question should be included or excluded and then presented them to the other authors involved in the selection of the articles and the two supervisors. Throughout this process, Rayyan,46 an online software, was used to keep track and organise the scientific literature. This proved to be particularly helpful in the disagreement resolution process. The same process characterised the qualitative synthesis of the results, in which the first, third and fourth authors first independently reviewed the articles and identified thematic categories and, based on a process of comparison with the second and last authors, produced the final version of the qualitative analysis.
Data Analysis
A standardised data extraction form was used to conduct the data analysis, covering 1) general study details (publication year, authors, title, publication source); 2) study type; 3) sample characteristics; 4) measures; 5) outcomes; 6) country of research.
In this systematic review, the articles were thoroughly assessed with the Joanna Briggs Institute’s47 (JBI) Critical Appraisal Checklist. This toolset is designed to evaluate bias across various research types, including cohort, cross-sectional, qualitative, quasi-experimental studies, systematic reviews, and expert opinion texts.47 The JBI checklist is well-regarded for its reliable framework, supporting a consistent and detailed quality evaluation process.
Articles were rated based on established thresholds: those scoring above 70% “yes” responses were labelled as Low risk, 50–69% as moderate risk, and below 49% as high risk. Evaluation methods, scoring, and cut-off points were defined and approved in advance to ensure fairness. This approach allowed only articles meeting essential quality standards to be included in the review’s findings. All the criteria for all the research types are shown in the description of Table S2.
Results
A total of 10801 articles were found through the electronic database search. Specifically, the search yielded 5289 on the topic of menstruation, 5371 on the topic of maternity and 141 on the topic of menopause. A previous filter was set so that the first result already excluded articles that were published outside the period between January 2010 and September 2024 and were not written in English. 4446 articles were immediately excluded as they were duplicates of others. This process resulted in 3266 that were about menstruation, 3009 about maternity and 80 about menopause. Initially, the records were screened by title resulting with the exclusion of 3810 articles and then by abstract which resulted in the exclusion of 1703 more articles. A total of 842 articles were screened on the basis of their full text, with the further exclusion of 772 articles and leaving only 70 records. The bibliographic references of the selected papers were checked and a further 4798 cited articles were screened. After excluding 1505 articles because they were duplicates, first the titles and then the abstracts were checked, which led to the exclusion of 2966 articles first and then 283 articles. 44 papers were checked in their full-text version, which led to the exclusion of 33 articles. The remaining 11 articles were added to the 69 previously selected articles. This resulted in a final sample of 81 articles that were included in qualitative analysis. Of these, 6 deal with menstrual discrimination in the workplace, 58 with maternity discrimination in the workplace and finally 17 with menopause discrimination in the workplace.
Study Characteristics
Most of the articles in the overall sample were conducted in Anglophone Western countries. Specifically, of the 58 articles that dealt with motherhood, 38 were conducted in the USA, 2 in the UK, 2 in Canada, 2 were a collaboration between the USA and the UK, and 1 in New Zealand. Of the 6 articles dealing with menstruation, 2 were conducted in the UK, 1 was a collaboration between the UK, the US and Germany and 1 was developed in the US. Of the 17 articles examining the menopause, 11 were conducted in the UK, 2 in Australia and 1 was a collaboration between an Australian and a US research team.
Of the remaining 18 articles in the total sample, 4 articles (1 on menstruation, 1 on maternity and 2 on menopause) were conducted in the Netherlands; on the topic of maternity, the search has resulted in 2 articles in Switzerland, 2 in Japan, 2 in Germany and 2 in Pakistan; on menstruation, 1 study was conducted in Bangladesh; on maternity 1 study was conducted in South Korea,1 in a collaboration between Portugal and France, 1 in China, and 1 in Austria; finally, on menopause, 1 paper was conducted in Poland. The 6 articles on menstruation were published between 2019 and 2023, with a higher frequency in 2021 and 2023, with 2 articles published during these years. The 58 articles on maternity were published between 2011 and 2024, with a higher frequency in 2023, when 10 articles were published. The 17 articles on menopause were published between 2013 and 2024, with a higher frequency in 2020 and 2021, when 3 articles were published in these two years. Overall, 2023 was the year in which the most articles on the three topics were published.
Our findings indicate that academic interest in the discrimination, taboo, and stigmatization of the three Ms in the workplace has increased over time, with a clear rise in publications from 2011 to 2023 and 2024 (Figure 1). Specifically, research on menstruation in the workplace emerged only recently, with the earliest publication identified in 2019. While subsequent years have seen minor fluctuations, the overall number of articles has not demonstrated significant growth. Similarly, research on menopause in the workplace began in 2013 and shows a comparable trend, with the number of publications slightly increasing, remaining stable, or occasionally decreasing over time. In contrast, maternity-related research demonstrates a more established and steadily growing body of literature. The first publication appeared in 2011, earlier than for menstruation and menopause, and the number of studies has increased consistently since then. Although there were occasional years with fewer publications, the general trend is positive: by 2023, the number of publications was more than four times higher than in 2011.
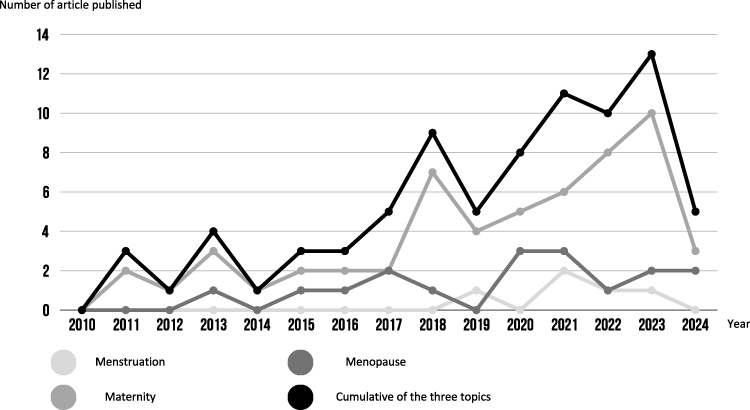 |
Figure 1 Interest’s progression over time. |
Regarding the methodology adopted, 2 of the 6 articles investigating menstruation used a qualitative methodology, the other 4 used a quantitative methodology, being cross-sectional articles. Of the 58 articles that looked at maternity, 19 were cross-sectional articles, 19 used a qualitative methodology, 6 were cohort articles, 6 were systematic reviews, 5 were quasi-experimental articles, 1 was an expert opinion. 2 articles adopted a mixed methodology, one of them using both a qualitative approach and being a cross-sectional study and the other being both a quasi-experimental and a cross-sectional study. Among the 17 articles examining menopause, 11 used a qualitative methodology, 4 were cross-sectional articles and 2 were systematic reviews.
The quality assessment of the included articles is detailed in Tables S2 and S3, while a summarization of the study characteristics aforementioned is presented in the Table 1. An evaluation conducted with the Joanna Briggs Institute47 checklist determined that all articles met the required standards for acceptable quality, qualifying them for inclusion in this review. In the following section, the levels of risk—moderate, low, and high—will be outlined for each category of research, providing a nuanced understanding of the methodological strengths and limitations across the included articles.
 |
Table 1 Study Characteristics |
Among the cross-sectional studies, 25 had a low level of risk, 2 a moderate level of risk and 3 a high level of risk; among the qualitative studies, 31 had a low level of risk, 1 a moderate level of risk and 1 a high level of risk; among the systematic reviews, 4 had a low level of risk, 2 a moderate level of risk and 2 a high level of risk; all of the 6 cohort studies and the 6 quasi-experimental studies had a low level of risk and the 1 textual evidence: expert opinion had a low level of risk. Three articles adopted a mixed methodology, therefore they appear in more of a category.
