Back to Journals » Open Access Emergency Medicine » Volume 18
Diagnostic Performance of the BE-FAST-V Scale for Detecting Strokes in the Emergency Department: A Prospective Cohort Study
Authors Zhou L, Xu Y, Hu B, Lou J, Zhou X, Chu H, Ye Z
Received 14 April 2026
Accepted for publication 4 July 2026
Published 14 July 2026 Volume 2026:18 616905
DOI https://doi.org/10.2147/OAEM.S616905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Liping Zhou, Yiqing Xu, Beibei Hu, Jiexiang Lou, Xinying Zhou, Huilin Chu, Zhihong Ye
Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed to the work equally
Correspondence: Zhihong Ye, Email [email protected]
Background: Acute stroke, particularly posterior circulation stroke, is often missed in emergency departments due to non-specific symptoms. We aimed to evaluate the diagnostic performance of the BE-FAST-V scale, which adds Vertigo assessment to the original BE-FAST, for acute stroke screening.
Methods: The study included 1,094 patients presenting to a tertiary hospital’s emergency department with suspected stroke. On arrival, the BE-FAST-V scale, which assesses Balance, Eyes, Face, Arm, Speech, Time, and Vertigo, was administered. Stroke diagnoses were confirmed through imaging. Diagnostic accuracy metrics, including sensitivity, specificity, and predictive values, were calculated.
Results: The BE-FAST-V scale demonstrated high diagnostic accuracy, strong sensitivity, and moderate specificity. Adding vertigo improved the detection of posterior circulation strokes, which are often missed due to nonspecific symptoms.
Conclusion: The BE-FAST-V tool presented a highly sensitive and practical value for stroke screening in the emergency department. Its ability to identify posterior circulation strokes, including those presenting with vertigo, addresses a critical gap in stroke diagnosis and supports early treatment initiation. Broader implementation and further validation across multiple centers could enhance its role in improving stroke outcomes globally.
Keywords: BE-FAST-V, stroke, emergency department, screening scale, posterior circulation stroke, vertigo
Introduction
Stroke is a leading cause of morbidity and mortality worldwide. According to the World Health Organization (WHO), stroke was the second-leading cause of death and the third-leading cause of disability globally in 2019.1 In China, the burden of stroke is particularly significant. The Global Burden of Disease Study 2016 reported that the lifetime risk of stroke in China is 39.9%, the highest globally.2 This high prevalence underscores the urgent need for effective strategies for early identification and management of stroke, particularly in emergency department (ED) settings where time-sensitive treatment decisions are critical.
Acute ischemic stroke (AIS), or acute cerebral infarction, is the most common type of stroke, accounting for 69.6% to 70.8% of all cases.3 Recent studies in China highlight the severe outcomes of AIS, with a one-year mortality rate of 14.4% to 15.4% and a mortality/disability rate of 33.4% to 33.8% among hospitalized patients.4 Early diagnosis and treatment are essential to improving outcomes. For instance, the ECASS III trial demonstrated that intravenous thrombolytic therapy within a 3–4.5-hour window significantly improves outcomes in AIS patients.5 Clinical guidelines now recommend completing the initial assessment and initiating thrombolysis within 60 minutes of ED arrival.6 Despite these recommendations, delays in stroke diagnosis and treatment remain a significant challenge in clinical practice.
The early identification of stroke symptoms is the cornerstone of effective stroke management. Prehospital and in-hospital stroke screening tools are widely used to facilitate rapid diagnosis. Commonly employed scales include the Face Arm Speech Test (FAST), Los Angeles Prehospital Stroke Screen (LAPSS), Recognition of Stroke in the Emergency Room Scale (ROSIER), and Cincinnati Prehospital Stroke Scale (CPSS). These tools primarily focus on anterior circulation stroke symptoms, which may lead to missed diagnoses of posterior circulation strokes due to their atypical clinical presentations.7
Recent advancements in stroke screening include the BE-FAST (Balance, Eyes, Face, Arm, Speech, Time) scale, which incorporates assessments of balance and eye movements to improve the detection of posterior circulation strokes. Aroor et al demonstrated that BE-FAST reduced the missed diagnosis rate from 14.1% (using FAST) to 4.4% by identifying patients with unsteady gait or visual disturbances.8 The 2023 Chinese Guidelines for the Diagnosis and Management of Acute Ischemic Stroke also recommend BE-FAST for its potential to reduce underdiagnosis rates in specific populations, such as patients with posterior circulation strokes, normal levels of consciousness, or in-hospital strokes.9 However, the BE-FAST screening scale has limitations, and no prospective studies have confirmed its sensitivity as a screening tool.10
Posterior circulation strokes, which account for 20% of all ischemic strokes, often present with non-specific symptoms such as vertigo or dizziness (47%), unilateral limb weakness (41%), and dysarthria (31%).11,12 Other symptoms may include visual disturbances, disturbances in consciousness, vomiting, and headache. Vertigo and dizziness are extremely common chief complaints in emergency departments. In the United States, around 26,000 patients visit EDs annually due to dizziness or vertigo, accounting for 4% of all emergency visits. Only 4% of these patients are ultimately diagnosed with ischemic stroke, while the vast majority suffer from benign vestibular disorders or nonspecific dizziness.13 The complexity of these overlapping clinical manifestations highlights the limitations of traditional screening tools for detecting posterior circulation strokes in the emergency setting. In routine clinical work, misdiagnosis and delayed diagnosis of posterior circulation stroke frequently occur, especially among patients presenting with acute vestibular syndrome (AVS).14
Nevertheless, despite its promise, using BE-FAST in emergency settings remains underexplored in China. Studies from other regions, such as a retrospective study at the Advanced Stroke Center in Sydney, suggest that incorporating balance and eye assessments increases the detection rate of posterior circulation suspected strokes, albeit with an increase in false positives.15 Additionally, systematic reviews indicate no universally superior screening tool for posterior circulation strokes, emphasizing the need for further validation of scales like BE-FAST in clinical settings.9 Considering the high prevalence of posterior circulation strokes and the prominent symptom of vertigo, we added vertigo screening to BE-FAST, hoping to increase the sensitivity and specificity of the BE-FAST in screening such type of suspected stroke. Our previous unreported study among 305 suspected strokes in ER using BE-FAST-V (“V” for vertigo) to assess the stroke showed a sensitivity of 100%, specificity of 50.7%, and missed suspected stroke of 0%. However, the sample size was relatively small in determining its efficacy for stroke screening. Therefore, the BE-FAST-V screening scale is more widely applicable as a posterior circulation-oriented screening tool. The BE-FAST scale, which adds symptoms specific to posterior circulation stroke (balance/coordination and eye movement/diplopia) to the original FAST scale, does not improve the detection of vestibular stroke, as confirmed by the similar AUC values between BE-FAST and FAST.16 We added a V (Vertigo) item to the BE-FAST scale to assess dizziness or vertigo. Therefore, this study aimed to evaluate the diagnostic performance of the BE-FAST-V scale for identifying strokes in emergency department patients, particularly posterior circulation strokes.
