Back to Journals » International Journal of Women's Health » Volume 17
Diagnostic Value of MRI for Pelvic Lymph Node Extracapsular Invasion in Early-Stage Endometrial Carcinoma
Authors Bao Q, Zheng L, Hong L ![]()
Received 17 January 2025
Accepted for publication 16 April 2025
Published 17 May 2025 Volume 2025:17 Pages 1409—1419
DOI https://doi.org/10.2147/IJWH.S511642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Qiufang Bao,1,2 Liping Zheng,1 Linliang Hong3,4
1Department of Obstetrics and Gynecology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian Province, 350005, People’s Republic of China; 2Department of Obstetrics and Gynecology, The First Clinical College of Fujian Medical University, Fuzhou, Fujian Province, 350005, People’s Republic of China; 3Department of Pediatrics, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian Province, 350005, People’s Republic of China; 4Department of Pediatrics, the First Clinical College of Fujian Medical University, Fuzhou, Fujian Province, 350005, People’s Republic of China
Correspondence: Linliang Hong, Department of Pediatrics, The First Affiliated Hospital of Fujian Medical University, No. 20 Chazhong Road, Fuzhou, Fujian, 350005, People’s Republic of China, Tel +86-18850376822, Email [email protected]
Objective: Endometrial cancer (EC) is the major female malignant tumor in developed countries. MRI is frequently applied in gynecologic malignancies. We probed the diagnostic value of MRI for pelvic lymph node extracapsular invasion (PLNEI) in early-stage EC patients.
Methods: Totally 142 early-stage EC patients were retrospectively enrolled and divided into the PLNEInegative/PLNEIpositive groups. Differences in MRI parameters [volume index (VI), total tumor volume (TTV), tumor volume ratio (TVR), mean apparent diffusion coefficient (ADCmean)] were analyzed. Early-stage EC patients with PLNEI were categorized into the high/low VI, TTV, TVR, ADCmean groups. The relationships of VI, TTV, TVR and ADCmean with clinicopathological characteristics were analyzed. Independent influencing factors for PLNEI, and the diagnostic value of VI, TTV, TVR and ADCmean for PLNEI were analyzed by logistic univariate/multivariate regression and receiver operating characteristic curve, with differences in areas under the curves compared by Delong test.
Results: There were significant differences in the histological type, histological grade, myometrial invasion depth, LVSI positive detection, LVSI type, cervical involvement, and CA125 level between the two groups. The VI, TTV and TVR values were elevated and ADCmean value was reduced in patients with PLNEI, which were associated with the clinicopathological characteristics of early-stage EC patients. The CA125 level, VI, TTV, TVR and ADCmean were independent influencing factors for PLNEI, showing high diagnostic value for PLNEI.
Conclusion: VI, TTV, TVR, and ADCmean had high diagnostic value for PLNEI in early-stage EC patients. MRI was a good method to detect PLNEI in EC patients.
Keywords: endometrial carcinoma, magnetic resonance imaging, pelvic lymph node extracapsular invasion, mean apparent diffusion coefficient
Introduction
As the most common malignant tumor of the female reproductive system,1 endometrial carcinoma (EC) ranks as the fourth among cancers in women in developed countries.2 There are close to 200000 new cases per year globally.3 Treatment options for EC include radiotherapy, hormone therapy, surgery, and chemotherapy, with the choice of treatment mainly relying on staging.4 About 70% of patients with EC are diagnosed as stage I, and the overall prognosis is optimal, with 5-year survival rates of 74%-91%, but pelvic lymph node metastasis (LNM) still occurs in about 10% of patients in the early clinical phase, and LNM is associated with a poorer prognosis in EC.5 A prior study has shown specific expression of cancer antigen 125 (CA125) in EC patients.6 Notably, preoperative CA125 can act as a risk stratification predictor for EC LNM and lymphovascular space invasion (LVSI).7 Meanwhile, several studies have evidenced that serum CA125 predicts LNM.6,8 Lymph node extracapsular invasion (LNEI) refers to cancer cells breaking through the outer membrane of a lymph node and invading its surrounding tissues such as nerves, blood vessels, fat or muscle.9 It has been documented that LNEI is a common microscopic feature of LNM bound up with metastasis and recurrence in patients with tumors.10,11 What’s more, LNEI has been implicated as an important factor in poor prognosis in many tumors, such as thyroid cancer, bladder cancer, head and neck cancer.12–14 To date, there are relatively few studies on pelvic lymph node extracapsular invasion (PLNEI) in EC. Therefore, the diagnosis of PLNEI in patients with early-stage EC and accurate assessment of the disease are crucial for the prognosis of these patients.
Magnetic resonance imaging (MRI) is widely regarded as the most precise modality for the preoperative evaluation of EC, and is effective in assessing local extent and deep myometrial invasion of tumors in EC.15,16 The capability of MRI to provide multiplanar imaging, combined with its superior soft-tissue contrast resolution, enhances the identification of critical prognostic factors in low-risk patients, which informs subsequent treatment decisions.17 MRI has been demonstrated to be accurate in evaluating various prognostic indicators, including parametrial invasion, tumor size, lymph node invasion, and pelvic sidewall involvement.18 MR volumetric measurement can be utilized as a tool for tumor response evaluation, surgical planning, and prognosis assessment.19,20 Furthermore, quantitative parameters derived from MRI, such as volume index (VI), total tumor volume (TTV), tumor volume ratio (TVR), and mean apparent diffusion coefficient (ADCmean), can be utilized to assess tumor grade and LVSI. Among which, VI refers to products of maximum anterior-posterior, transverse, and cranial-caudal tumor diameters, TTV is defined as the tumor volume measured on fat-saturated T1-weighted postcontrast images, TVR is calculated as (TTV/TUV) * 100, and ADCmean is the mean of ADC value of the primary tumor, a normal, and a suspicious LN.21,22 It has been documented that VI > 15.29 is linked with high-risk tumors, and VI > 25.45 and TVR > 21.1 predict LVSI in EC.23 EC patients usually exhibit diffusion limitation and reduced ADC values.24,25 Nakamura et al have revealed that patients with lower ADC values display shorter disease-free survival than those with higher ADC values, and it can be regarded as an independent prognostic factor for disease recurrence.26 Moreover, a tumor diameter ≥ 2 cm suggests a high risk of type 1 tumor.27 However, in EC patients, tumor volume measurements have shown a stronger correlation with LNM, parametrial involvement and tumor differentiation than the single diameter tumor analysis.28 However, few studies have reported on the diagnostic value of MRI for PLNEI in EC patients. Therefore, the aim of this study was to probe the diagnostic value of MRI for PLNEI in patients with early-stage EC, which was of great significance for the prognosis and treatment of EC.
