Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Differences in NAFLD/NASH Management by Provider Specialty: Opportunities for Optimizing Multidisciplinary Care
Authors Porayko MK ![]() , Articolo A, Cerenzia W, Coleman B, Patel D, Stacy S
, Articolo A, Cerenzia W, Coleman B, Patel D, Stacy S
Received 22 April 2022
Accepted for publication 1 July 2022
Published 19 July 2022 Volume 2022:15 Pages 1533—1545
DOI https://doi.org/10.2147/JMDH.S367607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Michael K Porayko,1 Amy Articolo,2 Wendy Cerenzia,3 Brandon Coleman,3 Daxa Patel,2 Sylvie Stacy3
1Division of Gastroenterology, Hepatology and Nutrition, Vanderbilt University Medical Center, Nashville, TN, USA; 2Novo Nordisk, Inc, Plainsboro, NJ, USA; 3CE Outcomes, LLC, Birmingham, AL, USA
Correspondence: Wendy Cerenzia, CE Outcomes, LLC, 2101 Highland Ave S, #300A, Birmingham, AL, 35205, USA, Tel +1 205 259 1519, Fax +1 205 259 1501, Email [email protected]
Purpose: Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are a part of a complex metabolic disease process requiring a multi-faceted and multidisciplinary management approach. This study was conducted to identify areas where medical education across a multidisciplinary team could be optimized in providing optimal care of patients with NAFLD/NASH.
Methods: A survey instrument including a patient case vignette was developed to understand approaches of US clinicians to diagnosis and management of patients with NAFLD/NASH. The survey was fielded via email in December 2020–January 2021. Analysis was conducted using embedded Qualtrics analytic software.
Results: There were 629 survey respondents: 318 PCPs, including physicians, NPs, and PAs, 57 hepatologists, 156 gastroenterologists, and 98 endocrinologists. Survey results demonstrated variation in likelihood to screen patients for NAFLD/NASH among specialists and PCPs as well as in the types of clinicians that respondents would involve in the initial management of a patient diagnosed with NASH. Notably, between 15% and 33% across respondent clinician types would not include any other clinicians or medical specialists in initial management. For a patient with newly diagnosed NASH, the most likely initial management recommendations included drug therapy to improve control of diabetes and therapy to lower lipids and were less likely to recommend drug therapy for weight loss, drug therapy for NASH, or bariatric surgery. Respondents rated “poor patient adherence to lifestyle modifications” and “lack of approved therapies for NASH” as the most significant barriers to optimal management of patients with NASH.
Conclusion: Variation in the evaluation and management of patients with NAFLD/NASH across PCPs and medical subspecialists was identified in this study. Education aimed at multidisciplinary roles in optimally managing patients with NAFLD/NASH, can be beneficial, particularly if focused on increasing screening, implementing guideline updates as they emerge, and incorporating new therapies as they gain approval for clinical practice.
Keywords: continuing medical education, patient care, specialty care, primary care, educational needs
Introduction
Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are a part of a complex metabolic disease process requiring a broad and often multi-faceted management approach involving primary care providers (PCPs) and medical subspecialists (endocrinologists, gastroenterologists, and hepatologists). The estimated prevalence of NAFLD in the United States is reported to be as high as 37%, while a progression to NASH impacts approximately 5% of the population.1,2
Gaps in recognition of NAFLD by clinicians may prevent patients from receiving optimal care. In particular, delays in diagnosis and implementation of appropriate management of NAFLD/NASH can result in progressive liver injury associated with increased morbidity and mortality from the disease.3
Early-stage NAFLD may present without symptoms, requiring a need for heightened awareness among clinicians of the clinical characteristics that may lead to an appropriate diagnosis. The diagnosis is often based on the suspicion of NASH and made through exclusion of alternative etiologies of underlying liver disease and use of noninvasive radiographic imaging techniques. Liver biopsy can be diagnostic, but there has been a growing reluctance by physicians and patients to utilize this invasive method due to the potential risks and the emerging availability of noninvasive diagnostic modalities that can obviate the need for liver biopsy in many instances.4 Furthermore, there is little guidance regarding when liver biopsy is best implemented in the diagnostic algorithm, leading to variation in clinical practice.5 Failure to recognize patients at risk for more severe consequences of fatty liver infiltration, as well as a lack of understanding of the clinical management of these patients, can negatively impact patient health.
Currently, there are no FDA-approved treatments indicated for NAFLD/NASH. While multiple therapies are being investigated in clinical trials, recommended treatment approaches are largely aimed at reducing risks of the disease through lifestyle changes aimed at improving metabolic abnormalities and optimized treatment of blood glucose and lipids.6,7,8
Given the complexities of diagnosis, the need for multidisciplinary expertise in management, and the lack of approved therapeutic options for NAFLD/NASH, the American Gastroenterology Association (AGA) recently published a clinical care pathway for primary care clinicians and specialists with the goal of addressing screening, risk stratification, and management of NAFLD/NASH with an algorithmic care approach.2 While many studies have pointed out gaps in NAFLD/NASH management, we hypothesized that multiple barriers to optimal patient management and multidisciplinary care remain prevalent, leaving areas where medical educational may be beneficial.
Therefore, in order to identify potential areas where medical education could be optimized in the care of patients with NAFLD/NASH, a survey was developed to explore US-practicing clinician approaches to the diagnosis and management of simulated patient case scenarios. These scenarios allowed for the exploration of clinicians’ knowledge of NAFLD/NASH pathophysiology and emerging treatment options, as well as attitudes related to managing patients with NAFLD/NASH. Analysis of the results focused on the identification of key differences between clinicians regarding the understanding and management approaches of patients with NAFLD/NASH.
Methods
Development of Clinician Surveys
This study used a survey containing patient case vignettes, including progression over time, when relevant, to investigate the clinical approach and knowledge of clinicians related to the diagnosis and management of patients with NAFLD/NASH. The clinicians included in the study were comprised of those involved in the care of patients with NASH/NAFLD, including specialists in hepatology, gastroenterology, and endocrinology, and primary care. The survey was developed and underwent pilot testing via cognitive interviews of four clinicians, including two gastroenterologists, one hepatologist, and one primary care physician with experience managing patients with NAFLD/NASH. The pilot testing allowed for the identification of any areas of ambiguity, ensure that all questions were being interpreted as intended and that the survey questions were appropriate to each clinician group included within the survey audience. The survey was built in an online portal (Qualtrics, Provo, UT) for distribution.
Data Collection and Analysis
This case-based study protocol was determined to be exempt from IRB review by Western Institutional Review Board (WIRB, Puyallup, WA) under 45 CFR § 46.104(d)(2) because the research only included interactions involving educational tests, survey procedures, interview procedures, or observations of public behavior. The survey was distributed between December 2020 and January 2021 via an email invitation to US-practicing physicians, nurse practitioners (NPs), and physician assistants (PAs). In order to limit participation bias due to interest in the topic and to avoid skewing initial questions about diagnosis, the invitation did not mention NAFLD or NASH, blinding respondents to the subject matter. Within the study invitation, clinicians were informed that participation was voluntary, and there was no penalty associated with not completing the study. Further, information was provided to clinicians about the purpose of the study and details regarding the anonymity of the data being collected. All respondents provided informed consent electronically by acknowledging this information prior to completing the online survey. A modest monetary incentive (equivalent to 50 USD) was offered to clinicians for their participation, which was expected to take 20-25 minutes to complete. The study was limited to actively practicing clinicians in fields that are involved in the care of patients with NASH/NAFLD, including specialists in hepatology, gastroenterology, and endocrinology, and primary care physicians and advanced practice providers. Data collection was halted when established sample size quotas were reached. All responses were validated for accuracy and thoroughness prior to analysis, which included descriptive statistics using embedded Qualtrics analytic software.
