Back to Journals » International Journal of Women's Health » Volume 18
Differential Maternal Physiological Stress Responses During Rooming-In: High Stress in Newborn Sleeping versus Relief in Breastfeeding
Authors Lin HH ![]() , Lee WC, Chen CI, Lin HD, Tsai YL, Kang J, Yang CF, Chang HY
, Lee WC, Chen CI, Lin HD, Tsai YL, Kang J, Yang CF, Chang HY
Received 6 March 2026
Accepted for publication 13 June 2026
Published 9 July 2026 Volume 2026:18 607469
DOI https://doi.org/10.2147/IJWH.S607469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Hui-Hsuan Lin,1 Wei-Chung Lee,2 Cheng-I Chen,3 Hong-Dun Lin,4 Yi-Lu Tsai,5 Jessica Kang,6 Cheng-Fang Yang,7,8 Hao-Yuan Chang1,7,9
1School of Nursing, College of Medicine, National Taiwan University, Taipei, Taiwan; 2Department of Management, Singular Wings Medical, Hsinchu, Taiwan; 3Department of Algorithm, Singular Wings Medical, Hsinchu, Taiwan; 4Culture and Sports Technology Service Division, Service Systems Technology Centre, Industrial Technology Research Institute, Hsinchu, Taiwan; 5Department of AI Research & Development, ZPOWER Technology Co., Ltd., Hsinchu, Taiwan; 6Department of Obstetrics and Gynaecology, National Taiwan University Hospital, Taipei, Taiwan; 7Department of Second Degree Bachelor of Science in Nursing, College of Medicine, National Taiwan University, Taipei, Taiwan; 8Department of Nursing, National Taiwan University Hospital Yunlin Branch, Yunlin, Taiwan; 9Department of Nursing, National Taiwan University Hospital, Taipei, Taiwan
Correspondence: Hao-Yuan Chang, School of Nursing, College of Medicine, National Taiwan University, No. 1, Sec. 1, Jen-Ai Road, Taipei, 100233, Taiwan, Tel +886223123456 ext. 288893, Fax +886223219913, Email [email protected]
Background: Postpartum stress (PPS) significantly risks maternal-infant health, yet how specific newborn behavioral states are dynamically associated with maternal physiological stress during rooming-in remains unknown.
Purpose: This study examined the associations among maternal stress, rooming-in levels, and newborn states during early postpartum hospitalization.
Methods: A prospective repeated-measures observational study with consecutive sampling was conducted at a hospital in Taiwan. Eligible participants were healthy, full-term, primiparous women after vaginal birth accompanied by a partner; those with clinical complications or cardiac arrhythmias were excluded. A total of 43 women completed the overall longitudinal assessments. Maternal normalized low frequency (nLF) was monitored via portable ECG across four newborn states (crying, breastfeeding, being held, sleeping). Among them, a subgroup of 30 mothers provided complete newborn state diaries and continuous ECG data for synchronized analysis. Data were analyzed with descriptive statistics, paired samples t-tests, and correlation tests.
Results: Overall maternal nLF increased significantly from Day 1 (T1) to Day 3 (T2) (p=0.022, N=43). No significant associations were observed between nLF and rooming-in levels (p> 0.05, n=30). Contrary to our hypothesis, 73% of participants experienced the highest level of maternal physiological stress while the infant slept (nLF=65.4%), suggesting a state of situational alertness. Conversely, breastfeeding demonstrated a distinct stress-relieving potential, with 40% of participants exhibiting their lowest stress levels (nLF=60.2%).
Conclusion: Infant sleep is linked to maternal situational alertness rather than rest, while breastfeeding offers stress-relief potential. This study provides preliminary exploratory evidence that maternal autonomic activity varies across caregiving contexts.
Keywords: postpartum women, postpartum maternal stress, newborn states, rooming-in care, electrocardiography, heart rate variability
Introduction
Postpartum stress (PPS) is defined as a mother’s reaction to an external or internal stressor, managed through adaptive or maladaptive coping mechanisms. PPS is positively correlated with postpartum depression,1,2 which shares risk factors such as high life stress, poor social support, and prenatal depression.3 Elevated PPS poses risks for both mother and infant, including neonatal developmental delays and maternal mental health disorders.4,5 International evidence reveals that these elevated maternal stress levels and physiological regulatory mechanisms are directly manifested through alterations in biomarkers such as cortisol and heart rate variability (HRV), which in turn negatively influence exclusive breastfeeding outcomes and maternal-infant bonding.6,7
Common PPS triggers, especially for first-time mothers (primiparous), involve frequent newborn crying, health concerns, partner relationship difficulties, and lack of social support.8–11 Furthermore, Asian primiparous women face additional socio-cultural and breastfeeding pressures.12 Beyond these external factors, maternal states, such as fatigue and pain, are potential stressors that may confound the assessment of PPS. Postpartum fatigue has been consistently identified as a core component of the maternal distress burden, showing strong correlations with depressive symptoms and stress in both meta-analytic and longitudinal studies.13,14 Similarly, postpartum pain, including childbirth-related and immediate physical discomfort, is associated with increased psychological distress and traumatic symptomatology.15
Emerging evidence has indicated that newborn neurobehavioral indicators and early behavioral states (e.g., arousal and attention) can significantly correlate with or predict maternal psychological and physiological stress responses.16,17 However, current research has neglected to explore the relationship between specific newborn behaviors (i.e., crying, breastfeeding, sleeping, or being held) and maternal stress during the rooming-in period.
To ensure the rigor of our comparison across newborn states, this study also examines whether these observed physiological responses are influenced by maternal fatigue and pain, treating them as critical variables to assess for potential baseline differences among different stress-level categories. HRV serves as an objective and valid physiological tool to assess human psychological stress responses. When an individual encounters psychological or environmental stressors, homeostatic balance is disrupted, triggering a classic autonomic nervous system (ANS) shift characterized by sympathetic activation and parasympathetic (vagal) inhibition. A recent comprehensive review indicated that among various metrics, low-frequency (LF)/ high frequency (HF) ratio (reflecting sympathetic dominance) is one of the most frequently reported indices significantly correlated with stress experiences.18,19 Therefore, tracking relative variations in these frequency-domain components provides a rigorous, real-time reflection of maternal situational alertness and autonomic adaptation.
Hypothesis Development: Infant States and Maternal Stress
The impact of infant behavioral states on maternal well-being is multifaceted. Infant crying serves as a primary stressor, significantly increasing maternal emotional distress and perceived stress that persists up to six months postpartum.20,21 During the rooming-in period, the urgency of responding to a crying infant often exacerbates maternal exhaustion and severe sleep deprivation.22
While breastfeeding and holding involve nurturing behaviors, their impact on stress is nuanced. Breastfeeding presents a bidirectional relationship with stress: although oxytocin promotes a calming effect, elevated cortisol from postpartum stressors can impair milk production.23 Similarly, although skin-to-skin contact (SSC) is known to reduce anxiety,24,25 the physical demands of holding remain a form of active caregiving.
In contrast, the infant sleep state provides a period of physiological stability and reduced caregiving demands. Evidence suggests that longer infant sleep duration and fewer mother night awakenings correlate with lower maternal perceived stress,20,26 even among mothers with a history of depression.27 Unlike the active demands of crying, breastfeeding, or being held, sleep offers a critical window for maternal recovery.