Methods
This study has adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cohort studies.
Study Design and Participants
This prospective cohort study collected data from patients presenting with suspected stroke in the ED of a tertiary hospital between July 2023 and June 2024. Inclusion criteria: (1) age ≥ 18 years; (2) alert; (3) blood glucose level:3.9–22.2mmol/L; (4) presented with one of the symptoms or signs suggestive of stroke, such as double vision or blindness in one or both eyes; facial drooping; inability to lift or a dropping of one limb when lifted; slurred or difficult speech; time of symptom onset ≤ 24 hours; and vertigo. Exclusion Criteria: (1) history of traumatic brain injury; (2) impaired consciousness, inability to cooperate; (3) patients already diagnosed with stroke; (4) BE-FAST-V assessment data were incomplete, or imaging results were unavailable, or imaging findings were inconclusive.
The enrollment and clinical management workflow of all subjects is presented in Figure 1, which complies with the STARD diagnostic reporting standard. This flow chart displays initial screening, eligibility exclusion, triage screening using BE-FAST-V scale, subsequent imaging examination, final diagnosis and data analysis procedures of patients with dizziness and vertigo in emergency department.
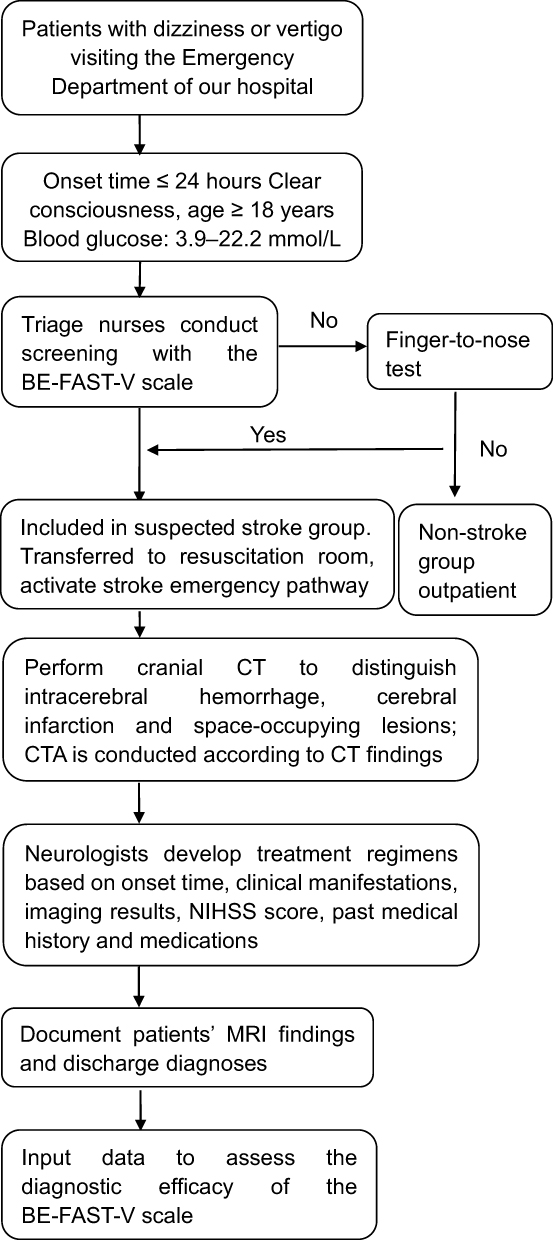 |
Figure 1 Participant flow chart of the study. This diagram illustrates the screening, enrollment, clinical management and data analysis procedures of all patients with dizziness or vertigo visiting the emergency department, detailing inclusion/exclusion standards, triage screening workflow, imaging assessment, final diagnostic outcomes and subsequent data evaluation. |
Sample Size and Sampling
This study used a convenience sampling method to collect data. We tried to use all valid data during a year to evaluate the actual value of the BE-FAST-V in a real work setting. No prospective sample size calculation was performed before patient enrollment. This study adopted a consecutive sampling strategy and retrospectively enrolled 1094 eligible patients with dizziness or vertigo visiting the emergency department within a predefined research period. We have supplemented post-hoc power analysis to evaluate the statistical reliability of the current sample size. Post-hoc power calculation revealed that the existing 1094 subjects provided sufficient statistical power to compare the diagnostic performance indicators of BE-FAST-V.
Instrument for Data Collection
BE-FAST-V tool, which assesses Balance, Eyes, Face, Arm, Speech, Time,8 and Vertigo, was used to assess the patients. Balance: Imbalance or decreased muscle strength in the lower limbs; Eye: Double vision or blindness in one or both eyes; Face: Facial drooping; Arm: Inability to lift or a dropping of one limb when lifted; Speech: Slurred or difficult speech; Time: Time of symptom onset ≤ 24 hours. Vertigo: Patient complains the dizziness. We also collected demographic data, including age, sex, blood sugar, blood pressure, and other diseases such as hypertension, cardiovascular diseases, and pulmonary diseases.
Data Collection
For patients whose chief complaint was dizziness or vertigo occurring within 24 hours, triage nurses first completed the standard BE-FAST assessment. If all items of Balance, Eyes, Face, Arm and Speech were negative, the finger-to-nose test was performed. Patients with abnormal finger-to-nose test results were classified as suspected stroke and entered the stroke diagnostic workflow. Notably, the finger-to-nose test is not an official component of the BE-FAST-V scale. It is an auxiliary triage step exclusively applied to patients with isolated vertigo and negative BE-FAST findings. We added the Vertigo item to BE-FAST to form the BE-FAST-V scale. This unified mnemonic helps emergency triage nurses memorize screening criteria easily and ensures standardized stroke screening for all patients presenting with dizziness or vertigo.
