Back to Journals » Substance Abuse and Rehabilitation » Volume 12
Disability Status, Unemployment, and Alcohol-Related Liver Disease (ALD) Mortality: A Large Sample Individual Level Longitudinal Study
Authors Kposowa AJ, Breault K ![]()
Received 18 August 2021
Accepted for publication 5 October 2021
Published 19 October 2021 Volume 2021:12 Pages 81—88
DOI https://doi.org/10.2147/SAR.S334851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Augustine J Kposowa,1 Kevin Breault2
1Department of Sociology, University of California, Riverside, CA, USA; 2Department of Sociology and Anthropology, Middle Tennessee State University, Murfreesboro, TN, USA
Correspondence: Kevin Breault
Department of Sociology and Anthropology, Middle Tennessee State University, 1301 E. Main Street, Murfreesboro, TN, 37132, USA
Tel +1 615 948 8208
Fax +1 615 898 5427
Email [email protected]
Purpose: Unlike previous research, we evaluate disability within expanded employment status factors and stratify gender, race and ethnicity in alcohol-related liver disease (ALD) mortality in a large sample individual level longitudinal study.
Materials and Methods: The National Longitudinal Mortality Study (NLMS) was used covering the period 1990– 2011. Statistical analysis involved the use of proportional hazards regression on a sample of almost 1.4 million people aged 18 and older, of whom 2638 died of ALD by the end of the follow-up period.
Results: With expanded employment status factors, disability (HR=3.76 [95%] CI 3.22, 4.39), unemployment (HR=1.90, CI 1.56, 2.31), and those not otherwise in the labor force (HR=2.31, CI 2.08, 2.56) were strongly related to ALD mortality compared to the employed. When stratified, gender, race, and ethnicity were not important modifiers in the relationships between disability, unemployment, those not in the labor force and subsequent ALD mortality. Consistent with other studies, males, minority status, living in a highly urban area, renting as opposed to owning a home, lower educational attainment, marital statuses other than marriage, low income, and age were related to ALD mortality.
Conclusion: In addition to unemployment which has been previously studied in a large longitudinal sample, disabled people who were unable to work and those not looking for work had a higher risk of ALD mortality. Alcohol consumption, abuse and morbidity in these populations are of considerable clinical concern.
Keywords: cirrhosis, hepatitis, disability, unemployment, gender
Introduction
Alcohol consumption is a continuing public health concern in the United States with an expected 75% increase in alcohol-related liver disease (ALD) by 2040.1 ALD is also associated with a high economic burden said to involve $5 billion of direct health care costs.2 Among demographic groups in the US, young people between the ages of 25 and 34 currently have the highest relative increase in ALD mortality.3
Epidemiological research has focused on males and minority status as significantly associated with ALD mortality,3–5 with some exceptions based on samples with small sizes.6,7 Marital status too has been related to ALD mortality with statuses other than marriage generally at high risk.8–10 In one recent study from South Korea, widowed status had a lower risk of ALD mortality.11 Research on socioeconomic status has found that ALD mortality increases with lower status,12,13 but unemployment and other employment categories have been less studied. One exception is United States research from the years 1935–1997 covering almost 200,000 people, in which unemployment was highly related to ALD mortality.14 Alcohol consumption is related to disability status,15–17 but studies of disability and ALD mortality have been limited, and we are unaware of research on ALD mortality and disability in large sample longitudinal studies.18 The purpose of this study is to evaluate ALD mortality by evaluating disability status and those otherwise unemployed and not looking for work, and by stratifying gender, race and ethnicity with appropriate covariates in a large longitudinal sample.
Materials and Methods
Sample
Data come from the Public Use Microdata Sample (PUMS) of the National Longitudinal Mortality Study (NLMS). The purpose of the NLMS is to develop a greater understanding of mortality related to disparities across diverse populations in the US. It is conducted by the US Bureau of the Census in collaboration with the US National Center for Health Statistics. A full description of the NLMS and PUMS has been provided elsewhere and in our previous work.19,20 The data include approximately 1.4 million people of whom almost 161,000 had mortality events from April 1990 to 2011. The sample was restricted to those aged 18 and over in order to evaluate marital status because that is the age when people are able to marry in all jurisdictions in the US. The resulting sample was 1,384,507 individuals, 160,750 all-cause mortality events, and 2638 who died of ALD.
