Back to Journals » Nutrition and Dietary Supplements » Volume 18
Dietary Salt Consumption and Behavioral Predictors Among Adults in Afghanistan: Analysis of the WHO STEPS Survey
Authors Noormal AS ![]() , Noormal ASh, El Hajj Hassan O
, Noormal ASh, El Hajj Hassan O ![]() , Dambach P
, Dambach P
Received 11 March 2026
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:18 608430
DOI https://doi.org/10.2147/NDS.S608430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ara Kirakosyan
Ahmad Siyar Noormal,1,2 Ajmal Shekeb Noormal,3 Ola El Hajj Hassan,2 Peter Dambach2
1Department of Public Health, Afghan International Islamic University, Kabul, Afghanistan; 2Heidelberg Institute of Global Health, University Hospital Heidelberg, Heidelberg, Germany; 3School of Life Sciences, University of Essex, Colchester, UK
Correspondence: Ahmad Siyar Noormal, Email [email protected]
Background: Excess dietary salt intake is a major modifiable risk factor for hypertension and cardiovascular disease, yet nationally representative data from Afghanistan are limited. This study estimated the prevalence of high salt intake and identified associated behavioral and sociodemographic determinants among Afghan adults.
Methods: We analyzed data from the 2018 Afghanistan WHO STEPwise survey, a nationally representative cross-sectional household survey of adults aged 18– 69 years (n = 3,955). High salt intake was defined based on self-perceived consumption. Survey-weighted descriptive statistics, Rao–Scott chi-square tests, and logistic regression models were used to examine associations between participant characteristics and high salt intake. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported.
Results: Overall, 15.1% (95% CI: 12.7– 17.8) of participants reported high salt intake. Behavioral factors showed the strongest associations. Adding salt at the table (AOR 2.61, 95% CI 1.56– 4.37), frequent consumption of processed foods (AOR 3.60, 95% CI 2.15– 6.02), and eating meals outside the home 1– 2 times per week (AOR 1.68, 95% CI 1.00– 2.84) were independently associated with higher odds of high salt intake. Awareness of salt-related health harms was protective (AOR 0.42, 95% CI 0.26– 0.67). Most sociodemographic factors, including sex, age, education, wealth, and residence, were not significantly associated, although regional differences were observed.
Conclusion: High salt intake in Afghanistan appears to be primarily determined by modifiable food behaviors rather than demographic characteristics. Population-level strategies, including reducing discretionary salt use, improving food environments, reformulating processed foods, and strengthening public awareness, may be effective approaches for lowering salt consumption and preventing non-communicable diseases.
Plain Language Summary: Excess salt consumption is a major risk factor for high blood pressure, heart disease, and other non-communicable diseases. Reducing salt intake is therefore an important public health strategy worldwide. However, little is known about how adults in Afghanistan perceive their own salt consumption and which groups may be more likely to report high intake.
In this study, we analyzed data from the World Health Organization’s STEPwise survey, a nationally representative survey of adults in Afghanistan. The aim was to examine how many adults believe they consume too much salt and to identify factors associated with self-reported high salt intake.
We found that about one in seven adults reported consuming a high amount of salt. Men, younger adults, and people who frequently ate meals outside the home were more likely to report higher salt intake. However, previous reports suggest that actual salt consumption in Afghanistan is much higher than what people report. This indicates that many individuals may underestimate how much salt they consume.
These findings highlight an important awareness gap. Public health programs in Afghanistan should strengthen education on the health risks of high salt intake and promote strategies to reduce salt consumption at both household and community levels.
Keywords: salt intake, sodium, dietary behavior, WHO STEPS, Afghanistan, non-communicable diseases
Introduction
Dietary salt (sodium chloride) is an essential nutrient required for maintaining extracellular fluid balance, nerve transmission, and cellular homeostasis. However, regular sodium intake in most populations has been significantly higher than physiological needs and public health recommendations. The World Health Organization (WHO) recommends that adults consume less than 2,000 mg of sodium per day (approximately 5 g of salt) to reduce the risk of elevated blood pressure and associated cardiovascular outcomes. Despite this guidance, the Global Burden of Disease (GBD) 2021 analysis estimated mean global sodium intake at approximately 4,310 mg/day (≈10.8 g salt/day), more than double the recommended limit.1
This excessive salt consumption represents one of the significant dietary risk factors for non-communicable diseases (NCDs) worldwide. It is estimated that 1.89 million deaths per year are attributable to high sodium intake, which is a proven risk factor for hypertension and cardiovascular disease.2,3 Excess dietary sodium has been causally linked to hypertension, stroke, ischemic heart disease, gastric cancer, chronic kidney disease, and atrial fibrillation, and aortic aneurysm.1,2,4,5 In 2021, the age-standardized mortality rate and disability-adjusted life-year (DALY) rate attributable to high sodium intake were 20.4 and 437.7 per 100,000 population, respectively, underscoring the substantial population-level health burden.3 The highest mortality and DALY rates are found in Southeast Asia, East Asia, and Oceania, and in Central and Eastern Europe and Central Asia, which are significantly higher than the global average.3
Although salt reduction has been recognized as a cost-effective public health strategy, intake remains above recommended levels across both high- and low-income settings. United States national survey indicate mean sodium intake of approximately 3,400 mg/day (≈8.5 g salt/day), with only 20.9% of adults meeting the <2,300 mg guideline.6 Similarly, salt intake in Europe remains high with Western European countries exceeding the recommended levels. A WHO review found that 98% of European countries exceed the 5 g salt/day target, with reported daily intakes ranging from 5.39 to 18.51 g/day among men and 4.27 to 16.14 g/day among women.7
