")
Back to Journals » Open Access Emergency Medicine » Volume 12
Disaster Preparedness in Selected Hospitals of Western Ethiopia and Risk Perceptions of Their Authorities
Authors Woyessa AH , Teshome M , Mulatu B, Abadiga M , Hiko N, Kebede B
Received 20 May 2020
Accepted for publication 21 September 2020
Published 8 October 2020 Volume 2020:12 Pages 219—225
DOI https://doi.org/10.2147/OAEM.S260314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Ashenafi Habte Woyessa,1 Misganu Teshome,2,3 Befirdu Mulatu,4 Muktar Abadiga,5 Nesru Hiko,1 Burtukan Kebede5
1Department of Emergency and Critical Care Nursing, Institute of Health Science, Wollega University, Nekemte, Ethiopia; 2School of Nursing and Midwifery, Institute of Health Science, Wollega University, Nekemte, Ethiopia; 3Department of Midwifery, Institute of Health Science, Wollega University, Nekemte, Ethiopia; 4Department of Public Health, Institute of Health Science, Wollega University, Nekemte, Ethiopia; 5Department of Nursing, Institute of Health Science, Wollega University, Nekemte, Ethiopia
Correspondence: Ashenafi Habte Woyessa
Department of Emergency and Critical Care Nursing, Institute of Health Science, Wollega University, Nekemte, Ethiopia
Tel +251 922183065
Fax +251 576617980
Email [email protected]
Purpose: Despite the fact that hospitals are always at a high risk of disasters, the preparedness status in many of the Ethiopian hospitals is not well recognized. It is with this research gap in mind that this study motivated the authors to assess disaster preparedness level in selected hospitals of the western part of Ethiopia and their authorities’ risk perceptions.
Methods: This was a facility-based study conducted by using mixed qualitative and quantitative research designs among selected hospitals of western Ethiopia. While disaster and emergency readiness was evaluated using a modified World Health Organization observation check list. The key informant interview method was used to assess the disaster risk perception of the hospitals’ authorities in the study area.
Results: The overall level of emergency and disaster preparedness in the selected hospitals was weak with an average calculated preparedness score of 45.6%. The score of readiness in terms of disaster response and recovery planning was 33.3%. Moreover, we have not got a documented disaster plan in all of the hospitals and the hazard-specific response sub plans were also not consistently in place. Of prime concerns, this study has revealed that there was no patient evacuation plan in all of the selected hospitals. The human resource preparations of the hospitals were relatively better with an average readiness score of 60%. The study has found that no committee was responsible for emergency readiness at all of the sampled hospitals. The hospital authorities’ disaster risk perception was found to vary according to the type of calamities and this was from moderate to high level.
Conclusion: This study concludes that although their authorities’ risk perception of disasters was high, the selected hospitals were ill-prepared for the potential disaster strikes in this study area.
