Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Diet and Physical Activity Intervention in Normal Weight Obesity Population Base on Smartphone App: Protocol for a Randomized Controlled Trial
Authors Liu G ![]() , Yang K, Wang C, Yang J
, Yang K, Wang C, Yang J ![]()
Received 11 November 2024
Accepted for publication 22 March 2025
Published 3 April 2025 Volume 2025:18 Pages 1005—1013
DOI https://doi.org/10.2147/DMSO.S505820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Liang Wang
Guoqiang Liu,1,* Kun Yang,1,* Chen Wang,1,2 Jin Yang1
1Department of Endocrinology and Metabolism, State Key Laboratory of Female Fertility Promotion, Peking University Third Hospital, Beijing, 100191, People’s Republic of China; 2Department of Clinical Nutrition, Peking University Third Hospital, Beijing, 100191, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Wang; Jin Yang, Email [email protected]; [email protected]
Background: Normal weight obesity (NWO) is defined as normal body mass index (BMI) but increased body fat percentage (BF%). NWO population tend to develop metabolic syndrome, type 2 diabetes and cardiovascular disease. BF% is the key parameter applied in the evaluation of NWO. The exact prevalence of NWO and the cutoff point for the diagnosis of NWO are not well established. Diet and physical activity interventions are the main approach for NWO management. Smartphone apps are widely used for their effectiveness and individualization, making them ideal tool for simplifying the follow-up process in behavioral interventions for both investigators and participants.
Methods: A single center, prospective, randomized trial will be conducted in Beijing, China. The aim of this 12-week trial is to assess the efficacy of different lifestyle interventions, including diet control only, aerobic training only, resistance training only, and a combination of aerobic and resistance training based on a smartphone app on BF% and metabolic parameters in the NWO population. The primary outcome is the change of BF% between the baseline and 12 weeks post-intervention. The secondary outcomes include changes in measures of anthropometry, blood glucose, insulin, lipids and uric acid between the baseline and 12 weeks of intervention. A sample size of 200 subjects with normal BMI and glucose abnormality confirmed by oral glucose tolerance test will be recruited. Two follow-ups face-to-face and five follow-ups via smartphone app will be included in this trial. Statistical analyses will focus on the differences among different lifestyle interventions and the cutoff point of BF% for diagnosis of NWO.
Discussion: This trial will provide evidence of the efficacy of lifestyle interventions based on smartphone app. The differences in effect among different lifestyle intervention groups will be elucidated. It will be helpful to propose the cutoff point of BF% for diagnosis of NWO.
Trial Registration Number: This study was registered with chictr.org.cn: ChiCTR2200063583.
Keywords: normal weight obesity, body fat percentage, randomized controlled trial, smartphone app
Introduction
Obesity and associated disorders have been identified as serious public health challenges as a major determinant of disability and death in China and worldwide nowadays.1–3 The prevalence of metabolic syndrome, type 2 diabetes (T2DM), and cardiovascular diseases in obese population is higher than that of normal weight population. Obesity is defined as excessive accumulation and/or abnormal distribution of body fat that may impair health. Body mass index (BMI) is the most widely applied parameter in the assessment of obesity due to its simplicity. However, a significant limitation of BMI is its failure to distinguish between fat and lean tissue. In some cases, body fat is excessive, while BMI remains within the normal range.4 De Lorenzo5 et al first defined the term normal weight obesity (NWO) as adequate value of BMI but increased body fat percentage (BF%) and metabolic abnormalities. However, NWO has not been widely recognized in clinical practice and there remains a rather large NWO proportion with apparently normal shape but with high metabolic and cardiovascular risks. Similar to the obese population, NWO population tend to develop certain health conditions, such as metabolic syndrome, T2DM, cardiovascular disease, sarcopenia, adverse reproductive outcomes and low bone mineral density.6–10
The prevalence of NWO is not well established, and there is wide variation among different studies, attributing to ethnic differences, methodologies used to assess body composition, and different cutoff points for the diagnosis of NWO.
