Back to Journals » International Journal of General Medicine » Volume 15
Differences in Overweight and Obesity Prevalence in Middle-Aged Men from Twelve Middle Eastern and Asian Countries Living in Saudi Arabia
Authors AlTamimi JZ, Alshwaiyat NM ![]() , AlFaris NA
, AlFaris NA ![]() , AlKehayez NM
, AlKehayez NM ![]() , Ahmad A, Alagal RI
, Ahmad A, Alagal RI ![]()
Received 23 January 2022
Accepted for publication 10 March 2022
Published 24 March 2022 Volume 2022:15 Pages 3333—3343
DOI https://doi.org/10.2147/IJGM.S359639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jozaa Z AlTamimi,1 Naseem M Alshwaiyat,2 Nora A AlFaris,1 Nora M AlKehayez,1 Aryati Ahmad,2,3 Reham I Alagal1
1Department of Physical Sports Sciences, College of Education, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 2School of Nutrition and Dietetics, Faculty of Health Sciences, Universiti Sultan Zainal Abidin, Kuala Nerus, Terengganu, Malaysia; 3Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
Correspondence: Reham I Alagal, Department of Physical Sports Sciences, College of Education, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia, Email [email protected]
Purpose: This study was conducted to determine differences in overweight and obesity prevalence and the associated sociodemographic variables among middle-aged men from twelve Middle Eastern and Asian countries living in Riyadh, Saudi Arabia.
Methods: This is a cross-sectional study. The study sample was chosen randomly using a stratified clustered sampling technique. The weight and height of 1800 middle-aged men (36 to 59 years) from twelve Middle Eastern and Asian countries living in Riyadh, Saudi Arabia, were measured using standardized methods. Face-to-face interviews were used to gather sociodemographic information from participants.
Results: Overweight and obesity were reported among 51.9% and 14.7% of participants, respectively. Nationality was a predictor of overweight and obesity. Subjects from Bangladesh and Saudi Arabia had the lowest (41.0%) and highest (85.1%) rates of overweight and obesity, respectively. Increasing age, staying in Saudi Arabia for a longer period, being single, and earning a high monthly income were associated with a significantly higher risk of overweight and obesity among the participants.
Conclusion: The findings revealed significant differences in the prevalence of overweight and obesity among participants from different countries living in Saudi Arabia. Sociodemographic variables associated with overweight and obesity among participants were identified.
Keywords: overweight, obesity, middle-aged men, Middle East, Asia
Introduction
Obesity is now a global phenomenon, with a steady rise in incidence over the last few decades.1,2 It is linked to an increased adulthood health burden, which manifests in the form of many non-communicable diseases such as coronary heart disease, stroke, hypertension, dyslipidemia, and type 2 diabetes.3,4 Obesity is associated with an increased leptin level in the serum due to high adipose tissue mass and the development of leptin resistance. Leptin is a hormone produced mainly by adipocytes and is considered a key regulator of body weight through inhibition of food intake and stimulation of energy expenditure. Endothelial function is disrupted by elevated serum leptin levels, which increase reactive oxygen species formation while lowering nitric oxide synthesis.5 Angiogenesis, the development of new blood vessels from pre-existing ones, is prone in obese patients as a compensation strategy for ischemia and hypoxia. The mitogen vascular endothelial growth factor (VEGF), which stimulates endothelial cell proliferation and angiogenesis, is produced by vascular endothelial cells and appears to be a key proangiogenic factor.5 A recent study found that VEGF-A serum level is positively associated with leptin level in humans with excess body mass and CC genotype of the rs699947 variant of the VEGF gene.6 Moreover, obesity is connected to alterations in mineral levels in the body. Excess body mass is associated with decreased selenium level, which plays an important role in defense against oxidative stress, zinc level, which plays a crucial role in lipid metabolism and glucose homeostasis, and iron level, which is important for hemoglobin synthesis.7,8
Obesity in adults is a multidimensional health issue caused by a complex interaction between modifiable and non-modifiable risk factors, including genetic, metabolic, behavioral, and environmental factors.9,10 Nevertheless, the rapid increase in the incidence of overweight and obesity is primarily due to behavioral and environmental factors.11 Overweight and obesity usually begin in adolescence and young adulthood and continue into middle-aged adulthood.12 Gradual changes in adults’ lifestyles could occur over time that moves mostly toward unhealthy behaviors such as consumption of high-energy foods, lower intake of vegetables and fruits, less engagement in regular physical activities and increased screen times.13 These indications emphasize the importance of implementing effective strategies to combat overweight and obesity associated with aging, including nutrition education promoting healthy lifestyle patterns.14
Saudi Arabia has experienced a rapid socioeconomic change in the recent decades, which has coincided with changes in the incidence of many health problems among Saudis.15 One of the most noteworthy aspects of these changes is the steady rise in overweight and obesity prevalence among the Saudi population of various ages.16 Elevation observed in the prevalence of overweight and obesity in the Saudi community is mainly linked to increasing sedentary behaviors and unhealthy foods consumed in the usual diet.17–20 Furthermore, Saudi Arabia has the world’s second-largest proven oil reserves and is one of the Middle East’s emerging high-income countries. As a result, Saudi Arabia is a popular destination for migrant workers worldwide, especially those from the Middle East, South Asia, and Southeast Asia. In Saudi Arabia, migrants make up more than half of the workforce and the backbone for private-sector jobs.21 According to the fifth Saudi census, non-Saudi residents made up around one-third of the population in Saudi Arabia; about 70% of them were males.22 This is especially intriguing because migrants from various countries allow for a cross-sectional study of differences among them in various areas, including lifestyle preferences and health indicators. Therefore, the current study was conducted to determine differences in overweight and obesity prevalence and associated sociodemographic variables among middle-aged men from twelve Middle Eastern and Asian countries living in Riyadh, Saudi Arabia.