Results
Respondent Demographics
Overall, there were 629 respondents to the survey: 318 PCPs, including physicians, NPs, and PAs, 57 hepatologists, 156 gastroenterologists, and 98 endocrinologists. Full respondent demographics can be found in Table 1. Compared to the other specialty groups, the hepatologist cohort had fewer years in practice, were more often located in urban/academic settings, and saw more patients with NAFLD per month.
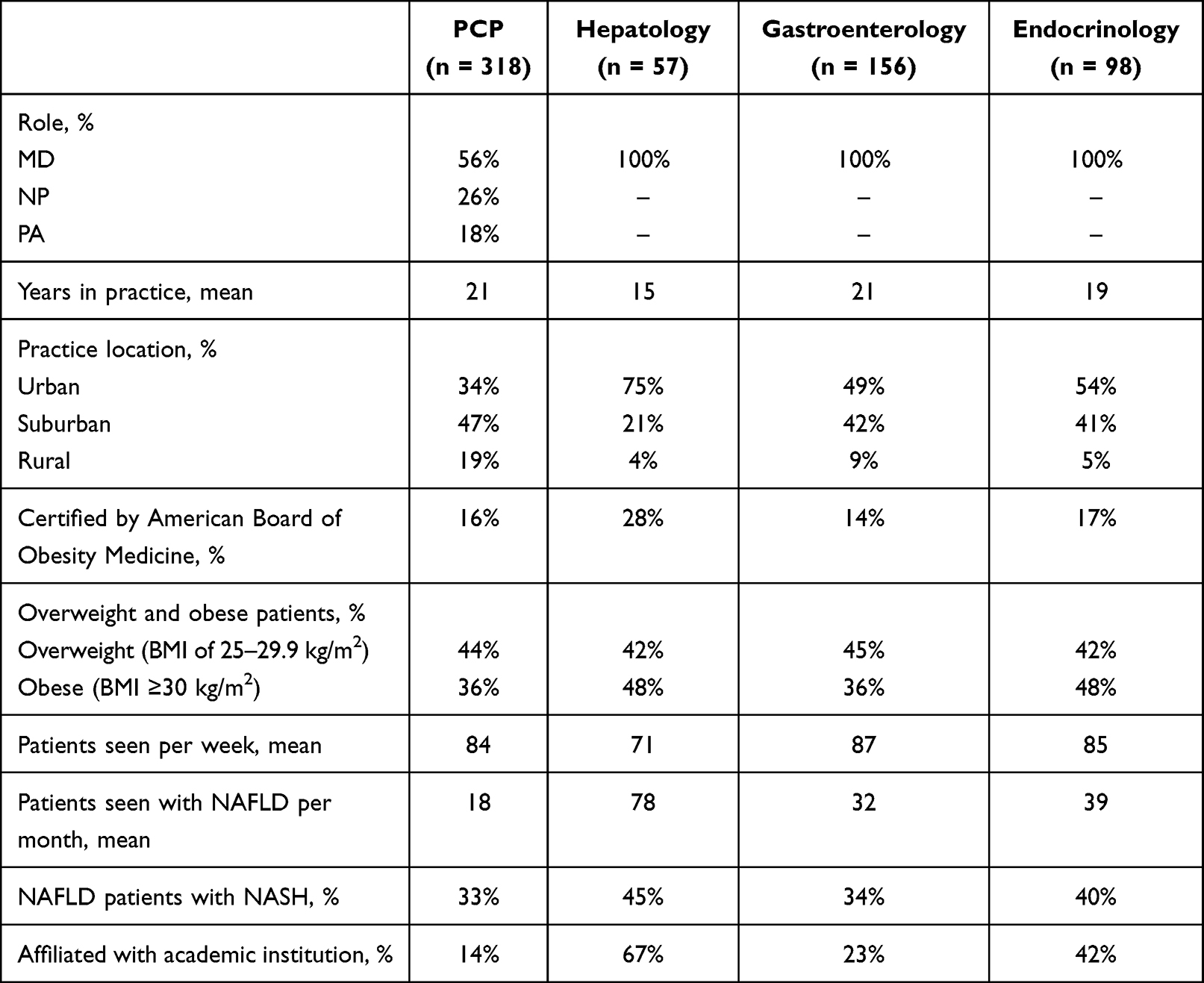 |
Table 1 Clinician Respondent Demographics |
Patient Screening and Evaluation
Respondents were asked to consider their likelihood to screen for NAFLD/NASH in an otherwise healthy 50-year-old man if he presented with various comorbid conditions. Hepatologists were more likely than other clinicians to screen the patient for NAFLD/NASH in the case of presentation with metabolic syndrome, type 2 diabetes mellitus (T2DM), or obesity (Table 2). Primary care clinicians and gastroenterologists had lower likelihood to screen a patient for NASH/NAFLD if the patient presented with T2DM as opposed to if the patient presented with metabolic syndrome or obesity.
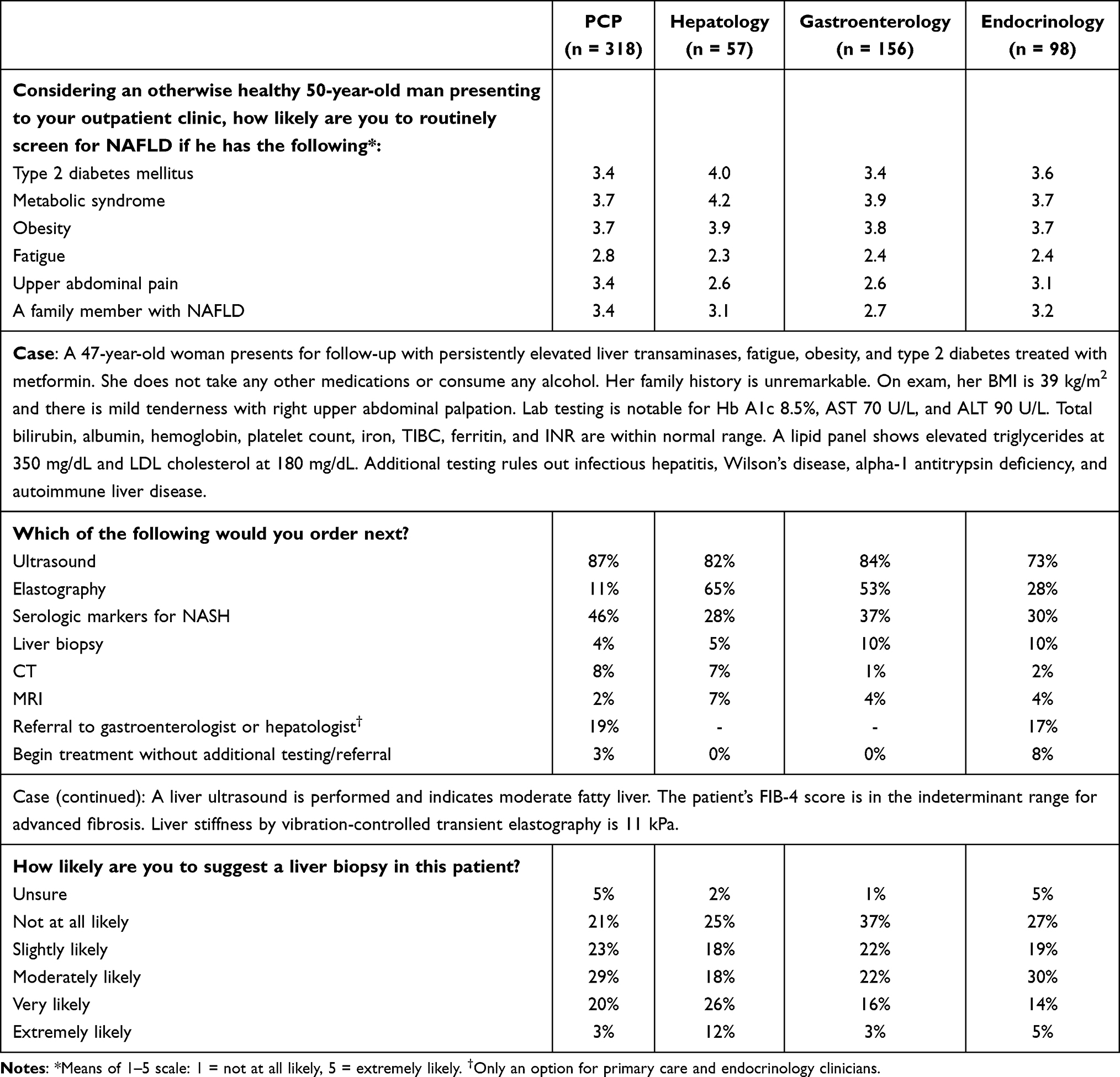 |
Table 2 Patient Screening and Evaluation |
Respondents were presented with a case of a 47-year-old woman with obesity (body mass index (BMI) 39 kg/m2) and T2DM presenting with right upper quadrant tenderness, hemoglobin A1c (Hb A1c) 8.5%, aspartate transaminase (AST) 70 U/L, and alanine aminotransferase (ALT) 90 U/L, and elevated triglycerides. Based on the full case details provided (as shown in Table 2), the majority of respondents (ranging from 83% of PCPs to 98% of endocrinologists) suspected NAFLD/NASH as the most likely cause of the patient’s presentation. Most clinicians indicated that they would order an ultrasound as part of the patient evaluation, but a majority of gastroenterologists