BF% is the key parameter applied in the evaluation of NWO. De Lorenzo et al,11 based on the data of 74 women, firstly proposed the diagnosis cutoff point of NWO as normal BMI but BF% is >30% of the total body weight measured with dual-energy X-ray absorptiometry (DEXA). Bioelectrical impedance analysis (BIA) is another method widely used to evaluate BF%. In a pilot study with a sample of 100 women, depending on the cutoff point of >30% body fat measured by BIA, Čuta et al12 demonstrated that up to 14% of the women were diagnosed with NWO. However, there is no clear consensus on the cutoff points of NWO. Using the BF% of ≥26% for men and ≥38% for women as the cutoff values, Marques-Vidal et al found an NWO prevalence of 2.8% in men and 5.4% in women in Switzerland.13 Kim et al14 reported a NWO prevalence of 36% in men and 29% in women in Korea, using the cutoff point of men with BF%≥20.6% and women with BF%≥33.4%. Chinese researchers suggested that the optimal BF% cutoff values are 20% and 30% for Chinese men and women, respectively.15,16 Romero-Corral et al found an overall NWO prevalence of 33.4% in Americans using a cutoff point of 23.1% for men and 33.3% for women based on the upper tertile.17 The variation among the results suggests that it is critical to define the cutoff point of BF% for diagnosis, as well as prevention and management of NWO.
The data (unpublished) we collected from 22 outpatients from Peking University Third Hospital with normal BMI (<24 kg/m2, according to the criteria of the Chinese Society of Endocrinology1) and abnormal glucose metabolism confirmed by oral glucose tolerance test (OGTT) showed that most of the subjects were women (20 women and 6 men), which is consistent with the researches from Asian population.16,18 The mean BMI and BF% of the patients were 22.06 kg/m2 and 28.55%. Among the subjects, 3 had impaired fasting glucose (IFG), 14 had impaired glucose tolerance (IGT), 4 subjects are IFG accompanied by IGT, and 5 subjects met the criteria of T2DM. Eight out of 15 patients who had blood lipid tests showed abnormalities. The data suggest that it is important to identify metabolic risks and exert intervention in individuals with normal BMI to prevent the risk of metabolic and cardiovascular diseases.
Lifestyle improvement, including diet and physical activity intervention, is the main approach for NWO management.19,20 In fact, it is not necessary for the subjects to receive face-to-face intervention of weight management in each follow-up, as blood tests or other examinations are not required during each follow-up, nor distribution of medications involved. Consequently, innovative solutions are needed to improve the effectiveness of obesity management trials. Smartphone apps could support behavioral interventions, thereby increasing the effectiveness of intervention. Compared to face-to-face interventions, app-based interventions can be advantageous to investigators over long distances, at the same time, app-based interventions reduce the frequency of hospital visits for participants.
The potential influence of lifestyle intervention on NWO population is not well studied. We hypothesize that lifestyle intervention will decrease the BF% and improve the metabolic parameters of the NWO population. The primary outcome is the change in BF% between the baseline and 12 weeks post-intervention. The secondary outcomes include changes in measures of anthropometry, blood glucose, insulin, lipids and uric acid between the baseline and 12 weeks of intervention. The aim of this 12-week proposed trial is to assess the efficacy of different lifestyle interventions, including diet control only, aerobic training only, resistance training only, and a combination of aerobic and resistance training based on a smartphone app on the BF% and metabolic parameters in the NWO population. According to the BF% of participants whose OGTT return to normal after intervention, we will propose the cutoff point of BF% for diagnosis of NWO. The results of this study could contribute to clinical practice of the management of obesity.
Methods and Analysis
Study Design
A single center randomized controlled trial will assess the efficacy of 12-week lifestyle intervention in the NWO population in Beijing, China, from August 2024 to December 2026 (Figure 1).
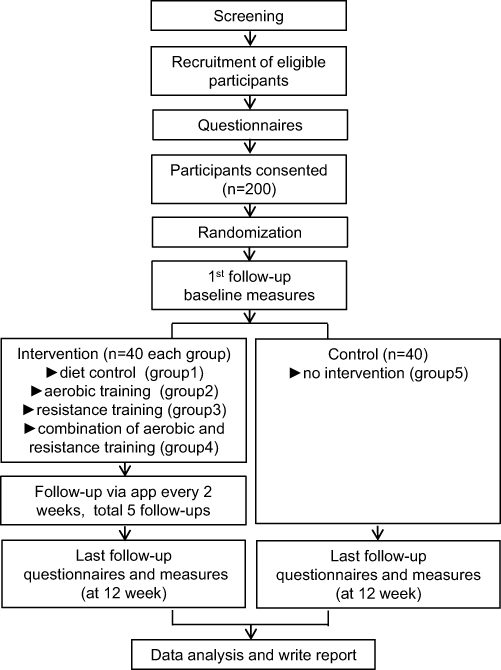 |
Figure 1 Study design and flow chart. |
Participants
Participants are eligible for the trial if they meet the following inclusion/exclusion criteria.
