")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Direct Medical Expenses and Influencing Factors of MDR/RR-TB in Eastern China: Based on Data from Multi-Hospital Information Systems
Authors Zhou M, Peng Y, Liu K , Zhou L, Wang F, Chen X , Chen B , Hu C
Received 5 May 2023
Accepted for publication 2 September 2023
Published 20 September 2023 Volume 2023:16 Pages 1955—1965
DOI https://doi.org/10.2147/RMHP.S420082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jongwha Chang
Meng Zhou,1 Ying Peng,2 Kui Liu,2 Lin Zhou,2 Fei Wang,2 Xinyi Chen,2 Bin Chen,2,3,* Chonggao Hu2,*
1Department of Social Medicine of School of Public Health, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China; 3School of Public Health, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Chen; Chonggao Hu, Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China, Email [email protected]; [email protected]
Background: Multidrug-resistant (MDR) and rifampicin-resistant (RR) tuberculosis (TB) is related to high healthcare costs. However, studies on direct healthcare expenditure in different settings remain inconclusive. Hence, we aimed to examine the direct medical expenses (DME) of patients with MDR/RR-TB and assessed which patient characteristics were associated with higher costs.
Methods: DME was evaluated using records from the hospital information system in three cities with different economic levels in Zhejiang Province, Eastern China, matching with data (including socio-demographics, disease treatment status, etc.) collected in the Tuberculosis Management Information System. A logistic regression model was used to identify variables associated with higher costs.
Results: Of 193 patients with MDR/RR-TB, the average DME was $10,491 (interquartile range (IQR) $4679– 16,710), consisting of $2696 (IQR $1019– 5100) out-of-pocket costs, medical reimbursement, and subsidies, accounting for 32%, 50.3% and 14%, respectively. A total of 74.2% and 56% of DME were for drugs and anti-TB drugs, respectively. Only 16.9% of the patients were treated with an all-oral regimen. Higher DME was significantly associated with local residents 7.29 (95% confidence interval (CI) [2.62– 20.3]), hospitalization experience 7.63 (95% (CI) [2.54– 22.95]), longer duration of treatment 6.63 (95% CI [2.27– 19.35]), and lower health insurance reimbursement 5.65 (95% CI [1.90– 16.79]).
Conclusion: DME of patients with MDR/RR-TB was still significant, and domestic migrants, hospitalization, long treatment duration, and high health insurance rates increased the financial burden on MDR/RR-TB patients. Reasonable intervention programs should be developed to reduce the medical burden of patients with MDR/RR-TB, according to the DME and its component of MDR-TB patients, besides the economic status of their regions.
Keywords: multidrug-resistant tuberculosis, rifampicin-resistant tuberculosis, direct medical expenses, anti-TB drugs, burden
Introduction
The World Health Organisation’s (WHO) proposal to end the global tuberculosis (TB) epidemic by 2035 1 was gradually hampered by the emergence of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB), associated with long-term and complex treatment, expensive drug treatment, severe adverse drug effects, and high mortality rates.2 The burden of morbidity, prevalence, and mortality due to MDR/RR-TB varies globally. In 2022, 33,000 new cases of drug-resistant TB estimated were reported in China, one of the three countries with the highest disease burden of drug-resistant TB in the world.3
Research organizations worldwide had been exploring MDR/RR-TB treatments for nearly 20 years4 since the first edition of the Guidelines for the Treatment of Drug-Resistant Tuberculosis was issued in 1997.5 Subsequently, the Bangladeshi regimen successfully reduced the duration of treatment to 9–11 months and increased the success rate of relapse-free treatments to 87.9%.6,7 The WHO, respectively, recommended the drug combination of moxifloxacin, linezolid, and bedaquiline as the basis for an all-oral long-course regimen in 2018,8 an all-oral short-course regimen of 9–11 months in 2020,9 and a shorter 6-month all-oral regimen of bedaquiline, pretomanid, linezolid, and moxifloxacin (BPaLM) regimen in 2022.10 In China, the treatment regimens for MDR/RR-TB included long-term and short-term therapies,11 in which the long-term one referred to 18–20 month treatment consisting of at least four effective anti-tuberculosis drugs selected from the A, B, and C groups of anti-tuberculosis drugs according to the previous medical history and the results of drug susceptibility test, and the short-term one was a 9–11 month regimen containing bedaquiline, levofloxacin/moxifloxacin, ethionamide, ethambutol, pyrazinamide, high-dose isoniazid, clofazimine (4~6Bdq-Lfx/MFX-Eto-E-Hh-Cfz/5 Lfx/MFX-Cfz-Z-E). Due to the high prevalence of MDR/RR-TB, in addition to sub-optimal cure rates and long treatment duration, the continuous updating of second-line drugs imposes a high financial burden on patients.12 Data from cost analysis studies conducted before 2015 revealed that the average cost of treating MDR/RR-TB cases in high-income, upper-middle-income, lower-middle-income, and low-income countries was $83,365, $5284, $6313, and $1218, respectively.12 In 2016, the WHO reported that the cost per patient for MDR/RR-TB treatment typically ranged from $2000–20,000.13 Recently, T Feuth et al discovered that in Turku, Finland, treatment costs with the new regimen could increase by 10% or decrease by 18%, compared to the old regimen including the use of injections, depending on the duration of bedaquiline use (6 months vs 20 months) in 2019. However, the