Back to Journals » Journal of Pain Research » Volume 18
Digital Cognitive Behavioral Therapy for Insomnia in Cancer Pain Patients: Protocol for a Prospective, Randomized Controlled Trial
Authors Lan X, Hu X, Lan Z, Wang L ![]() , He R, Jiang Z
, He R, Jiang Z
Received 28 July 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:18 Pages 7053—7063
DOI https://doi.org/10.2147/JPR.S556779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Xiaoxiao Lan,* Xin Hu,* Zhixuan Lan,* Liu Wang, Ruilin He, Zongbin Jiang
Department of Pain Medicine, The Second Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530007, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruilin He, Email [email protected] Zongbin Jiang, Email [email protected]
Introduction: Insomnia is one of the most common complications in cancer patients, and Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment for insomnia in the general population and patients with a cancer diagnosis. Traditional CBT-I is susceptible to limitations such as geography, physical condition, and cost of access to healthcare, hindering its widespread adoption. With the application and development of digitalization and artificial intelligence providing opportunities for the administration and promotion of Digital Cognitive Behavioral Therapy for Insomnia (DCBT-I) to provide a better sleep treatment option for cancer pain patients, this study aims to evaluate its efficacy.
Methods: This single-center trial will randomize 158 cancer pain patients with insomnia to DCBT-I or sleep hygiene education (1:1) to test if DCBT-I is superior for improving sleep quality. Assessments will also cover pain intensity, mental health, and quality of life.
Discussion: This study will provide valuable clinical evidence that DCBT-I helps to improve sleep quality, pain intensity, mental health, and quality of life in cancer pain patients suffering from insomnia and contributes to the dissemination of this non-pharmacological alternative treatment option.
Conclusion: This study protocol outlines a rigorous randomized controlled trial to evaluate the efficacy of Digital Cognitive Behavioral Therapy for Insomnia (DCBT-I) compared to Sleep Hygiene Education (SHE) in cancer pain patients with comorbid insomnia. The Resleep smartphone-based intervention integrates evidence-based CBT-I components (sleep restriction, stimulus control, cognitive restructuring, and relaxation training) to address the limitations of traditional therapy, such as accessibility and cost.
Clinical Trial Registration: This study is a registered clinical trial.
Registry: Chinese Clinical Trial Registry (ChiCTR), listed in the WHO International Clinical Trials Registry Platform (WHO ICTRP).
Trial Registration Number: ChiCTR2500096855.
Date of Registration: 07 February 2025.
Registration Url: https://www.chictr.org.cn/index.html.
Keywords: cancer pain, insomnia, DCBT-I, sleep hygiene education
Background
Insomnia is recognized as a prevalent comorbidity among oncology patients. Epidemiological investigations have demonstrated that the occurrence of cancer-related insomnia approaches threefold that observed in the general population, with approximately 30–50% of individuals with malignancy exhibiting clinically significant insomnia symptoms.1 Of particular significance, pain and sleep dysfunction have been identified as critical determinants of survival quality in patients with intermediate to advanced-stage neoplastic disease. Furthermore, a complex bidirectional relationship between sleep dysregulation and oncological progression has been posited.2 Sleep disorders in cancer patients may be caused by a variety of reasons, including pre-existing sleep problems, cancer-induced dysphoria, or side effects of cancer treatment, and sleep disorders themselves may exacerbate the side effects of cancer treatment or trigger cancer-related psychological dysfunction.2
The pathogenesis of nocturnal disturbances in cancer populations is multifactorial, potentially encompassing pre-existing insomnia, disease-related distress, or treatment-induced adverse effects. Conversely, such disturbances have been shown to exacerbate therapy-related complications or contribute to malignancy-associated psychological morbidity.2 More specifically, oncologic pain has been demonstrated to directly disrupt sleep architecture, while maladaptive cognitions regarding the sleep–pain relationship in cases with comorbid insomnia and chronic pain may further perpetuate this condition.3 Notably, insomnia and its clinical consequences have been reported by some long-term survivors as being more distressing than antineoplastic therapy itself.4
About 25% to 50% of cancer patients use medications to improve condition,5 but the effectiveness of these treatments is often limited by undesirable side effects. In contrast, complementary and integrative modalities have emerged as viable alternatives for oncology-related insomnia management, with accumulating evidence indicating that non-pharmacological interventions can yield substantial therapeutic benefits.6–8 Established behavioral sleep interventions include Sleep Hygiene Education (SHE), stimulus control therapy, relaxation techniques, and Cognitive Behavioral Therapy for Insomnia (CBT-I).9,10 While SHE is predominantly employed in primary care settings for insomnia,9,10 the latter approach has been recommended as first-line treatment for chronic insomnia in clinical practice guidelines.9
However, the administration of conventional CBT-I is constrained by geographical barriers, patient physical limitations, and economic considerations. With the advancement of digital therapeutics, internet-delivered CBT-I has been developed as an innovative treatment delivery system.1,11 It has been established that this digital intervention demonstrates superior efficacy to waitlist controls or SHE in both short- and long-term outcomes, positioning it as an effective comprehensive therapeutic strategy – particularly for cases with comorbidities such as chronic pain, fibromyalgia, or breast malignancy.10–14 Nevertheless, the comparative effectiveness of digital versus conventional SHE in oncological patients with comorbid pain and insomnia remains to be elucidated, particularly within the Chinese cultural context.