Methods
Study Design and Participants
This study is part of a research project called Relationship between Obesity, physical Activity and Dietary pattern among men living in the Kingdom of Saudi Arabia (ROAD-KSA). It is a cross-sectional study aimed to determine the prevalence of overweight and obesity, physical activity levels, and dietary patterns among young and middle-aged men from twelve Middle Eastern and Asian countries living in Riyadh, Saudi Arabia. The sample size was calculated using a medium effect size of approximately 0.20, with 80% power and a 95% confidence interval. As a result, each subgroup of subjects is required 115 participants to have a total sample size of 1380 participants. Larger sample size was recruited because different groups of researchers were collecting data at different sites concurrently. The study sample was chosen randomly from public places in Riyadh, such as public gardens and shopping centers, using a stratified clustered sampling technique based on geographic locations in Riyadh. The inclusion criteria involved middle-aged men (36–59 years) who live in Riyadh, are physically fit and have a single nationality of one of the following Middle Eastern and Asian countries (Saudi Arabia, Egypt, Yemen, Syria, Jordan, Sudan, Turkey, Pakistan, Afghanistan, India, Bangladesh, and the Philippines). Prior to enrollment, the recruited participants signed an informed consent form written in their native language, as required by the Helsinki Declaration. The research ethics committee at Princess Nourah bint Abdulrahman University in Riyadh, Saudi Arabia, approved the study protocol.
Sociodemographic Data Collection
Face-to-face interviews were used to gather sociodemographic data from study participants, including nationality, age, residency period in Saudi Arabia, household type, marital status, education level, and monthly income.
Anthropometry Data Collection
Standardized procedures were followed to measure study participants’ body weight and height. A calibrated digital weight scale was used to calculate the body weight to the nearest 0.1 kg when wearing minimal clothing and without shoes. Using a calibrated portable stadiometer, the subject’s body height was measured to the nearest 0.1 cm in full standing posture without shoes. The body mass index (BMI) was determined by dividing the weight (kg) by height (m2). Participants were classified based on BMI to underweight (< 18.5), normal weight (18.5–24.9), overweight (25–29.9), or obese (≥30).23
Statistical Analysis
IBM SPSS Statistics for Windows (version 26. Armonk, New York, United States, 2019) was used for data analysis. Categorical variables were analyzed using the Chi-squared test and presented as frequencies and percentages. Post hoc correlations were obtained using the Chi-squared test for different pairs of subgroups (nationalities). Continuous variables were analyzed using a one-way ANOVA test and presented as means and standard deviations. The Tukey post hoc test was used to determine significant differences between subgroups. Univariate and multivariate logistic regression analyses were performed to detect the independent variables related to overweight and obesity risk. Multivariate logistic regression analysis was used after adjusting for the following sociodemographic variables: nationality, age, residency period, household type, marital status, education level, and monthly income. The assumptions of the logistic regression model were evaluated, including linearity. In addition, the logistic regression model was evaluated to observe if interaction or modification of the effect and collinearity can affect the results. All reported P values were made based on two-tailed tests. Differences were considered statistically significant when P values < 0.05.
Results
The current research included 1800 middle-aged men from twelve Middle Eastern and Asian countries living in Riyadh, Saudi Arabia. Table 1 shows the sociodemographic variables and BMI of study participants. The lowest and highest number of subjects by nationality were from the Philippines (n = 71; 3.9%) and Turkey (n = 247; 13.7%). The average age of participants was 40.9 ± 3.8 years, while the average residency period in Saudi Arabia was 13.2 ± 10.6 years. Around one-third of study participants (36.9%) live in their family households, and most of them (88.1%) were married. High education level (college degree or more) and high monthly income (≥ 1000 United States Dollars (USD)) were reported among 34.3% and 44.6% of study participants, respectively. Finally, the mean BMI of all subjects was 26.6 ± 3.6. There were statistically significant differences (P ˂ 0.001) in mean BMI among subjects from different countries (see Figure 1). The mean BMI for Bangladeshi participants (23.9 ± 2.6) was significantly lower than that for the participants from the remaining nationalities. On the other hand, the mean BMI for Pakistani (28.5 ± 5.3), Egyptian (28.4 ± 3.3), and Saudi (28.4 ± 3.6) participants was significantly higher than that for the participants from the remaining nationalities. The mean BMI for Sudanese (26.9 ± 3.0) and Afghan (26.8 ± 4.0) participants was significantly higher than that for the participants from India, the Philippines, and Bangladesh, and significantly lower than that for the participants from Pakistan, Egypt, and Saudi Arabia. The mean BMI for Syrian participants (26.6 ± 3.9) was significantly higher than that for the participants from the Philippines and Bangladesh and significantly lower than that for the participants from Pakistan, Egypt, and Saudi Arabia. The mean BMI for Jordanian (26.3 ± 2.6), Yemeni (26.1 ± 3.4), and Turkish (25.7 ± 2.6) participants was significantly higher than that for the participants from Bangladesh and significantly lower than that for the participants from Pakistan, Egypt, and Saudi Arabia. The mean BMI for Indian participants (25.3 ± 2.8) was significantly higher than that for the participants from Bangladesh and significantly lower than that for the participants from Pakistan, Egypt, Saudi Arabia, Sudan, and Afghanistan. Finally, the mean BMI for Filipino participants (25.2 ± 2.7) was significantly lower than that for the participants from Pakistan, Egypt, Saudi Arabia, Sudan, Afghanistan, and Syria.