Measurements
The outcome variable was ALD mortality, codes K70.1-4,9 from the International Statistical Classification of Diseases.21 These categories include cirrhosis, alcoholic fibrosis and hepatitis, fatty liver, and hepatic failure. Dummy variables were used for all variables. For example, employment status categories included the employed as the reference category, with 1 each for unemployed but looking for work; those who were disabled and unable to work; and those otherwise not in the labor force—retired, housekeepers, students, and others doing something not classified. Note that many people who are disabled are able to work and are therefore in the employed category. Race and ethnicity categories included non-Hispanic whites, and non-whites, combining African Americans, Asians, Hispanics and Native Americans. These groups were collapsed into minority status for small cell size problems, but results for each group were available upon request. Place of Residence categories involved areas in Standard Metropolitan Statistical Areas (SMSA), and rural places. Housing Tenure categories included those who owned their own homes and those who did not. Marital status categories included the married, divorced/separated, single/never married, and widowed. Educational Attainment categories were some college, high school graduates, and those with less than high school attainment. Family Income categories comprised seven income categories with those earning less than $20,000 the lowest, and $60,000 or more the highest. There were three age groups, 18–44, 45–64, and 65 and older.
Statistical Analysis
Cox proportional hazards regression was used (PHREG in SAS version 9.4) with estimates exponentiated for 95% confidence intervals and adjusted hazards ratios (HR).22 As noted previously, the utility of logistic versus Cox proportional hazards regression depends on whether the variables are related to the follow-up period.23,24 If so, results from the Cox and logistic models will be different. In the present study, no variables were related to the follow-up period and so results for the Cox model are presented. However, similar results for logistic regression are available upon request.
Results
As can be seen in Table 1, based on the statistics for the full sample, unemployment, disability, and those not in the labor force were significantly related to ALD mortality, respectively (HR=1.90 [95%], CI=1.56, 2.31; HR=3.76, CI=3.22, 4.39; and HR=2.31, CI=2.08, 2.56). Similar to the previous literature, males and non-white–minority status were related to ALD mortality, respectively (HR=2.83, CI=2.60, 3.09; and HR=1.55, CI=1.53, 1.85). Generally, similar results were found for marital status with respect to the divorced/separated and widowed, respectively (HR=1.73, CI=1.54, 1.94; and HR=1.51, CI=1.33, 1.70), with the exception that the single/never married were negatively related to ALD mortality (HR=0.79, CI=0.68, 0.92). Among socioeconomic variables, renting status, low educational attainment and low family income were significantly related to ALD mortality. Of these, the highest HR was for low family income (HR=1.42, CI=1.19, 1.69). Living in a central city of a SMSA had a significant effect on ALD mortality (HR=1.13, CI=1.03, 1.24), but living in a rural area had a negative impact with reference to central city residence (HR=0.88, CI=0.80, 0.97). Finally, as expected, the higher the age category, the stronger the effect on ALD mortality.
