Back to Journals » Journal of Pain Research » Volume 7
Differences in pain perception during open muscle biopsy and Bergstroem needle muscle biopsy
Authors Dengler J, Linke P, Gdynia HJ, Wolf S, Ludolph AC, Vajkoczy P, Meyer T
Received 16 June 2014
Accepted for publication 15 August 2014
Published 17 November 2014 Volume 2014:7 Pages 645—650
DOI https://doi.org/10.2147/JPR.S69458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Michael Schatman
Julius Dengler,1 Peter Linke,2 Hans J Gdynia,3 Stefan Wolf,1 Albert C Ludolph,3 Peter Vajkoczy,1 Thomas Meyer2
1Department of Neurosurgery, 2Department of Neurology, Charité – Universitätsmedizin Berlin, Berlin, Germany; 3Department of Neurology, Universitätsklinikum Ulm, Ulm, Germany
Purpose: Open surgical muscle biopsy (OB) and percutaneous Bergstroem needle muscle biopsy (NB) are equally accepted procedures. However, there are no data comparing intraprocedural pain for both techniques. We designed this prospective trial to test the hypothesis that the less invasive NB causes less intraprocedural pain than OB.
Methods: In a two-center prospective trial, 33 patients underwent both procedures in one session. All patients quantified intraprocedural pain using the numeric rating scale (NRS). Mean NRS values were calculated along with the difference in NRS values (ΔNRS) between both types of biopsies.
Results: Mean NRS values were 4.5 (±2.7 standard deviation [SD]) for NB and 3.2 (±2.1) for OB (P=0.02). Of the patients, 57.6% described the ΔNRS as ≤2 NRS points. Regarding the pain categories “mild” (NRS 0–3), “moderate” (NRS 4–7), and “severe”(NRS 8–10), no significant difference was observed between NB and OB. Patients who found NB to be more uncomfortable were more likely to quantify the ΔNRS as >2 NRS points than patients finding OB more uncomfortable.
Conclusion: Our results do not support the hypothesis that intraprocedural pain in NB is less than in OB. When informing the patient about both types of muscle biopsies, the amount of intraprocedural pain should not serve as a differentiating characteristic.
Keywords: Bergstroem needle, muscle biopsy, percutaneous, pain, numeric rating scale
Introduction
Muscle biopsies are essential diagnostic procedures for various neurological diseases.1–3 They are usually conducted using either an open surgical approach or a minimally invasive percutaneous needle technique. Ever since Bergstroem first described the needle biopsy technique, one of the main controversies regarding this approach was that its sample yield might be too small for sufficient diagnostics and that therefore the needle technique might not be able to compete with the open biopsy (OB).4 Advocates of the percutaneous Bergstroem needle biopsy (NB) technique reacted to this by introducing certain technical modifications that were shown to significantly increase sample yield.5–7 These advances and the fact that percutaneous techniques produce significantly less scarring due to a smaller skin incision prompted many centers to abandon the open surgical approach completely.8,9 Another supporting argument for percutaneous muscle biopsy techniques is the general assumption that less invasive techniques might be less painful for the patient.10,11
However, a factor that has been neglected in the literature is the patient’s actual perception of pain during a muscle biopsy. Since muscle biopsies are predominantly conducted with only local anesthesia, the patient has to deal with relevant side effects of an awake surgical procedure – mainly pain. The hypothesis that the NB technique might decrease pain and discomfort during muscle biopsy when compared to the open approach has never been tested before.
To test this hypothesis we designed a two-center prospective trial to compare pain sensation in patients undergoing both procedures in one surgical session.
Methods
The trial was designed as a two-center prospective study (Ulm and Berlin). This pain assessment study was approved by the local ethics committee of the Charité in Berlin (EA4/043/13). It was conducted as an adjunct to a separate, ongoing study of patients with amyotrophic lateral sclerosis who underwent both an OB and an NB of the deltoid muscle as part of the study protocol of the NOG113531 trial. All patients were fully informed about the trial and gave written consent.
