Back to Journals » Open Access Emergency Medicine » Volume 14
Differential Association Between Significant Coronary Stenosis and Cardiac Troponin T Serial Algorithms in Chronic Kidney Disease Patients Diagnosed with Non-ST-Segment Elevation Acute Coronary Syndromes
Authors Tangpaisarn T, Srimakam N, Senthong V, Phungoen P, Kotruchin P ![]()
Received 15 November 2021
Accepted for publication 17 January 2022
Published 2 February 2022 Volume 2022:14 Pages 41—49
DOI https://doi.org/10.2147/OAEM.S348378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Thanat Tangpaisarn,1 Nirut Srimakam,1 Vichai Senthong,2 Pariwat Phungoen,1 Praew Kotruchin1
1Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Internal Medicine, Faculty of Medicine Srinagarind Hospital, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Praew Kotruchin
Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
, Tel +66 65 5269 422
, Email [email protected]
Background: High-sensitivity cardiac troponin T (hs-cTnT) is recommended for diagnosing non-ST segment elevation acute coronary syndromes (NSTE-ACS). While the guidelines recommend using the 0,1-hour (hr) and 0,3-hr hs-cTnT algorithms, their efficacy has not been clearly established in chronic kidney disease (CKD) patients. We aimed to assess the differential associations between the two algorithms mentioned above with significant coronary stenosis in CKD patients.
Methods: This was a retrospective cohort study. Patients aged ≥ 18 years who were diagnosed with NSTE-ACS and had undergone coronary angiogram were recruited. The differential association between significant coronary stenosis and being ruled in based on the 0,1-hr and 0,3-hr hs-cTnT algorithm was analyzed and reported.
Results: There were 158 and 160 patients in the CKD and normal renal function groups. Among CKD patients, determinants of significant coronary stenosis were hypertension (OR = 2.68; 95% CI 1.10– 6.50) and being ruled in by the 0,3-hr algorithm (OR = 3.65; 95% CI 1.27– 10.52). In the normal renal function group, age (OR = 1.04; 95% CI 1.01– 1.06), male sex (OR = 2.15; 95% CI 1.09– 4.22), and being ruled in by the 0,1-hr algorithm (OR = 3.12; 95% CI 1.20– 8.10) were associated with significant coronary stenosis.
Conclusion: Being ruled in according to the 0,3-hr algorithm was significantly associated with coronary stenosis in CKD patients, making this a likely algorithm of choice in these patients.
Keywords: renal dysfunction, cardiac biomarkers, troponin, acute coronary syndromes, Asian
Introduction
Coronary artery disease (CAD) is a leading cause of death worldwide.1 There are several known atherosclerotic risk factors for CAD, both reversible and irreversible.2 One significant risk factor is renal dysfunction.3,4 Patients who have an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2 or chronic kidney disease (CKD)5 are at risk of cardiovascular disease, partly due to preexisting cardiovascular risk factors (eg, hypertension and dyslipidemia).3,6–8 Other novel cardiovascular risk factors in CKD patients are chronic inflammation, calcium–phosphate metabolism disturbances, oxidative stress, malnutrition, anemia, fluid overload, fluctuation in systemic fluid volume, disturbances in the coagulation system, accumulation of metabolic products, and numerous undefined toxic agents associated with atherosclerosis.9–11 Unfortunately, the diagnosis of CAD in CKD patients often requires thorough history taking and physical examination as well as a high level of suspicion due to their atypical presentations.12
Generally, an electrocardiogram (ECG) is performed in patients who present at the emergency department (ED) with symptoms compatible with acute coronary syndromes (ACS). If the ECG does not show ST-segment elevation myocardial infarction (STEMI), high-sensitivity cardiac troponin (hs-cTn) is recommended as a cardiac biomarker for evaluating whether patients have non-ST segment elevation acute coronary syndromes (NSTE-ACS).13
CKD is one of the determinants of cardiac troponin (cTn) level.14 There is evidence of chronic cTn elevation in CKD patients, even in the absence of significant coronary artery stenosis.15 There have also been studies aimed at determining the cTn cut-off level for diagnosing myocardial infarction in CKD patients.16–18 However, serial testing has yielded the best results in the screening for and diagnosing of NSTE-ACS in both CKD patients and those with normal renal function.19–23
Previous treatment guidelines recommended using a 0,3-hour algorithm in the serial testing of cTn, and this method has since been adopted worldwide.24 However, due to the development of hs-cTn assays, the latest European Society of Cardiology (ESC) guidelines for the management of ACS in patients presenting without persistent ST-segment elevation recommend the use of a 0,1-hour algorithm regardless of renal function to rule in and rule out NSTE-ACS at the ED rapidly.13 Many studies, however, have shown the efficacy of the 0,1-hour algorithm to be lower than that of the 0,3-hour algorithm in CKD patients.19,23 Furthermore, in current real-world practice, it is not uncommon for ED physicians to use the 0,3-hour algorithm to test for NSTE-ACS regardless of the recommendations.22,23
We, therefore, aimed to assess the differential association between these two algorithms and significant coronary stenosis in CKD patients.
