Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Diaphragmatic Thickening Fraction and Excursion: Different Clinical Values in Non-Critically Ill Patients with AECOPD — An Exploratory Study
Received 10 March 2026
Accepted for publication 9 June 2026
Published 13 June 2026 Volume 2026:21 608108
DOI https://doi.org/10.2147/COPD.S608108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Xun Yang,1,* Liangdong Zhu,2,* Ruijie Ren3
1Department of Respiratory and Critical Care Medicine, Chongqing Hospital of Jiangsu Province Hospital, Chongqing, 401420, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, The First Hospital of Changsha, Changsha, 410005, People’s Republic of China; 3Department of Ultrasound Medicine, Chongqing Hospital of Jiangsu Province Hospital, Chongqing, 401420, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xun Yang, Department of Respiratory and Critical Care Medicine, Chongqing Hospital of Jiangsu Province Hospital, Chongqing, 401420, People’s Republic of China, Email [email protected]
Purpose: Diaphragm dysfunction is a key mechanism of respiratory failure during acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Diaphragmatic thickening fraction (DTF) and excursion (DE) are commonly used ultrasound parameters, but their clinical value in non-critically ill AECOPD patients remains unclear. This study aimed to investigate the association of early DTF and DE with subsequent noninvasive ventilation (NIV) requirement and treatment response.
Patients and Methods: This retrospective observational study enrolled AECOPD patients admitted between December 2025 and January 2026. DTF and DE were measured within 24 hours of admission and before NIV initiation. Primary outcomes were NIV requirement within 48 hours, and among NIV recipients, the difference in ultrasound parameters between treatment responders and non-responders. Multivariable logistic regression assessed whether DTF provided incremental information beyond traditional clinical predictors.
Results: Of 123 included patients, 56 received NIV. DTF was significantly higher in the NIV group than in the non-NIV group (P=0.033), while DE did not differ. After adjusting for traditional clinical indicators, DTF was no longer significant (P=0.121). Among NIV-treated patients, DE was significantly higher in responders than in non-responders (P=0.015), while DTF did not differ.
Conclusion: In non-critically ill AECOPD patients, elevated DTF is associated with NIV requirement but does not provide independent predictive information beyond traditional clinical indicators. DE is associated with NIV treatment response and may reflect diaphragmatic contractile reserve. These exploratory findings, including subgroup analyses and threshold estimates, require prospective validation before clinical application. The two parameters have distinct clinical values, and their interpretation should consider disease stage.
Keywords: AECOPD, noninvasive ventilation, diaphragmatic ultrasound, diaphragmatic thickening fraction, diaphragmatic excursion
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the diseases with the highest morbidity and mortality worldwide,1,2 and acute exacerbations (AECOPD) are key events leading to hospitalization and death.3,4 As the primary respiratory muscle, the diaphragm plays an important role in the development of respiratory failure during AECOPD. Diaphragmatic dysfunction, resulting from increased load, dynamic pulmonary hyperinflation, and systemic inflammation, directly affects ventilation capacity and increases the need for respiratory support.5,6
Bedside ultrasound enables non-invasive assessment of diaphragmatic function. Commonly used parameters include diaphragmatic excursion (DE) and diaphragmatic thickening fraction (DTF). DE primarily reflects the amplitude of diaphragmatic contraction and is related to ventilation capacity; DTF reflects the intensity of diaphragmatic contraction and may indirectly indicate diaphragmatic load.7 Currently, research on diaphragmatic ultrasound in COPD has mainly focused on intensive care units (ICU) or emergency departments, primarily investigating its value in predicting weaning from invasive ventilation or NIV failure.8–11 However, the majority of AECOPD patients are initially admitted to general wards, with relatively milder disease at an early stage. The diaphragmatic ultrasound characteristics of these patients within 24 hours of admission, whether DE and DTF differ between those who require NIV and those who do not, and whether these two parameters may reflect different clinical values, remain unclear. Research specifically targeting non‑critically ill AECOPD patients in general wards is lacking.8
Therefore, this retrospective observational study aimed to: (1) describe the early DE and DTF characteristics of non‑critically ill AECOPD patients; (2) compare DE and DTF between patients requiring NIV and those not requiring NIV; (3) assess whether DTF provides incremental information beyond traditional clinical indicators using multivariable regression analysis; and (4) explore the possible associations of DE and DTF with NIV treatment response and comorbidities, providing preliminary insights into their distinct clinical values in AECOPD management.
Materials and Methods
Study Design and Population
This single-center retrospective observational study consecutively enrolled AECOPD patients admitted to the Department of Respiratory and Critical Care Medicine, Chongqing Hospital of Jiangsu Province Hospital, between December 2025 and January 2026, who underwent bedside diaphragmatic ultrasound examination within 24 hours of admission.
Inclusion Criteria
(1) AECOPD meeting the GOLD diagnostic criteria;12 (2) age ≥18 years; (3) bedside diaphragmatic ultrasound completed within 24 hours of admission.
Exclusion Criteria
(1) immediate need for invasive mechanical ventilation upon admission; (2) incomplete clinical data precluding acquisition of key variables (eg., arterial blood gas, outcome measures).
The patient selection process is shown in Figure 1.
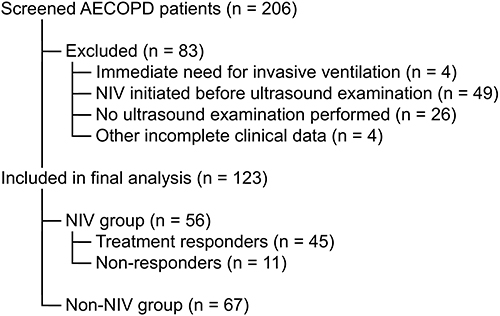 |
Figure 1 Flowchart of patient selection. A total of 206 patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) were screened. After excluding 83 patients (immediate need for invasive ventilation, n=4; noninvasive ventilation initiated before ultrasound examination, n=49; no ultrasound examination performed, n=26; incomplete clinical data, n=4), 123 patients were included in the final analysis. Of these, 56 patients received noninvasive ventilation (NIV) within 48 hours of admission (NIV group), among whom 45 were treatment responders (remained on NIV without escalation to invasive ventilation or ICU transfer) and 11 were non responders (required invasive ventilation or ICU transfer). The remaining 67 patients did not receive NIV (non NIV group). Abbreviation: NIV, noninvasive ventilation. |
This study was approved by the Ethics Committee of Chongqing Hospital of Jiangsu Province Hospital (Approval No. KY2026-003). The requirement for informed consent was waived due to the retrospective design. Patient data confidentiality was strictly maintained in accordance with the hospital’s data protection policy.