Keywords: disaster, emergency, hospitals, perception, preparedness, western Ethiopia
Introduction
Disaster is a sudden ecological phenomenon of sufficient magnitude to require external assistance and medical disaster, one form of catastrophe, is an entity that denotes a situation in which the health care system response capabilities are overwhelmed.1,2 In human history, disasters have caused huge destructions. They have a long history of disrupting people’s lives and causing human suffering with communities finding it difficult to cope with.3
In the past quarter-century nearly 4 million lives have been lost and trillions of dollars in related damages have been seen worldwide due to natural disasters.4,5 Besides their devastating effects on human lives and economy, disasters place heavy burdens on health care facilities. There have been countless cases of health infrastructures from sophisticated hospitals to small but vital health centers that have suffered this fate.6
Over the past several decades, sub-Saharan African countries have experienced thousands of disasters. The Global Facility for Disaster Reduction and Recovery has indicated that natural hazards mainly drought, floods, landslides, epidemics, earthquakes, and fires are present in Ethiopia. The country is one of the 20 countries identified for their highest vulnerability to natural hazards and with a low economic resilience.7,8
Disasters are certainly a part of human life and they are a concern of all communities on earth. Although there might be a variation in the degree of exposure, emergencies and disasters could happen anywhere and at any point in time without seeking permission to occur. In a community with a lesser disaster experience, people usually say “it will never happen here”. In reality however, the daily news tells us that terrible events do happen anywhere and at any time.3,5,9
Over the past four decades, reducing the effects of disasters through community-based risk reduction and emergency preparedness has been recognized as an essential aspect for the attainment and protection of sustainable development. Disasters are events that neither human knowledge nor technology can exactly predict the accurate time of their occurrences. As such, preparedness is most often considered as a central activity in disaster science. Nowadays, a marked shift is being made in the way disasters are handled. In past times, more emphasis has been given to the humanitarian responses and relief activities rather than on the strategies and actions to mitigate them.6,10
The increasing of disaster occurrences around the world warns all countries and all institutions to be ready to reduce the devastating outcomes. However, past disasters and more recent events demonstrate that we are still often not fully prepared. Despite the fact that lack of disasters preparation unquestionably affects all nations around our globe, ill-preparedness is a double jeopardy to low-income countries with poor resilience.11,12
Lack of coordination emanating from low perceived risks across the spectrum of public health has been the main barrier to health care disaster preparedness.7,13 An all-hazard approach and institutionalized disaster preparedness in which the hospitals play a pivotal role are advised to be in place. Enabling health care systems to cope with emergencies is one of the strategic objectives contained in the Ethiopian health policy and strategy. Nevertheless, an “all-hazard approach” and institutionalized disaster preparedness in which the health care facilities take a preliminary role is missing in the Ethiopian health care system.14–16
Even though it merits intellectual attention and resources, very few studies have been done on the health sector disaster preparedness in Ethiopia. As a result, there is a shortage of evidences regarding the current level of hospitals’ preparedness including the perceived risk of disaster events among their authorities. It is with this research gap in mind that this study was motivated to assess the emergency and disaster preparedness of the selected hospitals in consort with the perceived risks among the selected hospital managers. The findings of this study have paramount importance in drawing hospital managers’ attention towards disaster preparedness in the hospital management planning.
Materials and Methods
Study Setting and Period
This study was carried out from March to April 2019 in four comparable zonal hospitals selected from East Wollega, West Wollega, Kelem Wollega, and Horoguduru Wollega administrative zones. The selected hospitals are located in the capital towns of the respective zones. The four zones are the administrative divisions in the Oromia regional state, western part of Ethiopia and they have collectively a population of more than 4 million.
Study Design
This was a facility-based cross-sectional study which was conducted by using a mixed qualitative and quantitative research design. The risk perception of the authorities in the selected hospitals was assessed through gathering quantitative data. The disaster preparedness level of the hospitals was evaluated quantitatively using scores from a checklist supplemented qualitatively by observation.
Sampling Techniques and Procedures
An area sampling technique was used to select the four hospitals. Six administrative zones in west Ethiopia, namely, Buno Bedele, Kelem Wollega, West Wollega, East Wollega, and Horo Guduru Wollega were initially selected as a geographic cluster. Then, four administrative zones (West Wollega, East Wollega, Kelem Wollega, and Horo Guduru Wollega) were purposively chosen. Finally, four zonal hospitals (one hospital from each of the four zones) were conveniently selected and included in this study. To select the hospitals conveniently we have taken into consideration the similarity of the hospitals in their level of services, representativeness to the selected zones, and proximity of the hospitals. Accordingly, the selected hospitals were zonal hospitals located around east Wollega administrative zone, the radius of this study area, and they were similar in their level of services including number of beds and overall standards of service and management systems.
Data Collection Tool
The readiness level of the hospitals was assessed by the World Health Organization hospital safety index evaluation checklists. The checklist was modified into seven prioritized evaluation domains containing a total of 39 questions. The coordination of emergency and disaster management activities, aimed to evaluate how well the selected hospitals have integrated the coordinated emergency and disaster activities in their routine health care delivery system was one parameter. Emergency and disaster response and recovery planning was included to appraise the hospitals’ level of readiness to possible emergencies and disaster. The other aspects of the check list were regarding human resources, logistics, and finance, and the communication and information management system. Patient care and support services, which was comprised of eight questions in the checklist, was the other component of the parameters utilized to assess the status of the hospitals on the care of emergency patients and support services. Similarly, patients’ evacuation procedures, decontamination, and security concerns have been addressed in the evaluation checklist.