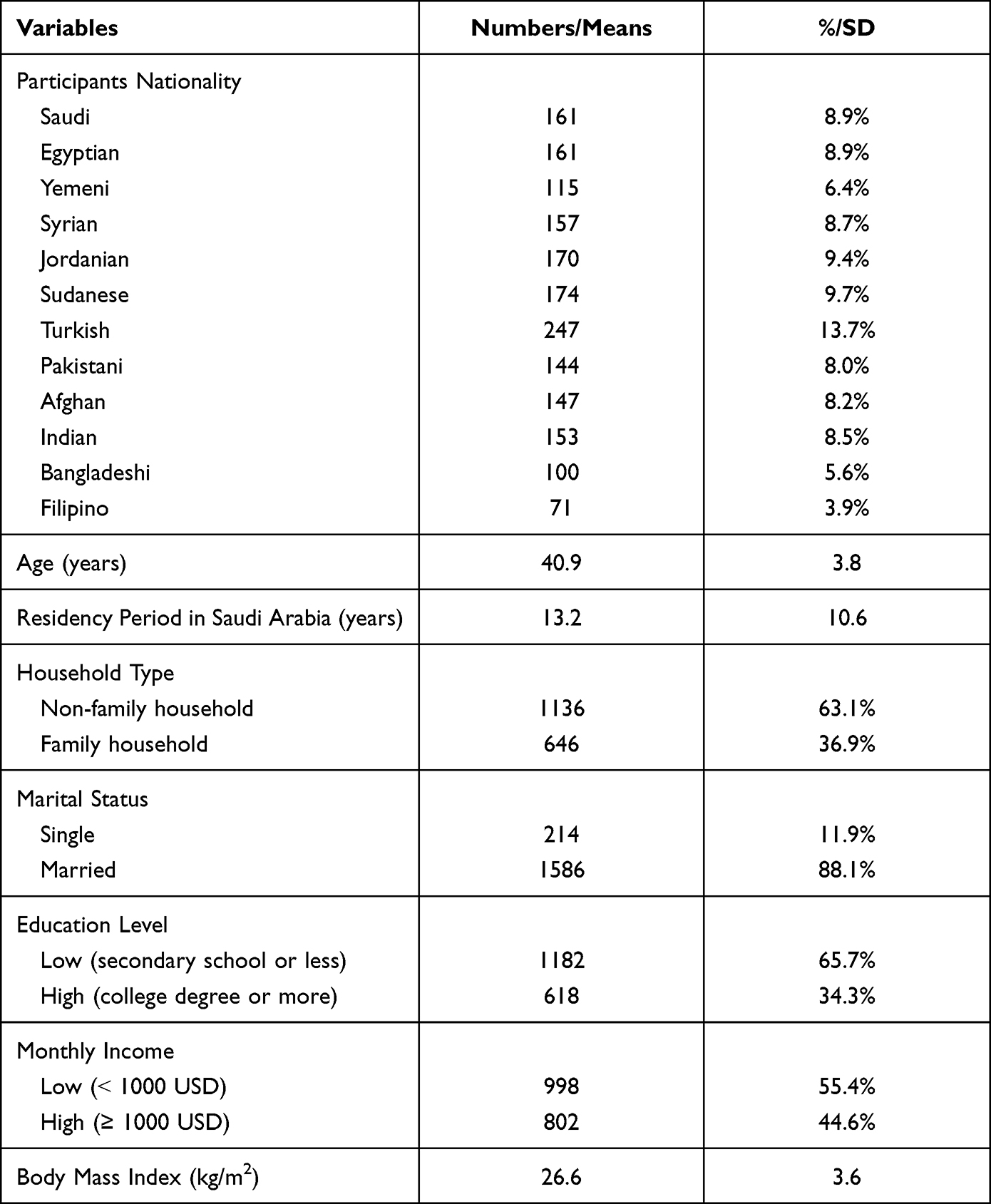 |
Table 1 Sociodemographic Variables and Body Mass Index of Study Participants (n = 1800) |
 |
Figure 1 Bar charts illustrating mean body mass index for study participants from different countries. Means that were labeled with different letters (a, b, c, d, or e) are significantly different at P value ˂ 0.05. |
Overweight and obesity rates among study participants stratified based on their nationality are presented in Table 2. Remarkably, 66.6% of study participants were overweight or obese. By nationalities, the lowest and highest rates of overweight and obesity were reported among subjects from Bangladesh (41.0%) and Saudi Arabia (85.1%), respectively. However, obesity was reported among 14.7% of subjects, whilst by nationalities, the lowest and highest rates of obesity were reported among subjects from Bangladesh (0.0%) and Saudi Arabia (30.4%), respectively. A relatively high rate of obesity was also seen among subjects from Pakistan (29.9%), and Egypt (29.8%). Obesity rates among subjects from the remaining countries (Yemen, Syria, Jordan, Sudan, Turkey, Afghanistan, India and the Philippines) were ranged from 5.2% to 15.6%. There were statistically significant differences (P values ˂ 0.001) in overweight and obesity prevalence among participants with different nationalities. Post hoc correlation coefficients were obtained for different pairs of participants subgroups (different nationalities) and presented in Table 3.