To address this knowledge gap, a randomized clinical trial protocol is proposed to compare the therapeutic outcomes of digital CBT-I and SHE in individuals with cancer-related pain and concomitant insomnia. The experimental intervention is delivered through “Resleep,” a smartphone application,13 that implements CBT-I principles via algorithmically personalized treatment regimens. The core therapeutic components comprise sleep hygiene education, stimulus control procedures, relaxation techniques, sleep restriction, and cognitive restructuring. Of note, participant interaction with an AI chatbot enables continuous collection and analysis of sleep parameters, insomnia symptoms, and sleep-related cognitions, facilitating the generation of individualized treatment plans. By comparison, the control cohort utilizes the identical digital platform while receiving only SHE and stimulus control content. Relevant to this investigation, preliminary studies have validated the efficacy of this application for managing uncomplicated insomnia in Chinese populations.13
Aims and Hypothesis
This study aims to: Examine the effects of Digital Cognitive Behavioral Therapy for Insomnia compared to Sleep Hygiene Education on sleep quality, pain intensity, mental health, and quality of life in patients with cancer pain combined with insomnia.
The research hypotheses to be tested are: Compared to the SHE group, patients with cancer pain combined with insomnia who receive DCBT-I experience greater positive changes in sleep quality, pain intensity, mental health, and quality-of-life responses at the end of the intervention, and at 1- and 3-month follow-up.
Methods
Patient and Public Participation
Patients and/or the public did not participate in any stage of the design, execution, reporting, or distribution of the plans of this study.
Study Design and Participants
Participants will be enrolled and screened from March 2025 to April 2025 through advertisement-based and inpatient recruitment at the Second Affiliated Hospital of Guangxi Medical University, with a focus on oncology and pain management wards. Comprehensive study disclosures are administered to potential subjects by trained attending physicians, including detailed explanations of: (1) research objectives, (2) the aforementioned intervention protocol, (3) anticipated benefits, (4) potential risks, and (5) corresponding mitigation strategies. Written informed consent is secured, after which baseline evaluations are conducted, including acquisition of demographic characteristics, medical history, and relevant clinical parameters during the screening visit.
Eligible candidates who completed a 7-day sleep log are randomly allocated in a 1:1 ratio to either Digital Cognitive Behavioral Therapy for Insomnia (dCBT-I; experimental group) or Sleep Hygiene Education (SHE; comparator group). Upon enrollment, all study subjects are equipped with a study-specific wearable device and are directed to install and access the designated mobile platform according to their group allocation. The 6-week therapeutic period is commenced immediately post-enrollment, with treatment compliance and clinical outcomes being tracked by investigators through passive data acquisition without active intervention. The study design schematic is presented in Figure 1.
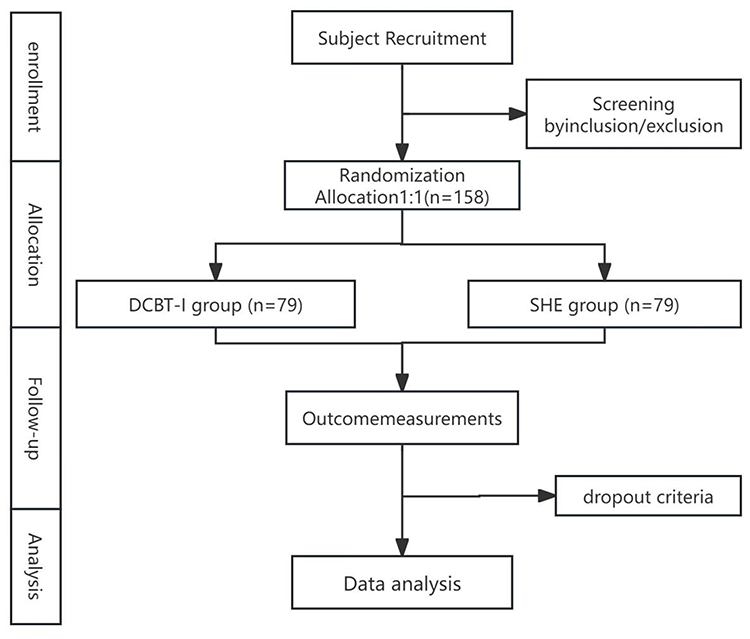 |
Figure 1 Trials flow diagram of the trial. Abbreviations: DCBT-I, Digital Cognitive Behavioral Therapy for Insomnia; SHE, Sleep Hygiene Education. |
The study strictly adhered to the 2013 SPIRIT Statement and the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Guangxi Medical University (Approval No. 2024-KY(0819)).
This clinical trial has been prospectively registered in the Chinese Clinical Trial Registry (ChiCTR), listed in the WHO International Clinical Trials Registry Platform (WHO ICTRP), under the registration number ChiCTR2500096855 on 07 February 2025. The registration details can be accessed at https://www.chictr.org.cn/index.html.
The results of this study will be disseminated through scientific journals and conferences to provide evidence-based support for the global application of DCBT-I in cancer pain patients with insomnia. Participant recruitment will begin on 01 March 2025 and is expected to continue until 31 December 2028.