Based on these behavioral and biobehavioral rationales, we hypothesized that the complete removal of active caregiving demands during infant sleep would shift maternal autonomic regulation toward a state of rest, thereby minimizing objective physiological stress. Thus, we hypothesized that maternal stress levels would be significantly lower when the newborn was in a sleep state compared to the other three states (crying, breastfeeding, and being held).
Although rooming-in is widely implemented to support breastfeeding and maternal-infant bonding, limited research has examined maternal physiological stress responses during rooming-in using objective autonomic measures. To address the limitations of conventional subjective questionnaire-based stress measurement,28 this study adopts a rigorous objective approach. We use HRV, an established physiological measurement of stress,29 measured via portable electrocardiogram (ECG) sensors, which are considered the gold standard for accurate data capture.30
Furthermore, to enhance the internal validity of our findings, we assessed the potential confounding effects of fatigue and pain by comparing maternal fatigue and pain levels in the neonatal states that elicited the highest and lowest normalized low frequency (nLF) responses. This analytical approach allowed us to determine whether differences in physiological stress were independent of maternal subjective fatigue and pain.
Aim
This study aims (1) to examine the association between maternal stress during hospitalization and rooming-in levels, and (2) to investigate the relationship between maternal PPS and newborn states. To achieve these aims, this study evaluates maternal HRV responses across different newborn behavioral states to better understand maternal stress in early postpartum care. We hypothesize that: (1) maternal stress is negatively associated with rooming-in engagement, and (2) the mother’s PPS level will be lowest when the newborn is asleep, compared to other newborn states. Understanding these patterns will enable healthcare professionals to provide targeted, proactive postpartum support strategies to reduce maternal stress, optimize maternal recovery, and support successful rooming-in implementation.
Methods
Study Design & Setting
We adopted a prospective repeated-measures observational design with consecutive sampling. This design was specifically selected to capture two distinct layers of maternal physiological stress during rooming-in. First, it allows us to evaluate the longitudinal changes in maternal physiological stress between two postpartum time points: Postpartum Day 1 (T1) and Day 3 (T2). Second, it enables the examination of the relative differences in maternal physiological stress responses associated with various newborn states (sleeping, crying, being held, and breastfeeding) from T1 to T2.
We collected data in the postpartum ward of a northern hospital in Taiwan from January to June 2023. Each participant completed informed consent before participation. Before data collection, the study protocol was reviewed and approved by the Research Ethics Committee of National Taiwan University Hospital (Approval No. 202012271RIPD).
Population and Sampling
The sample size was calculated using G*Power 3.1.9.631 to examine the correlation between newborn states and postpartum stress. A two-tailed point-biserial correlation model was employed, setting the α error rate at 0.05, the statistical power (1-β) at 0.80, and the effect size at 0.5, resulting in a required sample size of 26 families. Considering a 15% dropout rate based on prior studies,32 the recruitment target was adjusted to 31 families (26/0.85 = 30.58, rounded up). Ultimately, 43 families participated in this study.
The inclusion criteria were: primiparous participants (a) 4 to 24 hours after vaginal birth (considering the clearance of exogenous oxytocin and epidural anesthesia); (b) over the age of 18; (c) gestational age of between 37 and 42 weeks; and (d) accompanied by a partner during postpartum hospitalization.
The exclusion criteria included: (a) people with clinical conditions during pregnancy or childbirth, such as coagulation dysfunction, severe placenta previa, or complications during childbirth; (b) fetus or newborn with congenital or acquired abnormalities in the fetus or newborn; or (c) people with cardiac arrhythmias, as irregular rhythms with an R-R interval greater than 0.12 seconds affect HRV results.33
Among the 236 vaginal birth postpartum women screened, 56 met the inclusion criteria. We measured maternal stress at 2 different time points (i.e., Day 1 [T1] and Day 3 [T2] postpartum) for comparison. Among the 56 individuals who met the inclusion criteria, 11 declined to participate, resulting in a total of 45 participants (80% participation rate). During the study, 2 participants were excluded because their newborns were transferred to a special care nursery on the second day due to jaundice, resulting in a dropout rate of 4%. Thus, 43 participants completed the study. When analyzing maternal HRV on different newborn states, any poor HRV signal detection and incomplete records on newborn states were excluded when examining whether stress levels were associated with various newborn states during rooming-in (N = 30). The flowchart is shown in Figure 1.
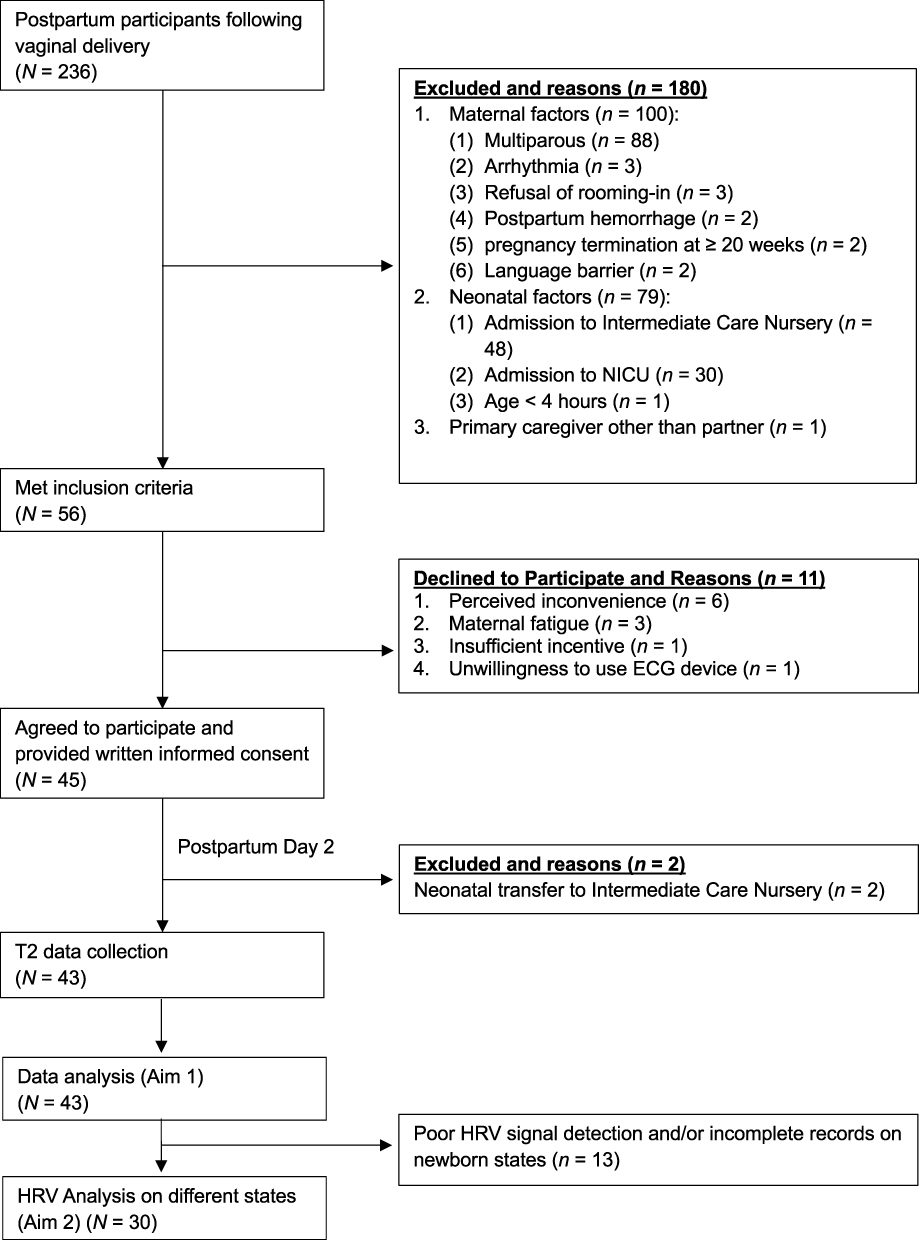 |
Figure 1 Flow diagram of individual recruitment and enrollment. Abbreviations: N, total number of screened individuals; n, number of participants in a specific subgroup; PPH, postpartum hemorrhage; SCN, special care nursery; NICU, neonatal intensive care unit; ECG, electrocardiogram; HRV, heart rate variability. |
Measures
Maternal Postpartum Stress (HRV)
We measured maternal stress levels through HRV using a portable ECG device.34 ECG offers much better reliability and validity than photoplethysmography in detecting R–R intervals and reflecting autonomic nervous system activity.30,35
To ensure accurate temporal synchronization between the continuous maternal HRV recordings and specific newborn behavioral states, both data sources were aligned using standardized network time. The internal clock of the ECG device was automatically synchronized with internet time via Bluetooth pairing with the research smartphone. Simultaneously, participants recorded the onset and offset of newborn states using the timestamps from their mobile devices, which were also synchronized with network time. This standardized reference facilitated the precise alignment of physiological data with observed newborn states.
