Back to Journals » International Journal of General Medicine » Volume 17
Differences in Treatment Patterns and Patient Characteristics Between COVID-19 Patients Treated with Nirmatrelvir/Ritonavir and Ensitrelvir in Japan
Authors Seki M ![]()
Received 27 April 2024
Accepted for publication 9 August 2024
Published 20 August 2024 Volume 2024:17 Pages 3621—3624
DOI https://doi.org/10.2147/IJGM.S475833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Masafumi Seki
Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Hidaka City, Saitama, Japan
Correspondence: Masafumi Seki, Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Yamane 1397-1, Hidaka City, Saitama, 350-1298, Japan, Tel +81-22-983-1221, Fax +81-22-983-1232, Email [email protected]
Abstract: Both nirmatrelvir/ritonavir (NMV-r) and ensitrelvir (ESV) are similar protease inhibitors that act against 3C-like protease (3CL protease) which is related the viral replication of SARS-CoV-2, and are recommended as oral treatment for COVID-19 patients in the guidance. However, NMV-r was approved in 2022 for the treatment of patients who are at high risk of progressing to severe COVID-19 based on the clinical trial data during severe original strain period, whereas ESV was approved in 2023 for the treatment of non-risk patients based on the clinical trial data during mild Omicron strain period in Japan. In this study, we investigated the differences in treatment patterns and patient characteristics between COVID-19 patients treated with NMV-r and ESV. NMV-r has usually been used for elderly patients with malignant tumors in the hospital, whereas ESV has been used for younger patients in the outpatient clinic as the common practice. It has been suggested that NMV-r and ESV have been used differently in Japan because there might be gaps in the implementation periods and the evidence from clinical trials. We should use each oral agent appropriately and make different recommendations in the guidance in the near future.
Keywords: SARS-CoV-2, 3C-like protease, cytochrome P450, guidance
COVID-19 has had an enormous impact on societies worldwide from the end of 2019 in Japan, and it has recently increased again from 2022 with some mutant lineages, such as Omicron variants, which were usually mild compared with original strains that induced severe pneumonia in COVID-19 patients with high risks, such as middle to high age males with obesity, and have the underlying diseases including malignancies and diabetes mellitus.1 The guidelines usually targeted these high risk populations for treatment by the antiviral agents even though the patients initially had mild to moderate status.2–4
Nirmatrelvir (NMV) is an oral protease inhibitor that is active against the main proteases of SARS-CoV-2, including 3C-like protease (3CL protease), that play essential roles in viral replication by cleaving the 2 viral polyproteins.5 NMV is packaged with ritonavir, a strong cytochrome P450 (CYP) 3A4 inhibitor, and co-administration of ritonavir is required to increase NMV concentrations to the target therapeutic range.6 Therefore, NMV combined with ritonavir (NMV-r, as Paxlovid, Pfizer Inc., NY, USA) is approved by the Food and Drug Administration (FDA) for the treatment of mild to moderate COVID-19 in adults who are at high risk of progressing to severe COVID-19 in the USA, and it also became available in Japan in February 2022.6,7
Recently, ensitrelvir (ESV; Shionogi CO. LTD., Osaka, Japan) was developed; its use started from March 2023 in Japan, and strong activity for eliminating SARS-CoV-2 was reported.8,9 ESV also inhibits 3CL protease and effectively reduces viral replication. In fact, ESV treatment was reported to result in clinical improvement of symptoms along with the strong elimination of SARS-CoV-2 in COVID-19 patients.10
However, it is still unclear the differences of patient characteristics between those we should treat by either NMV-r or ESV although the guidance in Japan recommend the NMV-r for the high risk patients rather than ESV and there is no mention about use of ESV in the other countries because ESV is now available only in Japan.2–4 Therefore, we need to investigate the differences in treatment patterns and patient characteristics between COVID-19 patients treated with NMV-r and ESV.
In this study, the clinical use of NMV-r and ESV in this first year, from April 01/2023 to March 31/2024, was retrospectively investigated, and make clear the differences of patterns/background of the patients who received NMV-r and ESV. NMV-r was administered as nirmatrelvir 300 mg with ritonavir 100 mg orally twice daily for 5 days, and ESV were used orally 375 mg once at first day and followed 125mg once more four days. The patients who received and completed 5 day treatments by these two agents were included. The one-year study period may be relatively shorter follow-up period for typical COVID-19 studies, however, ESV became available only one year ago.