The Rome criteria for AECOPD severity classification were not used in this study, as the study period (December 2025 – January 2026) predated the routine documentation of these criteria in our electronic medical records.
Diaphragmatic Ultrasound Measurements
Diaphragmatic ultrasound examinations were performed by a single respiratory physician trained in diaphragmatic ultrasound. The measurement protocols followed published recommendations for diaphragmatic ultrasound.7 The operator performed only the examination and did not intervene in patient outcomes. All examinations were completed within 24 hours of admission and before NIV initiation. Patients were placed in a semi-recumbent position and instructed to breathe quietly to minimize the impact of respiratory state variation on measurements. The measured parameters included diaphragmatic excursion (DE) and diaphragmatic thickening fraction (DTF), with the following methods:
DE measurement: A low-frequency convex probe (2–5 MHz) was placed in the right subcostal region, using the liver as an acoustic window. M-mode ultrasound was used with the sampling line perpendicular to the dome of the diaphragm. The vertical distance of diaphragmatic movement from end-expiration to peak inspiration during quiet breathing was measured. Three consecutive respiratory cycles were measured, and the average value was taken as the final DE (unit: cm).
DTF measurement: A high-frequency linear probe (6–13 MHz) was placed in the right 8th–10th intercostal space at the mid-axillary line to clearly visualize the three-layered structure of pleura–diaphragm–peritoneum. In B-mode, diaphragm thickness at end-expiration (DTE) and at peak inspiration (DTI) was measured, avoiding blood vessels and the pleural/peritoneal lines. DTF was calculated as: DTF = (DTI – DTE) / DTE × 100%. Three consecutive respiratory cycles were measured, and the average value was taken as the final DTF (unit: %).
NIV Definition and Objective Criteria Assessment
Patients were divided into NIV group and non-NIV group based on whether they received noninvasive ventilation within 48 hours of admission. NIV use was recorded from the electronic medical order system and nursing records. All NIV treatments were initiated by attending physicians based on comprehensive assessment of clinical presentation and arterial blood gas results.
To assess whether patients met objective clinical criteria for NIV initiation, two researchers independently reviewed medical records, including vital signs, arterial blood gas results, nursing records, and physician progress notes within 48 hours of admission. Referring to the GOLD 2025 report and relevant national guidelines,12 objective clinical criteria for NIV initiation included: (1) worsening gas exchange: arterial pH <7.35 and PaCO2 >45 mmHg; (2) signs of respiratory distress: respiratory rate >25 breaths/min, with use of accessory muscles or paradoxical abdominal breathing; (3) refractory hypoxemia: SpO2 persistently <92% despite oxygen therapy via nasal cannula or face mask (oxygen flow ≥5 L/min). Researchers judged whether patients met at least one of these criteria within 48 hours of admission. Disagreements were resolved through discussion or by a third researcher. This judgment was not used to reclassify NIV groups but only for sensitivity analysis to assess the consistency between actual NIV use and objective criteria.
In the NIV group, patients who did not require escalation to invasive mechanical ventilation or ICU transfer during hospitalization were defined as “treatment responders”; those who required endotracheal intubation or ICU transfer were defined as “non-responders”.
Data Collection
The following data were collected from the electronic medical record system: (1) demographic characteristics: age, sex, body mass index (BMI); (2) comorbidities: hypertension, coronary heart disease, diabetes mellitus, pulmonary arterial hypertension (diagnosed by echocardiography); (3) disease severity: APACHE II score within 24 hours of admission, respiratory rate; (4) laboratory and blood gas parameters: arterial pH, PaCO2, PaO2/FiO2, NT-proBNP, eosinophil count; (5) functional scores: Nutritional Risk Screening 2002 (NRS‑2002), Activities of Daily Living (ADL) score; (6) hospitalization outcomes: NIV use, NIV efficacy, ICU transfer, invasive ventilation.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and R 4.1.0. Continuous variables were first tested for normality using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation and compared using the independent samples t-test. Non-normally distributed data are presented as median (interquartile range) [M (Q1, Q3)] and compared using the Mann–Whitney U-test. Categorical variables are presented as frequency (%) and compared using the χ2-test or Fisher’s exact test.
To assess whether diaphragmatic ultrasound parameters (DTF, DE) provided incremental information beyond traditional NIV initiation indicators, multivariable binary logistic regression analysis (Enter method) was performed, including respiratory rate, pH, PaCO2, PaO2/FiO2, DE, and DTF simultaneously in the model, with NIV requirement as the dependent variable. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. Model goodness‑of‑fit was evaluated using the Hosmer-Lemeshow test.
Subgroup analyses: (1) DE and DTF were compared between patients with and without hypertension, diabetes mellitus, coronary heart disease, and pulmonary arterial hypertension using the Mann–Whitney U-test; (2) in the NIV group, DE and DTF were compared between treatment responders and non-responders using the Mann–Whitney U-test.
Exploratory ROC curve analysis: (1) in the overall cohort of 123 patients, the predictive performance of DTF for NIV requirement was analyzed; (2) in the 56 patients receiving NIV, the predictive performance of DE for NIV failure (defined as need for invasive ventilation or ICU transfer) was analyzed. Area under the curve (AUC) and 95% CI were calculated. The optimal cut‑off value was determined by the Youden index (sensitivity + specificity – 1), and the corresponding sensitivity and specificity were reported. Due to the small sample size and low AUC values, ROC results are presented only as exploratory findings and are not emphasized in the main text.