We have used the key informant interview method to evaluate the risk perception of hospital authorities for disaster events. Chief Executive Officers (CEO) of the hospitals where available during the data collection period or their representatives in the absence of the CEO were purposively selected for the key informant interview. Risk perception was assessed by using a descriptive question stated as “what is the perceived risk of disaster events related to these three major types of disasters?” The three major types of disasters, namely natural disasters (ND), mass casualty or vehicular accidents (VA), manmade disasters (MD) were provided for the key informants. Each event was self-reported as low, moderate, or high risk and coded as a “1,” “2,” or “3,” respectively.
Data Collection Techniques
The checklist was carefully filled with the support from the representatives of the selected hospitals and the key informant interview was made by four trained data collectors.
Data Processing and Analysis
Quantitative data from 39 questions filled for all hospitals was analyzed computing an average score percentage obtained by the hospitals. A score for each question was considered out of 3 points with 1 representing low readiness and 3 indicating the highest level of preparation. Finally, level of preparedness was categorized as “weak” if the average percentage score was 33.3% to 66.6% and “good” if the percentage score was from 66.7–100%. Qualitative data from the observation evaluation checklist were organized into six themes according to the seven parameters contained in the checklist. The description of key qualitative findings obtained from the observation were summarized under each theme and presented in the form of text. The quantitative data regarding the risk perceptions of the hospital authorities was done using the weighting system that yields an “All-Hazards Measure” (AHM), whereby: AHM = 5 (VA) +5 (ND) + 1 (ET + BT + NT + CT + RT). The range of possible responses was from 15–45, with 15–25 representing low risk, 26–35 a moderate risk, and 36–45 representing a high perception of risks.
Study Variables
While the level of preparedness was considered as a dependent variable, the perceptions of risks toward the potential disasters around this study area were viewed as independent variables.
Results
Level of Hospital Disaster Readiness
Overall, the emergency and disaster preparedness level of the selected hospitals was found to be under the category of weak level (Table 1). The key evaluation results related to each of the checklist questions of the parameters are thematically summarized and presented under the following six sub headings.
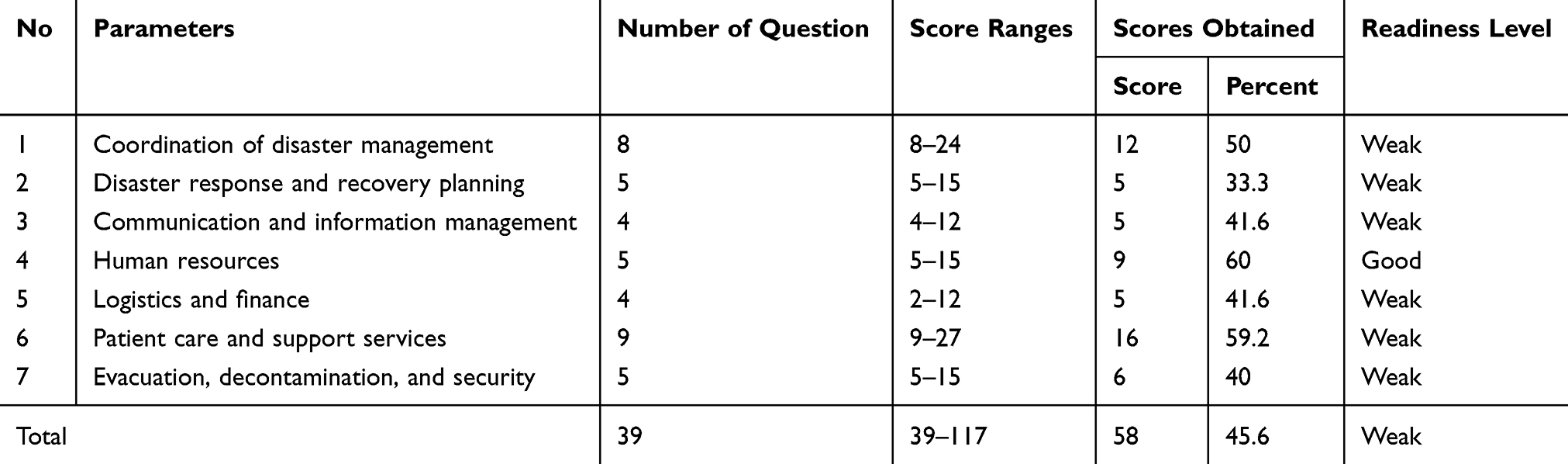 |
Table 1 Level of Emergency and Disaster Preparedness of Selected Hospitals in Western Ethiopia, 2019 |
Coordination of Emergency and Disaster Management Activities
One of the primary aims of this survey was to check how well the selected hospitals have integrated the coordinated emergency and disaster activities in their routine health care delivery system. In relation to this, this study has found that there were no responsible committees for emergency readiness in all of the sampled hospitals. There were not even any staff members who havd been assigned as the emergency/disaster management coordinator. The preparedness programs for strengthening emergency and disaster response and recovery which are expected to be in place were totally absent. Furthermore, we have found no arrangements regarding the hospital incident management system. An emergency operation Centre (EOC) that must have been available in a safe, secure, and accessible location with immediate operational capacity were also not designated. Another aspect of emergency coordination that this study has evaluated was the coordination mechanisms and the cooperative arrangements with local emergency/disaster management agencies. In this regard, there have been only a few arrangements but they were not fully operational.
