")
Back to Journals » Medical Devices: Evidence and Research » Volume 17
Detecting Stroke at the Emergency Department by a Point of Care Device: A Multicenter Feasibility Study
Authors Tsiftsis D , Manioti EA, Touris G, Kyriakakis E, Tsamopoulos N, Gamvroudi M
Received 14 November 2023
Accepted for publication 28 February 2024
Published 5 March 2024 Volume 2024:17 Pages 107—112
DOI https://doi.org/10.2147/MDER.S445075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dimitrios Tsiftsis,1 Eleni Alexandra Manioti,1 Georgios Touris,2 Eleftherios Kyriakakis,1 Nikolaos Tsamopoulos,3 Maria Gamvroudi2
1Emergency Department, “Agios Panteleimon” General Hospital, Nikaia, Greece; 2Emergency Department “Konstantopouleio - Patision” General Hospital, Nea Ionia, Greece; 3Department of Interventional Radiology, Mediterraneo Hospital, Athens, Greece
Correspondence: Dimitrios Tsiftsis, Emergency Department, “Agios Panteleimon” General Hospital, Parnasidos 29, Agios Dimitrios, 17341, Greece, Tel +306945491406, Email [email protected]
Purpose: To evaluate if the Strokefinder MD 100 by Medfield Diagnostics AB can be used as a point of care device in overcrowded Emergency Departments (ED).
Patients and Methods: We used the strokefinder MD 100 by Medfield Diagnostics AB in two Greek National Health System (NHS) Hospitals Emergency Departments. Our research protocol was approved by local scientific and ethics committees. We prospectively enrolled 71 adult patients from two NHS emergency departments in whom stroke was included as a differential diagnosis after triage. The feasibility of using the Strokefinder MD 100 by Medfield Diagnostics AB in various emergency department settings was evaluated through a structured questionnaire.
Results: The strokefinder MD 100 was used on 71 patients in various settings in the Emergency Department. In every case, the test was completed at the patient bedside without interfering with other ongoing and diagnostic and resuscitation procedures. There was no additional delay to patient care caused by performing the test when compared with current local Emergency Department practice and protocol. In almost 90% of the cases, a clear result was produced by the device.
Conclusion: The Strokefinder MD 100 can be safely used as a point of care device by all trained healthcare professionals, in the most overcrowded emergency department, in various ED locations.
MeSH terms: Point of Care Systems, Cerebrovascular Stroke, Proof of Concept Study.
Keywords: stroke, point of care device, emergency department
Introduction
Overcrowding has been identified as a global emergency department reality1,2 Emergency department crowding has a well-documented negative effect on patient outcomes.3,4 Over the years, many different strategies have been proposed to alleviate the effects of overcrowding to patient outcome with various results.5 At the same time, stroke remains a major time-sensitive, potentially treatable, disease that needs immediate diagnostic and therapeutic actions.6 According to CDC data, there are almost 800,000 new stroke diagnoses in the USA every year7. Definite diagnosis can be obtained by neuroimaging. From all investigated radiologic imaging modalities, none of them alone is considered to be perfect in diagnosis and even more in outcome prognosis. In everyday clinical life, the choice of imaging to be performed depends on purpose and availability.8,9 In order to stratify and correctly prioritize patients most likely to have a stroke several clinical screening tools have been developed. Their diagnostic sensitivity and specificity ranges vary widely in different studies (sensitivity 73.9%–91%, specificity 64%–88.7%).10 Several stroke mimics and chameleons have been identified ranging from life threatening to benign, complicating fast and accurate diagnosis even further.11,12 To further increase triage and prognostic accuracy, several ultrasound and microwave-based modalities are being actively investigated as diagnostic adjuncts, to be used bedside in the Emergency Department as Point-of-Care testing modalities. Transcranial Doppler Ultrasonography is a simple, non-invasive, bedside method of examining intracerebral blood flow. However, the supporting level of evidence is weak.13 Carotid artery ultrasonography provides considerable information when used to evaluate a specific site. In emergency medicine practice, carotid artery ultrasonography can be used to diagnose internal carotid artery stenosis, an occluded vessel, and infer the cause of ischemic stroke. Further studies will be needed for its incorporation into clinical diagnostic pathways and guidelines.14 There is vigorous research on ultrasound technology point-of-care devices capable of enhancing clinical prehospital stroke diagnosis.15 Other research takes advantage of microwave scattering and imaging, near-infrared spectroscopy, bioelectrical impedance spectroscopy in an effort to reduce time to treatment for stroke patients.16,17 Medfields MD 100 Strokefinder is a microwave technology-based implementation, intended for measuring dielectric properties of brain tissue. The purpose of the measurement is to provide information regarding the presence of stroke. The system is transportable and aimed for usage in a prehospital environment and in emergency and neurology departments in hospital.18
Materials and Methods
The study protocol was reviewed and approved by the ethics and scientific committees of Nikaia General Hospital and Nea Ionia General Hospital. The study was conducted according to the revised Declaration of Helsinki and good clinical practice.