All tests were two‑sided, and P < 0.05 was considered statistically significant.
Results
Patient Selection and Baseline Characteristics
A total of 206 AECOPD patients were screened. After excluding 83 patients, 123 were included in the final analysis (Figure 1). Reasons for exclusion included: immediate need for invasive ventilation (n=4), NIV initiated before ultrasound examination (n=49), no ultrasound examination performed (n=26, mainly due to pneumothorax/pleural effusion [n=18] or inability to cooperate with the examination position [n=8]), and missing key covariates (prealbumin/NT-proBNP) (n=4). Of the 123 included patients, 56 (45.5%) received NIV within 48 hours of admission (NIV group), and 67 (54.5%) did not receive NIV (non-NIV group).
Baseline characteristics of the two groups are compared in Table 1. There were no significant differences in age, sex, or BMI between the NIV and non-NIV groups (all P > 0.05). Compared with the non-NIV group, patients in the NIV group had higher APACHE II scores, respiratory rates, PaCO2 levels, and NT-proBNP levels; lower pH, PaO2/FiO2 ratios, ADL scores, and eosinophil counts; and a higher proportion of pulmonary arterial hypertension (all P < 0.05).
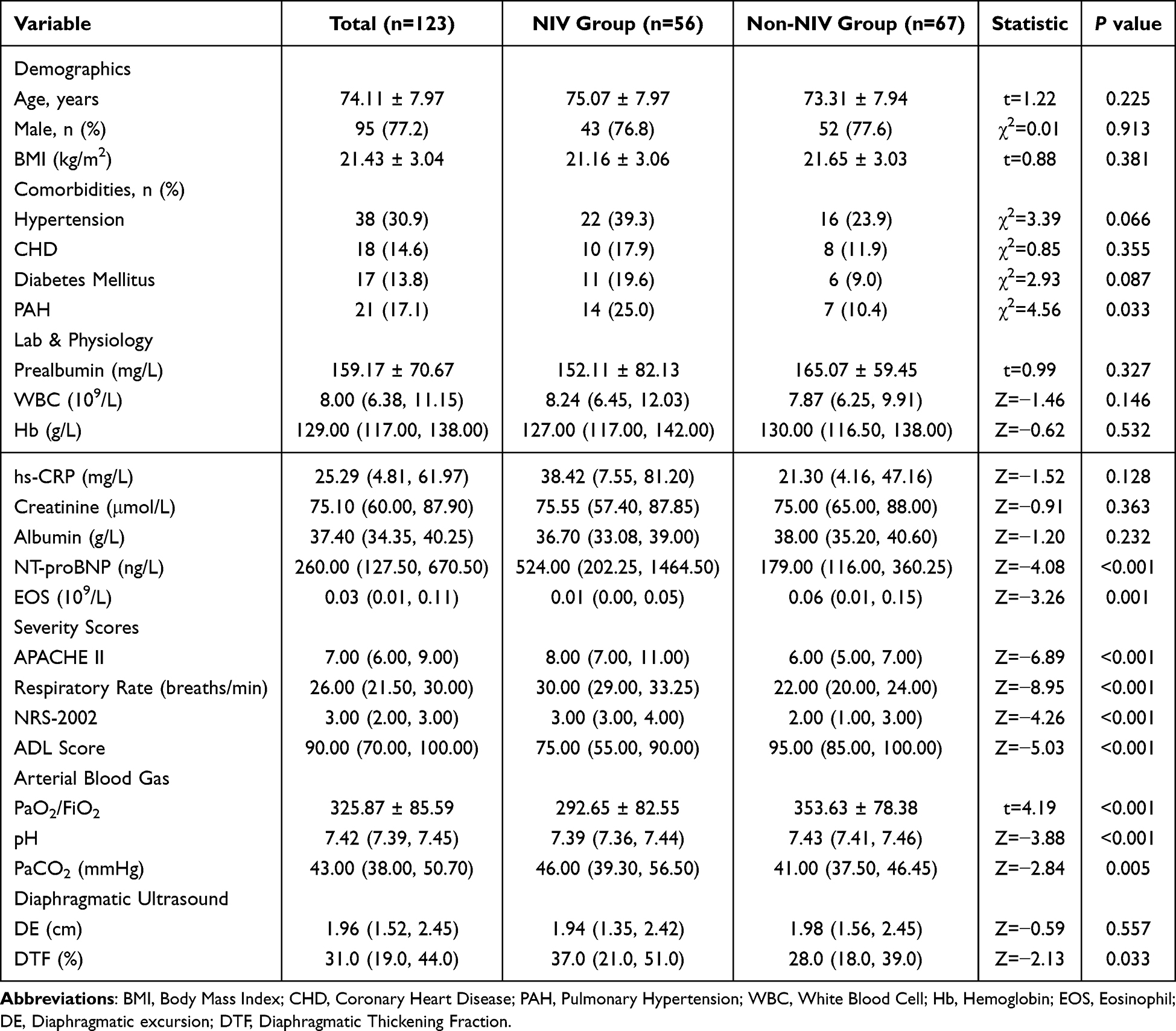 |
Table 1 Comparison of Clinical Data Between NIV Group and Non-NIV Group |
Comparison of Diaphragmatic Ultrasound Parameters
DTF was significantly higher in the NIV group than in the non-NIV group [37.0% (21.0%, 51.0%) vs. 28.0% (18.0%, 39.0%), P = 0.033]; DE did not differ significantly between the two groups [1.94 (1.35, 2.42) cm vs. 1.98 (1.56, 2.45) cm, P = 0.557] (Table 1).