Eligibility Criteria
Inclusion Criteria
- Age at least 18 years;
- Pathological diagnosis of malignant tumor;
- Meet the diagnostic criteria for chronic insomnia disorder according to the International Classification of insomnia, Third Edition (ICSD-3), including problems with falling asleep or maintaining sleep for at least 3 months (3 times per week) with impaired daytime functioning, despite the availability of sleep opportunities;
- Pittsburgh Sleep Quality Index (PSQI) score greater than 11 points;
- Patients on prescription sleep medications who have been on the same medication and the exact dosage for at least 1 month are not expected to have changes in medication and dosage during the acute intervention phase.
- Proficient in the use of a smartphone app and comfortable reading, filling out the electronic questionnaire, communicating, and fully understanding the content;
- Sign the informed consent form.
Exclusion Criteria
- Have severe cognitive dysfunction or mental illness (eg, significant suicidal ideation, bipolar disorder, aggressive behavior, manic or schizophrenic disorder, severe dementia, etc).;
- Have apnea-sleep apnea syndrome, severe heart or lung disease;
- Previously undergoing psychotherapy for insomnia or anticipating such treatment within the next 6 months;
- A score of ≥12 on the Epworth Sleepiness Scale;
- Failure to provide informed consent.
Dropout Criteria
- If a subject develops other comorbidities, complications, or specific physiologic changes during the trial deemed inappropriate for continuation, the subject will be classified as a case withdrawal.
- If a subject experiences a serious or critical adverse event during the trial that our research team judges as inappropriate for continuation, the subject will be withdrawn.
- If a subject adds a drug not listed in the protocol or receives an external treatment, it will be considered a protocol violation and must be removed from the trial.
- Subjects may choose to recuse themselves for personal reasons or may be lost to follow-up in the final stages of the trial.
Our research team will actively complete the final follow-up and examination for all withdrawal cases, collect data, and analyze effectiveness and safety. Details of all withdrawal cases, including trial results and reasons for withdrawal, will be fully documented on the case report form.
Randomization and Blinding
The randomization algorithm is computationally generated utilizing IBM SPSS Statistics 25.0 (IBM Corp, Armonk, NY). Concealment of allocation is safeguarded by an independent trial coordinator at the Second Affiliated Hospital of Guangxi Medical University who had no involvement in therapeutic delivery.
Subject assignment to either the Digital Cognitive Behavioral Therapy for Insomnia (dCBT-I) or the sleep hygiene education cohort is performed in a 1:1 ratio following the predetermined randomization matrix. Blinding regarding treatment allocation is rigorously maintained for all study participants throughout the investigation period.