and hepatologists recommended elastography as well (Table 2). Only a minority of other clinicians (19% of PCPs and 17% of endocrinologists) would refer to a gastroenterologist or hepatologist for initial evaluation. After being presented with a progression of the case in which a liver ultrasound showed moderate fatty liver and likely fibrosis via elastography, clinicians were mixed in whether they would suggest a liver biopsy. While 38% of the hepatologists would be very or extremely likely to suggest a liver biopsy, 25% of the hepatologists and 37% of the gastroenterologists would not be at all likely to suggest a biopsy. For those who were not at all or only slightly likely to suggest a liver biopsy, the main reasons include a preference to avoid invasive testing and the belief that biopsy results would not alter their management.
Goals and Approach to NASH Management
Respondents were asked to rank five goals to establish their priorities for NAFLD/NASH management of the patient presented in the case, including weight loss, diabetes control, improved lipid profile, halting NASH progression, and symptom improvement. All the specialty groups ranked the goals similarly: the most important goals were weight loss and improving control of diabetes, while symptom improvement was the least important (Table 3).
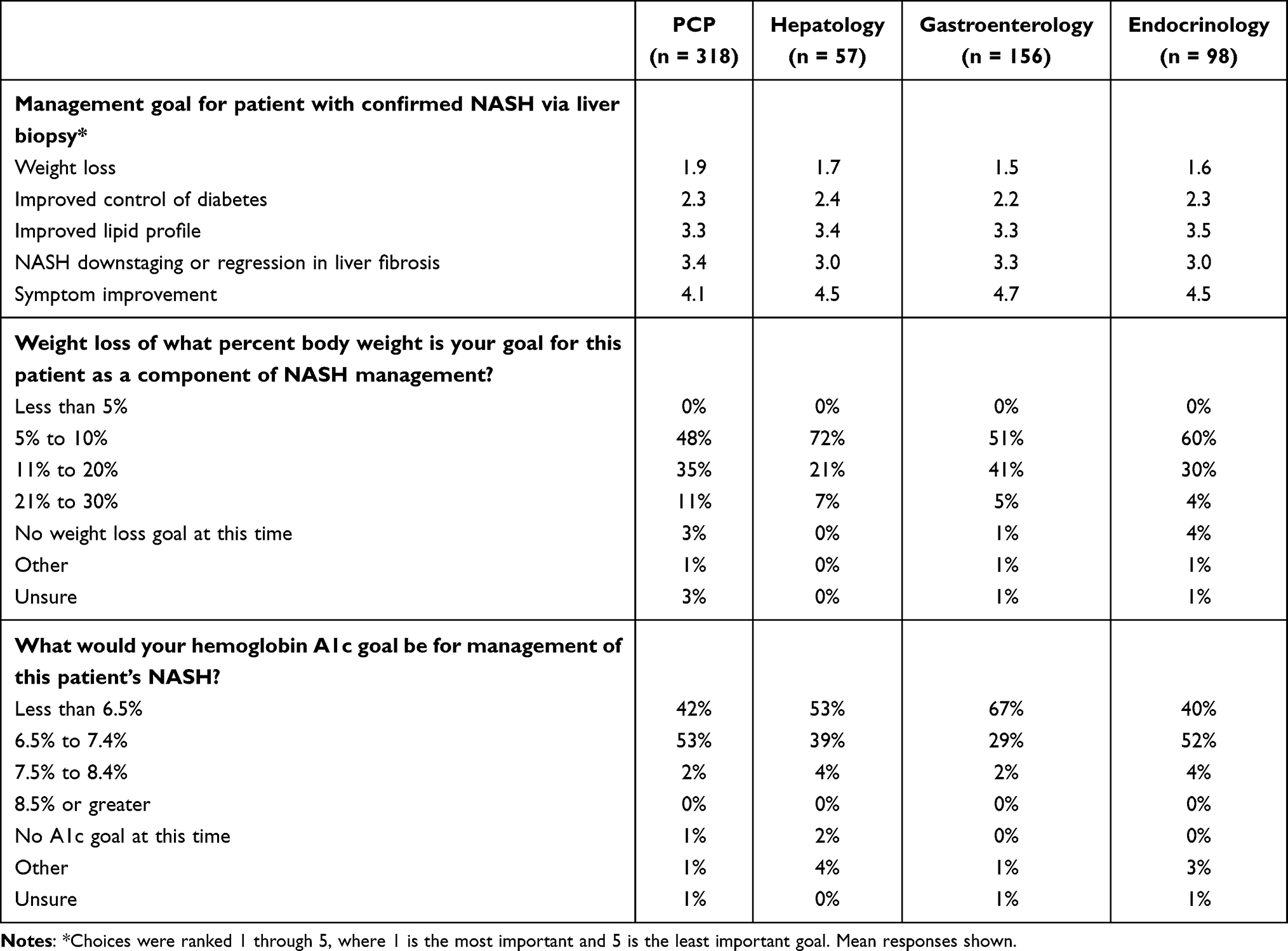 |
Table 3 Management Goals |
Additionally, respondents were asked to select the weight loss and Hb A1c goals that they would have for this patient. Overall, the slight majority of clinicians would target a weight loss goal of 5% to 10% body weight. However, nearly half (46%) of gastroenterologists would set a goal of losing 11% body weight or more. Most hepatologists and gastroenterologists would target an Hb A1c less than 6.5%, while the slight majority of endocrinologists and PCPs targeted between 6.5% and 7.4%.