Inclusion Criteria
- Aged 18–44 years
- BMI of 18.5–23.9 kg/m2
- BF% > 20% for men and BF% > 30% for women
- Glucose abnormality (IFG, IGT, T2DM, confirmed by OGTT)
- Access to a smartphone
Exclusion Criteria
- Medication of antihyperglycemia 12 weeks before enrollment
- Severe liver and/or kidney damage (ie, alanine aminotransferase and/or aspartate aminotransferase >2.5-fold the upper limit of the normal range; glomerular filtration rate < 45 mL/min)
- Severe heart failure (ie, New York Heart Association Class > III), acute coronary syndrome, or acute myocardial infarction, occurring within 12 weeks
- Systolic pressure > 159 mmHg and/or diastolic pressure > 99 mmHg
- Currently suffering from endocrine disorders, such as hyperthyroidism or hypercortisolism
- History of cancer
- History of joint illness, osteoporosis, or nontraumatic fracture
- Pregnancy or plan to get pregnant within 12 weeks
- Dementia
- Previously a participant in a clinical trial 12 weeks before enrollment
- Training habits 12 weeks before enrollment
- Changing in diet habit intending to lose weight 12 weeks before enrollment
Recruitment
A multipoint recruitment strategy will be employed to enroll participants, primarily involving recruitment via:
- Outpatient clinics
- Health management center
- Community hospitals
- WeChat official account
- All individuals interested in this study may contact the study team directly about enrolment via the phone number or WeChat.
Consent and Randomization
200 eligible participants will be randomized in a 1:1:1:1:1 ratio into 5 groups.
- Diet control only (group1)
- Aerobic training only (group2)
- Resistance training only (group3)
- Combination of aerobic and resistance training (group4)
Control (group5)
Consent form will be signed after participants complete baseline data collection procedures and questionnaires. Participants will be allocated a unique randomization number. Allocation will be performed after the participant has signed the consent form.
Sample Size Calculation
The sample size calculation was performed using an ANOVA F-test for means in a randomized design function implemented in PASS 15. The parameters used for sample size calculation were based on the results of a single-arm, paired-sample trial evaluating the effect of time-restricted eating on reducing weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome21 and a randomized controlled trial evaluating the effect of 12 weeks of euenergetic high-protein diet in regulating appetite and body composition of women with normal-weight obesity.22 Anticipating a 20% dropout rate, the estimated sample size for the intervention group is n = 40 and the control group is n = 40, using a 5% significance level (α) and 80% power (1-β).
Intervention
Diet Intervention
A questionnaire from nutritionists is used to identify food choices and assess dietary habit within recent 3 days of each participant. Based on the questionnaire, nutritionists will provide the corresponding diet advice to each participant according to the Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition).23 Participants will be requested to upload pictures of 3 meals every day. In the following 12 weeks, nutritionists will provide further diet advice through the iHealthLabs app every 2 weeks according to the pictures. Rather than caloric reduction, the primary means of diet intervention in this trial is improvement of dietary components, such as restricting sugar and refined carbohydrates, replacing them with whole intact grains.
Cardiorespiratory Fitness and Muscular Strength Evaluation
Cardiorespiratory fitness will be evaluated using Bruce’s stress testing protocol24 on a treadmill, the most widely used protocol to assess aerobic capacity.25 The protocol will provide participants with a safe heart rate range during the training session. Upper limb muscular strength will be evaluated using handgrip dynamometry,26,27 and the lower limb muscular strength will be evaluated using the 30s chair stand test. Based on the strength evaluation, researchers will provide individualized resistance training recommendations to each participant.
Physical Activity Intervention
After screening for eligibility, all participants of the training control group will receive instructions for physical activity (PA). The Physical Activity Readiness Questionnaire (PAR-Q)28 is a simple screening tool for participants who plan to undergo a fitness assessment. The Physical Activity Readiness Medical Evaluation (PARmed-X)29 is a second form in addressing medical concerns related to PA participation that were identified by the PAR-Q. PAR-Q and PARmed-X are the most widely utilized screening tools in clinical trials that involving exercise, which can be found at www.eparmedx.com. After completing both questionnaires to exclude the contraindication of PA, participants will sign an informed consent.