Materials and Methods
Ethics Statements
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the Academic Ethics Committee of The First Affiliated Hospital of Fujian Medical University. All patients who participated in this study were fully informed of the purpose of the study and all signed an informed consent before MRI examination.
Sample Size Estimation
G*Power 3.0.10 software (Heinrich-Heine-Universität Düsseldorf, Nordrhein-Westfalen, Germany) was utilized for sample size estimation prior to this study (Supplementary Figure 1). The t test was was selected as the test method, with significance level (α) set at 0.05, the test efficacy (1-β) set at 0.80, and an anticipated effect size (Cohen’s d) of 0.5 (medium effect). Sample size calculations were performed using G*Power 3.1 software. The results indicated that a minimum sample size of 128 cases was necessary to ensure sufficient statistical power for detecting the findings.
Study Subjects
The 186 patients with early-stage EC admitted to The First Affiliated Hospital of Fujian Medical University from August 2017 to July 2022 were retrospectively and consecutively selected, and 142 patients were finally enrolled as the study subjects based on the inclusion and exclusion criteria. They were then arranged into the PLNEInegative group (64 cases) and the PLNEIpositive group (78 cases) according to the histopathological results of radical resection of EC.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) diagnosed as EC by histological examination; (2) International Federation of Gynecology and Obstetrics stage I–II; (3) with complete clinical information, pathological and follow-up data; (4) underwent MRI examination before surgery.
Exclusion criteria included (1) patients who have received other treatments (such as radiotherapy, chemotherapy) before the imaging examination; (2) complicated with the other malignant tumors, systemic inflammatory diseases and chronic diseases; (3) with lung, heart, liver, kidney dysfunctions or in the acute phase of cardiovascular and cerebrovascular adverse events; (4) whose parameter measurements were affected by the artifacts of the MRI.
Data and Sample Collection
By consulting the electronic medical records, the general clinical data of enrolled subjects were collected, including age (years), body mass index (BMI) (kg/m2), smoking history, drinking history, and menopausal status. Additionally, clinicopathological data were also recorded, such as histological type (EC, non-EC), histological grade (G1, G2, and G3 grade represented high, intermediate, and low differentiation, respectively, with the lower differentiation manifesting the higher malignancy), depth of myometrial invasion (< 1/2, ≥ 1/2), LVSI positive detection (negative, positive), LVSI type (conjoined, satellite), cervical involvement (negative, positive), progesterone receptor (negative, positive) and serum CA125 level.
Pelvic MRI
MRI were carried out utilizing a 1.5-T Siemens Avanto system. The patients experienced a fasting period for ≥ 4 h. No antispasmodic medication was used at the time of the examination, and the bladders of the patients were mildly distended. The imaging protocol consisted of T2-weighted axial, coronal, and sagittal images [repetition time (TR)/echo time (TE): 5190/108, 4450/108, 4290/108, respectively; section thickness: 5, 4, 4.5 mm; field of view (FOV): 420, 450, 280 mm]. In addition, diffusion-weighted imaging was performed at b-values of 50, 400, and 800 s/mm2 (TR/TE: 6600/81; slice thickness: 5 mm; FOV: 420 mm). T1-weighted axial images (TR/TE: 716/10; section thickness: 5 mm; FOV: 420 mm) and pre- and post-contrast fat-saturated T1-weighted axial images (TR/TE: 716/10; section thickness: 5 mm; FOV: 420 mm) were obtained. Gadolinium-diethylenetriamine pentaacetic acid was intravenously administered at a dose of 0.1 mmol/kg body weight, followed by contrast-enhanced imaging in axial, coronal, and sagittal planes.
Image Analysis
All MRI images were uploaded to a GE AW4.6 workstation (GE Healthcare, Waukesha, WI, USA). A number of senior radiology physicians reviewed the films in a blind method. Osirix MD version 10 (Pixmeo SARL, Bernex, Switzerland) software was adopted for image analysis. VI was defined as the products of maximum anterior-posterior, transverse, and cranial-caudal diameters of the tumor. TVR was calculated using the formula TTV/total uterine volume (TUV) × 100, where TTV was measured on fat-saturated T1-weighted postcontrast images, which provides enhanced delineation of lesion boundaries, and TUV was measured on high-resolution T2-weighted sagittal images (excluding the cervix and fibroids that deformed the outer edge of the uterus). For the calculation of the ADC, regions of interest (ROIs) were delineated around the tumor on each section of the high b-value images, and these ROIs were subsequently copied on the ADC map. The ADCmean of the primary tumor (ADCtumor), as well as a normal lymph node and a suspicious lymph node, were computed.
Statistical Analysis
Data were statistically analyzed and graphed using the SPSS 21.0 (IBM, Armonk, NY, USA) and GraphPad Prism 8.0.1 (GraphPad Software, San Diego, CA, USA) software. The Shapiro–Wilk test was utilized for normal distribution, and normally distributed measures were expressed as mean ± standard deviation, with t test for comparisons between groups. Categorical data were expressed as frequency and percentage, using Chi-square test for comparisons between groups. Independent influencing factors affecting PLNEI in patients with early-stage EC were assessed using multivariate logistic regression. The individual influencing factors were first subjected to univariate analysis, and those with P < 0.05 were included in the multivariate logistic regression analysis (Enter method was chosen to screen the independent variables). The analysis of differences in the area under the receiver operating characteristic (ROC) curve (AUC) was performed by Delong test. t test was a two-sided test, with P < 0.05 and P < 0.01 considered statistically significant.
Results
Analysis on the Clinical Baseline Data of Early-Stage EC Patients
There were significant differences in histological type, histological grade, depth of myometrial invasion, LVSI positive detection, LVSI type, cervical involvement and serum CA125 level between the PLNEInegative group and the PLNEIpositive group (all P < 0.05). No significant differences in age, BMI, smoking history, drinking history, menopausal status, and progesterone receptor were noted between the two groups (all P > 0.05) (Table 1).