Biopsy procedures
In all patients the same deltoid muscle was used for both types of biopsies. The patients were informed that after both biopsies they would be asked for an assessment of intraprocedural pain. The NB was carried out first and immediately followed by the OB. Both sites of biopsy were placed at least 3 cm apart from each other. All procedures were carried out in an operating room.
For the NB, the skin and subcutaneous tissue were infiltrated with about 2 mL of lidocain (2%) for local anesthesia at the site of biopsy, after which 3 minutes was given for the lidocain to take effect. Care was taken not to enter the muscle tissue, so that the lidocain would have no effect on the numeric rating scale (NRS) assessment and the histological read out. Next, the skin and the muscle fascia were stab incised with a size 11 blade, creating an opening large enough to allow for passage of the 5 mm type Bergstroem needle. Then, the needle was advanced through the muscle fascia into the muscle at a depth of about 1 cm. Next, a 50 mL syringe was connected to the suction port of the needle via a 10 cm extension tube. To open the cutting port of the needle the trochar was pulled out by about 1–2 cm. The surgeon and the assistant then synchronized manual suction (via the syringe) and the closure of the needle, so that the muscle parts that were sucked into the needle lumen would be cut out. The needle was then removed and the muscle sample recovered. Finally, the wound was closed using a 3.0 nylon suture.
For the OB, an incision mark of about 3–4 cm was drawn onto the skin over the deltoid muscle at least 3 cm distant to the site of the NB. Local anesthesia of this area was conducted using about 2–5 mL of lidocain (2%) and taking care not to enter below the subcutaneous tissue. Again, 3 minutes was given for the lidocain to take effect. Next, the skin was incised using a size 11 blade and the muscle fascia was visualized using blunt preparation. Next, a cube of about 1×1×1 cm3 was cut out of the muscle using a scalpel or scissors. Excess bleeding was addressed with cauterization. Finally, the muscle fascia was closed using resorbable sutures and the skin was closed using 3.0 nylon sutures.
Wound healing was checked 7–10 days after biopsy, followed by removal of the sutures.
Pain assessment
Both biopsies, NB and OB, were conducted consecutively. Within the first minute after completion of the skin closure of the second biopsy, each patient was asked to rate the amount of pain for each biopsy separately on the NRS with values from 0–10; “0” represented no pain, “10” maximal pain. NRS values were then grouped into the following categories: “mild pain” (NRS 0–3), “moderate pain” (NRS 4–7), and “severe pain” (NRS 8–10). In accordance with previously published data, a difference in NRS (ΔNRS) of ≤2 points was considered not to be clinically relevant.11 The patient was also asked which biopsy procedure he/she found more uncomfortable.
Statistics
All analyses were performed using SPSS software, Version 22.0.0.0 (IBM Corporation, Armonk, NY, USA). We used the Shapiro–Wilk test to analyze whether data were distributed normally. Since NRS values were normally distributed, the paired samples t-test was applied to analyze NRS values regarding NB versus OB (including subgroup analyses for sex and study centers). Values are given as mean ± standard deviation (SD). To visualize the distribution of differences in pain assessment, including the limits of agreement with upper and lower 95% confidence intervals (CIs), we used the method suggested by Bland and Altman:12 for each patient, the difference in NRS value between NB and OB was related to the average of both NRS values. Linear regression was used to examine a possible age dependency of NRS values. Chi-square analysis and Fisher’s exact test were applied for frequency analysis of the different pain categories in patients who found either OB or NB more uncomfortable.