Data were collected by the Triage nurses who had to meet the national standards, including (1) nurses working in the emergency department for more than five years and having passed eligibility evaluation for triage duties and (2) complete training on the use of BE-FAST-V scale and pass the competency evaluation by the panel of the emergency department in the hospital. Upon ED arrival, the Triage nurses took the medical history and vital signs. When one of the B, E, F, A, S, and V symptoms were complained or observed, the nurse initiated the B, E, F, A, S, T, and V assessment. Any positive finding in B, E, F, A, S, and time of onset within 24 hours (T) was considered as a suspected acute stroke. However, when vertigo presented, but none of B, E, F, A, and S were positive, the finger-to-nose test was performed to determine whether the patient had a suspected stroke. The finger-to-nose test was performed in the following way: A part of the coordination movement examination, where the patient was instructed to rotate and extend their forearm externally, then touch their nose with their index finger, starting slowly and then speeding up, repeated multiple times. Abnormal results were indicated by clumsy, inaccurate, uncoordinated, and unsteady finger-to-nose movements, with the cerebellar hemisphere lesion being more pronounced on the affected side. All suspected stroke patients received imaging confirmation, including computed tomography (CT) or magnetic resonance imaging (MRI), which served as the gold standard to classify strokes as ischemic, hemorrhagic, transient ischemic attack (TIA), or no stroke.
We did not implement blinding for radiologists who interpreted cranial imaging; they had access to the recorded BE-FAST-V screening results of each patient during image reading. All suspected stroke patients received imaging confirmation, including computed tomography (CT) or magnetic resonance imaging (MRI), which served as the gold standard to classify strokes as ischemic, hemorrhagic, transient ischemic attack (TIA), or no stroke. The final stroke diagnosis was determined based entirely on cranial CT or MRI imaging findings.
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Review Board or Ethics Committee of Sir Run Run Shaw Hospital affiliated with Zhejiang University, School of Medicine (Approval ID: 20200423–37, 2025–2793-01). The study’s observational nature allowed for a waiver of written informed consent. Data were anonymized to ensure patient confidentiality throughout the analysis.
Statistical Analysis
Data processing and statistical analysis were conducted using Python 3.9.6 (Pandas, NumPy, SciPy, Scikit-learn, and Stats Models). To ensure data integrity, duplicate patient records were removed based on medical record numbers (MRN). Missing values in categorical variables were imputed with zero, while continuous variables were imputed with their respective means. The missing proportion of all variables was less than 1%. For categorical comorbidity variables, missing entries implied no relevant disease history per triage records, justifying zero assignment. Mean imputation for continuous indicators would not induce substantial bias given the small volume of missing data and large sample size of 1094 participants.
Descriptive statistics were calculated for both continuous and categorical variables, stratified by stroke status. Continuous variables were summarized using means and standard deviations (SD), while categorical variables were expressed as counts and percentages. To evaluate the diagnostic performance of the BE-FAST-V screening tool in identifying stroke, a confusion matrix was constructed, and sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. Additionally, receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) was computed to assess diagnostic accuracy. Cohen’s kappa was also calculated to assess the agreement between the BE-FAST-V tool and the reference standard, providing further insight into its reliability.
Results
Demographics and Clinical Characteristics
A total of 1,094 patients with suspected stroke were included in the final analysis. Among them, 834 patients (76.3%) were confirmed as stroke, and 260 patients (23.7%) were diagnosed as non-stroke. In terms of admission route, 641 patients arrived at the hospital by self-referral, and 453 patients were transferred by emergency medical services (EMS, 120).
The baseline characteristics of the two groups are presented in Table 1. The mean age of the stroke group was 67.70 ± 13.99 years, significantly higher than that of the non-stroke group (53.48 ± 19.20 years). The mean blood glucose level in the stroke group was 8.20 ± 3.11 mmol/L, higher than 6.95 ± 2.04 mmol/L in the non-stroke group. The mean systolic blood pressure was 160.71 ± 28.97 mmHg in the stroke group and 145.60 ± 25.72 mmHg in the non-stroke group; the mean diastolic blood pressure was 89.82 ± 19.43 mmHg and 84.74 ± 15.11 mmHg, respectively. The mean SpO2 was similar between the stroke group (97.41 ± 5.11%) and the non-stroke group (97.68 ± 1.71%).