The burden is particularly pronounced in low- and middle-income countries (LMICs), where rapid nutrition transitions, increasing reliance on processed foods, and limited prevention programs contribute to persistently high salt consumption. A systematic review showed that the mean salt intake in South Asian countries is approximately twice compared to the WHO recommended intake level.8 Another scoping review conducted in 2023 revealed that in South Asia, population-level salt intake ranges from 6.7 to 13.3 g/day, which is much higher than the recommended level of 5g/day.9 In Iran, nationally representative data from 2021 demonstrate a mean salt intake of 9.71 g/day, with 97.98% of adults exceeding the recommended threshold.10 These high intake patterns are closely linked to rising hypertension and cardiovascular disease burdens across LMICs, where healthcare systems face additional challenges in managing NCDs.11
Afghanistan represents a particularly under-researched context within this global landscape. The 2018 Afghanistan WHO STEPS survey provided the first nationally representative estimate of salt intake in the country, revealing an average consumption of 12.1 g/day.9 However, beyond these estimates of overall intake little is known about the distribution of high salt consumption or the behavioral and sociodemographic factors that may influence excessive intake. Public health surveillance and research in Afghanistan have historically been limited by prolonged conflict, fragile health infrastructure, and resource constraints, resulting in important evidence gaps to inform prevention strategies.12–14 The country faces a triple burden of disease, with NCDs accounting for approximately half of all deaths and health financing heavily dependent on out-of-pocket payments.14
Although prior research in Afghanistan has documented high average salt intake, mean population estimates provide limited guidance for intervention planning. Population averages mask substantial heterogeneity across sociodemographic groups and do not identify the behavioral practices that contribute most to excessive consumption. Effective salt reduction strategies require an understanding of who is at highest risk and which modifiable behaviors drive intake. In fragile and resource-constrained settings, where prevention resources are limited, such evidence is essential to prioritize high-risk groups and inform targeted, culturally appropriate public health policies. Generating this information is particularly important in Afghanistan, where the burden of hypertension and cardiovascular disease is rising but actionable dietary surveillance data remain scarce.
Given this substantial knowledge gap regarding behavioral determinants of sodium consumption in this under-researched setting, this study aims to:1 estimate the prevalence of self-reported high salt intake among Afghan adults,2 describe salt-related dietary behaviors; and3 identify sociodemographic and behavioral factors independently associated with high salt consumption. Understanding these determinants is essential for developing targeted, culturally appropriate salt reduction interventions that can address the growing burden of hypertension and cardiovascular disease in Afghanistan.
Methodology
Study Design and Sampling
Data from Afghanistan WHO STEPS survey 2018 were used to conduct this analysis. This was a nationally representative cross-sectional survey which targeted permanent residents aged 18–69 years from selected households who consented to participate. Temporary residents (residents for less than 12 weeks) and those who were beyond the age limit (18–69 years) were excluded. The survey employed a multistage cluster sampling method to ensure national representativeness. The sample size for this study was defined as 3972 household members across 50 randomly selected districts in 6 zones of Afghanistan; however, data was collected from 3955 participants. Data collection followed the WHO STEPwise approach to surveillance (STEPS), using a previously published and validated questionnaire. Detailed demographic and behavioral information were collected through structured interviews, followed by physical measurements including weight, height, waist circumference, and blood pressure. Fasting blood samples were collected for biochemical measurements. Additional details are available elsewhere.15 To ensure the representativeness of the data, sample and non-response weights were applied.
Measurement of Variables
Outcome Variable
The primary outcome for this analysis was high salt intake, which was defined using the question “How much salt do you consume?”, and responses of “far too much” or “too much” were classified as high salt intake, while all other responses were categorized as not high. This measure reflects perceived salt intake rather than objective sodium consumption.
Although the Afghanistan STEPS survey included biomarker data on urinary sodium and creatinine for a subsample of participants, these measurements were available only for approximately 12% of the total sample. Given the substantial proportion of missing biomarker data and the risk of reduced representativeness, these data were not used for primary outcome estimation in this study. Instead, we used the self-reported dietary salt intake variable, which was available for the full nationally representative sample.
Covariables
Independent variables were grouped into sociodemographic, behavioral, and knowledge-related factors. Sociodemographic variables included sex, age group, education, wealth, place of residence, and region. Behavioral variables included adding salt just before eating, adding salt before cooking, processed food consumption, and frequency of meals eaten outside the home. Knowledge-related variables included awareness of salt-related health harms and perceived importance of salt reduction.
Adding salt before eating or during cooking was considered habitual if participants reported always or often engaging in these behaviors. Frequent consumption of processed foods high in salt was defined as always or often consuming such foods. Perceived importance of reducing salt intake was categorized as positive if reported as very or somewhat important. Frequency of meals consumed outside the home was recorded as meals per week and categorized for analysis, and the type of cooking fat most commonly used was grouped as solid versus non-solid fats.
