")
Back to Journals » Clinical Ophthalmology » Volume 17
Direct and Dural Carotid Cavernous Sinus Fistulas: Comparison of Clinical Characteristics
Authors Supasai P, Kanjana K, Yospaiboon Y
Received 3 March 2023
Accepted for publication 18 April 2023
Published 25 April 2023 Volume 2023:17 Pages 1207—1214
DOI https://doi.org/10.2147/OPTH.S410930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pawasoot Supasai, Kanwasee Kanjana, Yosanan Yospaiboon
KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Yosanan Yospaiboon, KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, 123 Mitraparb Highway, Khon Kaen, 40002, Thailand, Tel +66-4336-3010, Fax +66-4334-8383, Email [email protected]
Purpose: To compare the clinical characteristics of patients with direct and dural carotid cavernous sinus fistulas (CCFs).
Methods: The medical records of 60 patients diagnosed with CCFs were retrospectively reviewed. The collected data included demographic characteristics, clinical findings, and ocular manifestation. The clinical characteristics of the direct and the dural CCFs were compared on head-to-head basis. Logistic regression analysis was used to demonstrate the direction and magnitude of the difference and reported as odds ratio with its 95% confidence interval.
Results: There were 28 patients (46.67%) with direct CCFs, and 32 patients (53.33%) with dural CCFs. Patients with direct CCF were mostly male (p=0.023), younger age (p< 0.001), had history of trauma (p< 0.001), and more visual impairment at presentation (p=0.025), when compared to those with dural CCFs. In addition, patients with direct CCF had significantly more chemosis (p=0.005), proptosis (p=0.042), bruit (p< 0.001) and dilated retinal vessels (p=0.008) than those with dural CCF. Thirty patients (50%) had increased intraocular pressure (IOP). Mean IOP of the affected eyes was significantly higher than the unaffected eyes (p< 0.0001). In patients with normal IOP, mean IOP of the affected eyes was also higher than the unaffected eyes (p=0.0027).
Conclusion: Patients with direct CCF were younger age, associated with trauma, and more visual impairment at presentation. Chemosis, proptosis, bruit and dilated retinal vessels were detected more in the direct CCF than the dural CCF. Despite normal IOP, affected eyes had significantly higher IOP than the unaffected eyes. Information on these clinical characteristics may be helpful in discrimination of the direct type, which is more urgent for further investigation and treatment.
Keywords: direct carotid cavernous fistula, dural carotid cavernous fistula, clinical characteristics
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Graziano has been published for this article.
Introduction
Carotid cavernous sinus fistulas (CCFs) are abnormal vascular shunts, allowing blood to flow either directly or indirectly from the carotid artery into the cavernous sinus.1 CCFs can be classified based on the hemodynamic properties as low flow or high flow; the etiology as traumatic or spontaneous; and the angiographic anatomy of the shunts following Barrow classification.2 Barrow et al classified CCFs into direct and indirect or dural CCFs.2 Direct CCFs are those arising directly from the carotid artery, while Dural CCFs are those originating from the carotid artery branch vessels. The direct CCF (type A) is the most common type, defined as a direct high-flow shunt between the internal carotid artery and the cavernous sinus. The dural CCF is subdivided into type B, C, and D. Type B is a dural shunt between meningeal branches of the internal carotid artery and the cavernous sinus. Type C is a dural shunt between meningeal branches of the external carotid artery and the cavernous sinus. Type D is a dural shunt between meningeal branches of both the internal and external carotid arteries and the cavernous sinus. The direct CCFs often present acutely and progress rapidly, necessitating urgent treatment, while the dural CCFs tend to be more insidious onset and progress slowly.1
Previous studies have reported the ocular manifestations, angiographic features, endovascular management, treatment outcomes and complications in patients with CCFs.3–18 Although there were numerous studies on the clinical findings of these patients in the literature, most of them were small case series,2,12,15,17,18 or focused on the specific issues. Some studies reported on diagnosis and management of only the dural type.11–14 Some studies emphasized on endovascular management and treatment outcomes,7–9 whereas others studied on glaucoma management and visual outcome.5,16–18 To date, information on comparison of clinical characteristics between direct and dural CCF has been limited.19,20 Therefore, this study aims to report the clinical characteristics of patients with CCFs and compare between the direct and the dural CCFs in a larger series of patients.