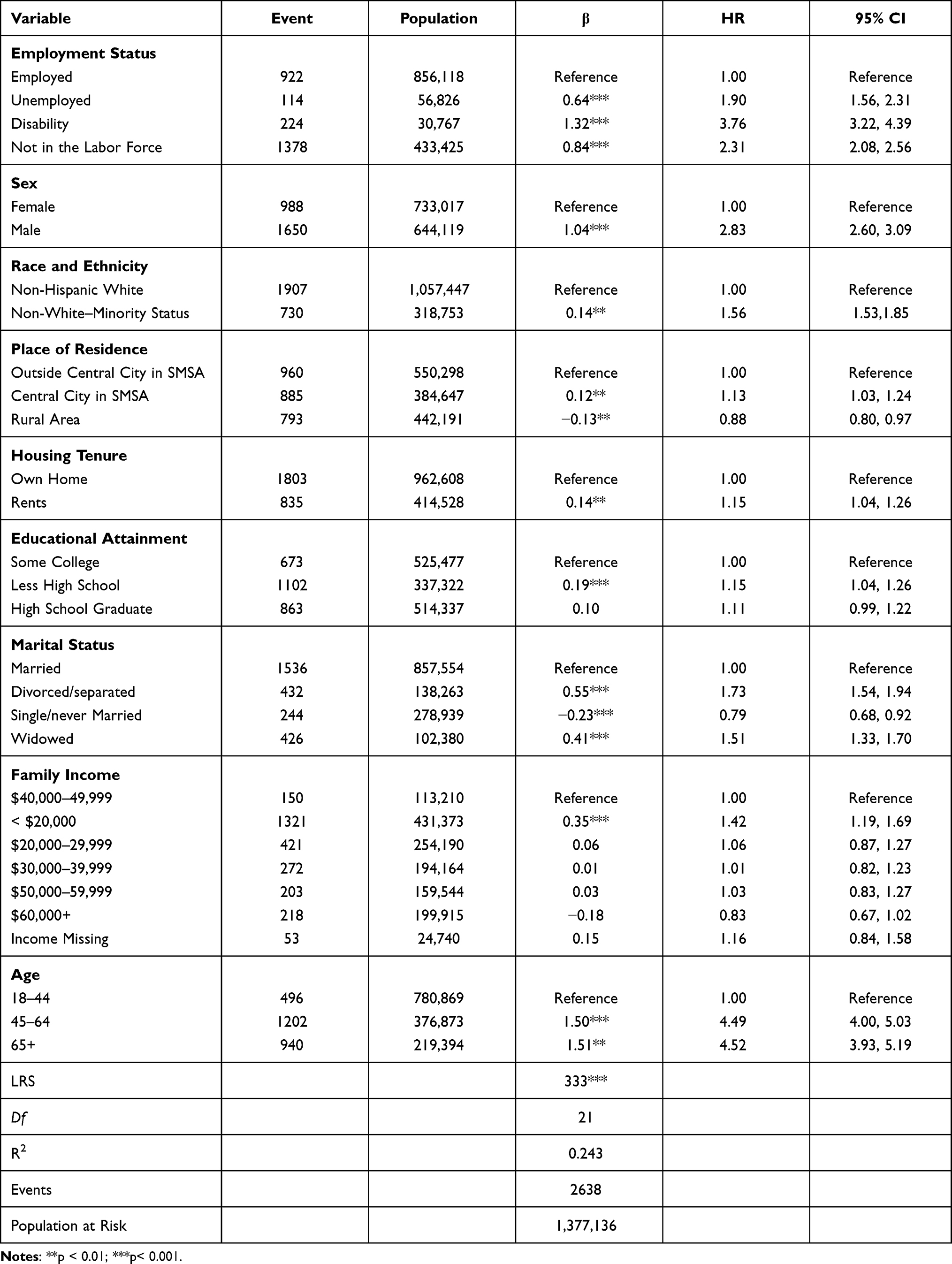 |
Table 1 Descriptive Statistics and Results for Alcohol-Related Liver Disease Mortality, Entire Sample |
In order to see if other covariates modify the relationship between unemployment, disability, those otherwise not looking for work and ALD mortality, Table 2 stratifies males by minorities and non-Hispanic whites with the findings that unemployed minority and non-Hispanic white men were highly related to ALD mortality, respectively (HR=1.57, CI=1.07, 2.31; HR=2.19, CI=1.67, 2.87). Similar results were found for disabled minority and non-Hispanic white men, respectively (HR=3.94, CI=3.13, 4.97; HR=3.47, CI=2.55, 4.73), and for those otherwise not in the labor force (HR=2.47, CI=2.93, 3.17; HR=2.28, CI 1.94, 2.69). Other significant findings in the positive direction included minority men living in a central city of a SMSA, divorced/separated, and age. Single/never married minority men were significant in the negative direction. For non-Hispanic white men, renting a home, divorced/separated, widowed status, low income, and age were significant in the positive direction. For non-Hispanic white men, living in a rural area and single/never married were negatively related.