Based on the Guideline for the Prevention and Treatment of T2DM in China (2020 edition),23 the exercise prescription is 150 minutes moderate-intensity training per week. Exercise intensity followed the safe heart rate range given by the Bruce’s stress testing protocol. Each training session will include a 5-minute warm-up and 5-minute cool-down and stretching period. Fast walking and jogging are the most popular exercises in China due to the convenience, which will be applied in this trial as aerobic training. One hundred and fifty-minute were divided into 4 sessions of training of 35–40 min each. Participants who were assigned to the aerobic training only group will complete 4 sessions of fast walking per week, and participants of the combination of aerobic and resistance training group will complete 2 sessions of fast walking per week. Resistance training participants will exercise 4 days per week, with each session consisting of 3–5 sets deep squat, push-up, crunch and plank. No specific amount of time is recommended for resistance training, but resistance training should be performed to the point at which it would be difficult to do another repetition. Until the muscle strength improves, participants will complete 10 repetitions per set if they could.
Those in the combination exercise group will have 2 resistance training and 2 aerobic training sessions per week. The control group will be required to maintain current diet and activity during the 12-week study period. Participants will be requested to upload pictures of each training session.
To reduce the risk of injury, it is important to increase the amount of physical activity gradually, and participants of groups 2, 3 and 4 will receive training instruction every 2 weeks via an app by a certified fitness instructor.
Data Collection Protocol
Outcome measures will be collected at baseline and after 12 weeks of intervention. Each participant will download the smartphone app iHealthLabs from Android or Apple’s app store. ihealthLabs is a smartphone-based self-monitoring and interaction app. The app focuses on 2 key behaviors, improvement of diet habits and establishment of exercise habits. Participants are required to upload pictures of all the food and beverages consumed every day, as well as pictures of each training session, including walking or jogging distance. If the participants fail to upload pictures, investigators will contact them via phone calls and WeChat. The data of weight will be collected every 2 weeks.
Once the data is uploaded, the research team will analyze the data remotely. Every 2 weeks, investigators will provide personalized feedback about their daily meals and training sessions, and offer advice via the app. Participants may review the corresponding feedback, adjust their diet and fulfil their training schedule. At the same time, participants may also interact with the investigators. The trial data will be doubly entered into a password-protected computer within 2 weeks of data collection. To ensure data quality, double data entry will be conducted.
Outcome Measures
The primary outcome of this trial is the change in BF% before and after intervention. The secondary outcomes are skeletal muscle percent, body weight, BMI, waist hip ratio, blood glucose, hemoglobin A1c (HbA1c), insulin, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and uric acid (UA).
Anthropometry and Body Composition
Body weight, BF% and skeletal muscle percent will be measured in an overnight fasting state, after emptying the urinary bladder and in light underwear using an InBody 770 bio-impedance device (Biospace, Co., Ltd., Seoul, Korea).30,31
Height will be measured to the nearest 0.1 cm using a wall-mounted height scale. Waist circumference will be measured twice to the nearest 0.1 cm (a third measure will be taken if the difference is >1.0 cm.) at the midpoint between the lower costal margin and the level of the anterior superior iliac crests. Hip circumference will also be measured twice to the nearest 0.1 cm around the widest point of the buttocks. The mean of the two measurements will be used for statistical analysis. Both the waist circumference and the hip circumference will be measured by a flexible tape rule.
BMI is calculated as the body mass (kg) divided by the square of the body height (m). Waist hip ratio is calculated as the waist circumference (cm) divided by the hip circumference (cm).
Blood Pressure
Resting systolic and diastolic blood pressure will be measured in a seated position by a mercury sphygmomanometer. The measurement will be performed twice at the interval of 2 min by a trained researcher. The mean of the two measurements will be used for statistical analysis.
Biochemical Measures
Blood tests will be performed at baseline and 12 weeks post-intervention. Each blood test will include an OGTT and a blood biochemical assay. OGTT will include blood glucose and insulin at 0 min and 120 min after consuming 75 g glucose dissolved in 200–300 mL of water. Biochemical assay will include HbA1c, TC, LDL-C, HDL-C, TG, and UA. Glucose will be determined by the hexokinase method. Insulin will be measured using a chemiluminescence assay. HbA1c concentration will be measured by high-performance liquid chromatography. TC, LDL-C, HDL-C, TG, and UA testing will be performed using turbidimetric assay.