Results
Of the 38 patients eligible for this trial, one patient refused participation, one patient died before any biopsies were conducted, and three patients did not give a pain assessment due to organizational reasons. We therefore included 33 patients (17 females and 16 males) in this trial (five from the Ulm group and 28 from the Berlin group). Mean age was 63 (±8) years. The mean NRS score for the initial NB was 4.5 (±2.7) and for the OB was 3.2 (±2.1) with a statistically significant difference between both groups (P=0.02) (Figure 1A). To examine the clinical relevance of this finding, the differences between NRS in both biopsy techniques were evaluated using the Bland–Altman method (Figure 1B). Of the patients, 57.6% described the difference as ≤2 NRS points. The plot shows that the majority of people found the NB more painful. The limits of agreement for the entire cohort ranged between −4.9 and +7.5.
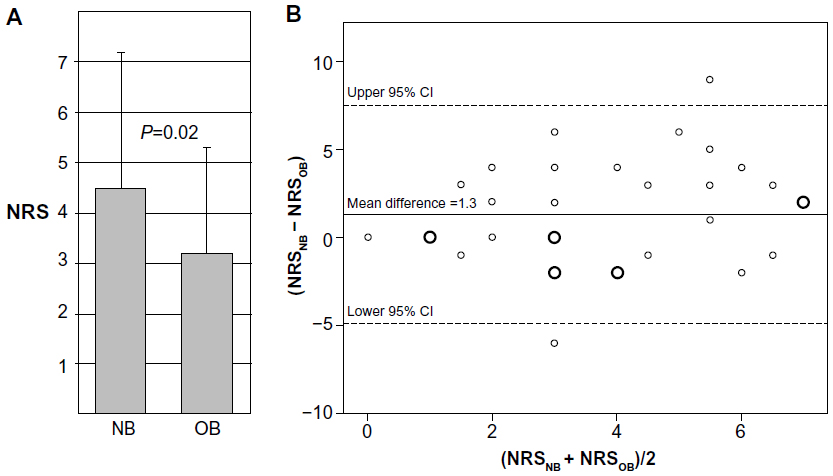 | Figure 1 Pain perception during NB and OB. |
Pain distribution for OB and NB was “mild” in 54.5% and 42.4%, “moderate” in 39.4% and 33.3%, and “severe” in 6.1% and 24.2% of patients (Figure 2A), respectively. When comparing these pain categories there was no significant difference between both biopsy techniques (P=0.12).
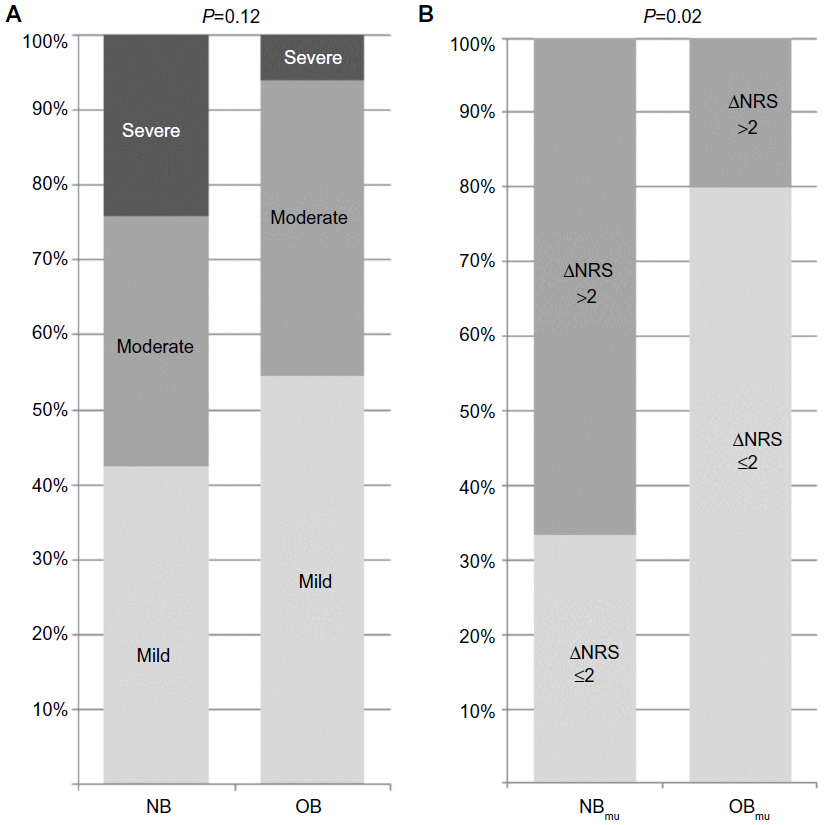 | Figure 2 Pain categories and differences in pain during OB and NB. |
All patients were asked to rate which biopsy technique was more uncomfortable. NB was chosen by 54.5% of the patients as more uncomfortable, 30.3% chose OB, and 15.2% found both procedures equally uncomfortable. Next, we conducted a separate analysis of those patients who had described one of the biopsy techniques to be more uncomfortable than the other. This separate analysis aimed to describe how often the difference in NRS (ΔNRS) between both biopsy techniques was >2. A ΔNRS of 2 had been defined as the cutoff for clinically relevant difference in pain (Figure 2B). The ΔNRS was >2 in 66.7% of patients rating NB as more uncomfortable, compared to 20.0% of patients who had found OB more uncomfortable (P=0.02).
Pain assessment was not dependent on age or sex, both for raw NRS values and for pain categories. Also, the data from both centers were compared to each other, showing no significant difference (P=0.13): at both centers mean NRS values for the NB were higher than those for the OB. Wound healing was regular in all cases, no infections were observed.
Discussion
The main results of this trial do not support the general assumption that a less invasive muscle biopsy technique also causes less intraprocedural pain. When NRS values were grouped into mild, moderate, and severe categories, both biopsy techniques produced equivalent pain perception (Figure 2A). Once raw NRS values were used for pain assessment we found that the NB was significantly more painful than the OB procedure (Figure 1A). Nevertheless, the Bland–Altman analysis showed that the majority of patients described the difference in pain perception as equal to or less than 2 NRS points (Figure 1B), which from a clinical point of view can be interpreted as below the cutoff for a clear difference.11