Multivariable Regression Analysis: Incremental Value of DTF
To assess whether DTF provided independent information beyond traditional NIV initiation indicators, respiratory rate, pH, PaCO2, PaO2/FiO2, DE, and DTF were simultaneously entered into a logistic regression model (Enter method). The results showed that only respiratory rate was independently associated with NIV requirement (OR = 2.272, 95% CI 1.607–3.212, P < 0.001), while DTF did not reach statistical significance (OR = 1.033, 95% CI 0.991–1.076, P = 0.121). The Hosmer-Lemeshow test indicated good model fit (P = 0.635). Detailed results are shown in Table 2. This finding suggests that DTF does not provide additional predictive information beyond traditional clinical indicators for NIV initiation.
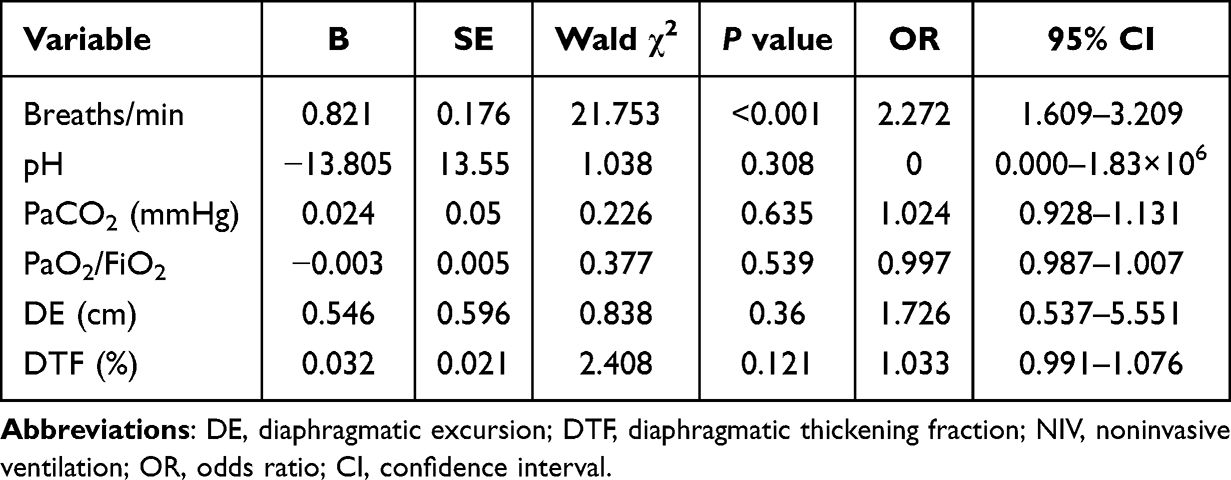 |
Table 2 Multivariate Logistic Regression Analysis: Incremental Value of DTF Beyond Traditional Predictors for NIV Requirement |
Exploratory Analysis of DTF and DE Thresholds
Based on the baseline comparisons (Table 1 and NIV subgroup analysis), only DTF was associated with NIV requirement and only DE was associated with NIV treatment response. Therefore, we performed two exploratory ROC analyses: To explore potential cut-off values of diaphragmatic ultrasound parameters for clinical reference, receiver operating characteristic (ROC) curve analyses were performed. For predicting NIV requirement within 48 hours of admission (n=123), DTF yielded an area under the curve (AUC) of 0.61 (95% CI 0.51–0.71). The optimal cut‑off value determined by the Youden index was ≥41%, with a sensitivity of 82.0% and a specificity of 45.0% for identifying patients requiring NIV. Among the 56 patients receiving NIV, DE showed an AUC of 0.75 (95% CI 0.55–0.95) for predicting NIV failure (defined as need for invasive ventilation or ICU transfer). Using the optimal cut-off of ≤2.08 cm, the sensitivity was 90.9% and the specificity was 46.7% for identifying non-responders (Table 3).
 |
Table 3 ROC Curve Analysis of Diaphragmatic Ultrasound Parameters for Predicting NIV Requirement and NIV Failure |
Given the modest AUC values and the small number of events in the NIV failure subgroup (n=11), these threshold findings should be interpreted with caution. They are presented primarily as exploratory data to inform future studies and do not represent validated clinical cut-points, requiring confirmation in larger prospective cohorts.
Subgroup Analyses
In comorbidity subgroups, no significant differences in DTF or DE were observed between patients with and without hypertension (n=38), coronary heart disease (n=18), or pulmonary arterial hypertension (n=21) (all P > 0.05). A significant difference was observed only in the diabetes subgroup: diabetic patients had significantly higher DTF than non‑diabetic patients [41.67% (33.81%, 63.92%) vs. 27.78% (18.61%, 41.30%), P = 0.009]; DE did not differ between these groups (Table 4).