total cost of the updated treatment regimen increased by 40% in Estonia, illustrating that the cost of treatment varied considerably between countries and even within the same country and was largely dependent on the drug regimen implemented and the practices related to care.14 In 2018, Wang Yun et al assessed patients’ catastrophic expenditures according to national guidelines for the treatment of MDR/RR-TB in 2 prefecture-level hospitals in Guizhou for the diagnosis and treatment of MDR/RR-TB in China; the study revealed that the average total cost of 161 patients with MDR/RR-TB in the first year of treatment was $8266, including 72% of DME covered by a combination of reimbursement (37%) and out-of-pocket (OOP) costs (63%). Specifically, OOP costs ($3715) accounted for 45% of the total costs after reimbursement, indicating that direct medical expenses (DME) of patients represent a large percentage of the total costs and a high financial burden of the disease.15 From 2010 to 2014, with the support of the Global Fund, 89 cities in 30 provinces in China have implemented a plan to strengthen the management of drug resistance. However, with the China Global Fund tuberculosis Project ending in June 2014, the economic burden of drug-resistant tuberculosis patients in regions lacking government subsidies has increased significantly. Although in recent years, China’s basic medical insurance network, consisting of urban employee basic medical insurance (UEMI), new rural cooperative medical insurance (NCMS), and urban resident medical insurance (URMI), has achieved significant development, covering over 1.3 billion people (approximately 95% of the total population) in 2018.16 Simultaneously, a certain financial subsidy for patients with MDR-TB was also provided by the government through designated hospitals or local disease prevention and control centers for disease.
Consistent with non-drug-resistant TB, the economic burden of MDR/RR-TB is due to multiple factors, including delayed visits, length of stay (LOS), low patient adherence, interruptions in the course of treatment, and adverse drug effects.17,18 However, most previous studies estimated the economic burden of patients with MDR/RR-TB based on the results of questionnaire surveys, which have a large retrospective bias.18 Furthermore, with the increasing standardization of treatment regimens for patients with MDR/RR-TB in China and the inclusion of more effective but more expensive drugs in treatment guidelines, the economic burden on patients with MDR/RR-TB may further increase. Therefore, it is important to accurately estimate the economic burden of patients with MDR/RR-TB promptly and understand the factors affecting it. We conducted a cross-sectional study of the DME of patients with MDR/RR-TB based on data from the hospital information system (HIS).
China has unveiled measures for building a zone of common prosperity through high-quality development in Zhejiang province, to explore effective approaches to address the problem of the country’s unbalanced and inadequate development. The prevention and control of major illnesses are also included in the Health Zhejiang Action Plan. As one of the major infectious diseases, the prevention and control of MDR/RR-TB is important to eliminate tuberculosis. The aims of this study are not only to understand the amount and structure of medical costs of patients with MDR/RR-TB but also to provide an evidence basis for policy recommendations for reducing the economic burden of MDR/RR-TB patients in southeastern China and other regions.
Methods
Study Design, Procedures, and Participants
Based on the diagnosis of pulmonary tuberculosis using imaging, sputum smear test, isolation and culture of mycobacterium, and microbiological testing, drug susceptibility tests (DST) were further carried out to diagnose MDR/RR-TB, according to the guidelines for the prevention and treatment of MDR/RR-TB.11 To evaluate the economic level of MDR/RR-TB patients in Zhejiang Province, we randomly selected three prefecture-level cities with high, medium, and low Gross Domestic Product (GDP) in Zhejiang Province, which accounted for more than 33% of the total number of registered MDR/RR-TB cases in Zhejiang in 2018, as the research location. Namely, Hangzhou, Jinhua, and Shaoxing, located in the northern, central, and north-central areas of Zhejiang Province (Figure 1), which we surveyed the economic burden of disease among patients with MDR/RR-TB who registered for treatment in 2018 and completed treatment by 2020 at three MDR/RR-TB designated hospitals in three cities, as drug-resistant patients in Zhejiang were mainly screened at county-level TB designated hospitals and further treated at MDR/RR-TB municipal-level designated hospitals after diagnosis. Among them, patients under the age of 18, as well as ordinary tuberculosis and extrapulmonary tuberculosis, were excluded.
 |
Figure 1 Three cities were selected for the survey in Zhejiang Province, China: Hangzhou, Jinhua, and Shaoxing. |
Additionally, we selected variables available in Tuberculosis Management Information System (TBIMS) for 2018 and retrieved information on case distribution (region), patient characteristics (sex, age), clinical characteristics (drug sensitivity testing, treatment category), treatment (drug regimen, therapeutic department, duration of treatment, frequency of out-patient visits, frequency of hospitalization, and LOS), and outcomes. In cases where the number of patients with MDR/RR-TB registered in each hospital in 2018 was less than 50, sampling was extended to all registered patients with confirmed MDR/RR-TB between July 2017 and June 2019.
