Back to Journals » Risk Management and Healthcare Policy » Volume 14
Director’s Perceived Competition and Its Relationship with Hospital’s Competitive Behaviors: Evidence from County Hospitals in China
Authors Zhou T, Yang Y, Hu M, Jian W, Pan J ![]()
Received 12 July 2021
Accepted for publication 14 September 2021
Published 1 October 2021 Volume 2021:14 Pages 4113—4125
DOI https://doi.org/10.2147/RMHP.S328807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Tingting Zhou,1,2 Yili Yang,2 Min Hu,3 Weiyan Jian,4 Jay Pan1,2
1HEOA Group, West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Institute for Healthy Cities and West China Research Center for Rural Health Development, Sichuan University, Chengdu, People’s Republic of China; 3School of Public Health, Fudan University, Shanghai, People’s Republic of China; 4Department of Health Policy and Management, School of Public Health, Peking University Health Science Center, Beijing, People’s Republic of China
Correspondence: Jay Pan
HEOA Group, West China School of Public Health and West China Fourth Hospital, Sichuan University, No. 17, Section 3, Ren Min Nan Road, Chengdu, Sichuan, 610041, People’s Republic of China
Email [email protected]
Background: This study was conducted for assessing the degrees of perceived competition reported by county hospital directors in rural China as well as hospitals’ competitive behaviors in response to competition.
Methods: The data were collected from Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project which had been implemented among county hospitals in China’s Guizhou province. Competition was measured by asking hospital directors to rate the levels of competitive pressure as they perceived. Hospitals’ competitive behaviors were obtained by asking hospitals’ directors about specific strategies they had adopted. A multivariable linear regression model was developed to examine the relationship between perceived competition and the positivity of competitive behavior, and multivariable logistic regressions were used to evaluate the influence of perceived competition on the adoption of specific competitive strategies.
Results: Among 218 directors engaged in this study, 210 (96.3%) directors reported the perception of certain degrees of competition, for which the competitive pressure was mainly posed by public hospitals (42.4%). Director-perceived competition level was found to be positively associated with the positivity of competitive behavior, and directors under higher competitive pressure were found to be more likely to adopt multiple competitive strategies including improving the efficiency of hospitals’ internal management, optimizing hospitals’ environment as well as promoting health-care services.
Conclusion: This study suggested that almost all of the county hospital directors in rural China perceived certain degrees of competitive pressure, and higher levels of perceived competition were found to be significantly associated with increased positivity in adopting competitive strategies. Our findings are expected to provide evidence-based implications for the implementation of a series of pro-competition policies throughout health-care reforms.
Keywords: perceived competition, hospital behavior, county hospital, director, China
Introduction
The introduction of competition into hospital markets has been adopted by multiple countries as a tactic for improving the quality and efficiency of healthcare delivery.1–4 Similarly, a series of pro-competition policies has been proposed and implemented by the Chinese government throughout the nationwide health care reform as the key strategy to facilitate the improvement of hospital market performance5 such as reducing medical costs and improving quality and efficiency of healthcare delivery.6–8 On the one hand, the governmental encouragement on private hospital development has facilitated the formation of a diversified hospital market in China, which increases the provision of medical services and to some extent allows patients to “vote with their feet”.9 On the other hand, the mode of investment in health-care industry has been switched from supply-side toward demand-side financing.10 Specifically, the Chinese government has invested largely in the national basic medical insurance system, while financial subsidy for public hospitals is reduced to only about 10% of hospital’s total revenue,11,12 which has consequently created the motivation for public hospitals to compete for patients.
Market-oriented healthcare reform initiated by the Chinese government changed the nationwide hospital market previously monopolized by public hospitals. Encouraged by the Chinese government, the number of private hospitals has been constantly increasing and finally exceeded the number of public hospitals in 2015, with proportion of private hospitals reaching 63.5% in 2018.11,13 According to Structure-Conduct-Performance (SCP) framework,14 the market structure determines behaviors of the enterprise in the market, while behaviors of the enterprise determines the economic performance of the market in various aspects (Figure 1). Based on such mechanism, changes in the structure of the hospital market will further affect the performance of the hospital market by changing the behaviors of hospitals. It can be seen that behaviors of hospitals would largely affect hospitals’ ultimate performances, which fundamentally determines whether the goal of the pro-competition policies can be achieved. However, it is noteworthy that quite a number of studies from previous literature have been focused on investigating the reduced impacts of hospital competition on health-care delivery outcomes,7,15–21 rather than evaluating hospitals’ behaviors when confronted with competitions.22
 |
Figure 1 Theoretical framework. |
To date, the impact of competition on hospitals’ behaviors remains ambiguous. According to dynamic competition theory established by Mingzhe Chen,23 awareness, motivation and capability (AMC) are three essential drivers of competitive actions (Figure 1). Specifically, competitive actions will only be activated when participants have adequate awareness of competition as well as having enough motivation and capacity to respond to the competition.24–26
Generally, awareness for competition is regarded as a necessary prerequisite for competitive behaviors. In China, the autonomy of public hospitals has been enhanced by a policy named “guan ban fen kai” (making the operational system within public hospitals administratively independent from the surveillance of governmental divisions), which has highlighted the key role of hospital directors in hospitals’ operations.27 Under such context, it can be easily predicted that the perceived competition of hospital directors would determine the initiation of competitive strategies when confronted with competition. However, the degree of competition was usually measured by objective indicators such as Herfindahl-Hirschman Index (HHI) in most of the previous studies,10,16,28 which may lead to biased outcomes.29–31 More crucially, competitive strategies will only be adopted under the precondition that hospital directors have perceived certain degrees of competitions,32 indicating that perceived competition by hospital directors should be addressed as an essential subjective indicator for explaining hospitals’ competitive behaviors.
In addition, both adequate motivation and capacity would also serve as prerequisites for hospitals to initiate the implementation of a series of competitive strategies. Decisions made by hospital directors are typically impacted by both drivers and barriers from internal and external environments, thus increasing the uncertainty of hospitals’ behaviors in response to perceived competitions. As agents appointed by the government or shareholders, hospital directors receive supervisions from their principals, and performance appraisal for directors stimulates them to behave well.33 However, severe information asymmetry persistently embedded in the medical industry has provided the opportunity for hospital directors to seek for opportunism at their convenience when needed.34 Moreover, insufficient financial incentives would also add to hospital directors’ lack of motivation for adopting competitive strategies even when confronted with competitions.35 Due to the influences of various factors, it is hard to determine whether hospital directors have the adequate motivation and capacity for initiating competitive strategies in response to competitions.
It is noteworthy that the competitive behavior adopted by hospitals may not necessarily be positive. Information asymmetry embedded in the medical market is generally more serious than in the commodity market because medical products are highly specialized with the lack of substitutability.36 Natural information advantages may encourage hospitals to obtain more economic benefits via inducing patients’ demands, such as prescribing unnecessary drugs and tests, which is obviously unfavorable to medical cost control.37 In addition, the hospital may invest a large amount of money in infrastructure construction and purchasing high-tech equipment to demonstrate high quality of healthcare from patients’ perspectives, thus ultimately achieving the goal of attracting patients. Some scholars define this kind of competitive behavior as “medical arms race”, which is believed to be a significant contributor to increased medical expenses.38 In addition, characteristics of medical care markets under particular contexts might also add to the complexity of impacts posed by market competition on hospitals’ competitive behaviors. Therefore, whether the competition serves as a positive stimulant for guiding hospitals to adopt positive competitive measures remains controversial.