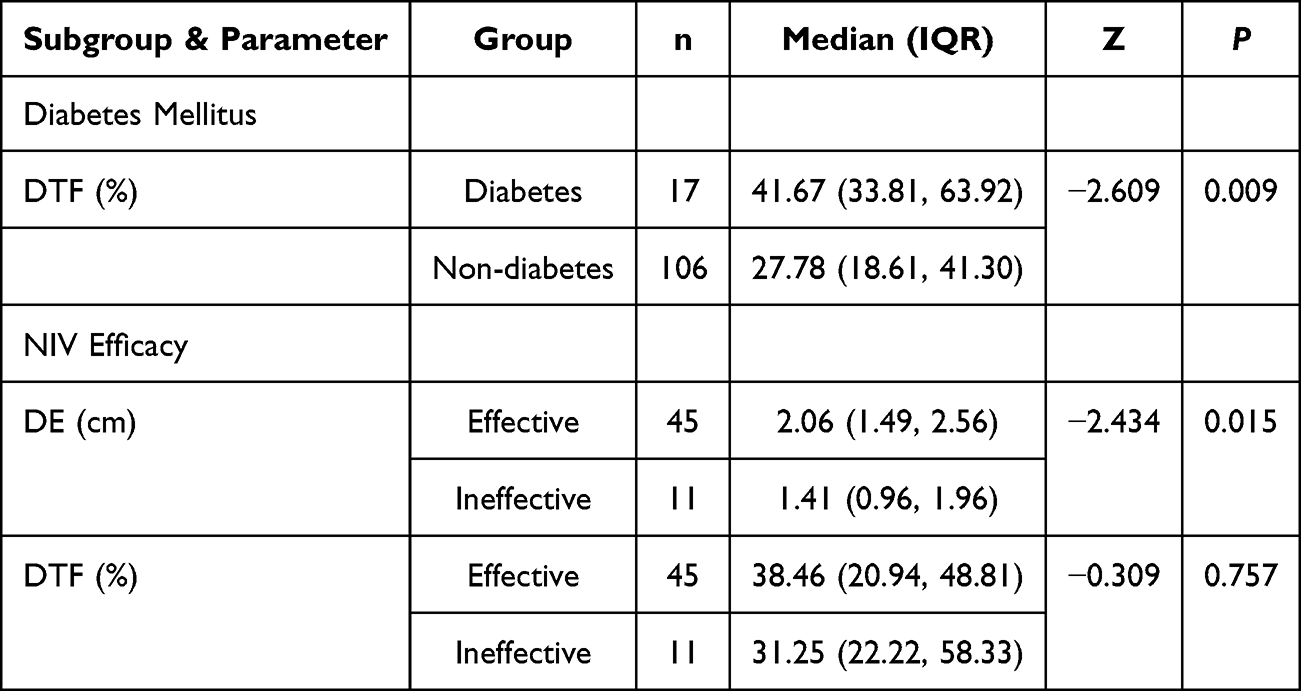 |
Table 4 Comparison of Diaphragmatic Ultrasound Parameters in Subgroup Analyses |
NIV efficacy subgroup: Of the 56 patients receiving NIV, 45 (80.4%) were treatment responders and 11 (19.6%) were non-responders. DE was significantly higher in responders than in non‑responders [2.06 (1.49, 2.56) cm vs. 1.41 (0.96, 1.96) cm, P = 0.015]; DTF did not differ significantly between the two groups [38.46% (20.94%, 48.81%) vs. 31.25% (22.22%, 58.33%), P = 0.757] (Table 4).
Sensitivity Analysis
Analysis of consistency between actual NIV use and objective criteria showed that among the 123 patients, 62 (50.4%) met at least one objective criterion for NIV initiation. Of these, 56 (90.3%) actually received NIV, and 6 (9.7%) did not receive NIV despite meeting the criteria. Overall agreement was 95.1%, with a Kappa value of 0.90, indicating a high degree of consistency between clinical decision-making and guideline criteria.
Discussion
This study, based on early diaphragmatic ultrasound measurements in 123 AECOPD patients admitted to general wards, yielded three main findings. First, DTF was significantly higher in patients requiring NIV, but this association was no longer independent after adjusting for traditional NIV initiation indicators (blood gas parameters and respiratory rate). Second, DE was closely associated with NIV treatment response, with non-responders having significantly lower DE than responders, while DTF did not differ between these efficacy subgroups. Third, diabetic patients had significantly higher DTF. These findings suggest that in non-critically ill AECOPD patients, early DTF and DE have different clinical values: DTF may reflect a real‑time diaphragmatic response to systemic load, while DE may be closer to reflecting actual ventilatory capacity and functional reserve.
The diaphragm plays a crucial role in AECOPD. Ottenheijm et al found that chronic hypoxia and systemic inflammation in COPD patients induce myofiber type shifting, fiber atrophy, and contractile protein dysfunction, leading to diaphragmatic weakness.13 Laghi and Tobin, in their classic review, highlighted that dynamic pulmonary hyperinflation-induced shortening of diaphragmatic initial length is a key mechanism of reduced diaphragmatic mechanical efficiency during AECOPD.14 These mechanisms provide a pathophysiological foundation for understanding the clinical significance of diaphragmatic ultrasound parameters. With the recent standardization of diaphragmatic ultrasound measurement methods,7,15 bedside ultrasound has become an important tool for assessing respiratory muscle function and has been shown to have value in predicting mechanical ventilation outcomes, evaluating prognosis, and guiding pulmonary rehabilitation in AECOPD patients.16–25
Comparing the present findings with previous studies reveals a spectrum based on disease severity. Marchioni et al24 included more severely ill AECOPD patients (median APACHE II score 22) and found that DTF <20% was an independent predictor of NIV failure. Qu et al17 observed in AECOPD patients undergoing invasive mechanical ventilation that successful weaning was associated with significantly higher DTF (approximately 42.5% vs. 27.1%). Both studies in critically ill patients showed an association between low DTF and adverse outcomes. In a moderately ill population (median APACHE II score 15), Cammarota et al18 found that DE (but not DTF) was an independent predictor of NIV failure, with DE <1 cm indicating significantly higher failure risk. This finding aligns with the present study in milder patients (median APACHE II score 7), where DE was significantly lower in NIV non-responders, while DTF did not differ between response groups. Synthesizing these findings, a disease-stage-dependent pattern emerges, which is conceptually illustrated in Figure 2. In the earliest stage (as in the present study), elevated DTF may indicate a “high-load compensatory state” of the diaphragm. Although not an independent determinant of NIV requirement, as an organ-level reflection of overall disease severity, it may serve as a reference for early identification of high-risk patients. As the disease progresses to a moderate stage (as in the Cammarota study),18 diaphragmatic contractile amplitude becomes more impaired, and the predictive value of DE becomes prominent. When progressing to ICU-level severe respiratory failure, reduced DTF becomes a clear marker of diaphragmatic decompensation.17,24 Decompensation implies a higher risk of NIV failure and extubation failure. In contrast, patients with preserved DE and DTF (ie., retained diaphragmatic function) are more likely to have a favorable treatment response to NIV or invasive ventilation.11 These observations suggest that the clinical interpretation of diaphragmatic ultrasound parameters is highly context-dependent and must be closely linked to the patient’s specific disease stage. The dissociation between DE and DTF observed in a retrospective study by An et al26 and a case report27 further supports the notion that these two parameters may reflect different dimensions of diaphragmatic function.