Statistical Analysis
All analyses accounted for the complex survey design. Sampling weights, primary sampling units, and stratification were specified using Stata’s survey (svy) procedures. Descriptive statistics were used to summarize participant characteristics and the prevalence of high salt intake. Bivariate associations between categorical variables and high salt intake were assessed using the Rao–Scott design-adjusted Pearson chi-square test to account for the complex survey design. Associations were further examined using survey-weighted logistic regression models. Bivariate logistic regression models were used to calculate crude odds ratios (CORs), while multivariable models were fitted to estimate adjusted odds ratios (AORs). Variables for the multivariable model were selected based on conceptual relevance and prior evidence rather than solely on bivariate statistical significance. All sociodemographic variables were included a priori as potential confounders, and behavioral and knowledge variables directly related to salt consumption practices were included as primary exposures. Variables representing similar or overlapping constructs, such as salt use during cooking and perceived importance of salt reduction, were excluded from the final adjusted model to avoid over-adjustment and multicollinearity. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs), and statistical significance was defined as p < 0.05. Multicollinearity among predictors was assessed using variance inflation factors (VIFs) from an ordinary least squares model including the same independent variables. All VIFs were below 3 (mean VIF = 1.43), indicating no evidence of problematic collinearity. Missingness was assessed for all study variables prior to analysis. The proportion of missing data was low (<3%) for most variables, although household wealth had a higher proportion of missing values (14.5%). Analyses were conducted using complete-case data. Observations with missing values were excluded through listwise deletion, as implemented by Stata’s survey (svy) procedures. Given the generally low level of missingness and the absence of evident systematic patterns, multiple imputation was not performed. All analyses incorporated sampling weights to maintain population representativeness. Stata version 15 IC was used to perform the analysis.
Ethical Considerations
The original study protocol received ethical approval from the Ministry of Public Health Institutional Review Board. All procedures were conducted in accordance with relevant guidelines and regulations. Participation was voluntary, informed consent was obtained, and no personal identifiers were collected. No additional ethical approval was required for this secondary analysis, as it used de-identified publicly available data.15
Results
Demographic Characteristics and Prevalence of Risk Factors
Table 1 describes the characteristics of the study participants. Values are presented as unweighted counts (n) and weighted percentages (%) to account for the complex survey design; weighted percentages reflect the population distribution and may differ from raw counts.
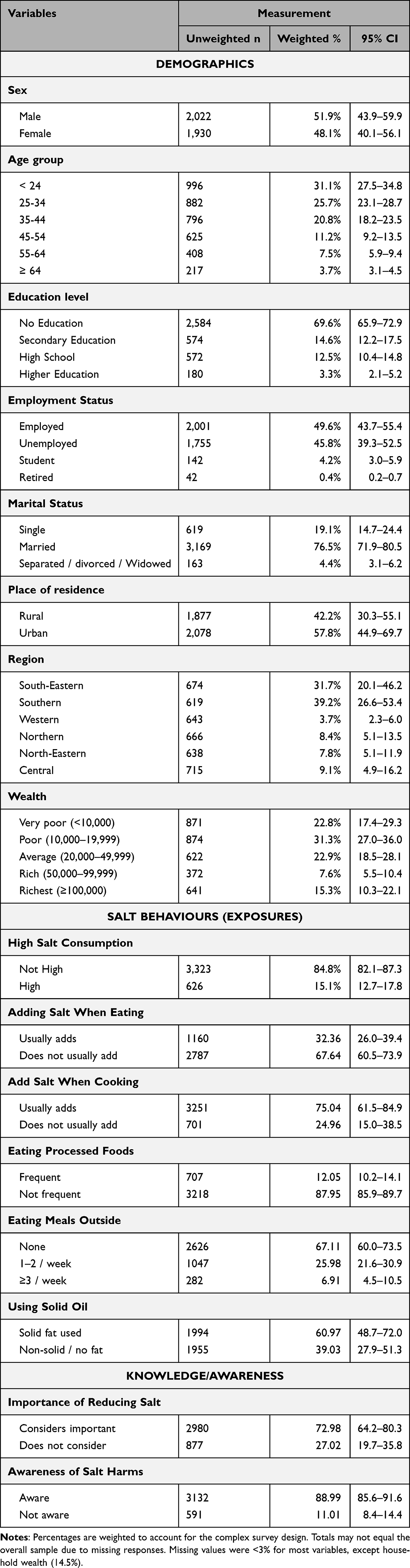 |
Table 1 Characteristics of Study Participants (N = 3,955) |
As shown in Table 1, a total of 3,955 participants were included in the study. Overall, 15.1% (n = 626; weighted) of participants reported high salt intake. Slightly more than half of participants were male (51.9%). The largest age group was <24 years (31.1%), followed by 25–34 years (25.7%), and the smallest proportion was among those aged ≥64 years (3.7%).
Most participants had no formal education (69.6%), while only 3.3% had higher education. Regarding employment, approximately half were employed, 45.8% were unemployed, 4.2% were students, and 0.4% were retired.
The majority were married (76.5%), with 19.1% single and 4.4% either separated, divorced, or widowed. About 57.8% resided in urban areas, and 42.2% in rural areas. Regional representation varied, with participants from the Southern (39.2% and South-Eastern (31.7%) regions being the largest groups.