Interventions
Intervention Group
Participants in the intervention group receive a 6-week digitally delivered CBT-I program through the Resleep platform (Shenzhen Zeen Health Technology Co., Ltd). The aforementioned therapeutic regimen integrates five evidence-based modalities: (1) sleep hygiene instruction, (2) stimulus control procedures, (3) relaxation training, (4) sleep restriction protocol, and (5) cognitive therapeutic techniques. The complete intervention framework and corresponding treatment components are comprehensively detailed in Table 1.
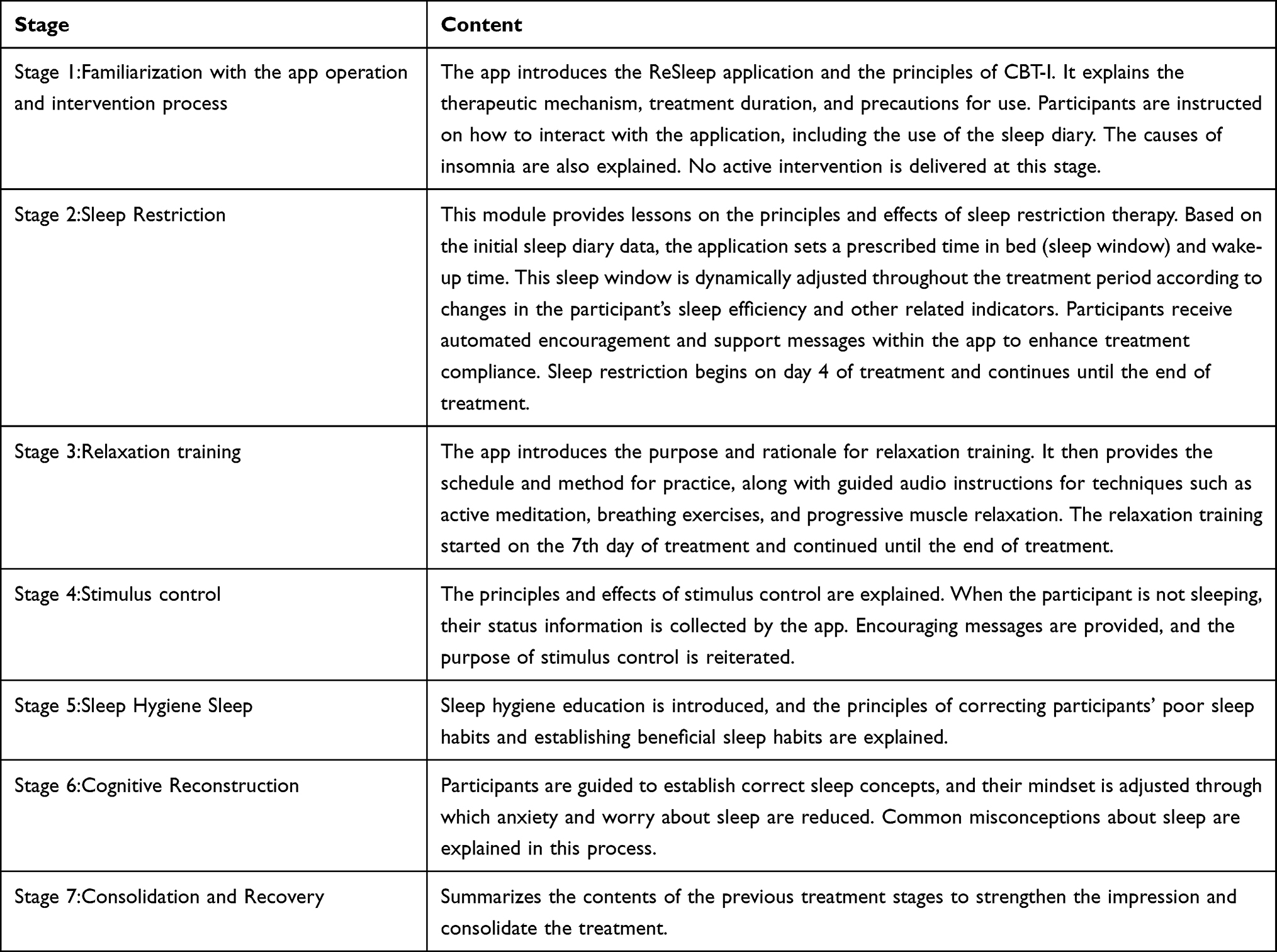 |
Table 1 Contents of DCBT-I Application Phases |
Control Group
The SHE is delivered on the same online platform as the DCBT-I intervention, with matched format and contact time to ensure parity in delivery. The SHE content consists of structured, didactic materials covering standard sleep hygiene principles, including guidance on optimizing the sleep environment, regulating daily behaviors and diet, establishing exercise routines, and developing healthy pre-sleep habits.
Follow-up and Participant Timeline
Patients are systematically followed up from baseline (D0), throughout the 6-week DCBT-I or SHE intervention, and at 1- and 3-month post-intervention follow-up (M1 and M3). The schedule of enrolment, interventions, and assessments is shown in Table 2.
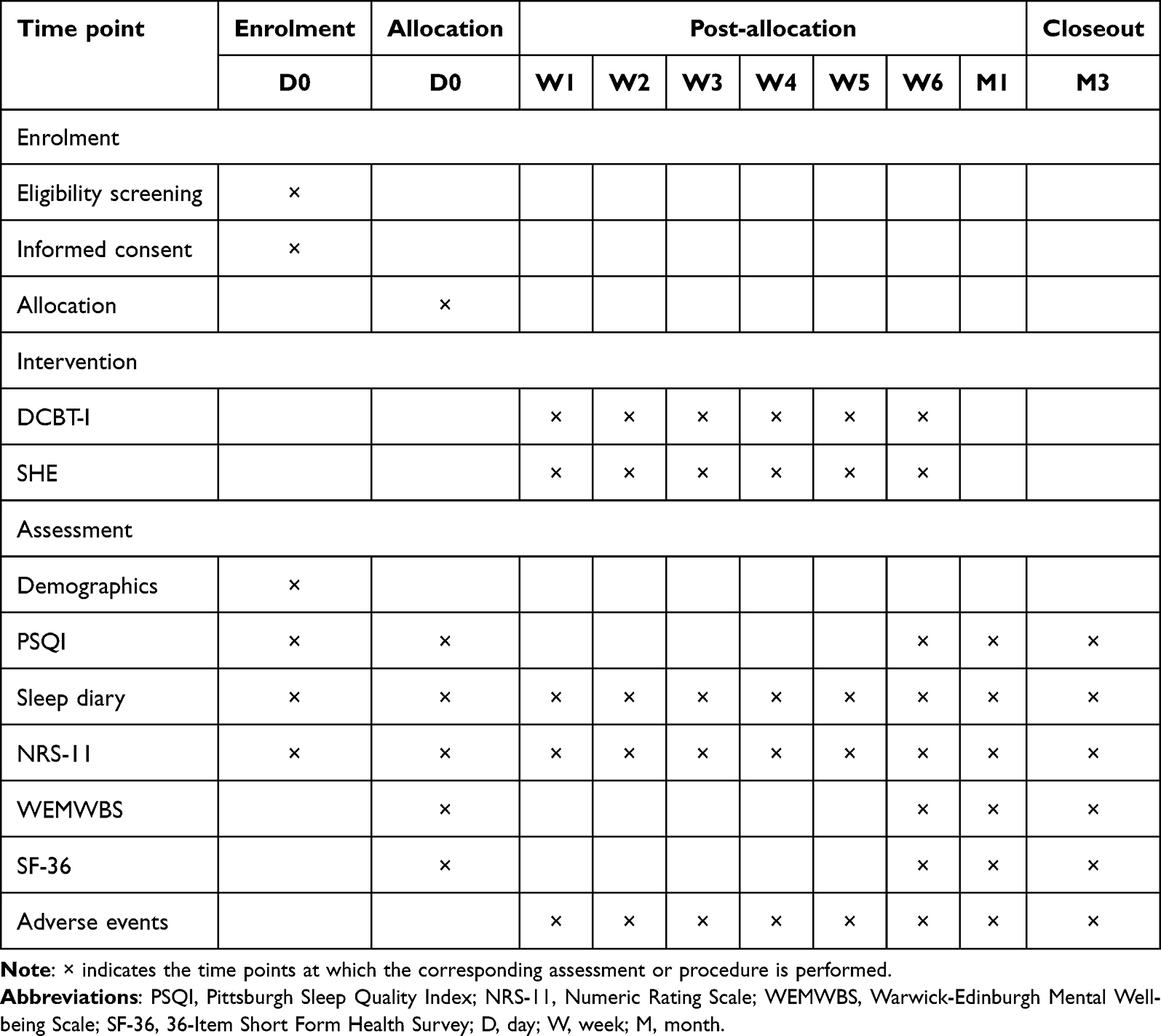 |
Table 2 Time Schedule of Participant Enrolment, Allocation, and Assessment |
Outcome Assessment
Primary Outcomes
Nocturnal sleep parameters are evaluated using the Pittsburgh Sleep Quality Index (PSQI), a well-established self-report instrument that quantifies sleep quality over a 1-month period. The measure comprises 19 items grouped into seven components: (1) subjective sleep quality, (2) sleep latency, (3) sleep duration, (4) sleep efficiency, (5) sleep disturbances, (6) use of sleep medication, and (7) daytime dysfunction. Each component is scored on a 0 to 3 scale. The global PSQI score, ranging from 0 to 21, represents the sum of these components, with higher scores indicating worse sleep quality. The primary outcome is the global PSQI score at 6 weeks (post-intervention). PSQI assessments are conducted at baseline (D0), post-intervention (W6), and at 1- and 3-month follow-ups (M1 and M3) to evaluate short- and longer-term effects. Scores at M1 and M3 are analyzed as secondary outcomes to examine the sustainability of treatment effects.
Secondary Outcomes
- Sleep Parameters Assessment: Sleep metrics are continuously monitored through a wearable actigraphy device, with complementary data being collected via a 7-day digital sleep diary. Participants are instructed to maintain daily sleep logs throughout the 6-week intervention period and during the 7-day pre-follow-up phase. Four key parameters are derived by the research team: (i) total time in bed (TIB), (ii) total sleep time (TST), (iii) sleep efficiency (SE), and (iv) wake after sleep onset (WASO), all of which are calculated using standardized algorithms.