Participant Schedule
After randomization, participants will receive the assigned intervention regimen. As displayed in Table 1, during the 12-week study period, diet control only group, aerobic training only group, resistance training only group, and combination of aerobic and resistance training group are required to complete follow-ups 1 ~ 7. Control group will complete follow-ups 1 and 7.
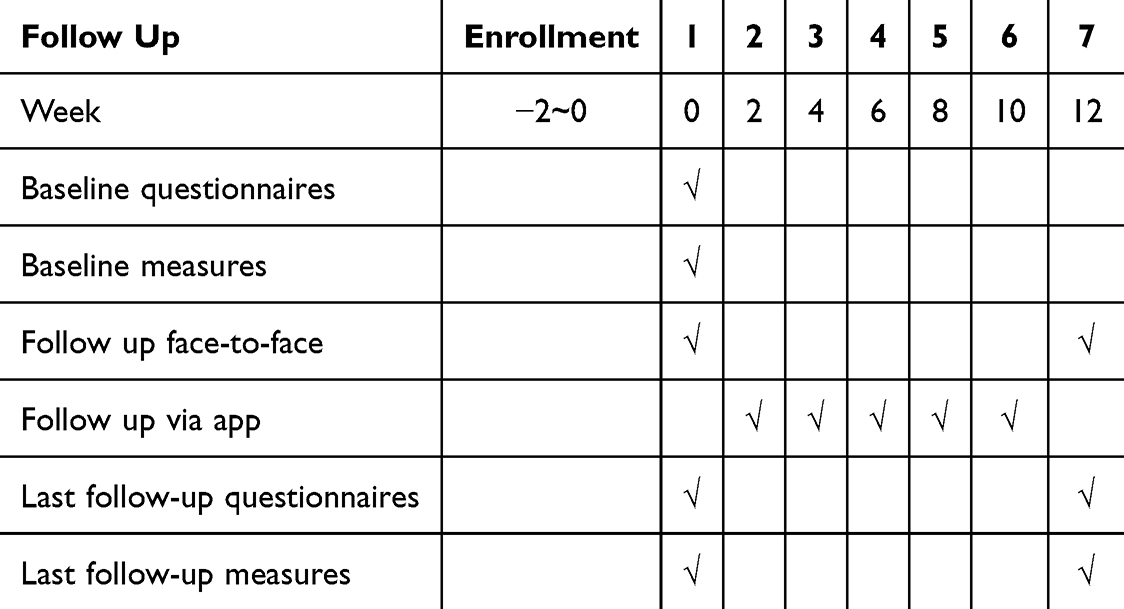 |
Table 1 Overview of Study Schedule |
Process Evaluation
Process evaluation will follow the key recommendations of Medical Research Council (MRC) guidelines for process evaluations of lifestyle interventions.32 The implementation of the intervention is monitored using a series of methods.
- Regular team meetings with standardized records focusing on implementation components and unexpected adverse events
- Standardized records on the individual participant’s participation and behavioral responses to intervention
- Standardized forms to record key information relating to each study component
- Regular direct observation of all aspects of implementation fidelity will be conducted by trained individuals who are not involved in the trial
Data Analysis
The outcomes will be analyzed using an intention-to-treat approach. The distributions of the continuous variables will be evaluated. If the distribution is significantly skewed, a suitable transformation will be applied. The primary aim of this study is to evaluate whether the change in BF% differs among different interventions. The differences of BF% at 12 weeks post-intervention among the 4 intervention and control groups will be evaluated using a univariate linear regression adjusted for baseline outcome measures. Secondary outcomes will follow a similar statistical approach as the primary outcome analysis. The analysis will be performed by two independent researchers. If agreements cannot be reached, a third researcher will be consulted. As part of the process evaluation, adherence will be evaluated by conducting per protocol analysis. Finally, multiple imputation methods will be performed to address missing data if data are missing at random. All outcome comparisons at both baseline and 12 weeks post-intervention will be considered significant at the 5% level. Intervention effects will be reported on the difference scale.
Strengths and Limitations
To our knowledge, this is the first randomized controlled intervention trial on NWO population in China. The novelty of this pioneering study lies in the application of a blended intervention approach combining app-based and face-to-face interactions. The study aims to elucidate the differences among different lifestyle interventions, including diet control, aerobic training and resistance training. The study includes a comprehensive and explicit design of the intervention, as well as includes a robust process evaluation plan. The sample size is large enough to detect a significant clinical effect.