The DME of patients was evaluated based on treatment costs and information on medical insurance reimbursements of in-patients and out-patients recorded by the HIS. Besides, with the payment of medical costs in Zhejiang Province deducted directly from the HIS, a cash subsidy was given to the patients by the government, and government subsidies were collected from the Zhejiang Provincial Center for Disease Control and Prevention for the investigated patients throughout their treatment.
Study Definitions
All confirmed TB cases were classified as initial treatment or retreatment. Initial treatment was defined as patients who denied any prior anti-TB treatment or had received anti-TB treatment for ≤30 days. Retreatment was defined as patients who had received anti-TB treatment for>30 days or who had documented evidence of prior treatment from case reports or surveillance databases. The treatment outcomes of patients with MDR/RR-TB, categorised as successful and adverse, were recorded according to the WHO criteria adopted by the TBIMS of China. Successful treatments were defined as cure and treatment completion. Cure was defined as patients who completed treatment without evidence of failure at least three subsequent consecutive cultures are negative with a 30-day interval. Completed treatment was defined as patients who completed treatment without evidence of failure but had insufficient bacterial records; Adverse treatment outcomes, defined as death, discontinued treatment due to adverse effects, loss to follow-up, treatment with ordinary TB regimens, refusal to treat; and other adverse treatment outcomes for reasons other than those listed above.19 Treatment failure was defined as one or more positive sputum cultures in the five final cultures, or one positive culture in the last 12 months of treatment. Death was defined as death from any cause during treatment. Loss of follow-up (default) was defined as a patient whose treatment was interrupted for more than two consecutive months.
Estimation of Costs
We calculated the DME, including out-patient and hospitalization costs of patients with MDR/RR-TB, inclusive of laboratory tests, examinations and treatments, medications, medical devices and nursing care, and accommodation at the hospital. Direct non-medical costs were not included, such as nutrition and transportation costs. DME was estimated by the total medical bill before any deduction for insurance claims and government subsidies. Direct medical OOP costs were defined as the actual direct medical expenses paid by patients, specifically the total medical expenses excluding basic medical reimbursement and government subsidies.20 All costs were recorded in RMB (yuan) and then converted into $ at a currency exchange rate of $1.0 = CNY 6.321 (January 2018).
Statistical Analysis
Continuous variables were first assessed using the Kolmogorov–Smirnov test for normality of distribution; categorical variables were calculated as frequencies. The results for normally distributed data were shown as standard deviation (SD) ± mean, and differences were assessed using the Student’s t-test. Due to the cost-skewed distribution, the median and quartiles (interquartile range (IQR)) were used and examined using the Mann–Whitney U-test and Kruskal–Wallis H-test. We modelled DME as a function of demographic characteristics and treatments, with outcome variables categorized as high and low direct cost burdens based on whether they were above the average DME. Multivariate analyses retained all variables with coefficients significant at P<0.05, were performed using a binary logistic regression model, and odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were calculated. All data were analyzed using SPSS Statistics for Windows (Version 24.0, IBM Corporation, Armonk, NY, USA).
Ethical Approval
This study was approved by the Ethics Committee of the Zhejiang Provincial Center for Disease Control and Prevention, and informed consent was obtained from all participants.
Results
Patient Characteristics
Of the 211 patients with MDR/RR-TB, 193 were included, and 18 were excluded due to a lack of records of out-patient or in-patient medical expenses. Of the eligible patients, with an average age of 46 years (Table 1), the number of men with MDR/RR-TB was more than twice of women (140 vs 53). Nearly 1/4 of the patients were domestic migrants, and more than 2/3 were successfully treated. The average DME of all 193 patients with MDR/RR-TB including medical insurance reimbursement and subsidy costs per case of patients with MDR/RR-TB across all hospitals, was $10,491 (IQR $4679–16,710) (Table 2) higher for the local residents (median $12,616; IQR $6579–14,298) than for the domestic migrants (median $5874; IQR $2815–10,556), and higher for successfully treated patients (median $13,520; IQR $7601–18,175), than for failed treated patients (median $5665; IQR $2079–10,254). The average length of treatment was 20.6 months (IQR 14.2–24.2), and the average length of stay (LOS) was 38 days (IQR 22–58) (Table 1).