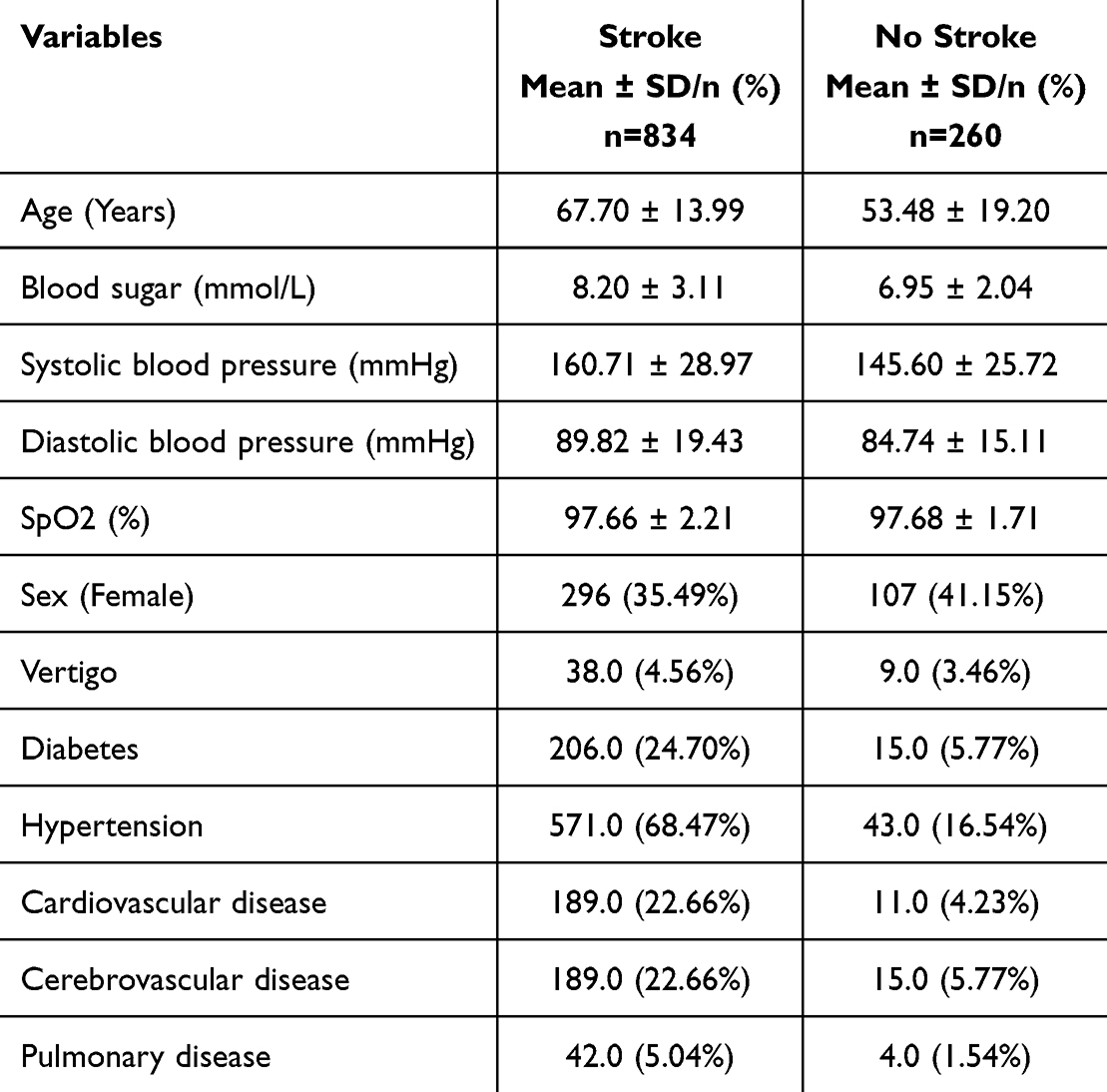 |
Table 1 Demographics of Patients by Stroke |
In the stroke group, 296 (35.49%) were male. Comorbidities included vertigo in 38 patients (4.56%), diabetes in 206 (24.70%), hypertension in 571 (68.47%), cardiovascular disease in 189 (22.66%), cerebrovascular disease in 189 (22.66%), and pulmonary disease in 42 (5.04%). In the non-stroke group, 107 (41.15%) were male; 9 (3.46%) had vertigo, 15 (5.77%) had diabetes, 43 (16.54%) had hypertension, 11 (4.23%) had cardiovascular disease, 15 (5.77%) had cerebrovascular disease, and 4 (1.54%) had pulmonary disease.
Stroke Type Distribution
Among the 834 confirmed stroke patients, the subtype distribution is shown in Table 2. Ischemic stroke accounted for the majority (712 cases, 85.4%), followed by hemorrhagic stroke (76 cases, 9.1%) and transient ischemic attack (TIA) (46 cases, 5.5%).
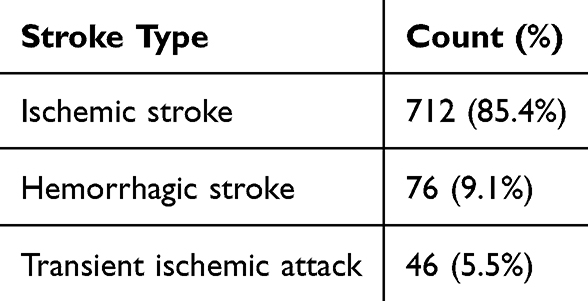 |
Table 2 Stroke Type Distribution |
Diagnostic Performance of BE-FAST-V
As shown in Table 3 (contingency table), the diagnostic performance of the BE‑FAST‑V scale was assessed against the imaging‑based gold standard among all 1,094 enrolled patients. Among the 834 patients confirmed to have stroke, the BE‑FAST‑V scale correctly identified 833 patients as positive (true positives), while only 1 patient was falsely classified as negative (false negatives). Among the 260 patients who were excluded from a stroke diagnosis, 214 patients were correctly identified as negative (true negatives) and 46 patients were incorrectly identified as positive (false positives). In total, 879 patients had a positive result on the BE‑FAST‑V scale and 215 patients had a negative result. This fourfold table provides the basic data for calculating all core diagnostic indicators of the BE‑FAST‑V scale.
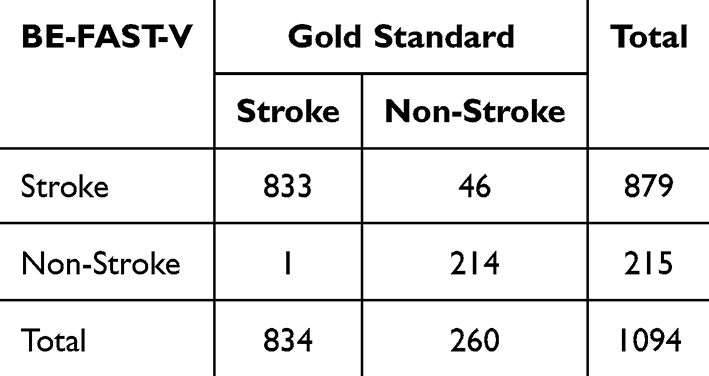 |
Table 3 Contingency Table for Diagnostic Accuracy of BE-FAST-V |
The diagnostic performance of the BE-FAST-V scale is summarized in Table 4. Among 1,094 patients, there were 833 true positives, 46 false positives, 214 true negatives, and 1 false negative. The BE-FAST-V scale achieved an exceedingly high sensitivity of 0.999 (99.9%), a moderate specificity of 0.823 (82.3%), a positive predictive value (PPV) of 0.948 (94.8%), and a negative predictive value (NPV) of 0.995 (99.5%). The area under the receiver operating characteristic curve (AUC) was 0.910, indicating excellent overall diagnostic accuracy (Figure 2). The Cohen’s kappa coefficient was 0.874, suggesting almost perfect agreement between the BE-FAST-V scale and the imaging-based gold standard.