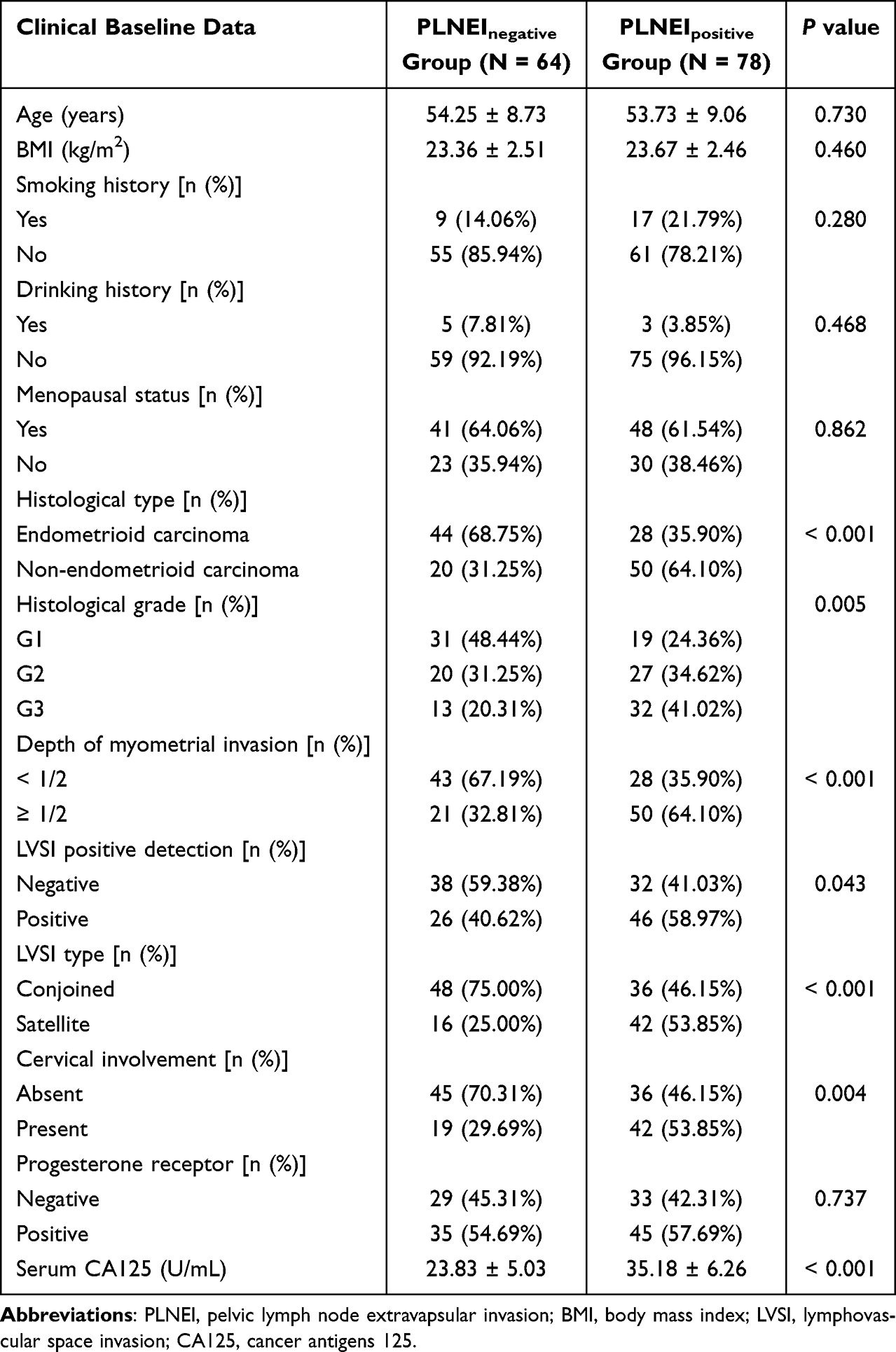 |
Table 1 Analysis on the Clinical Baseline Data of Patients with Early-Stage EC |
Comparative Analysis on VI, TTV, TVR, and ADCmean Between Early-Stage EC Patients with/without PLNEI
The differences in VI, TTV, TVR and ADCmean were comparatively analyzed between early-stage EC patients without and with PLNEI. The results indicated that early-stage EC patients without PLNEI exhibited a VI value of 25.30 ± 7.47 cm³, a TTV value of 12.96 ± 5.32 cm³, a TVR value of 20.57 ± 3.85 cm³, and an ADCmean value of 0.80 ± 0.07 (× 10⁻³ mm²/s). In contrast, early-stage EC patients with PLNEI demonstrated VI, TTV, TVR and ADCmean values of 39.72 ± 9.90 cm³, 23.64 ± 7.19 cm³, 25.45 ± 3.72 cm³, and 0.75 ± 0.07 (× 10⁻³ mm²/s), respectively. Notably, the VI, TTV, and TVR values were higher in early-stage EC patients with PLNEI than those without PLNEI (P < 0.001) (Figure 1A–C). Conversely, the ADCmean value was lower in early-stage EC patients with PLNEI than in those without PLNEI (P < 0.001) (Figure 1D).
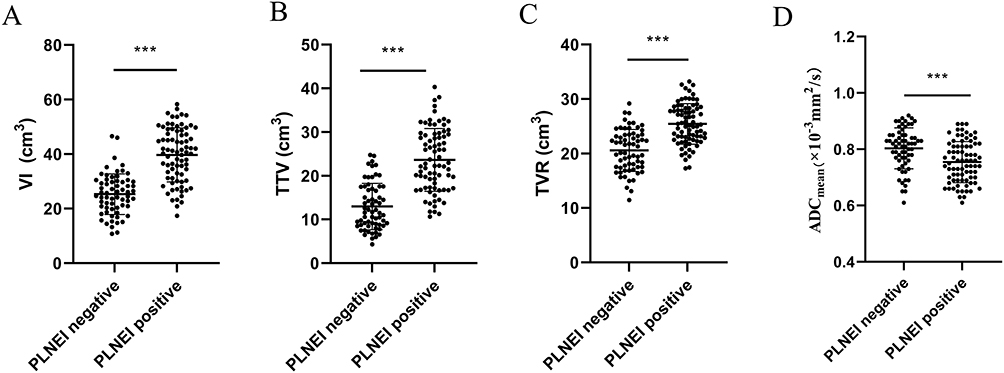 |
Figure 1 Comparative analyses on MRI parameters (VI, TTV, TVR, ADCmean) between the two groups of early-stage EC patients with or without PLNEI. Comparisons of VI (A), TTV (B), TVR (C), and (D) ADCmean values between the two groups of patients. Data were expressed as mean ± standard deviation. Comparisons between the two groups of data were performed using t test. *** P < 0.001. |
Analysis on the Relationships of VI, TTV, TVR and ADCmean Values with Clinicopathological Characteristics
To further explore the relationships of VI, TTV, TVR and ADCmean values with the clinicopathological characteristics of patients with early-stage EC, all patients were were allocated into the low expression groups (L-VI, L-TTV, L-TVR, L-ADCmean) and the high expression groups (H-VI, H-TTV, H-TVR, H-ADCmean) based on the median values of VI, TTV, TVR, and ADCmean. A comparative analysis on the clinicopathological characteristics in early-stage EC patients was conducted. Among early-stage EC patients, significant differences were observed in the H-VI group regarding the histological type, histological grade, depth of myometrial infiltration, LVSI positive detection, LVSI type, cervical involvement, and serum CA125 level (all P < 0.05). Similarly, patients in the H-TTV group demonstrated significant differences in the histological grade, depth of myometrial infiltration, LVSI positive detection, LVSI type, cervical involvement, and serum CA125 level (all P < 0.05). Furthermore, patients in the H-TVR group showed significant differences in the histological grade, depth of myometrial infiltration, cervical involvement, LVSI type, and serum CA125 level (all P < 0.05). Additionally, patients with high ADCmean value exhibited significant differences in the histological grade, depth of myometrial infiltration, cervical involvement, and serum CA125 level (all P < 0.05) (Table 2).