In our hospital, a total of 257 COVID-19 patients admitted as inpatients and/or visited the outpatient clinic, 160 patients received drip infusion of remdesivir (Gilead, Foster City, CA, USA) and 50 patients were treated by oral molnupiravir (Merck. and Co, Inc., New Rahway, NJ, USA) because these two agents were used antecedently from 2021 in Japan, and the patients who received these two agents were excluded in this study.
The Mann–Whitney test and the chi-squared test were used to compare continuous variables between two groups. Because samples are small size and non-normal data distribution, we used the non-parametric analysis and could not do additional analysis, including regression model. Therefore, adjusting for potential confounders or exploring relationships between variables could not be performed. These are limitations of this study. A p-value of less than 0.05 was defined as indicating a significant difference. All analyses were performed using Stat View software (Abacus Concepts, Cary, NC, USA), which is available in Japan as same as Easy R software (Saitama, Japan) and SPSS (IBM, Chicago, IL, USA), and have been used.11
The characteristics of the COVID-19 patients differed by the drug used. The 15 patients treated by NMV-r were significantly older and significantly more often hospitalized than the 32 patients treated by ESV (age: 63.2 vs 56.8 years, p=0.022; and outpatient/inpatient: 1/14 vs 18/14, p=0.0012, respectively) (Table 1). The male/female ratio and the number of patients who had underlying diseases were similar between the NMV-r group and ESV group, but the patients treated by NMV-r had more malignant tumors than the patients treated by ESV (66.7% vs 26.3%, p=0.026).
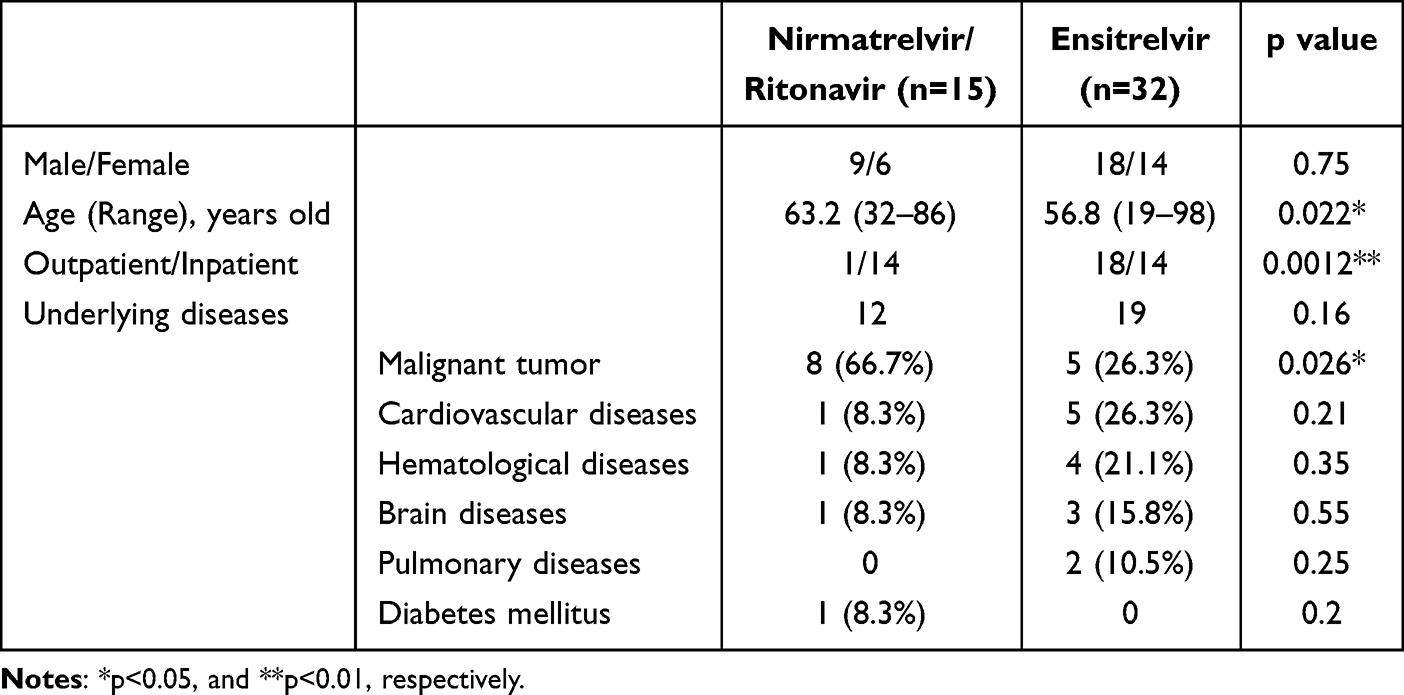 |
Table 1 Patients’ Characteristics by Drug Administered |
These data suggest that NMV-r was used for inpatients who had malignant tumors. These patients might be a relatively small number because most of the inpatients preferred drip infusions remdesivir as we previously mentioned, rather than oral agents when appetite loss appeared with the growth of the malignant tumors and more severe conditions. In fact, NMV-r was used for these types of patients, such as those with mild to moderate severity, but they had high-risk underlying diseases in the clinical trials and in the real world,6,7 and NMV-r was recommended for them in both the USA and Japan.2–4
In contrast, ESV was used for young outpatients, and half of them did not have any underlying diseases. The clinical trials and real world use of ESV were started later than for NMV-r, during the Omicron strain-dominant era, and most of the evidence was collected from more mild COVID-19 patients.9,10,12 Therefore, the use of ESV was mainly recommended for mild to moderate patients without underlying diseases, and it might be used predominantly in the outpatient clinic. However, the present investigation was performed at only one hospital, and ESV showed strong viral