Patients and Methods
This study was carried out in accordance with the tenets of the Declaration of Helsinki and was approved by the Khon Kaen University Ethics Committee for Human Research (HE641379). Retrospective medical chart reviews of all patients diagnosed as CCF at the KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand from January 2015 to December 2020 were performed. Although patient consent to review their medical records was not required by the ethics committees, the case report forms had no linkage to the patient identities and the researchers respected the privacy of the patients. The inclusion criteria were patients diagnosed as CCFs and confirmed with radiographic imaging and cerebral angiography. The exclusion criteria were patients who was suspected of CCFs and later proved to be other diagnosis, and who had incomplete data. The collected data included age, gender, duration of symptoms, accidental history, and underlying diseases. The data on eye examination included best-corrected visual acuity (BCVA), intraocular pressure (IOP) and blood in Schlemm’s canal on gonioscopy, proptosis, ophthalmoplegia, bruit, dilated episcleral vessels, and chemosis. The data on posterior segment included dilated retinal vessels, macular edema, intraretinal hemorrhage, and optic nerve head findings.
Intraocular pressure was measured in both the affected eyes and unaffected eyes. We defined increased IOP as IOP >21 mmHg. Patients with IOP ≤ 21 mmHg were classified as normal IOP. In this study, visual acuity was recorded in Snellen notation and converted to logarithm of the minimum angle of resolution (logMAR) unit for analysis. Counting fingers (CF), hand movement (HM), light perception (LP) and no light perception (NLP) were recorded as 2.1, 2.4, 2.7 and 3.0 logMAR respectively, in accordance with the criteria employed by Day et al.21
Statistical Analysis
The collected data were analyzed using Stata version 16.1 (StataCorp, College Station, TX77845 USA). Categorical data such as gender, accident history, underlying diseases, and the clinical signs in CCF patients were reported with frequency and percentage distributions. Age, duration of symptoms, BCVA, and IOP were reported as the mean and standard deviation. Chi-squared test or the Fisher Exact Test was used to compare categorical data between two groups. Independent samples t-test was used to compare numerical data between groups. Paired t-test was used to compare IOP between affected eyes and unaffected eyes. Logistic regression analysis was used to compare the clinical characteristics of direct and dural CCFs, to demonstrate the direction and magnitude of the difference, and reported as odds ratio with its 95% confidence interval. P value < 0.05 was considered statistical significance.
Results
Sixty patients consisted of 25 males (41.67%) and 35 females (58.33%). Mean age of the patients was 47.28 ± 19.03 (95% CI 42.37, 52.19) years. Duration of symptom before attending ophthalmologist was 2.34 ± 2.42 (95% CI 1.70, 2.97) months. Thirty-one patients (51.67%) had history of head trauma, and 20 patients (33.33%) had underlying diseases such as diabetes mellitus, hypertension and dyslipidemia. Mean visual acuity of the patients was 0.71 ± 8.46 (95% CI 0.48, 0.93) logMAR, and mean intraocular pressure was 22.27 ± 8.46 (95% CI 20.08, 24.45) mmHg. There were 28 patients (46.67%) diagnosed with direct CCFs, and 32 patients (53.33%) with dural CCFs, confirmed by catheter cerebral angiography. The demographic characteristics and clinical manifestation of patients with CCFs are shown in Table 1 and Table 2.