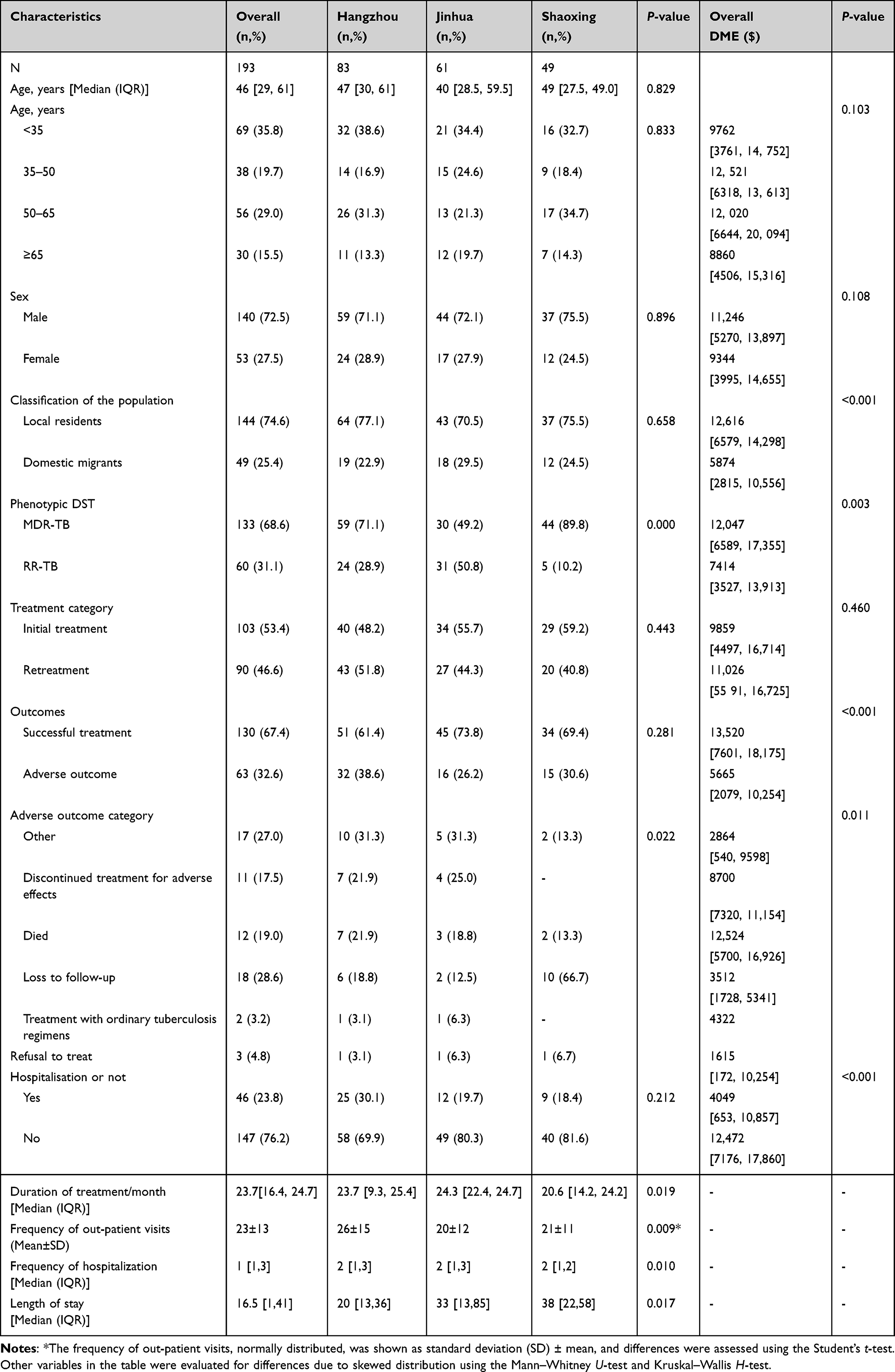 |
Table 1 Baseline Characteristics of the Patients with MDR/RR-TB and Corresponding DME |
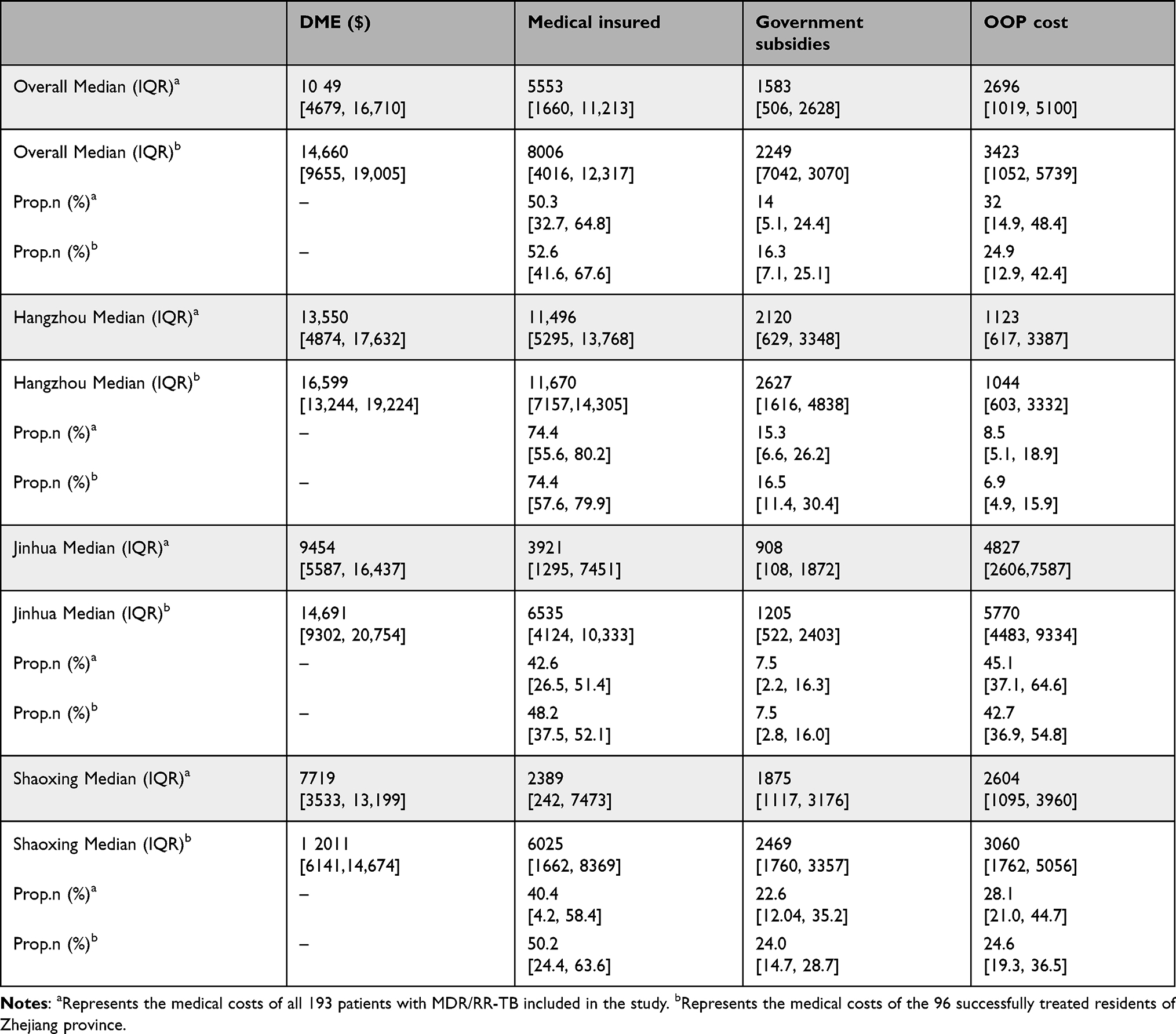 |
Table 2 In-Patient DME per Case Stratified by the Type of Payment |
DME and Direct Medical OOP Cost
The average DME and direct medical OOP cost costs for all patients were $10,491, and $2696, respectively (Table 2). Almost half of the DME was reimbursed by medical insurance, with patients paying 32% of the DME. Among the three hospitals surveyed, the highest proportion of medical insurance costs and lowest direct medical OOP costs were incurred by patients with MDR/RR-TB treated in hospitals in Hangzhou (Appendix 1a). The largest share of DME accounts for the cost of drugs, particularly anti-TB drugs (Appendix 1b). In addition, the average DME and direct medical OOP costs for patients treated successfully with local residents ($14,660; $3423, respectively) were higher than those for all patients ($10,491; $2696, respectively).
Use of Therapeutic Drugs and Related DME
For general TB treatment, among the traditional four therapeutic drugs, 5 (2.6%) patients remained on rifampicin, despite resistance to rifampicin (Appendix 2). In addition, 83.1% of the patients received amikacin, capreomycin, and streptomycin injections. However, few emerging drugs have been used in the anti-TB regimen, of which only 2 (1.1%) patients used bedaquiline, 6 (3.2%) used linezolid, and 10 (5.3%) used clofazimine.
Factors Affecting the Medical Costs
Multivariate regression models comparing the factors associated with DME among patients with MDR/RR-TB broadly replicated the correlations described in the univariate regression analyses (Figure 2). The domicile address, hospitalization, treatment duration, and medical insurance ratio were significantly associated with DME in patients with MDR/RR-TB. Lower DME was significantly associated with domestic migrants with MDR/RR-TB (7.29; 95% CI, 2.62–20.3), and hospitalization was significantly associated with higher DME compared to out-patient treatment only (7.63; 95% CI, 2.54–22.95). Both longer treatment duration (6.63; 95% CI, 2.27–19.35) and lower medical insurance reimbursement ratios (5.65; 95% CI, 1.90–16.79) were associated with higher DME.