As the leading health-care organizations at the top of the rural three-level medical service network, county-level hospitals are expected to provide essential health-care services for rural residents in China (about 40% of the total population of China).39 However, studies focusing on hospital competition in rural China remain limited. Compared with urban areas, medical resources distributed in rural China are relatively insufficient. The 2019 China Health Statistics Yearbook indicated that about 5.5 hospitals are allocated in rural regions per county, while an averaged amount of 52.4 hospitals are distributed in urban regions per city.11 In rural China, a general hospital and a traditional Chinese medicine (TCM) hospital are usually the only two public hospitals located in a county, along with several other private hospitals. Besides, county hospitals are usually small-scaled with fewer beds equipped compared with urban hospitals, an averaged amount of 173 beds are equipped per county hospital, while 220 beds are equipped per city hospital.11 Under such circumstances, it is not difficult to imagine that in a rural hospital market with relatively fewer competitors, the intensity of hospital competition as well as its impacts on hospitals’ behaviors tend to be inconclusive.
Nevertheless, limited studies from previous literature have been focused on exploring the relationship of rural hospital directors’ perceived competition and the competitive strategies adopted in response to perceived competition. Through the literature review, we find that there are three notable gaps embedded in the existing literature. Firstly, most of the studies were focused on analyzing the impact of hospital competition on health-care outcomes,7,15–18 while limited studies evaluated hospitals’ behaviors when confronted with competitions 22. Secondly, quite a number of objective indicators adopted for measuring the degrees of competition from previous literature might probably induce biased outcomes,29,30 while limited research measured the hospital director’s perception of competition. Thirdly, studies focused on hospital competition in rural areas were found to be limited.
In an attempt to bridge such gaps embedded in previous literature, in this study self-reported data collected from a survey among county hospital directors in rural China was adopted for evaluating the degrees of competition from rural hospital directors’ perspectives as well as the association between perceived competition and hospitals’ competitive behaviors. The degrees of perceived competition were reflected by hospital directors’ self-reported data for which they were asked to scale the level of pressure posed by other hospitals from their own perspectives. Competitive strategies were also asked in the survey in order to reflect hospitals’ behaviors for tackling with issues induced by intensified hospital competition.
Our study is expected to contribute to the relevant literature mainly in three aspects. Specifically, our study is expected to add evidence to the previous literature by describing the competitive hospital market in rural China via reporting the intensity of competition, the source of competition as well as hospitals’ competitive strategies. In addition, the relationship between hospital directors’ perceived competition levels and the positivity of competitive behaviors was investigated thus providing evidence-based implications for the introduction of a series of pro-competition policies into hospital markets, especially for other countries confronted with similar circumstances. Instead of using objective indicators, in this study self-reported data directly collected from hospital directors was adopted as subjective indicators for reflecting the degrees of hospital competition, which provides a feasible method for measuring the actual degrees of hospital competition.
Methods
Data Source
This study was conducted in China’s Guizhou province. Guizhou province, located in southwest China, consists of 88 counties. Limited by its mountainous natural environment, the transportation in Guizhou province remains underdeveloped, which has posed huge obstacle on its regional economic development. The Gross domestic product (GDP) per capita of Guizhou province in 2018 was 41,244 yuan (about 6230 US dollars).40 There are 18.9 million permanent residents live in rural areas of Guizhou Province, accounting for 52.5% of its total population.40 Under such circumstances, county hospitals have been expected to serve as essential health-care providers for a large number of rural residents in Guizhou province.
Data were mainly extracted from Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project, which was carried out on county-level hospitals in China’s Guizhou province from 2015 to 2018. The County Hospital Survey (CHS) questionnaire was designed by the research group and was used for collecting self-reported data among county hospital directors. A total of 218 hospital directors participated in the questionnaire survey. In addition, the gross domestic product (GDP) per capita of counties were extracted from the official website of Guizhou Bureau of Statistics (http://stjj.guizhou.gov.cn).
Hospital Behavior Measurement
Hospitals’ behaviors were dependent variables of this study, which were extracted from the multiple choices question “what measures did the hospital adopt to cope with the competition?”. This question has been proposed and added into the survey for reflecting hospital directors’ behaviors in adopting competitive strategies based on a systematic review of the relevant literature.22,41 In attempt to incorporate multiple aspects reflective of hospitals’ both internal and external conditions for comprehensive analysis, including strengths, weaknesses, opportunities and threats,42 six options were finally designed for this question: (1) improving the efficiency of hospitals’ internal management; (2) recruiting highly competent doctors; (3) investing in high-tech medical equipment; (4) improving the environment of the hospital; (5) improving health-care services; (6) others (specify). Only 7 respondents (3.2%) chose “(6) others”. In order to facilitate data processing, the specific contents of strategies adopted were analyzed and categorized into five main aspects reflective of hospitals’ competitive behaviors, which were generalized as follows: (1) management optimization; (2) professional recruiting; (3) equipment expansion; (4) environment optimization; (5) service promotion.
The behavioral positivity of hospital directors in adopting competitive strategies was measured by calculating the number of strategies hospital adopted, which ranged from 0 to 5. To further explore the relationship between perceived competition and hospitals’ specific competitive behaviors, the five main strategies as generalized above were used as explained variables. For each specific strategy as mentioned above, the implementation of this specific strategy would be defined as one, and failure to adopt this specific strategy would be defined as zero. The definitions of variables reflective of hospital directors’ competitive behaviors are shown in Table 1.
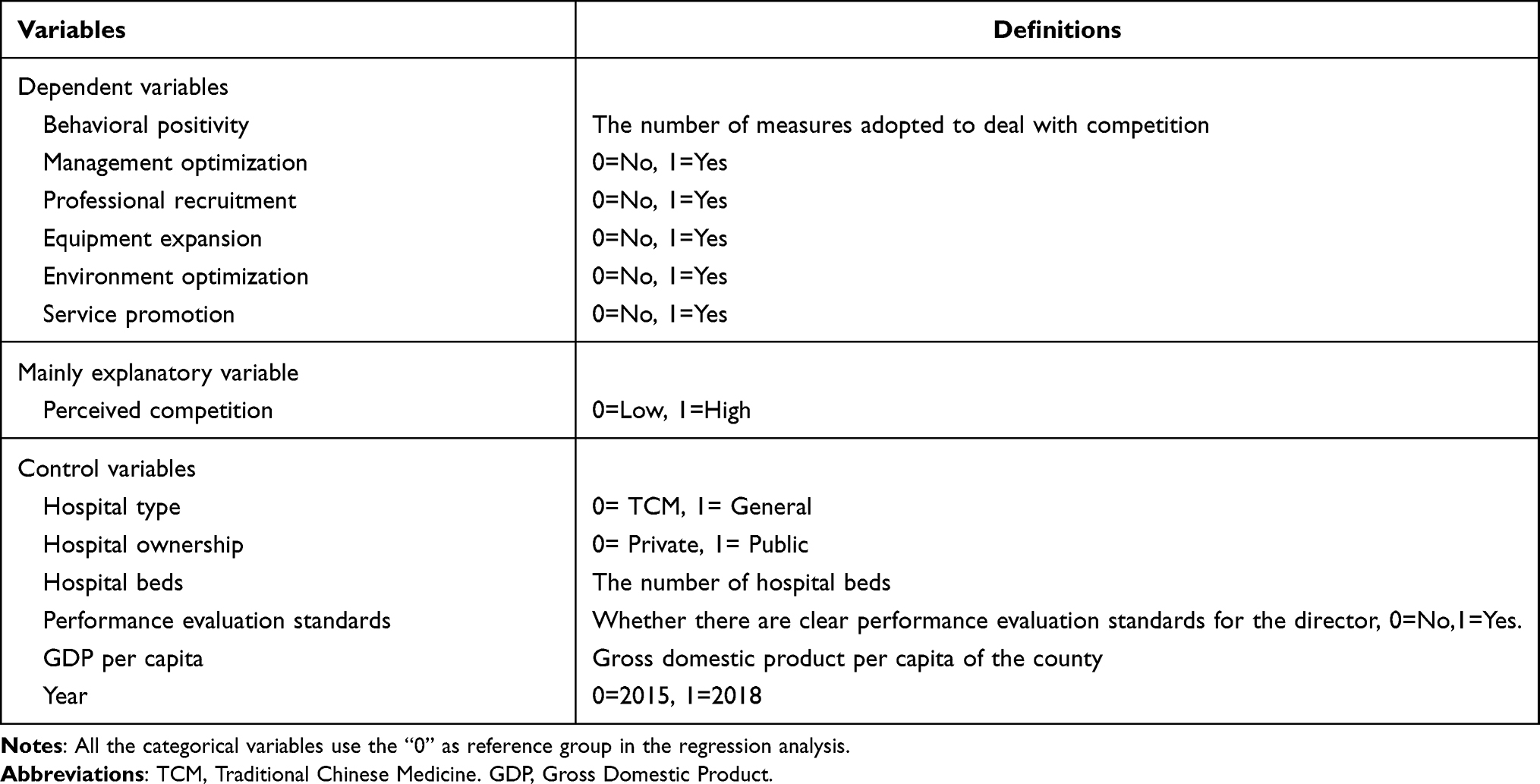 |
Table 1 Variable Definition |
Competition Measurement
Perceived competition of hospital director was the key explanatory variable of this study extracted from the question “did your hospital face competition from other hospitals?” Three options were designed for this question: (1) intense competition; (2) moderate competition; (3) no competition. Only 8 respondents (3.7%) reported the absence of perceived competition. Based on previous research,43 “no competition” and “moderate competition” were defined as low competition groups (as references) with an assigned value of zero, and “intense competition” was defined as the high competition group with an assigned value of one. Directors who reported the perception of intense competition or moderate competition were further asked about where the competition pressure mainly came from, which included multiple potential sources namely hospitals out of the county, public hospitals within the county, private hospitals within the county, or other.