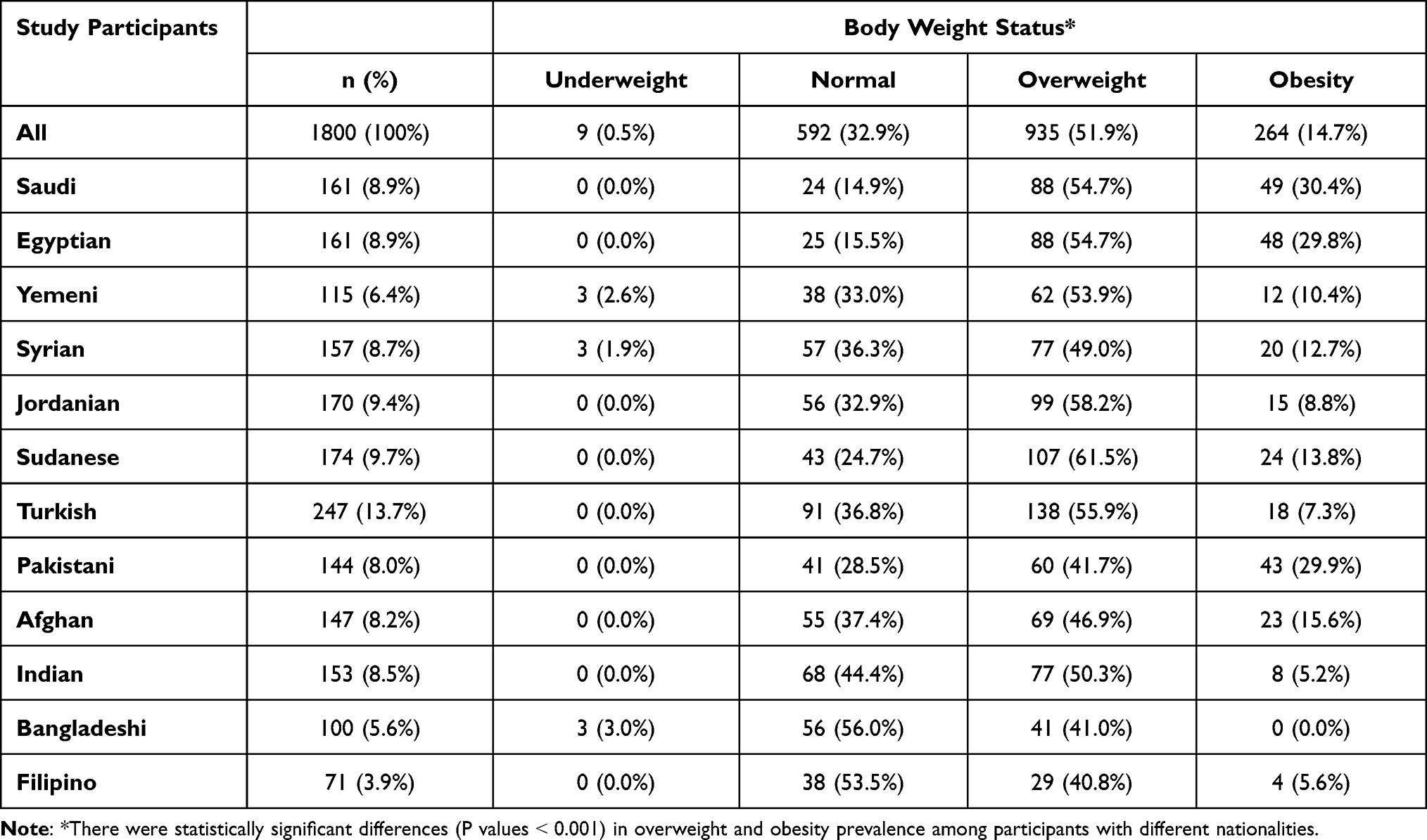 |
Table 2 Overweight and Obesity Prevalence Among Study Participants Stratified Based on Their Nationality |
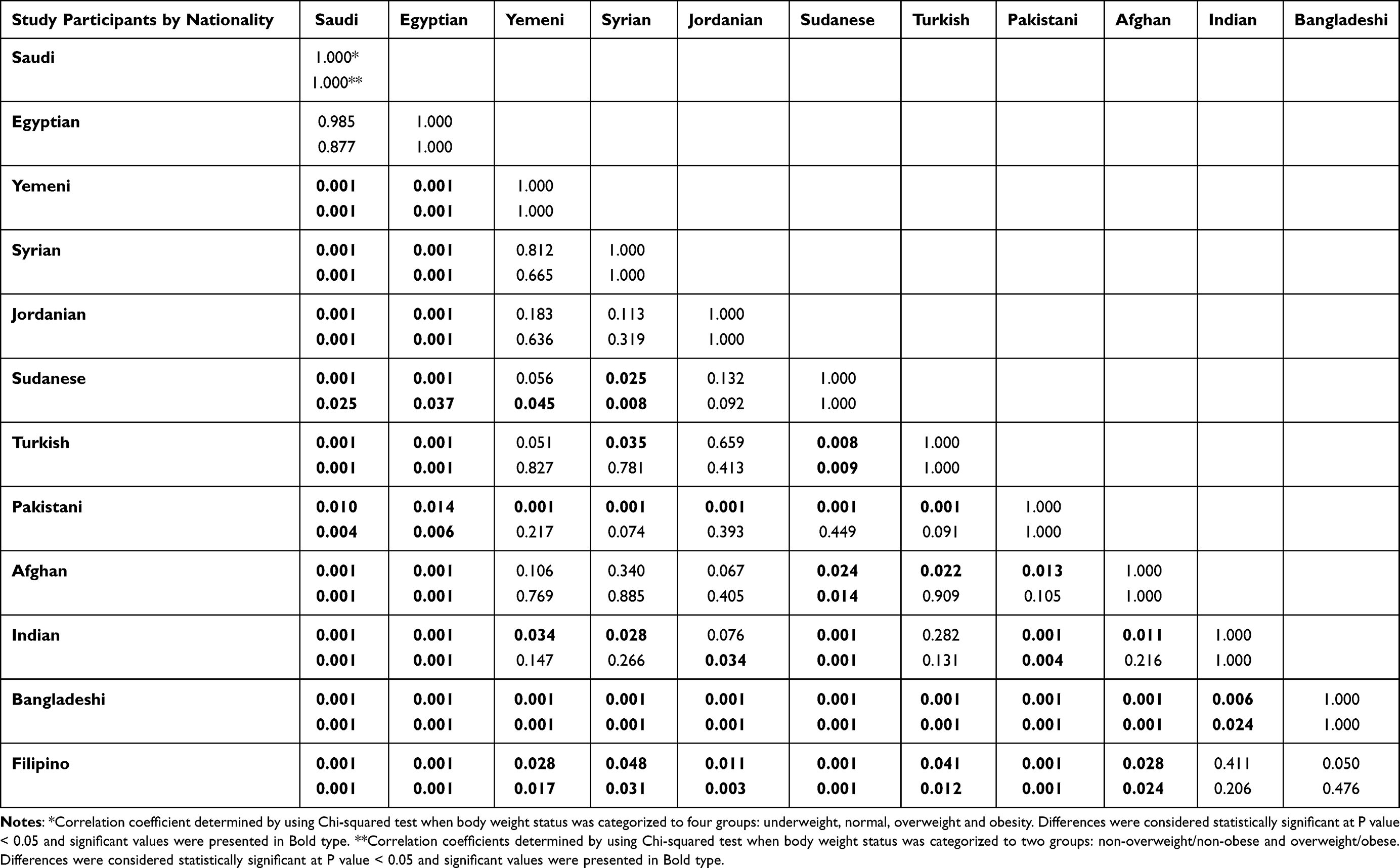 |
Table 3 Correlation Matrix Showing Association Coefficients for Correlation for Overweight and Obesity Prevalence Among Subjects Stratified by Nationality |
The risk of overweight and obesity among study participants for sociodemographic variables is shown in Table 4. Compared with subjects from Bangladesh who have the lowest prevalence of overweight and obesity, participants from other countries except the Philippines had a significantly higher risk of being overweight or obese (adjusted odds ratio [OR] were ranged from 1.78 (for Indian subjects) to 7.08 (for Egyptian subjects), P < 0.05). Older age was significantly associated with a higher risk of overweight and obesity (adjusted OR = 1.05, P = 0.002). A longer residency period in Saudi Arabia was significantly associated with a higher risk of overweight and obesity (adjusted OR = 1.05, P < 0.001). Furthermore, married subjects had a significantly lower risk of overweight and obesity than single subjects (adjusted OR = 0.49, P < 0.001). Finally, participants who had a high monthly income (1000 USD or more) had a significantly higher risk of overweight and obesity than those who earned lower monthly income (adjusted OR = 1.59, P = 0.002). However, the results of multivariate analysis were not significant for two independent variables: household type (adjusted OR = 1.01, P = 0.981) and education level (adjusted OR = 0.86, P = 0.415).
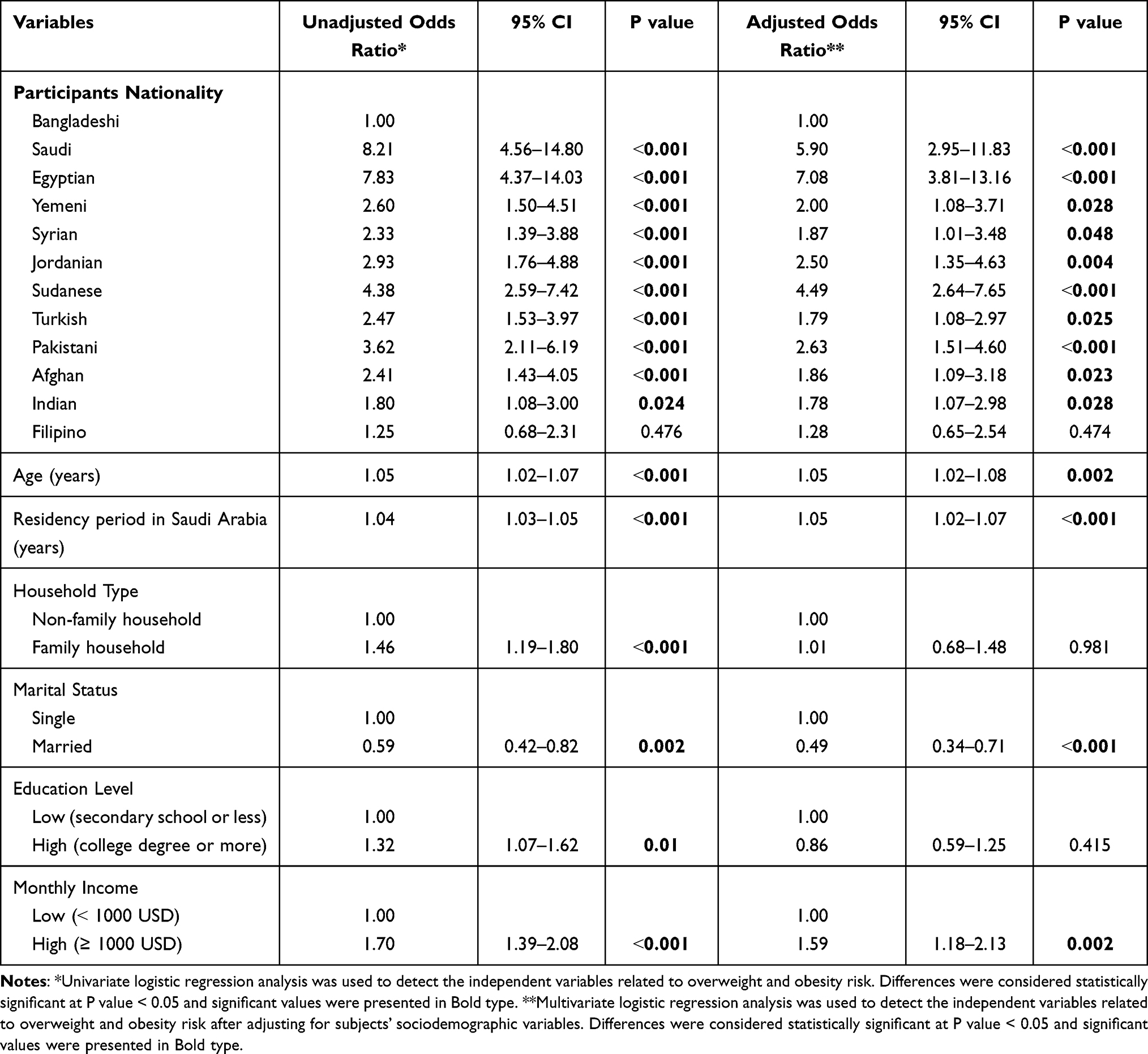 |
Table 4 Risk of Overweight and Obesity Among Study Participants for Sociodemographic Variables |
Discussion
This study investigated differences in the prevalence of overweight and obesity and associated sociodemographic variables in middle-aged men from twelve Middle Eastern and Asian countries living in Saudi Arabia. The findings showed that about two-thirds of the participants were overweight or obese. Saudi Arabia has one of the highest overweight and obesity rates globally.15 A representative national survey revealed that obesity was identified among 28.7% of Saudis aged 15 years and older, 33.5% of women and 24.1% of men.16 According to a recent survey, the national prevalence of obesity in Saudi Arabia among adults aged 18 years and older was 21.7% (17.9% among men and 25.5% among women). Moreover, the obesity rates among Saudi adults in their thirties, forties and fifties were 18.1%, 29.8%, and 32.8%, respectively.24