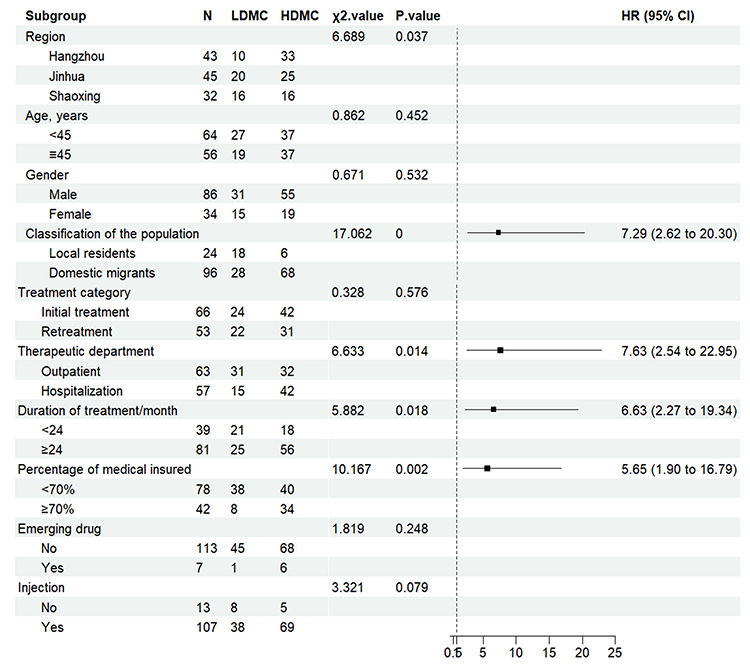 |
Figure 2 Univariate and multifactor comparisons of influencing factors in the low direct burden group (LDME) and the high direct burden group (HDME). |
Discussion
To our knowledge, this is the first study after the update of MDR/RR-TB treatment guidelines by WHO in 2018 to describe DME and associated influences on patients treated in multi-center MDR/RR-TB designated hospitals in Eastern China under real-world conditions, based on data from the HIS but not collected by questionnaires, recalled by patients. Although the proportion of medical insurance reimbursement exceeded 50% of DME, direct medical OOP expense was still high with the use of emerging second-line drugs. And patients with MDR/RR-TB who have been hospitalized, had a long-term treatment, and had medical insurance reimbursement ratio of less than 70% bear a heavier burden of OOP expense.
Under the multi-payer model of medical insurance and financial subsidies, in addition to the basic medical insurance reimbursement for MDR/RR-TB patients in Zhejiang Province, some personal medical expenses were subsidized by the government,22 however, medical costs were still significantly higher than that of treatment for non-drug-resistant TB and MDR/RR-TB in previous studies.23,24 It may be caused by the fact that most of the MDR/RR-TB patients in Zhejiang Province in this survey used cycloserine, moxifloxacin, and other second-line anti-tuberculosis drugs newly recommended in WHO guidelines, which have better efficacy but were more expensive. The reimbursement ratio of multi-drug tuberculosis medical insurance was only 50.3%. The main reason was that the treatment of second-line drugs (cycloserine, linezolid, clofazimine) required for the treatment of MDR/RR-TB was included in the medical insurance as Class B drugs with a low reimbursement rate. In addition, under the background of hierarchical medical policy, the reimbursement rate of medical insurance in China has continued to decrease with the increase of the hospital level, moreover, designated MDR-TB hospitals belonged to high-level hospitals in Zhejiang Province, and medical insurance reimbursement can only be processed after each admission exceeds the deductible. However, there was still a big gap between the reimbursement ratio of outpatient service for TB recommended by the government not less than 70%. In addition, in the medical insurance catalogue, bedaquiline and delamanid drugs can only be reimbursed for MDR/RR-TB patients, suggesting that RR-TB patients may bear a serious financial burden of tuberculosis diagnosis and treatment. Meanwhile, drug expenses accounted for 72.4% of the total expenses in this study. The medical insurance department should further increase the reimbursement ratio, set a zero deductible and increase the types of anti-tuberculosis drugs included in the medical insurance reimbursement category for MDR-TB treatment. The government should optimize the existing medical insurance reimbursement directory and free policies.
In this study, we discovered that the prevalence of the use of newly emerged second-line drugs (eg, bedaquiline, linezolid, and clofazimine) for MDR/RR-TB was low, and the rate of regimens with all-oral drugs was low; possibly caused by drug accessibility, there were bedaquiline supply only in in Hangzhou MDR/RR-TB designated hospitals at that time, in addition, linezolid, clofazimine did not include in the hospital unified procurement catalogue in designated hospitals in Zhejiang Province, in 2018. A long treatment duration, with all regimens lasting an average of approximately 20.6 months, which also aggravated the economic burden of patients to some extent. However, under the new WHO treatment regimen, the cost of treating MDR/RR-TB may be even higher. Therefore, it was important to determine whether the duration and cost of treatment can be further reduced through shorter hospital stays and earlier culture conversion.25 The DME of domestic migrants was higher than that of the local residents in the province due to differences in local government subsidy policies and basic medical insurance in previous studies.18 On the contrary, the DME of domestic migrants in this study was lower, possibly due to the long treatment cycle of MDR/RR-TB, patients may returned to registered residence outside Zhejiang Province for treatment several times during the treatment period, resulting in a lower DME collection.18
The average DME of 284 patients with MDR/RR-TB in Guangzhou in 2018, a city in southern China, was $18,011,26 1.7 times higher than that in this study, and the use of linezolid in Guangzhou was 14 times higher than in this study (44.7% vs 3.2%). Research has shown that after global funds withdraw from China, domestic capital investment has decreased, and the supply of second-line drugs cannot be effectively guaranteed.27 The results of this study suggest that local residents, hospitalization, low medical insurance reimbursement (<70%), and long duration of treatment (≥24 months) were associated with higher DME, which was consistent with the results of many other studies.26 Higher medical costs for MDR/RR-TB treatment would trigger major medical insurance, based on secondary reimbursement on top of medical insurance, reimbursing patients for the high medical costs when suffering from a major disease and preventing them from suffering financial hardship due to the disease. An MDR/RR-TB treatment model with out-patients as the primary treatment modality and shorter treatment duration would reduce the direct financial burden, as the combined effect of the ongoing introduction of drug treatment to shorten LOS and the emergence of more short-term MDR/RR-TB treatment regimens,28,29 would have some impact on the DME of patients with MDR/RR-TB.