Control Variables
To control the influence of other factors, we included hospital-level and county-level covariates. At hospital level, we included hospital type (traditional Chinese medicine hospital = 0, general hospital = 1), hospital ownership (private hospital = 0, public hospital =1), hospital beds as well as whether there are clear performance evaluation standards established for the director (no = 0, yes = 1). At county level, gross domestic product (GDP) per capita was used to control county variations. Besides, year was set as a dummy variable. The definitions of control variables are shown in Table 1.
Statistical Analysis
Firstly, descriptive analysis was conducted. The degree of competition perceived by hospital directors was grouped to compare the distribution of variables. The continuous variables were described by the means with standard deviation (SDs) and were evaluated by t-test, while categorical variables were described using frequency and estimated by Chi-square test or Fisher exact test. Hospital beds and GDP per capita were natural log transformed to satisfy a normal distribution.
Secondly, multivariable linear regression was adopted to examine the relationship between perceived competition and the behavioral positivity of hospital directors in adopting competitive strategies. The model was set as follows:

where Yit is the main dependent variable of interest, which refers to behavioral positivity of director i in year t. Competitionit is our main independent variable, which indicates the degree of competition director i perceives in year t. Hospitalit and Countyit are the hospital-level and county-level control variables. Year refers to the survey year. εit is the error term. The key coefficient of interest is represented by β1, which indicates the relationship between perceived competition and hospitals’ behavioral positivity. A positive value indicates a positive relationship between perceived competition and the hospital’s behavioral positivity in terms of adopting competitive strategies. Robust standard errors were used to correct heteroskedasticity.
Thirdly, multivariable logistic regressions were used to estimate the influence of director-perceived competition on the adoption of specific behaviors, and average marginal effects were calculated to measure the effects. The model was set as follows:

where Behaviorit indicates the behavior of director i adopted in year t, including (1) management optimization; (2) professional recruiting; (3) equipment expansion; (4) environment optimization; (5) service promotion. For example, Behaviorit equals one if the director i reported the investment in purchasing high-tech equipment; otherwise, the value would be zero. Competitionit is our main independent variable, which indicates the degree of competition director i perceived in year t. Hospitalit and Countyit are the hospital-level and county-level control variables. Year refers to the survey year. υit is the error term. The key coefficient of interest is represented by θ1, a positive value means that perceived competition is positively associated with the hospital’s competitive strategy. Robust standard errors were used to correct heteroskedasticity.
Finally, to examine the interaction relationship between perceived competition and hospital ownership types and the number of hospital beds, we further added the interaction term of perceived competition and hospital ownership as well as hospital beds in the regression models, respectively.
All analyses were performed using Stata/SE (Version 15.0, Stata Corp, TX, USA). P < 0.05 was considered as statistically significant.
Results
Descriptive Statistics
Table 2 presents the summary statistics for control variables, as well as comparisons between high competition and low competition groups. Among 218 directors in this study, 130 (59.6%) directors perceived intense competition, 80 (36.7%) directors reported moderate competition, while only 8 respondents (3.7%) perceived no competition. Most directors engaged in this study came from general hospitals (69.7%) and public hospitals (74.3%), and most hospitals (70.2%) have established clear performance evaluation standards for directors. Besides, 142 (65.1%) and 76 (34.9%) hospitals were investigated in 2015 and 2018, respectively. It was noteworthy that increased number of hospital beds was found to be associated with reduced intensity of perceived competition. However, no significant differences were identified between high and low competition groups in terms of hospital types, hospital ownership, performance evaluation standards established for directors, GDP per capita and survey years.