The current study found significant differences in the prevalence of overweight and obesity in middle-aged men from twelve Middle Eastern and Asian countries living in Saudi Arabia. Certain lifestyle factors, such as typical dietary behaviors, cultural food consumption, and typical physical activity levels, could explain the differences.25,26 For example, Saudi people consume a lot of processed and animal foods at the expense of fruits and vegetables.27 On the other hand, Indians consume excessive cereals and insufficient animal foods.28 Furthermore, the level of physical activity could vary significantly in middle-aged men from different countries.26 For example, most middle-aged Bangladeshi men engage in moderate to vigorous physical activity. For instance, bicycles are often used for short-distance transport by Bangladeshi men. In contrast, a high proportion of Saudi men have low physical activity levels and spend much time doing sedentary activities.26,29
Determining risk factors associated with the prevalence of overweight and obesity among various population subgroups is important for health-promoting actions to reduce their prevalence.30 According to the results of this study, several sociodemographic variables were found to be strongly connected with an increased risk of overweight or obesity. One of these variables was the subjects’ nationality, which might be explained by cross-cultural differences in lifestyles behaviors such as eating habits and physical activity levels among participants from different countries.25,26 Age was also identified in our study results to have a significant association with the risk of overweight and obesity among participants. In general, adults with aging tend to engage in less physical activities and adopt more sedentary lifestyles.26,29,31 Extended residency in Saudi Arabia was linked to a higher risk of being overweight or obese among participants, which could be justified by the urbanization and development commonly seen in Saudi Arabia and their impact on adults’ lifestyle choices.19 Emigrants’ health is expected to worsen with increasing the length of time spent in a new community. Cultural influences, social and economic alterations, and behavior modification connected with migration in terms of diet habits and physical activity may lead to health complications.32,33 Our results showed that single participants have a significantly higher risk of overweight and obesity than married participants. This could be related to the high dependence on out-home foods, especially from fast food restaurants by single men in Saudi Arabia. A high-income level was linked to a higher risk of being overweight or obese among participants. In Saudi Arabia, financially secured men are more likely to work in office professions that require them to sit for long periods and rely on cars for mobility, leading them to be physically inactive.34