For a patient with newly diagnosed NASH, respondents were asked to rate their likelihood to recommend drug therapy or bariatric surgery on initial presentation and/or following 12 months of unsuccessful diet and exercise. Respondents were excluded from this analysis if they reported they were “unsure” of their choice or would defer to another specialist for management. The most likely initial management recommendations included drug therapy to improve control of diabetes, with average ratings of 4.1–4.6 on a scale of 1 (not at all likely) to 5 (extremely likely), and lipid lowering, with average ratings of 4.0–4.4 (Table 4). Despite ranking weight loss as a top management goal for this patient, respondents appeared considerably less likely to recommend drug therapy for weight loss, drug therapy for NASH, or bariatric surgery at the initial time point, with average ratings of 2.0 to 2.9 reported. One outlier was endocrinologists, who appeared somewhat more likely to recommend specific drug therapy for weight loss (eg, medications designed to suppress appetite or lower caloric absorption) initially (average rating of 3.4).
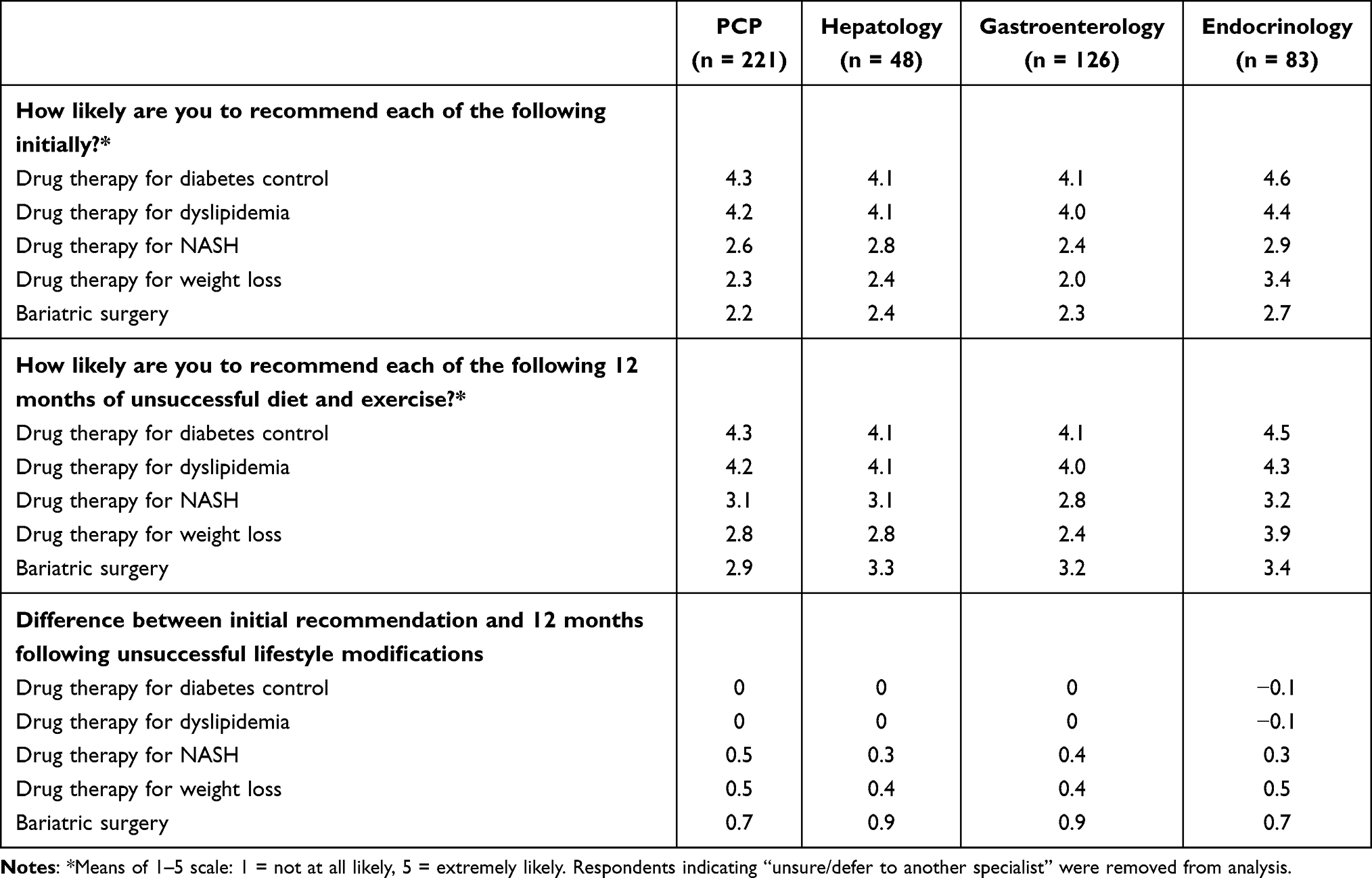 |
Table 4 Management Approach for a Patient with Confirmed NASH via Liver Biopsy |
By contrast, respondents were more likely to recommend drug therapy aimed at lowering hepatic steatosis and/or inflammation, drug therapy for weight loss or bariatric surgery if 12 months of diet and exercise were not successful. In this scenario, average scores for these drug therapies and surgical interventions increased by 0.3 to 0.9 points. Even in the setting of poor responses to diet and exercise, clinicians were still only moderately likely to recommend these treatment options, with ratings ranging from 2.4 (gastroenterologist likelihood to recommend specific drug therapy for weight loss) to 3.4 (endocrinologist likelihood to recommend bariatric surgery). However, endocrinologists’ likelihood to recommend drug therapy for weight loss remained an outlier (average rating of 3.9).
When asked whether they would recommend specific drug therapies or a clinical trial as an initial management approach, endocrinologists were most likely to recommend a glucagon-like peptide-1 (GLP-1) receptor agonist, and PCPs were most likely to recommend a GLP-1 receptor agonist or Omega-3 fatty acids, while hepatologists would be more likely to refer the patient to a clinical trial than opt for other therapeutic options. At the 1-year time point (ie, 12 months of unsuccessful diet and exercise), trends of recommendations for specific therapies for NASH remained similar to what was observed at the initial time point. Endocrinologists were again more likely than other clinicians to recommend a GLP-1 receptor agonist, while hepatologists were more likely to refer the patient to a clinical trial.
Respondents were asked to rate a list of potential barriers to the optimal management of patients with NASH. Poor patient adherence to lifestyle modifications was rated as the most significant barrier, followed by the lack of approved therapies (Table 5). Interestingly, establishing a diagnosis without biopsy was not felt to be a significant barrier, particularly among hepatologists.