This study had some limitations. Firstly, because our study sites were three prefecture-level designated hospitals for MDR/RR-TB in three cities, the cost of presenting with symptoms before having a diagnosis confirmed by treatment at other hospitals was excluded. Therefore, the actual DME may have been underestimated in our study. Secondly, this study focused on DME in patients with MDR/RR-TB, not considering direct and indirect non-medical costs. It has been shown that indirect costs may be higher than direct costs, ranging from 30% to 56% of total costs. Finally, we did not distinguish between the HIV status of patients with MDR/RR-TB and other comorbid conditions, which may have affected the cost differences.
Despite some significant limitations, this study confirms the high cost of MDR/RR-TB treatment in southeastern China. As the prevalence of MDR/RR-TB continues to rise in the coming years and the WHO continues to update treatment regimens in 2022,10 the potential costs associated with MDR/RR-TB prevention and management were expected to be high. DME was much higher in hospitalized patients with low medical reimbursement rates and long treatment duration. Therefore, to improve patient health and manage the long-term increase in healthcare costs, well-designed, high-quality studies are needed to confirm our findings. Also, health insurance reimbursement policies should be adjusted and improved to address the changing economic burden on patients with MDR/RR-TB.
Conclusion
Our findings found that patients with MDR⁃TB were facing a heavy economic burden based on data from the HIS. Domestic migrants, hospitalization, length of treatment, and proportion of medical insurance were strongly associated with the economic burden on patients with MDR/RR-TB. It can expand the coverage of relief policies by improving the accessibility of MDR/RR-TB diagnosis and treatment services particularly the next generation second-line drugs. Based on a greater player of the basic reimbursement of medical insurance, in developing second -line drug procurement and supply and the amount of the subsidy after improving medical insurance reimbursement, multiple parties jointly reduce the burden on patients with MDR/RR-TB. The Chinese government should promote investment in MDR/RR-TB treatment and reduce the economic burden of medical costs. Simultaneously, governments should improve access to, and equity in, healthcare for patients with different types of health insurance.
Abbreviations
DME, Direct medical expenses; IQR, Interquartile range; WHO, World Health Organisation; TB, Tuberculosis; MDR-TB, Multidrug-resistant tuberculosis; RR-TB, Rifampicin-resistant tuberculosis; BPaLM, Bedaquiline, pretomanid, linezolid and moxifloxacin; Bdq, Bedaqualine; Lfx, Levofloxacin; Mfx, Moxifloxacin; Eto, Ethylthioisoniazid; Z, Pyrdinamide; E, Ethambutol; Hh, High-dose isoniazid; Cfz, Chlorofazimine; OOP, Out-of-pocket; LOS, Length of stay; DST, Drug susceptibility tests; TBIMS, Tuberculosis Management Information System; SD, Standard deviation; ORs, Odds ratios; CIs, Confidence intervals; LDME, Low direct burden group; HDME, High direct burden group.
Data Sharing Statement
All data and materials were included in this paper. The corresponding author, Bin Chen, can provide all data upon reasonable request after all studies and sub-studies have been completed.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention and informed consent was obtained from the investigated participants. All participants diagnosed with MDR-TB were fully anonymized before further analysis.
Acknowledgments
We acknowledge and thank Hangzhou, Jinhua, and Shaoxing Center for Disease Control and Prevention (CDC), local community healthcare centers, and tuberculosis-designated hospitals for the implementation of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Zhejiang Provincial Medical and Health Project (Grant Nos.2023KY645) and the National-Zhejiang Health commission Major S&T Project (Grant Nos. WKJ-ZJ-2118).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The end TB strategy 2015; 2015. Available from: https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19.
2. Lange C, Aarnoutse RE, Alffenaar JWC, et al. Management of patients with multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2019;23(6):645–662.PMID: 31315696. doi:10.5588/ijtld.18.0622.
3. World Health Organization. Global tuberculosis report 2022; 2022. Available from: https://www.who.int/publications/i/item/9789240061729.
4. Yang L, Wenhong Z. Evolution of drugs and new advances in the treatment of multidrug-resistant tuberculosis. Adv Pharm. 2021;45(06):419–426.
5. World Health Organization. Guidelines for surveillance of drug resistance in tuberculosis, Guidelines for drug-resistant tuberculosis; 1997.
6. Ahuja SD, Ashkin D, Avendano M, et al. Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: an individual patient data meta-analysis of 9153 patients. PLoS Med. 2012;9(8):e1001300. PMID: 22952439. doi:10.1371/journal.pmed.1001300
7. World Health Organization. WHO.Treatment guidelines for drug-resistant tuberculosis.Geneva:World Health Organization; 2016. Available from: https://www.who.int/publications/i/item/9789241549639.
8. World Health Organization. Treatment guidelines for drug-resistant tuberculosis; 2018. Available from: https://www.who.int/publications/i/item/9789241550079.