Materials and Methods
Study Design and Population
This was a retrospective cohort study conducted in the ED of Srinagarind hospital, a 1000-bed tertiary care university hospital in northeast Thailand, from December 2014 to December 2018.
Patients aged 18 years (yr) or over who presented with chest pain were initially diagnosed with NSTE-ACS and underwent coronary angiogram (CAG) during the same admission were recruited. Patients who presented with cardiac arrest or had incomplete data regarding serum creatinine levels, CAG, or hs-cTnT were excluded from the study.
This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The Khon Kaen University Ethics Committee for Human Research approved the study and waived the written individual informed consent as the research is no more than minimal risk. To protect confidentiality, all identifiers were eliminated from the obtained data (HE621312).
Operating Definitions
NSTE-ACS
NSTE-ACS, including unstable angina and non-ST-elevation myocardial infarction (NSTEMI), was diagnosed by an intervention cardiologist on duty according to the 4th universal definition of myocardial infarction criteria (details are provided in the Online Supplementary Materials).25
CKD
CKD was defined as an eGFR of less than 60 mL/min/1.73 m2 computed according to the KDICO formula (details are provided in the Online Supplementary Materials).26
0,1-hr Algorithm
NSTE-ACS was ruled in according to the 0,1-hr algorithm if hs-cTnT was ≥52 ng/l at presentation or if the difference between hs-cTnT at presentation and after 1 hour was ≥5 ng/l (Figure 1) in accordance with the latest ESC guidelines.13
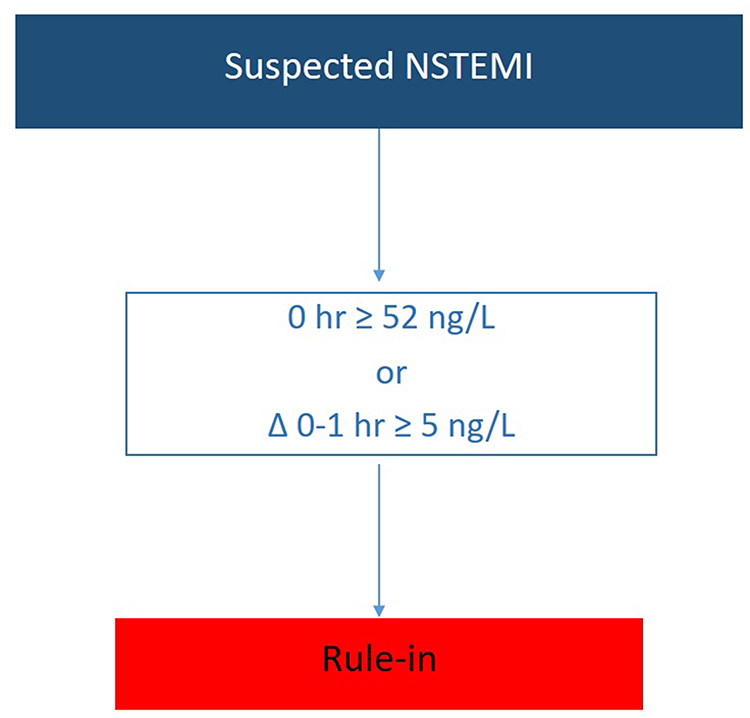 |
Figure 1 0,1-hr rule-in algorithms using hs-cTnT assays (Elecsys®) in patients presenting with suspected non-ST-elevation acute coronary syndromes. |
0,3-hr Algorithm
NSTE-ACS was ruled in according to the 0,3-hr algorithm if hs-cTnT was ≥70 ng/l at presentation, if there was a >20% difference in hs-cTnT at presentation and after 3 hours, if hs-cTnT at presentation was ≥14 ng/l, or if there was a >7 ng/l change in hs-cTnT after 3 hours, if hs-cTnT at presentation was <14 ng/l (Figure 2), according to the 2015 ESC guidelines.24
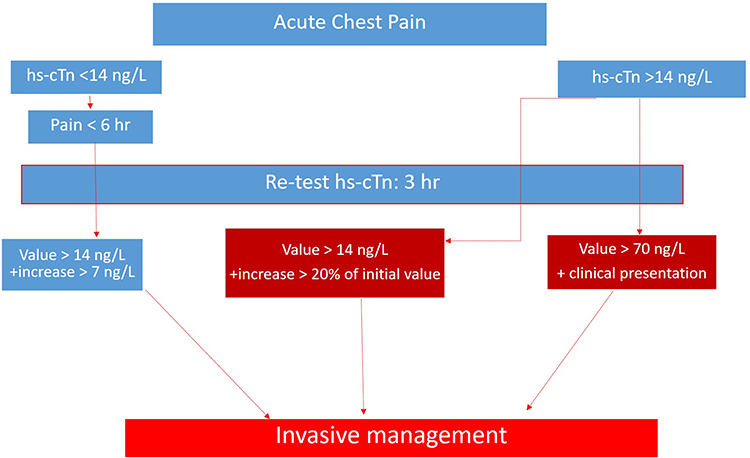 |
Figure 2 0,3-hr rule-in algorithm of non-ST-elevation acute coronary syndromes using high-sensitivity cardiac troponin assays (Elecsys®). |