Qualitative Synthesis of Results
The results have been organised into three main categories, reflecting different levels and manifestations of these phenomena in the workplace context: the first concerns individual and subjective perceptions, exploring how women interpret and internalise discriminatory dynamics, particularly in relation to social expectations, cultural norms, and gendered assumptions around the three Ms; the second focuses on organisational and structural dimensions, highlighting how workplace environments, norms, and institutional arrangements can reinforce or mitigate these dynamics; and the third addresses how stigma, discrimination, and taboos related to three Ms could present implications for quality of life and well-being, both psychologically and physically. Some studies, due to the complexity and breadth of the issues addressed, were relevant to more than one category.
Menstruation
Menstruation-related discrimination, stigma, and taboos emerged as the least widely studied topic within the three Ms literature, with 6 articles (7,41% of the total number of articles) found related to the topic.
Individual and Subjective Level
This was the most represented category with 5 out of 6 articles examining perceptions of menstruation-related discrimination, stigma and taboo in the workplace on an individual and subjective level. The studies show how these perceptions impact women on both a personal and professional level, often leading to additional workload and increased stress. Due to the breadth of social stigma associated with menstruation, women themselves may perceive the experience of the menstrual cycle as “disgusting, shameful and polluting”,48 demonstrating an internalisation of stigma.
To better understand this area, it has been highlighted a particularly salient sub-theme:
- Openness to Disclosure and Perceived Need to Conceal (4 Articles): The need for concealment and the potential benefits of disclosing menstrual symptoms in the workplace are widely debated in the current literature on menstruation. The general perception is that people are not allowed to disclose their menstrual-related symptoms at work,49 creating an unspoken menstrual etiquette.41 Disclosure is more likely when menstrual symptoms are moderate to severe and employees need to be absent from work, even though period pain and symptoms are often not considered from the affected individual themselves a valid reason for absence from work and could lead to discrimination or embarrassment.26 The literature suggests that a higher likelihood of disclosing this to supervisors could prevent presenteeism habits to occur at work. Closeness and trust with colleagues or managers play a crucial role in the likelihood of disclosure, as does the perception of a gendered work environment.26,50 The perception of having to conceal menstrual symptoms at work add up additional requests to the workload.41
Organisational Environment and Attitudes
The second category focuses on the organisational and structural dimensions of menstruation-related stigma, discrimination and taboos, which were identified in 3 out of 6 articles. The included studies highlight how organisational policies, or the lack thereof, can perpetuate inequalities and influence women’s experiences during their menstrual cycle and managing menstruation-related physiologic manifestations while at work. Literature paid attention to this subcategory by focusing on the facilitating policies and practical support that people that experience menstruation need. As Sang et al41 noted, many work environments do not provide easy access to appropriate facilities, which does not facilitate coping with the additional burden of managing menstruation in the workplace. Barnack-Tavlaris et al9 described in detail people’s perceptions of menstrual leave, an important measure that could improve the experience of menstrual-related symptoms while being employed The attitudes of respondents varied widely: many indicated that they were in favour of such a measure in the workplace, that could potentially provide support, while many others felt it was unfair to men, useless, or even that it could exacerbate discrimination against workers suffering from menstrual symptoms. Ponzo et al49 examined the experiences of people who menstruate with the support of a digital tool that allows users to track physical and mood symptoms throughout the menstrual cycle, assessing that the use increased bodily awareness, the perception of support and the likelihood to disclose to others, including colleagues and managers.
Implications for Well-Being
The consequences of the discriminatory dynamics, taboo and stigma towards menstruation in the workplace have been little explored in the literature: 1 out of 6 articles mentions the topic. In the work of Cook & van den Hoek,50 presenteeism behaviour is considered. They note that many people experiencing severe menstrual symptoms attend work despite their debilitating symptoms or pain, and do not take proper care of themselves.
Maternity
Maternity-related discrimination, stigma, and taboos emerged as the most widely studied topic within the three Ms literature, with 58 articles (71,60% of the total number of articles) found related to the topic.
Individual and Subjective Level
The first category had a large representation with 29 out of 58 articles focusing on perceptions of maternity-related discrimination in the workplace. The studies reveal how these perceptions shape both personal and professional trajectories, often resulting in reduced opportunities, increased stress, and anticipatory self-censorship.
To better understand this area, the findings have been grouped into three sub-themes.
- Motherhood Myths and Taboos (6 Articles): Persistent socio-cultural beliefs, moral norms, and symbolic representations of motherhood that justify gender inequality and discrimination. These myths often portray caregiving as a natural female role and suggest that a mother’s professional commitment threatens family well-being, thereby reinforcing opposition to women’s careers and legitimising gendered expectations in the workplace.51–56
- Power Imbalances and the Delegitimation of Motherhood (13 Articles): Relational power imbalances shape how pregnancy and motherhood are perceived and treated in the workplace. Rather than through formal policies, discrimination often emerges in subtle, interpersonal dynamics where women’s professional legitimacy is undermined. These dynamics include being excluded from decision-making, having competence questioned, or being deemed less committed, reflecting broader social mechanisms that construct motherhood as incompatible with ideal worker norms.18,57–68
- Career Penalty and Silencing Dynamics (10 Articles): Experiences of discrimination often translate into career penalties, including limited advancement opportunities and exclusion from support policies. Hostile attitudes from colleagues and supervisors reinforce unequal expectations around motherhood, framing it as incompatible with ideal worker norms. As a result, many women face implicit pressure to not disclose pregnancy or caregiving responsibilities to avoid stigma or marginalisation.69–80
Organisational Environment and Attitudes
This was the most represented category, with 34 of 58 articles exploring the organisational and structural dimensions of maternity-related stigma, discrimination, and taboos. This level of analysis explores how workplace environments, norms, and institutional arrangements can reinforce or mitigate these dynamics. The included studies highlight how organisational structures, or their absence, may perpetuate inequities and shape women’s experiences during pregnancy, maternity leave, and return to work.
This Category Includes Three Sub-Themes:
- Structural Stigma Embedded in Organisational Systems (16 Articles): This sub-theme explores how certain formal and informal workplace systems can perpetuate discrimination. Studies under this sub-theme suggest that organisational culture and systems can create barriers for women, making them feel stigmatised, especially during pregnancy or after returning from maternity leave. These barriers may include a status loss, such as diminished responsibilities, or being overlooked for key projects or roles.68,72,81–94
- Absence or Inadequacy of Maternity-Supportive Policies (18 Articles): This sub-theme is based on studies that highlight the negative impact of a lack of supportive policies. When maternity leave policies or flexible work arrangements are absent or inadequate, women face greater difficulty in balancing work and family responsibilities. The absence of clear policies can lead to feelings of exclusion and uncertainty, reinforcing discrimination and stigma;51,59,61,65,66,70,80,82,90,91,94–101
- The Role of Perceived Support from Colleagues and Supervisors (9 Articles): These studies emphasise how perceived support from colleagues, supervisors, and the broader organisational environment plays a crucial role in shaping women’s experiences during and after maternity. These studies also highlighted the importance of effective leadership in fostering inclusive workplace cultures, capable of countering stigma and reducing the risk of marginalisation.18,57,66,81,94,100,102–104
Implications for Well-Being
11 studies out of 58 investigate the negative consequences of these workplace dynamics, focusing on stress, burnout and mental health challenges such as anxiety and depression, sometimes leading to miscarriage. The findings highlight the toll these factors take on women’s overall quality of life, including the emotional strain of navigating these challenges during pregnancy, maternity leave, and their return to work.57,61,62,64,68,80,83,102,103,105,106
Menopause
17 articles (20,99% of the total number of articles) were found related to the topic of Menopause-related discrimination, stigma, and taboos.