Overweight and obesity mostly begin in adolescence and young adulthood and progress into middle-aged adulthood.35,36 Body weight usually increases until around the age of 60 to 65 years, after which it falls in most of the population. Reduced energy expenditure is one factor that may be causing weight gain in middle-aged adults. This could be caused by the drop in resting metabolic rate with aging due to fat-free mass loss and typical physical activity level reduction.12 Another factor contributing to adulthood weight gain is an unhealthy diet that provides high amounts of energy and fats.19 Higher BMI values are linked to higher morbidity and mortality rates in middle-aged men.37,38 Being overweight or obese is associated with an increased risk of cardiovascular disease and diabetes in middle-aged adults.39–41 Obesity is also linked to the onset of depression in middle-aged adults.42 Obesity and its comorbidities management in middle-aged adults are critical for lifelong optimum health.43 A combination of reduced energy intake and regular exercise appears essential to reduce adipose tissue accumulation in the body as adults aging. This possibly could lower the risk of obesity-related metabolic disorders reported in middle-aged adulthood.10,12
According to this study’s findings, there are significant differences in overweight and obesity prevalence among participants with different nationalities. The improvement of community public health contributes significantly to the country’s social, cultural, and economic development. Our study provides valuable outcomes for decision-makers in Saudi Arabia about differences in overweight and obesity incidence among a multiethnic population of middle-aged men and associated factors. The health sector in Saudi Arabia is encouraged to develop strategic policy actions for implementation in the short, medium, and long terms to combat overweight and obesity prevalence in various population subgroups. These policy actions should be adjusted to meet the needs of different population subgroups based on the national context. There were some limitations to this study. The first is the cross-sectional design, which cannot include a cause-and-effect relationship between overweight and obesity and the studied sociodemographic variables. Secondly, this study included only middle-aged men and excluded their counterpart women. Thirdly, this study only included participants living in Riyadh city. However, this study still provides useful information about the prevalence of overweight and obesity and the related sociodemographic variables among middle-aged men in Saudi Arabia from twelve Middle Eastern and Asian countries.