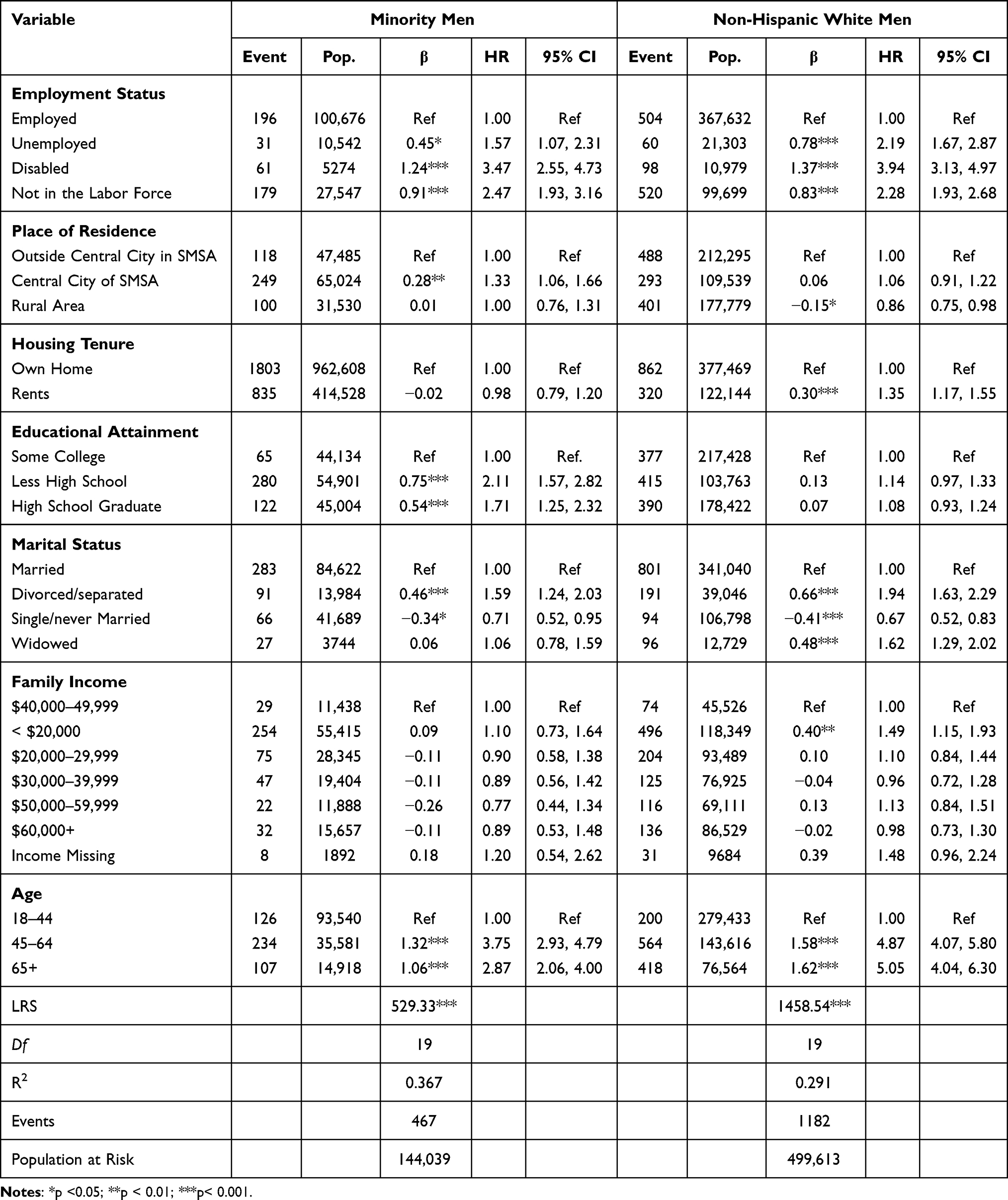 |
Table 2 Minority Men and Non-Hispanic White Men: Alcohol-Related Liver Disease Mortality |
Table 3 stratifies females by minority and non-Hispanic whites. Here, non-Hispanic white and minority women who were disabled were, respectively, 337% and 234% more likely to die of ALD compared to the employed (HR=4.37, CI=3.04, 6.28; HR=3.34, CI=2.05, 5.43). Minority and non-Hispanic white women not in the labor force were also highly related to ALD mortality, respectively (HR=2.13, CI=1.54, 2.96; HR=2.50, CI=2.04, 3.06), and while unemployment was not significant for minority women, it was significantly related to ALD for non-Hispanic white women (HR=1.76, CI=1.07, 3.05). For minority women, widowed status and age were significantly related to ALD in a positive direction, and for non-Hispanic white women divorced/separated, widowed, low income, and age were positively related. Living in a rural area was negatively related to ALD for non-Hispanic white women.