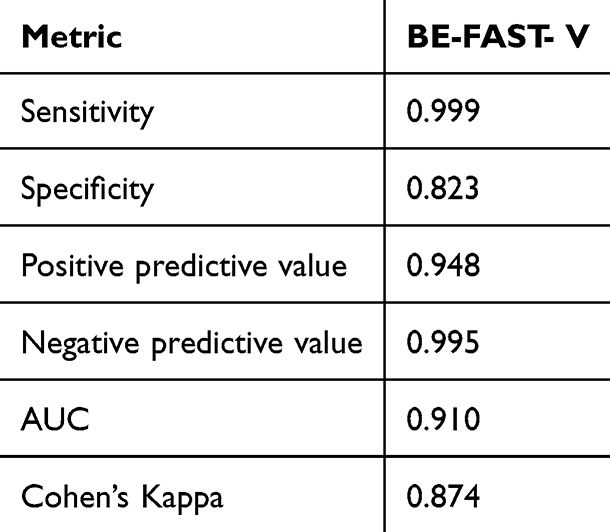 |
Table 4 Diagnostic Performance of BE-FAST-V |
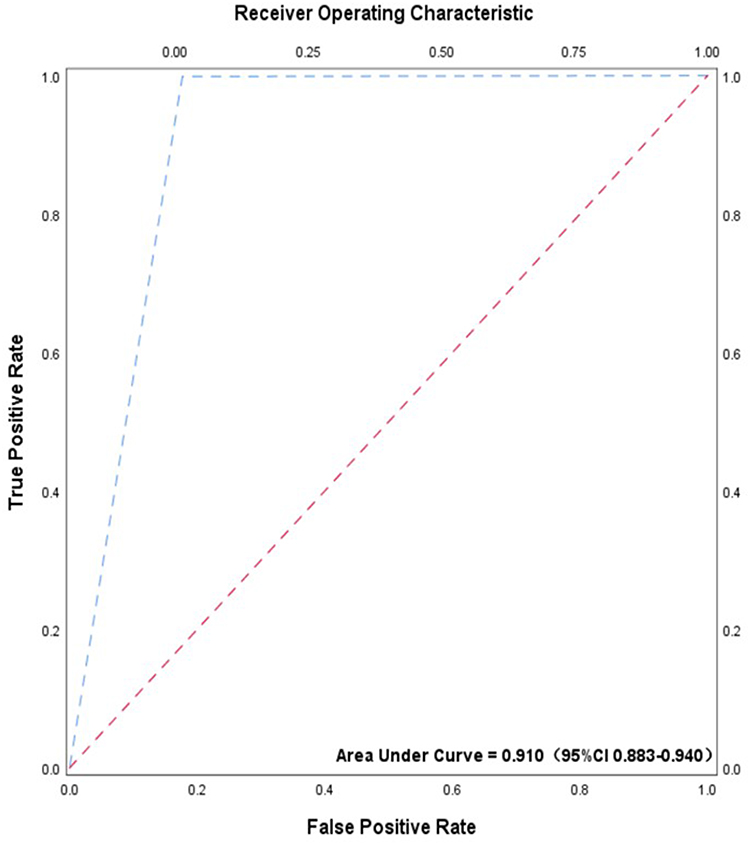 |
Figure 2 The ROC of BE-FAST-V. Receiver operating characteristic curve for the BE-FAST-V scale to identify stroke among emergency patients with dizziness or vertigo. The AUC value was 0.910, and the 95% confidence interval of AUC was added to the curve plot to improve statistical reporting quality. |
Diagnostic Performance Comparison Between FAST and BE-FAST-V
To quantitatively evaluate the incremental diagnostic value of the supplementary vertigo item, we conducted a head-to-head comparison between the traditional FAST scale and our modified BE-FAST-V scale. The fourfold contingency tables of the two screening tools are shown in Table 5, and all diagnostic indicators with statistical comparisons are listed in Table 6. The sensitivity of BE-FAST-V (99.88%, 95% CI: 99.32–100.00) was markedly higher than FAST (95.80%, 95% CI: 94.21–97.00), with a statistically significant difference (χ2=32.82, P<0.001). No significant intergroup difference was found in specificity (82.31% for BE-FAST-V vs 85.26% for FAST, χ2=0.82, P=0.366). BE-FAST-V had an excellent negative predictive value of 99.53% and a higher Cohen’s Kappa value (0.874) than FAST (0.813), reflecting better consistency with imaging gold standard and stronger stroke exclusion ability. Both scales had AUC values greater than 0.9, showing favorable overall discrimination performance, and BE-FAST-V had a marginally elevated Youden’s index.