Positive CAG
Positive CAG was defined as >50% stenosis of the left main coronary artery or >70% stenosis of right coronary artery (RCA), left circumflex coronary artery (LCx), or left anterior descending (LAD) coronary artery.27
Primary Outcome and Statistical Analysis
The primary outcome was the association between significant coronary stenosis and NSTE-ACS being ruled in based on the two hs-cTnT algorithms (0,1-hr and 0,3-hr) in both CKD patients and those with normal renal function. The secondary outcomes were other determinants of significant coronary stenosis.
The patient’s baseline characteristics and clinical measurements were reported as mean ± standard deviation (SD) for continuous variables and number and percentage for categorical variables. For comparison between the CKD and the normal renal function groups, an independent sample t-test was used for continuous variables and Pearson’s chi-square test for proportions for categorical variables.
We used the cross tables derived from the official ESC assay-specific cut-off criteria for rule-in to determine the rule-in group.13,24 The association between significant coronary stenosis and rule-in status as a categorical variable (1 = ruled in, 0 = not ruled in) together with other conventional cardiovascular risk factors were subjected to binary logistic regression analysis and presented as unadjusted odd ratios (OR). Considering clinical importance and using P < 0.20 as a criterion, age, sex (male), and hypertension (HT) were included in the regression analysis, with the rule-in group from the 0,1-hr algorithm in model 1 and the 0,3-hr algorithm in model 2. The adjusted ORs were also reported.
All hypothesis testing was 2-tailed, and P < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS statistics for MAC, version 23.0 (SPSS Inc).
Results
Patient Characteristics
We enrolled 318 patients in this study, 158 in the CKD group and 160 in the normal renal function group. Baseline characteristics of patients with CKD differed from those with normal renal function in multiple respects, including older age (70 yr vs 62 yr, P < 0.001) and higher prevalence of HT and diabetes mellitus (DM; 83.0% vs 54.7% and 63.3% vs 26.7%, respectively; P < 0001). More patients in the CKD group were ruled in by both the 0,1-hr and the 0,3-hr algorithm (Table 1).