9. World Health Organization. WHO consolidated guidelines on tuberculosis: module 4: treatment: drug-resistant tuberculosis treatment; 2020Available from: https://www.who.int/publications/i/item/9789240007048.
10. World Health Organization. WHO consolidated guidelines on tuberculosis. Module 4: treatment - drug-resistant tuberculosis treatment; 2022. Available from: https://www.who.int/publications/i/item/9789240063129.
11. Prevention CCfDCa. Chinese technical guidelines for tuberculosis control and prevention 2021; 2021 Available from: https://tb.chinacdc.cn/xxjlg/202111/W020211119672904030470.pdf.
12. Park H-Y, Ku H-M, Sohn H-S, et al. Cost-effectiveness of Bedaquiline for the treatment of multidrug-resistant tuberculosis in the Republic of Korea. Clin Ther. 2016;38(3):655–667. doi:10.1016/j.clinthera.2016.01.023.
13. World Health Organization. Global tuberculosis report 2016; 2016. Available from: https://www.who.int/publications/i/item/9789241565394.
14. Feuth T, Patovirta RL, Grierson S, et al. Costs of multidrug-resistant TB treatment in Finland and Estonia affected by the 2019 WHO guidelines. Int J Tuberc Lung Dis. 2021;25(7):554–559.PMID: 34183100; PMCID: PMCPMC8259121. doi:10.5588/ijtld.20.0892.
15. Wang Y, McNeil EB, Huang Z, et al. Household financial burden among multidrug-resistant tuberculosis patients in Guizhou province, China: a cross-sectional study. Medicine. 2020;99:28.
16. The L. China through the lens of health in 2018 and beyond. Lancet. 2018;391(10125):999. doi:10.1016/S0140-6736(18)30563-4.
17. Zhang G. Analysis of the Economic Burden of Multidrug-Resistant Tuberculosis in Guangzhou and the Influencing Factors. Guangdong University of Pharmaceutical Sciences; 2021.
18. Jiali Y, Huizhong W, Xia Z, et al. Analysis of factors influencing the economic burden of 162 patients with multidrug-resistant tuberculosis. J Trop Med. 2020;20(04):441–445.
19. Kamara RF, Saunders MJ, Sahr F, et al. Social and health factors associated with adverse treatment outcomes among people with multidrug-resistant tuberculosis in Sierra Leone: a national, retrospective cohort study. Lancet Glob Health. 2022;10(4):e543–e54.PMID: 35303463; PMCID: PMCPMC8938764. doi:10.1016/s2214-109x(22)00004-3
20. Liu Y, Xu C-H, Wang X-M, et al. Out-of-pocket payments and economic consequences from tuberculosis care in eastern China: income inequality. Infect Dis Poverty. 2020;9(1):14. doi:10.1186/s40249-020-0623-8.
21. Exchange SAoF. Table of conversion rates of various currencies to the U.S. dollar; 2018. Available from: https://www.safe.gov.cn/safe/2018/0131/8255.html.
22. Zhao L, Guolong Z, Yulong G, et al. Research and policy recommendations on the current situation of supply security of second-line anti-tuberculosis drugs in 5 provinces and cities. Pharmacoeconomics. 2021;16(02):121–124.
23. Xingxing L, Xun L, Jianjun Y, et al. Investigation and analysis of the economic burden of pulmonary tuberculosis patients in two different economic regions of Hubei Province. Chi J Prev Med. 2016;50(1):1–6. doi:10.3760/cma.j.issn.0253-9624.2016.01.001
24. Ruan YZ, Li RZ, Wang XX, et al. The affordability for patients of a new universal MDR-TB coverage model in China. Int J Tuberc Lung Dis. 2016;20(5):638–644.PMID: 27084818. doi:10.5588/ijtld.15.0413.
25. Diel R, Sotgiu G, Andres S, Hillemann D, Maurer FP. Cost of multidrug resistant tuberculosis in Germany—An update. Int J Infect Dis. 2021;103:102–109. doi:10.1016/j.ijid.2020.10.084.
26. Guangchuan Z. Analysis of the Economic Burden of Multidrug-Resistant Tuberculosis in Guangzhou and the Factors Affecting It. Guangdong University of Pharmaceutical Sciences; 2021.
27. Li R. A Comparative Study on the Effectiveness of Prevention and Treatment Before and After the Conclusion of MDR-TB Control Project of Shandong Global Fund. Shandong University; 2019.
28. Wei T, Feng W. Impact analysis of the payment reform of “same disease with the same price in the same level of hospital” diagnosis-related group based on L City, Guizhou Province: an empirical study. Lancet. 2019;394:S63. doi:10.1016/S0140-6736(19)32399-2.
29. Mok J, Lee M, Kim DK, et al. 9 months of delamanid, linezolid, levofloxacin, and pyrazinamide versus conventional therapy for treatment of fluoroquinolone-sensitive multidrug-resistant tuberculosis (MDR-END): a multicentre, randomised, open-label Phase 2/3 non-inferiority trial in South Korea. Lancet. 2022;400(10362):1522–1530.PMID: 36522208. doi:10.1016/s0140-6736(22)01883-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.