To measure a baseline HRV, at T1, participants were first asked to wear a portable ECG device for 5 minutes while listening to light music in a supine position with their eyes closed.36 Once the baseline had been ascertained, the participants continued to wear the device until the end of the study. Participants were also asked to record the time of newborn states (i.e., crying, breastfeeding, being held by the father or mother, sleeping in a bassinet) during participation (from Day 1 to Day 3). At T2, the participants underwent a further 5-minute HRV test using the same posture and context. Finally, they completed an online questionnaire on basic information.
We adopted the time points in the R-R interval37 and transformed the R-R interval to the frequency domain using the Fourier transform for the spectral analysis.38 The Fourier transform formula and spectral distribution are shown in Figure S1 and S2, respectively.
In frequency domain analysis, significant stress is characterized by a decrease in HF and an increase in LF components, supporting the use of HRV as an objective assessment tool for stress and psychological well-being.39 In this study, we computed the nLF through the formula LF/(LF+HF).37,40,41 Since nLF is associated with psychological stress and an increase in sympathetic nervous system activity under high-stress conditions,42 it represents a viable indicator where a higher nLF indicates higher stress levels.
To ensure data quality, a mother’s nLF data were excluded when there was poor detection of signals from the ECG device or, at the time, any missing record of the newborn’s states.
Newborn States
We measured the newborns’ states (i.e., crying, breastfeeding, being held by the father or mother, sleeping) using the timesheet completed by the parents. The sheet was developed based on the researcher’s clinical observation of the interactive patterns of newborns and their parents during rooming-in. The newborn state recording sheet underwent a formal review by an expert committee to establish content validity. To ensure feasibility and clarity, a pilot test was conducted with three postpartum mother-infant dyads before the main study, confirming that the tool was highly usable and that the operational definitions were well-understood by parents. Parents were asked to record the start and end times of each state on the sheet, with a minute as the measurement unit. Time according to the cellphone time. Thus, the HRV window could be synchronized with newborn states. Furthermore, they were requested to note any phenomena meaningful to them. Their notes written on the timesheets were used as contextual references to interpret the quantitative HRV findings.
The operational definitions of the newborn states are: (1) Breastfeeding: breastfeeding until when the newborn rests for more than 30 seconds after sucking, remains quiet, and has relaxed elbows. (2) Being held by parents: The newborn is held on either the partner’s or the mother’s chest. (3) Crying: Crying that persists for more than 10 seconds without a spontaneous stop. (4) Sleeping in a bassinet: The newborn has closed eyes and is not easily awakened.
Levels of Rooming-in
According to the distribution of our rooming-in time data, the 24-hour rooming-in duration was classified into four groups: (1) less than 8 hours, (2) 8 hours or more but less than 16 hours, (3) 16 hours or more but less than 24 hours, and (4) exactly 24 hours.
Fatigue
We used the Fatigue Continuum Form (FCF) to measure fatigue on Day1 as the control variable. The FCF was modified by Pugh43 from the Modified Fatigue Symptom Checklist (MFSC), which utilizes a Likert scale to indicate varying levels of fatigue: 1 = Not at all, 2 = Mild, 3 = Moderate, and 4 = Severe. Possible total scores range from 30 to 120. Higher scores refer to greater fatigue intensity. According to Pugh et al,44 a total score of ≤ 38.5 is classified as low fatigue, 38.6 to 64.4 as moderate fatigue, and ≥ 64.5 as high fatigue. Kuo et al45 noted that the FCF is an appropriate tool for this study due to its concise response format, which minimizes the burden on participants. Regarding the reliability of this instrument, the Cronbach’s α values range from 0.77 to 0.92, indicating high internal consistency.46
Pain
Pain is measured using a proxy indicator based on previously experienced breastfeeding issues (specifically nipple pain). The measurement scale assesses the perceived level of difficulty: 1 = No problem, 2 = Mild difficulty, 3 = Moderate difficulty, and 4 = Severe difficulty. Breastfeeding difficulties also included perceived insufficiency of human milk for the newborn, breast engorgement, flat or inverted nipples, newborn latching difficulties, and mastitis.
Demographic and Obstetrics Data
Demographics (i.e., age, education, marital status, intended pregnancy, employment status, and family income) were collected by online self-administered questionnaires. Obstetric data included whether assisted birth and feeding methods were used during hospitalization.
Data Collection
Data collection followed a strict chronological sequence from T1 to T2, with all devices synchronized to network time to ensure precise alignment.
Phase 1: Baseline Assessment (Postpartum Day 1, T1)
Within 4 to 24 hours post-vaginal birth, eligible primiparous women provided written informed consent for study enrollment. Following the setup and Bluetooth pairing of the portable ECG device by the research team, participants underwent a 5-minute baseline HRV assessment while remaining in a supine position with their eyes closed, listening to a standardized track (Air on the G String by J.S. Bach).
Phase 2: Continuous HRV Monitoring and Newborn States Tracking (Day 1 to 3)
Following the baseline test, participants wore the ECG device continuously during their hospital stay. Both parents were trained to reapply the device after showering using an illustrated pamphlet, and the research team monitored connectivity online. Concurrently, parents used a standardized paper timesheet to log the exact start and end times (to the nearest minute) of four newborn states: breastfeeding, being held, crying, or sleeping in a bassinet.
Phase 3: Follow-Up and Study Completion (Postpartum Day 3, T2)
At T2, participants completed a second 5-minute resting HRV test under identical contextual parameters. Finally, participants filled out online questionnaires regarding demographics, obstetric history, FCF, and localized breastfeeding pain.
Signal Processing and Data Alignment
Continuous ECG data were processed into maternal nLF parameters using a 5-minute sliding window with 1-minute increments and then chronologically matched with the newborn state logs. Detailed technical specifications of the ECG hardware and formulas are provided in the Supplementary Material.