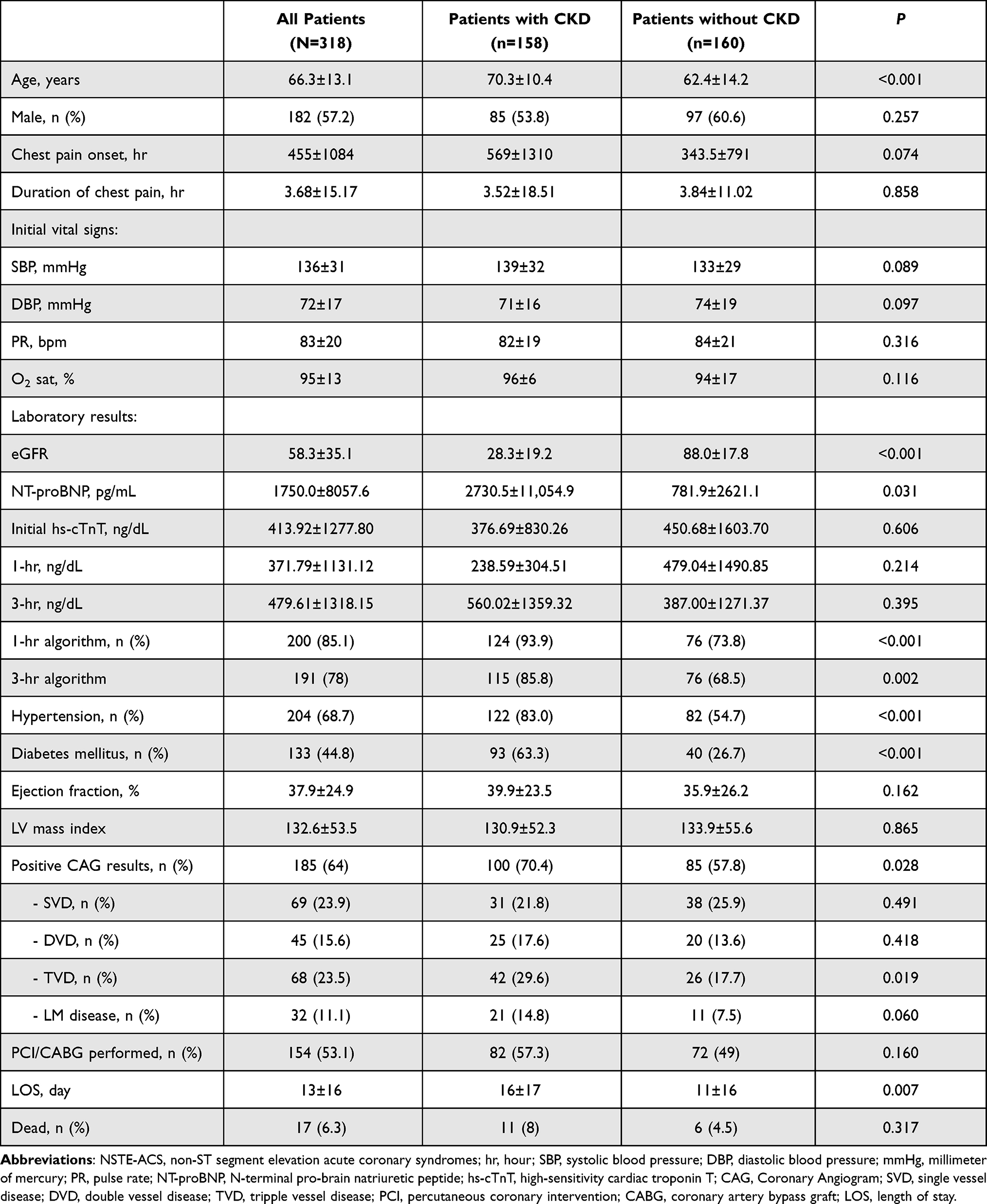 |
Table 1 Baseline Characteristics of the NSTE-ACS Patients, Categorized by Kidney Function |
There was a higher prevalence of significant coronary stenosis in the CKD group than in the normal renal function group (70.4% vs 57.8%, P = 0.028). Furthermore, length of stay (LOS) was longer in the former group than in the latter (16 days vs 11 days, P = 0.007; Table 1).
Determinants of a Significant Coronary Stenosis
Factors associated with significant coronary stenosis in the total study population were an older age (OR = 1.04; 95% CI 1.02–1.06), male sex (OR = 1.82; 95% CI 1.12–2.95), HT (OR = 1.93; 95% CI 1.16–3.22), and NSTE-ACS being ruled in by the 0,1-hr algorithm (OR = 3.53; 95% CI 1.61–7.73) or 0,3-hr algorithm (OR 2.24; 95% CI = 1.16–4.34; Table 2).