Conclusions
There were relatively high rates of overweight and obesity among middle-aged men from twelve Middle Eastern and Asian countries living in Saudi Arabia. Nationality was a predictor of overweight and obesity. Our findings revealed significant differences in the prevalence of overweight and obesity among participants from different countries. Age, residency period in Saudi Arabia, marital status, and monthly income correlate significantly with the risk of overweight or obesity among the participants.
Abbreviations
BMI, body mass index; OR, odds ratio; VEGF, mitogen vascular endothelial growth factor; USD, United States Dollars.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. If someone wants to request the data from this study, they can contact the corresponding author.
Ethics Approval and Consent to Participate
The study protocol was approved by the research ethics committee at Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The recruited participants were signed an informed consent form written in their native language prior to enrollment, according to Helsinki Declaration (IRB Log Number: 21-0223).
Acknowledgments
The authors would like to thank Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia, for supporting this study through Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R34).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R34), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Jaacks LM, Vandevijvere S, Pan A, et al. The obesity transition: stages of the global epidemic. Lancet Diabetes Endocrinol. 2019;7(3):231–240. doi:10.1016/S2213-8587(19)30026-9
2. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10. doi:10.1016/j.metabol.2018.09.005
3. Gregg EW, Shaw JE. Global health effects of overweight and obesity. N Engl J Med. 2017;377:80–81. doi:10.1056/NEJMe1706095
4. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–298. doi:10.1038/s41574-019-0176-8
5. Skrypnik D, Skrypnik K, Pelczyńska M, et al. The effect of Plantago major supplementation on leptin and VEGF-A serum levels, endothelial dysfunction and angiogenesis in obese women–a randomised trial. Food Funct. 2021;12(4):1708–1718. doi:10.1039/d0fo01878c
6. Skrypnik D, Mostowska A, Jagodziński PP, et al. Association of rs699947 (− 2578 C/A) and rs2010963 (− 634 G/C) single nucleotide polymorphisms of the VEGF Gene, VEGF-A and leptin serum level, and cardiovascular risk in patients with excess body mass: a case–control study. J Clin Med. 2020;9(2):469. doi:10.3390/jcm9020469
7. Banach W, Nitschke K, Krajewska N, et al. The association between excess body mass and disturbances in somatic mineral levels. Int J Mol Sci. 2020;21(19):7306. doi:10.3390/ijms21197306
8. Alshwaiyat NM, Ahmad A, Wan Hassan WMR, Al-Jamal HAN. Association between obesity and iron deficiency (Review). Exp Ther Med. 2021;22(5):1268. doi:10.3892/etm.2021.10703
9. Fruh SM. Obesity: risk factors, complications, and strategies for sustainable long‐term weight management. J Am Assoc Nurse Pract. 2017;29(S1):S3–S14. doi:10.1002/2327-6924.12510
10. Wharton S, Lau DC, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875–E891. doi:10.1503/cmaj.191707
11. Albuquerque D, Nóbrega C, Manco L, Padez C. The contribution of genetics and environment to obesity. Br Med Bull. 2017;123(1):159–173. doi:10.1093/bmb/ldx022
12. Chen RYT, Wittert GA. Obesity in middle-aged men. In: Lunenfeld B, Gooren LJG, Morales A, Morley JE, editors. Textbook of Men’s Health and Aging.
13. Kopp W. How western diet and lifestyle drive the pandemic of obesity and civilization diseases. Diabetes Metabol Syndr Obes. 2019;12:2221. doi:10.2147/DMSO.S216791
14. Wadden TA, Tronieri JS, Butryn ML. Lifestyle modification approaches for the treatment of obesity in adults. Am Psychol. 2020;75(2):235. doi:10.1037/amp0000517
15. DeNicola E, Aburizaiza OS, Siddique A, Khwaja H, Carpenter DO. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. 2015;30(3):191–205. doi:10.1515/reveh-2015-0008
16. Memish ZA, El Bcheraoui C, Tuffaha M, et al. Obesity and associated factors—Kingdom of Saudi Arabia, 2013. Prev Chronic Dis. 2014;11:40236. doi:10.5888/pcd11.140236
17. Al-Rethaiaa AS, Fahmy AEA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutr J. 2010;9(1):39. doi:10.1186/1475-2891-9-39
18. ALFaris NA, Al-Tamimi JZ, Al-Jobair MO, Al-Shwaiyat NM. Trends of fast food consumption among adolescent and young adult Saudi girls living in Riyadh. Food Nutr Res. 2015;59(1):26488. doi:10.3402/fnr.v59.26488
19. AlQuaiz AM, Kazi A, Almigbal TH, AlHazmi AM, Qureshi R, AlHabeeb KM. Factors associated with an unhealthy lifestyle among adults in Riyadh City, Saudi Arabia. Healthcare. 2021;9:2, 221. doi:10.3390/healthcare9020221
20. AlTamimi JZ, Alshwaiyat NM, Alkhalidy H, AlFaris NA, AlKehayez NM, Alagal RI. Breakfast skipping among a multi-ethnic population of young men and relationship with sociodemographic determinants and weight status. Int J Environ Res Public Health. 2022;19:2903. doi:10.3390/ijerph19052903
21. De Bel-Air F. Demography, migration and labour market in Saudi Arabia. Gulf labour markets and migration. European University Institute (EUI) and Gulf Research Center (GRC). GLMM - EN - No. 1/2014; 2014. Available from: https://cadmus.eui.eu/bitstream/handle/1814/32151/GLMM%20ExpNote_01-2014.pdf.