Emergency and Disaster Response and Recovery Planning
The second domain of questions used to appraise the hospitals’ level of readiness to possible emergencies and disasters was the response and recovery planning. The availability of disaster response plans, hospital hazard-specific sub plans were checked out. Moreover, the hospitals were assessed for the presence of the procedures to activate and deactivate a disaster plan, how they are exercised and means of evaluation. Overall, we have not got a documented disaster plan in these public hospitals. Similarly, the hazard-specific response sub plans were not in place.
Communication and Information Management
The communication and information management system was viewed in relation to the system of communication, availability of procedures for communicating with the public and media, and the management of patient information. The findings indicate that the emergency/disaster communication and information management have been assigned to a staff member in two of the hospitals but this was not his or her main task. Of particular concern, the procedures for communicating with the public and media were absent and no spokesperson nominated in all of the selected hospitals. Similarly, the procedure for management of patient information during an emergency situation was lacking at the hospitals. Above all, no personnel have been trained and no resources were available for communication and information management during emergency situations.
Human Resources, Logistics, and Finance
Checking the availability of trained staff with their contact address in the hospitals was another facet of preparedness of assessment. In all of the hospitals under the study, staff contacts list were available but not up to date and not a full version. Even though about 80–100% of the staff members were believed to be available for any potential duty, the overall human resources were not available to meet the anticipated needs of an emergency. The tendency to mobilize and recruit personnel during an emergency or disaster shows that the procedures exist. According to the checklist, the well-being of hospital personnel during an emergency or disaster have not been ensured as a designated space and measures were not uniformly in place in all of the hospitals. This study has investigated the availability of logistics and financial arrangements in the observed hospitals. Regarding the formal agreements with local suppliers and vendors for emergencies, we have found that some arrangements exist but they were not fully operational.
As one of the important components of logistics, the ordinary transportation vehicles and type C ambulances were available for transportation during an emergency, but not in sufficient numbers. Availability of arrangements with food and drinking-water during unexpected emergency conditions has been checked as another logistics fulfillment and we have confirmed that these requirements were not met. Finally, it has also been observed that the required financial resources for emergencies and disasters were not ensured at these hospitals. Sufficient budget was not available to manage routine emergencies that are assumed to take less than 24 hours of hospital duration.