All patients fulfilling enrollment criteria were informed by the researcher performing the test on the scope and aims of the study. The procedure was explained, and all relevant questions answered. If a patient was not able to comprehend, all the above were explained to his health care proxy. All included in the study patients have provided their informed consent to participate.
We designed a prospective study to be implemented in two different Greek NHS Hospital Emergency departments.
A structured questionnaire was constructed aiming at identifying the feasibility of using the strokefinder in the emergency department in various areas (triage, resuscitation, fast track, intermediate) by health care professionals (attending emergency physicians, residents, intensivists, residents, nurses) by the patients’ bed-side without altering or interfering with standard local operational protocols. The principal study question to be answered was if the device could produce additional information without prolonging the patient's stay in the emergency department.
As part of the manufacturer’s quality control, a second questionnaire provided by the manufacturer was completed by all investigators.
All patients with a presenting complaint of headache or altered mental status and an initial triage differential diagnosis that included stroke were eligible for enrollment. All enrolled patients were admitted to the emergency department between March 2023 and May 2023. According to local protocols, they were triaged to the resuscitation area or fast-track area or intermediate acuity area. All healthcare professionals involved in this study were adequately trained in its operation and all adhered to the user manual provided. In those patients in whom stroke was part of the differential diagnosis, the stokefinder could be applied. The inclusion and exclusion criteria are listed in Table 1.
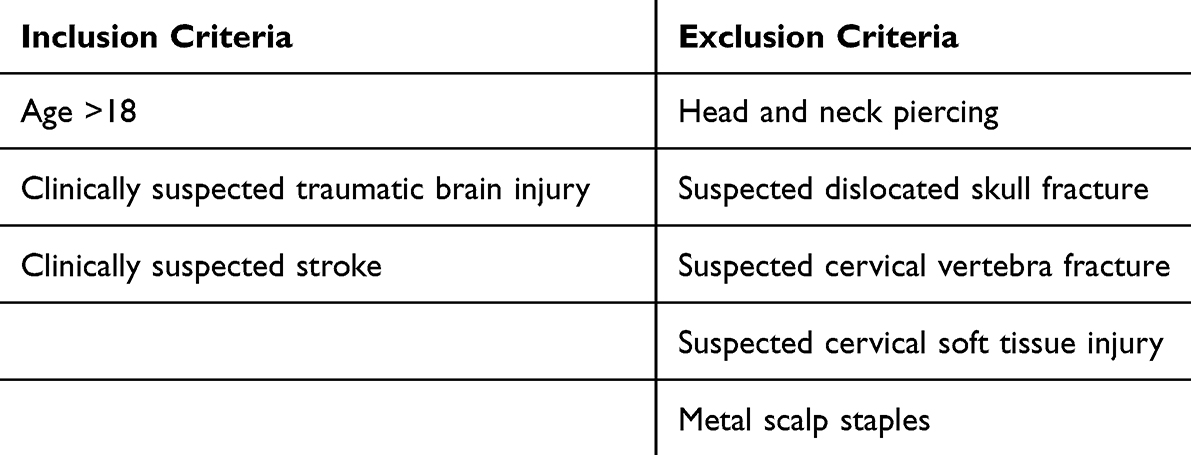 |
Table 1 Study Inclusion Criteria |
It was not within the scope of this study to evaluate the sensitivity and specificity of the results produced by the strokefinder.