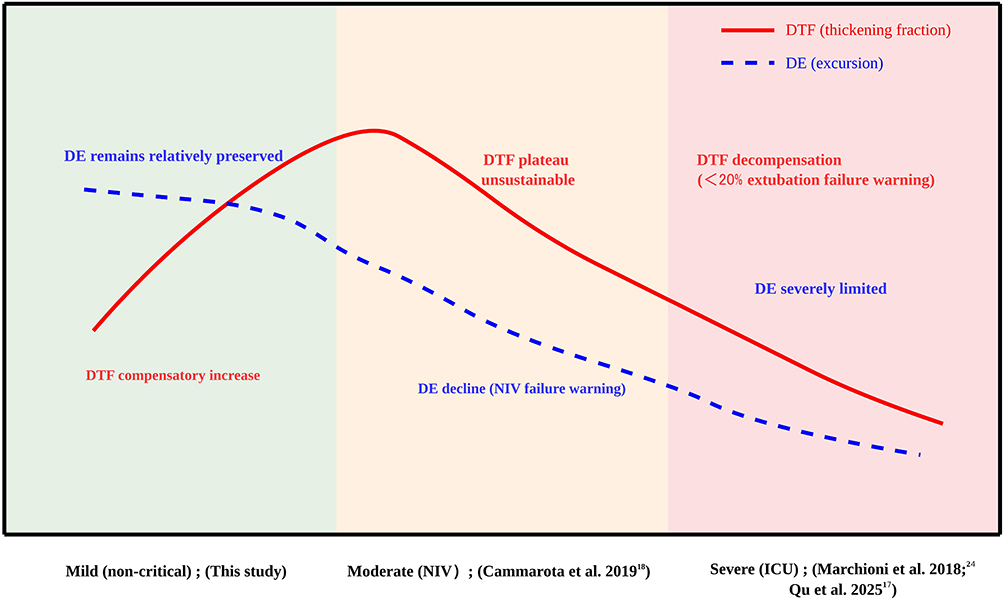 |
Figure 2 Hypothetical model of the evolution of diaphragm ultrasound parameters with AECOPD severity. The graph illustrates the proposed trajectory of diaphragmatic thickening fraction (DTF, solid line) and diaphragmatic excursion (DE, dashed line) across the spectrum of AECOPD severity, from mild (non‑critical) to severe (ICU). In the mild stage (represented by the current study), DTF is elevated, reflecting compensatory hyperfunction under increased load, while DE remains relatively preserved. As disease progresses to moderate severity requiring noninvasive ventilation (based on Cammarota et al18), DTF plateaus or becomes unsustainable, and DE begins to decline, signalling depletion of functional reserve and warning of NIV failure. In the severe stage (ICU, based on Marchioni et al24 and Qu et al17), both parameters decrease: DTF falls below normal, suggesting a possible risk of extubation failure, and DE becomes severely limited. This model underscores the stage‑dependent interpretation of DTF and DE in AECOPD. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; DTF, diaphragmatic thickening fraction; DE, diaphragmatic excursion; NIV, noninvasive ventilation; ICU, intensive care unit. |
This pattern is consistent with the review by Zhao et al,28 which systematically discussed the “commonality and conflict” between DE and DTF, indicating that they reflect diaphragmatic efficiency and contractile intensity, respectively. When respiratory load increases acutely, DTF may increase to maintain ventilation, while DE may be limited by factors such as pulmonary hyperinflation. Conversely, in some situations, DE may increase while DTF decreases. Poddighe et al29 further emphasized that assessment of respiratory muscle dysfunction should distinguish between the dimensions of “load” and “capacity” throughout the course of acute and chronic respiratory failure, consistent with the hypothesis derived from the present disease spectrum analysis.
This study further explored whether DTF provides incremental information beyond traditional indicators. The results showed that the association between DTF and NIV requirement was not independent after adjustment, suggesting that diaphragmatic function is an integral part of the systemic disease state, with parameters often correlated with overall disease severity.24 Global clinical scores such as APACHE II,30 NRS-2002,31 and ADL32 have been shown to be closely associated with prognosis in COPD patients. Diaphragmatic parameters, as organ-level measurements, may complement these scores. In the present study, patients requiring NIV exhibited worse status across multiple dimensions, including organ function (DTF), overall disease severity (APACHE II), nutritional status (NRS-2002), and activities of daily living (ADL). This suggests that NIV requirement is not driven by any single abnormal indicator but reflects a comprehensive deterioration of the patient’s overall condition. Therefore, as one component of this multi-dimensional assessment, the clinical significance of diaphragmatic parameters should not be interpreted in isolation but rather understood within the context of the overall disease state. The value of DTF lies not in replacing traditional indicators but in providing another window for observing the organ-level response to systemic load.
Subgroup analyses provided further clinical insights. In the present study, diabetic patients had significantly higher DTF and a higher rate of NIV use. This phenomenon suggests that diabetic patients may enter a state of high diaphragmatic load compensation earlier during acute exacerbations, with functional reserve more prone to depletion. This mechanism may partly explain why diabetes is recognized as an independent risk factor for poor prognosis in COPD patients.33 Diabetes-related metabolic abnormalities, microvascular complications, and accumulation of advanced glycation end-products may impair diaphragmatic fiber structure and function,34 predisposing to decompensation under acute stress. Therefore, early attention to diaphragmatic function and enhanced respiratory support monitoring may be particularly important for AECOPD patients with diabetes.
Based on the findings of this study and the literature spectrum, we propose a hypothesis for future validation: the interpretation of diaphragmatic ultrasound parameters should be disease-stage dependent. In milder disease, elevated DTF reflects compensatory diaphragmatic effort and may serve as a reference indicator of disease severity. In moderate disease, reduced DE may warn of NIV failure. In severe disease, reduced DTF may predict adverse outcomes. If validated, this hypothesis would help explain discrepancies in the predictive value of diaphragmatic parameters across different studies and provide a basis for individualized application of diaphragmatic ultrasound. DTF and DE should be interpreted jointly: DTF reflects the degree of effort under load, while DE is closer to representing functional reserve and actual ventilatory capacity. In diabetic patients, even with milder disease, diaphragmatic function warrants attention.