For salt-related behaviors, 32.4% reported usually adding salt when eating, and 75.0% usually adding salt during cooking. About 12.1% reported frequently consuming processed salty foods, and 6.9% ate ≥3 meals outside per week. Solid fat was used by 61.0% of participants.
In terms of knowledge and awareness, 73.0% considered reducing salt important, and 89.0% were aware of the harmful effects of excess salt consumption.
Association Between Participant Characteristics and High Salt Intake
Table 2 presents the distribution of high salt intake across sociodemographic characteristics, salt-related behaviors, and knowledge indicators.
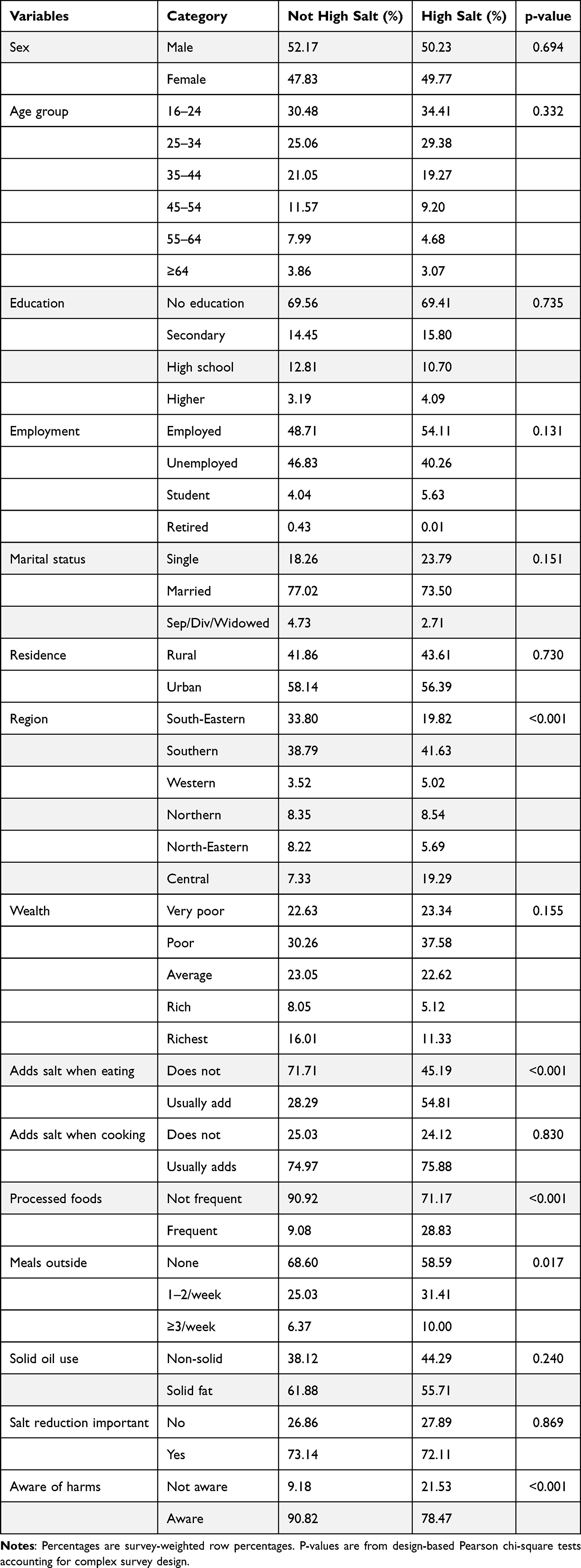 |
Table 2 Distribution of High Salt Intake According to Demographic, Behavioral, and Knowledge Characteristics (Survey-Weighted) |
High salt intake was associated with discretionary salt use at the table, frequent processed food consumption, eating meals outside the home, and lack of awareness of salt-related health harms. No significant differences were observed across different demographic characteristics including sex, age group, education level, employment, marital status, place of residence, or wealth. However, high salt intake varied significantly by region (p<0.001), indicating important geographic differences in consumption patterns.
Several salt-related behaviors were significantly associated with high salt intake. Participants who usually added salt at the table had nearly double the prevalence of high salt intake compared with those who did not (54.8% vs 28.3%, p<0.001). Similarly, frequent consumption of processed foods was associated with substantially higher high salt intake (28.8% vs 9.1%, p<0.001).
Eating meals outside the home was also significantly associated with high salt intake (p=0.017), with a dose–response pattern observed as frequency increased.
Regarding knowledge, awareness of the health harms of salt was significantly associated with lower high salt intake; individuals unaware of salt-related harms had more than twice the prevalence of high salt intake compared with those who were aware (21.5% vs 9.2%, p<0.001).
Crude and Adjusted Regression Model
Table 3 presents the crude and adjusted odds ratios of high salt intake among different demographic and behavioral categories.