 |
Table 1 Demographic Characteristics of the Patients with CCFs |
 |
Table 2 Ocular Manifestations of the Patients with CCFs |
Mean IOP in patients with direct and dural CCFs were 22.93 ± 8.18 and 21.69 ± 8.79 mmHg, respectively. This difference was not statistically significant. In this study, the mean IOP of the affected eyes was higher than the unaffected eyes in all patients (22.27 ± 8.46 vs 15.25 ± 5.12 mmHg; P < 0.001). The direct and dural CCFs also had the mean IOP of the affected eyes higher than unaffected eyes (22.93 ± 8.18 vs 14.96 ± 4.13 mmHg; P < 0.001) and (21.71 ± 9.42 vs 15.75 ± 6.21 mmHg; P < 0.001), respectively (Table 3). Of all 60 patients, increased IOP was present in only 30 patients (50%): 15 patients (53.57%) in the direct CCFs and 15 patients (46.88%) in the dural CCFs. The mean IOP in the increased IOP subgroup was higher than that in the normal IOP subgroup (28.4 ± 7.02 vs 16.13 ± 4.31 mmHg; P < 0.001). Patients with the direct and dural CCF also had similar results (Table 4). In the increased IOP subgroup, affected eyes had higher mean IOP compared with the unaffected eyes (28.4 ± 7.02 vs 17 ± 5.84 mmHg; P<0.001). In the normal IOP subgroup, affected eyes also had higher mean IOP compared with the unaffected eyes (16.13 ± 4.31 vs 13.5 ± 3.59 mmHg; P=0.003). The mean difference was 2.63 ± 4.41 mmHg (95% confidence interval: 0.99, 4.28; Table 5).
 |
Table 3 Mean IOP of Affected and Unaffected Eyes in Patients with Direct and Dural CCFs |
 |
Table 4 Mean IOP of Affected Eyes in Increased IOP and Normal IOP Subgroups |
 |
Table 5 Mean IOP of Affected and Unaffected Eyes in Increased IOP and Normal IOP Subgroups |
Using logistic regression analysis, the clinical characteristics of direct and dural CCFs were compared and shown in Table 6.