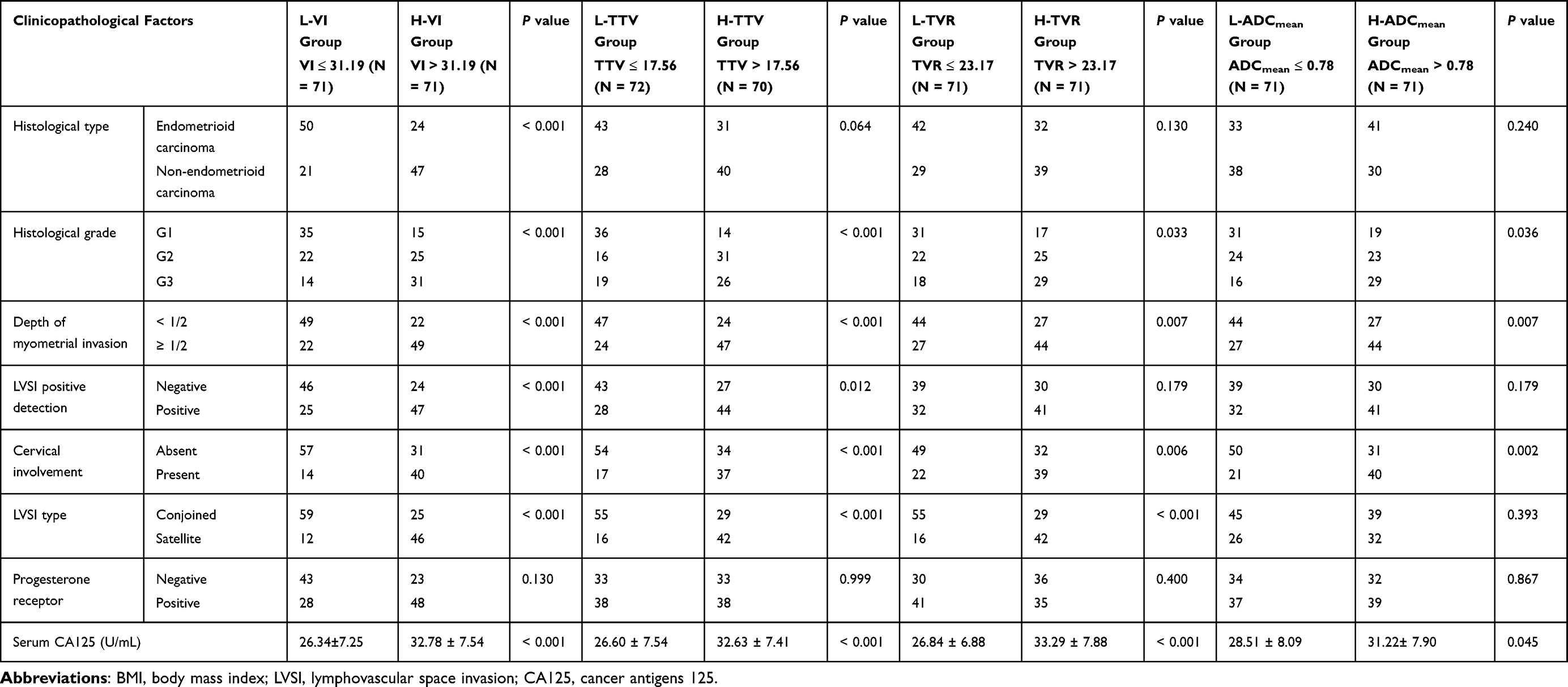 |
Table 2 The Relationships of VI, TTV, TVR, and ADCmean Values with Clinicopathological Characteristics of Early-Stage EC Patients |
VI, TTV, TVR, and ADCmean Were Independent Influencing Factors for PLNEI in Patients with Early-Stage EC
To further assess the independent influencing factors affecting PLNEI in patients with early-stage EC, combining with the results of the analysis in Table 1 (independent variables at P < 0.05), we included the presence or absence of PLNEI as the dependent variable, and the histological type, histological grade, depth of myometrial invasion, LVSI positive detection, LVSI type, cervical involvement, serum CA125, VI, TTV, TVR, and ADCmean as the independent variables in a logistic univariate regression analysis model, which showed that all of the above parameters were influencing factors for the occurrence of PLNEI in patients with early-stage EC. Subsequently, logistics multivariate regression analysis was performed using the indicators with P < 0.05 in the logistics univariate regression analysis as the independent variables. As reflected by the results, serum CA125, VI, TTV, TVR, and ADCmean were all independent influencing factors for PLNEI. The details were listed in Table 3.