Patient Care and Support Services
The status of the hospitals on the care of the emergency patients and support services was evaluated by eight questions in the checklist. Maintaining emergency and critical care services, expansion of usable space, arrangement of the referral system during disasters are expected to be ensured by the hospitals. In relation to this, our study has found that there have been no procedures for the fulfillment of these particular expectations. This study has confirmed that the expansion was not totally identified and there was no designated triage location and there were not even any triage processes. On the other hand, the assessment result of this study related to the psychosocial support services arrangement shows that the procedure for this specific requirement was not in place in the selected hospitals. The policies and procedures on infection prevention and control measures were unvaryingly available in all of the hospitals. Likewise, the procedures to establish a system for referral, transfer and reception of patients were arranged.
Evacuation Procedures, Decontamination, and Security Concerns
This study has investigated the hospitals preparations on the matters of patients’ evacuation procedure, capacity testing, and security concerns. It has identified that there have been no evacuation plan in all of the included hospitals. Correspondingly, the staff training and the periodic capacity testing procedures have never been done by the hospitals. Furthermore, this survey has looked into issues related to decontamination for chemical and radiological hazards, personal protection equipment and isolation for infectious diseases and epidemics. The supply for personal protective equipment and arrangement for isolation during infectious diseases outbreak were available but insufficient and established for only momentary use. Correspondingly, the staff training and the capacity testing procedures that are anticipated to be periodically conducted have never been done by the hospitals. Similarly, the emergency security procedures including computer system network security have been evaluated. While there was a documented emergency security procedure in only one of the four hospitals, we have not found the training of personnel and other procedures at the remaining facilities.
Disaster Risk Perception of Hospitals’ Authorities
The key informants interview were asked their risk perceptions of the three major types of disaster namely: natural disasters (ND), mass casualty or vehicular accidents (VA), manmade disasters (MD) that is comprised of chemical threats (CT), biological threats (BT), radiological threats (RT), nuclear threats (NT), and explosive threats (ET) were provided for the key informants. The disaster risk perception of these authorities was found to vary according to the type of calamities and the perception ranges from moderate to high level (Table 2).
 |
Table 2 Hospital Authorities’ Disaster Risk Perceptions in Selected Hospitals of Western Ethiopia, 2019 |
Discussion
As a human being, we might not have the power to prevent tragedies from arising. However, we have at least the ability to protect our health facilities by anticipating, mitigating, preparing for, responding to, and recovering from hazards. Hospitals are some of the most important institutions in disaster responses and therefore warrant special preparations.17–19 In this study, we have assessed the disaster and emergency preparedness level in selected public hospitals and we have evaluated the disaster risk perception among the hospitals’ top managers.
In our study, we found that the overall emergency and disaster preparedness level in the selected hospitals was weak with an average calculated preparedness score of 45.6%. This is in line with the finding of one Ethiopian-based study and consistent with other published studies undertaken elsewhere.1,20,21 Yet, the finding is lower as compared to two other similar studies done in Iran and South Africa.22,23 The observed difference could be due to the variation in the experiences of disaster incidents between Ethiopia and the other countries. A documented disaster plan, the hazard-specific response, and recovery planning were consistently not in place in the evaluated hospitals. This is a terrifying result as compared to the findings reported from many African countries which have at least a documented contingency plan.11,17,24
Most experts in the field of emergency management agree that the primary source of information for the general public about disasters is the mass media.25–27 In this regard, our evaluations regarding the status of the hospitals on the communication and information management system reveals that although a specific discipline has nominally represented the responsibility, the expectations have not been fulfilled and the systems have not been established. In the time of disaster strikes, the hospitals are anticipated to stay functional and continue to provide care of the patients.28,29 In the present study, we noticed that there were neither the procedures to maintain service provision nor the arrangements for evacuation of patients.