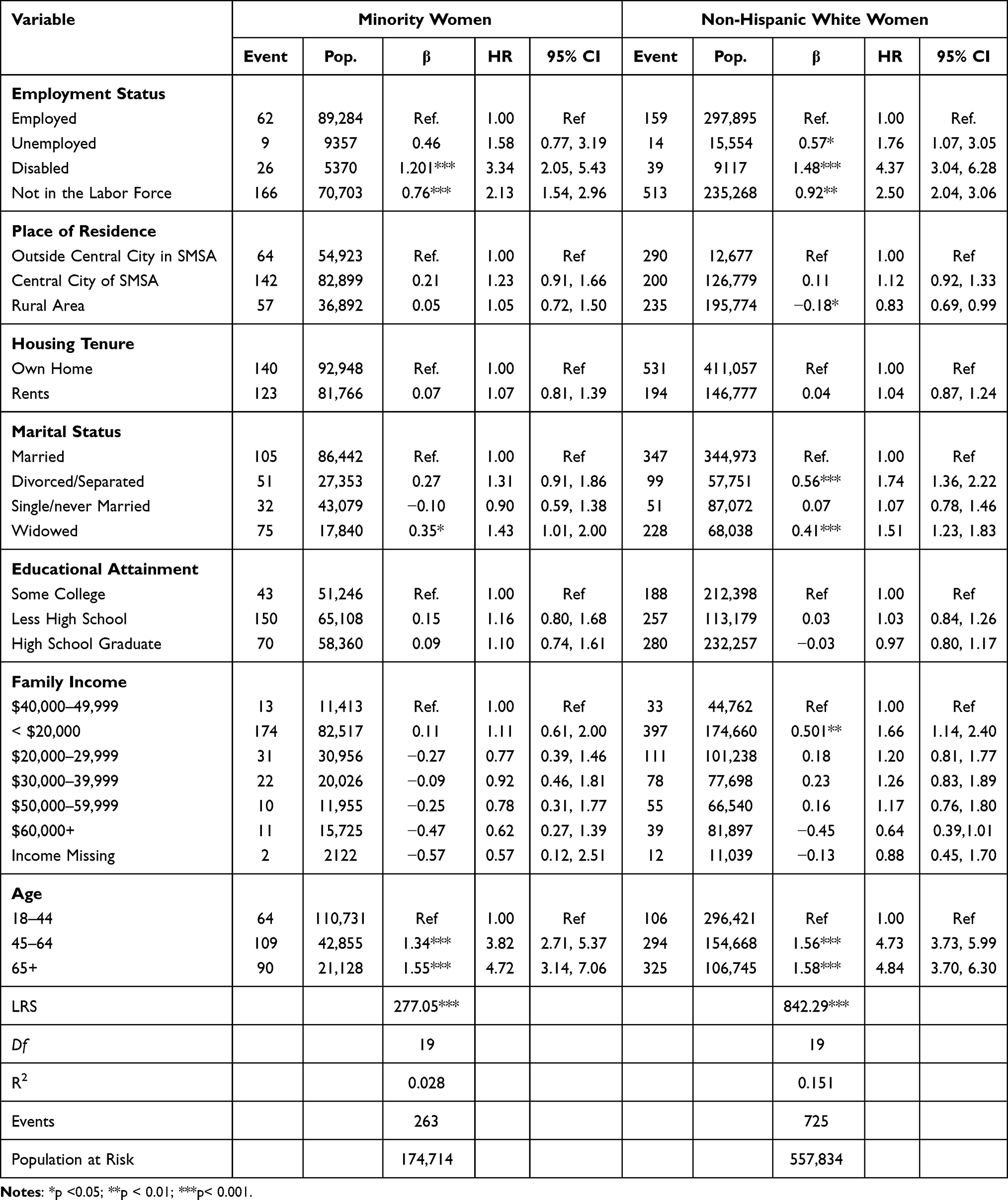 |
Table 3 Minority Women and Non-Hispanic White Women: Alcohol-Related Liver Disease Mortality |
Discussion
The research literature has shown that along with covariates such as males, minority status, marital status other than marriage, and low socioeconomic status, unemployment (people looking for work) is related to ALD mortality. The current study advances this understanding by showing that disabled persons who are unable to work, and those not otherwise in the labor force and not seeking employment, are at high risk for ALD mortality. The disabled who are unable to work and the retired are especially concerning regarding ALD mortality because their non-working status is often permanent. Others not looking for work, such as students and housekeepers are likely to enter the workforce at some point, and the unemployed and those looking for work may similarly find employment.
The main limitation of the study is that the NLMS does not include genetic factors and psychiatric morbidity. Some race and ethnic groups appear to be genetically predisposed to ALD morbidity, and for them, the relationship between those not working because of disability and ALD mortality may be modified such that these factors are less important.25 In addition, depression and other psychiatric disorders may have an important role in the likelihood of ALD morbidity and mortality.26 More effort is needed to incorporate such variables into large longitudinal US datasets. Also, disability status and being without work not only contributes to ALD mortality but also alcohol abuse, addiction and morbidity increase disability and long-term unemployment. For example, in the current study alcohol abuse and morbidity in employed persons at the beginning of the study may have caused some of them to lose their employment and subsequently die of ALD. As with many health-related problems, more research is needed on understanding the causal directions involving risk factors and morbidity. However, there is strong evidence that disability is related to alcohol abuse and may be the primary cause of self-medication and coping,27,28 and if some employed persons with alcohol-related morbidity died of ALD by the end of the study that suggests our results for the unemployed, disabled and those not otherwise unemployment may be conservative and underestimate the hazard for these factors.