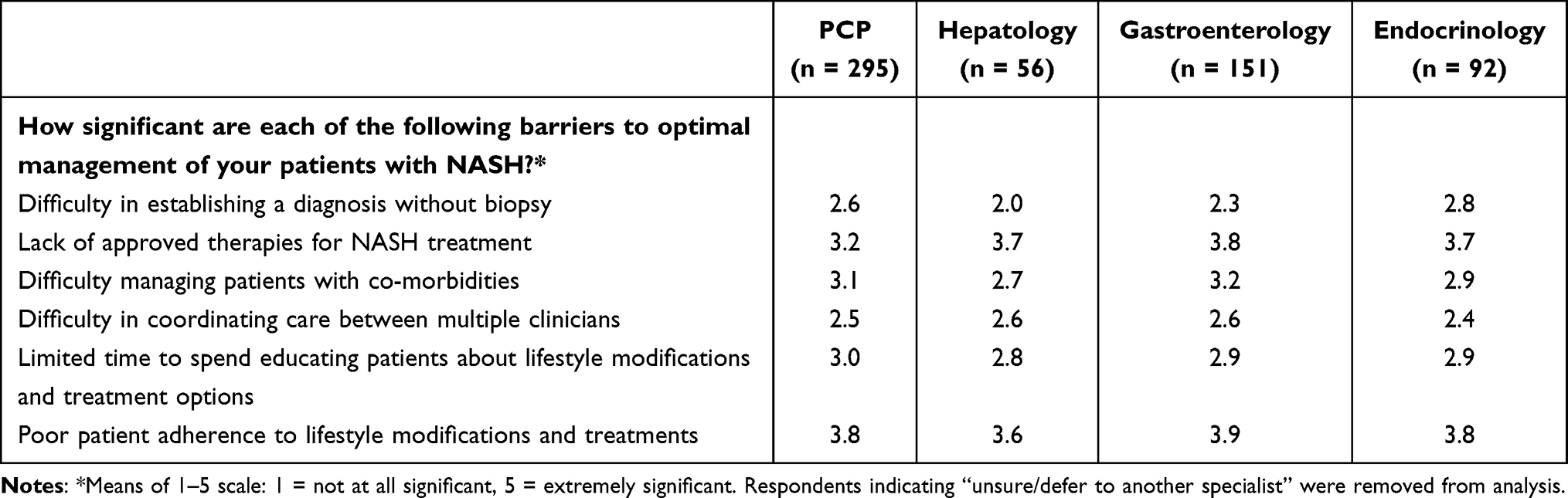 |
Table 5 Barriers to Optimally Managing Patients with NASH |
Multidisciplinary Care
In the survey, variations were seen in the types of clinicians or medical specialists that respondents would involve in the initial management of a patient with a diagnosis of NASH. Between 15% and 33% of the clinicians would not include any other clinicians or medical specialists in initial management (Table 6). Over one-half would involve a dietitian and almost two-thirds of PCPs and endocrinologists would engage a gastroenterologist or hepatologist; about half of hepatologists and a third of gastroenterologists said they would involve a PCP or endocrinologist. More hepatologists would include an obesity specialist or bariatrician in initial management as compared to gastroenterologists, PCPs, or endocrinologists.
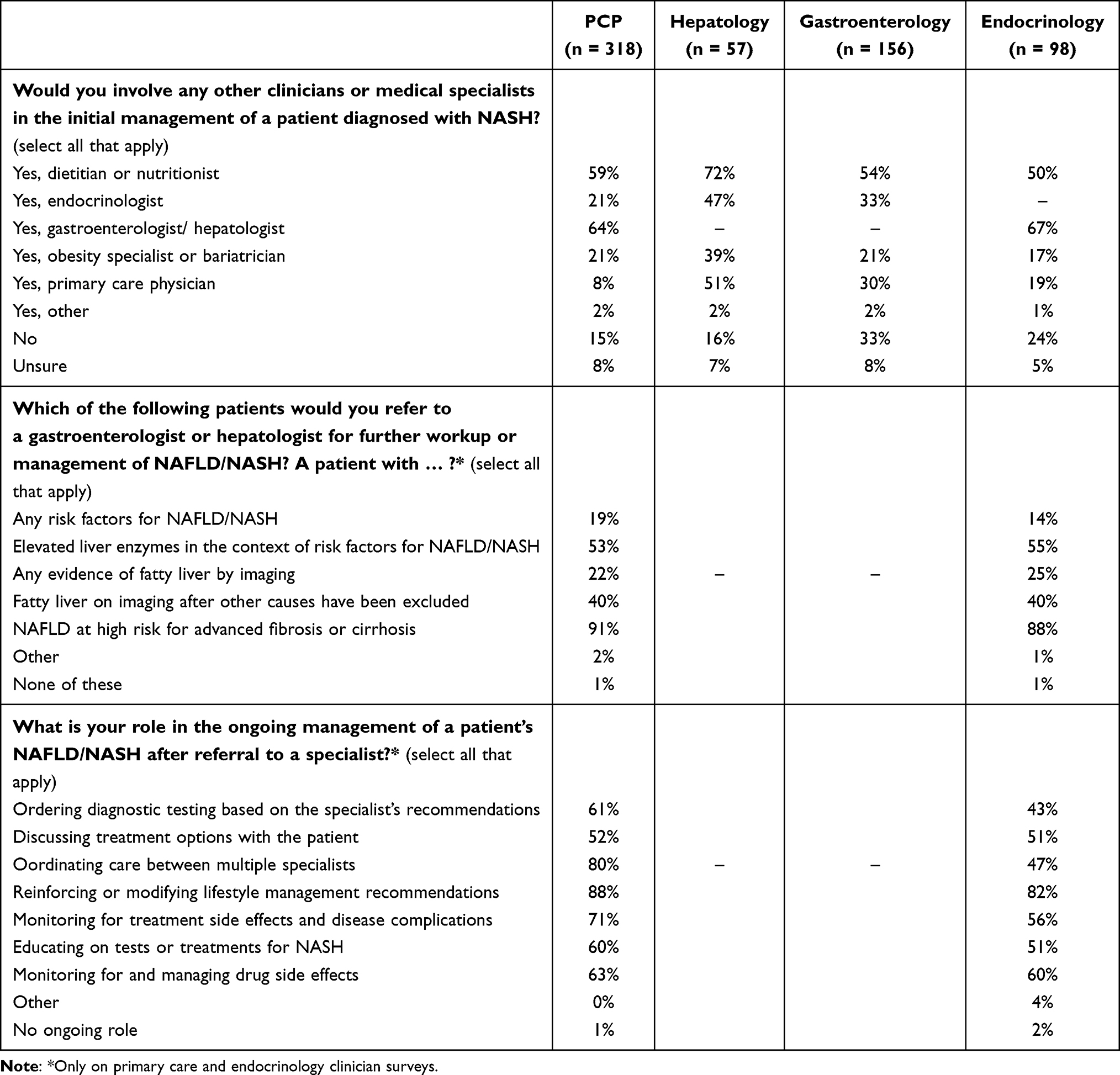 |
Table 6 Multidisciplinary Teams and Referral |
Referral Patterns
Among PCPs and endocrinologists, intent to refer patients to hepatologists or gastroenterologists for further work-up or management of NAFLD/NASH varied according to the patient characteristics and clinical findings. Among PCPs, only 19% said they would refer a patient based on risk factors for NAFLD/NASH, though 53% said they would refer a patient with elevated liver enzymes in the context of risk factors for NAFLD/NASH (Table 6). Only 22% of the respondents said they would refer based on any evidence of fatty liver on imaging, while 40% said they would refer patients with fatty liver based on imaging after other etiologies of underlying liver disease had been excluded. Nearly all (91%) said they would refer patients with NASH felt to be at high risk for advanced fibrosis or cirrhosis.
Primary care providers and endocrinologists reported varied roles in the ongoing management of a patient with NAFLD/NASH after referral to a specialist. The most commonly reported role was reinforcing or modifying lifestyle management recommendations, as reported by PCPs (88%) and endocrinologists (82%) (Table 6). Also, a majority of PCPs also reported that they would be involved in coordinating care between multiple specialists (80%) and in monitoring for treatment side effects and disease complications (71%).
Guideline Use and Utility
Clinical practice guideline use for NAFLD/NASH varied by specialty. Among hepatologists and gastroenterologists, AASLD guidelines were the predominant choice to inform or guide clinician management decisions for patients with suspected or diagnosed NASH (Table 7). Other options, including the EASL-EASD-EASO guidelines, the World Gastroenterology Organization guidelines, payor policies, or guidelines developed by their practice or institution, were reported to be used by fewer clinicians. Nearly one-quarter of PCPs and 33% of the endocrinologists reported not using any guidelines for the management of NASH. The minority of clinicians (24% to 32%) reported that guidelines were “very useful” or “extremely useful” for management of patients with a suspected or confirmed diagnosis of NASH.