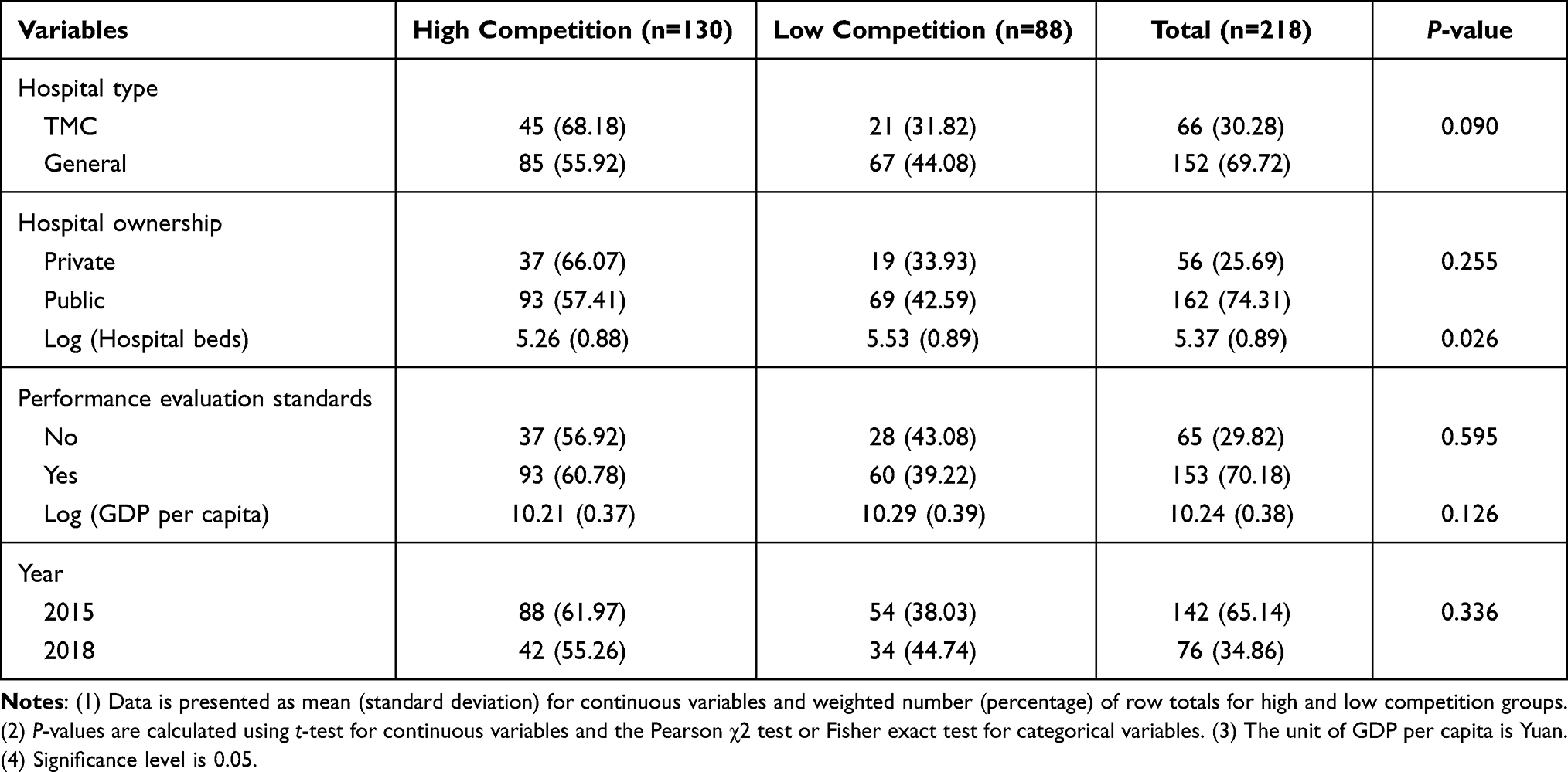 |
Table 2 Control Variables Characteristics |
Table 3 shows hospitals’ competitive behaviors confronted with competition, as well as the comparisons between high competition and low competition groups. The average number of competitive behaviors adopted by hospital directors was found to be 4.11. Specifically, 202 directors (92.7%) choose to optimize the internal management systems within hospitals, 168 (77.1%) directors recruited highly skilled health-care professionals, 140 (64.2%) directors invested in the purchase of high-tech medical equipment, 186 (85.3%) directors choose to improve hospitals’ environment, and 199 (91.3%) directors adopted strategies for medical service promotion. Overall, compared with low competition group, directors with higher levels of perceived competition presented to be more responsive to the competitive environment (4.28 VS 3.85, P<0.05). Similarly, it was suggested by subgroup analysis that hospital directors from high competition group were significantly more positive in adopting multiple competitive strategies for dealing with their competitive pressure, including optimizing the internal management of hospitals (99.2% VS 83.0%, P<0.001), optimizing hospitals’ environments (90.0% VS 78.4%, P<0.05) as well as promoting the quality and efficiency of health-care services (96.2% VS 84.1%, P<0.01). However, no significant differences were found between high and low competition groups in terms of recruiting highly skilled health-care professionals (P>0.05) or investing in the purchase of high-tech medical equipment (P>0.05).
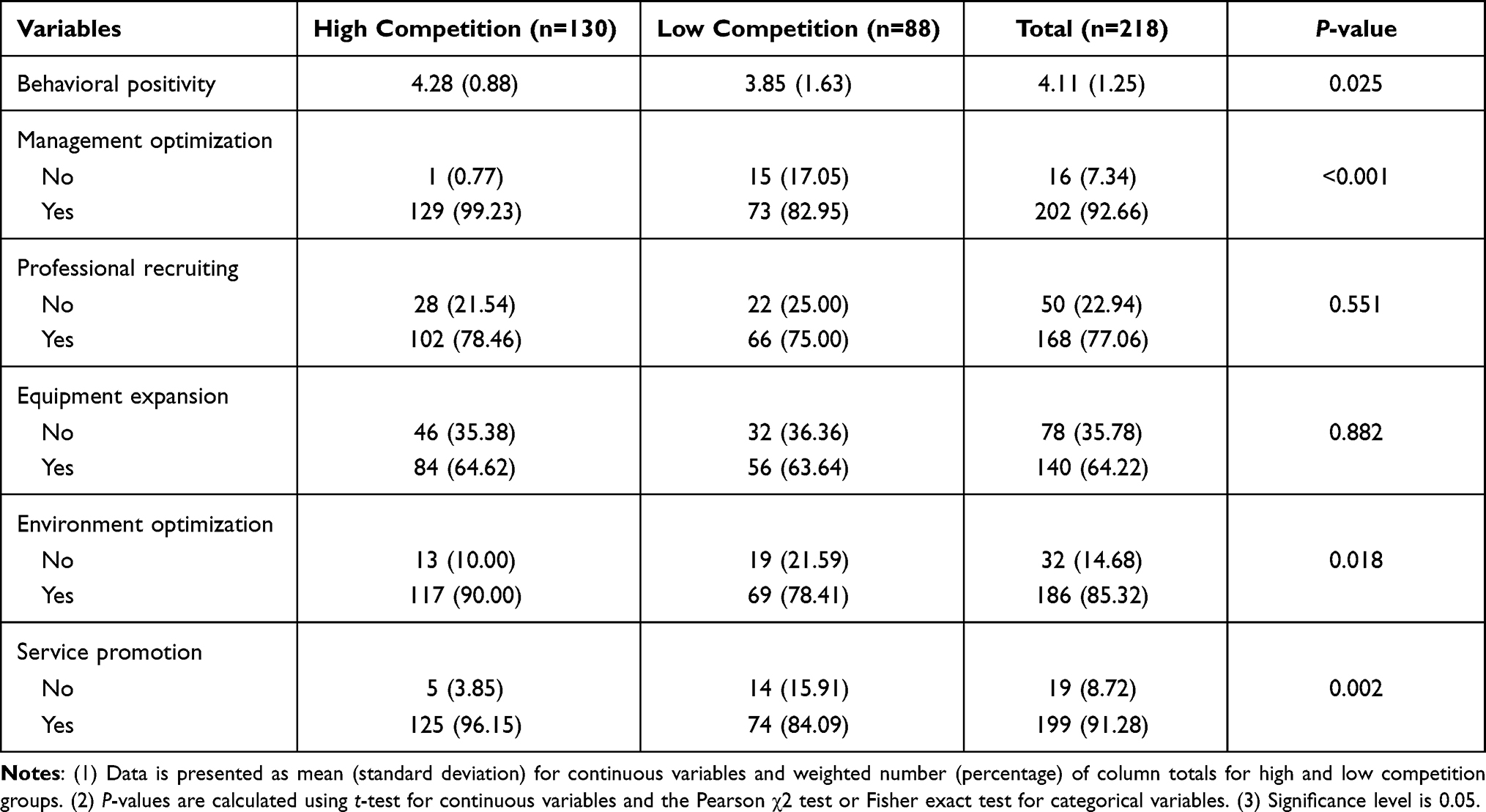 |
Table 3 Hospitals’ Competitive Behaviors |
In addition, among 210 directors with different levels of perceived competition, 72 (34.3%) directors reported that the competition pressure mainly came from hospitals out of the county, while 89 (42.4%) and 18 (8.6%) directors, respectively, reported public hospitals and non-public hospitals within the county as the leading sources of competitive pressure. Thirty-one (14.8%) directors reported others as the leading source of competitive pressure.