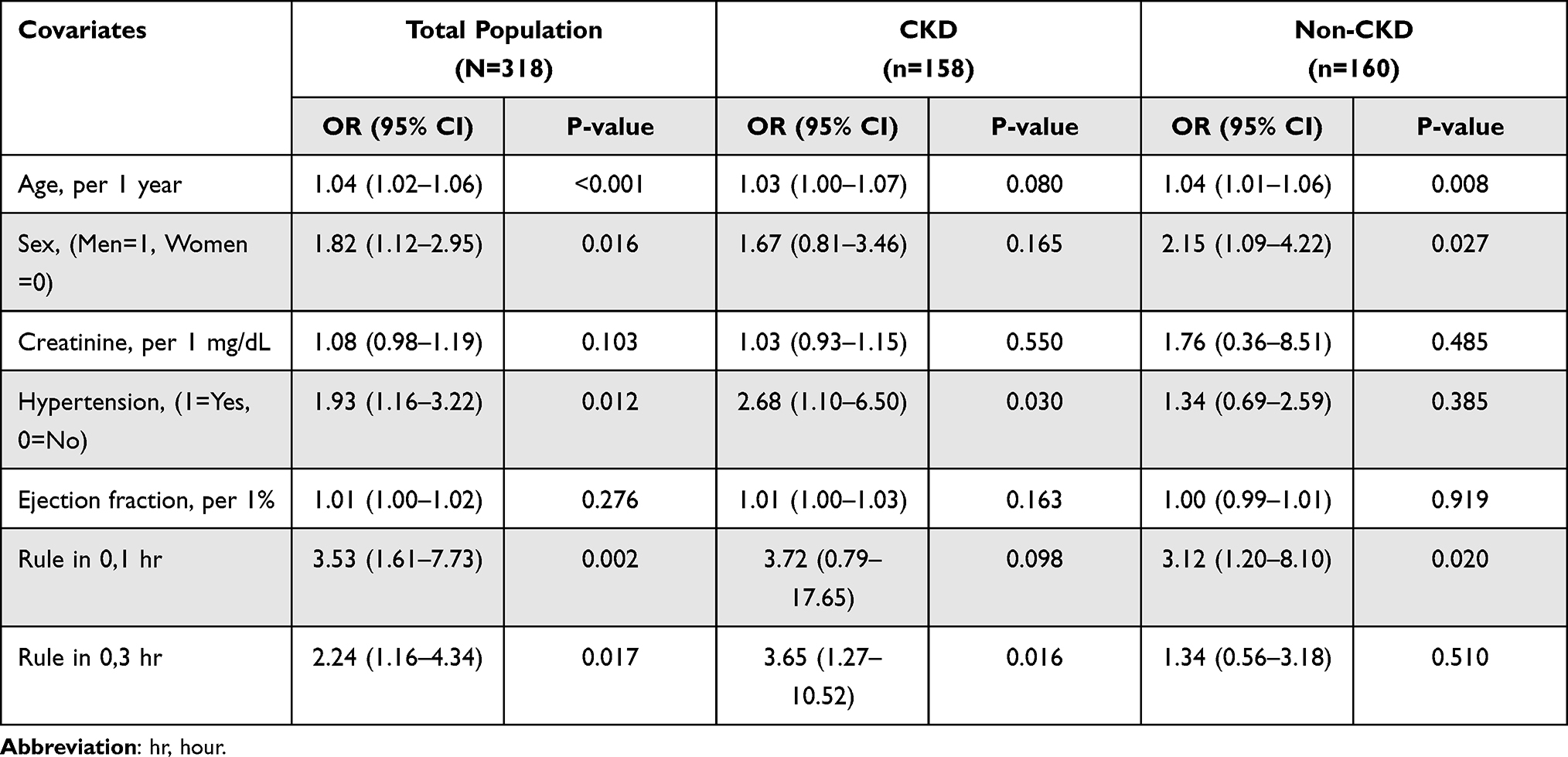 |
Table 2 Unadjusted Odd Ratio (OR) of a Significant Coronary Stenosis by Using Regression Analysis in the Total Population and After Categorized by Kidney Function |
Among CKD patients, factors associated with significant coronary stenosis were HT (OR = 2.68; 95% CI 1.10–6.50), and NSTE-ACS being ruled in based on the 0,3-hr algorithm (OR = 3.65; 95% CI 1.27–10.52; Table 2). In the normal renal function group, factors associated with significant coronary stenosis were older age (OR = 1.04; 95% CI 1.01–1.06), male sex (OR = 2.15; 95% CI 1.09–4.22), and NSTE-ACS being ruled in by the 0,1-hr algorithm (OR = 3.12; 95% CI 1.20–8.10).
After adjusting for age, male sex, and HT, patients in the total population ruled in by either the 0,1-hr algorithm or 0,3-hr algorithm were significantly more likely to have significant coronary stenosis (OR = 3.09; 95% CI 1.37–6.94 and OR = 2.60; 95% CI 1.27–5.34, respectively; Table 3). However, NSTE-ACS being ruled in by the 0,3-hr algorithm was the only independent determinant of significant coronary stenosis in the CKD patients. In patients with normal renal function, older age, male sex, and NSTE-ACS being ruled in by the 0,1-hr algorithm were significantly associated with significant coronary stenosis, but being ruled in by the 0,3-hr algorithm was not (Table 3).