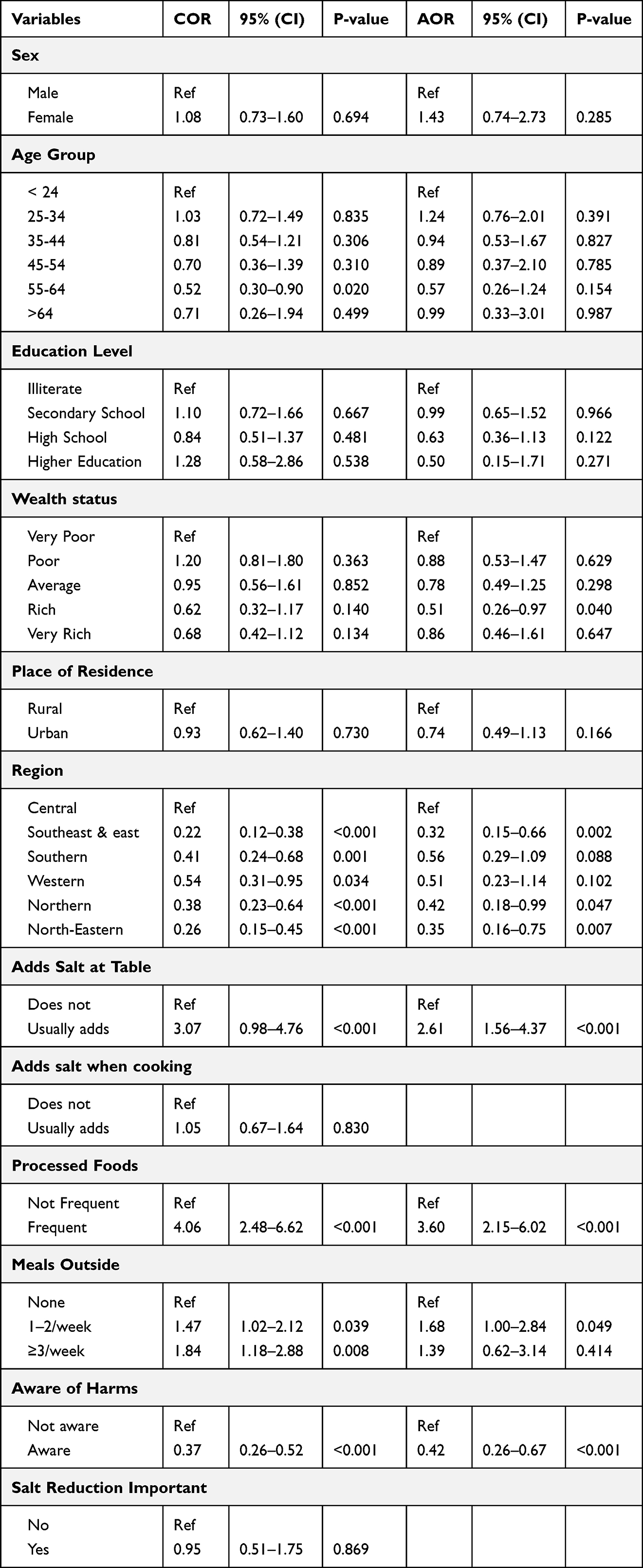 |
Table 3 Bivariate and Multiple Logistic Regression |
As shown in Table 3, in bivariate analyses, high salt intake was significantly associated with several behavioral factors, including adding salt at the table, frequent consumption of processed foods, eating meals outside the home, and lack of awareness of the health harms of excess salt. Regional differences were also observed. Sociodemographic characteristics such as sex, education, wealth, and place of residence were not significantly associated with high salt intake in crude models.
After adjusting for potential confounders in the multivariable survey-weighted logistic regression model, most sociodemographic variables remained non-significant, while strong associations persisted for several behavioral factors. Participants who usually added salt at the table had more than twice the odds of high salt intake compared with those who did not (AOR = 2.61; 95% CI: 1.56–4.37). Frequent consumption of processed foods (AOR 3.60, 95% CI 2.15–6.02) was independently associated with substantially higher likelihood of high salt intake. Eating meals outside the home was associated with higher salt intake in bivariate analysis; however, the association was weakened after adjustment, and only eating 1–2 meals outside the home remained significantly associated with the outcome (AOR 1.69, 95% CI 1.00–2.84). Awareness of excess salt harms was protective (AOR 0.42, 95% CI 0.26–0.67).
Among demographic characteristics, only region disparities remained evident in adjusted analysis. Compared with the Central region, participants in the South East & East (AOR 0.32, 95% CI 0.15–0.66), Northern (AOR 0.42, 95% CI 0.18–0.99), and North-East regions (AOR 0.35, 95% CI 0.16–0.75) had significantly lower odds of high salt intake. No significant associations were observed for sex, age, place of residence, or education after adjustment.
Discussion
This study provides the first nationally representative assessment of high salt intake and its associated determinants among adults in Afghanistan using WHO STEPS survey data. It is worth mentioning that the outcome of this study was the self-perceived salt intake, it is therefore necessary to be careful while interpreting the results of this study. Approximately one in six adults perceived their salt intake as high, and this perception was consistently linked to specific modifiable behaviors, particularly adding salt before eating, frequent consumption of processed foods, and eating meals outside the home. In contrast, most sociodemographic characteristics did not show any association with salt intake. On the other hand, awareness of the harms of salt was associated with lower odds of high salt intake. Taken together, these findings suggest that salt exposure in Afghanistan is less a function of who people are and more a reflection of how food is prepared, purchased, and consumed in everyday life.