Regression Results
Table 4 reports the relationship between director-perceived competition and hospitals’ competitive behaviors, among which column 1 presents the multivariable linear regression results, and columns 2–6 show the multivariable logistic regression results. Column 1 reports the positivity of hospitals’ competitive behaviors when confronted with competition, which suggests that each 10% increase in the degree of perceived competition is associated with an average increase of 5.2% in the number of hospitals’ competitive behaviors (P<0.01). Column 2 shows the relationship between perceived competition and the behavior of optimizing hospitals’ internal management systems, which indicates that each 10% increase in the perceived competition level is associated with an average increase of 2.0% in the likelihood of adopting strategies for improving hospitals’ internal management systems (P<0.01). As shown in Column 3, no significant association was found between the degrees of perceived competition and strategies adopted for health-care professional recruitment (P>0.05). Likewise, as indicated by Column 4, no statistical significance was found between the degrees of perceived competition and the investments made by hospitals in purchasing high-tech medical equipment (P>0.05). Column 5 suggests that each 10% increase in the degrees of perceived competition is associated with an average increase of 1.3% in the likelihood of adopting strategies for optimizing hospitals’ environments (P<0.01). Column 6 indicates that each 10% increase in the degrees of perceived competition is associated with an average increase of 1.3% in the likelihood of adopting strategies for medical service promotion (P<0.01).
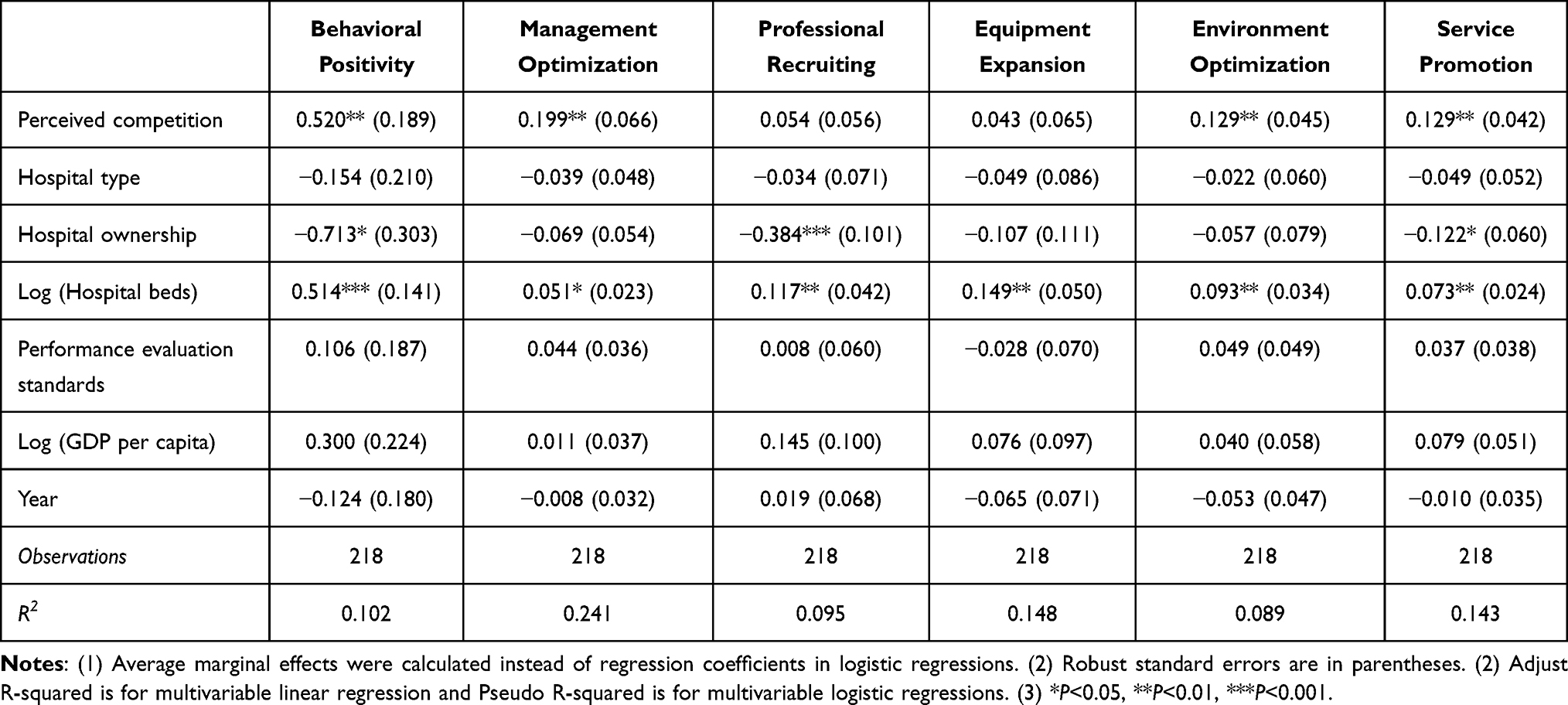 |
Table 4 The Relationship Between Perceived Competition and Hospital Behaviors |
Additionally, considering that hospitals with different ownership and scale would respond differently to competition, we further added the interaction term of perceived competition and hospital ownership, as well as hospital beds in the regression models, respectively. The reference group was low competition and private hospital. Hospital beds were also logarithmically converted as before.
Table 5 shows the results of the models after adding the interaction term of perceived competition with hospital ownership and hospital beds. The estimates of the interaction terms of perceived competition with hospital beds were all found to be insignificant (P>0.05), which indicated that no interaction relationship existed between perceived competition and hospital beds. However, the interaction term of perceived competition with hospital ownership in terms of optimizing internal management was found to be significantly negative (P<0.001), which suggested that compared with public hospitals, private hospitals were more likely to adopt strategies for improving hospitals’ internal management systems in response to changed competition degree posed by the hospital market.
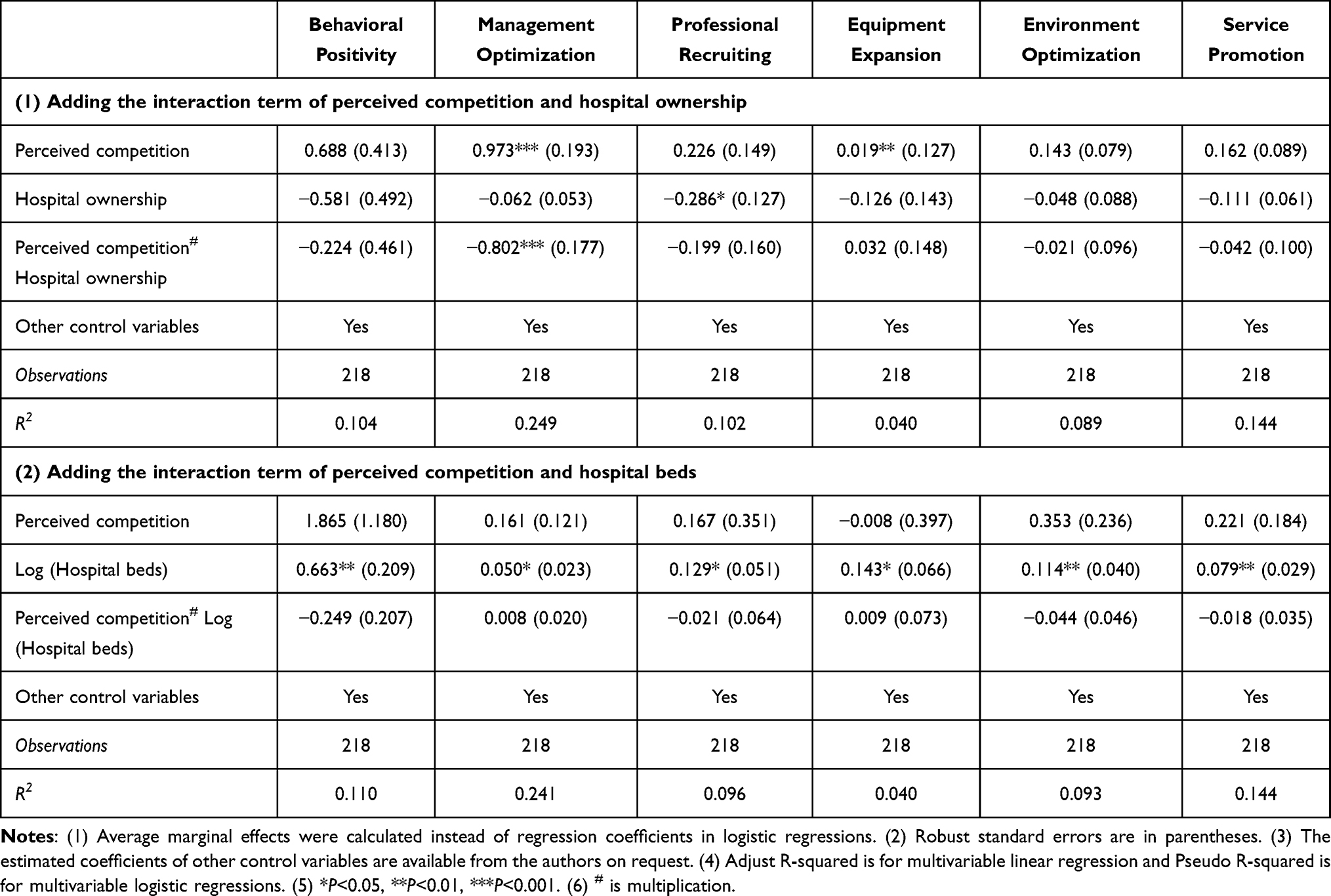 |
Table 5 The Interaction Relationship Between Perceived Competition and Hospital Ownership and Beds |
Robust Check
To test the robustness of the statistical outcomes, we replaced the variable named hospital beds in the regression model with hospital level for analysis because hospitals’ levels are typically correlated with the number of hospital beds. Specifically, hospitals were classified into ungraded, primary, secondary and tertiary hospitals, among which ungraded hospitals were set as references. Table 6 reports the results, which only shows the estimated competition coefficients as the key parameters for robustness analysis. The results were found to be similar with the regression results in Table 4 in terms of both signs and statistical significance of the coefficient estimates, thus indicating the robustness of our results.