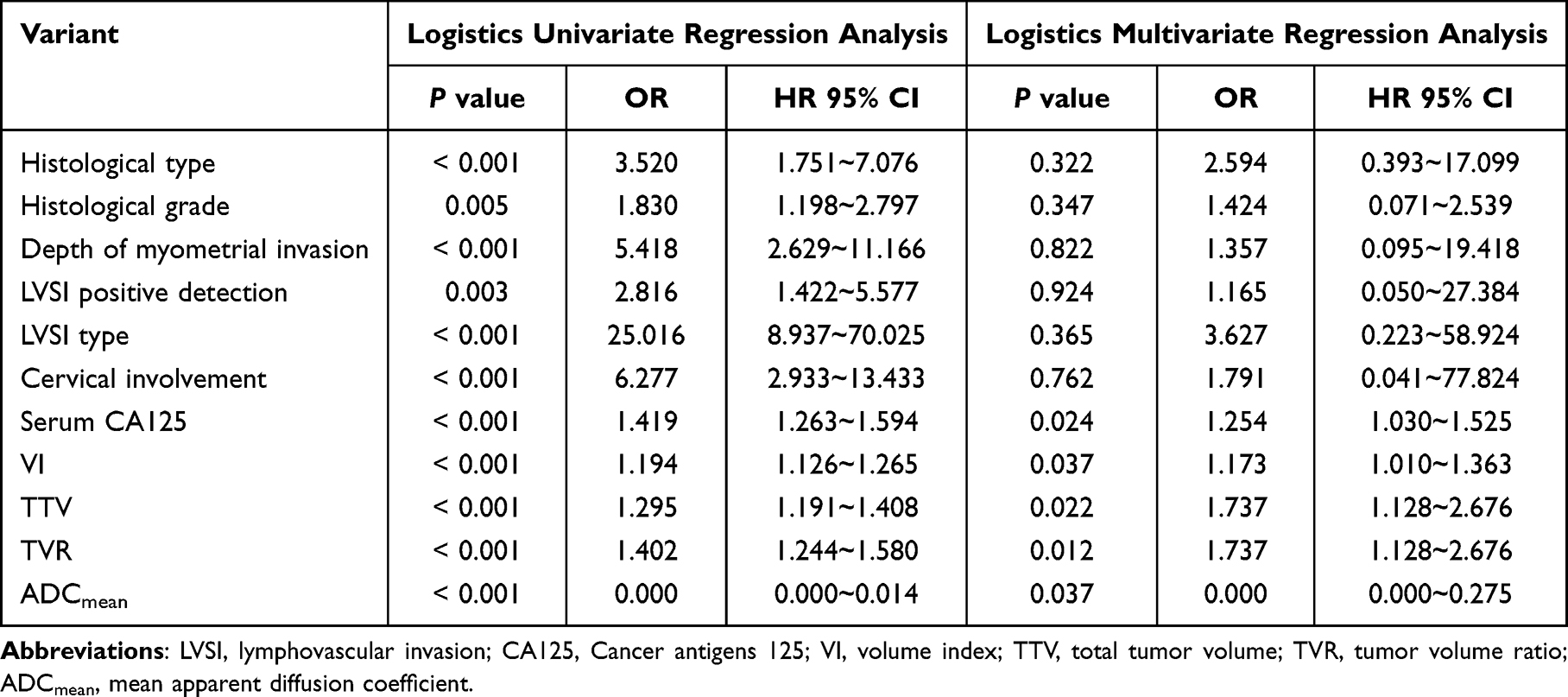 |
Table 3 Logistic Univariate/Multivariate Regression Analyses on Influencing Factors for PLNEI in Patients with Early-Stage EC |
VI, TTV, TVR and ADCmean Had High Diagnostic Value for PLNEI in Patients with Early-Stage EC
ROC curve analysis was performed to evaluate the diagnostic value of VI, TTV, TVR and ADCmean for PLNEI in early-stage EC patients. The results suggested that the AUC of VI value for diagnosing PLNEI in early-stage EC patients was 0.871, with the cut-off value of 33.94, the sensitivity of 71.43%, and the specificity of 92.19% (Figure 2A), that of TTV value was 0.875, with the cut-off value of 18.01, the sensitivity of 87.18%, and the specificity of 70.31% (Figure 2B), that of TVR value was 0.812, with the cut-off value of 24.80, the sensitivity of 55.13%, and the specificity of 89.06% (Figure 2C), and that of ADCmean value was 0.683, with the cut-off value of 0.76, a sensitivity of 56.41%, and a specificity of 75.00% (Figure 2D). These findings indicated that VI value > 33.94, TTV value > 18.01, TVR value > 24.80, and ADCmean value < 0.76 could aid in the diagnosis of PLNEI in early-stage EC patients. Furthermore, the AUC for their combination detection was 0.937, which was higher than the diagnostic value of VI, TTV, TVR or ADCmean alone (all P < 0.05) (Figure 2E and F). Collectively, these data suggested that VI, TTV, TVR and ADCmean had high diagnostic value for PLNEI in patients with early-stage EC. Please refer to Table 4 for more details.
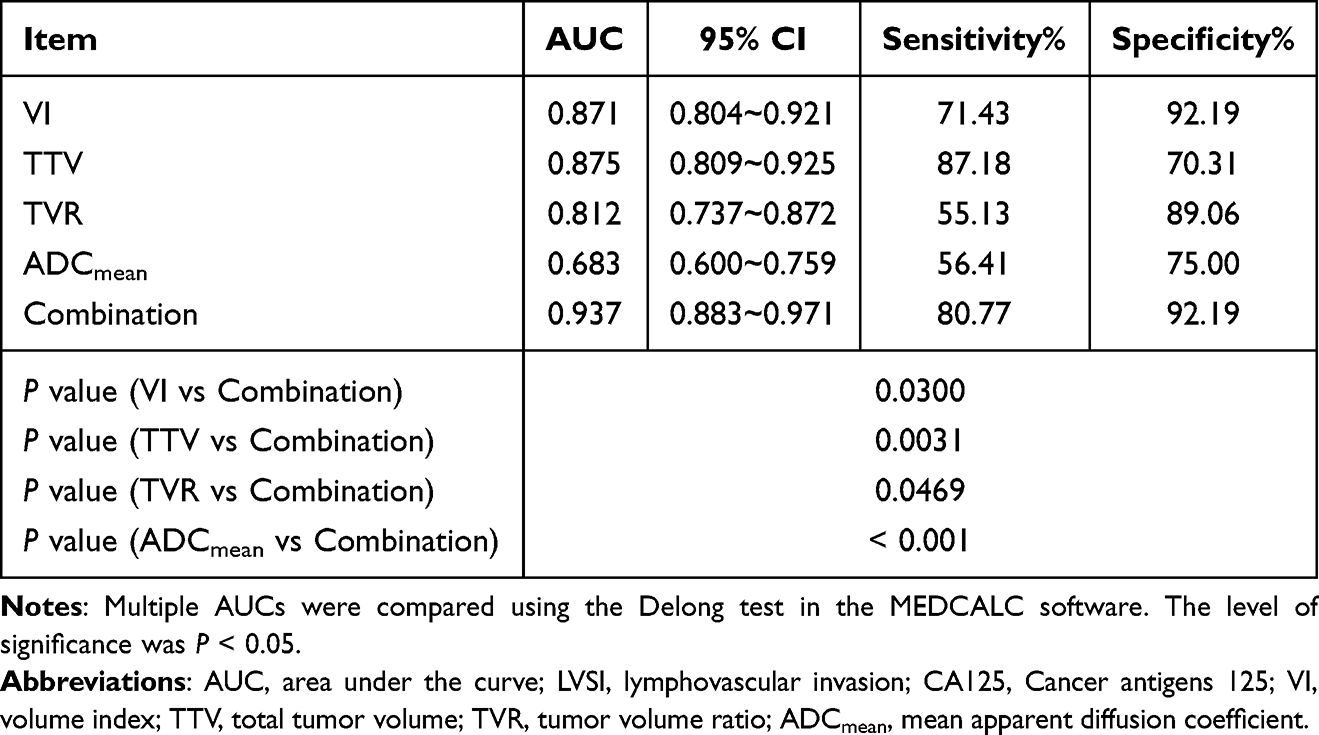 |
Table 4 Independent Diagnostic Value of VI, TTV, TVR, and ADCmean and in Combination for PLNEI in Patients with Early-Stage EC |
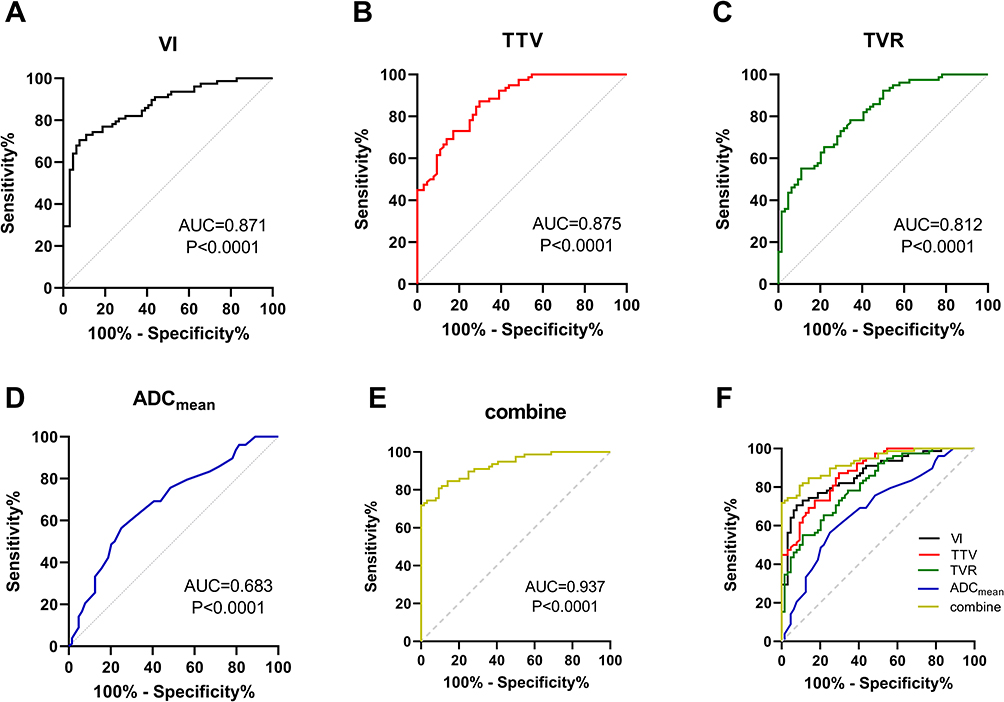 |
Figure 2 Diagnostic value of MRI parameters (VI, TTV, TVR, ADCmean) for PLNEI in patients with early-stage EC. ROC curve analysis to evaluate the diagnostic value of VI (A), TTV (B), TVR (C), and ADCmean values (D) and their combination (E) for PLNEI in patients with early-stage EC, respectively. Multiple ROC curves were compared (F). |
Discussion
EC is the most frequent gynecologic malignancy in rich countries, with a mortality rate of about one-fifth.29 EC is staged as per the International Federation of Obstetrics and Gynecology surgical system, and early diagnosis of the gynecologic malignancy stage is crucial for outcome prediction and treatment planning.30 Among which, symptoms in patients diagnosed with early-stage EC tend to be postmenopausal vaginal bleeding, and EC in early-stage has a good survival rate and requires an adjunctive treatment in the light of the risk of recurrence.31 Notably, MRI occupies an important position in examining local staging of gynecologic tumors.32 Moreover, a growing number of studies have demonstrated that MRI has been applied to the study of clinical gynecologic malignancies.33–35 Based on this context, our study probed the diagnostic value of MRI for PLNEI in early-stage EC patients. The experiment result unveiled that MRI was a good method to detect PLNEI in EC patients, and VI, TTV, TVR, and ADCmean had high diagnostic value for PLNEI in early-stage EC patients.