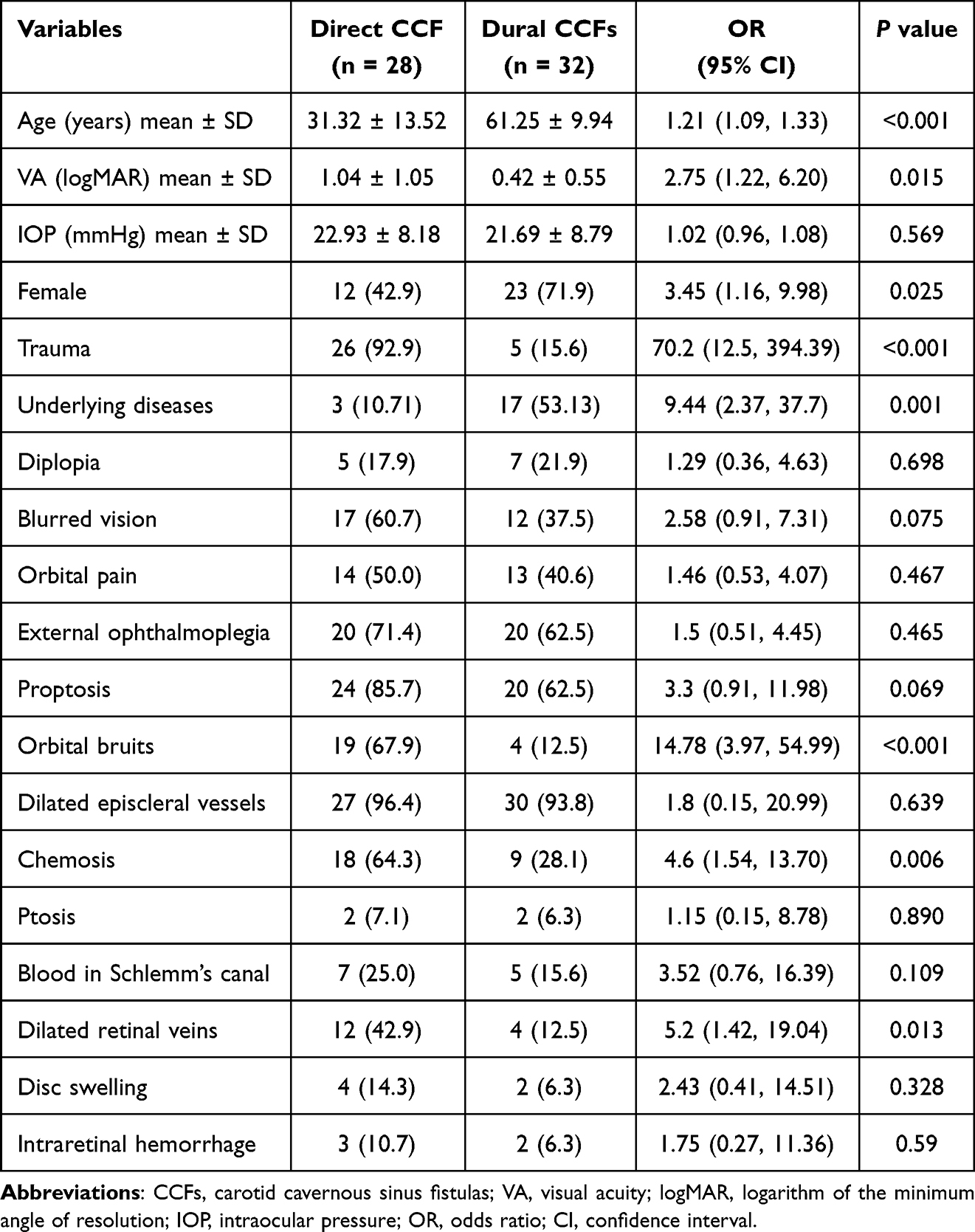 |
Table 6 Logistic Regression Analysis of Clinical Characteristics of CCF Patients |
Age
Mean age of patients with direct and dural CCFs was 31.32 ± 13.52 and 61.25 ± 9.94 years, respectively. Patients with direct CCFs were significantly younger than those with dural CCFs (p < 0.001).
Gender
Patients in the dural CCFs were 23 females (71.9%) and 9 males (28.1%), while those in the direct CCFs were 16 males (57.1%) and 12 females (42.9%). The odds of female patients in the dural group were 3.41 times higher than those in the direct group (p = 0.023).
Trauma
Twenty-six patients (92.9%) in the direct CCF group had history of head trauma, whereas 5 patients (15.6%) in the dural CCF group did. The odds of having trauma in the direct group were 70.2 times higher than those in the dural group (p < 0.001).
Underlying Diseases
Concomitant diseases with CCFs found in this study were diabetic 3.6% in the direct CCF group, and 34.4% in the dural CCF group (p = 0.006), hypertension 7.1% and 34.4% respectively (p = 0.011), and dyslipidemia 0.0% and 15.6%, respectively (p = 0.055). The odds of having underlying diseases in the dural group were 9.44 times higher than those in the direct group (p = 0.001).
Visual Acuity
Mean visual acuity at presentation of patients in the direct CCFs was 1.04 ± 1.05 logMAR, whereas that in the dural CCFs was 0.42 ± 0.55 logMAR. The visual acuity at presentation of patients in the direct CCF group was significantly poorer than that in the dural CCF group (p = 0.005). Moreover, visual loss was noted more in the direct CCFs (60.7%) than in the dural CCFs (37.5%). The odds of having visual loss in the direct group were 2.58 times higher than those in the dural group. However, the difference did not reach a significant level (p = 0.075).