Data Analysis
We used the SPSS software version 22.0 for data analysis. Initially, descriptive statistics were employed to summarize the variables. Paired sample t-tests were conducted to examine the change in nLF stress level between T1 and T2.
Maternal HRV parameters were calculated using a 5-minute sliding window with 1-minute increments, ensuring a continuous stream of physiological data. These HRV values were then matched to the corresponding time periods in the newborn state record. Given that the parents’ recording unit was one minute, the minimum duration threshold for a newborn state episode to be included in the matching analysis was set at one minute.
Maternal nLF data were matched to the newborn state diaries (breastfeeding, crying, being held, and sleeping) using a 5-minute sliding window. Considering HRV metrics are strongly influenced by inter-individual differences and measurement context.40 Normative HRV values vary by age, sex, recording duration, and physiological state, and different HRV standards are not interchangeable.40,47 To mitigate this confounding effect, we applied a within-subject ranking approach, which allows participants to self-compare against their own baseline and may provide a more robust approach than direct between-subject comparison. Thus, we computed and ranked the average nLF across these four behavioral states from 1 (lowest) to 4 (highest) for each participant.
To examine the association between maternal physiological stress and newborn states, Chi-square tests were performed based on the frequency distribution of participants who exhibited their lowest or highest stress levels in each corresponding state. Originally, we hypothesized that maternal stress levels would be the lowest when newborns were in the sleeping state compared to the other behavioral states.
During the analysis of HRV data, participants with poor ECG signal quality or incomplete newborn state diaries were excluded, yielding a final analytical sample of 30 participants for the newborn states comparison. Furthermore, when evaluating the specific impact of rooming-in, four additional participants were excluded: two who engaged in full rooming-in (leaving no non-rooming-in baseline data) and two who lacked HRV data during the non-rooming-in period. Consequently, a subgroup of 26 participants was analyzed for rooming-in comparisons to ensure data consistency and methodological rigor.
To evaluate the potential confounding effects of maternal physical distress, we conducted a post-hoc analysis comparing fatigue and pain across four types of newborn states for the lowest (ranked 1st) and highest (ranked 4th) maternal nLF categories. We analyzed the maternal fatigue levels across the four types of newborns when mothers’ nLF was lowest (or highest) using Kruskal–Wallis tests. For maternal pain, we assessed the distribution of nipple pain difficulties in the four types of newborns when mothers’ nLF was lowest (or highest) by Chi-square tests. These analyses aimed to verify whether the observed maternal stress variations were independent of the mother’s baseline fatigue and localized pain levels.
Results
A total of 43 participants completed the overall longitudinal follow-up. For the synchronized newborn states analysis, after excluding 13 participants due to poor ECG signal quality or missing timesheet entries, data from 30 participants were successfully analyzed using relative ranking.
Demographic Data
Among the 43 participants, the average (SD) maternal age at childbirth was 33.3 (4.03) years. Almost all the participants had an education above college level (98%), and more than half of the participants reported a monthly family income exceeding United States Dollars (USD) 3,000 (54%). Additionally, 58% of participants practiced rooming-in for more than 16 hours per day but less than 24 hours. Just under half of the participants exclusively breastfed (46%). Some of the participants (47%) experienced moderate or severe difficulty with perceived insufficiency of human milk production, as shown in Table 1.
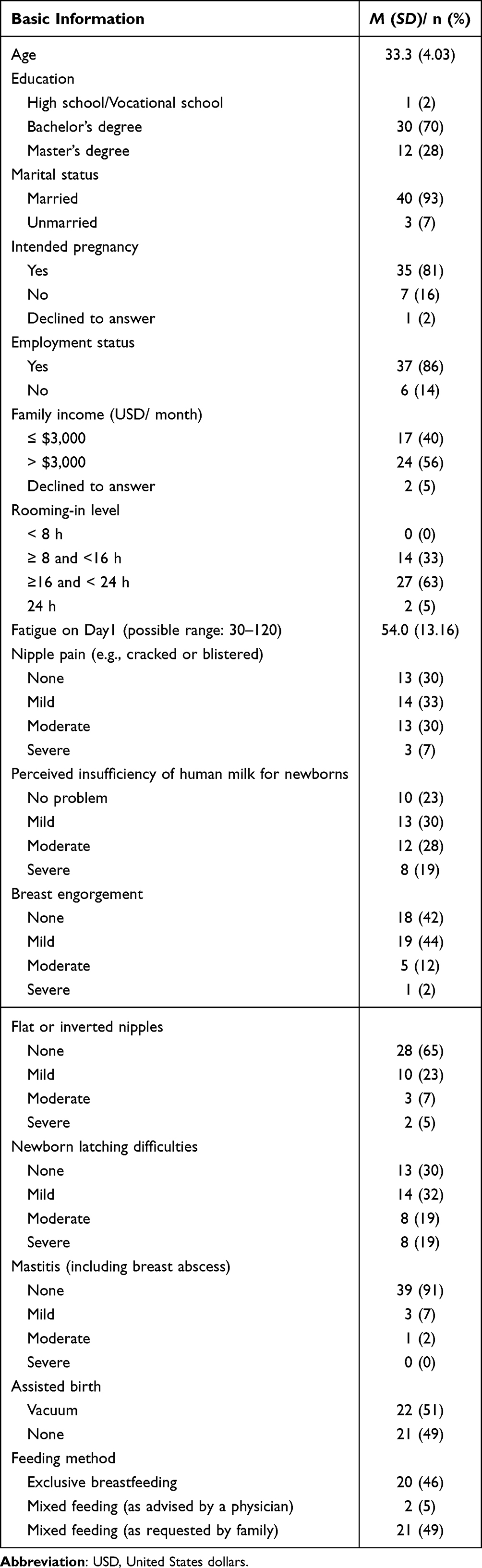 |
Table 1 Distribution of Basic Information of Participants (N = 43) |
Change in Overall Maternal Stress
The overall physiological stress (nLF) showed an increasing trend. Specifically, the mean (SD) nLF at T1 was 52.2 (20.70), while the mean (SD) nLF rose to 61.3 (19.19) at T2, indicating a significant increase in overall stress (t = 2.38, p = 0.022).
To control for the potential confounding effects of physical symptoms over time, a linear mixed model (LMM) with a first-order autoregressive [AR(1)] covariance structure was adopted. Maternal pain and fatigue scores were entered as time-varying covariates. After adjusting for these concurrent confounders, the fixed effect of time (T1 vs. T2) on overall physiological stress (nLF) remained statistically significant (F(1, 40.52) = 5.17, p = 0.028). This solidifies that the increasing trend in maternal physiological stress occurred independently of changes in physical pain and fatigue levels.
Association Between Maternal Stress and Rooming-in Level
Pearson’s correlation coefficients (r) between maternal stress (nLF) and rooming-in level were 0.05 (p = 0.778) and 0.06 (p = 0.697) at T1 and T2, respectively, indicating no significant association between maternal stress and rooming-in levels.
To control for the potential confounding factors (i.e., fatigue and pain), partial correlation analysis was performed. After adjusting for maternal fatigue and pain scores, the partial correlation coefficients remained non-significant at both T1 (r = 0.10, p = 0.553) and T2 (r = 0.07, p = 0.697), confirming that the lack of associations was independent of these physiological confounders.