Eligible patients who were included in the study were investigated with a microwave-based technology device (Strokefinder MD100, Medfield Diagnostics AB, Gothenburg, Sweden) when the attending healthcare professional felt it would be appropriate. The device was readily available in the emergency department and would be brought to the patient's bedside. Application of the device did not interfere with other diagnostic or therapeutic procedures. Measurements were performed with the subjects lying on a hospital stretcher or examination bed. A manufacturer approved plastic protective cover was used to cover the device before it came into contact with the patient for hygienic reasons. All tested patients needed to lay still throughout the duration of the measurement (approximately 45 sec). Investigators performing the tests included attendings, residents, or nurses that had been appropriately trained by the manufacturer.
The Strokefinder MD100 is designed like helmet to be used on a hospital bed or ambulance stretcher. The device has eight antennas mounted in four pairs, encircling the patient's head. Good contact of the antennas with the patient’s head can be achieved with minimal patient discomfort. The investigators adhered to the manufacturers standardized procedure on positioning the patient’s head with minimal patient manipulation. For a valid result to be produced, the head should be placed symmetrically in the device. The device’s software would perform a self-test verifying adequate contact of the antennas with the patient’s head before measurements could be allowed. If a bad alignment was indicated by the device the patient’s head would be repositioned and the diagnostics would run again. All time intervals, including repositioning, were recorded.
Results
A total of 71 patients were enrolled. All investigations were performed by trained personnel.
In 11 cases, the stokefinder was applied in the main examination area, in 21 in the triage area, in 39 cases in the resuscitation area.
In 68/71 patients, the strokefinder 100 MD was made available on the patient’s bedside and ready to apply in less than 10 minutes. In 60/71 patients, the strokefinder examination was completed with a usable result within 10 minutes. In 10/71 patients, the test did not produce usable results and in 1/71 patients, results were available in more than 10 minutes due to bad patient collaboration.
The main reasons for failure to produce a usable result with the stroke finder were anatomical difficulties due to patient built 5/10 in 4/10 cases system error and in 1/10 cases user error.
In no case (0/71), the patient was called to CT or examination by a specialist before the application of the strokefinder was completed. In no case (0/71), the application of the strokefinder was aborted due to interference with on-going resuscitation or other investigations. In no cases (0/71), the strokefinder was unable to be transferred and placed on the patient’s head due to stretcher type, patient location or crowding.
At the end of the study, all examiners described the use of strokefinder as easy to use and interpret results, easy to transfer and that the time from decision to apply until usable results where produced was short.
Discussion
This study was performed in two Greek NHS emergency departments.
The emergency department of Nikaia General Hospital “Agios Panteleimon” is the busiest in Greece with more than 1000 patient visits within 24 hours. All patients are immediately triaged upon presentation by health professionals using several triage scales including Emergency Severity Index, NEWS2 Score, HEART score and ROSIER score. High priority cases (ESI −1 and 2) are immediately transferred to the resuscitation area and whereas the rest (ESI 3–5) will wait under observation, until a healthcare professional is made available. The mean waiting time for (ESI 3–5) non-trauma patients might be as long as 6 hours. Once a patient has been evaluated by a healthcare provider and a CT scan is ordered, waiting time for transfer to CT may vary from 15 minutes for high priority cases to more than 2 hours for medium and low priority cases.
Patient arrivals at the Emergency Department of Nea Ionia “Konstantopouleio – Patision” General Hospital range from 3.500 to 4.500 per month. There is an organized triage room, where healthcare professionals using the Emergency Severity Index scoring system as well as the ROSIER SCORE access the patient and prioritize according to severity. Patients scored ESI 1 and ESI 2 are immediately transferred to the resuscitation area, whereas the others (ESI 3–5) can wait until a healthcare professional is available for up to three hours. Since there is no Neurology Specialist on call available in Konstantopouleio hospital, patients with high probability for STROKE are considered high priority cases in order to be examined and have a CT scan soon, as they need to be transferred to a hospital with a Neurology Department.