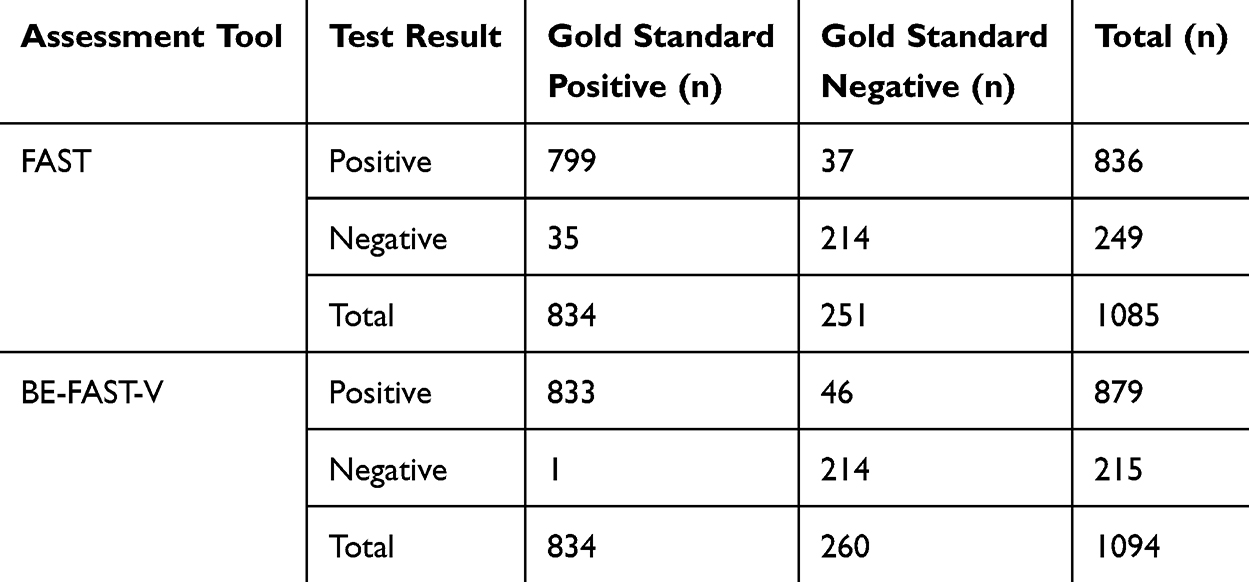 |
Table 5 Contingency Tables for FAST and BE-FAST-V Scales in Detecting Stroke Patients |
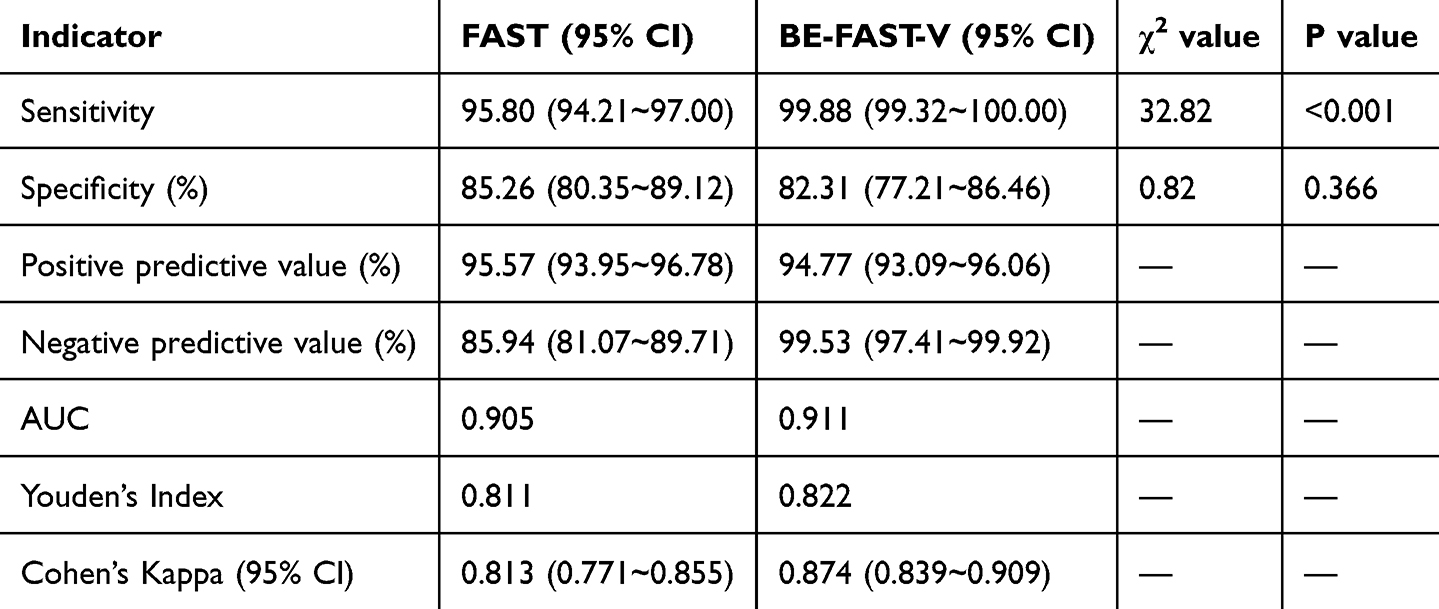 |
Table 6 Comparison of Diagnostic Performance Between FAST and BE-FAST-V Scales |
Discussion
Early Recognition Is Key in the Diagnosis and Treatment of Acute Ischemic Stroke
The management of acute ischemic stroke (AIS) relies heavily on early recognition and timely intervention, given the narrow therapeutic window for effective treatment. Guidelines emphasize that the “golden hour” for AIS treatment involves completing diagnostic assessments and initiating thrombolysis within 60 minutes of emergency department (ED) arrival, minimizing Door-to-Needle Time (DNT).6 Advanced stroke centers have further reduced DNT to 30 minutes,17 yet the average DNT in China remains 86 minutes.18 Delays in hospital processes and in prehospital triage significantly contribute to these prolonged times. Rapid and accurate triage of suspected stroke patients in the ED is critical to initiating treatment promptly. Screening tools like BE-FAST have been widely used globally to improve early detection and streamline patient management.19,20 However, prehospital stroke awareness in China remains limited, emphasizing the importance of simple, sensitive, and easily implemented screening tools for emergency nurses. The BE-FAST-V scale, like BE-FAST, can address delays and enhance the efficiency of the stroke treatment process, especially for those presenting with vertigo with any of the other symptoms and complaints.
Diagnostic Performance of the BE-FAST-V Tool
The BE-FAST-V scale showed exceptional diagnostic accuracy in this study, with a sensitivity of 99.9% and a leakage rate of just 0.1%. These findings prove that BE-FAST-V remained the strength of BE-FAST, which has high sensitivity (92–98.3%) and significantly reduced missed diagnoses compared to FAST.21,22 Including “V: Vertigo” further improved the tool’s performance by addressing a critical gap in identifying posterior circulation strokes, often underdiagnosed due to their atypical presentation. The sensitivity in this study was higher than our previous unreported study with a smaller sample size, demonstrating the practical value of the BE-FAST-V tool in the accrual working setting. By incorporating vertigo assessment, triage nurses were reminded not to miss out on patients with vertigo as the only symptom, facilitating targeted treatment within critical time frames. With an area under the ROC curve of 0.910 and strong concordance (kappa value = 0.874), the BE-FAST-V tool proved reliable and efficient. The unified BE-FAST-V mnemonic is easy for emergency triage nurses to memorize. The supplementary vertigo assessment only requires brief verbal inquiry rather than complex physical examination procedures, which may not markedly increase routine triage burden while improving screening accuracy.