Volume MRI-derived parameters, specifically VI, TTV, TVR have been shown to predict LVSI, and these MRI volume parameters can effectively stratify patients into high- and low-risk profiles prior to surgical intervention.23 A prior study conducted by Nougaret et al has found that a TVR of 25% or greater indicates deep myometrial invasion, high-grade tumors, and LVSI.24 The ADC value may play a significant role in the management of individualized treatment plans and in enhancing outcomes for patients diagnosed with EC, with a low ADC value usually representing the aggressive biological behavior of malignancies.36,37 The ADCmean is effective in characterizing the cellular properties of lesions, which exhibits latent intrinsic heterogeneity, and is the most commonly utilized metric for assessing the diffusion capacity of lesions.21 In line with the previous study, our study found that compared with EC patients without PLNEI, EC patients with PLNEI had higher VI, TTV and TVR values and lower ADCmean value. Additionally, VI value > 33.94, TTV value > 18.01, TVR value > 24.80, and ADCmean value < 0.76 had high diagnostic value for PLNEI in early-stage EC patients, with their combination manifesting higher value than them along. VI is recognized as a significant factor for predicting LNM in patients with EC.38 Specifically, a VI > 17 cm³has been demonstrated to be correlated with diminished disease-free survival and overall survival rates, and the largest tumor volume exerts an independent effect on the recurrence and survival outcomes of EC patients.39 The ADCmean value of EC patients with stronger invasiveness and worse prognosis is lower.40 Another key focus of our study, preoperative serum CA125, a pivotal indicator for predicting the prognosis of EC patients, comes into play in the selection of surgical treatment options.6 Serum CA125 level is distinctly higher in patients with worsening disease and with LNM in EC patients.41 Similarly, our study revealed that serum CA125 level, VI, TTV, TVR, and ADCmean were independent influencing factors for PLNEI. To conclude, the evidence altogether unmasked that the MRI parameters played crucial clinical parts in diagnosing PLNEI in EC patients.
Various pathological parameters such as histological grade, histological type, depth of myometrial invasion, surgical pathological stage, and cervical involvement play a key part in the prognosis of EC.42 A prior study has demonstrated that histological grade, histological type, depth of myometrial invasion, cervical involvement, LVSI, parametrial involvement are distinctly relevant to LNM.5 Innovatively, our study unraveled that there were significant differences in histological type, histological grade, depth of myometrial invasion, LVSI positive detection, LVSI type, cervical involvement and serum CA125 level between early-stage EC patients with or without PLNEI. Moreover, distinct differences in histological type, histological grade, depth of myometrial infiltration, LVSI positive detection, LVSI type, cervical involvement, and serum CA125 level were found between patients with high or low VI values. Similarly, patients with high or low TTV values demonstrated significant differences in histological grade, depth of myometrial infiltration, LVSI positive detection, LVSI type, cervical involvement, and serum CA125 levels. Furthermore, prominent differences in histological grade, depth of myometrial infiltration, cervical involvement, LVSI type, and serum CA125 level were noticed between the patients with high or low TVR values. Additionally, patients with high or low ADCmean values exhibited significant differences in histological grade, depth of myometrial infiltration, cervical involvement, and serum CA125 levels. Thus, it was persuasive to conclude that the MRI parameters had close associations with clinicopathological characteristics of patients with early-stage EC.