Association Between Maternal Stress and Newborn States
Contrary to our hypothesis, when the newborns were asleep during rooming-in, participants experienced the highest nLF stress (65.4% [SD 8.91]). However, when breastfeeding, the nLF percentage was the lowest (60.2% [SD 9.76]; Table 2). Further, the average stress level was only 56.7% (SD 11.06) when they were not rooming in.
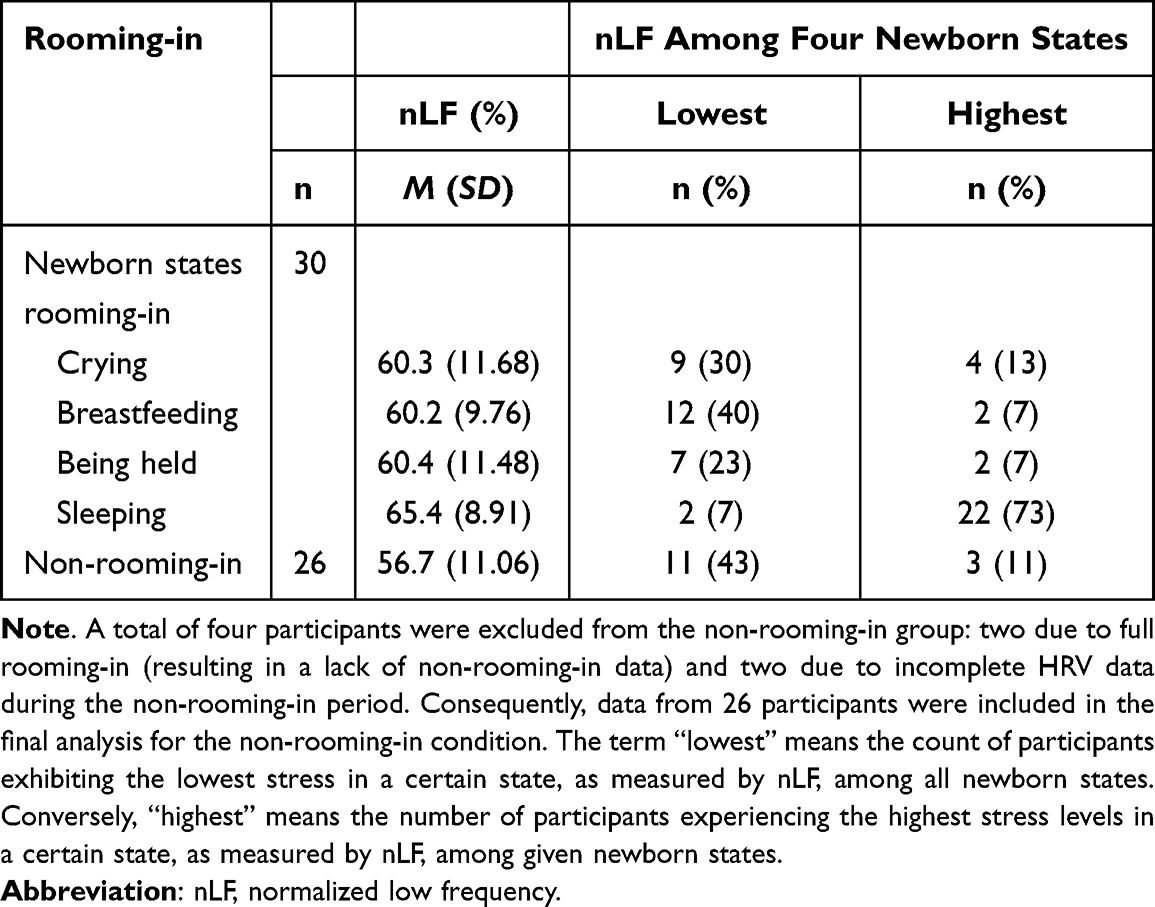 |
Table 2 Comparison of Maternal Stress Variations with Newborn States (N = 30) |
To control for potential confounding factors (i.e., fatigue and pain), the post-hoc analysis compared fatigue and pain across four newborn states for the lowest (ranked 1st) and highest (ranked 4th) maternal nLF categories. Kruskal–Wallis tests showed no significant difference in the maternal fatigue levels across the four types of newborns when mothers’ nLF was lowest (or highest). For maternal pain, Chi-square tests showed non-significant differences in the distribution of nipple pain difficulties across the four types of newborns when mothers’ nLF was lowest (either for highest). These analyses aimed to verify whether the observed maternal stress variations were independent of the mother’s baseline fatigue and localized pain levels.
Missing Data and Sensitivity Analysis
To evaluate the potential for attrition and selection bias, we compared the baseline characteristics of the excluded participants (n = 13, due to poor HRV signal quality or incomplete logs) with those of the included participants (n = 30). As shown in Table S1, the two groups did not differ significantly in most demographic or clinical characteristics (all ps > 0.05), with the exception of the rooming-in levels (p = 0.025). Participants with lower rooming-in levels had a higher rate of HRV data exclusion, suggesting that the missingness mechanism may be missing at random (MAR) rather than missing completely at random (MCAR). This pattern may be attributed to increased maternal physical mobility or varying levels of maternal-infant interaction, which can mechanically affect the signal stability of ambulatory HRV recordings.
To address potential selection bias, we performed a sensitivity analysis using multiple imputation (MI) by IBM SPSS Statistics (version 26.0). The missing HRV values were imputed based on the non-missing demographic and clinical data for 20 iterations, including rooming-in characteristics. The primary statistical analyses were then re-run using the pooled imputed dataset (N =43).
As presented in Table S2, the results of the sensitivity analysis were highly consistent with our original analysis based on complete cases, demonstrating that the systematic missingness related to rooming-in did not significantly bias the primary findings or change the statistical conclusions of this study.
Discussion
This study is the first to utilize portable ECG devices worn by postpartum women to examine maternal physiological stress in relation to various newborn states during hospitalization. Our investigation revealed two key findings: (1) the highest stress levels occurred when newborns were asleep, and (2) maternal stress showed no significant association with rooming-in level. These findings enhance neonatal and maternity nurses’ understanding of situational stress during rooming-in, thereby facilitating targeted interventions and guidance. Our findings highlight that while rooming-in is beneficial for bonding, it can also pose challenges for postpartum women. This phenomenon underscores the importance of prenatal preparation.48 Once the postpartum family has parenting skills, the stress during rooming-in may decrease.
Maternal Physiological Stress and the Paradox of Infant Sleep
A key finding of this study is that the greatest physiological stress for the majority of participants (73%) occurred concurrently with the newborn’s sleep state. Although it was hypothesized that infant sleep would provide a window for maternal recovery, our objective physiological data revealed a contrary pattern. This unexpected finding demonstrates that infant sleep does not automatically equate to maternal rest; instead, this period is characterized by heightened physiological alertness. Our systematic quantitative findings support the highly contextual nature of maternal stress, as evidenced by a distinct pattern where the highest nLF power, reflecting sympathetic dominance or a situational sympathovagal shift, was observed during the newborn’s sleep state. This evidence reframes the understanding of the postpartum rooming-in experience, indicating that the infant’s sleep window does not inherently translate into a restorative period for the mother.