The apparent discrepancy between the estimated average salt intake in Afghanistan (around 12.1 g/day) and the relatively low proportion of participants reporting high salt intake in this analysis (15%), likely reflects a perception gap. The observed prevalence of self-reported high salt intake is lower than the proportions observed in other studies using objective measurement of sodium intake, where a majority of the adults exceed the WHO recommended limit of 5g/day. For example, studies in some neighboring countries such as Nepal and Iran found that 70.8% and 98% of adults, respectively, consumed more than the WHO daily average recommendation.10,16 Similarly, systematic reviews in other regions indicate that mean salt intake among adults commonly exceeds recommended levels.17 The lower prevalence observed in the current study likely reflects the limitation of self-perceptions, as individuals often underestimate their own salt consumption or may not recognize hidden sources of sodium in different foods. Therefore, the true burden of excessive salt intake in Afghanistan is likely higher than what is captured here.
Behavioral factors showed the strongest and most consistent associations. Frequent consumption of processed foods emerged as the strongest predictor in our multivariate model. This finding is aligned with the existing global data from both high-income18,19 and low-income20,21 countries where processed foods are considered the main source of dietary salt. Although Afghanistan’s processed food market is smaller than that of many middle and high-income countries, the availability of packaged snacks, street foods, and commercially prepared products has increased in recent years, particularly in urban areas. International experience suggests that reformulation of processed foods,22 front-of-pack labeling,23 and regulatory sodium targets are among the most effective strategies to reduce population salt intake.
The strong association between adding salt before eating and high salt intake is consistent with the existing global evidence where discretionary salt use before eating meals remains a major source of sodium exposure which in turn can increase the risk of premature mortality.24,25 This practice likely reflects habitual taste preferences rather than necessity and represents a simple and potentially modifiable behavior. Low-cost interventions, such as behavior change campaigns, salt-restriction counseling in primary care, or household education could meaningfully reduce salt use.
Eating meals outside the home was another important factor. Foods prepared by restaurants, small eateries, and street vendors often prioritize taste, preservation, and cost, which may result in higher salt content. This pattern is well documented globally,26,27 as commercially prepared foods often prioritize taste over nutritional quality. Given that much of Afghanistan’s food sector is informal and lightly regulated, engagement with vendors and food preparers may be a practical entry point for salt reduction efforts. Even small reductions in salt during cooking at the community level could translate into substantial population benefits.
An interesting finding was the apparent gap between knowledge and behavior. Although a large proportion of participants reported being aware of the harms of excessive salt intake, this awareness did not uniformly translate into healthier practice. While awareness of harms of excessive salt was associated with lower odds of high intake, a considerable proportion of individuals still reported high salt consumption. This suggests that knowledge alone may not be sufficient to fully change behavior without supportive changes in the food environment. Similar knowledge–behavior gaps have been documented in other LMICs28–32 and reinforce the idea that structural and policy-level approaches are generally more effective than relying solely on individual responsibility.
Interestingly, most sociodemographic variables like sex, age, education, and residence were not independently associated with high salt intake. This finding contrasts with findings from some neighboring countries like Pakistan,33 Bangladesh,34 and India35 where high salt intake was found to be significantly associated with sex, education, wealth and age. This difference may reflect the relatively uniform dietary patterns within Afghanistan, where traditional foods and shared household practices remain dominant across groups. From a public health perspective, this supports the need for broad, population-wide strategies rather than narrowly targeted interventions.
We also observed clear regional variation. Participants in northern and eastern regions had substantially lower odds of high salt intake compared with those in the central region. These differences may reflect variations in food availability, market access, urbanization, and cultural cooking practices. Regions that rely more heavily on home-prepared traditional foods and have less exposure to commercially prepared products may naturally have lower sodium intake. Understanding these contextual differences could help identify protective practices that might inform tailored interventions in higher-risk areas. Future research should explore region-specific dietary sources of sodium.
The findings of this study have clear implications for national non-communicable disease prevention strategies. Given the strong influence of behavioral and environmental determinants, salt reduction efforts should prioritize public education campaigns to discourage discretionary salt use, reformulation initiatives for processed foods, engagement with restaurants and street vendors to reduce salt during food preparation, clear labeling and consumer awareness tools, and integration of salt reduction messages into primary health care and community programs.
Strengths and Limitations
This study has several strengths. It used nationally representative WHO STEPS data, applied appropriate sampling weights, and accounted for the complex survey design. Standardized data collection procedures enhance comparability with other countries. Additionally, the inclusion of multiple behavioral indicators allowed identification of specific modifiable determinants.
Several limitations should be considered. The use of self-reported salt intake instead of urinary sodium estimation may introduce measurement bias. Although the STEPS survey includes biomarker-based sodium assessment for a subsample of participants, the limited coverage of these measurements restricts their use for nationally representative analysis. The cross-sectional design may not allow causal inference. Some variables had missing data, although the proportion was low and complete-case analysis was unlikely to substantially affect estimates. Finally, residual confounding from unmeasured dietary factors cannot be excluded.
Conclusion
In this nationally representative study of Afghan adults, high salt intake was strongly associated with discretionary salt use, processed food consumption, and eating meals outside the home, while most demographic characteristics showed little independent effect. Overall, these findings indicate that salt consumption in Afghanistan is closely linked to everyday food practices and the local food environment. Policies that combine behavior change communication with structural measures, such as food reformulation, vendor engagement, and regulation of the food environment are likely to have the greatest impact. Early action may help prevent further increases in sodium intake and contribute to reducing the growing burden of hypertension and cardiovascular disease in the country.