Limitations
This study has several limitations. First, as a single-center retrospective study, inherent selection bias is possible. Although data collection followed prospective principles (consecutive enrollment, standardized measurements, strict time windows) and sensitivity analysis showed high consistency between clinical decisions and guideline criteria (Kappa = 0.90), unmeasured confounding factors may exist. Second, due to the retrospective design, although a single trained operator performed all ultrasound measurements and averaging over three cycles reduced random error, intra-operator reproducibility could not be assessed. Measurement results may still contain potential intra-operator variability. Future prospective studies should include intra- and inter-operator reliability testing to further standardize measurements.No formal sample size calculation was performed given the exploratory nature of this study. Third, the sample size was relatively small, particularly in the NIV efficacy subgroup analysis, with only 11 non-responders. The small number of positive events limited the power of multivariable analysis and may have led to overestimation of the predictive value of DE, and the stability of the optimal DE cut-off (≤2.08 cm) determined by ROC analysis is questionable. The AUC for DTF predicting NIV requirement was only 0.61, indicating limited clinical utility. Therefore, all threshold-related findings should be considered exploratory and require external validation in larger prospective cohorts. Fourth, this study examined diaphragmatic characteristics only at a single early time point and did not capture dynamic changes in diaphragmatic function, which may evolve rapidly during early AECOPD.
Despite these limitations, as an exploratory study, by contextualizing its findings within the continuous spectrum of studies across different disease severities, this study provides a preliminary framework for understanding the potential value of diaphragmatic ultrasound at different stages of AECOPD. It should be emphasized that this framework is based on an integrated interpretation of previous prospective studies, which have heterogeneity in population selection, measurement methods, and outcome definitions. Therefore, it should be regarded as a hypothesis-generating starting point, not conclusive evidence, and requires cautious interpretation. Future prospective multicenter studies are needed to validate the stage-dependent interpretation of DTF and DE in AECOPD.
The primary intention of this study is to provide directions for future prospective research. Future studies should focus on: first, conducting multi-center prospective studies with standardized measurement methods and reliability testing to validate the disease-stage-dependent evolution pattern of diaphragmatic parameters; second, performing dynamic monitoring studies to explore the transition markers and time window from compensation to decompensation; third, combining biomarkers to investigate the molecular mechanisms of diabetes affecting diaphragmatic function; and fourth, developing multi-dimensional assessment models integrating diaphragmatic parameters and clinical scores to achieve individualized risk stratification and explore their value in guiding respiratory support strategies and pulmonary rehabilitation.
Conclusion
In non-critically ill AECOPD patients, the diaphragmatic ultrasound parameters DTF and DE demonstrated distinct clinical values. Early elevation of DTF primarily reflected overall disease severity associated with NIV requirement and did not provide independent incremental predictive information. In contrast, DE was associated with NIV treatment response, with significantly higher DE in responders, suggesting that DE may reflect diaphragmatic contractile reserve. However, these findings are exploratory and require prospective validation before clinical application. The observation of higher DTF in diabetic patients is exploratory and should be interpreted with caution. Therefore, the interpretation of DTF and DE should be integrated with consideration of disease stage and patient background, while awaiting confirmation from larger prospective studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Chongqing Hospital of Jiangsu Province Hospital (Approval No. KY2026-003). The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study.Patient data confidentiality was strictly maintained in accordance with the hospital’s data protection policy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Project of Qijiang District, Chongqing (Grant No. 2025065).
Disclosure
The authors declare no competing interests in this work.
References
1. Momtazmanesh S, Moghaddam SS, Ghamari S-H; GBD. Chronic respiratory diseases collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
2. Halpin DMG, Celli BR, Criner GJ, et al. The GOLD Summit on chronic obstructive pulmonary disease in low- and middle-income countries. Int J Tuberc Lung Dis. 2019;23(11):1131–11. doi:10.5588/ijtld.19.0397
3. Seemungal TERENCEAR, Donaldson GC, Paul EA, et al. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5):1418–1422. doi:10.1164/ajrccm.157.5.9709032
4. Soler-Cataluna JJ, Martínez-García MÁ, Sánchez PR, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
5. Gosker HR, Schols AM, Wouters EF. Mechanisms of striated muscle dysfunction during acute exacerbations of COPD. J Appl Physiol. 2013;114(2):205–213. doi:10.1152/japplphysiol.00847.2012
6. Barreiro E, Gea J. Respiratory and limb muscle dysfunction in COPD. COPD. 2015;12(4):413–426. doi:10.3109/15412555.2014.974737
7. Haaksma ME, Smit JM, Boussuges A, et al. EXpert consensus on diaphragm ultrasonography in the critically ill (EXODUS): a Delphi consensus statement on the measurement of diaphragm ultrasound-derived parameters in a critical care setting. Crit Care. 2022;26(1):99. doi:10.1186/s13054-022-03975-5
8. Mu H, Zhang Q. The application of diaphragm ultrasound in chronic obstructive pulmonary disease: a narrative review. COPD. 2024;21(1):2331202. doi:10.1080/15412555.2024.2331202
9. Qu -L-L, Zhao W-P, Li J-P, Zhang W. Predictive value of diaphragm ultrasound for mechanical ventilation outcome in patients with acute exacerbation of chronic obstructive pulmonary disease. World J Clin Cases. 2024;12(26):5893–5900. doi:10.12998/wjcc.v12.i26.5893
10. Malhotra N, Gothi D, Kumar R, et al. Ultrasound-guided diaphragm evaluation and outcomes in severe acute exacerbation of chronic obstructive pulmonary disease (uDISCO Study): an observational study. Monaldi Arch Chest Dis. 2025. doi:10.4081/monaldi.2025.3483
11. Aksoy Y, Ozgultekin A, Balk Y, Ekinci O. Comparison of standardized diaphragm ultrasound measurement and conventional methods for predicting weaning failure: a prospective observational study. J Anesth. 2026. doi:10.1007/s00540-026-03724-w
12. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 report). Fontana, WI: Global Initiative for Chronic Obstructive Lung Disease; 2025. Available from: https://goldcopd.org/2025-gold-report/.