Taken together, this study found that MRI had a good effect on the detection of PLNEI in EC patients, and VI, TTV, TVR and ADCmean values had high diagnostic value for PLNEI in early-stage EC patients. There were still limitations in our study. First, the numbers of cases and events included in this study for analysis were limited. Second, only the MRI parameters (VI, TTV, TVR and ADCmean) were utilized for evaluation. In the future, we will conduct a larger multi-center study to expand the sample size and matched controls to increase the reliability of the results. In addition to MRI parameters (VI, TTV, TVR and ADCmean), we will also combine MRI imaging, multifunctional MRI and positron emission tomography/MRI for differential diagnosis of PLNEI in patients with early-stage EC, thus further clarifying the diagnostic value of MRI for PLNEI in patients with early-stage EC.
Conclusion
All in all, our study highlighted that MRI parameters (VI, TTV, TVR, ADCmean) were associated with clinicopathological characteristic of early EC patients, and were independent influencing factors for the occurrence of PLNEI. VI value >33.94, TTV value > 18.01, TVR value > 24.80, and ADCmean value < 0.76 had high diagnostic value for PLNEI in early EC patients. These parameters assisted clinicians in the preoperative stratification of patients into high and low risk for PLNEI and played an important role in the planning of personalized treatment strategies and the selection of appropriate surgical interventions.
Data Sharing Statement
All the data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the Academic Ethics Committee of The First Affiliated Hospital of Fujian Medical University. All patients who participated in this study were fully informed of the purpose of the study and all signed an informed consent before MRI examination.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Fujian Provincial Health Technology Project (Grant No. 2023TG012) and Natural Science Foundation of Fujian Province (Grant No. 2022J01218).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huvila J, Pors J, Thompsonand EF, Gilks CB. Endometrial carcinoma: molecular subtypes, precursors and the role of pathology in early diagnosis. J Pathol. 2021;253(4):355–365. doi:10.1002/path.5608
2. Zhou J, Tomashefski JF, Sawady J, Ferrerand H, Khiyami A. The diagnostic value of the ThinPrep pap test in endometrial carcinoma: a prospective study with histological follow-up. Diagn Cytopathol. 2013;41(5):408–412. doi:10.1002/dc.22841
3. Bendifallah S, Ilenkoand A, Darai E. High risk endometrial cancer: clues towards a revision of the therapeutic paradigm. J Gynecol Obstet Hum Reprod. 2019;48(10):863–871. doi:10.1016/j.jogoh.2019.06.003
4. Yu Y, Zhang L, Sultana B, Wangand B, Sun H. Diagnostic value of integrated (18)F-FDG PET/MRI for staging of endometrial carcinoma: comparison with PET/CT. BMC Cancer. 2022;22(1):947. doi:10.1186/s12885-022-10037-0
5. Wang Z, Zhang S, Ma Y, Li W, Tianand J, Liu T. A nomogram prediction model for lymph node metastasis in endometrial cancer patients. BMC Cancer. 2021;21(1):748. doi:10.1186/s12885-021-08466-4
6. Jiang T, Huangand L, Zhang S. Preoperative serum CA125: a useful marker for surgical management of endometrial cancer. BMC Cancer. 2015;15(1):396. doi:10.1186/s12885-015-1260-7
7. Shawn LyBarger K, Millerand HA, Frieboes HB. CA125 as a predictor of endometrial cancer lymphovascular space invasion and lymph node metastasis for risk stratification in the preoperative setting. Sci Rep. 2022;12(1):19783. doi:10.1038/s41598-022-22026-1
8. Prueksaritanond N, Angsathaponand S, Insin P. The utility of preoperative serum CA125 combined with HE4 to predict lymph node metastasis in endometrial cancer. Gynecol Obstet Invest. 2023;88(1):53–60. doi:10.1159/000528851
9. Shingaki S, Nomura T, Takada M, Kobayashi T, Suzukiand I, Nakajima T. The impact of extranodal spread of lymph node metastases in patients with oral cancer. Int J Oral Maxillofac Surg. 1999;28(4):279–284. doi:10.1016/S0901-5027(99)80158-1
10. Gooch J, King TA, Eaton A, et al. The extent of extracapsular extension may influence the need for axillary lymph node dissection in patients with T1-T2 breast cancer. Ann Surg Oncol. 2014;21(9):2897–2903. doi:10.1245/s10434-014-3752-0
11. Drinka E, Allen P, McBride A, Buchholzand T, Sahin A. Metastatic tumor volume and extranodal tumor extension: clinical significance in patients with stage II breast cancer. Arch Pathol Lab Med. 2015;139(10):1288–1294. doi:10.5858/arpa.2014-0375-OA
12. Wu MH, Shen WT, Gosnelland J, Duh QY. Prognostic significance of extranodal extension of regional lymph node metastasis in papillary thyroid cancer. Head Neck. 2015;37(9):1336–1343. doi:10.1002/hed.23747
13. Fajkovic H, Cha EK, Jeldres C, et al. Extranodal extension is a powerful prognostic factor in bladder cancer patients with lymph node metastasis. Eur Urol. 2013;64(5):837–845. doi:10.1016/j.eururo.2012.07.026
14. Almulla A, Noel CW, Lu L, et al. Radiologic-pathologic correlation of extranodal extension in patients with squamous cell carcinoma of the oral cavity: implications for future editions of the TNM classification. Int J Radiat Oncol Biol Phys. 2018;102(4):698–708. doi:10.1016/j.ijrobp.2018.05.020
15. Sbarra M, Lupinelli M, Brook OR, Venkatesanand AM, Nougaret S. Imaging of endometrial cancer. Radiol Clin North Am. 2023;61(4):609–625. doi:10.1016/j.rcl.2023.02.007
16. Huang ML, Ren J, Jin ZY, et al. Application of magnetic resonance imaging radiomics in endometrial cancer: a systematic review and meta-analysis. Radiol Med. 2024;129(3):439–456. doi:10.1007/s11547-024-01765-3