One of the big challenges the managers could face in disaster events is a logistic deficiency which involves lack of funds and inadequacy of appropriate places to provide medical services, and shortage human resources.30,31 In this study, we have assessed a logistic preparation in terms of the financial arrangements, agreements with local suppliers and vendors for potential emergencies and disasters. The results showed that arrangements exist, but they were not fully operational. This is a consistent finding with the findings reported in a number of similar studies undertaken in developing countries.1,11,17,24
Disaster risk perception is one of the essential aspects of preparedness. A great number of studies have revealed that the perceived risk has a positive correlation with hospital disaster preparedness.16,21,28,32 This survey has examined the subjective perception of selected hospital managers on disaster risks and found a moderate-to-high risk perception.
Conclusion
This study concludes that even though the authorities' disasters risk perception was high at this study area, the selected hospitals were not satisfactorily prepared for the potential disaster strikes and unexpected emergency conditions. It is therefore recommended that indicating that the health care system planners in general and hospital managers in particular must come together and design a sound intervention strategy.
Ethics Approval and Consent to Participate
This research was approved by Wollega University research ethics committee (Reference Number: Ref/WU: 117,969/Re-29). To collect the required data, a formal letter of support was written to each of the four zonal health offices and to respective hospitals. We have taken written informed consents to participate in the study from both the hospital representatives and the members of key informant interview.
Acknowledgment
We would like to acknowledge Wollega University for funding the data collection part of this research. We would also like to extend our heartfelt gratitude to the selected hospital administrations for their cooperation in providing the required data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Habte A, Addisie A, Azazh A. Assessment of knowledge, attitude and the practice of disaster preparedness among tikur anbessa specialized hospital health care workers, Addis Ababa, Ethiopia. Am J Nurs Sci. 2018;7(1):39–48. doi:10.11648/j.ajns.20180701.15
2. Alwan A. Assistant director-general, health action in crises World Health Organization, world disaster campaign 2008–2009, “hospitals safe from disaster”. Available from: www.unisdr.org/wdrc-2008-2009.
3. World bank and global facility for disaster reduction and recovery; 2010. Available from: http://www.cred.be/sites/default/files/ADSR_2011.
4. Literature and best practice review and assessment: identifying people’s needs in humanitarian response. Available from: www.unisdr org. uk/public/reports/60-1.pdf.
5. World bank and global facility for disaster reduction and recovery. November 2012.
6. Sahdeo J, Green B, Millo Y, Shamloo C, Donnellan J, DeAtley C. Development of an “all-hazards” hospital disaster preparedness training course utilizing multi-modality teaching. Prehosp Disaster Med. 2008;23(1):63–67. doi:http://dx.doi.10.1017/S1049023X00005598
7. Facility for disaster reduction and recovery (GFDRR) secretariat, “management programs for priority countries”; 2009. Available from: www.gfdrr.org.
8. Slepski LA. Emergency preparedness and professional competency among health care providers during hurricanes Katrina and Rita: pilot study results. Disaster Manag Response. 2007;5(4):99–110. doi:10.1016/j.dmr.2007.08.001
9. Prizzia R, Helfind G. Emergency preparedness and disaster management in Hawaii, case study; 2004. Available from: http://www.emeraldinsight.com/insight/viewContentServlet.
10. Wong K, Turner PS, Boppana A, et al. Preparedness for the next major incident: are we ready? Emerg Med J. 2006;23(9):709–712. doi:10.1136/emj.2005.034025
11. Fung OW, Loke AY, Lai CK. Disaster preparedness among Hong Kong nurses. J Adv Nurs. 2008;62(6):698–703. doi:10.1111/j.1365-2648.2008.04655.x
12. Williams J, Nocera M, Casteel C. The effectiveness of disaster training for health care workers: a systemic review. Ann Emerg Med. 2008;52(3):211–222. doi:10.1016/j.annemergmed.2007.09.030
13. Leiba A, Drayman N, Amsalem Y, et al. Establishing a high level of knowledge regarding bioterrorist threats in emergency department physicians: methodology and the results of a national bio-preparedness project. Prehosp Disaster Med. 2007;22(3):207–211. doi:10.1017/S1049023X00004672
14. Chongjian W, Wei S, Hao X, et al. Evaluating the effectiveness of an emergency preparedness training program for public health staff in China. Public Health. 2008;122(5):471–477. doi:10.1016/j.puhe.2007.08.006
15. American Society of Public Health. 2009. Available from: http://www.asph.org/cphp/CPHP_ResourceReport.cfm.
16. Hermawati D, Hatthakit U, Chaowalit A. Nurses’ Preparedness of Knowledge and Skills in Caring for Patients Attacked by Tsunami in Banda Aceh, Indonesia and Its Relating Factors. Thesis, Prince Songkla University. Vol. 3. 2010: 5–10.