22. General Authority of Statistics of Saudi Arabia. Population by gender, age groups and nationality (Saudi/Non-Saudi), the fifth Saudi census; 2010. Available from: https://www.stats.gov.sa/sites/default/files/ar-census2010-dtl-result_2_1.pdf.
23. World Health Organization. Obesity and Overweight. Geneva: World Health Organization; 2017.
24. Althumiri NA, Basyouni MH, AlMousa N, et al. Obesity in Saudi Arabia in 2020: prevalence, distribution, and its current association with various health conditions. Healthcare. 2021;9:3, 311. doi:10.3390/healthcare9030311
25. AlFaris NA, Alshwaiyat NM, Alkhalidy H, Alagal RI, AlTamimi JZ, AlKehayez NM. Breakfast skipping in a multi-ethnic population of middle-aged men and relationship with sociodemographic variables and weight status. Front Nutr. 2022;8:761383. doi:10.3389/fnut.2021.761383
26. AlFaris NA, Alshwaiyat NM, AlTamimi JZ, Alagal RI, Al-Jamal HA, AlKehayez NM. Physical activity levels of a multi-ethnic population of middle-aged men living in Saudi Arabia and factors associated with physical inactivity. Int J Public Health. 2022;66:1604328. doi:10.3389/ijph.2021.1604328
27. Moradi-Lakeh M, El Bcheraoui C, Afshin A, et al. Diet in Saudi Arabia: findings from a nationally representative survey. Public Health Nutr. 2017;20(6):1075–1081. doi:10.1017/S1368980016003141
28. Sharma M, Kishore A, Roy D, Joshi K. A comparison of the Indian diet with the EAT-Lancet reference diet. BMC Public Health. 2020;20:1–13. doi:10.1186/s12889-020-08951-8
29. AlTamimi JZ, Alagal RI, AlKehayez NM, Alshwaiyat NM, Al-Jamal HA, AlFaris NA. Physical activity levels of a multi-ethnic population of young men living in Saudi Arabia and factors associated with physical inactivity. Front Public Health. 2022;9:734968. doi:10.3389/fpubh.2021.734968
30. World Health Organization. Global Strategy on Diet, Physical Activity and Health. Geneva: World Health Organization; 2004.
31. Caspersen CJ, Pereira MA, Curran KM. Changes in physical activity patterns in the United States, by sex and cross-sectional age. Med Sci Sports Exerc. 2000;32(9):1601–1609. doi:10.1097/00005768-200009000-00013
32. Alzeidan RA, Rabiee-Khan F, Mandil AA, Hersi AS, Ullah AA. Changes in dietary habits and physical activity and status of metabolic syndrome among expatriates in Saudi Arabia. East Mediterr Health J. 2017;23(12):836–844. doi:10.26719/2017.23.12.836
33. Lassetter JH, Callister LC. The impact of migration on the health of voluntary migrants in western societies: a review of the literature. JTranscult Nurs. 2009;20(1):93–104. doi:10.1177/1043659608325841
34. Almuzaini Y, Jradi H. Correlates and levels of physical activity and body mass index among Saudi men working in office-based jobs. J Community Health. 2019;44(4):815–821. doi:10.1007/s10900-019-00639-4
35. Gordon‐Larsen P, The NS, Adair LS. Longitudinal trends in obesity in the United States from adolescence to the third decade of life. Obesity. 2010;18(9):1801–1804. doi:10.1038/oby.2009.451
36. Zajacova A, Burgard SA. Body weight and health from early to mid-adulthood: a longitudinal analysis. J Health Soc Behav. 2010;51(1):92–107. doi:10.1177/0022146509361183
37. Mehta NK, Chang VW. Mortality attributable to obesity among middle-aged adults in the United States. Demography. 2009;46(4):851–872. doi:10.1353/dem.0.0077
38. Wannamethee SG, Shaper AG, Walker M. Overweight and obesity and weight change in middle aged men: impact on cardiovascular disease and diabetes. J Epidemiol Community Health. 2005;59(2):134–139. doi:10.1136/jech.2003.015651
39. Strasser B, Arvandi M, Pasha EP, Haley AP, Stanforth P, Tanaka H. Abdominal obesity is associated with arterial stiffness in middle-aged adults. Nutr Metabol Cardiovasc Dis. 2015;25(5):495–502. doi:10.1016/j.numecd.2015.01.002
40. Lamichhane AP, Couper D, Jenkins GP, Stevens J. Longitudinal associations between body mass index during young adulthood, subsequent weight change, and incident diabetes during mid-and older-adulthood in non-Hispanic White and African American populations: the atherosclerosis risk in communities study. Metab Syndr Relat Disord. 2020;18(7):313–320. doi:10.1089/met.2020.0005
41. Liu M, Zhang Z, Zhou C, et al. Relationship of weight change patterns from young to middle adulthood with incident cardiovascular diseases. J Clin Endocrinol Metab. 2021;106(2):e812–e823. doi:10.1210/clinem/dgaa823
42. Xiang X, An R. Obesity and onset of depression among US middle-aged and older adults. J Psychosom Res. 2015;78(3):242–248. doi:10.1016/j.jpsychores.2014.12.008
43. Näslindh‐Ylispangar A, Sihvonen M, Sarna S, Kekki P. Health status, symptoms and health counselling among middle‐aged men: comparison of men at low and high risk. Scand J Caring Sci. 2008;22(4):529–535. doi:10.1111/j.1471-6712.2007.00565.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.