We did find, however, that patients who described the NB to be more painful were significantly more likely to quantify the difference in pain as clinically relevant with more than 2 NRS points. In contrast, most patients who found the OB more uncomfortable described the difference in pain as equal to or less than 2 NRS points (Figure 2B). So if patients were able to identify one biopsy technique as being more painful, this added pain was more likely to be clinically relevant during the NB than during the OB.
When planning a muscle biopsy, health care professionals are often confronted with a certain anxiety on the patient’s part concerning potential pain during the intervention. The patient is interested to know which biopsy technique might allow for the least possible amount of discomfort during the procedure. Many therapists find it difficult to sufficiently inform the patient on this issue and generally assume that the less invasive technique might also be less painful. Data on pain perception during muscle biopsy procedures, be it OB or any type of minimally invasive biopsy, are scarce or anecdotal. This prompted us to plan this trial, which is the first to present comparative data on NB versus OB.
Dietrichson et al compared pain during muscle biopsy with two different minimally invasive techniques: the Liverpool needle, which is similar to the Bergstroem technique, and the chonchotome forceps.10 They reported that the conchotome was subjectively less painful for the patients, yet no objective data on pain were given. Magistris et al evaluated pain in patients who underwent muscle biopsy with a spring-loaded automatic microbiopsy needle device.13 They reported that “pain related to the biopsy procedure, when experienced, is very brief”. However, no further details were presented. Hayot et al compared pain during muscle biopsy with such an automatic microbiopsy device versus the Bergstroem NB in the same surgical session in 21 patients.11 The automatic microbiopsy was conducted first, followed by the NB. They stated that pain ranged between 0–1 on the NRS during the microbiopsy and between 4–6 during the NB. No more details on absolute NRS values or mean values were presented. The only trial giving more detailed information was published by Derry et al.14 This trial did not compare NB to another technique but did evaluate the level of discomfort in 18 patients during the Bergstroem NB on a scale from 1 to 10: the mean value was 3.9 (±2.9).