The Value of the BE-FAST-V Scale in Patients with Vertigo
Posterior circulation strokes account for 20% of all ischemic strokes and are often associated with diagnostic delays due to nonspecific symptoms, such as vertigo or dizziness.23,24 Vertigo is a common presenting symptom in such cases, but its heterogeneous nature poses challenges in distinguishing stroke from benign conditions like vestibular disorders.13,25 “V: Vertigo” in the BE-FAST tool ensures that patients with vertigo undergo thorough assessment, including a finger-nose test for posterior circulation stroke suspicion.16 This approach significantly reduced the risk of missed diagnoses. In our study, 3% of patients presented with vertigo as the primary symptom, and 81.58% of them were confirmed to have stroke by imaging. Of these, 22 patients presented to the emergency department with dizziness or vertigo accompanied by other BE-FAST positive signs, while 3 patients had isolated dizziness with a positive finger-to-nose test. The finger-to-nose test significantly increased the detection rate of posterior circulation stroke from 45.8% to 74.1% and shortened the median door-to-CT time in the tested group.26 Only one patient in our study with vertigo was initially missed during the nurse-led triage but was later identified by a physician during follow-up evaluation; this highlights the tool’s value in capturing posterior circulation strokes, particularly in patients presenting with isolated vertigo. It also underscores the need for emergency nurses to remain vigilant in screening vertigo patients and emphasizes the importance of implementing BE-FAST-V in ED settings.
This study constructed BE-FAST-V by adding a vertigo evaluation item to the traditional stroke screening system and verified its diagnostic efficiency in a large emergency cohort. A major strength of the present study is the direct quantitative comparison between BE-FAST-V and the classic FAST scale based on a large emergency cohort. Statistical results verified that adding the vertigo assessment item substantially elevated screening sensitivity and negative predictive value without obvious loss of specificity, which robustly proves the incremental diagnostic value of BE-FAST-V. This head-to-head comparison makes up for the deficiency of lacking comparison with existing screening tools, and further highlights the novelty and clinical practicability of our modified scale.
All conclusions in this discussion are highly consistent with our statistical results and core research objectives. Dizziness and vertigo are common complaints in the emergency department. Although most cases are caused by vestibular disorders or non-specific symptoms, they may also result from posterior circulation stroke. Therefore, routine BE-FAST-V screening is required for patients presenting with dizziness or vertigo to prevent missed detection of posterior circulation stroke and delays in intravenous thrombolysis. The intravenous thrombolysis time window for acute ischemic stroke is merely 4.5 hours; in China, nurses conduct emergency triage, and suspected stroke patients are immediately sent to the resuscitation room for rapid stroke pathway activation, neurology consultation and urgent cranial CT scanning, making accurate nurse-led screening essential. Only 4% of dizziness/vertigo patients in our cohort had acute ischemic stroke, and such patients are prone to missed diagnosis via conventional FAST, so we developed BE-FAST-V to screen both typical stroke cases and patients with isolated dizziness or vertigo, which fully fulfills our research purpose.
Limitations
A few limitations are noted in the current study. Firstly, this study was conducted at a single advanced stroke center, and data from 12 months were analyzed. While the results were promising, the findings may not be generalizable to other healthcare settings. Future multicenter studies must validate the tool’s performance in diverse clinical environments and prehospital settings. Second, although the BE-FAST-V scale demonstrated high sensitivity, the diagnosis of posterior circulation strokes with isolated vertigo remains a challenge due to the nonspecific nature of these symptoms. Further research on isolated vertigo is needed to refine screening protocols and reduce underdiagnosis in this subgroup. Third, we adopted simple zero filling for categorical missing data and mean imputation for continuous variables, which may narrow data variance and introduce minor statistical bias. More sophisticated multiple imputation methods will be utilized in subsequent multi-center studies to optimize missing data processing. Fourth, all conclusions regarding improved screening efficiency and reduced missed triage screening are only supported by single-center data without external multicenter validation, which limits the generalizability of our optimistic observations. Future external validation studies are required to confirm whether the scale can consistently reduce missed stroke identification in diversified emergency environments. In addition, the diagnostic performance of BE-FAST-V observed in this cohort may not generalize to undifferentiated patients with dizziness or vertigo visiting emergency departments in non-specialized stroke centers.
Conclusion
The BE-FAST-V tool presented a highly sensitive and practical value for stroke screening in the emergency department. Its ability to identify posterior circulation strokes, including those presenting with vertigo, addresses a critical gap in stroke diagnosis and supports early treatment initiation. Broader implementation and further validation across multiple centers could enhance its role in improving stroke outcomes globally.
Ethics Approval and Consent to Participate
All methods were performed in accordance with the relevant guidelines and regulations. Under the guidance of principles of the World Medical Association Declaration of Helsinki, it was taken into the first consideration to respect participants’ rights and to protect their health and rights. This study adheres to ethical principles. Ethical approval for the study was obtained from the Institutional Review Board or Ethics Committee of Sir Run Run Shaw Hospital affiliated with Zhejiang University, School of Medicine (Approval ID: 2025-2793-01). The study’s observational nature allowed for a waiver of written informed consent. Data were anonymized to ensure patient confidentiality throughout the analysis.
Acknowledgment
Liping Zhou and Yiqing Xu are co-first authors for this study. Thanks Dr. Yang Lili for her big contribution in designing of the study and manuscript writing and editing.
Author Contributions
Liping Zhou and Yiqing Xu conceived and designed the study, and drafted the manuscript. Jiexiang Lou and Huilin Chu performed study execution and data collection, who collected and checked the data. Jiexiang Lou, Huilin Chu, and Xinying Zhou undertook data analysis and interpretation. Zhihong Ye made a significant contribution to the overall research; he took part in revising and critically reviewing the article, gave final approval of the version to be published, agreed on the target journal, and accepts accountability for all aspects of this work. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by Health Commission program of Zhejiang Provincial in China (Grant No.2023KY118).
Disclosure
The authors declare no competing interests in this work.