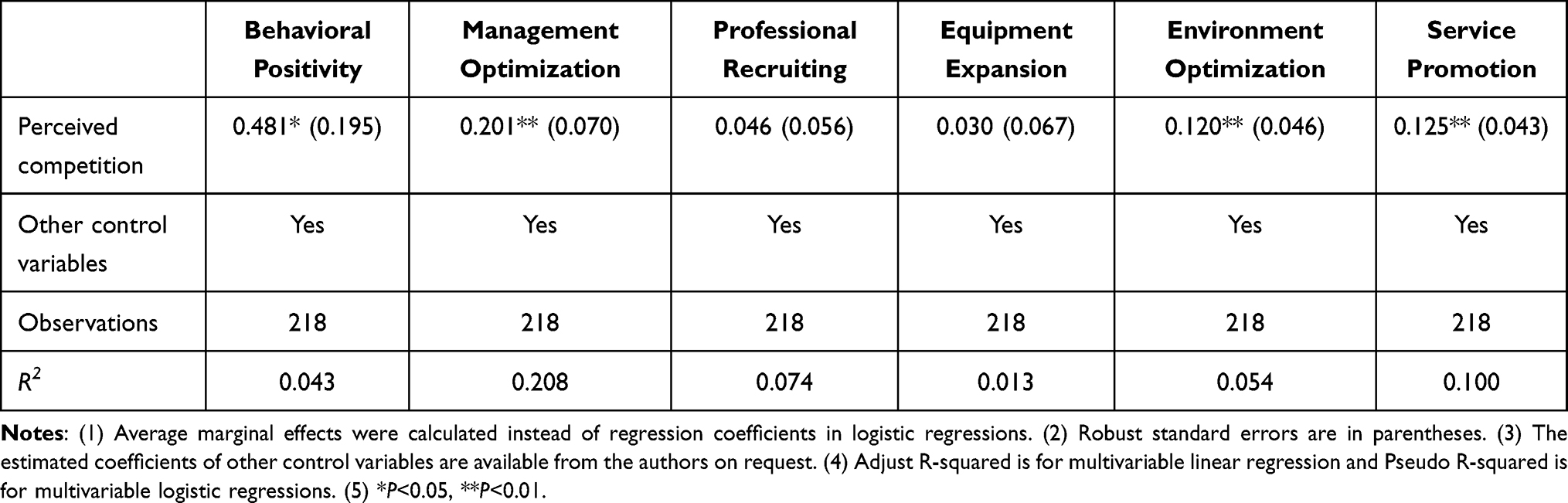 |
Table 6 Robustness Checks |
Discussion
In this study, we explored the perceived competition reported by county hospital directors as well as its association with hospitals’ competitive behaviors. As indicated by the results, almost all the county hospital directors have perceived certain degrees of hospital competition, for which the competitive pressure was mainly posed by public hospitals as their leading competitors in the rural hospital market. More importantly, we found that the degree of director-perceived competition was positively associate with hospitals’ competitive behaviors. Further, directors under higher competition were found to be more likely to optimize the management efficiency within the hospital, improve hospitals’ environments as well as promote health-care services.
In China, fewer hospitals are located in rural areas compared with urban areas which are typically found to be small-scaled.44 It remains unclear whether hospitals have to compete for attracting patients in rural areas where health-care resources are relatively scarce. Our findings provided potent evidences that competition exists among county hospitals in rural China. There might be two reasons for inducing such competitive situation. On the one hand, the increasing number of health-care providers in rural medical market drives hospitals to compete for limited market share in a fixed area.45 On the other hand, the government’s financial subsidies provided to public hospitals have been greatly reduced, while the drug revenue, as the main source of hospital’s income, was cut off by the zero mark-up policy for drugs.44,46 These policies motivated hospitals to compete for patients for financial interests. In summary, the pro-competition policy boosted the vitality of the rural hospital market and was conducive to optimizing the allocation of health-care resources.
An unexpected finding identified in our study was that public hospital was reported by 42.4% of county hospital directors as the leading source of competitive pressure, while only 8.6% of hospital directors perceived private hospitals as the leading source of competitive pressure. A possible explanation for such results might be that private hospitals in China are mainly located in economically developed urban areas thus they tend to pose much fewer impacts on rural hospital markets. In addition, as more than around 80% of private hospitals in China are equipped with fewer than 100 beds and are only capable of providing about 10% of all hospital visits in a nationwide range,11 it is not imprudent to conclude that public hospitals have persistently dominated the hospital market in China in spite of the rapid development of private hospitals during recent years.
It should be highlighted that a significantly positive association was found between director-perceived competition and the positivity of competitive behavior, which showed that the hospital director has sufficient motivation and ability to promote hospital performance on realizing the existence of certain degrees of competition posed by the environment. The principal-agent problems between hospital managers and hospital owners are exacerbated by the high information asymmetry in the medical industry. Improving the incentive and supervision mechanism for hospital directors has always been one of the essential goals embedded throughout medical market reforms in China as well as for countries confronted with similar problems. Considering the inconsistency inherent in the goals pursued by the principal and the agent, it is necessary to establish a certain incentive mechanism to stimulate agents’ motivation to work towards the principal’s goal. To achieve a consistent objective function between the agent and the principal, the incentive schemes should be designed based on the agent’s risk preference, which not only enables the agent to obtain a certain stable income, but also associates income gained with efforts made by agents. In addition, strengthening the supervision mechanism for agents is also an important means to protect the interests of hospital owners and to improve hospitals’ performances. A transparent information disclosure system should be established to maximize the possible circulation of information and to reduce information asymmetry.