Although efforts will be made to minimize contamination among the 5 study groups, complete avoidance is still impractical. To reduce the contamination among groups, investigators will give each participant recommendations that follow the interventions of the group strictly and repeat the recommendations on each follow-up day. Due to the nature of app and face-to-face blended intervention study, the implementation of participants cannot be fully monitored, and the participants may feel a lack of support compared with face-to-face visits, so as to reduce adherence. A 12-week study period may not be sufficient to evaluate the effects of diet and physical activity intervention. Follow-up assessments will be conducted 6 or 12 months post-study to further evaluate the sustainability of the changes.
Ethics and Dissemination
All participants will provide written consent. This trial was registered with the Chinese Clinical Trials Registry at West China Hospital, Sichuan University (ChiCTR2200063583). Local ethical approval was granted by the Ethical Committee of Peking University Third Hospital (M2022556). The trial will comply with the Declaration of Helsinki. The primary and secondary outcomes valuation results of the trial will be disseminated through international peer-reviewed journals. After the publication of these results, all the data would be available on request by contacting the corresponding author of this study.
Acknowledgments
We appreciate all the valuable assistance and advice from the colleagues in the Department of Endocrinology and Metabolism, Peking University Third Hospital.
Funding
This work was supported by the National Natural Science Foundation of China (82070319, 82371588) and the special fund of the National Clinical Key Specialty Construction Program, P. R. China (2023).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chinese Society of Endocrinology. Consensus of experts on prevention and treatment of adult obesity in China. Chin J Endocrinol Metab. 2011;27(9):711–717. doi:10.3760/cma.j.issn.1000-6699.2011.09.003
2. World Health Organization. Obesity and overweight Fact sheet, 2021. https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
3. Pi-Sunyer FX. The obesity epidemic: pathophysiology and consequences of obesity. Obes Res. 2002;10(Suppl 2):97S–104S. doi:10.1038/oby.2002.202
4. Kennedy AP, Shea JL, Sun G. Comparison of the classification of obesity by BMI vs. dual-energy X-ray absorptiometry in the Newfoundland population. Obesity. 2009;17(11):2094–2099. doi:10.1038/oby.2009.101
5. Lorenzo AD, Martinoli R, Vaia F, et al. Normal weight obese (NWO) women: an evaluation of a candidate new syndrome. Nutr Metab Cardiovasc Dis. 2006;16(8):513–523. doi:10.1016/j.numecd.2005.10.010
6. De Lorenzo A, Pellegrini M, Gualtieri P, et al. The risk of sarcopenia among adults with normal-weight obesity in a nutritional management setting. Nutrients. 2022;14(24):5295. doi:10.3390/nu14245295
7. Kim J, Kang S, Kang H. Normal-weight obesity and metabolic syndrome in Korean adults: a population-based cross-sectional study. Healthcare. 2023;11(16):2303. doi:10.3390/healthcare11162303
8. Ccnds C, Mlbm B, de Oliveira BR, et al. Incidence of metabolic syndrome in adults with healthy weight, normal weight obesity, and overweight/obesity. Nutrition. 2021;85:111134. doi:10.1016/j.nut.2020.111134
9. Yao Y, Liu W, Zhang X, et al. Normal weight obesity is associated with lower AFC and adverse IVF outcomes. Front Endocrinol. 2024;15. doi:10.3389/fendo.2024.1332995
10. Kim J, Kang S, Kang H. Association between normal-weight obesity and bone mineral density in older Korean adults: a population-based cross-sectional study. Maturitas. 2024;180:107891. doi:10.1016/j.maturitas.2023.107891
11. De Lorenzo A, Del Gobbo V, Premrov MG, et al. Normal-weight obese syndrome: early inflammation? Am J Clin Nutr. 2007;85(1):40–45. doi:10.1093/ajcn/85.1.40
12. Čuta M, Bařicová K, Černý D, et al. Normal-weight obesity frequency in the Central European urban adult female population of Brno, Czech Republic. Cent Eur J Public Health. 2019;27(2):131–134. doi:10.21101/cejph.a5133