The presence of stroke cannot be determined or excluded reliably with the available clinical diagnostic tools, while the window for beneficial therapeutic interventions is closing quickly.19 All clinical stroke scales have a sensitivity between (61%-91) and a specificity between (68–92%),20 about 25% of patients will present atypical stroke symptoms.21 Both high-probability stroke patients and possible stroke mimics will need a non-contrast CT exam.12 This may lead to either under-triaging stroke patients to wait even as long as beyond the therapeutic window of IVT or over-triaging adding to the overcrowding of the CT scanner. Best practice recommendations for acute management of stroke highlight the need for early diagnosis even with a minimal level of resource availability.22 To facilitate and enhance clinical triage in detecting and stratifying stroke numerous portable technologies have emerged.23
Several different technologies are being explored including near-infrared spectroscopy, bioelectrical impedance spectroscopy and microwave imaging.
Medfield diagnostics AB has developed the MD100 Strokefinder™, as a triage support tool providing an indication of the presence of stroke. The MD 100 Strokefinder is a microwave-based technique. In controlled environments, it has shown sensitivity for detecting stroke (true positive rate) 0.97 with a 95% confidence interval of 0.75–0.97 and specificity for correctly indicating the absence of stroke (true negative rate) is 0.48 with a 95% confidence interval of 0.35–0.65.
This is the first study to investigate the feasibility of using the MD 100 Stroke finder as a point of care device in crowded emergency departments.
Point-of-Care Testing (POCT) is defined as testing at or near the site of patient care. As such, all testing is performed where clinical care or treatment is provided. The major advantage of POCT testing is rapid turnaround of test results answering specific clinical questions. This offers the potential to generate immediate and appropriate patient management response.24,25
Access to rapid diagnostic information is a core value of point-of-care (POC) technology. This is particularly relevant in acute, emergency, and critical care settings where diagnostic speed and precision directly guide the management of patients with potentially life-threatening conditions.26
The following features of POCT are ubiquitous:27
- POCT should be simple to use.
- Reagents and consumables should have durable resistance during storage and use.
- POCT results should align with established laboratory methods.
- POCT should ensure safety during testing.
Testing at or Near the Site of Patient Care
In our study this was feasible at all cases. The device lightweight and compact enough making it easy to carry to every part of the emergency department within 10 minutes. It was easy to place on any kind of bed or stretcher. As it is battery operated a power supply is not necessary. Placement of the head helmet requires very little space and is comfortable for the patient. Being remotely controlled from a wirelessly connected tablet enabled the operator not to interfere with any other resuscitation or investigational procedure. In our experience in 68/71 cases, the device was placed on the patient and was ready to use within 10 minutes from the decision to use. There was no difference in time to application neither between the two different emergency departments participating in the study nor between the different settings (examination area, triage, resuscitation area).
POCT Should Be Simple to Use
After a short training session of 12 hour, all investigators felt comfortable to use the strokefinder MD 100. There were only 1/71 cases in which an operator error occurred that led to a non-usable test result. In 5/71 cases, investigators did not manage to effectively place the device on the patient, thus not being able to complete the test. All investigators completed after each case the manufacturer’s quality control questionnaire from which derives that all investigators feel that the device is easy to use, easy to start and easy to place on a patient.
Reagents and Consumables Should Have Durable Resistance During Storage and Use
The device proved to be durable during our testing period even though it was used in a busy emergency department where instruments, despite every effort, are treated more carelessly than in other departments. The software was reliable and only in 4/71 patients did an unexplained software system error prevent obtaining usable results. The only consumable to be used with the device is the disposable hygiene cover which is placed over the instrument and in contact with the patient’s head. The battery life was adequate for a couple of tests and the charging setup made sure power supply was never a problem.
POCT Results Should Align with Established Laboratory Methods
It was not the intent of this study to verify the sensitivity or specificity of the strokefinder MD 100. Since the device has been proven to be part of our point-of-care armamentarium, a follow-up study is being designed to verify its specificity and sensitivity in various clinical settings.
POCT Should Ensure Safety During Testing
As the strokefinder MD 100 was used adhering to the manufacturer’s user manual no safety issues were raised during the testing period. No interference with or by any other device was reported despite being used in crowded areas with many other medical devices working simultaneously.