17. Alice Ncube GN, Chimenya T. Hospital disaster emergency preparedness: a study of Onandjokwe Lutheran hospital, Northern Namibia. Afr Saf Promot. 2016;14(2).
18. Candice Davenport BS, PerezdeAlejo ME, Morris RJ. Low Cost Measures to Improve Local Emergency Preparedness and Response in New Jersey. 2011:10–12.
19. Academic Medicine. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):515–526.
20. Zarei V. Emergency preparedness of hospitals in Tehran and its relation with crisis management measures. Int J Med Res Health Sci. 2016;5(9S):471–478.
21. Sjoberg L, Moen B, Rundmo T. Explaining risk perception: an evaluation of the psychometric paradigm in risk perception research; 2004. Available from: http://www.svt.ntnu.no/psy/.
22. Abhinav Sinha DK, Pal PK, Kasar R, Sharma TA, Sharma A. Knowledge, attitude and practice of disaster preparedness and mitigation among medical students. Disaster Prev Manag. 2008;17(4):503–507. doi:10.1108/09653560810901746
23. Rahmati F, Najarkolaei A, Ebadi A, Heidaranlu E. Assessment of a military hospital’s disaster preparedness using a health incident command system. TraumaMon. 2017;22(2):e31448.
24. Rosemary M. Knowledge, Attitudes, and Practices of Health Care Workers Regarding Disaster Preparedness at Johannesburg Hospital in Gauteng Province, South Africa. Vol. 1. 2008: 33–39.
25. Chaffe MW, Oster NS, et al. The role of hospitals in disasters. In: Ciottone GR, Anderson PD, Jacoby I, Der Heide EA, Noji E, Darling RG, editors. Disaster Medicine,
26. Spranger C, Villegas D, Kazda M, Harris A, Mathew S, Migala W. Assessment of physician preparedness and response capacity to bioterrorism or other public health emergency events in a major metropolitan area. Disaster Manag Response. 2007;5(3):82–86. doi:10.1016/j.dmr.2007.05.001
27. Ostad Taghizadeh A, Hosseini M, Navidi I, Mahaki AA, Ammari H, Ardalan A. Knowledge, attitude and practice of Tehran’s inhabitants for an earthquake and related determinants. PLoS Curr. 2012;4:e4fbbbe1668eef. doi:10.1371/4fbbbe1668eef
28. Eybpoosh M, Dikmen I, Talat Birgonul M. Identification of risk paths in international construction projects using structural equation modeling. J Constr Eng Manag. 2011;137(12):1164–1175. doi:10.1061/(asce)co.1943-7862.0000382
29. Barbera JA, Yeatts DJ, Macintyre AG. Challenge of hospital emergency preparedness: analysis and recommendations. Disaster Med Public Health Prep. 2009;3(S1):S74–S82. doi:10.1097/dmp.0b013e31819f754c
30. Ardalan A, Masoomi GR, Goya MM, et al. Disaster health management: Iran’s progress and challenges. Iran J Public Health. 2009;38(1):93–97.
31. Boin A, McConnell A. Preparing for critical infrastructure breakdowns: the limits of crisis management and the need for resilience. J Contingencies Crisis Manag. 2007;15(1):50–59. doi:10.1111/j.1468-5973.2007.00504.x
32. Kaji AH, Lewis RJ. Hospital disaster preparedness in Los Angeles county. Acad Emerg Med. 2006;13(11):1198–1203. doi:10.1197/j.aem.2006.05.007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.