Based on findings of this study, hospital directors have adopted positive competitive strategies to compete for market share. The hospital’s internal organizational structure was optimized to improve management efficiency. Optimized medical resource allocation within health-care organizations has been considered as an essential strategy for cost saving, while the optimization of organizational structure among various departments facilitates the improvement of technical efficiency needed in the process of health-care deliveries.47 In addition, improving the quality of health-care services was also adopted as an important competitive strategy. The severe information asymmetry issue persistently embedded in the medical service market has compromised the well-established trust between health-care professionals and patients, which consequently exacerbates the conflicts between doctors and patients. Patients with information disadvantage are typically sensitive to the quality of healthcare service delivered by doctors; thus, patients’ satisfaction level towards medical services mainly depends on whether the treatment outcomes have been achieved as expected. Under such circumstances, implementing patient-centered care and providing high-quality medical services would serve as significant contributors to gaining patients’ trust as well as improving the reputation of the hospital.
It is noteworthy that some competitive strategies adopted by the hospitals might also have negative impacts. Our results suggested that quite a number of directors adopted the “medical arms race” strategy such as making huge investments in infrastructure and high-tech medical equipment.36,48 The availability of high-tech equipment and well-constructed infrastructure are perceived as key indicators reflective of the quality of healthcare from patients’ perspective due to the fact that patients lack the expertise to measure the actual quality of healthcare delivered. Patients’ options for medical services are given relatively lower price flexibility,49,50 which therefore creates an opportunity for the prescription of expensive medical tests based on the utilization of high-tech medical facilities. In addition, the competition among hospitals to expand medical infrastructure and medical equipment will increase the fixed costs and sunk costs of hospitals, which will be passed on to patients and ultimately lead to increased medical expenses.51 Under such context, the reform of medical insurance scheme with a switch from post-payment method to prospective payment method should be proposed as an effective strategy to curtail increased medical expenses induced by medical arms race.
An interesting finding from our study was that compared with public hospital directors, private hospital owners were more likely to improve their internal management efficiency when confronted with intensified competition level. After several decades of development, public hospitals in China have established a relatively mature internal management system under the strict surveillance of the Chinese government. By contrast, the internal management systems within private hospitals have demonstrated a number of deficiencies such as the lack of standardized budget controls and poor-established performance evaluation system.52 As the low efficiency embedded in hospitals’ internal management system is very much likely to result in reduced profits, it is not difficult to predict that private hospital owners would be stimulated to optimize their internal management system as a critical strategy for increasing their profits when confronted with intensified hospital competition.
Overall, our study suggested that fierce competition exists among county hospitals in rural China, where the expansion of private hospitals had only posed limited impacts on the hospital market. Based on these findings, a series of compensation measures should be proposed and implemented at the governmental level in order to create a fair competition environment for private hospitals, which would further contribute to boosting the vitality of the healthcare market and promoting the overall quality of healthcare delivery. In addition, we found that hospitals may engage in competitive behaviors with the aim of gaining their own interest at the risk of compromising the overall interests of the whole society. It is therefore highly implicated that strict regulations should be proposed accordingly at health administrative levels in order to facilitate the formation of a well-organized competitive environment via posing strict governmental surveillance on hospitals’ competitive behaviors.
Several limitations should be noted in our study. Firstly, subjective indicator was used for measuring the degrees of competition, but biased outcomes might be induced as self-reported data would largely depend on the cognition of respondents under specific situations. Therefore, it is highly recommended that both objective and subjective indicators be adopted in future studies to identify the differences caused by competition measurements. Secondly, we were not able to avoid the disparities inherent in hospital directors’ characteristics due to data limitations. Thirdly, in our study, the correlation instead of the causal relationship between perceived competition and hospitals’ competitive behaviors was investigated, and potential reversed causality might exist in our model. For example, hospitals that have positively responded to competition are more likely to achieve better hospital performances as well as gaining more market shares, which as the result would pose less competitive pressure on hospital directors. In order to avoid such endogenous issues that potentially existed in our model, panel data or instrumental variables are highly recommended to be adopted in future studies. Fourthly, limited by the small sample size (only 218) and data’s characteristics, the statistical method used in this study might lack complexity in spite of its suitableness for this study. As such, the adoption of other suitable statistical methods might produce generate more interesting results. Last but not least, as we were not able to provide adequate evidences on whether or not the competitive strategies adopted by hospital directors would actually affect hospitals’ performances in the hospital market due to data availability issue, this remains an interesting area to be further explored.
Conclusion
The competition strategy adopted by the hospital when confronted with competition determines whether the goal of pro-competition policy can be achieved. In this study, we explored the relationship between director’s perceived competition and the hospital’s competitive behaviors. The results suggested that higher degrees of perceived competition were found to be significantly associated with higher behavioral positivity levels in terms of adopting competitive strategies. Specifically, hospital directors under higher degrees of competition were found to be more likely to adopt a list of competitive strategies such as improving the efficiency of management, optimizing hospitals’ environment as well as improving the quality and efficiency of health-care services. Strict governmental surveillance should be posed on hospitals’ competitive behaviors in order to facilitate a well-organized competitive environment. Our findings are expected to provide evidence-based implications to inform the implementation of a series of pro-competition policies throughout health-care reforms.
Ethics Approval and Informed Consent
The Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project was initiated by Harvard University, and experts from Peking University, Tsinghua University, Fudan University, Sun Yat-sen University and Sichuan University participated. Ethical approval for this study was obtained from Peking University (IRB00001052-18056) and Harvard University (IRB18-0030). Informed consent to participate in the study has been obtained from the research subjects prior to study commencement.
Acknowledgments
We thank all those who have worked on the Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project. We also thank Xiaojun Lin, Shangle Li, Qingling Jiang, Xiaoshuang Zhao, Tianjiao Lan, and Yufan Deng from Sichuan University for their valuable suggestions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Health Result Innovation Trust Fund (No grant number), the World Bank Group (No grant number), the National Natural Science Foundation of China (Grant No. 71874116 and 72074163), Ministry of Education of China (Grant No. 18YJA790062 and 20YJC790179), Chengdu Federation of Social Science Association (Grant No. ZZ05), Sichuan University (Grant No. 2018hhf-27 and SKSYL201811), and China Medical Board (Grant No. 17-276). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Longo F, Siciliani L, Moscelli G, Gravelle H. Does hospital competition improve efficiency? The effect of the patient choice reform in England. Health Econ. 2019;28(5):618–640. doi:10.1002/hec.3868
2. Shi Z, Zhang W, Wang C, Wu Y. The development history of managed care in USA and lessons to China. China Health Law. 2013;21(04):37–39.
3. Cooper Z, Gibbons S, Jones S, McGuire A. Does hospital competition save lives? Evidence from the English NHS patient choice reforms. Econ J. 2011;121(554):F228–F260. doi:10.1111/j.1468-0297.2011.02449.x
4. Narcı HÖ, Ozcan YA, Şahin İ, Tarcan M, Narcı M. An examination of competition and efficiency for hospital industry in Turkey. Health Care Manag Sci. 2015;18(4):407–418. doi:10.1007/s10729-014-9315-x
5. Pan J. Competition as policy tool for public hospital reform in China. Chinese J Health Pol. 2014;11:48–53.
6. Siciliani L, Chalkley M, Gravelle H. Policies towards hospital and GP competition in five European countries. Health Policy (New York). 2017;121(2):103–110. doi:10.1016/j.healthpol.2016.11.011
7. Pan J, Qin X, Hsieh CR. Is the pro-competition policy an effective solution for China’s public hospital reform? Health Econ. 2016;11:337–357. doi:10.1017/S1744133116000220
8. Jiang Q, Pan J. The evolving hospital market in China after the 2009 healthcare reform. Inquiry. 2020;57:004695802096878.