Abbreviations
AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; CI, Confidence Interval; DALY, Disability-Adjusted Life-Year; GBD, Global Burden of Disease; LMIC, Low- and Middle-Income Countries; NCD, Non-Communicable Disease; STEPS, STEPwise approach to NCD risk factor surveillance; VIF, Variance Inflation Factors; WHO, World Health Organization.
AI Statement
During the preparation of this manuscript, the authors used ChatGPT (OpenAI, GPT-5.3) to assist with language editing and improving the clarity and readability of the text. The tool was not used for data analysis, interpretation of results, or generation of scientific conclusions. All content was reviewed, verified, and approved by the authors, who take full responsibility for the final manuscript.
Data Sharing Statement
We used the dataset from WHO STEP survey 2018. The data is available through the following website: https://extranet.who.int/ncdsmicrodata/index.php/catalog/782.
Ethical Approval and Consent to Participate
No additional ethical approval was required for this secondary analysis of de-identified publicly available data. The original survey was approved by the Afghan Ministry of Public Health ethics board (IRB). Written consent was obtained from participants, and in cases involving minors or individuals unable to provide consent, the forms were signed by legal guardians or appropriate representatives.
Acknowledgment
We extend our deepest appreciation to the Heidelberg Institute of Global Health for their support and collaboration during the process. Additionally, we express our gratitude to the World Health Organization for providing access to the data from the Afghanistan STEP survey. Last but not least we would like to dedicate this work to the memory of Prof. Volker Winkler, whose mentorship, guidance, and unwavering support profoundly shaped the first author’s academic and professional journey. His commitment to global health research continues to inspire this work.
Author Contributions
ASN contributed to conceptualization, methodology, formal analysis, investigation, data curation, writing of the original draft, review and editing, and visualization. PD contributed to the conceptualization, methodology, review and editing of the manuscript. AShN contributed to the methodology, writing and editing. OEHH contributed to the writing and editing of the manuscript. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project received no specific grant from any funding agency in the public commercial or not-for-profit sectors.
Disclosure
The authors declare no competing interests in this work.
References
1. Nie Y, Wang N, Huang M, et al. Global burden of disease from high-sodium diets, 1990–2021: analysis of GBD 2021 data. Front Nutri. 2025;12:1617644. doi:10.3389/fnut.2025.1617644
2. World Health Organization. Sodium reduction: WHO fact sheets; 2025 Available from: https://www.who.int/news-room/fact-sheets/detail/sodium-reduction.
3. Lin J, Wang H, Xiao M, et al. Trends of global burden of cardiovascular diseases attributable to high sodium intake from 1990 to 2021 and projections to 2030: a Population-Based Study. J Clin Hypertens. 2025;27(12):e70169. doi:10.1111/jch.70169
4. Liu W, Zhou L, Yin W, Wang J, Zuo X. Global, regional, and national burden of chronic kidney disease attributable to high sodium intake from 1990 to 2019. Front Nutri. 2023;10:1078371. doi:10.3389/fnut.2023.1078371
5. Wang K, Jin Y, Wang M, et al. Global cardiovascular diseases burden attributable to high sodium intake from 1990 to 2019. J Clin Hypertens. 2023;25(9):868–14. doi:10.1111/jch.14717
6. Hu J-R, Sahni S, Mukamal KJ, et al. Dietary sodium intake and sodium density in the United States: estimates from NHANES 2005–2006 and 2015–2016. Am J Hypertens. 2020;33(9):825–830. doi:10.1093/ajh/hpaa104
7. Kwong EJL, Whiting S, Bunge AC, et al. Population-level salt intake in the WHO European Region in 2022: a systematic review. Public Health Nutrition. 2023;26(S1):s6–s19. doi:10.1017/S136898002200218X
8. Ghimire K, Mishra SR, Satheesh G, et al. Salt intake and salt-reduction strategies in South Asia: from evidence to action. J Clin Hypertens. 2021;23(10):1815–1829. doi:10.1111/jch.14365
9. Afroza U, Abrar AK, Nowar A, et al. Salt intake estimation from urine samples in south asian population: scoping review. Nutrients. 2023;15(20):4358. doi:10.3390/nu15204358
10. Nosratinia N, Azadnajafabad S, Masinaei M, et al. Salt intake among the iranian population and public attitudes toward salt consumption: national and subnational report from STEPS 2021. Food Sci Nutr. 2026;14(1):e71399. doi:10.1002/fsn3.71399
11. Younas S, Parvathi H, Sahu S, et al. Salt substitutes in low-income settings: blood pressure benefits, cardiovascular outcomes, and safety considerations: a narrative review. J Vascular Dis. 2025;4(4):42. doi:10.3390/jvd4040042
12. Neyazi N, Mosadeghrad AM, Afshari M, Isfahani P, Safi N. Strategies to tackle non-communicable diseases in Afghanistan: a scoping review. Front Public Health. 2023;11:982416. doi:10.3389/fpubh.2023.982416
13. Noormal AS, Winkler V, Bhusari SB, et al. Prevalence of major non-communicable diseases and their associated risk factors in Afghanistan: a systematic review and meta-analysis. Therap Adv Chronic Dis. 2024;15:20406223241229850. doi:10.1177/20406223241229850
14. Neyazi N, Mosadeghrad AM, Tajvar M, Safi N. Financing of non-communicable diseases in Afghanistan. Int J EquityHealth. 2025;24(1):99. doi:10.1186/s12939-025-02423-4