Research has suggested caution in drawing causal inferences based on estimates from a multivariate model.29 For example, it is quite plausible that structural racism impacts employment status, housing tenure, educational attainment, income, and other related variables not in our models as it limits the employment status of minorities, reduces education and income, and prevents minority members from owning homes. Including these covariates in models tends to ignore the overall macro effect of structural racism. However, this study concerns individual level micro variables, and the NLMS does not include macro-level covariates. It is also not possible to draw conclusions on factors that are at a higher level of aggregation when they are not in the analysis. Nevertheless, findings from this study and others14,30 suggest that strong racial differences exist even after taking into account other variables in the equation, and macro-level structural racism is not excluded in this or similar research.
Prior research indicates males, minorities, marital statuses other than marriage, and socioeconomic status are related to ALD mortality. Among socioeconomic variables, employment and employment categories other than unemployment have received less attention. As noted, in one US study, unemployment was among the highest risk factors for ALD mortality.14 And while disability status has been the subject of research, large sample longitudinal studies of ALD mortality have been lacking.15–18 The current paper analyzed a sample of 1.4 million individuals and 167,000 mortality events with a set of relevant covariates including expanded socioeconomic variables, including disabled status and those otherwise not working, notably the retired, housekeepers and students. Among other factors, results show a strong relationship between unemployment (those looking for work), disability status (unable to work), and those otherwise not looking for work. Stratifying the results for gender and race and ethnic groups did not reduce these findings.