Individual and Subjective Level
This category includes 13 of 17 articles considered that examine perceptions of menopause-related discrimination, stigma and taboo in the workplace from the individual’s perspective. The studies show how these perceptions shape both personal work experiences and career trajectories, often leading to fewer opportunities, more stress and hiding one’s experiences from the eyes of others. Rowson et al107 reported on the stigmatising portrayal of menopause in the media, which is perfectly intertwined with a biomedical perspective. This stigmatisation process goes so far that menopause disappears completely from the discourse, if not in close relationships108 and becomes a real taboo.109
To better understand this area, the results were grouped into four subthemes:
- Openness to Disclosure and Perceived Need to Conceal (12 Articles): Menopause is accompanied by various bodily phenomena and experiences that make it dirty and therefore must be hidden and concealed in order to present a more desirable version of womanhood in public,19 and for that it is a topic that is not often disclosed in most workplaces.110–114 All of this represents a proper social taboo and distancing others from this type of experience serves the purpose of protecting women from being exposed to social judgement, especially in the workplace and towards young or male colleagues,19,43,109 to avoid embarrassing or discriminatory reactions114 and to continue to be perceived as the ideal older worker.115,116 Aside from being taboo, disclosing menopause in the workplace may be unhelpful.26 It is often the severity of symptoms that makes the difference in who can afford to choose to disclose or not.108 The general perception is that dealing with menopause is more of a personal issue rather than something that could be supported or even just addressed in the workplace,43,110,115 which is conveyed by the fact that women themselves know very little about menopause.112
- Internalized Stigma and the Lack of Positive Representation (4 Articles): Steffan115 noted how the participants in the study reinforced themselves the perception that menopause is something negative and detrimental. This could increase the likelihood of menopause being perceived as a taboo in the workplace. A taboo that is often reinforced by menopausal women themselves.109 One issue that may be related to this internalization process of social stigma towards menopause could be the lack of positive representations of menopausal status.107 Participants in the work of Beck et al112 were surprised to find that menopause could actually be a positive experience, suggesting that it is generally portrayed negatively. This attitude of women towards menopause is based on the fear that they may be perceived negatively or that their abilities may be questioned due to their menopausal status.112
- Gendered Ageism and Stereotypes About Menopause (8 Articles): Menopause symbolically marks the transition to the onset of aging and often exposes women to gendered ageism,19 which may be among the causes that prevent them from advancing in their careers107 and disclosing their symptoms in the workplace to seek support.108,110,111 Steffan115 discusses how many older women reinforce the anti-aging discourse themselves. One stereotype that menopausal women fear is being considered old or “past it”,112 or that their work productivity will be questioned.117
- Decline of the Ideal Worker and Body and the Pressure to Compensate (6 Articles): Menopause is often seen as the inevitable decline of a woman as a whole, marking the beginning of the loss of her youth, femininity and fertility, making her “less of a woman”.19,110 This perception of decline extends to a person’s physical, cognitive and psychological functioning to the point of losing their status as a desirable and ideal worker19,107,110 and being perceived as “less able and less competent”,19,110,111 for the fact that the ideal older worker “hasn’t aged at all”.115 Repositioning away from the ideal worker standard could allow menopausal women to embrace a more complex and richer experience as a whole person and worker.116
Organisational Environment and Attitudes
This category was the most represented, with 15 out of 17 articles focusing on the organisational and contextual dimensions of stigma, discrimination and taboos associated with menopause. In the article by Whiley et al,19 participants reported that menopause is perceived as more socially stigmatising when experienced in a male-dominated work environment, whereas a female-dominated work environment is perceived as more supportive and understanding110 Supervisors and managers could play an important role in destigmatizing menopause in the work context by engaging in menopause-specific support118 More generally, a “Menopause-friendly” work environment that allows for open discussion of the topic without fear of judgement or negative reactions was seen as very important. The authors stated that this could increase the chance for menopausal women to stay employed and even advance their careers.117 A facilitating environment for menopausal workers also concerns tangible aspects, such as the ability to control room temperature and ventilation or having access to rest/sanitary facilities.113,114
One particularly salient sub-theme was identified in the literature:
- Facilitating Policies and Organizational Practical Support (13 Articles): It has been noted that too little attention has been paid to menopause in the workplace, both in the literature on the subject and in organizational facilitating policies,110,112 giving the impression that this target group of workers may be less important than others.43 Recognizing the issues that menopausal women face during their employment could be the proper trigger to encourage the implementation of supportive measures in the workplace.107 Hobson and Dennis,119 Beck et al,111 Geukes et al,109 Hardy et al120 and Żołnierczuk-Kieliszek et al121 supported the introduction of supportive policies through their work Those policies should not necessarily target only menopausal people but potentially being taken advantage of by all the workers, such as flexible working solutions and paid sick leave, organisations could reduce the impact of menopause-related stigma. Creating a comfortable and accessible work environment could be another discrete way to support menopausal workers.108 Other suggestions include raising awareness and training managers to deal with menopause sensitively and appropriately.120 It is important that interventions could be educational in nature too, aimed at menopausal women, their colleagues and their managers.112–114,121
Implications for Well-Being
5 studies out of 17 articles investigate the negative consequences of these workplace dynamics, focusing on stress and mental health problems such as anxiety. Beck et al111 found in their work that the perception of menopausal workers to be felt as less competent may lead them to experience high levels of anxiety in relation to their own work performance. Similarly, the constant perceived pressure to cope with and conceal their menopausal symptoms in the workplace could expose women to states of tension and anxiety.114 The belief that some physical symptoms, such as hot flushes, could be perceived negatively could also contribute to distress and the constant effort to conceal them could itself be a stressor.113 Hobson and Dennis119 stated in their work that promoting an open culture and reducing stigma in the work context could help with the management of menopause-related symptoms. Feeling understood and valued in their experiences can help menopausal women cope with the management of their symptoms.118
Discussion
The aim of this systematic review was to analyse how recent literature has addressed the phenomena of stigma, discrimination and stereotyping around the taboo topics of menstruation, maternity and menopause in the workplace for women. As previously mentioned, the three Ms are, to varying degrees, phenomena that occur in every woman’s life and affect her everyday life in diverse and unique ways. As highlighted in the work of Grandey and et al,16 the three Ms still represent a taboo in the workplace, making it difficult to admit one’s condition in the work context.9,89,112 Gatrell et al76 discuss how rituals and standardised work practises, rooted in the concept of the ideal employee, are considered sacred and inviolable in the work context. These norms often disregard the biopsychological rhythms of different workers, particularly women and mothers, and the emphasis on productivity standards tends to ignore the female body, labelling it a priori as a “failure” and subjecting it to medicalisation even in its natural manifestations. Despite the promotion of good awareness and practice, gender inequality in the post-industrial with high income countries is still present in 2024, with a significant gap of 10.7% in employment and 13% in pay gap.2,4,13 Considering that almost all women will be confronted with the three Ms in the course of their professional lives, the scientific literature on this topic is not as extensive and exhaustive as one might expect. Indeed, the results of this systematic literature review show that although these topics have received increasing attention in recent years, as can be seen in Figure 2 (particularly in terms of research into these issues in relation to maternity) it is still a poorly researched area. Moreover, it is worth noting that most of the articles included in the qualitative analysis refer to studies conducted in post-industrial, English-speaking countries, and only a few of them were conducted in non-post-industrial and low-income countries such as Pakistan and Bangladesh.