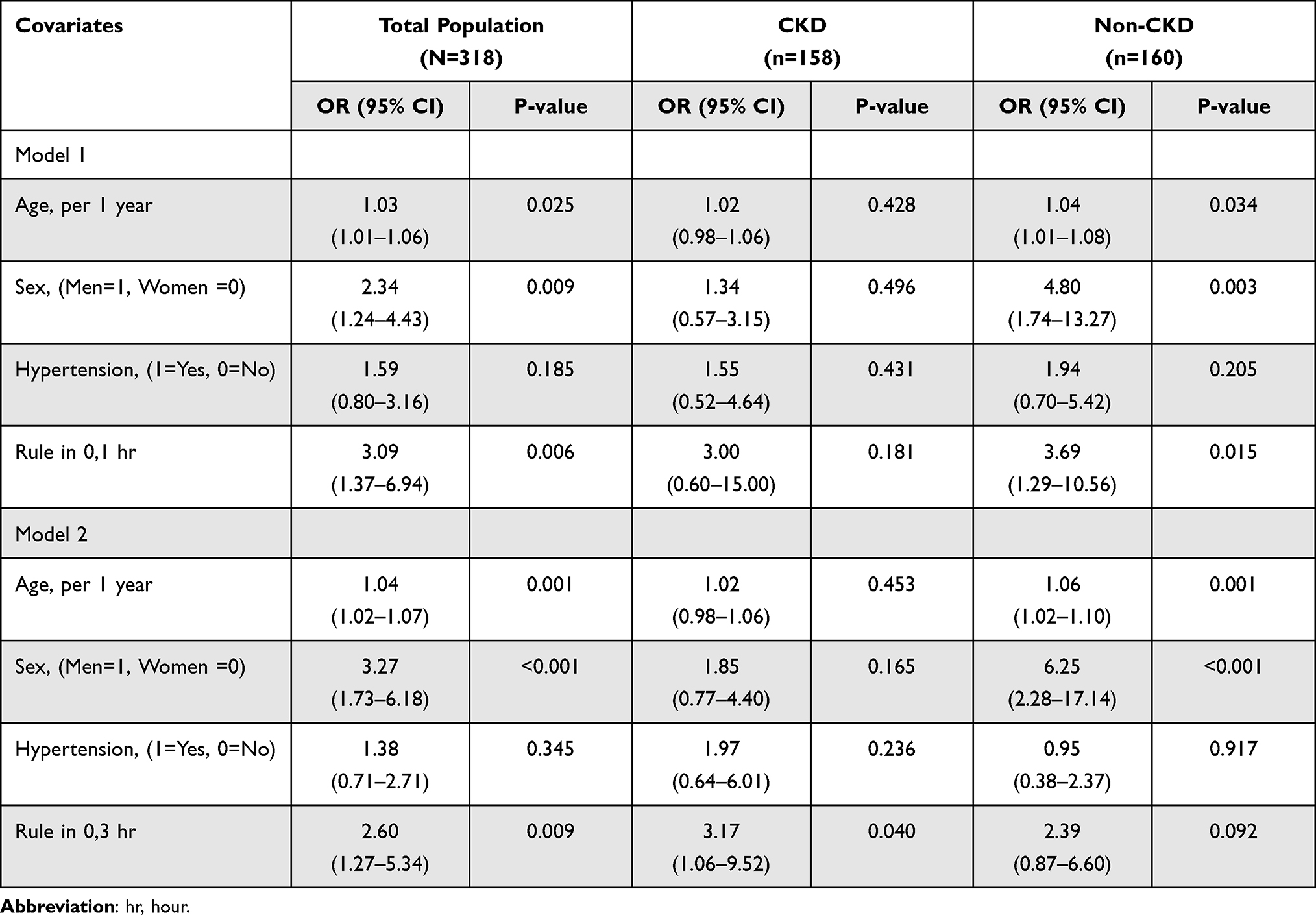 |
Table 3 Adjusted Odd Ratio (OR) of a Significant Coronary Stenosis by Using Regression Analysis |
Discussion
This study showed that being ruled in by either the 0,1-hr algorithm or the 0,3-hr algorithm was significantly associated with significant coronary stenosis in patients with suspected NSTE-ACS. However, there was a differential association between the rule-in group determined by each algorithm in CKD patients. CKD patients ruled in based on the 0,3-hr algorithm but not the 0,1-hr algorithm were more likely to have significant coronary stenosis.