Limitations of the Study
The study was performed in only two Emergency Departments of the same health care system. Since each healthcare system and maybe even each emergency department might have different waiting times and operating procedures for triage, these results might not be globally reproducible. Further studies are needed to focus on specificity and sensitivity of the Strokefinder MD 100.
Conclusion
Among other high-risk situations cerebral stroke needs to be diagnosed as soon and as accurately as possible to prioritize the patients correct, allocate timely the necessary resources and expedite treatment. Point-of-care devices aid clinical diagnosis by performing tests and measurements at the patient's bedside. This can be challenging in a crowded emergency department where time and space are rare commodities. The Strokefinder MD 100 by Medfield Diagnostics AB fulfills all the prerequisites to be considered a point-of-care device even in the busiest emergency departments. It is easy to use, portable and durable.
Acknowledgements
The strokefinder MD 100 tested in this paper was provided for the purpose of this paper by FlexMed, 6 Semitelou Str, Athens Greece. There has been no further involvement of Medfield Diagnostics AB or FlexMed in any phase of this study. No financial or other kind of support has been received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lindner G, Woitok BK. Emergency department overcrowding: analysis and strategies to manage an international phenomenon. Wien Klin Wochenschr. 2021;133(5–6):229–233. doi:10.1007/s00508-019-01596-7
2. Sartini M, Carbone A, Demartini A, et al. Overcrowding in emergency department: causes, consequences, and solutions-a narrative review. Healthcare. 2022;10(9):1625. doi:10.3390/healthcare10091625 PMID: 36141237; PMCID: PMC9498666.
3. Ortiz SS, Huang Y, Rowe BH, Zheng B, Rosychuk RJ. Emergency department crowding negatively influences outcomes for adults presenting for chronic obstructive pulmonary disease. CJEM. 2023;25(5):411–420. doi:10.1007/s43678-023-00502-5 PMID: 37087522.
4. Pearce S, Marchand T, Shannon T, Ganshorn H, Lang E. Emergency department crowding: an overview of reviews describing measures causes, and harms. Intern Emerg Med. 2023;18(4):1137–1158. doi:10.1007/s11739-023-03239-2 PMID: 36854999; PMCID: PMC9974385.
5. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316 PMID: 30161242; PMCID: PMC6117060.
6. Zedde M, Pascarella R. Stroke is an emergency, even during a pandemic. Chest. 2023;163(3):471–472. doi:10.1016/j.chest.2022.11.017 PMID: 36894255; PMCID: PMC9989322.
7. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2023 update: a report from the American heart association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
8. Zameer S, Siddiqui AS, Riaz R. Multimodality imaging in acute ischemic stroke. Curr Med Imaging. 2021;17(5):567–577. doi:10.2174/1573405616666201130094948 PMID: 33256582.
9. Kakkar P, Kakkar T, Patankar T, Saha S. Current approaches and advances in the imaging of stroke. Dis Model Mech. 2021;14(12):dmm048785. doi:10.1242/dmm.048785 PMID: 34874055; PMCID: PMC8669490.
10. Chaudhary D, Diaz J, Lu Y, Li J, Abedi V, Zand R. An updated review and meta-analysis of screening tools for stroke in the emergency room and prehospital setting. J Neurol Sci. 2022;442:120423. doi:10.1016/j.jns.2022.120423 PMID: 36201961.
11. Hosseininezhad M, Sohrabnejad R. Stroke mimics in patients with clinical signs of stroke. Caspian J Intern Med. 2017;8(3):213–216. doi:10.22088/cjim.8.3.213 PMID: 28932374; PMCID: PMC5596193.
12. Buck H, Akhtar B, Alrohimi N, Khan A, Shuaib K. Stroke mimics: incidence, aetiology, clinical features and treatment. Ann Med. 2021;53(1):420–436. doi:10.1080/07853890.2021.1890205 PMID: 33678099; PMCID: PMC7939567.