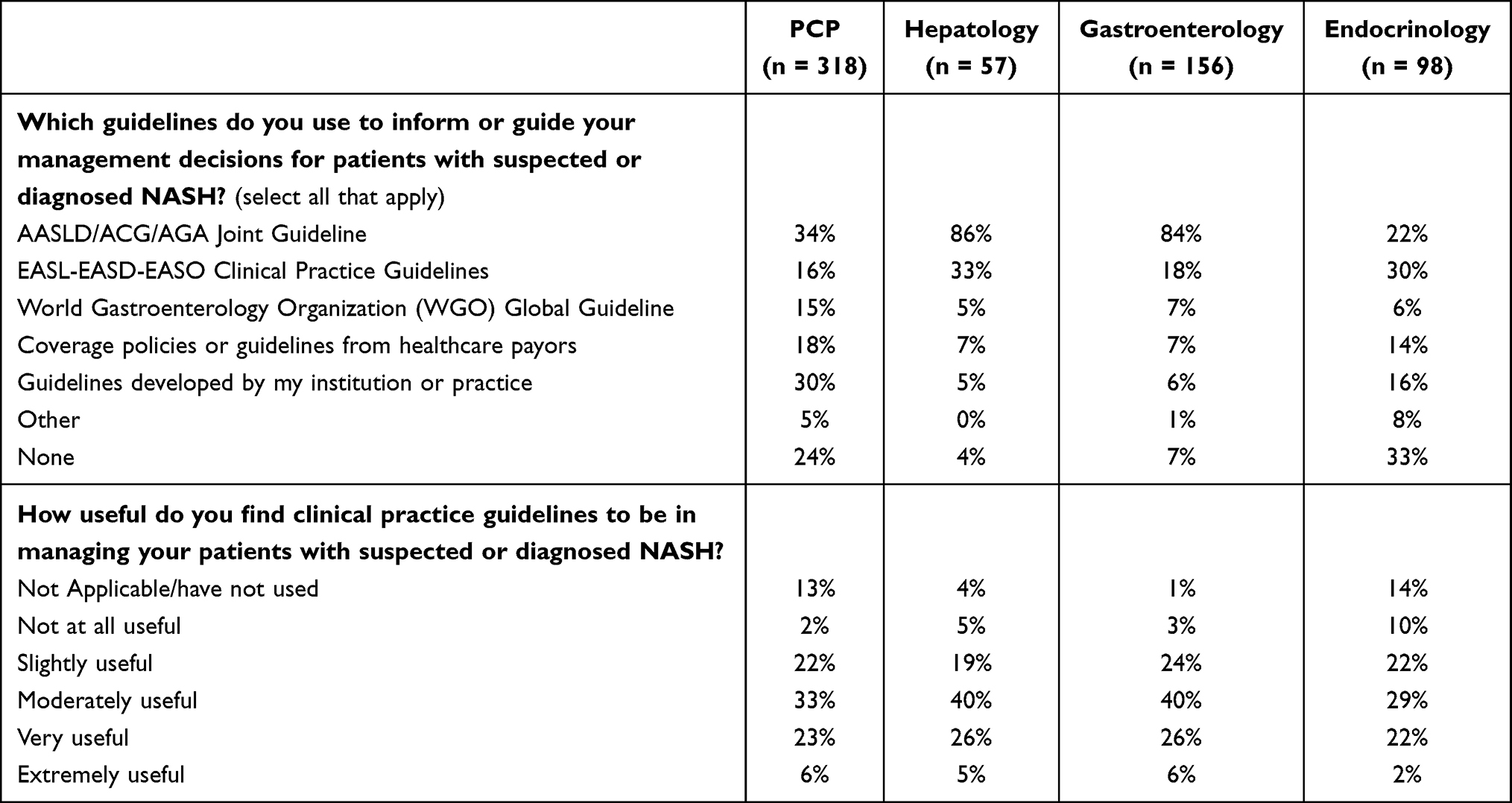 |
Table 7 Guideline Use and Utility |
Clinician Knowledge of Disease Pathophysiology and Emerging Therapies
In the survey, respondents were asked to select the pathophysiological processes of NASH. Most hepatologists, gastroenterologists, and endocrinologists identified insulin resistance, oxidative stress, and proinflammatory cytokine production (Table 8). There is less awareness on the role of impaired GLP-1 secretion, increased glucagon levels, and de novo hepatic lipogenesis in NASH. Nineteen percent of PCPs indicated general uncertainty about the pathophysiology of NASH.
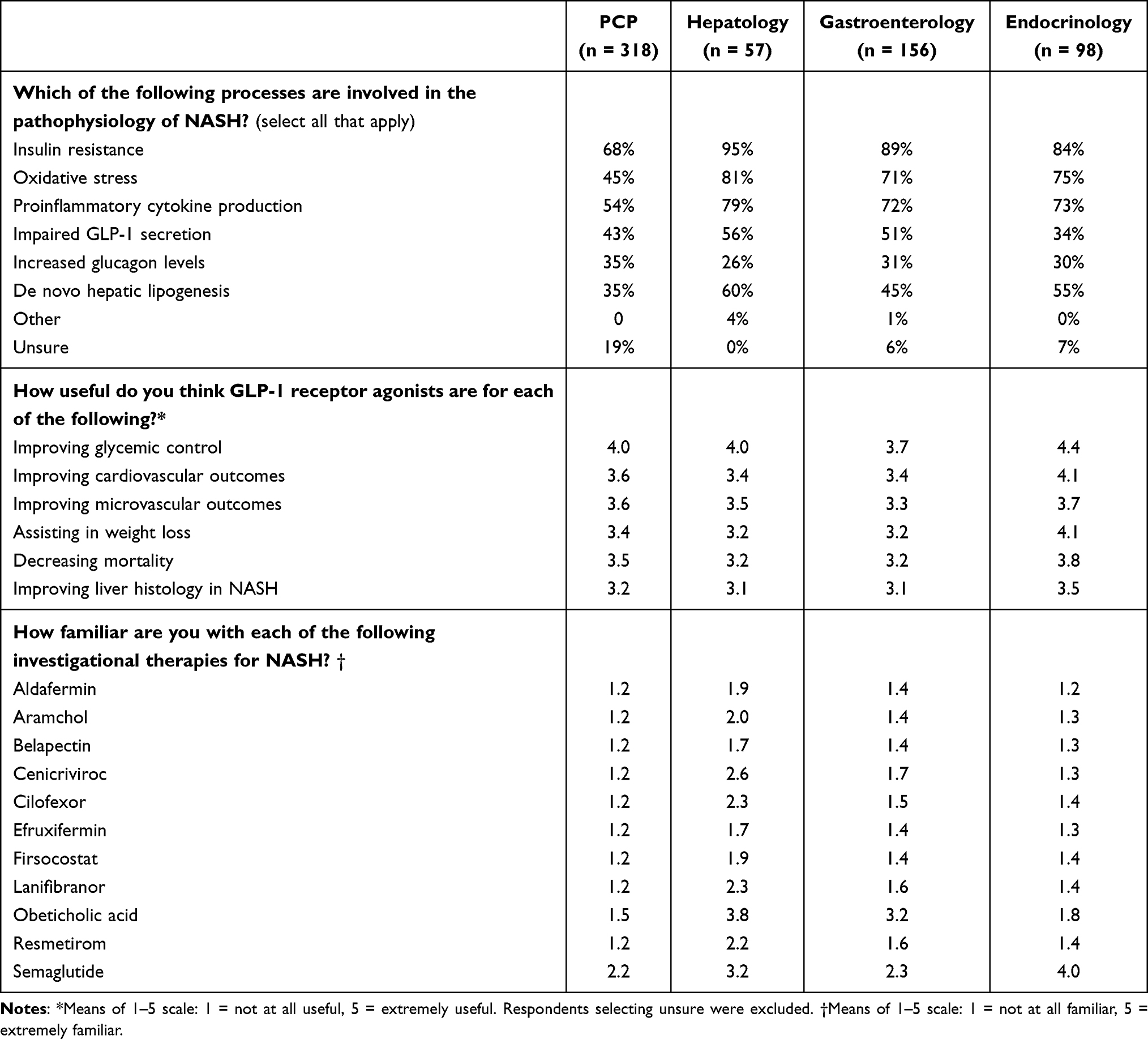 |
Table 8 Clinician Knowledge of Disease Pathophysiology and Emerging Therapies |
Out of the groups surveyed, endocrinologists were the most likely to perceive GLP-1 receptor agonists as useful for a range of effects in patients with NASH. On a scale ranging from 1 (not at all useful) to 5 (extremely useful), endocrinologists rated GLP-1 receptor agonists as very useful in improving glycemic control, with an average score of 4.4, as compared to 4.0 for hepatologists, 4.0 for PCPs, and 3.7 for gastroenterologists. Compared to the other clinician groups, endocrinologists likewise gave these agents higher ratings, on average, with respect to their perceived benefit in improving cardiovascular outcomes, improving microvascular outcomes, assisting in weight loss, decreasing mortality, and improving liver histology in NASH.