- Pain Intensity Evaluation: Pain levels are quantified utilizing the 11-point Numeric Rating Scale (NRS-11),15 wherein participants are required to indicate current pain intensity on a scale from 0 (“no pain”) to 10 (“worst imaginable pain”). Pain severity is categorized as follows: mild (1–3) is defined as being tolerable without functional impairment; moderate (4–6) is characterized by interference with daily activities; and severe (7–10) is classified as being debilitating and necessitating urgent clinical intervention.
- Mental Well-being Analysis: Psychological status is assessed employing the validated 14-item Warwick-Edinburgh Mental Well-Being Scale (WEMWBS),16 which encompasses three domains: affective (eg, “I feel happy”), cognitive (eg, “I am hopeful about the future”), and conative functioning. Each item is rated on a 5-point Likert scale (1=“never” to 5=“always”) based on the preceding two-week period. A composite score (range: 14–70) is generated through summation, with higher values being positively correlated with greater psychological well-being.
- Health-related Quality of Life Measurement: Quality of life is evaluated using the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36).17–19 This instrument’s 36 items capture eight health domains, which are subsequently transformed into standardized scores (range: 0–100) through norm-based scoring algorithms. Higher scores are consistently associated with more favorable health outcomes across all measured dimensions.
Statistical Analysis
All statistical analyses will be performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) and R (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics will be used to summarize baseline characteristics and outcome measures: continuous variables will be presented as means ± standard deviations (or medians and interquartile ranges, as appropriate), and categorical variables as frequencies and percentages. Between-group comparisons of baseline demographic and clinical characteristics will be conducted using independent-samples t-tests (or non-parametric tests if normality assumptions are violated) for continuous variables and χ2-tests (or Fisher’s exact tests) for categorical variables to assess the success of randomization.
The primary outcome is the global PSQI score at 6 weeks (post-intervention). The primary hypothesis is that patients receiving DCBT-I will show a greater improvement in PSQI compared with those receiving SHE at 6 weeks. To test this hypothesis, we will use a linear mixed-effects model with a random intercept for each participant and fixed effects for group (DCBT-I vs SHE), time (baseline, 6 weeks, 1-month follow-up, 3-month follow-up), and the group × time interaction. Baseline PSQI and any baseline variables showing clinically relevant imbalance between groups will be included as covariates. The primary comparison will focus on the group × time interaction at the 6-week time point, corresponding to the difference in change from baseline to 6 weeks between groups.