In a 2018 study by Twerenbold et al,19 the 0,1-hr algorithm yielded a lower specificity and overall efficacy in CKD patients than those with normal renal function (96.5% vs 88.7% and 81% vs 51%, respectively). Furthermore, Chesnaye et al found that CKD patients had chronically elevated cTn.15 In addition, Sittichanbuncha et al, Chenevier-Gobeaux et al, and Van Lente et al found a higher cTn cut-off point to be more effective in CKD patients.16–18
Studies by Eggers et al and Chesnaye et al found that cTn was elevated in conditions other than type 1 myocardial infarction (MI) such as tachycardia, heart failure, and hypertensive crisis.14,15 The two algorithms’ differential association with significant coronary stenosis in this study may be explained by the false or chronic elevation of hs-cTnT in CKD patients. The initial hs-cTnT cut-off level for the 0,1-hr algorithm is 52 ng/L, much lower than that of the 0,3-hr algorithm (70 ng/L). The lower cut-off level of the 0,1-hr algorithm might result in patients being recruited whose hs-cTnT elevation is caused by diseases or conditions other than type 1 MI.
Our study showed that the determinants of significant coronary stenosis patients with normal renal function were older age and male sex, generally considered conventional risk factors for CAD.2 Another factor significantly associated with significant coronary stenosis was NSTE-ACS being ruled in based on the 0,1-hr algorithm, which has proven its efficacy and is recommended for use in the latest ESC guidelines.13 However, we found that being ruled in based on the 0,3-hr algorithm was not associated with significant coronary stenosis. A possible explanation might be that a 3-hour interval for serial hs-cTnT measurement allows for its elevation by conditions associated with cardiac myocyte injury other than acute type 1 MI. This hypothesis is supported by some previous studies, which have attributed cTn release to tachycardia, pericarditis, congestive heart failure, myocarditis, Takotsubo syndrome, pulmonary embolus, hypertrophic cardiomyopathy, and severe aortic stenosis.28,29 Furthermore, we explored the final diagnoses in patients with a normal renal function whose coronary angiograms did not reveal significant lesions. These patients were diagnosed with vasospasm (17%), arrhythmias (13%), myocarditis (13%), heart failure (13%), sepsis (13%), hypertrophic cardiomyopathy (6%), stroke (6%), Takotsubo syndrome (6%), and endocarditis (3%).
To the best of our knowledge, this was the first study to examine the association between significant coronary stenosis and the hs-cTnT algorithm used. All coronary angiograms were performed in the same tertiary care center. The same hs-cTnT assay (Elecsys®) was used for both the 0,1-hr and 0,3-hr algorithm, which allowed for clear data, unbiased comparison. However, there were some potential limitations to this study. First, due to the retrospective nature of the data collection, some laboratory data and some risk factors that might influence the results were missing. Second, although interventional cardiologists determined coronary angiogram results, we did not collect the data regarding any additional angiogram methods used such as intravascular ultrasound (IVUS) or fractional flow reserve (FFR). Third, this was a single-center study conducted at a university hospital in rural Thailand, apart from the relatively small sample size which may have some effect on the power of the study, our study population may differ from others in terms of biological, genetic, and cultural factors. Care should thus be taken when extrapolating the results.
Conclusions
Patients ruled in using the 0,3-hr algorithm were significantly more likely to have significant coronary stenosis, making this algorithm a possible algorithm of choice in CKD patients. However, a randomized clinical trial might be needed to determine the clinical efficacy of this algorithm in predicting coronary angiogram results in CKD patients.
Acknowledgments
The authors would like to thank the physicians and nurses at the Srinagarind Hospital accident and emergency department and Khon Kaen University Faculty of Medicine’s Department of Emergency Medicine for their support. We would like to acknowledge Dr. Dylan Southard for editing the MS via the KKU Publication Clinic (Thailand).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 Update: a report from the American Heart Association. Circulation. 2020;141:e139–596.
2. Mahmood SS, Levy D, Vasan RS, et al. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014;383:999–1008.
3. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305.
4. Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertens. 2003;42:1050–1065.
5. Malyszko J, Bachorzewska-Gajewska H, Malyszko J, et al. Markers of kidney function in the elderly in relation to the new CKD-EPI formula for estimation of glomerular filtration rate. Arch Med Sci AMS. 2011;7:658–664.
6. De Santo NG, Cirillo M, Perna A, et al. The heart in uremia: role of hypertension, hypotension, and sleep apnea. Am J Kidney Dis off J Natl Kidney Found. 2001;38:S38–46.