inhibitory activity similar to NMV-r, and it may also be useful for the treatment of inpatients who showed delayed improvement, including those with hematological diseases.13 There are no direct comparative data between NMV-r and ESV in the virological effectiveness, however, similar viral inhibitory effects that the patients received with treatment by the agents showed about 10 times lower viral RNA amounts, compared with the patients who received placebo treatments, were found in the both of the clinical trial data in NMV-r and ESV.6,12 We did not find direct comparison data among NMV-r/ESV, remdesivir, and monoclonal antibodies in the clinical trial for severe and immunocompromised patients, however, NMV-r showed similar viral inhibitory effects with remdesivir in vitro study that SARS-CoV-2 were infected with VeroE6-GFP cells.14
In addition, drug-drug interaction is a critical issue in use of NMV-r and ESV because these agents inhibit the cytochrome P450 activity, and change the concentration of other related drugs, including sleeping pills, diabetic agents, and antilipidemic drugs.15,16 However, ESV has about 30 contraindicated drugs although NMV-r has about 50 contraindicated drugs as co-administration agents. These data suggest that ESV might be a little easier to use, compared with NMV-r in the hospital/clinic.
This study has the limitations of a small sample size, which may limit the generalizability of the findings. The potential for bias in treatment selection, as patients with more severe conditions may have been more likely to receive NMV-r. Additionally, further research would be needed to confirm these results and establish causal relationships between the drugs and patient outcomes.
In conclusion, NMV-r and ESV were similarly strong protease inhibitors for SARS-CoV-2, but they were used for different types of COVID-19 patients, although both of them were administered orally to mild to moderate patients. NMV-r was used mainly in the hospital, but its greater use for outpatients in the clinic could be considered in Japan.
Ethics
This study and related analysis were approved by the Institutional Review Board of Saitama Medical University International Medical Center on July 06 and December 27, 2022 as #2022-032 and #2022-146, and registered as UMIN000047691. The patients whose specimens were analyzed provided written, informed consent to have any accompanying images and their case details published. This study was performed according to the Declaration of Helsinki.
Acknowledgments
The author would like to thank all healthcare staff, including physicians, pharmacists, nurses, and medical clinical microbiological technicians, for their kind support with COVID-19 and influenza management in Saitama Medical University International Medical Center and Tohoku Medical and Pharmaceutical University.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Wu C, Cheng X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA. 2020;180:934–943.