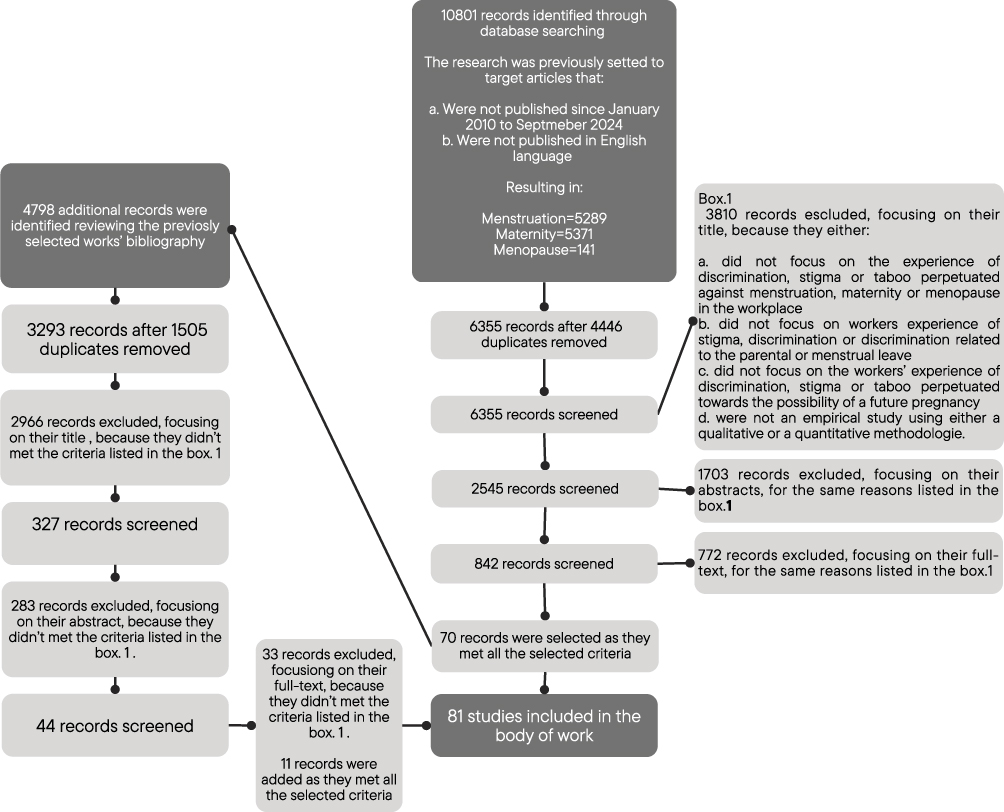 |
Figure 2 Flow Chart. |
The qualitative synthesis has enabled various themes to emerge that align with our interpretative lenses, showing how menstruation, menopause and maternity are labelled on the basis of societal representations and consequently subjected to processes of stereotyping, separation, status loss and discrimination.25 The thematic analysis was guided by three interpretive lenses: (1) the individual and subjective level, focusing on personal experiences, psychological responses, and identity-related processes; (2) the organisational environment, examining the role of workplace policies, professional cultures, and institutional practises; and (3) attitudes and implications for well-being, addressing societal perceptions, stigma, and their impact on psychological and overall health.
At the individual and subjective level many women report high levels of stress, embarrassment, reluctance to disclose their needs, silenced dynamics and presenteeism habits.41,50 These findings suggest that striving to embody the ideal worker model leads to self-silencing and health-compromising behaviours.15 For example, individuals suffering from heavy menstrual symptoms often avoid taking leave, risking burnout, and neglecting self-care.50 Sang et al41 emphasise that many people invest a lot of time and effort in managing menstrual symptoms at work. This burden is influenced by both pain management and specific concerns that entail a change in work routines, impacting both the person and work performance.41,50 Similar dynamics affect menopausal women, who may conceal their symptoms to avoid being perceived as less competent, which further increases stress.9,43,111–113 This suggests that stigma operates through self-silencing and health-compromising behaviours, showing how the ideal worker model is internalised and reproduced at the expense of women’s well-being.
At the organisational and environmental level, the absence of adequate policies often can generate feelings of exclusion and uncertainty, reinforcing discrimination and stigma. Motherhood is particularly affected, since major life changes intersect with insufficient institutional support, creating structural career barriers. These discriminatory experiences often result in career penalties, limited advancement opportunities and exclusion from support measures. In addition, hostile attitudes from colleagues and supervisors, reinforced by unsupportive workplace norms and unequal expectations that position women’s careers as misaligned with the ideal worker model.122 The competitive and work-centric culture that emerges in many accounts highlights how support is often seen as a critical resource, as if providing accommodations for some workers is perceived as taking away from others, which discourages collective solidarity and reinforces stigma. Years of experience with this type of culture has led to it being internalised with the associated stigma towards anything that could potentially disrupt the expected flow of productivity. On the other hand, there is strong evidence that a supportive and open workplace culture can help to reduce this stress and promote emotional well-being.118,119,122
These findings indicate that organisational practices are not neutral but central mechanisms through which inequality regimes are sustained, positioning women’s careers as structurally misaligned with dominant workplace norms.
Finally at the level of implication for well-being, stigma and taboo were linked to stress, anxiety, depressive symptoms and overall poorer mental health, particularly for those managing heavy menstrual symptoms or menopausal changes. The internalisation of the stigma translates into embarrassment and fear of discrimination, which correlates with presenteeism and reduced self-care. Although progress has been made in promoting workplace inclusivity, the psychological impact of the stigma of menstruation and menopause remains largely neglected.59 This lack of attention points to a link between these taboos and outcomes such as stress, presenteeism and poorer mental health, particularly of a depressive nature, which also has an impact on the family context, highlights the urgent need for organisations to adopt supportive practices that acknowledge women’s bodily transitions as part of working life.62,64,76,89,103
The persistence of stress, anxiety and depressive symptoms illustrates that stigma and taboo are not only cultural constructs but also determinants of health inequities, linking organisational expectations with psychosocial outcomes.
This review has also highlighted how structural stigma embedded in organisation tends to emerge as the tendency to view occupational norms and standards as intrinsic rather than culturally determined not only results in reinforcing taboos, but also encouraging employers to unfairly apply discriminatory practises towards working women, with detrimental consequences for both the women and the occupational context itself.16,18,76,89 In addition to the issues that most directly reflect the role of stigma and its impact on the stereotypes and discriminatory behaviours experienced by women, there is also evidence of the role that interpersonal relationships and workplace policies play. The need to promote good workplace practises that can be integrated at multiple levels was emphasised by several authors as a way to improve well-being and general and working conditions.
From an organisational perspective, qualitative studies reported a number of easily accessible habits that could be implemented to improve the work experience of people with the three Ms.9,26,111 Among these, a number of good practises were highlighted that are suitable for individual professionals, such as the importance of using inclusive language, acknowledging, understanding and accepting that gynaecological health experiences occur and, most importantly, that this must be done without judgement and with an attempt to be empathetic. At the organisational level, recommendations include flexible workload123 and inclusive spaces that can ensure privacy or practical assistance (such as sinks in each bathroom or the availability of hygiene items), and workplace environments that are safe, healthy and non-discriminatory.26 In addition, ensuring easy control over workplace equipment (eg, temperature or lighting controls) or developing health promotion programmes that include information about menstruation, menopause, ageing and basic general health issues could be helpful in supporting women to manage their symptoms in the best possible way.114,124
Such customisation of work should be considered and managed, but in terms of policy, the debate is quite extensive and varies greatly depending on the topic. Hardy and Hunter26 use the example of menstrual leave to show that there are conflicting views on this in the literature. In fact, a menstrual leave policy in the workplace could be beneficial and lead to an increase in productivity, as menstrual symptoms can be a significant obstacle to the work schedule of menstruating women. Taking the right amount of time to rest and recover, could allow women to come back to work restored and able to work at their best. On the other hand, according to Barnack-Tavlaris et al,9 menstrual leave would put women in a bad light and perpetuate the stigma around menstruation, supporting the various concerns about the impact that a menstrual leave policy could have on the workplace This controversy illustrates how policy solutions can themselves reproduce stigma if not accompanied by cultural change. Overall, our finding highlights the need for multi-level interventions that go beyond health management and address the cultural assumptions embedded in organisational structures. This is essential not only to implement policies that meet women’s needs, but also to foster broader cultural change within workplaces. Moreover, studies that involve different cultural contexts should be implemented as well. Experiencing stigma depends on how power is held and used in specific contexts, between people, and through the cultural, institutional and structural systems in place.125 Nevertheless, the dearth of literature is otherwise a consistent disservice to the health promotion of working women, a missed opportunity to lay the groundwork for effective preventative action, and in some ways reinforces the culture of stigma, prejudice and discrimination that appears to exist.