These results have obvious clinical importance. For both men and women, minority and non-Hispanic whites who were not employed or looking for employment, as in the case of disabled status, the risks for alcohol consumption (the cause of ALD morbidity and mortality) were quite high, independent of other covariates often thought to be more important. Health care professionals should be aware that alcohol use may not only contribute to employment loss and reductions in employment chances, but the lack of employment and disability status is strongly related to subsequent ALD mortality.
Conclusion
Gender, minority status, marital statuses other than marriage, and socioeconomic variables have been found to be important in the ALD mortality literature. Unemployment and other employment factors have been less studied. In this large sample longitudinal study with expanded employment status factors, disability (HR=3.76, CI 3.22, 4.39), unemployment (HR=1.90, CI 1.56, 2.31), and those not otherwise in the labor force (HR=2.31, CI 2.08, 2.56), were strongly related to ALD mortality compared to the employed. Gender, minority status and other covariates shown to be related to ALD mortality in the research literature were similarly associated but generally did not modify the relationships between the non-employment factors and ALD mortality. Those who are not employed and not looking for work, including the disabled, have high risk for ALD mortality. Health professionals should consider these findings and guide health care directives accordingly.
Ethical Approval and Informed Consent
An institutional review board (IRB) or ethics committee was not required for this research. The IRB guidelines for research at the University of California, Riverside, Ca states that in order to be exempt, data must be publicly available, such as census data, public use data, labor statistics, vital statistics, and similar statistics that are published by federal agencies. These data must have been de-identified and are anonymous. The NLMS data used in this study come from US federal agencies and are anonymized prior to release to researchers, and they are publicly available on the World Wide Web.
Acknowledgments
We are indebted to the US Bureau of the Census and the National Center for Health Statistics for providing the data for this research study. All statements, views and opinions in the current paper do not necessarily reflect those of these institutions. We also thank the reviewers of this paper for their generous help.
Disclosure
The authors report no conflicts of interest in this study.
References
1. Julien J, Ayer T, Bethea ED, Tapper EB, Chhatwal J. Projected prevalence and mortality associated with alcohol-related liver disease in the USA, 2019–40: a Modelling Study. Lancet Public Health. 2020;5(6):316–323. doi:10.1016/S2468-2667(20)30062-1
2. Mellinger JL, Shedden K, Winder GS, et al. The high burden of alcoholic cirrhosis in privately insured persons in the United States. Hepatology. 2018;68(3):872–882. doi:10.1002/hep.29887
3. Tapper EB, Parikh ND. Mortality due to cirrhosis and liver cancer in the United States, 1999–2016: Observational Study. BMJ. 2018;362. doi:10.1136/bmj.k2817
4. Mann RE, Smart RG, Govoni R. The epidemiology of alcoholic liver disease. Alcohol Res Health. 2003;28:209–219.
5. Vong S, Bell BP. Chronic liver disease mortality in the United States, 1990–1998. Hepatology. 2004;39(2):476–483. doi:10.1002/hep.20049
6. Trimble G, Zheng L, Mishra A, Kalwaney S, Mir HM, Younossi M. Mortality associated with alcohol-related liver disease. Aliment Pharmacol Ther. 2013;38(6):596–602. doi:10.1111/apt.12432
7. Sofair AN, Barry V, Manos MM, et al. The epidemiology and clinical characteristics of patients with newly diagnosed alcohol-related liver disease: results from population-based surveillance. J Clin Gastroenterol. 2010;44(4):301–307. doi:10.1097/MCG.0b013e3181b3f760
8. Kendler KS, Lonn SL, Salvatore J, Sundquist J, Sundquist K. Effect of marriage on risk for onset of alcohol use disorder: a longitudinal and co-relative analysis in a Swedish national sample. Am J Psychiatry. 2016;9(9):911–918. doi:10.1176/appi.ajp.2016.15111373
9. Martikainen P, Martelin T, Nihtila E, Majamaa K, Koskinen S. Differences in mortality by marital status in Finland from 1976 to 2000: analyses of changes in marital-status distributions, socio-demographic and household composition, and cause of death. Popul Stud. 2005;59(1):99–115. doi:10.1080/0032472052000332737
10. Poikolainen K, Paljarvi T, Makela P. Risk factors for alcohol-specific hospitalization and deaths: Prospective Cohort Study. Alcohol Alcohol. 2011;46(3):342–348. doi:10.1093/alcalc/agr013
11. Kim JW, Jung HY, Noh JH, Park JY. Long-term trends in death rates from alcohol-related disease in South Korea. Am J Health Behav. 2019;43(3):648–658. doi:10.5993/AJHB.43.3.17
12. Budhiraja M, Landberg J. Socioeconomic disparities in alcohol-related mortality in Sweden, 1991–2006: a Register-Based Follow-Up Study. Alcohol Alcohol. 2016;51(3):307–314. doi:10.1093/alcalc/agv108
13. Makela P. Alcohol-related mortality as a function of socio-economic status. Addiction. 1999;94(6):867–886. doi:10.1046/j.1360-0443.1999.94686710.x
14. Singh GK, Hoyert DL. Social epidemiology of chronic liver disease and cirrhosis mortality in the United States, 1935–1997: trends and differentials by ethnicity, socioeconomic status and alcohol consumption. Hum Biol. 2000;72:801–820.