2. Bhimraj A, Morgan R, Shumaker AH, et al. Infectious diseases society of America guidelines on the treatment and management of patients with COVID-19. Clin Infect Dis. 2020. doi:10.1093/cid/ciaa478
3. Japanese Ministry of Health Labour and Welfare. The guidance of management for the patients with COVID-19; 2022. Available from: https://www.mhlw.go.jp/content/001136687.pdf.
4. NIH. Coronavirus disease 2019 (COVID-19) treatment guidelines; 2023. Available from: https://www.covid19treatmentguidelines.nih.gov/.
5. Pillaiyar T, Manickam M, Namasivayam V, Hayashi Y, Jung SH. An overview of severe acute respiratory syndrome-coronavirus (SARS-CoV) 3CL protease inhibitors: peptidomimetics and small molecule chemotherapy. J Med Chem. 2026;59(14):6595–6628. doi:10.1021/acs.jmedchem.5b01461
6. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19. N Engl J Med. 2022;386(15):1397–1408. doi:10.1056/NEJMoa2118542
7. Ganatra S, Dani SS, Ahmad J, et al. Oral nirmatrelvir and ritonavir in nonhospitalized vaccinated patients with coronavirus disease 2019. Clin Infect Dis. 2023;76(4):563–572. doi:10.1093/cid/ciac673
8. Shimizu R, Sonoyama T, Fukuhara T, Kuwata A, Matsuo Y, Kubota R. Safety, tolerability, and pharmacokinetics of the novel antiviral agent ensitrelvir fumaric acid, a SARS-CoV-2 3CL protease inhibitor, in healthy adults. Antimicrob Agents Chemother. 2022;66(10):e0063222. doi:10.1128/aac.00632-22
9. Mukae H, Yotsuyanagi H, Ohmagari N, et al. A randomized phase 2/3 study of ensitrelvir, a novel oral SARS-CoV-2 3C-like protease inhibitor, in Japanese patients with mild-to-moderate COVID-19 or asymptomatic SARS-CoV-2 infection: results of the phase 2a part. Antimicrob Agents Chemother. 2022;66(10):e0069722. doi:10.1128/aac.00697-22
10. Mukae H, Yotsuyanagi H, Ohmagari N, et al. Efficacy and safety of ensitrelvir in patients with mild-to-moderate coronavirus disease 2019: the phase 2b part of a randomized, placebo-controlled, phase 2/3 study. Clin Infect Dis. 2023;76(8):1403–1411. doi:10.1093/cid/ciac933
11. Shimada D, Seki M. Effectiveness of drip infusion of lascufloxacin, a novel fluoroquinolone antibiotic, for patients with pneumonia including chronic lung disease exacerbations and lung abscesses. Infect Drug Resist. 2024;8(17):911–918. doi:10.2147/IDR.S453634
12. Yotsuyanagi H, Ohmagari N, Doi Y, et al. Efficacy and safety of 5-day oral ensitrelvir for patients with mild to moderate COVID-19: the SCORPIO-SR randomized clinical trial. JAMA Network Open. 2024;7(2):e2354991. doi:10.1001/jamanetworkopen.2023.54991
13. Seki M, Mitsutake K, Shimizu A, et al. Ensitrelvir improved SARS-CoV-2 viral titers of COVID-19 patients refractory to remdesivir. World J Clin Med Res. 2023;3(1):27–31. doi:10.31586/wjcmr.2023.796
14. Vangeel L, Chiu W, De Jonghe S, et al. Remdesivir, molnupiravir and nirmatrelvir remain active against SARS-CoV-2 omicron and other variants of concern. Antiviral Res. 2022;198:105252. doi:10.1016/j.antiviral.2022.105252
15. Marzolini C, Kuritzkes DR, Marra F, et al. Recommendations for the management of drug-drug interactions between the COVID-19 antiviral nirmatrelvir/ritonavir (paxlovid) and comedications. Clin Pharmacol Ther. 2022;112(6):1191–1200. doi:10.1002/cpt.2646
16. Shimizu R, Matsuzaki T, Oka R, et al. Evaluation of drug-drug interactions of ensitrelvir, a SARS-CoV-2 3CL protease inhibitor, with transporter substrates based on in vitro and clinical studies. J Clin Pharmacol. 2023;63(8):918–927. doi:10.1002/jcph.2247
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.