9. Pan J, Zhao H, Wang X, Shi X. Assessing spatial access to public and private hospitals in Sichuan, China: the influence of the private sector on the healthcare geography in China. Soc Sci Med. 2016;170:35–45.
10. Lu L, Pan J. The association of hospital competition with inpatient costs of stroke: evidence from China. Soc Sci Med. 2019;230:234–245. doi:10.1016/j.socscimed.2019.04.017
11. National Health Commission. China Health Statistics Yearbook; 2019.
12. Pan J, Lei X, Liu GG. Health insurance and health status: exploring the causal effect from a policy intervention. Health Econ. 2016;25:11. doi:10.1002/hec.3225
13. Deng C, Li X, Pan J. Private hospital expansion in China: a global perspective. Global Health J. 2018;2(2):2. doi:10.1016/S2414-6447(19)30138-1
14. Tirole J. The Theory of Industrial Organization. MIT Press; 1988.
15. Krabbe-Alkemade YJFM, Groot TLCM, Lindeboom M. Competition in the Dutch hospital sector: an analysis of health care volume and cost. Eur J Health Econ. 2017;18(2):139–153. doi:10.1007/s10198-016-0762-9
16. Aggarwal A, Lewis D, Mason M, Purushotham A, Sullivan R, Meulen J. Effect of patient choice and hospital competition on service configuration and technology adoption within cancer surgery: a national, population-based study. Lancet Oncol. 2017;18(11):1445–1453. doi:10.1016/S1470-2045(17)30572-7
17. Pan J, Liu D, Ali S. Patient dissatisfaction in China: what matters. Soc Sci Med. 2015;143:145–153. doi:10.1016/j.socscimed.2015.08.051
18. Lin X, Cai M, Fu Q, et al. Does hospital competition harm inpatient quality? Empirical evidence from Shanxi, China. Int J Environ Res Public Health. 2018;15(10):2283. doi:10.3390/ijerph15102283
19. Jiang Q, Tian F, Liu Z, Pan J. Hospital competition and unplanned readmission: evidence from a systematic review. Risk Manag Healthc Policy. 2021;14:473.
20. Qian Y, Jay P. Control under times of uncertainty: the relationship between hospital competition and physician-patient disputes. Int J Equity Health. 2017;16:1.
21. Pan J, Qin X, Li Q, Messina JP, Delamater PL. Does hospital competition improve health care delivery in China? China Econ Rev. 2015;33:179–199. doi:10.1016/j.chieco.2015.02.002
22. Chang C, Chiao Y, Tsai Y. Identifying competitive strategies to improve the performance of hospitals in a competitive environment. BMC Health Serv Res. 2017;17(1):756. doi:10.1186/s12913-017-2699-9
23. Chen M. Dynamic Competition. Peking University Press; 2009.
24. Chen M, Smith KG, Grimm CM. Action characteristics as predictors of competitive responses. Manage Sci. 1992;38(3):439–455. doi:10.1287/mnsc.38.3.439
25. Sara K, Lee S. Managerial response to changing environments: perspectives on problem sensing from social cognition. Adm Sci Q. 1982;27(4):548–570. doi:10.2307/2392530
26. Chen X, Chen L, Wu D. Factors that influence employees’ security policy compliance: an awareness-motivation-capability perspective. J Comp Inf Syst. 2018;58(4):312–324. doi:10.1080/08874417.2016.1258679
27. Pan J, Liu GG, Gao C. How does separating government regulatory and operational control of public hospitals matter to healthcare supply? China Econ Rev. 2013;27:1–14. doi:10.1016/j.chieco.2013.07.002
28. Deng C, Pan J. Hospital competition and the expenses for treatments of acute and non-acute common diseases: evidence from China. BMC Health Serv Res. 2019;19(1):1–14. doi:10.1186/s12913-019-4543-x
29. Cooper Z, McGuire A. Competition on the hospital sector. Encyclopedia Health Econ. 1998;1:117–120. doi:10.1016/B978-0-12-375678-7.01310-9
30. Yu T, Tung Y, Wei C. Can hospital competition really affect hospital behavior or not? An empirical study of different competition measures comparison in Taiwan. Inquiry. 2017;54:1–7. doi:10.1177/0046958017690289
31. Pietro G, Massimo I, Andrea P, Domenico S. Measures of hospital competition and their impact on early mortality for congestive heart failure, acute myocardial infarction and cardiac surgery. Int J Qual Health Care. 2019;31(8):598–605. doi:10.1093/intqhc/mzy220
32. Zinn JS, Weech RJ, Brannon D. Resource dependence and institutional elements in nursing home TQM adoption. Health Serv Res. 1998;33:261–273.
33. Li W. Study on Corporate Governance and Its Pathway of Public Hospital in China. Huazhong University of Science and Technology; 2009.
34. Zhuang J The research of principal-agent and performance management on the head of public hospital in China [Doctor]. Huazhong University of Science and Technology; 2007.
35. Jiao R, Zhang Y. Research on corporate governance structure of public hospitals: from the perspective of principal-agent theory. China Market. 2020;08:112–113.
36. Luft HS, Robinson JC. The impact of hospital market structure on patient volume, average length of stay, and the cost of care. J Health Econ. 1985;4:333–356. doi:10.1016/0167-6296(85)90012-8
37. Delamater PL, Messina JP, Grady SC, WinklerPrins V, Shortridge AM. Do more hospital beds lead to higher hospitalization rates? a spatial examination of Roemer’s Law. PLoS One. 2017;8:2.
38. Luft HS, Robinson JC, Garnick DW, Maerki SC, McPhee SJ. The role of specialized clinical services in competition among hospitals. Inquiry. 1986;23:1.
39. Liu J, Mao Y. Patient satisfaction with rural medical services: a cross-sectional survey in 11 Western Provinces in China. Int J Environ Res Public Health. 2019;16:20.
40. Guizhou Bureau of Statistics. Guizhou Statistical Yearbook; 2019.
41. Guo P Operating environment analysis and competitive strategy of LD hospital in Lanzhou [Master]. Lanzhou University; 2006.
42. Çınar F, Eren E, Mendeş H. Decentralization in health services and its impacts: SWOT analysis of current applications in Turkey. Procedia. 2013;99:711–718. doi:10.1016/j.sbspro.2013.10.542
43. Lin X, Jian W, Yip W, Perceived Competition PJ. Process of care in rural China. Risk Manag Healthc Policy. 2020;13:1161–1173. doi:10.2147/RMHP.S258812
44. Wang X, Yang H, Duan Z, Pan J. Spatial accessibility of primary health care in China: a case study in Sichuan Province. Soc Sci Med. 2018;209:14.
45. Libby MHC, Wm HBJ, et al. Regional market competition is associated with aneurysm diameter at time of EVAR. Ann Vasc Surg. 2020;70:190–196.
46. Li Q, Chen F, Yang M, et al. The effect of China’s national essential medicine policy on health expenses: evidence from a national study. Inquiry. 2018;55:04695801878705.
47. Yang W, Li M, Guo S, et al. The impact of management practice on technical efficiency in public hospitals in China: based on PLS-Structural Equation Modeling. Chin J Health Pol. 2019;12(12):48–54.
48. Liu M, Qin X, Pan J. Does medical equipment expansion lead to more diagnostic services? Evidence from China’s Sichuan Province. Emerg Markets Finan Trade. 2017;53:6. doi:10.1080/1540496X.2016.1247689
49. Phelps CE. Health Economics (Sixth Edition). Routledge; 2017.
50. Folland S. The Economics of Health and Health Care. Routledge;2003.
51. Grossman JM, Banks DA. Unrestricted entry and nonprice competition: the case of technological adoption in hospitals. Int J Econ Business. 1998;5:223–245. doi:10.1080/13571519884521
52. Zhu S. Research on Internal Management of Private Hospitals. Nanchang University; 2011.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.