15. Ostermann J, Sloan FA. Effects of alcohol consumption on disability among the near elderly: a longitudinal analysis. Milbank Q. 2001;79(4):487–515. doi:10.1111/1468-0009.00219
16. Sidorchuk A, Hemmingsson T, Romelsjo A, Allebeck P, Miles J. Alcohol use in adolescence and risk of disability pension: a 39 year follow-up of a population-based conscription survey. PLoS One. 2012;7(8):e42083. doi:10.1371/journal.pone.0042083
17. Skogen JC, Knudsen AK, Mykletun A, Nesvag S, Overland S. Alcohol consumption, problem drinking, abstention and disability pension award. The Nord-Trondelag Health Study (HUNT). Addiction. 2011;107(1):98–108. doi:10.1111/j.1360-0443.2011.03551.x
18. Rehm J, Gmel G, Sempos CT, Trevisan M. Alcohol-related morbidity and mortality. Alcohol Res Health. 2003;27:39–51.
19. U.S Bureau of the Census. Public Use Microdata Sample (PUMS) Release 5 Documentation. Washington: Department of Commerce; 2015.
20. Kposowa AJ, Ezzat DA, Breault K. New findings on gender: the effects of employment status on suicide. Int J Women Health. 2019;11:569–575. doi:10.2147/IJWH.S216504
21. World Health Organization. International Statistical Classification of Diseases and Related Health Problems.
22. SAS Institute. SAS/STAT Software. Cary: SAS Institute; 2018.
23. Selvin S. Statistical Analysis of Epidemiological Data. London: Oxford University Press; 1991.
24. Collett D. Modeling Survival Data in Medical Research. London: Chapman and Hall; 2003.
25. Edenberg HJ. The genetics of alcohol metabolism. Role of alcohol dehydrogenase and aldehyde dehydrogenase variants. Alcohol Res Health. 2007;30:5–13.
26. McHugh RK, Weiss RD. Alcohol use disorders and depressive disorders. Alcohol Res. 2019;40:1.
27. Chapman SL, Wu L-T. Substance abuse among individuals with intellectual disabilities. Res Dev Disabil. 2012;33(4):1147–1156. doi:10.1016/j.ridd.2012.02.009
28. Oh S, Lee S, Jang S-I, Park E-C. Chronic alcoholism and all-cause mortality among disabled individuals: findings from the Korea national health insurance service-national sample cohort. Alcohol. 2020;89:57–62. doi:10.1016/j.alcohol.2020.08.006
29. Westreich D, Greenland S. The table 2 fallacy: presenting and interpreting confounder and modifier coefficients. Am J Epidemiol. 2013;177(4):292–298. doi:10.1093/aje/kws412
30. Kposowa AJ, Ezzat DA, Breault K. Diabetes mellitus and marital status: evidence from the National Longitudinal Mortality Study on the effect of marital dissolution and the death of a spouse. Int J Gen Med. 2021;14:1881–1888. doi:10.2147/IJGM.S307436
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.