15. JS Consultancy Services. Survey report: national noncommunicable diseases risk factors survey. Afghanistan 2018.
16. Bhattarai S, Bista B, Yadav BK, et al. Estimation of mean population salt intakes using spot urine samples and associations with body mass index, hypertension, raised blood sugar and hypercholesterolemia: findings from STEPS Survey 2019, Nepal. PLoS One. 2022;17(4):e0266662. doi:10.1371/journal.pone.0266662
17. Bhat S, Marklund M, Henry ME, et al. A systematic review of the sources of dietary salt around the world. Adv Nutr. 2020;11(3):677–686. doi:10.1093/advances/nmz134
18. Thomson BM. Nutritional modelling: distributions of salt intake from processed foods in New Zealand. Br J Nutr. 2009;102(5):757–765. doi:10.1017/S000711450928901X
19. Webster JL, Dunford EK, Neal BC. A systematic survey of the sodium contents of processed foods. Am J Clin Nutri. 2010;91(2):413–420. doi:10.3945/ajcn.2009.28688
20. Menyanu E, Russell J, Charlton K. Dietary sources of salt in low-and middle-income countries: a systematic literature review. Int J Environ Res Public Health. 2019;16(12):2082. doi:10.3390/ijerph16122082
21. George A, George A. High salt intake in India: health and economic impacts. Zenodo. 2024.
22. World Health Organization. Reformulation of food and beverage products for healthier diets: policy brief. World Health Organization. 2022.
23. Crosbie E, Gomes FS, Olvera J, Patiño SR-G, Hoeper S, Carriedo A. A policy study on front–of–pack nutrition labeling in the Americas: emerging developments and outcomes. Lancet Reg Health Am. 2023;18.
24. Ma H, Xue Q, Wang X, et al. Adding salt to foods and hazard of premature mortality. Eur Heart J. 2022;43(30):2878–2888. doi:10.1093/eurheartj/ehac208
25. Kronsteiner-Gicevic S, Thompson AS, Gaggl M, Bell W, Cassidy A, Kühn T. Adding salt to food at table as an indicator of gastric cancer risk among adults: a prospective study. Gastric Cancer. 2024;27(4):714–721. doi:10.1007/s10120-024-01502-9
26. Ruiz AMP, Lima MG, Medina L, Pinto RL, de Azevedo Barros MB, de Azevedo Barros Filho A. Can meals outside homes impact sodium intake? Curr Dev Nutr. 2020;4(6):nzaa091. doi:10.1093/cdn/nzaa091
27. Pita Ruiz A, Lima M, Luz R, et al. Sodium intake among adolescents who eat inside and outside the home. Eur J Public Health. 2020;30(Supplement_5):
28. Sharma D, Gupta S, Goel NK, Katariya B, Singh P, Sareen A. Exploring knowledge, attitudes, and practices regarding salt intake: a community-based cross-sectional study. Int Jo Noncommun Dis. 2024;9(4):144–149. doi:10.4103/jncd.jncd_59_24
29. Bhattacharya S, Thakur J, Singh A. Knowledge attitude, and practice regarding dietary salt intake among urban slum population of North India. J Fam Med Primary Care. 2018;7(3):526–530. doi:10.4103/jfmpc.jfmpc_60_17
30. Akter R, Rahman T, Miah MI, et al. Knowledge and practice of salt consumption in Dhaka’s urban population: a Cross-Sectional Public Health Study. IUBAT Rev. 2025;8(2):59–81. doi:10.3329/iubatr.v8i2.86880
31. Shaikh MM, Alkhayari AH, Alabdulsalam QA, AlHashmi K, Nadar SK. Estimation of salt intake and its relation to knowledge and attitude regarding the dangers of high salt intake among an urban omani population: a pilot study. Sultan Qaboos Univer Med J. 2022;22(4):486. doi:10.18295/squmj.9.2021.134
32. Zafar A, Rizwan B, Jaffar HM, et al. Knowledge, attitude and practices regarding dietary salt intake among university students: dietary salt intake among university students. Diet Factor. 2023;17–24.
33. Saqib MAN, Rafique I, Rahat T, Rahat T. High salt intake implications as risk factor for hypertension and comparison of three salt estimation methods-findings from Islamabad, Pakistan. Pakistan Heart J. 2021;54(4):309–314. doi:10.47144/phj.v54i4.2156
34. Jahan S, Bhuiya A, Hanifi S, Iqbal M, Rasheed S. Abstract P094: Determinants of Salt Consumption in Rural Bangladesh: Findings From Assessment of 24 H Urinary Sodium Excretions. Lippincott Williams & Wilkins; 2013.
35. Mathur P, Kulothungan V, Nath A, Vinay Urs K, Ramakrishnan L. Awareness, behavior, and determinants of dietary salt intake in adults: results from the National NCD Monitoring Survey, India. Sci Rep. 2023;13(1):15890. doi:10.1038/s41598-023-42694-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.