Secondary continuous outcomes (actigraphy-derived sleep parameters, NRS-11 pain scores, WEMWBS scores, and SF-36 domain scores) will be analyzed using similar linear mixed-effects models with appropriate link functions. Model assumptions (linearity, homoscedasticity, and normality of residuals) will be checked; if serious violations are detected, data transformation, robust standard errors, or generalized linear mixed models will be considered. Bivariate relationships among changes in sleep parameters, pain indices, psychological metrics, and quality-of-life measures will be explored using Pearson correlation coefficients with 95% confidence intervals. These analyses will be regarded as exploratory, and no formal adjustment for multiple comparisons will be applied; results will be interpreted cautiously.
All primary analyses will follow the intention-to-treat (ITT) principle, including all randomized participants in the groups to which they are originally allocated, regardless of adherence. A per-protocol analysis including only participants who complete the intervention according to the predefined protocol will be conducted as a sensitivity analysis. Missing data will be handled using multiple imputation under the assumption of missing at random. Multiple imputation by chained equations will be used to generate 20 imputed datasets including all outcome variables, treatment group, time points, and relevant baseline covariates; parameter estimates will be combined using Rubin’s rules. Outliers and influential observations will be identified using standardized residuals and influence diagnostics (eg, Cook’s distance). Data entry errors, when identified, will be corrected; plausible outliers will be retained in the primary ITT analyses, with additional sensitivity analyses conducted excluding these observations. Statistical significance for all inferential analyses will be determined using a two-tailed α level of 0.05.
Sample Size Calculation
The sample size calculation was based on the primary outcome, the global PSQI score at the end of the 6-week intervention (W6). Based on previous studies,20 the mean PSQI score after sleep hygiene education and reflexology is 5.5 with a standard deviation (SD) of 2.1. We assumed a similar mean and SD for the SHE control group in the present trial. Based on clinical experience and the existing literature, we considered a between-group difference of 1.0 point in the PSQI global score at 6 weeks to be clinically relevant. Using a two-sided, two-sample t-test to compare the mean PSQI at W6 between groups, with a significance level of 0.05, a power of 80%, and an SD of 2.1 in each group, we calculated with PASS software (version 15.0.5; NCSS, Kaysville, Utah, USA) that a minimum of 71 patients would be required per group.
Allowing for an anticipated dropout rate of approximately 10%, we plan to enrol 79 patients in each group, for a total sample size of 158 participants. Since the main analysis will use a linear mixed-effects model with repeated measures, which typically provides greater statistical efficiency than a simple two-sample comparison at a single time point, this sample size calculation based on the 6-week PSQI can be regarded as conservative.
Handling of Outliers and Missing Data
A multiple-fill approach will be applied to address missing data. Outliers will be identified based on their source and nature to determine whether correction, removal, or application of data transformation methods are necessary to mitigate their impact.
Data Collection and Management
Data Collection
We will use an electronic data capture (EDC) system to collect pre-treatment baseline data, including demographic characteristics, PSQI, NRS-11, WEMWBS, and SF-36. To ensure data accuracy and confidentiality, all data will initially be recorded on a paper Case Report Form (CRF) and then verified and entered into the EDC by the Data Manager.
Data Safety Monitoring Committee: The Data Safety Monitoring Committee (DSMC) will conduct periodic data reviews to ensure that the study is conducted safely and that any potential safety issues are identified promptly and on time.
Data Access and Protection
All participant information and assessments will be collected through an electronic data collector that complies with China’s Data Security Law (DSL) and China’s healthcare information specification standards. All researchers accessing the data must sign a confidentiality agreement and receive training on data protection regulations.
Adverse Events
Adverse events (AEs) will be recorded in detail in the CRF and assessed by the researchers for their causal relationship with treatment. The physician will record and evaluate adverse events’ nature, timing, duration, severity, and outcome. All adverse events will be promptly addressed and reported to the study monitor and the Institutional Review Board (IRB), especially those that are serious or life-threatening. The aim is to deal with problems promptly and on time, including stopping the study if necessary.
Discussion
This study aims to investigate the effectiveness of DCBT-I in the treatment of cancer pain combined with insomnia. Given the tremendous burden of insomnia on patients’ quality of life, it is critical to find an effective and inexpensive non-pharmacologic treatment for insomnia in patients with cancer pain.
Strengths and Innovations
Innovative Digital Therapeutic Intervention
This investigation introduces a mobile health-delivered Digital Cognitive Behavioral Therapy for Insomnia (dCBT-I) specifically developed for patients with cancer-related pain and comorbid insomnia. The aforementioned digital platform substantially improves therapeutic accessibility while addressing China’s unique healthcare challenges: (1) extensive geographical service demands, (2) unequal medical resource distribution, (3) heightened cancer pain-related insomnia prevalence, and (4) near-ubiquitous smartphone ownership.
Methodological Approach
The experimental design implements a randomized parallel-group comparison between the dCBT-I program and conventional sleep hygiene education. The therapeutic regimen incorporates four empirically validated components beyond standard protocols: (i) stimulus control methodology, (ii) relaxation training, (iii) sleep restriction protocol, and (iv) cognitive restructuring techniques.
Clinical Outcomes
As substantiated by prior research,21,22 the implemented intervention demonstrates significant reductions in dysfunctional sleep-related cognitions alongside measurable improvements in sleep architecture parameters among cancer pain patients. These physiological and psychological modifications subsequently yield enhanced sleep-related quality of life metrics, improved psychological well-being indices, and optimized pain modulation outcomes. The accumulated evidence positions dCBT-I as a primary non-pharmacological therapeutic alternative for insomnia management in this patient population.