Finally, within the socio-cultural context, casual discursive interactions outside the workplace are conducted in everyday life and in the media can play a crucial role in shaping perceptions of the three Ms. They could be empowering if the portrayals are positive and balanced, encouraging more open conversation that could improve women’s working lives, or otherwise lack of good representation may discourage talking about the topic or silence it altogether, reinforcing discrimination and taboos and limiting potential social change.107 This shows how stigma is reproduced not only in organisations but also in cultural narratives, and how academic research itself contributes to fuelling or challenging these discourses. Any study related to the three Ms would not only serve its primary purpose, but would also indirectly feed into this broader discourse. As a first step, increasing academic work on the three Ms can therefore help to change attitudes and prevent discriminatory behaviour in the workplace.
Conclusion
This review provided one of the first systematic syntheses of how menstruation, maternity and menopause are linked to stigma, discrimination and taboo in workplace contexts.
Our findings highlight that these issues remain under-researched particularly outside Western post-industrial countries, with only a few studies conducted in countries such as Japan, China, Bangladesh or Pakistan. Considering that among these latter contexts, women have lower levels of health, empowerment, and labour market participation,67 this underscores the need for cross-cultural comparative research on how stigma, stereotypes and discrimination are shaped across different systems, and for investigations into male workers’ representations and attitudes, which remain largely absent in the literature. By shedding light on the interplay between female bodily changes and workplace experiences, we aim e to encourage more comprehensive studies that address how taboos, stigma, and discrimination related to these changes affect women’s professional lives and well-being.
This review has some limitations. The research methods used may have affected the results: for example, the keywords used may have limited the selection of research papers considered;the inclusion criteria (eg., English-language published studies or reputable databases) may also have limited the sources; relevant evidence may exist in non-psychosocial or medical publications.
In conclusion, research on three Ms in the workplace context should help to move not only to a worker-centred perspective, but also to a people-centred perspective. This assumes that a healthy employee, from a biopsychosocial perspective, is better able to contribute effectively to organisational life. This perspective supports the development of inclusive policies and workplace cultures that benefit both individual well-being and collective performance.
Acknowledgments
The study has been supported by the following grants: “Mindfulness and quality of life during menopause” grant by CRT (PI: Sara Viotti) and “Work and Menopause” grant by University of Turin (PI: Sara Viotti).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gherardi S, Poggio B. Creating and recreating gender order in organizations. J World Bus. 2001;36(3):245–19. doi:10.1016/S1090-9516(01)00054-2
2. Eurostat. Gender statistics. Published 2024. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Gender_statistics.
3. U.S. Bureau of Labor Statistics. Women in the labor force: a databook. Available from: https://www.bls.gov/opub/reports/womens-databook/2020/home.htm.
4. Eurostat. Gender pay gap in the EU down to 13.0%. Available from: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20220307-2.
5. Zinn I, Hofmeister H. The gender order in action: consistent evidence from two distinct workplace settings. J Gender Stud. 2022;31:941–955. doi:10.1080/09589236.2022.2115019
6. Cech EA. Mechanism or myth? Family plans and the reproduction of occupational gender segregation. Gend Soc. 2016;30(2):265–288. doi:10.1177/0891243215608798
7. Acker J. Inequality regimes: gender, class, and race in organizations. Gender Soc. 2006;20(4):441–464. doi:10.1177/0891243206289499
8. Coron C. What does ‘gender equality’ mean? Social representations of gender equality in the workplace among French workers. Equal Divers Incl. doi:10.1108/EDI-05-2019-0153
9. Barnack-Tavlaris J, Hansen K, Levitt R, Reno M. Taking leave to bleed: perceptions and attitudes toward menstrual leave policy. Health Care Women Int. 2019;40(12):1355–1373. doi:10.1080/07399332.2019.1639709
10. Jarman J, Blackburn RM, Wacko G. The dimensions of occupational gender segregation in industrial countries. Sociology. 2012;46(6):1003–1019. doi:10.1177/0038038511435063
11. Eurostat. Gender employment gap still persists in 2022. Available from: https://ec.europa.eu/eurostat/web/products-eurostat-news/w/ddn-20231128-1.
12. European Commission. Gender pay gap in the EU remains at 13% on Equal Pay Day. Published 2023. Available from: https://ec.europa.eu/commission/presscorner/detail/en/statement_23_5692.
13. England P, Bearak J, Budig MJ, Hodges M. Do highly paid, highly skilled women experience the largest motherhood penalty? Am Sociol Rev. 2016;81(6):1161–1189. doi:10.1177/0003122416673598
14. Musumeci R, Solera C. Women’s and men’s career interruptions in Europe: the role of social policies. Observ Soc Brit. 2023;14:37–72. doi:10.4000/osb.1511
15. Acker J. Hierarchies, jobs, bodies: a theory of gendered organizations. Gender Soc. 1990;4(2):139–158. doi:10.1177/089124390004002002
16. Grandey AA, Gabriel A, King EB. Tackling taboo topics: a review of the three Ms in working women’s lives. J Manage. 2020;46(1):7–35. doi:10.1177/0149206319857144
17. De Jager E, Skouteris H, Broadbent J, Amir L, Mellor K. Psychosocial correlates of exclusive breastfeeding: a systematic review. Midwifery. 2013;29(5):506–518. doi:10.1016/j.midw.2012.04.009
18. Paustian-Underdahl SC, Little LM, Mandeville AM, Hinojosa AS, Keyes A. Examining the role of maternity benefit comparisons and pregnancy discrimination in women’s turnover decisions. Pers Psychol. 2024;77(2):819–846. doi:10.1111/peps.12577
19. Whiley LA, Wright A, Stutterheim SE, Grandy G. A part of being a woman, really: menopause at work as ‘dirty’ femininity. Gender Work Organ. 2023;30(3):897–916. doi:10.1111/gwao.12946
20. Howson A. The Body in Society: An Introduction. John Wiley & Sons; 2013. ISBN: 9780745676364.
21. Altman A. Discrimination. In: Zalta EN, editor. The Stanford Encyclopedia of Philosophy. Stanford University; 2020. https://plato.stanford.edu/archives/win2020/entries/discrimination/#ConDis.
22. Stigma GE. Notes on a Spoiled Identity. Prentice Hall; 1963.
23. Koenig AM, Eagly AH. Evidence for the social role theory of stereotype content: observations of groups’ roles shape stereotypes. J Pers Soc Psychol. 2014;107(3):371–392. doi:10.1037/a0037215
24. Selberg R, Padavic I, Tindell K. Scheduling conflicts in the low-wage labor force: the case of Swedish and US women.
25. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27:363–385. doi:10.1146/annurev.soc.27.1.363
26. Hardy C, Hunter M. Premenstrual symptoms and work: exploring female staff experiences and recommendations for workplaces. Int J Environ Res Public Health. 2021;18(7):3647. doi:10.3390/ijerph18073647
27. Correll SJ, Benard SA. Biased estimators? Comparing status and statistical theories of gender discrimination. Adv Group Process. 2006;23:89–116. doi:10.1016/S0882-6145(06)23004-2
28. Bos AER, Pryor JB, Reeder GD, Stutterheim SE. Stigma: advances in theory and research. Basic Appl Soc Psychol. 2013;35(1):1–9. doi:10.1080/01973533.2012.746147
29. Eurostat. Duration of working life - statistics. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Duration_of_working_life_-_statistics.