To explore potential contextual mechanisms underlying this high-nLF phenomenon, we examined supplementary activity logs on the newborn record (timesheets). These clinical notes suggested a notable behavioral pattern: when the newborn fell asleep, mothers frequently documented a compelling need to immediately complete delayed daily self-care activities (e.g., eating, showering, and toileting). Because direct infant care remained the primary focus during the newborn’s waking hours, mothers appeared to utilize these limited sleep windows to rapidly attend to their basic physiological needs. While not analyzed through a formal qualitative research design, these descriptive records provide a plausible contextual explanation; the elevated nLF levels during infant sleep may reflect a state of physiological time urgency, driven by the pressure to complete essential personal tasks within an unpredictable timeframe.
This contextual hypothesis is further illustrated by a distinct contrast observed in a limited subset of our sample (n=2), where participants manifested their lowest nLF levels when the newborn was asleep. Interestingly, their activity logs indicated that these low-stress intervals occurred exclusively when the spouse actively assumed infant care, thereby allowing the mothers to engage in undisturbed rest. While these individual observations are descriptive and lack statistical power for generalizing causal inference, this divergence aligned with developmental literature indicating that increased paternal caregiving is associated with more consolidated maternal sleep,49,50 suggesting that spousal involvement may play a vital role in facilitating maternal physiological and behavioral recovery. The contextual hypothesis underscores a critical area for future investigation: the potential buffer effect of partner support in relieving maternal sympathovagal shifts during postpartum rooming-in.
The Dual Impact of Breastfeeding on Maternal Stress
Our findings confirmed that 40% of participants exhibited the lowest stress levels during breastfeeding, with an average nLF (SD) of only 60.2 (9.76). This physiological relaxation is consistent with the established neuroendocrine pathway of breastfeeding, where the release of oxytocin and prolactin downregulates maternal stress responses.51 Additionally, a systematic review indicates a correlation between breastfeeding and the mother-infant relationship, with mothers frequently demonstrating positive indicators such as better mother-infant interaction and secure attachment during the breastfeeding process.52 Previous studies emphasized that practicing full rooming-in can improve postpartum bonding,53 reinforcing the psychological benefits of breastfeeding that support rooming-in practices.
Conversely, a small subgroup (n = 2) reported their highest stress level during breastfeeding. Timesheet notes revealed that these mothers experienced acute physical distress, including severe stinging or cracked nipples, alongside anxiety over infant crying due to perceived milk insufficiency. Prior research has established that such postpartum distress and concerns regarding newborn care are critical risk factors associated with the early cessation or abandonment of exclusive breastfeeding.8,9 These findings highlight that while breastfeeding itself promotes physiological relaxation, health professionals should prioritize the early screening and management of lactation challenges, such as nipple pain and perceived milk insufficiency, to prevent exacerbating maternal stress.
Maternal Stress and Rooming-in Decisions: Cultural and Clinical Implications
Contrary to our hypothesis, this study found no significant association between maternal physiological stress and rooming-in levels, suggesting that stress may not be the primary factor driving the refusal of rooming-in care. Current literature suggests that the relationship between maternal stress and rooming-in level is complex. For example, van Veenendaal et al54 found that mothers using a family-integrated care model and couplet-care for the mother-newborn dyad reported lower stress levels and higher infant care involvement. More than 90 minutes of daily Kangaroo Mother Care (KMC) reduced maternal stress (cortisol levels) and postpartum depression.55 Therefore, family-centered integrated care, especially with increased skin-to-skin contact time, is expected to reduce maternal stress. However, the early postpartum transition presents competing demands for rest and infant bonding.
In Taiwan, postpartum units typically allows mothers flexibility in deciding when to room-in, as newborn nurseries are available. Because of traditional Asian “doing-the-month” practices, many Taiwanese women prioritize physical rest during the postpartum period and therefore prefer to delegate infant care to nursery staff. Understanding these cultural preferences may help international maternity nurses better understand the cultural considerations of Asian populations, particularly those with a Chinese cultural background, and adjust their care strategies to address postpartum stress related to rooming-in.
Balancing the need for rest with the benefits of rooming-in requires effective prenatal education and timely, family-centered postpartum support. Mothers’ prenatal willingness to participate in full rooming-in is associated with postnatal maternal–infant bonding,53 and maternal bonding is related to maternal stress.56 Strengthening prenatal education to enhance mothers’ readiness for full rooming-in should therefore be a clinical priority.
Limitation
Several limitations of this study should be acknowledged. First, regarding the baseline HRV measurement, we did not utilize music specifically tailored to individuals’ stress relief. Instead, all participants underwent a five-minute baseline recording in a standard environment with Air on the G String by J.S. Bach in the background. This approach was explicitly chosen to maintain contextual consistency across all participants in this study.
Second, the inclusion and exclusion criteria restricted the participants to primiparous women without clinical complications during pregnancy or childbirth. This approach was essential to ensure the integrity of HRV data by minimizing physiological noise, such as arrhythmias or pharmacological interference from complications. It may have resulted in a healthier-than-average postpartum sample. Consequently, the physiological stress variability observed in this study might be underestimated compared to a more clinically diverse postpartum population. Future research should consider including high-risk postpartum groups to explore a broader spectrum of maternal stress responses.
Third, acute hormonal fluctuations (e.g., changes in oxytocin and cortisol) were not directly measured. Although these biomarkers closely modulate postpartum stress, this study prioritized non-invasive, continuous physiological monitoring to minimize disruption to maternal recovery and the rooming-in experience. Future studies could incorporate salivary biomarkers to complement these autonomic findings.
Fourth, because the newborn state measure relied on parental self-recording over a 48-hour window, the inherent risk of recall or reporting bias must be acknowledged. To mitigate this risk, the research team synchronized network time across all devices and provided comprehensive, illustrated training to both parents at enrollment to ensure real-time and precise data logging.
Fifth, due to poor signal quality and incomplete logs, 13 participants were excluded from the final analysis. Methodological evaluation indicated that this missingness was associated with the level of rooming-in (Missing at Random), which may limit the generalizability of the HRV findings to populations with exceptionally low rooming-in performance. Nevertheless, our sensitivity analysis via multiple imputation demonstrated that this attrition did not significantly alter the primary statistical conclusions.
Finally, due to rigorous quality control for physiological monitoring, the analyzable sample size decreased from the initial n = 43 to n = 30 for newborn states and n = 26 for rooming-in comparisons. This attrition compromised the statistical power of higher-order inferential tests (e.g., repeated measures), increasing the risk of Type II errors. Consequently, these subgroup findings are exploratory rather than confirmatory and should be interpreted with caution. Nevertheless, they provide valuable clinical insights into HRV trends across caregiving contexts, serving as a foundation for future, larger-scale investigations.
Conclusion
This study demonstrates that maternal physiological stress is highly contextual during the early postpartum hospitalization, operating independently of rooming-in levels. Notably, nearly three-quarters of postpartum women experienced their highest physiological stress when the newborn was asleep. Conversely, breastfeeding emerged as the primary context associated with the lowest stress levels, although this benefit remains vulnerable to early lactation challenges. This study provides preliminary exploratory evidence that maternal autonomic activity varies across caregiving contexts, suggesting that maternity health professionals should heighten support during newborn sleep periods and early management of lactation challenges.
Disclosure of AI tool use
The authors acknowledge the use of Grammarly (v1.2.238.1846) for grammar, spelling, and punctuation checking, and ChatGPT free version for improving the clarity and readability of the manuscript. All AI-generated suggestions were reviewed, verified, and edited by the authors, who retain full responsibility for the final content.