Orbital Bruit
Bruit was more common in the direct CCFs (67.9%) than in the dural CCFs (12.5%). The odds of having orbital bruits in the direct group were 14.78 times higher than those in the dural group (p < 0.001).
Chemosis
Chemosis was found in the direct and dural CCFs in 64.3% and 28.1%, respectively. The odds of having conjunctival chemosis in the direct group were 4.6 times higher than those in the dural group (p = 0.006).
Dilated Retinal Veins
The odds of having dilated retinal veins in the direct group is 5.2 times higher than that in the dural group (p = 0.013). Moreover, proptosis was detected in the direct and dural CCF groups in 85.7% and 62.5%, respectively (p = 0.042). Other details on comparison of clinical characteristics in patients with CCFs are shown in Table 6.
Discussion
In this study, the clinical characteristics of the direct and dural CCFs were studied in detail. The results demonstrated that patients with direct CCFs were younger age, more history of trauma, less underlying diseases, and more visual impairment at presentation, when compared with dural CCFs. In contrast, most of the dural CCF patients were female, older age, less history of head trauma, more association with underlying diseases and less visual impairment. Some of these results have been reported in previous case reports.3,9,12 Das et al reported three cases of spontaneous dural CCF and showed that these patients were usually elderly, women, and associated with atherosclerosis, hypertension and collagen vascular disease or may develop in females during peripartum period.12 Hassan et al showed that traumatic CCFs were usually direct internal carotid artery high-flow fistulas; whereas spontaneous CCFs were usually dural, low-flow fistulas and generally had less severe symptoms than direct CCFs.9 Alam et al revealed that patients in the high flow group were younger and had a history of trauma, when compared to the low flow group.3 Although these clinical characteristics have been reported in previous studies, our study compared these clinical findings in details, on head-to head basis, and used regression analysis to demonstrate clearly the direction and magnitude of the difference.
Regarding clinical findings, both direct and dural CCFs share the common clinical characteristics: diplopia, decreased vision, eye pain, external ophthalmoplegia, proptosis, bruit, arterialization of episcleral vessels, enlarged episcleral veins, chemosis, ptosis, blood in Schlemm ‘s canal on gonioscopy, dilated retinal vessels, enlarged retinal veins, disc swelling and intraretinal hemorrhage. However, the degree of symptoms and signs depend on the types of shunts, the rate of flow and the pressure in the venous drainage.22 Our study showed that patients with direct CCFs had significantly more chemosis, proptosis, bruit and dilated retinal vessels than those with dural CCFs. These clinical findings can be explained by the angiographic features and hemodynamic properties of the direct high flow fistula. Markedly increased venous pressure from the direct arteriovenous shunts cause higher back pressure to the ocular and adnexal tissues, and resulted in more chemosis, proptosis, bruit and dilated retinal vessels, as reported in the previous studies.6,23–26
In our study, the mean IOP was significantly higher in the affected eyes, both the increased IOP and the normal IOP eyes, compared with the unaffected eyes. The result agrees well with the study by Khurana et al that showed a significant difference in IOP between the two eyes of patients with unilateral CCFs.5 This implies that although the affected eyes had normal IOP, these eyes may gradually progress to be ocular hypertension, secondary glaucoma, and irreversible visual loss later in the course. Periodic IOP monitoring in these patients is, therefore, necessary in the follow up of these patients to avoid serious complication.
Patients may initially present to an ophthalmologist with red eyes, conjunctival chemosis, increased IOP, proptosis or decreased vision. Loss of vision may be due to increased IOP and secondary glaucoma, venous retinopathy, and ischemic optic neuropathy.22 Ophthalmologists should have CCFs in the differential diagnosis of patients who have not responded to treatment. Based on patient’s symptoms and signs, ophthalmologist may be the first physician to encounter the patients with CCFs. When there is a high degree of suspicion, they should ask for history of accident or head injury and look for orbital bruits or blood in Schlemm’s canal on gonioscopy. Moreover, patients who have IOP difference between both eyes, should be monitored periodically for secondary glaucoma. Patients with visual impairment or glaucoma, require early diagnosis and prompt treatment to prevent serious consequences of CCFs.