7. Levin A, Thompson CR, Ethier J, et al. Left ventricular mass index increase in early renal disease: impact of decline in hemoglobin. Am J Kidney Dis. 1999;34:125–134.
8. Blacher J, Safar ME, Guerin AP, et al. Aortic pulse wave velocity index and mortality in end-stage renal disease. Kidney Int. 2003;63:1852–1860.
9. Shlipak MG, Fried LF, Crump C, et al. Elevations of inflammatory and procoagulant biomarkers in elderly persons with renal insufficiency. Circulation. 2003;107:87–92.
10. Muntner P, Hamm LL, Kusek JW, et al. The prevalence of nontraditional risk factors for coronary heart disease in patients with chronic kidney disease. Ann Intern Med. 2004;140:9–17.
11. Hsu CY, McCulloch CE, Curhan GC. Epidemiology of anemia associated with chronic renal insufficiency among adults in the United States: results from the Third National Health and Nutrition Examination Survey. J Am Soc Nephrol. 2002;13:504–510.
12. Shroff GR, Frederick PD, Herzog CA. Renal failure and acute myocardial infarction: clinical characteristics in advanced chronic kidney disease, dialysis, and non-chronic kidney disease patients. A collaborative project of the United States Renal Data System/National Institutes of Health and the National Registry of Myocardial Infarction. Am Heart J. 2012;163:399–406.
13. Collet J-P, Thiele H, Barbato E, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2020;2020:ehaa575. doi:10.1093/eurheartj/ehaa575
14. Eggers KM, Jernberg T, Lindahl B. Cardiac troponin elevation in patients without a specific diagnosis. J Am Coll Cardiol. 2019;73:1–9.
15. Chesnaye NC, Szummer K, Bárány P, et al. Association between renal function and troponin T over time in stable chronic kidney disease patients. J Am Heart Assoc. 2019;8:e013091.
16. Sittichanbuncha Y, Sricharoen P, Tangkulpanich P, et al. The appropriate troponin T level associated with coronary occlusions in chronic kidney disease patients. Ther Clin Risk Manag. 2015;11:1143–1147.
17. Chenevier-Gobeaux C, Meune C, Freund Y, et al. Influence of age and renal function on high-sensitivity cardiac troponin T diagnostic accuracy for the diagnosis of acute myocardial infarction. Am J Cardiol. 2013;111:1701–1707.
18. Van Lente F, McErlean ES, DeLuca SA, et al. Ability of troponins to predict adverse outcomes in patients with renal insufficiency and suspected acute coronary syndromes: a case-matched study. J Am Coll Cardiol. 1999;33:471–478.
19. Twerenbold R, Badertscher P, Boeddinghaus J, et al. 0/1-Hour triage algorithm for myocardial infarction in patients with renal dysfunction. Circulation. 2018;137:436–451.
20. Twerenbold R, Neumann JT, Sörensen NA, et al. Prospective validation of the 0/1-h algorithm for early diagnosis of myocardial infarction. J Am Coll Cardiol. 2018;72:620–632.
21. Boeddinghaus J, Nestelberger T, Twerenbold R, et al. Impact of age on the performance of the ESC 0/1h-algorithms for early diagnosis of myocardial infarction. Eur Heart J. 2018;39:3780–3794.
22. Gunsolus I, Sandoval Y, Smith SW, et al. Renal dysfunction influences the diagnostic and prognostic performance of high-sensitivity cardiac troponin I. J Am Soc Nephrol. 2018;29:636–643.
23. Kraus D, von Jeinsen B, Tzikas S, et al. Cardiac troponins for the diagnosis of acute myocardial infarction in chronic kidney disease. J Am Heart Assoc. 2018;7:e008032.
24. Roffi M, Patrono C, Collet J-P, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315.
25. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618–e651.
26. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis off J Natl Kidney Found. 2014;63:713–735.
27. Pim ALT, Fearon WF, Bruyne BD, et al. Angiographic versus functional severity of coronary artery stenoses in the FAME Study: fractional flow reserve versus angiography in multivessel evaluation. JACC. 2010;55:2816–2821.
28. Ahmed M, Abdullah A, Kiernan T. 15 Elevated troponins and normal coronary angiogram. Heart. 2016;102:A9.
29. Bakshi TK, Choo MKF, Edwards CC, et al. Causes of elevated troponin I with a normal coronary angiogram. Intern Med J. 2002;32:520–525.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.