13. Ottenheijm CAC, Heunks LMA, Sieck GC, et al. Diaphragm dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172(2):200–205. doi:10.1164/rccm.200502-262OC
14. Laghi F, Tobin MJ. Disorders of the respiratory muscles. Am J Respir Crit Care Med. 2003;168(1):10–48. doi:10.1164/rccm.2206020
15. Goligher EC, Laghi F, Detsky ME, et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med. 2015;41(4):642–649. doi:10.1007/s00134-015-3687-3
16. Kocyigit H, Gunalp M, Genc S, Oguz AB, Koca A, Polat O. Diaphragm dysfunction detected with ultrasound to predict noninvasive mechanical ventilation failure: a prospective cohort study. Am J Emerg Med. 2021;45:202–207. doi:10.1016/j.ajem.2020.08.014
17. Qu L, Zhao W, Zhang W, Li J. Predictive value analysis of diaphragmatic ultrasound evaluation for mechanical ventilation outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm Med. 2025;25(1):478. doi:10.1186/s12890-025-03567-3
18. Cammarota G, Sguazzotti I, Zanoni M, et al. Diaphragmatic ultrasound assessment in subjects with acute hypercapnic respiratory failure admitted to the emergency department. Respir Care. 2019;64(12):1469–1477. doi:10.4187/respcare.06803
19. Goligher EC, Dres M, Fan E, et al. Mechanical Ventilation–induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. 2018;197(2):204–213. doi:10.1164/rccm.201703-0536OC
20. Suttapanit K, Lerdpaisarn P, Charoensuksombun C, et al. Diaphragmatic ultrasonographic evaluation as an assessment guide for predicting noninvasive ventilation failure in acute exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2025;93:13–20. doi:10.1016/j.ajem.2025.03.025
21. Hernandez Voth A, Sayas Catalan J, Corral Blanco M, et al. Long-term effect of noninvasive ventilation on diaphragm in chronic respiratory failure. Int J Chron Obstruct Pulmon Dis. 2022;17:205–212. doi:10.2147/COPD.S339498
22. Ran H, Chen Y, Zhang L, et al. A randomized controlled trial of graded exercise rehabilitation enhances diaphragm function and exercise tolerance in patients with AECOPD. Sci Rep. 2025;15(1):28510. doi:10.1038/s41598-025-09224-3
23. Lim SY, Lim G, Lee YJ, et al. Ultrasound assessment of diaphragmatic function during acute exacerbation of chronic obstructive pulmonary disease: a pilot study. Int J Chron Obstruct Pulmon Dis. 2019;14:2479–2484. doi:10.2147/COPD.S214716
24. Marchioni A, Castaniere I, Tonelli R, et al. Ultrasound-assessed diaphragmatic impairment is a predictor of outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease undergoing noninvasive ventilation. Crit Care. 2018;22(1):109. doi:10.1186/s13054-018-2033-x
25. Tabbì L, Marchioni A, Messina J, et al. Ultrasound-based evaluation of inspiratory muscle effort in patients with type 2 respiratory failure secondary to exacerbation of chronic obstructive pulmonary disease. Eur J Intern Med. 2026;145:106649. doi:10.1016/j.ejim.2025.106649
26. An TJ, Yoo YJ, Lim JU, et al. Diaphragm ultrasound is an imaging biomarker that distinguishes exacerbation status from stable chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:3–12. doi:10.2147/COPD.S341484
27. Kracht J, Ogna A, Fayssoil A. Dissociation between reduced diaphragm inspiratory motion and normal diaphragm thickening in acute chronic pulmonary obstructive disease exacerbation: a case report. Medicine. 2020;99(10):e19390. doi:10.1097/MD.0000000000019390
28. Zhao H, Liu K, Yan Y, Muhetaer Y, Li L. Diaphragm excursion and diaphragm thickening fraction: commonality and conflict. Eur Respir Rev. 2025;34(176):240285. doi:10.1183/16000617.0285-2024
29. Poddighe D, Van Hollebeke M, Rodrigues A, et al. Respiratory muscle dysfunction in acute and chronic respiratory failure: how to diagnose and how to treat? Eur Respir Rev. 2024;33(174):240150. doi:10.1183/16000617.0150-2024
30. Sweed RA, Shaheen MAEM, El Gendy EA. Usefulness of different prognostic scores for AECOPD: APACHE II, BAP65, 2008, and CAPS scores. Egypt J Bronchol. 2019;13(4):498–504. doi:10.4103/ejb.ejb_20_19
31. Chen R, Xing L, You C, Ou X. Prediction of prognosis in chronic obstructive pulmonary disease patients with respiratory failure: a comparison of three nutritional assessment methods. Eur J Intern Med. 2018;57:70–75. doi:10.1016/j.ejim.2018.06.006
32. Murakami Y, Yasui H, Sato J, et al. Predictors of poor clinical outcomes including in-hospital death and low ability to perform activities of daily living at discharge in hospitalized patients with chronic obstructive pulmonary disease exacerbation. Ther Adv Respir Dis. 2023;17:17534666231172924. doi:10.1177/17534666231172924
33. Wang Y, Stavem K, Dahl FA, Humerfelt S, Haugen T. Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2014;9:99–105. doi:10.2147/COPD.S51467
34. Callahan LA, Supinski GS. Hyperglycemia-induced diaphragm weakness is mediated by oxidative stress. Crit Care. 2014;18(3):R88. doi:10.1186/cc13855
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.