Comprehensive Evaluation
The study is designed to evaluate therapeutic efficacy through standardized follow-up assessments conducted at three time points: immediately following the 6-week intervention, and at 1-month and 3-month post-intervention intervals. This temporal design enables comparative analysis of both short- and long-term treatment effects between dCBT-I and SHE interventions.
The primary endpoint is defined as the Pittsburgh Sleep Quality Index (PSQI) global score measured at treatment completion and each follow-up assessment. Secondary outcomes included sleep parameters derived from 7-day sleep diaries recorded prior to each evaluation timepoint. Exploratory outcomes comprised: (i) pain intensity reduction (assessed via NRS-11), (ii) psychological well-being improvement (measured by WEMWBS), and (iii) quality-of-life enhancement (evaluated using SF-36).
Successful demonstration of intervention efficacy would establish this digital therapeutic approach as a novel, clinically viable non-pharmacological treatment option for insomnia in cancer pain patients.
Challenges and Limitations
Several study limitations merit careful consideration. First, ensuring protocol adherence during longitudinal follow-up represents a critical challenge for evaluating sustained therapeutic outcomes. To address this concern, an automated reminder system coupled with participant engagement protocols will be employed.
The experimental design incorporates single-blinding (allocation concealment only) due to the inherent characteristics of behavioral interventions, potentially introducing performance bias. This methodological constraint will be counterbalanced through implementation of blinded endpoint adjudication and standardized assessment protocols.
Regarding study generalizability, the single-center implementation, while facilitating rigorous protocol adherence and data uniformity, may limit population representativeness. Multicenter validation studies will consequently be required to establish broader clinical applicability.
Notably, physiological sleep monitoring is conducted using commercial wearable technology rather than polysomnographic equipment, potentially affecting measurement precision. Subsequent investigations would benefit from incorporating validated actigraphy devices or laboratory-based polysomnography to enhance objective sleep parameter quantification.
Conclusion
This study protocol outlines a rigorous randomized controlled trial to evaluate the efficacy of DCBT-I compared to SHE in cancer pain patients with comorbid insomnia. The Resleep smartphone-based intervention integrates evidence-based CBT-I components to address the limitations of traditional therapy. The use of SHE as a control group provides a credible and active comparator, strengthening the validity of our findings, though its inherent therapeutic value may constrain the observed effect size. The findings are designed to provide clinically meaningful evidence generalizable to the broader cancer pain population, with the lack of long-term follow-up identified as a focus for future research.
Trial Status
The Second Affiliated Hospital of Guangxi Medical University has approved the protocol. We plan to start recruiting trial subjects on March 1, 2025, and expect the study to last 3 years to reach the target of 158 participants. At the time of manuscript submission, no participants had been enrolled.
Abbreviations
AE, Adverse Event; CRF, Case Report Form; DCBT-I, Digital Cognitive Behavioral Therapy for Insomnia; DMC, Data Monitoring Committee; ICH-GCP, International Conference on Harmonisation - Good Clinical Practice; IRB, Institutional Review Board; ITT, Intention to Treat; NMPA, National Medical Products Administration; NRS, Numeric Rating Scale; PP, Per Protocol; PPS, Per Protocol Set; PSQI, Pittsburgh Sleep Quality Index; SHE, Sleep Hygiene Education; SAE, Serious Adverse Events; SF-36, 36-Item Short-Form Health Survey; WEMWBS, Warwick-Edinburgh Mental Well-being Scale.
Data Sharing Statement
The datasets generated or analysed during the current study are not publicly available due to the need to protect the privacy of individuals who participated in the study. However, they are available from the corresponding author R.H. on reasonable request.
Ethics Approval and Consent to Participate
This study strictly adheres to the 2013 SPIRIT Statement and the Declaration of Helsinki and has been approved by the Ethics Committee of the Second Affiliated Hospital of Guangxi Medical University (Approval Number: 2024-KY(0819)). This clinical trial is registered on the Chinese Clinical Trial Registry platform (ChiCTR) at https://www.chictr.org.cn/index.html (ChiCTR2500096855), registered on 2025-02-07. The results will be disseminated through scientific journals and conferences, aiming to provide evidence supporting the global management of cancer pain in patients with insomnia. The study is expected to start on March 1, 2025, and continue until December 31, 2028.
Author Contributions
X.L., X.H., and Z.L. contributed equally to the conception, study design, and drafting of the manuscript. They were primarily responsible for writing the initial draft and developing the methodology. L.W. was responsible for the graphical drafting and visualization. R.H. and Z.J., as co-principal investigators, made substantial contributions to the interpretation of data and the critical revision of the study design and protocol for important intellectual content. They also oversaw the scientific planning and coordination to ensure the integrity of the trial.
All authors made a significant contribution to the work reported, have approved the final version of the manuscript, and have agreed on the journal to which the article has been submitted. Furthermore, all authors reviewed and agreed on all versions of the manuscript throughout the revision process and are accountable for all aspects of the work.
Funding
This work was supported by the Guangxi Key R&D Program (Guike AB21220047) and the Guangxi Key Clinical Specialty Construction Project.
Disclosure
The authors declare no conflicts of interest.