Awareness of therapies considered investigational in NASH was generally low across clinician types. When asked to rate their familiarity with specific therapies, PCPs consistently had the lowest ratings across the range of agents (Table 8). By contrast, hepatologists gave themselves the highest ratings for familiarity with almost all investigational therapies in the survey; even so, ratings remained low except for semaglutide (3.2 average rating on a scale of 1 = not at all familiar to 5 = extremely familiar) and obeticholic acid (3.8 average rating). Endocrinologists were most familiar with semaglutide (4.0 average rating), and gastroenterologists were most familiar with obeticholic acid (3.2 average rating).
Discussion
Clinicians demonstrated variation in likelihood to screen patients for NAFLD/NASH. Hepatologists, in particular, were most likely to screen a patient for NAFLD/NASH in the case of either metabolic syndrome, obesity, or T2DM, as compared to other clinicians. Gastroenterologists and PCPs were less likely to screen for fatty liver disease in a patient who presented with T2DM as opposed to if the patient presented with metabolic syndrome or obesity.
This survey identified key differences in NAFLD/NASH knowledge and management across PCPs and medical subspecialists. With estimates indicating that up to 70% of the patients with T2DM have coexistent NAFLD, T2DM must be considered a notable risk factor for the development of NAFLD, triggering appropriate screening for the disorder.2 The survey pointed out that, while most PCPs and endocrinologists perform initial labs and ultrasound, they are less likely than gastroenterologists and hepatologists to order elastography, now considered an important diagnostic technique utilized in the evaluation and staging of NASH.9 Moreover, there are differences across clinicians as to the role of liver biopsy in the diagnostic workup once a liver ultrasound demonstrates characteristics of fatty liver and potential fibrosis. These results are in agreement with previous data that have suggested that PCPs may be less attuned to the diagnostic intricacies of fatty liver disease when compared to subspecialists, potentially delaying diagnosis.10,11
Most PCPs and endocrinologists reported an ongoing role in lifestyle management and coordination of care; however, varying percentages of PCPs and endocrinologists reported involvement in other aspects of care such as ordering tests and monitoring for treatment side effects and disease complications. The PCPs in this study had less familiarity with investigational therapies and a lower awareness of relevant pathophysiological processes than subspecialists. Continued focused educational efforts can heighten PCP awareness of appropriate decision-making strategies regarding screening, implementation of a cost-effective diagnostic work-up, and long-term multidisciplinary management of patients suspected to have NAFLD/NASH, potentially reducing the need for redundant or unnecessary subspecialized care in many instances.
This study demonstrated variation in approaches to inclusion of multidisciplinary care and in the management of patients with NASH across the groups surveyed, demonstrating potential gaps in optimal management. Only one-half of hepatologists and fewer gastroenterologists and endocrinologists indicated they would involve a PCP in initial management of a patient diagnosed with NASH; similar patterns of inclusion of endocrinologists by a gastroenterologist or hepatologist were seen. Many respondents, including almost three-quarters of hepatologists, felt it important to involve a dietitian or nutritionist in the management of their patients with NASH; however, almost one-half of the other respondents did not indicate the inclusion of a dietitian in the initial management of patients with NASH. Similarly, another recent study by Saeed et al, soliciting opinions from 440 primary care providers and referring subspecialists, reported less than half of their respondents saying that they would refer all or most of their NAFLD patients to dietitians. Reasons cited for this lack of referral included cost concerns and lack of patient interest, primarily.12 Altogether, these data suggest a substantial need to improve coordination of care among referring clinicians.
While hepatologists and gastroenterologists appear relatively likely to use the AASLD guidelines to help inform their patient management, 24% of PCPs and 33% of endocrinologists reported not using any guidelines for NAFLD/NASH management. Aspects of the AASLD guidelines are relevant to the practice of PCPs and endocrinologists, including recommendations regarding screening, initial evaluation, and nonpharmacologic interventions. Furthermore, fewer than one-third of the clinicians from each group report finding current guidelines very or extremely useful to their management. When designing education focused on multidisciplinary teams, the use of guidelines as a framework may be advantageous to provide the current perspective on recommendations for care. Once pharmaceutical therapies are approved and as the epidemiology of NAFLD/NASH continues to shift, guidelines are likely to be updated along with the need to adjust clinical relevance.
The results of this study corroborate those of other recent studies, including one survey of NAFLD knowledge and awareness completed by more than 2200 physicians in 40 countries. In that study, the extent of knowledge and approach to diagnostics and management varied considerably by provider type and experience managing patients with NAFLD.13 Although significant knowledge gaps were reported among PCPs, and to a lesser extent endocrinologists, some findings (including variations in screening methods, liver biopsy, and approaches to evaluating alcohol consumption) indicated that education would be beneficial to all provider types studied.13 Furthermore, the results of a needs assessment conducted by the AGA in 2020, composed of 751 physicians, including endocrinologists, gastroenterologists, hepatologists, and PCPs, demonstrated notable gaps in knowledge regarding screening and diagnosis of patients at risk for NAFLD/NASH, and treatment of patients with NAFLD/NASH.14 Primary care knowledge gaps were emphasized in another recent study including a small sample of primary care nurse practitioners (N = 20), of whom only about one-third felt prepared to manage NAFLD.15 Taken together, results of these and other recent studies identify a need for targeted educational interventions that take into account differences in baseline awareness and knowledge of NAFLD among PCPs and subspecialists.
Prior studies have indicated that a multidisciplinary management approach to NAFLD/NASH can lead to improved patient outcomes as well. Referral by PCPs to specialized multidisciplinary clinics has been shown to improve liver- and cardiometabolic-related health parameters and outcomes.16,17 These coordinated multidisciplinary clinics combine risk factor management with up-to-date treatment and monitoring. These types of clinics help organize the roles of each provider to improve efficiency. Unfortunately, many providers involved in NAFLD/NASH management continue to work independently, possibly contributing to and exacerbating many of the management gaps that have been identified.