30. Harness O. Occupational stigma among further education teaching staff in hair and beauty: mild but challenging. Gend Work Organ. 2022;29(6):1526–1541. doi:10.1111/gwao.12847
31. Heilman M, Caleo S, Manzi F. Women at work: pathways from gender stereotypes to gender bias and discrimination. Annu Rev Organ Psychol Organ Behav. 2024;11:165–192. doi:10.1146/annurev-orgpsych-110721-034105
32. Pescosolido BA, Martin JK. The stigma complex. Annu Rev Sociol. 2015;41:87–116. doi:10.1146/annurev-soc-071312-145702
33. Ridgeway CL. Framed by Gender: How Gender Inequality Persists in the Modern World. Oxford University Press; 2011.
34. Stepanikova I, Kukla L. Is perceived discrimination in pregnancy prospectively linked to postpartum depression? Exploring the role of education. Matern Child Health J. 2017;21:1669–1677. doi:10.1007/s10995-016-2259-7
35. Frey BN, Lord C, Soares CN. Depression during menopausal transition: a review of treatment strategies and pathophysiological correlates. Menopause Int. 2008;14(3):123–128. doi:10.1258/mi.2008.008019
36. Maqbool R, Maqbool M, Zehravi M, Arat I. Menstrual distress in females of reproductive age: a literature review. Int J Adolesc Med Health. 2022;34(2):11–17. doi:10.1515/ijamh-2021-0081
37. Utian WH. Psychosocial and socioeconomic burden of vasomotor symptoms in menopause: a comprehensive review. Health Qual Life Outcomes. 2005;3:47. doi:10.1186/1477-7525-3-47
38. Hardy C, Hunter MS, Griffiths A. Menopause and work: an overview of UK guidance. Occup Med. 2018;68(9):580–586. doi:10.1093/occmed/kqy134
39. Howe D, Duffy S, O’Shea M, et al. Policies, guidelines, and practices supporting women’s menstruation, menstrual disorders and menopause at work: a critical global scoping review. Healthcare. 2023;11(22):2945. doi:10.3390/healthcare11222945
40. Arena DF, Volpone SD, Jones KP. (Overcoming) maternity bias in the workplace: a systematic review. J Manage. 2023;49(1):52–84. doi:10.1177/01492063221086243
41. Sang K, Remnant J, Calvard T, Myhill K. Blood work: managing menstruation, menopause, and gynaecological health conditions in the workplace. Int J Environ Res Public Health. 2021;18(4):1951. doi:10.3390/ijerph18041951
42. Sasaki N, Imamura K, Watanabe K, et al. The impact of workplace psychosocial factors on menstrual disorders and infertility: a protocol for a systematic review and meta-analysis. Syst Rev. 2022;11. doi:10.1186/s13643-022-02066-4
43. Verdonk P, Bendien E, Appelman Y. Menopause and work: a narrative literature review about menopause, work and health. Work. 2022;72(2):483–496. doi:10.3233/WOR-205214
44. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Linee guida per il reporting di revisioni sistematiche e meta-analisi: il PRISMA statement. Evidence. 2015;7(6):1–8. doi:10.4470/E1000114
45. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1136/bmj.n71
46. Rayyan Systems Inc. Rayyan: intelligent systematic review. Accessed from: https://www.rayyan.ai.
47. Institute JB. JBI critical appraisal tools. Accessed from: https://jbi.global/critical-appraisal-tools.
48. Zaman RT, Mohiuddin MF. Impact of menstruation-related stigma and behaviour on female employee performance in Bangladesh: mediating role of non-work related stress. South Asian J Bus Stud. 2023;12(2):169–185. doi:10.1108/SAJBS-08-2020-0274
49. Ponzo S, Wickham A, Bamford R, et al. Menstrual cycle-associated symptoms and workplace productivity in US employees: a cross-sectional survey of users of the Flo mobile phone app. Digital Health. 2022;8:205520762211458. doi:10.1177/20552076221145852
50. Cook A, van den Hoek R. Period pain presenteeism: investigating associations of working while experiencing dysmenorrhea. J Psychosom Obstet Gynaecol. 2023;44(1). doi:10.1080/0167482X.2023.2236294
51. Halley MC, Rustagi AS, Torres JS, et al. Physician mothers’ experience of workplace discrimination: a qualitative analysis. BMJ. 2018;363:k4926. doi:10.1136/bmj.k4926
52. Mari G, Luijkx R. Gender, parenthood, and hiring intentions in sex-typical jobs: insights from a survey experiment. Res Soc Stratif Mobil. 2020;65. doi:10.1016/j.rssm.2019.100464.
53. Morgan WB, Walker SS, Hebl MR, King EB. A field experiment: reducing interpersonal discrimination toward pregnant job applicants. J Appl Psychol. 2013;98(5):799–809. doi:10.1037/a0032771
54. Peterson Gloor JL, Okimoto TG, King EB. Maybe baby? The employment risk of potential parenthood. J Appl Soc Psychol. 2022;52(8):623–642. doi:10.1111/jasp.12799
55. Verniers C, Vala J. Justifying gender discrimination in the workplace: the mediating role of motherhood myths. PLoS One. 2018;13(1):e0190657. doi:10.1371/journal.pone.0190657
56. Ziegler Y, Graml R, Uli V, Khachatryan K. Motherhood gap and employer discrimination: a qualitative investigation in the German context. Organizacija. 2023;56(4):281–296. doi:10.2478/orga-2023-0019
57. Borrowman JD, Krumboltz R, Jones M, Whitaker KM. Occupational pregnancy discrimination is associated with negative health impacts for pregnant persons and their children. J Occup Environ Med. 2023;65(12):e791–e796. doi:10.1097/JOM.0000000000002984
58. Borrowman JD, Unke M, Jones M, Whitaker KM. A qualitative study describing experiences of pregnancy discrimination in the workplace. J Occup Environ Med. 2023;66(8). doi:10.1097/JOM.0000000000003136
59. Byron RA, Roscigno VJ. Relational power, legitimation, and pregnancy discrimination. Gend Soc. 2014;28(3):435–462. doi:10.1177/0891243214523123
60. Chun LD, Ye R, Wilby KJ. Exploring discrimination towards pharmacists in practice settings. Pharm Pract. 2020;18(3). doi:10.18549/PharmPract.2020.3.1966
61. Gasior AC, Bergus KC, Beeler WH, Xi AS, Rialon KL. Pregnancy in medical training: a survey of physician moms on their experiences during residency and fellowship. J Surg Educ. 2024;81(1):84–92. doi:10.1016/j.jsurg.2023.09.013
62. Hackney K, Daniels S, Paustian-Underdahl S, Perrewé P, Mandeville A, Eaton A. Examining the effects of perceived pregnancy discrimination on mother and baby health. J Appl Psychol. 2021;106(5):774–783. doi:10.1037/apl0000788
63. Holton M, Bailey K. Women in urology. Urol Clin North Am. 2021;48(2):187–194. doi:10.1016/j.ucl.2020.12.003
64. Kachi Y, Fujiwara T, Inoue A, et al. The effects of pregnancy discrimination on postpartum depressive symptoms: a follow-up study. BMC Pregnancy Childbirth. 2022;22(1). doi:10.1186/s12884-022-05148-2
65. Steiner-Hofbauer V, Katz HW, Grundnig JS, Holzinger A. Female participation or “feminization” of medicine. Wien Med Wochenschr. 2023;173(5):125–130. doi:10.1007/s10354-022-00961-y
66. Wada A, Nakamura Y, Tsuno YS, et al. Factors associated with the work productivity of Japanese working pregnant women: a cross-sectional study. J Occup Environ Med. 2021;63(11):e759–e764. doi:10.1097/JOM.0000000000002359
67. Wang P, Chen J. Fertility-based employment discrimination and family policy: evidence from a field experiment. Soc Policy Adm. 2023;57(7):1135–1149. doi:10.1111/spol.12935
68. Wayne AS, Mueller MK, Rosenbaum M. Perceptions of maternal discrimination and pregnancy/postpartum experiences among veterinary mothers. Front Vet Sci. 2020;7:507230. doi:10.3389/fvets.2020.00091
69. Adesoye T, Mangurian C, Choo EK, Girgis C, Sabry-Elnaggar H, Linos E. Perceived discrimination experienced by physician mothers and desired workplace changes: a cross-sectional survey. JAMA Intern Med. 2017;177(7):1033–1036. doi:10.1001/jamainternmed.2017.1394
70. Akhtar T, Khan MA, Afzal S. A qualitative study of environmental and behavioural factors affecting mothers at workplace in an urban society. Indo Am J Pharm Sci. 2018;5(4):2905–2911.