References
1. Büttner-Teleagă A, Kim Y-T, Osel T, et al. insomnia in cancer–a systematic review. Int J Environ Res Public Health. 2021;18(21):11696. doi:10.3390/ijerph182111696
2. Mogavero MP, DelRosso LM, Fanfulla F, et al. insomnia and cancer: state of the art and future perspectives. Sleep Med Rev. 2021;56:101409. doi:10.1016/j.smrv.2020.101409
3. Ravyts SG, Perez E, Dzierzewski JM. Pain-related beliefs about sleep as a predictor of insomnia symptoms and treatment acceptability. Sleep Med. 2022;96:122–127. doi:10.1016/j.sleep.2022.05.008
4. Squires LR, Rash JA, Fawcett J, et al. Systematic review and meta-analysis of cognitive-behavioural therapy for insomnia on subjective and actigraphy-measured sleep and comorbid symptoms in cancer survivors. Sleep Med Rev. 2022;63(101615). doi:10.1016/j.smrv.2022.101615
5. Choi T-Y, Kim JI, Lim H-J, et al. Acupuncture for managing cancer-related insomnia: a systematic review of randomized clinical trials. Integr Cancer Ther. 2017;16(2):135–146. doi:10.1177/1534735416664172
6. Dupont A, Bower JE, Stanton AL, et al. Cancer-related intrusive thoughts predict behavioral symptoms following breast cancer treatment. Health Psychol. 2014;33(2):155–163. doi:10.1037/a0031131
7. Espie CA, Fleming L, Cassidy J, et al. Randomized controlled clinical effectiveness trial of cognitive behavior therapy compared with treatment as usual for persistent insomnia in patients with cancer. J Clin Oncol. 2008;26(28):4651–4658. doi:10.1200/JCO.2007.13.9006
8. Fleming L, Randell K, Harvey C-J, et al. Does cognitive behaviour therapy for insomnia reduce clinical levels of fatigue, anxiety and depression in cancer patients? Psychooncology. 2014;23(6):679–684. doi:10.1002/pon.3468
9. Sutton EL. Insomnia. Ann Intern Med. 2021;174(3):ITC33–ITC48. doi:10.7326/AITC202103160
10. Dopheide JA. Insomnia overview: epidemiology, pathophysiology, diagnosis and monitoring, and nonpharmacologic therapy. Am J Manag Care. 2020;26(4 Suppl):S76–S84. doi:10.37765/ajmc.2020.42769
11. Soh HL, Ho RC, Ho CS, et al. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med. 2020;75:315–325. doi:10.1016/j.sleep.2020.08.020
12. Horsch CH, Lancee J, Griffioen-Both F, et al. Mobile phone-delivered cognitive behavioral therapy for insomnia: a randomized waitlist controlled trial. J Med Internet Res. 2017;19(4):e70. doi:10.2196/jmir.6524
13. Zhang C, Liu Y, Guo X, et al. Digital cognitive behavioral therapy for insomnia using a smartphone application in china: a pilot randomized clinical trial. JAMA Network Open. 2023;6(3):e234866. doi:10.1001/jamanetworkopen.2023.4866
14. Cheng P, Kalmbach DA, Hsieh H-F, et al. Improved resilience following digital cognitive behavioral therapy for insomnia protects against insomnia and depression one year later. Psychol Med. 2023;53(9):3826–3836. doi:10.1017/S0033291722000472
15. Hartrick CT, Kovan JP, Shapiro S. The numeric rating scale for clinical pain measurement: a ratio measure? Pain Pract. 2003;3(4):310–316. doi:10.1111/j.1530-7085.2003.03034.x
16. Maheswaran H, Weich S, Powell J, et al. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): group and individual level analysis. Health Qual Life Outcomes. 2012;10(1):156. doi:10.1186/1477-7525-10-156
17. Roszkowska M, Białczyk K. Coping styles and quality of life in breast cancer patients undergoing radiotherapy. Cancers. 2023;15(23):5515. doi:10.3390/cancers15235515
18. Okayama T, Suzuki K, Morishita S, et al. Pretreatment quality of life and survival in patients with lung cancer: a systematic review and meta-analysis. BMC Cancer. 2024;24(495). doi:10.1186/s12885-024-12267-w
19. watt T, Christoffersen T, Brogaard MB, et al. Quality of life in thyroid cancer. Best Pract Res Clin Endocrinol Metab. 2023;37(1):101732. doi:10.1016/j.beem.2023.101732
20. Zengin L, Aylaz R. The effects of sleep hygiene education and reflexology on sleep quality and fatigue in patients receiving chemotherapy. Eur J Cancer Care. 2019;28(3):e13020. doi:10.1111/ecc.13020
21. Faaland P, Vedaa Ø, Langsrud K, et al. Dysfunctional beliefs and attitudes about sleep (DBAS) mediate outcomes in dCBT-I on psychological distress, fatigue, and insomnia severity. Sleep Med. 2023;110:1–6. doi:10.1016/j.sleep.2023.07.018
22. Gao Z, Gao Z, Zheng C, et al. Reliability and validity of the cancer-related dysfunctional beliefs and attitudes about sleep scale in cancer patients. BMC Psychiatry. 2024;24(1):144. doi:10.1186/s12888-024-05580-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.