Our trial’s mean NRS value of 4.5 for the NB corresponds to the pain levels for NB of Hayot et al11 (NRS range 4–6) and Derry et al14 (mean NRS 3.9). Hayot et al presented the only trial comparing the Bergstroem NB to another technique and found a less painful alternative with the spring-loaded microbiopsy needle. They described a difference between NRS during microbiopsy versus NB of at least 3 NRS points in every single patient. We agree that this can be called clinically relevant, especially in contrast to our data, in which Bland–Altman analysis revealed that the majority of our patients described either no difference or just a rather small difference equal to or less than 2 NRS points between the NB and the OB (Figure 1B). When interpreting our results as indicating clinical equivalence in pain levels during NB and OB, one must also conclude that our trial does not support the general assumption that a percutaneous biopsy technique like the Bergstroem NB is automatically less painful than OB techniques.10,11
Our data suggest that OB remains a valid option. It might therefore be worth considering some of its advantages. Especially when comparing it to the microbiopsy or the Bergstroem NB, OB allows for a larger muscle tissue yield, which can even be more easily modified according to individual diagnostic needs.15 Another advantage of OB is that it requires less profound knowledge of anatomy since the muscle tissue is visualized. It is therefore more intuitive for young physicians, who are usually the ones who conduct muscle biopsy procedures during their first or second year of residency. Also, OB requires less coordinative skills than a percutaneous NB. Another disadvantage of Bergstroem NB is that it requires the aid of an assistant who builds up suction via the 50 mL syringe so that muscle tissue gets trapped inside the needle lumen. Coordinating this important step during NB takes some practice. Such assistance by a second person is not needed during open muscle biopsy.
However, one major advantage of the needle technique remains unchallengeable: it leaves a significantly smaller scar. This is of special relevance when muscle biopsies are taken from parts of the body that are not always covered by clothes, such as the lower arm or the lower leg. Presumably, many patients would accept more pain during a biopsy procedure if only a smaller scar can be expected. In addition, OB carries a higher risk of muscle herniation, hematoma formation, or wound dehiscence than NB.16
So if both the Bergstroem needle and the open technique are equally available at a given center, we feel that the patient should have the opportunity to choose. When informed about the extent of invasiveness (eg, larger versus smaller scar) and intraoperative pain levels of both procedures, the patient will most likely be able to decide between both options. Nevertheless, in our opinion, the results of our trial stress that it is important not to insinuate that the Bergstroem NB is a less painful alternative to OB.
A strength of our study is that it is the first to directly compare pain during the open and the Bergstroem needle approach in the same patients. Each patient underwent both procedures. This is important, since, if each procedure had been carried out in separate groups, one could have argued that individual differences in pain perception might have served as a bias. Also, the trial showed matching results in both participating centers, which reduces the possible influence the surgeon might have had on pain perception.
Nevertheless, some limitations of this trial need to be discussed as well. First of all, our patient cohort exclusively comprised amyotrophic lateral sclerosis patients. One might argue that pain perception in this specific group of patients with varying degrees of degeneration of the central nervous system might be different from patients with other diseases, eg, myopathies. Also, since the mean age was 63 years, one may argue that our results may only be relevant for patients of this age group. Furthermore, like Hayot et al, we did not randomize the sequence of biopsy types: all patients first underwent NB followed by OB.11 The reason for this is that the actual study protocol for the trial underlying our pain assessment study demanded this exact sequence of biopsies since it wanted to rule out any negative influence on histological readout caused by initially conducting the more traumatizing OB. Also, since we exclusively included biopsies of deltoid muscles, our results may be limited to this muscle group and not generalized to other muscle groups. Another limitation is that the distance of 3 cm between both biopsy sites may be too small to allow for separate pain quantification between both sites. Nevertheless, the distance of 3 cm was part of the underlying study protocol and could not be changed for this pain study.