Abbreviations
PPS, Postpartum stress; nLF, Normalized low frequency; HRV, Heart rate variability; ECG, Electrocardiogram; HF, High-frequency; LF, low-frequency; USD, United States Dollars.
Data Sharing Statement
The datasets used and analyzed during the current study are not publicly available due to participant privacy and institutional restrictions.
Ethics Approval and Informed Consent
This study adhered to the principles of respect for autonomy, nonmaleficence, beneficence, and justice. Participants were informed about the study’s potential benefits, risks, and data handling procedures and were allowed to make an autonomous decision regarding participation. All collected data were treated confidentially to protect participants’ privacy. Prior to data collection, the study protocol was reviewed and approved by the Research Ethics Committee of National Taiwan University Hospital (Approval No. 202012271RIPD) and authorized by the Department of Teaching and Research, with the Department of Nursing serving as the executing audit unit. Before the study began, the researchers explained the study’s purpose, objectives, and procedures, emphasizing that participation would not affect routine care and that participants could withdraw from the study at any time. Written informed consent was obtained from all participants, and the collected data were anonymized, coded, and strictly used for research purposes only.
Acknowledgments
The authors thank all participants in this study. We also thank the technological support from Chin-Chang Liao and Man-Chin Chen in Singular Wings Medical and the clinical support from the Head Nurses Ya-Hsiu Chang and Yi-Hua Lee at National Taiwan University Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Oyetunji A, Chandra P. Postpartum stress and infant outcome: a review of current literature. Psychiatry Res. 2020;284:112769. doi:10.1016/j.psychres.2020.112769
2. Gila-Díaz A, Carrillo GH, López de Pablo ÁL, Arribas SM, Ramiro-Cortijo D. Association between maternal postpartum depression, stress, optimism, and breastfeeding pattern in the first six months. Int J Environ Res Public Health. 2020;17(19):7153. doi:10.3390/ijerph17197153
3. Hutchens BF, Kearney J. Risk factors for postpartum depression: an umbrella review. J Midwifery Women’s Health. 2020;65(1):96–15. doi:10.1111/jmwh.13067
4. Davis J, Mire E. Maternal obesity and developmental programming of neuropsychiatric disorders: an inflammatory hypothesis. Brain Neurosci Adv. 2021;5.
5. Makris G, Eleftheriades A, Pervanidou P. Early life stress, hormones, and neurodevelopmental disorders. Hormone Res Paediatrics. 2023;96(1):17–24. doi:10.1159/000523942
6. Fernandez-Vaz C, Gonzalez-Sanz JD. Cortisol, maternal stress, and breastfeeding rate at hospital discharge: a systematic review. Breastfeeding Med. 2022;17(12):984–993. doi:10.1089/bfm.2022.0165
7. Ionio C, Ciuffo G, Landoni M. Parent–infant skin-to-skin contact and stress regulation: a systematic review of the literature. Int J Environ Res Public Health. 2021;18(9):4695. doi:10.3390/ijerph18094695
8. Ritchie-Ewing G, Mitchell AM, Christian LM. Associations of maternal beliefs and distress in pregnancy and postpartum with breastfeeding initiation and early cessation. J Human Lactation. 2019;35(1):49–58. doi:10.1177/0890334418767832
9. Santacruz-Salas E, Segura-Fragoso A, Cobo-Cuenca AI, Carmona-Torres JM, Pozuelo-Carrascosa DP, Laredo-Aguilera JA. Factors associated with the abandonment of exclusive breastfeeding before three months. Children. 2020;7(12):298. doi:10.3390/children7120298
10. Amar AV, Sejfović H. Perceived social support, newborn temperament and socioeconomic status in postpartum depression: report from southwest Serbia. Arch Psychiatry Psychotherapy. 2023;25(1):33–41. doi:10.12740/APP/152779
11. Shuman CJ, Peahl AF, Pareddy N, et al. Postpartum depression and associated risk factors during the COVID-19 pandemic. BMC Res Notes. 2022;15(1):102. doi:10.1186/s13104-022-05991-8
12. Tarrant M, Dodgson JE, Tsang Fei S. Initiating and sustaining breastfeeding in Hong Kong: contextual influences on new mothers’ experiences. Nurs Health Sci. 2002;4(4):181–191. doi:10.1046/j.1442-2018.2002.00125.x
13. Cheng CY, Pickler RH. Perinatal stress, fatigue, depressive symptoms, and immune modulation in late pregnancy and one month postpartum. Scientific World J. 2014;2014(1):652630. doi:10.1155/2014/652630
14. Giallo R, Gartland D, Woolhouse H, Brown S. “I didn’t know it was possible to feel that tired”: exploring the complex bidirectional associations between maternal depressive symptoms and fatigue in a prospective pregnancy cohort study. Arch Women’s Mental Health. 2016;19(1):25–34. doi:10.1007/s00737-014-0494-8
15. Wang Y, Mao K, Deng J, Gu J. Comparison of symptoms of depression, anxiety, and stress in postpartum women with and without pain: a network analysis. BMC Pregnancy Childbirth. 2025;25(1):732. doi:10.1186/s12884-025-07858-9
16. Ramos BA, Formiga CKMR, NRGd O, et al. Relationship between maternal stress and neurobehavioral indicators of preterm infants in the neonatal intensive care unit. Children. 2024;11(8):889. doi:10.3390/children11080889
17. Gao M, Speck B, Ostlund B, et al. Developmental foundations of physiological dynamics among mother–infant dyads: the role of newborn neurobehavior. Child Develop. 2022;93(4):1090–1105. doi:10.1111/cdev.13769
18. Boonnithi S, Phongsuphap S. Comparison of heart rate variability measures for mental stress detection. Paper presented at: 2011 Computing in Cardiology. 2011.
19. Immanuel S, Teferra MN, Baumert M, Bidargaddi N. Heart rate variability for evaluating psychological stress changes in healthy adults: a scoping review. Neuropsychobiology. 2023;82(4):187–202. doi:10.1159/000530376
20. Bradley H, Fine D, Minai Y, et al. Maternal perceived stress and infant behavior during the COVID-19 pandemic. Pediatric Res. 2023;94(6):2098–2104. doi:10.1038/s41390-023-02748-2
21. Miller AR, Barr RG, Eaton WO. Crying and motor behavior of six-week-old infants and postpartum maternal mood. Pediatrics. 1993;92(4):551–558. doi:10.1542/peds.92.4.551
22. Kurth E, Spichiger E, Zemp Stutz E, Biedermann J, Hösli I, Kennedy HP. Crying babies, tired mothers - challenges of the postnatal hospital stay: an interpretive phenomenological study. BMC Pregnancy Childbirth. 2010;10(1):21. doi:10.1186/1471-2393-10-21
23. Fernandez-Vaz C, Cortisol G-SJD. Maternal stress, and breastfeeding rate at hospital discharge: a systematic review. Breastfeed Med. 2022;17(12):984–993.