13. Marques-Vidal P, Pécoud A, Hayoz D, et al. Normal weight obesity: relationship with lipids, glycaemic status, liver enzymes and inflammation. Nutr Metab Cardiovasc Dis. 2010;20(9):669–675. doi:10.1016/j.numecd.2009.06.001
14. Kim MK, Han K, Kwon HS, et al. Normal weight obesity in Korean adults. Clin Endocrinol. 2014;80(2):214–220. doi:10.1111/cen.12162
15. Maitiniyazi G, Chen Y, Qiu YY, et al. Characteristics of body composition and lifestyle in Chinese university students with normal-weight obesity: a cross-sectional study. Diabetes Metab Syndr Obes. 2021;14:3427–3436. doi:10.2147/DMSO.S325115
16. Zhang M, Schumann M, Huang T, et al. Normal weight obesity and physical fitness in Chinese university students: an overlooked association. BMC Public Health. 2018;18(1):1334. doi:10.1186/s12889-018-6238-3
17. Romero-Corral A, Somers VK, Sierra-Johnson J, et al. Normal weight obesity: a risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur Heart J. 2010;31(6):737–746. doi:10.1093/eurheartj/ehp487
18. Gallagher D, Heymsfield SB, Heo M, et al. Healthy percentage body fat ranges: an approach for developing guidelines based on body mass index. Am J Clin Nutr. 2000;72(3):694–701. doi:10.1093/ajcn/72.3.694
19. Haghighat N, Ashtary-Larky D, Bagheri R, et al. Effects of 6 months of soy-enriched high protein compared to eucaloric low protein snack replacement on appetite, dietary intake, and body composition in normal-weight obese women: a randomized controlled trial. Nutrients. 2021;13(7):2266. doi:10.3390/nu13072266
20. Hu J, Liu M, Yang R, et al. Effects of high-intensity interval training on improving arterial stiffness in Chinese female university students with normal weight obese: a pilot randomized controlled trial. J Transl Med. 2022;20(1):60. doi:10.1186/s12967-022-03250-9
21. Wilkinson MJ, Manoogian ENC, Zadourian A, et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020;31(1):92–104.e5. doi:10.1016/j.cmet.2019.11.004
22. Haghighat N, Ashtary-Larky D, Bagheri R, et al. The effect of 12 weeks of euenergetic high-protein diet in regulating appetite and body composition of women with normal-weight obesity: a randomised controlled trial. Br J Nutr. 2020;124(10):1044–1051. doi:10.1017/S0007114520002019
23. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus. 2021;13(4):315–409. doi:10.3760/cma.j.cn115791-20210221-00095
24. Bruce RA, Blackmon JR, Jones JW, et al. Exercising testing in adult normal subjects and cardiac patients. 1963. Ann Noninvasive Electrocardiol. 2004;9(3):291–303. doi:10.1111/j.1542-474X.2004.93003.x
25. Ross R, Blair SN, Arena R, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation. 2016;134(24):e653–e699. doi:10.1161/CIR.0000000000000461
26. Ruiz-Ruiz J, Mesa JLM, Gutiérrez A, et al. Hand size influences optimal grip span in women but not in men. J Hand Surg Am. 2002;27(5):897–901. doi:10.1053/jhsu.2002.34315
27. Rikli RE, Jones CJ. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical Independence in later years. Gerontologist. 2013;53(2):255–267. doi:10.1093/geront/gns071
28. Adams R. Revised physical activity readiness questionnaire. Can Fam Physician. 1999;992(995):1004–1005.
29. Warburton DE, Jamnik VK, Bredin SS, et al. The physical activity readiness questionnaire for everyone (PAR-Q+) and electronic physical activity readiness medical examination (ePARmed-X+). The Health Fitness J Canada. 2011;4(2):3–17. doi:10.14288/hfjc.v4i2.103
30. Ogawa H, Fujitani K, Tsujinaka T, et al. InBody 720 as a new method of evaluating visceral obesity. Hepatogastroenterology. 2011;58(105):42–44.
31. Volgyi E, Tylavsky FA, Lyytikainen A, et al. Assessing body composition with DXA and bioimpedance: effects of obesity, physical activity, and age. Obesity. 2008;16(3):700–705. doi:10.1038/oby.2007.94
32. Moore GF, Audrey S, Barker M, et al. Process evaluation of complex interventions: medical research council guidance. BMJ. 2015;350:h1258. doi:10.1136/bmj.h1258
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.