The AGA recently convened an expert panel tasked to develop a comprehensive and unified strategy aimed at identifying and caring for these complex patients in the hopes that a set of guidelines would improve patient outcomes through a coordinated effort by a variety of health care providers.14 The development of guidelines and other educational tools can support a team-based approach, identifying the potential roles of different specialists to help streamline patient care and improve outcomes.
Limitations
This study relies on the results of a survey including case vignettes to obtain clinician self-reports of awareness, knowledge, and practice, as opposed to a more objective method such as chart review or direct observation of practice. It is worth noting that patient case vignettes have been shown to be a valid and comprehensive method to measure a process of care in actual clinical practice.18,19 Nevertheless, the survey did not present all possible presentations of NAFLD/NASH and did not include an exhaustive list of clinical details that might impact management decisions. Further, while an attempt to limit selection bias was made by blinding respondents to the topic of the study, there may be practice differences between those that chose and did not choose to participate. Lastly, NAFLD/NASH may affect people in underserved communities at higher rates, such as those of Hispanic descent.20,21 This survey did not attempt to discern educational needs related to disparities of care in these populations.
Conclusion
By utilizing a practical questionnaire containing clinical case vignettes, variation in the practice of PCPs, endocrinologists, gastroenterologists, and hepatologists with respect to the evaluation and management of patients with NAFLD/NASH was identified. Recognizing potential gaps in understanding the diagnostic and management principles involved in the day-to-day care of these complex patients can help reduce inefficiencies and negative outcomes. Addressing the specific educational needs and potential barriers limiting optimized care by various health care providers would likely improve the coordinated care of patients with NAFLD/NASH.
Increased screening for early diagnosis, streamlined ongoing patient care, implementation of guideline updates as they emerge, and incorporation of new therapies as they gain approval for clinical practice are a few ways in which optimized patient care can be implemented, reducing morbidity, extending patient survival, and improving quality of life.
As demonstrated in this study, the use of case vignettes can be instructive in identifying the current practice, perceptions and extent of knowledge by various health care providers, but can also act as an educational tool, providing information in a practical way. Identifying and removing potential barriers to the coordinated care of NAFLD/NASH patients, who by the nature of this disorder involve an array of different types of health care providers, will be an important goal for the future. These issues are especially pertinent given the growing prevalence of patients with NAFLD/NASH around the world.
Acknowledgments
The authors would like to thank Andrew D. Bowser, ELS, CHCP, of iconCME in Philadelphia, PA, for providing medical writing support.
Funding
This study was financially supported by Novo Nordisk, Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cotter TG, Rinella M. Nonalcoholic fatty liver disease 2020: the state of the disease. Gastroenterology. 2020;158(7):1851–1864. doi:10.1053/j.gastro.2020.01.052
2. Kanwal F, Shubrook JH, Adams LA, et al. Clinical care pathway for the risk stratification and management of patients with nonalcoholic fatty liver disease. Gastroenterology. 2021;161(5):1657–1669. doi:10.1053/j.gastro.2021.07.049
3. Wieland AC, Quallick M, Truesdale A, Mettler P, Bambha KM. Identifying practice gaps to optimize medical care for patients with nonalcoholic fatty liver disease. Dig Dis Sci. 2013;58(10):2809–2816. doi:10.1007/s10620-013-2740-8
4. Cook N, Geier A, Schmid A, et al. Assessing physician preferences on future therapeutic options and diagnostic practices in non-alcoholic steatohepatitis. JHEP Rep. 2020;2(2):100081. doi:10.1016/j.jhepr.2020.100081
5. Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steatohepatitis: summary of an AASLD single topic conference. Hepatology. 2003;37(5):1202–1219. doi:10.1053/jhep.2003.50193
6. Petersen KF, Dufour S, Befroy D, Lehrke M, Hendler RE, Shulman GI. Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes. 2005;54(3):603–608. doi:10.2337/diabetes.54.3.603
7. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51(1):121–129. doi:10.1002/hep.23276
8. Negi CK, Babica P, Bajard L, Bienertova-Vasku J, Tarantino G. Insights into the molecular targets and emerging pharmacotherapeutic interventions for nonalcoholic fatty liver disease. Metabolism. 2022;126:154925. doi:10.1016/j.metabol.2021.154925 PMID: 34740573.
9. Balakrishnan M, Loomba R. The role of noninvasive tests for differentiating NASH from NAFL and diagnosing advanced fibrosis among patients with NAFLD. J Clin Gastroenterol. 2020;54(2):107–113. doi:10.1097/MCG.0000000000001284
10. Blais P, Husain N, Kramer JR, Kowalkowski M, El-Serag H, Kanwal F. Nonalcoholic fatty liver disease is underrecognized in the primary care setting. Am J Gastroenterol. 2015;110(1):10–14. doi:10.1038/ajg.2014.134
11. Polanco-Briceno S, Glass D, Stuntz M, Caze A. Awareness of nonalcoholic steatohepatitis and associated practice patterns of primary care physicians and specialists. BMC Res Notes. 2016;9:157. doi:10.1186/s13104-016-1946-1
12. Saeed N, Glass LM, Habbal H, et al. Primary care and referring physician perspectives on non-alcoholic fatty liver disease management: a nationwide survey. Therap Adv Gastroenterol. 2021;14:17562848211042200. doi:10.1177/17562848211042200
13. Younossi ZM, Ong JP, Takahashi H, et al. A global survey of physicians knowledge about nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2021;20:e1456–e1468.
14. Kanwal F, Shubrook JH, Younossi Z, et al. Preparing for the NASH epidemic: a call to action. Metabolism. 2021;122:154822. doi:10.1016/j.metabol.2021.154822
15. Casler K, Trees K, Bosak K. Providing care for fatty liver disease patients: primary care nurse practitioners’ knowledge, actions, and preparedness. Gastroenterol Nurs. 2020;43(5):E184–E189. doi:10.1097/SGA.0000000000000487
16. Cobbold JFL, Raveendran S, Peake CM, Anstee QM, Yee MS, Thursz MR. Piloting a multidisciplinary clinic for the management of non-alcoholic fatty liver disease: initial 5-year experience. Frontline Gastroenterol. 2013;4(4):263–269. doi:10.1136/flgastro-2013-100319
17. Moolla A, Motohashi K, Marjot T, et al. A multidisciplinary approach to the management of NAFLD is associated with improvement in markers of liver and cardio-metabolic health. Frontline Gastroenterol. 2019;10(4):337–346. doi:10.1136/flgastro-2018-101155
18. Peabody JW, Luck J, Glassman P, et al. Measuring the quality of physician practice by using clinical vignettes: a prospective validation study. Ann Intern Med. 2004;141(10):771–780. doi:10.7326/0003-4819-141-10-200411160-00008
19. Luck J, Peabody JW, Lewis BL. An automated scoring algorithm for computerized clinical vignettes: evaluating physician performance against explicit quality criteria. Int J Med Inform. 2006;75(10–11):701–707. doi:10.1016/j.ijmedinf.2005.10.005
20. Patel P, Muller C, Paul S. Racial disparities in nonalcoholic fatty liver disease clinical trial enrollment: a systematic review and meta-analysis. World J Hepatol. 2020;12(8):506–518. doi:10.4254/wjh.v12.i8.506
21. Rich NE, Oji S, Mufti AR, et al. Racial and ethnic disparities in nonalcoholic fatty liver disease prevalence, severity, and outcomes in the United States: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(2):198–210.e2. doi:10.1016/j.cgh.2017.09.041
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.