24. Cong S, Wang R, Fan X, et al. Skin-to-skin contact to improve premature mothers’ anxiety and stress state: a meta-analysis. Matern Child Nutr. 2021;17(4):e13245. doi:10.1111/mcn.13245
25. Bigelow AE, Power M. The effect of mother-infant skin-to-skin contact on infants’ response to the still face task from newborn to three months of age. Infant Behav Dev. 2012;35(2):240–251. doi:10.1016/j.infbeh.2011.12.008
26. Symon B, Bammann M, Crichton G, Lowings C, Tucsok J. Reducing postnatal depression, anxiety and stress using an infant sleep intervention. BMJ Open. 2012;2(5):e001662. doi:10.1136/bmjopen-2012-001662
27. Sharkey KM, Iko IN, Machan JT, Thompson-Westra J, Pearlstein TB. Infant sleep and feeding patterns are associated with maternal sleep, stress, and depressed mood in women with a history of major depressive disorder (MDD). Arch Womens Ment Health. 2016;19(2):209–218. doi:10.1007/s00737-015-0557-5
28. Walker LO, Murry N, Becker H, Li Y. Leading stressors and coping strategies associated with maternal physical and mental health during the extended postpartum period. J Midwifery Women’s Health. 2024;69:746–754. doi:10.1111/jmwh.13641
29. Giannakakis G, Grigoriadis D, Giannakaki K, Simantiraki O, Roniotis A, Tsiknakis M. Review on psychological stress detection using biosignals. IEEE Transact Affect Comp. 2019;13(1):440–460. doi:10.1109/TAFFC.2019.2927337
30. Polak AG, Klich B, Saganowski S, Prucnal MA, Kazienko P. Processing photoplethysmograms recorded by smartwatches to improve the quality of derived pulse rate variability. Sensors. 2022;22(18):7047. doi:10.3390/s22187047
31. Faul F, Erdfelder E, Lang A-G, Buchner A. G* power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Meth. 2007;39(2):175–191. doi:10.3758/BF03193146
32. Abu-Baker NN, Abusbaitan HA, Al-Ashram SA, Alshraifeen A. The effect of health education on dietary knowledge and practices of pregnant women in Jordan: a quasi-experimental study. Int J Women’s Health. 2021:433–443.
33. Soos MP, McComb D. Sinus arrhythmia. In: StatPearls [Internet]. StatPearls Publishing; 2022.
34. Wings S. BEATINFO sensor. date unknown. Available from: https://singularwings.com/zh/beatinfo-ecg-%e5%82%b3%e6%84%9f%e5%99%a8/.
35. Pankaj KA, Komaragiri R, Kumar M, Kumar M. A review on computation methods used in photoplethysmography signal analysis for heart rate estimation. Arch Computat Metho Engine. 2022;29(2):921–940. doi:10.1007/s11831-021-09597-4
36. Schlembach D, Moertl MG. Heart rate variability and blood pressure variability in obstetrics and gynecology. In: Heart Rate Variability (HRV) Signal Analysis: Clinical Applications. Boca Raton: CRC Press, Taylor & Francis Group; 2012:137–164.
37. Kuo TB, Chen C-Y, Wang YP, et al. The role of autonomic and baroreceptor reflex control in blood pressure dipping and nondipping in rats. J Hypertension. 2014;32(4):806–816. doi:10.1097/HJH.0000000000000099
38. Brigham EO, Morrow R. The fast Fourier transform. IEEE Spectrum. 1967;4(12):63–70. doi:10.1109/MSPEC.1967.5217220
39. Kim H-G, Cheon E-J, Bai D-S, Lee YH, Koo B-H. Stress and heart rate variability: a meta-analysis and review of the literature. Psychiatry Investigat. 2018;15(3):235. doi:10.30773/pi.2017.08.17
40. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. 2017;5:258. doi:10.3389/fpubh.2017.00258
41. Razjouyan J, Grewal GS, Talal TK, Armstrong DG, Mills JL, Najafi B. Does physiological stress slow down wound healing in patients with diabetes? J Diabetes Sci Technol. 2017;11(4):685–692. doi:10.1177/1932296817705397
42. Sloan R, Shapiro P, Bagiella E, et al. Effect of mental stress throughout the day on cardiac autonomic control. Biolog Psychol. 1994;37(2):89–99. doi:10.1016/0301-0511(94)90024-8
43. Pugh LC, Milligan R. A framework for the study of childbearing fatigue. Adv Nurs Sci. 1993;15(4):60–70. doi:10.1097/00012272-199306000-00007
44. Pugh LC, Milligan R, Parks PL, Lenz ER, Kitzman H. Clinical approaches in the assessment of childbearing fatigue. J Obstet Gynecologic Neonatal Nurs. 1999;28(1):74–80. doi:10.1111/j.1552-6909.1999.tb01967.x
45. Kuo SY, Yang YL, Kuo PC, Tseng CM, Tzeng YL. Trajectories of depressive symptoms and fatigue among postpartum women. J Obstet Gynecol Neonatal Nurs. 2012;41(2):216–226. doi:10.1111/j.1552-6909.2011.01331.x
46. Pugh LC. Psychophysiological Correlates of Fatigue During Childbirth. Baltimore: University of Maryland; 1990.
47. Williams PG, Cribbet MR, Tinajero R, Rau HK, Thayer JF, Suchy Y. The association between individual differences in executive functioning and resting high-frequency heart rate variability. Biological Psychology. 2019;148:107772. doi:10.1016/j.biopsycho.2019.107772
48. Guo K, Shang X, Deng X. The effects of a newborn care education program on mothers’ self-confidence, care knowledge, and breastfeeding behavior: a systematic review and meta-analysis. Public Health Nursing. 2025;42(1):395–410. doi:10.1111/phn.13484
49. Tikotzky L, Sadeh A, Volkovich E, Manber R, Meiri G, Shahar G. Infant sleep development from 3 to 6 months postpartum: links with maternal sleep and paternal involvement. Monographs Soc Res Child Develop. 2015;80(1):107–124. doi:10.1111/mono.12147
50. Tikotzky L, Volkovich E, Meiri G. Maternal emotional distress and infant sleep: a longitudinal study from pregnancy through 18 months. Dev Psychol. 2021;57(7):1111–1123. doi:10.1037/dev0001081
51. UvnäsMoberg K, Ekström-Bergström A, Buckley S, et al. Maternal plasma levels of oxytocin during breastfeeding—A systematic review. Public Library Sci One. 2020;15(8):e0235806. doi:10.1371/journal.pone.0235806
52. Peñacoba C, Catala P. Associations between breastfeeding and mother-infant relationships: a systematic review. Breastfeed Med. 2019;14(9):616–629. doi:10.1089/bfm.2019.0106
53. Handelzalts JE, Levy S, Molmen-Lichter M, et al. Associations of rooming-in with maternal postpartum bonding: the impact of mothers’ pre-delivery intentions. Midwifery. 2021;95:102942. doi:10.1016/j.midw.2021.102942
54. van Veenendaal NR, van Kempen AA, Broekman BF, et al. Association of a zero-separation neonatal care model with stress in mothers of preterm infants. JAMA Network Open. 2022;5(3):e224514–e. doi:10.1001/jamanetworkopen.2022.4514
55. Cristóbal Cañadas D, Parrón Carreño T, Sánchez Borja C, Bonillo Perales A. Benefits of kangaroo mother care on the physiological stress parameters of preterm infants and mothers in neonatal intensive care. Intl J Environ Res Public Health. 2022;19(12):7183. doi:10.3390/ijerph19127183
56. Pazzagli C, Buratta L, Coletti E, Mazzeschi C. Mother-to-infant bonding mediates the effects of depressive and anxious postpartum symptoms on parenting stress. J Psychosomatic Obstet Gynecol. 2023;44(1):2264487. doi:10.1080/0167482X.2023.2264487
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.