71. Akhtar T, Khan MA. Pregnancy and maternity at workplace: a qualitative study to know the employers’ perspective. J Evol Med Dent Sci. 2020;9(13):619–624. doi:10.14260/jemds/2020/137
72. Cheung HK, Anderson AJ, King EB, Mahabir B, Warner K, Jones KP. Beyond the baby bump: subtle discrimination against working mothers in the hiring process. J Bus Psychol. 2022;37(6):1181–1198. doi:10.1007/s10869-022-09790-7
73. Crowley JE. Perceiving and responding to maternal workplace discrimination in the United States. Womens Stud Int Forum. 2013;40:192–202. doi:10.1016/j.wsif.2013.08.001
74. Dunn MG, Rochlen AB, O’Brien KM. Employee, mother, and partner: an exploratory investigation of working women with stay-at-home fathers. J Career Dev. 2013;40(1):3–22. doi:10.1177/0894845311401744
75. Frodermann C, Müller D. Establishment closures in Germany: the motherhood penalty at job search durations. Eur Sociol Rev. 2019;35(6):845–859. doi:10.1093/esr/jcz043
76. Gatrell C, Ladge JJ, Powell GN. Profane pregnant bodies versus sacred organizational systems: exploring pregnancy discrimination at work (R2). J Bus Ethics. 2024;81(1):1–16. doi:10.1007/s10551-023-05518-6
77. Ishizuka P. The motherhood penalty in context: assessing discrimination in a polarized labor market. Demography. 2021;58(4):1275–1300. doi:10.1215/00703370-9373587
78. Little LM, Major VS, Hinojosa AS, Nelson DL. Professional image maintenance: how women navigate pregnancy in the workplace. Acad Manage J. 2015;58(1):8–37. doi:10.5465/amj.2013.0599
79. Morrison LJ, Abbott AG, Mack Z, Schneider P, Hiemstra LA. What are the challenges related to family planning, pregnancy, and parenthood faced by women in orthopaedic surgery? A systematic review. Clin Orthop Relat Res. 2023;481(7):1307–1318. doi:10.1097/CORR.0000000000002564
80. Salihu HM, Myers J, August EM. Pregnancy in the workplace. Occup Med. 2012;62(2):88–97. doi:10.1093/occmed/kqr198
81. Bresnahan M, Zhuang J, Anderson J, Zhu Y, Nelson J, Yan X. The “Pumpgate” incident: stigma against lactating mothers in the US workplace. Women Health. 2018;58(4):451–465. doi:10.1080/03630242.2017.1306608
82. Casilla-Lennon M, Hanchuk S, Zheng S, et al. Pregnancy in physicians: a scoping review. Am J Surg. 2022;223(1):36–46. doi:10.1016/j.amjsurg.2021.07.011
83. Champaloux EP, Acosta AS, Gray ST, Meyer TK, Bergmark RW. Otolaryngology residents’ experiences of pregnancy and return to work: a multisite qualitative study. Laryngoscope Investig Otolaryngol. 2022;7(5):1322–1328. doi:10.1002/lio2.878
84. Day MA, Gil-Rivas V, Quinlan MM. “Always on parade”: pregnancy experience of active-duty air force members. Am J Orthopsychiatry. 2023;93(1):41–49. doi:10.1037/ort0000654
85. Dillard N, Walker CM. Black mothers at work: a contemplative and anti-oppressive approach to dismantling workplace oppression. J Manag Spiritual Relig. 2022;19(2):97–123. doi:10.51327/OYWW2974
86. Fox AB, Quinn DM. Pregnant women at work: the role of stigma in predicting women’s intended exit from the workforce. Psychol Women Q. 2015;39(2):226–242. doi:10.1177/0361684314552653
87. Gabriel AS, Volpone SD, MacGowan RL, Butts MM, Moran CM. When work and family blend together: examining the daily experiences of breastfeeding mothers at work. Acad Manage J. 2020;63(5):1337–1369. doi:10.5465/amj.2017.1241
88. Jones KP, King EB, Gilrane VL, McCausland TC, Cortina JM, Grimm KJ. The baby bump: managing a dynamic stigma over time. J Manage. 2016;42(6):1530–1556. doi:10.1177/0149206313503012
89. Jones KP. To ‘tell or not to tell?’ Examining the role of discrimination in the pregnancy disclosure process at work. J Occup Health Psychol. 2017;22(2):239–250. doi:10.1037/ocp0000030
90. Kraus MB, Thomson HM, Dexter F, et al. Pregnancy and motherhood for trainees in anesthesiology: a survey of the American Society of Anesthesiologists. J Educ Perioper Med. 2021;23(1). doi:10.46374/volxxiii_issue1_kraus
91. Rangel EL, Castillo-Angeles M, Changala M, Haider AH, Doherty GM, Smink DS. Perspectives of pregnancy and motherhood among general surgery residents: a qualitative analysis. Am J Surg. 2018;216(4):754–759. doi:10.1016/j.amjsurg.2018.07.036
92. Todd AR, Cawthorn TR, Temple-Oberle C. Pregnancy and parenthood remain challenging during surgical residency: a systematic review. Acad Med. 2020;95(10):1607–1615. doi:10.1097/ACM.0000000000003351
93. Whitley M, Banks A. Work as an understudied driver of racial inequities in breastfeeding. New Solut. 2022;32(3):189–200. doi:10.1177/10482911221124558
94. Zhuang J, Bresnahan MI, Yan X, et al. Keep doing the good work: impact of coworker and community support on continuation of breastfeeding. Health Commun. 2019;34(11):1270–1278. doi:10.1080/10410236.2018.1476802
95. Fitzpatrick K, Sweet B. Motherhood in the music academy. J Res Music Educ. 2024;71(4):373–397. doi:10.1177/00224294231154277
96. Gatrell C. Managing the maternal body: a comprehensive review and transdisciplinary analysis. Int J Manag Rev. 2011;13(1):97–112. doi:10.1111/j.1468-2370.2010.00286.x
97. Gatrell C. Policy and the pregnant body at work: strategies of secrecy, silence and supra‐performance. Gend Work Organ. 2011;18(2):158–181. doi:10.1111/j.1468-0432.2009.00485.x
98. Gloor J, Li X, Lim S, Feierabend A. An inconvenient truth? Interpersonal and career consequences of ‘maybe baby’ expectations. J Vocat Behav. 2018;104:44–58. doi:10.1016/j.jvb.2017.10.001
99. Juengst SB, Royston A, Huang I, Wright B. Family leave and return-to-work experiences of physician mothers. JAMA Netw Open. 2019;2(10):e1913054. doi:10.1001/jamanetworkopen.2019.13054
100. Little L, Hinojosa A, Paustian-Underdahl S, Zipay KP. Managing the harmful effects of unsupportive organizations during pregnancy. J Appl Psychol. 2018;103(6):631–643. doi:10.1037/apl0000285
101. Zhuang J, Bresnahan MI, Zhu Y, et al. The impact of coworker support and stigma on breastfeeding after returning to work. J Appl Commun Res. 2018;46(4):491–508. doi:10.1080/00909882.2018.1498981