Conclusion
The results of this trial suggest that in our patient cohort the Bergstroem NB technique did not produce less intraprocedural pain than the OB technique. These findings are relevant since they contradict the general assumption that a less invasive muscle biopsy technique might also be less painful. We therefore feel that when informing the patient about advantages and disadvantages of both biopsy techniques, the amount of intraprocedural pain should not serve as a differentiating characteristic.
Acknowledgments
The authors contributed to this paper as follows:
Julius Dengler and Thomas Meyer: conception and design, collecting the data, analysis and interpretation, writing the article, and approving the final version of the manuscript.
Peter Linke and Hans J Gdynia: collecting the data, providing critical revisions, and approving the final version of the manuscript.
Stefan Wolf, Albert C Ludolph, and Peter Vajkoczy: analysis and interpretation, providing critical revisions, and approving the final version of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Zampieri S, Doria A, Adami N, et al. Subclinical myopathy in patients affected with newly diagnosed colorectal cancer at clinical onset of disease: evidence from skeletal muscle biopsies. Neurol Res. 2010;32(1):20–25. | |
Gáti I, Danielsson O, Betmark T, Ernerudh J, Ollinger K, Dizdar N. Culturing of diagnostic muscle biopsies as spheroid-like structures: a pilot study of morphology and viability. Neurol Res. 2010;32(6):650–655. | |
Filosto M, Tonin P, Vattemi G, et al. The role of muscle biopsy in investigating isolated muscle pain. Neurology. 2007;68(3):181–186. | |
Bergstrom J. Percutaneous needle biopsy of skeletal muscle in physiological and clinical research. Scand J Clin Lab Incest. 1975;35(7):609–616. | |
Evans WJ, Phinney SD, Young VR. Suction applied to a muscle biopsy maximizes sample size. Med Sci Sports Exerc. 1982;14(1):101–102. | |
Melendez MM, Vosswinkel JA, Shapiro MJ, et al. Wall suction applied to needle muscle biopsy – a novel technique for increasing sample size. J Surg Res. 2007;142(2):301–303. | |
Tarnopolsky MA, Pearce E, Smith K, Lach B. Suction-modified Bergström muscle biopsy technique: experience with 13,500 procedures. Muscle Nerve. 2011;43(5):717–725. | |
Pamphlett R, Harper C, Tan N, Kakulas BA. Needle muscle biopsy: will it make open biopsy obsolete? Aust N Z J Med. 1985;15(2):199–202. | |
Coté AM, Jiménez L, Adelman LS, Munsat TL. Needle muscle biopsy with the automatic Biopty instrument. Neurology. 1992;42(11):2212–2213. | |
Dietrichson P, Coakley J, Smith PE, Griffiths RD, Helliwell TR, Edwards RH. Conchotome and needle percutaneous biopsy of skeletal muscle. J Neurol Neurosurg Psychiatry. 1987;50(11):1461–1467. | |
Hayot M, Michaud A, Koechlin C, et al. Skeletal muscle microbiopsy: a validation study of a minimally invasive technique. Eur Respir J. 2005;25(3):431–440. | |
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical testing. Lancet. 1986;1(8476):307–310. | |
Magistris MR, Kohler A, Pizzolato G, et al. Needle muscle biopsy in the investigation of neuromuscular disorders. Muscle Nerve. 1998;21(2):194–200. | |
Derry KL, Nicolle MN, Keith-Rokosh JA, Hammond RR. Percutaneous muscle biopsies: review of 900 consecutive cases at London Health Sciences Centre. Can J Neurol Sci. 2009;36(2):201–206. | |
Lacomis D. The use of percutaneous needle muscle biopsy in the diagnosis of myopathy. Curr Rheumatol Rep. 2000;2(3):225–229. | |
Meola G, Bugiardini E, Cardani R. Muscle biopsy. J Neurol. 2012;259(4):601–610. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.