The strength of this study is the head-to-head comparison of the clinical characteristics between direct and dural CCFs. The logistic regression analysis demonstrates the direction and magnitude of the difference in odds ratio with its 95% confidence interval. These findings add the value and the level of evidence of the study. However, there were some limitations. First, the study was retrospective design resulting to incomplete data. Some CCF patients who had incomplete data were excluded from the study according to the exclusion criteria. Second, the data of CCF patients were retrieved from hospital medical charts via ICD-10 coding, which some CCF patients may be missing due to coding errors. These limitations may result in underestimated number of CCF patients in the study.
Conclusions
Our study compared the clinical characteristics in patients with direct and dural CCFs. Patients with direct CCFs were mostly male, younger age, had history of trauma, and more visual impairment at presentation, whereas most patients with dural CCFs were female, older age, less history of trauma, more association with underlying diseases and less visual impairment. Patients with direct CCFs had significantly more chemosis, proptosis, bruit and dilated retinal vessels than those with dural CCFs. Moreover, the mean IOP was significantly higher in the affected eyes, compared with the contralateral unaffected eyes, even though IOP in the affected eyes were normal. Information on these clinical characteristics may be helpful in discrimination of the direct type, which is more urgent for further investigation and treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ellis JA, Goldstein H, Connolly ES Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32(5):E9. doi:10.3171/2012.2.FOCUS1223
2. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62(2):248–256. doi:10.3171/jns.1985.62.2.0248
3. Alam MS, Jain M, Mukherjee B, et al. Visual impairment in high flow and low flow Carotid cavernous fistula. Sci Rep. 2019;9(1):12872. doi:10.1038/s41598-019-49342-3
4. Chaudhry IA, Eikhamry SM, Al-Rashed W, Bosley TM. Carotid cavernous fistula: ophthalmological implications. Middle East Afr J Ophthalmol. 2009;16(2):57–63. doi:10.4103/0974-9233.53862
5. Khurana M, Alam MS, Balekudaru S, et al. Intraocular pressure in the eyes of patients with carotid-cavernous fistula: profile, intereye asymmetry and treatment outcomes. J Glaucoma. 2019;28(12):1074–1078. doi:10.1097/IJG.0000000000001392
6. de Keizer RJW. Carotid-cavernous and orbital arteriovenous fistula: ocular features, diagnostic and hemodynamic considerations In relation to visual impairment and morbidity. Orbit. 2003;22(2):121–142. doi:10.1076/orbi.22.2.121.14315
7. Tan ACS, Farooqui S, Li X, et al. Ocular manifestations and the clinical course of carotid cavernous sinus fistula in Asian patients. Orbit. 2014;33(1):45–51. doi:10.3109/01676830.2013.851253
8. Gemmete JJ, Chaudhary N, Pandey A, Ansar S. Treatment of carotid cavernous fistulas. Curr Treat Options Neurol. 2010;12:43–53. doi:10.1007/s11940-009-0051-3
9. Hassan T, Rashad S, Aziz W, Sultan A, Ibrahim T. Endovascular modalities for the treatment of cavernous sinus arteriovenous fistula: a single-center experience. J Stroke Cerebrovasc Dis. 2015;24(12):2824–2838. doi:10.1016/j.jstrokecerebrovasdis.2015.08.016
10. Holland LJ, Ranzcr KM, Harrison JD, Brauchli D, Wong Y, Sullivan TJ. Endovascular treatment of carotid-cavernous sinus fistula: ophthalmic and visual outcomes. Orbit. 2019;38(4):290–299. doi:10.1080/01676830.2018.1544261
11. Preechawat P, Narmkerd P, Jiarakongmun P, Poonyarhalung A, Pongpech SMD. Dural carotid cavernous sinus fistula: ocular characteristics, endovascular management and clinical outcome. J Med Assoc Thai. 2008;91(6):852–858.