102. Hassard J, Wang W, Delic L, et al. Pregnancy-related discrimination and expectant workers’ psychological well-being and work engagement: understanding the moderating role of job resources. Int J Workplace Health Manag. 2023;16(2/3):188–204. doi:10.1108/IJWHM-01-2022-0005
103. Jones KP, Brady JM, Lindsey AP, Cortina LM, Major CK. The interactive effects of coworker and supervisor support on prenatal stress and postpartum health: a time-lagged investigation. J Bus Psychol. 2022;37(3):469–490. doi:10.1007/s10869-021-09756-1
104. Percival Carter E. Power and the perception of pregnancy in the academy. Gender Work Organ. 2024;31(5):1951–1975. doi:10.1111/gwao.13001
105. Chesak SS, Yngve KC, Taylor JM, Voth ER, Bhagra A. Challenges and solutions for physician mothers: a critical review of the literature. Mayo Clin Proc. 2021;96(6):1578–1591. doi:10.1016/j.mayocp.2020.10.008
106. Kim JH, Oh SS, Bae SW, Park EC, Jang SI. Gender discrimination in the workplace: effects on pregnancy planning and childbirth among South Korean women. Int J Environ Res Public Health. 2019;16(15). doi:10.3390/ijerph16152672
107. Rowson TS, Jaworska S, Gibas I. Hot topic: examining discursive representations of menopause and work in the British media. Gender Work Organ. 2023;30(6):1903–1921. doi:10.1111/gwao.13021
108. Riach K, Jack G. Women’s health in/and work: menopause as an intersectional experience. Int J Environ Res Public Health. 2021;18(20):10793. doi:10.3390/ijerph182010793
109. Geukes M, Oosterhof H, van Aalst MP, Anema JR. Attitude, confidence and social norm of Dutch occupational physicians regarding menopause in a work context. Maturitas. 2020;139:27–32. doi:10.1016/j.maturitas.2020.05.015
110. Atkinson C, Carmichael F, Duberley J. The menopause taboo at work: examining women’s embodied experiences of menopause in the UK police service. Work Employ Soc. 2021;35(4):657–676. doi:10.1177/0950017020971573
111. Beck V, Brewis J, Davies A. Women’s experiences of menopause at work and performance management. Organization. 2021;28(3):510–520. doi:10.1177/1350508419883386
112. Beck V, Brewis J, Davies A. The remains of the taboo: experiences, attitudes, and knowledge about menopause in the workplace. Climacteric. 2020;23(2):158–164. doi:10.1080/13697137.2019.1656184
113. Griffiths A, MacLennan SJ, Hassard J. Menopause and work: an electronic survey of employees’ attitudes in the UK. Maturitas. 2013;76(2):155–159. doi:10.1016/j.maturitas.2013.07.005
114. Jack G, Riach K, Bariola E, et al. Menopause in the workplace: what employers should be doing. Maturitas. 2015;85:88–95. doi:10.1016/j.maturitas.2015.12.006
115. Steffan B. Managing menopause at work: the contradictory nature of identity talk. Gender Work Organ. 2020;28(1):195–214. doi:10.1111/gwao.12539
116. Steffan B, Loretto W. Menopause, work and mid‐life: challenging the ideal worker stereotype. Gender Work Organ. 2024;32(1):116–131. doi:10.1111/gwao.13136
117. Hardy C, Griffiths A, Thorne E, Hunter M. Tackling the taboo: talking menopause-related problems at work. Int J Workplace Health Manag. 2018;12(1):28–38. doi:10.1108/IJWHM-03-2018-0035
118. Bariola E, Jack G, Pitts M, Riach K, Sarrel P. Employment conditions and work-related stressors are associated with menopausal symptom reporting among perimenopausal and postmenopausal women. Menopause. 2017;24(3):247–251. doi:10.1097/GME.0000000000000751
119. Hobson G, Dennis N. “I can’t be dealing with this brain fog”: a workplace focus group study investigating factors underpinning the menopausal experience for NHS staff. Maturitas. 2024;180. doi:10.1016/j.maturitas.2023.107889
120. Hardy C, Griffiths A, Hunter M. What do working menopausal women want? A qualitative investigation into women’s perspectives on employer and line manager support. Maturitas. 2017;101:37–41. doi:10.1016/j.maturitas.2017.04.011
121. Żołnierczuk-Kieliszek D, Janiszewska M, Mielniczuk A, Dziedzic MA, Firlej E. Professional activity of Polish peri- and postmenopausal women. Menopause Rev Przeglad Menopauzalny. 2016;15(3):138–142. doi:10.5114/pm.2016.62660
122. Gilbert SL, Dimoff JK, Brady JM, Macleod R, McPhee T. Pregnancy loss: a qualitative exploration of an experience stigmatized in the workplace. J Vocat Behav. 2023;142:103848. doi:10.1016/j.jvb.2023.103848
123. Viotti S, Guidetti G, Converso D, Sottimano I. Fostering work ability among menopausal women: does any work-related psychosocial factor help? Int J Womens Health. 2020;12:399–407. doi:10.2147/IJWH.S230796
124. Guidetti G, Viotti S, Converso D, Sottimano I. Work and health-related factors of presenteeism: a mediation analysis on the role of menopausal symptoms between job demands and presenteeism among a sample of social service women employees. Int J Workplace Health Manag. 2022;15(1):70–86. doi:10.1108/IJWHM-01-2021-0003
125. Caruana T. Reducing Stigma Within Pharmacy Opioid Agonist Treatment Encounters. Stigma Health. doi:10.1037/sah0000552
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Stigma and Discrimination of HIV/AIDs Recipients of Care in Western Uganda: Experiences and Roles of Expert Clients
Atwijukiire H, Jemba Nalubega H, Byaruhanga V, Atwiine P, Muhame K, Mpumwire P, Bukombi Muhindi E, Niyonzima V
HIV/AIDS - Research and Palliative Care 2022, 14:517-527
Published Date: 14 November 2022
The Unheard Stories: Experiences of Young People Living with Human Immunodeficiency Virus in Dealing with Discrimination in the Philippines

Sombrea DP, Santarin SLM, Verde TGM, Tidalgo AD, Tolosa CS
HIV/AIDS - Research and Palliative Care 2024, 16:33-43
Published Date: 14 February 2024
“Living with Silence and Shame”: A Meta-Synthesis of Women’s Lived Experiences of Infertility-Related Stigma
Lee J, Kim S, Nam SH
International Journal of Women's Health 2025, 17:2699-2713
Published Date: 27 August 2025
Cancer Screening Practices Among Women Living with HIV in Istanbul, Turkey: A Qualitative Study
Yagci-Caglayik D, Hidiroglu S, Doganc FB, Varol Y, Erdem K, Recai MS, Asker OF
International Journal of General Medicine 2025, 18:5673-5685
Published Date: 20 September 2025