References
1. Zhang GB, Huang HW, Guo W. [Prevention and treatment of stroke in Chinese and African young adults]. Zhonghua Yu Fang Yi Xue Za Zhi. 2022;56(8):1142–12. Chinese. doi:10.3760/cma.j.cn112150-20220104-00008
2. Feigin VL, Nguyen G, Cercy K, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379(25):2429–2437.
3. Patil S, Rossi R, Jabrah D, Doyle K. Detection, diagnosis and treatment of acute ischemic stroke: current and future perspectives. Front Med Technol. 2022;4:748949. doi:10.3389/fmedt.2022.748949
4. Gang W, Bangjiang F, Xuezhong Y, Zhijun L. [Interpretation of 2018 guidelines for the early management of patients with acute ischemic stroke]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018;30(4):289–295. Chinese. doi:10.3760/cma.j.issn.2095-4352.2018.04.001
5. Werner H, Markku K, Erich B, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
6. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
7. Rudd M, Buck D, Ford GA, Price CI. A systematic review of stroke recognition instruments in hospital and prehospital settings. Emerg Med J. 2016;33(11):818–822. doi:10.1136/emermed-2015-205197
8. Aroor S, Singh R, Goldstein LB. BE-FAST (Balance, Eyes, Face, Arm, Speech, Time): reducing the proportion of strokes missed using the FAST mnemonic. Stroke. 2017;48(2):479–481. doi:10.1161/STROKEAHA.116.015169
9. Liu L, Li Z, Zhou H, et al. Chinese Stroke Association guidelines for clinical management of ischaemic cerebrovascular diseases: executive summary and 2023 update. Stroke Vasc Neurol. 2023;8(6):e3. doi:10.1136/svn-2023-002998
10. Ammar FE, Ardelt A, Brutto VJD, et al. BE-FAST: a sensitive screening tool to identify in-hospital acute ischemic stroke. J Stroke Cerebrovasc Dis. 2020;29(7):104821. doi:10.1016/j.jstrokecerebrovasdis.2020.104821
11. Schulz UG, Fischer U. Posterior circulation cerebrovascular syndromes: diagnosis and management. J Neurol Neurosurg Psychiatry. 2017;88(1):45–53. doi:10.1136/jnnp-2015-311299
12. Novakovic-White R, Corona JM, White JA. Posterior circulation ischemia in the endovascular era. Neurology. 2021;97(20 Suppl 2):S158–S169. doi:10.1212/WNL.0000000000012808
13. Qiu D, Zhang L, Deng J, et al. New insights into vertigo attack frequency as a predictor of ischemic stroke. Front Neurol. 2020;11:593524. doi:10.3389/fneur.2020.593524
14. Zuo L, Zhan Y, Liu F, et al. Clinical and laboratory factors related to acute isolated vertigo or dizziness and cerebral infarction. Brain Behav. 2018;8(9):e01092. doi:10.1002/brb3.1092
15. Tanglay O, Cappelen-Smith C, Parsons MW, Cordato DJ. Enhancing stroke recognition: a comparative analysis of Balance and Eyes-Face, Arms, Speech, Time (BE-FAST) and Face, Arms, Speech, Time (FAST) in identifying posterior circulation strokes. J Clin Med. 2024;13(19):5912. doi:10.3390/jcm13195912
16. Pickham D, Valdez A, Demeestere J, et al. Prognostic value of BEFAST vs FAST to identify stroke in a prehospital setting. Prehosp Emerg Care. 2019;23(2):195–200. doi:10.1080/10903127.2018.1490837
17. Wang J, Dong YQ, Yeo J, et al. Improved functional outcomes and cost benefits of door-to-needle time under 30 min in acute ischemic stroke: an observational study. Front Stroke. 2025;4:1583875. doi:10.3389/fstro.2025.1583875
18. Yang H, Wu Z, Huang X, et al. In-hospital emergency treatment delay among chinese patients with acute ischaemic stroke: relation to hospital arrivals and implications for triage pathways. Int J Gen Med. 2023;16:57–68. doi:10.2147/IJGM.S371687
19. Dharmasaroja P, Uransilp N. Stroke awareness and knowledge in the at-risk population: a community-based study. Cureus. 2024;16(4):e57756.
20. Özdemir Z, Acar E. YouTube as a source of recognizing acute stroke; progress in 2 years. BMC Public Health. 2024;24(1):2208. doi:10.1186/s12889-024-19710-4
21. Scheitz JF, Abdul-Rahim AH, MacIsaac RL, et al. Clinical selection strategies to identify ischemic stroke patients with large anterior vessel occlusion: results from SITS-ISTR (Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Registry). Stroke. 2017;48(2):290–297. doi:10.1161/STROKEAHA.116.014431
22. Smith EE, Kent DM, Bulsara KR, et al. Accuracy of prediction instruments for diagnosing large vessel occlusion in individuals with suspected stroke: a systematic review for the 2018 guidelines for the early management of patients with acute ischemic stroke. Stroke. 2018;49(3):e111–e122. doi:10.1161/STR.0000000000000160
23. Ausman JI, Liebeskind DS, Gonzalez N, et al. A review of the diagnosis and management of vertebral basilar (posterior) circulation disease. Surg Neurol Int. 2018;9:106. doi:10.4103/sni.sni_373_17
24. Schneider AM, Neuhaus AA, Hadley G, et al. Posterior circulation ischaemic stroke diagnosis and management. Clin Med. 2023;23(3):219–227. doi:10.7861/clinmed.2022-0499
25. Hanna J, Malhotra A, Brauer PR, Luryi A, Michaelides E. A comparison of benign positional vertigo and stroke patients presenting to the emergency department with vertigo or dizziness. Am J Otolaryngol. 2019;40(6):102263. doi:10.1016/j.amjoto.2019.07.007
26. Oostema JA, Chassee T, Baer W, Edberg A, Reeves MJ. Educating paramedics on the finger-to-nose test improves recognition of posterior stroke. Stroke. 2019;50(10):2941–2943. doi:10.1161/STROKEAHA.119.026221
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Detecting Stroke at the Emergency Department by a Point of Care Device: A Multicenter Feasibility Study
Tsiftsis D, Manioti EA, Touris G, Kyriakakis E, Tsamopoulos N, Gamvroudi M
Medical Devices: Evidence and Research 2024, 17:107-112
Published Date: 5 March 2024