12. Theaudin M, Saint-Maurice JP, Chapot R, et al. Diagnosis and treatment of dural carotid-cavernous fistulas: a consecutive series of 27 patients. J Neurol Neurosurg Psychiatry. 2007;78(2):174–179. doi:10.1136/jnnp.2006.100776
13. Miller NR. Dural carotid-cavernous fistulas: epidemiology, clinical presentation, and management. Neurosurg Clin N Am. 2012;23(1):179–192. doi:10.1016/j.nec.2011.09.008
14. Miller NR. Diagnosis and management of dural carotid-cavernous sinus fistulas. Neurosurg Focus. 2007;23(5):E13. doi:10.3171/FOC-07/11/E13
15. Das JK, Medhi J, Bhattacharya P, et al. Clinical spectrum of spontaneous carotid-cavernous fistula. Indian J Ophthalmol. 2007;55(4):310–312. doi:10.4103/0301-4738.33051
16. Ishijima K, Kashiwagi K, Nakano K, Shibuya T, Tsumura T, Tsukahara S. Ocular manifestations and prognosis of secondary glaucoma in patients with carotid-cavernous fistula. Jpn J Ophthalmol. 2003;47(6):603–608. doi:10.1016/j.jjo.2003.08.002
17. Calafiore S, Perdicchi A, Scuderi G, Contestabile MT, Abdolrahimzadeh S, Recupero SM. Glaucoma management in carotid cavernous fistula. Case Rep Ophthalmol. 2016;7(2):296–302. doi:10.1159/000446151
18. Heichei J, Hammer T, Solymosi L, Brandt S, Winter I. Pressure lowering effect of fistula occlusion in a patient with secondary glaucoma due to an intracranial arteriovenous fistula. Ophthalmol Ther. 2015;4(2):135–141. doi:10.1007/s40123-015-0036-0
19. Wang YW, Zhong Y, Ma J, Yang N, Wang KF, Jiang Y. Clinical features of carotid-cavernous fistulas in 23 patients. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2014;36(2):158–163. doi:10.3881/j.issn.1000-503X.2014.02.008
20. Grumann AJ, Boivin-Faure L, Chapot R, Adenis JP, Robert PY. Ophthalmologic outcome of direct and indirect carotid cavernous fistulas. Int Ophthalmol. 2012;32(2):153–159. doi:10.1007/s10792-012-9550-4
21. Day AC, Donachie PHJ, Sparrow JM, Johnston RL. The royal college of ophthalmologists’ national ophthalmology database study of cataract surgery: report 1, visual outcomes and complications. Eye. 2015;29:552–560. doi:10.1038/eye.2015.3
22. Stiebel-Kalish H, Setton A, Nimii Y, et al. Cavernous sinus dural arteriovenous malformations: patterns of venous drainage are related to clinical signs and symptoms. Ophthalmology. 2002;109:1685–1691. doi:10.1016/S0161-6420(02)01166-1
23. Wang W, Li YD, Li MH, et al. Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: a single-center experience. J Clin Neurosci. 2011;18:24–28. doi:10.1016/j.jocn.2010.06.008
24. Gupta AK, Purkayastha S, Krishnamoorthy T, et al. Endovascular treatment of direct carotid cavernous fistulae: a pictorial review. Neuroradiology. 2006;48:831–839. doi:10.1007/s00234-006-0132-x
25. Lewis AI, Tomsick TA, Tew JM Jr. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995;36:239–245. doi:10.1227/00006123-199502000-00001
26. Meyers PM, Halbach VV, Dowd CF, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2002;134:85–92. doi:10.1016/S0002-9394(02)01515-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.