13. Best LM, Webb AC, Gurusamy KS, Cheng SF, Richards T. Transcranial Doppler ultrasound detection of microemboli as a predictor of cerebral events in patients with symptomatic and asymptomatic carotid disease: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2016;52(5):565–580. doi:10.1016/j.ejvs.2016.05.019 PMID: 27397116.
14. Gomez JR, Hobbs KS, Johnson LL, et al. The clinical contribution of neurovascular ultrasonography in acute ischemic stroke. J Neuroimaging. 2020;30(6):867–874. doi:10.1111/jon.12771 PMID: 32857913.
15. Kilic M, Scalzo F, Lyle C, et al. A mobile battery-powered brain perfusion ultrasound (BPU) device designed for prehospital stroke diagnosis: correlation to perfusion MRI in healthy volunteers. Neurol Res Pract. 2022;4(13):doi:10.1186/s42466-022-00179-8
16. Ismail D, Mustafa S. Diagnosis of a brain stroke using wideband microwave scattering. R Soc Open Sci. 2023;10(3):221560. doi:10.1098/rsos.221560 PMID: 36968233; PMCID: PMC10031409.
17. Di Biase L, Bonura A, Caminiti ML, Pecoraro PM, Di Lazzaro V. Neurophysiology tools to lower the stroke onset to treatment time during the golden hour: microwaves, bioelectrical impedance and near infrared spectroscopy. Ann Med. 2022;54(1):2658–2671. doi:10.1080/07853890.2022.2124448 PMID: 36154386; PMCID: PMC9542520.
18. Ljungqvist J, Candefjord S, Persson M, Jönsson L, Skoglund T, Elam M. Clinical evaluation of a microwave-based device for detection of traumatic intracranial hemorrhage. J Neurotrauma. 2017;34(13):2176–2182. doi:10.1089/neu.2016.4869 PMID: 28287909; PMCID: PMC5510669.
19. Schlemm L, Endres M, Scheitz JF, Ernst M, Nolte CH, Schlemm E. Comparative evaluation of 10 prehospital triage strategy paradigms for patients with suspected acute ischemic stroke. J Am Heart Assoc. 2019;8(12):e012665. doi:10.1161/JAHA.119.012665 PMID: 31189395; PMCID: PMC6645624.
20. Budinčević H, Meštrović A, Demarin V. Stroke scales as assessment tools in emergency settings: a narrative review. Medicina. 2022;58(11):1541. doi:10.3390/medicina58111541 PMID: 36363498; PMCID: PMC9696547.
21. Jones SP, Bray JE, Gibson JM, et al. Characteristics of patients who had a stroke not initially identified during emergency prehospital assessment: a systematic review. Emerg Med J. 2021;38(5):387–393. doi:10.1136/emermed-2020-209607 PMID: 33608393; PMCID: PMC8077214.
22. Mead GE, Sposato LA, Sampaio Silva G, et al. A systematic review and synthesis of global stroke guidelines on behalf of the world stroke organization. Int J Stroke. 2023;18(5):499–531. doi:10.1177/17474930231156753 PMID: 36725717; PMCID: PMC10196933.
23. Chennareddy S, Kalagara R, Smith C, et al. Portable stroke detection devices: a systematic scoping review of prehospital applications. BMC Emerg Med. 2022;22(1):111. doi:10.1186/s12873-022-00663-z PMID: 35710360; PMCID: PMC9204948.
24. Price CP. Regular review: point of care testing. BMJ. 2001;322(7297):1285–1288. doi:10.1136/bmj.322.7297.1285 PMID: 11375233; PMCID: PMC1120384.
25. Nichols JH. Utilizing point-of-care testing to optimize patient care. EJIFCC. 2021;32(2):140–144. PMID: 34421482; PMCID: PMC8343046.
26. Damhorst GL, Tyburski EA, Brand O, Martin GS, Lam WA. Diagnosis of acute serious illness: the role of point-of-care technologies. Curr Opin Biomed Eng. 2019;11:22–34. doi:10.1016/j.cobme.2019.08.012 PMID: 34079919; PMCID: PMC8168915.
27. St John A, Price CP. Existing and emerging technologies for point-of-care testing. Clin Biochem Rev. 2014;35(3):155–167. PMID: 25336761; PMCID: PMC4204237.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.