17. Maheshwari E, Nougaret S, Stein EB, et al. Update on MRI in evaluation and treatment of endometrial cancer. Radiographics. 2022;42(7):2112–2130. doi:10.1148/rg.220070
18. Otero-Garcia MM, Mesa-Alvarez A, Nikolic O, et al. Role of MRI in staging and follow-up of endometrial and cervical cancer: pitfalls and mimickers. Insights Imaging. 2019;10(1):19. doi:10.1186/s13244-019-0696-8
19. Nougaret S, Rouanet P, Molinari N, et al. MR volumetric measurement of low rectal cancer helps predict tumor response and outcome after combined chemotherapy and radiation therapy. Radiology. 2012;263(2):409–418. doi:10.1148/radiol.12111263
20. Murakami I, Fujii T, Kameyama K, et al. Tumor volume and lymphovascular space invasion as a prognostic factor in early invasive adenocarcinoma of the cervix. J Gynecol Oncol. 2012;23(3):153–158. doi:10.3802/jgo.2012.23.3.153
21. Mapelli P, Ironi G, Bergamini A, et al. Synergic role of preoperative 18F-fluorodeoxyglucose PET and MRI parameters in predicting histopathological features of endometrial cancer. Nucl Med Commun. 2020;41(10):1073–1080. doi:10.1097/MNM.0000000000001257
22. Keles DK, Evrimler S, Merdand N, Erdemoglu E. Endometrial cancer: the role of MRI quantitative assessment in preoperative staging and risk stratification. Acta Radiol. 2022;63(8):1126–1133. doi:10.1177/02841851211025853
23. Ironi G, Mapelli P, Bergamini A, et al. Hybrid PET/MRI in staging endometrial cancer: diagnostic and predictive value in a prospective cohort. Clin Nucl Med. 2022;47(3):e221–e229. doi:10.1097/RLU.0000000000004064
24. Nougaret S, Reinhold C, Alsharif SS, et al. Endometrial cancer: combined MR volumetry and diffusion-weighted imaging for assessment of myometrial and lymphovascular invasion and tumor grade. Radiology. 2015;276(3):797–808. doi:10.1148/radiol.15141212
25. Beddy P, Moyle P, Kataoka M, et al. Evaluation of depth of myometrial invasion and overall staging in endometrial cancer: comparison of diffusion-weighted and dynamic contrast-enhanced MR imaging. Radiology. 2012;262(2):530–537. doi:10.1148/radiol.11110984
26. Nakamura K, Imafuku N, Nishida T, et al. Measurement of the minimum apparent diffusion coefficient (ADCmin) of the primary tumor and CA125 are predictive of disease recurrence for patients with endometrial cancer. Gynecol Oncol. 2012;124(2):335–339. doi:10.1016/j.ygyno.2011.10.014
27. Oliver-Perez MR, Magrina J, Villalain-Gonzalez C, et al. Lymphovascular space invasion in endometrial carcinoma: tumor size and location matter. Surg Oncol. 2021;37:101541. doi:10.1016/j.suronc.2021.101541
28. Chen AC, Sung WH, Wang PH, Sheu MH, Doongand JL, Yuan CC. Correlation of three-dimensional tumor volumetry with cervical cancer prognostic parameters. Eur J Gynaecol Oncol. 2002;23(5):401–404.
29. Husseinand YR, Soslow RA. Molecular insights into the classification of high-grade endometrial carcinoma. Pathology. 2018;50(2):151–161. doi:10.1016/j.pathol.2017.09.010
30. Faria SC, Devine CE, Rao B, Sagebieland T, Bhosale P. Imaging and Staging of Endometrial Cancer. Semin Ultrasound CT MR. 2019;40(4):287–294. doi:10.1053/j.sult.2019.04.001
31. Goel P, Singh V, Sharma R, et al. Early endometrial carcinoma: experience and outcomes. J Cancer Res Ther. 2023;19(Supplement):S0. doi:10.4103/jcrt.jcrt_920_21
32. Khan SR, Arshad M, Wallitt K, Stewart V, Bharwaniand N, Barwick TD. What’s new in imaging for gynecologic cancer? Curr Oncol Rep. 2017;19(12):85. doi:10.1007/s11912-017-0640-3
33. Patel-Lippmann K, Robbins JB, Barroilhet L, Anderson B, Sadowskiand EA, Boyum J. MR imaging of cervical cancer. Magn Reson Imaging Clin N Am. 2017;25(3):635–649. doi:10.1016/j.mric.2017.03.007
34. Park SB. Functional MR imaging in gynecologic malignancies: current status and future perspectives. Abdom Radiol. 2016;41(12):2509–2523. doi:10.1007/s00261-016-0924-3
35. deSouza NM, Rockalland A, Freeman S. Functional MR Imaging in Gynecologic Cancer. Magn Reson Imaging Clin N Am. 2016;24(1):205–222. doi:10.1016/j.mric.2015.08.008
36. Quan Q, Lu Y, Xuan B, et al. The prominent value of apparent diffusion coefficient in assessing high-risk factors and prognosis for patients with endometrial carcinoma before treatment. Acta Radiol. 2021;62(6):830–838. doi:10.1177/0284185120940271
37. Inoue C, Fujii S, Kaneda S, et al. Correlation of apparent diffusion coefficient value with prognostic parameters of endometrioid carcinoma. J Magn Reson Imaging. 2015;41(1):213–219. doi:10.1002/jmri.24534
38. Todo Y, Choi HJ, Kang S, et al. Clinical significance of tumor volume in endometrial cancer: a Japan-Korea cooperative study. Gynecol Oncol. 2013;131(2):294–298. doi:10.1016/j.ygyno.2013.08.008
39. Lopez-Gonzalez E, Rodriguez-Jimenez A, Gomez-Salgado J, Daza-Manzano C, Rojas-Lunaand JA, Alvarez RM. Role of tumor volume in endometrial cancer: an imaging analysis and prognosis significance. Int J Gynaecol Obstet. 2023;163(3):840–846. doi:10.1002/ijgo.14954
40. Chen J, Fan W, Gu H, et al. The value of the apparent diffusion coefficient in differentiating type II from type I endometrial carcinoma. Acta Radiol. 2021;62(7):959–965. doi:10.1177/0284185120944913
41. Kotowicz B, Fuksiewicz M, Jonska-Gmyrek J, Wagrodzkiand M, Kowalska M. Preoperative serum levels of YKL 40 and CA125 as a prognostic indicators in patients with endometrial cancer. Eur J Obstet Gynecol Reprod Biol. 2017;215:141–147. doi:10.1016/j.ejogrb.2017.06.021
42. Li YT, Yangand ST, Wang PH. Molecular pathology and prognosis of endometrial cancer. Taiwan J Obstet Gynecol. 2022;61(6):921–922. doi:10.1016/j.tjog.2022.06.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.