Back to Journals » Infection and Drug Resistance » Volume 12
Diagnostic performance of direct latex agglutination, post-enrichment latex agglutination and culture methods in screening of group B streptococci in late pregnancy: a comparative study
Authors El Shahaway AA ![]() , El Maghraby HM, Mohammed HA, Abd Elhady RR, Abdelrhman AA
, El Maghraby HM, Mohammed HA, Abd Elhady RR, Abdelrhman AA ![]()
Received 5 February 2019
Accepted for publication 16 July 2019
Published 22 August 2019 Volume 2019:12 Pages 2583—2588
DOI https://doi.org/10.2147/IDR.S203543
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Alia A El Shahaway,1 Hanaa M El Maghraby,1 Heba A Mohammed,1 Rasha R Abd Elhady,2 Amr Ahmed Abdelrhman2
1Department of Medical Microbiology and Immunology, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 2Department of Obstetrics and Gynecology, Faculty of Medicine, Zagazig University, Zagazig, Egypt
Correspondence: Alia A El Shahaway
Department of Medical Microbiology and Immunology, Faculty of Medicine, Zagazig University, 12 Abdaziz Ali Street, Zagazig, Sharkia, Egypt
Tel +20 127 777 7056
Email [email protected]
Background: Group B streptococcus (GBS) is one of the main causes of neonatal sepsis.
Purpose: Evaluation of the diagnostic performance of direct latex agglutination test (DLA), post-enrichment latex agglutination (LA) test, and direct culture on chromogenic media in rapid identification of GBS carrier in pregnant women in comparison with the conventional post-enrichment CDC-recommended culture method and further to estimate GBS carriage prevalence and its antimicrobial susceptibility.
Methods: Two hundred pregnant women at gestational age (35–37 weeks) were enrolled. Three low vaginal swabs were obtained from each participant. One swab was directly inoculated into Strep B Select (SBS) agar. The second swab was inoculated in enrichment Lim broth for immunological antigen detection by post-enrichment latex agglutination (5 h and 24 h) and subculture for bacteriological detection. The third swab was used for immunological detection of GBS antigen by direct latex agglutination. The isolated GBS was subjected to antimicrobial susceptibility testing.
Results: Among 200 pregnant women, 47 (23.5%) were GBS carriers. Considering post-enrichment subculture on SBS medium as a gold standard, the sensitivities for post-enrichment 5 h and 24 h LA were 66% and 95.7%, respectively. However, direct cultivation of the vaginal swabs on SBS medium and DLA recorded 83% and 4.3%, respectively, for sensitivity. All GBS isolates (100%) were sensitive to penicillin G, ampicillin, ceftriaxone, and vancomycin. In contrast, 21.3% and 12.8% of isolated GBS were resistant to erythromycin and clindamycin, respectively.
Conclusion: Group B streptococcal antigen detection by latex agglutination after 5 h enrichment is a reliable, easy, and relatively rapid method for screening of GBS carriage in pregnant woman not in labor. Latex agglutination after 18–24 h enrichment can be used alternative to standard subculture method for screening GBS carriage.
Keywords: Streptococcus agalactiae, vaginal swab, post-enrichment, agglutination, neonatal infection
Introduction
Early-onset neonatal sepsis had been mainly attributed to Group B Streptococcus (GBS). The main method of neonate infection is passage through the birth canal of a GBS-colonized mother.1 Screening of pregnant females at gestational age (35–37 weeks) for carriage by GBS should be done, because genital GBS carriage is asymptomatic in most cases and is risky for occurrence of a neonatal disease.2,3 Infection by GBS in newborns could be anticipated by antibiotic prophylaxis for pregnant women with recto-vaginal GBS carriage, a mother who previously had a newborn with GBS illness, and pregnant women having GBS bacteriuria at any time during pregnancy.4
The Centre for Disease Control and Prevention (CDC) recommends many culture-based techniques for screening GBS carriage among pregnant females, including subculture on sheep blood agar following 24 h enrichment on Lim broth, which has a long turnaround time and the need for trained technical workers to identify suspected colonies. The use of chromogenic media is also CDC-recommended for improving recovery and simplifying identification of GBS in screening.3 Other techniques were evaluated in different studies for their effectiveness and efficacy in reducing turnaround time for the detection of GBS carriage during late pregnancy or labor, including nucleic acid amplification and hybridization techniques. Isolation and identification of GBS by post-enrichment subculture is considered the gold standard for GBS screening.3
This study aimed to compare the time effectiveness and the diagnostic performance of GBS recovery following direct culture on Strep B Select (SBS) agar as well as immunologic detection of GBS antigen either directly or post-enrichment for short-term (5 h) and long-term (18−24 h) incubation by latex agglutination with the GBS screening gold standard. This study also aimed to estimate prevalence of GBS carriage among preganant Egyptian women attending an antenatal care clinic in a tertiary care university hospital, and to further determine antibiotic-susceptibility of isolated GBS.
Subjects and methods
Study design and participants
This cross-sectional descriptive study was conducted at Zagazig University hospital, an Egyptian tertiary care hospital, during the period June 2016 to December 2017.
Using Open-Epi, the minimal sample size calculated for the study was 100 women based on an average previous estimate of 25.3% GBS colonization among Egyptian women,5 and at a 95% confidence interval. A total sample of 200 pregnant women were included in this study. The inclusion criteria were pregnant women at 35–37 weeks of gestation who planned to have vaginal delivery. Pregnant women who received antibiotics within the previous 2 weeks and those with evidence of recent urinary tract or vaginal infection were excluded.
Work-up
Triplicate distal vaginal swabs were collected from each patient for bacteriologic and immunologic tests. Two swabs were immediately cultivated for the bacteriological test. The third swab was refrigerated at 4–8°C for 48 h until GBS growth was confirmed to be immunologically tested by DLA test.
Bacteriological test
For each pregnant female, one vaginal swab of two swabs designed for bacteriological test was cultured on SBS agar (Bio-Rad, Marnes-la-Coquette, France) for evaluation of sensitivity of direct streaking on SBS agar and semi-quantification of GBS density. Immediately after collection, one vaginal swab was directly inoculated on SBS media. Plates were transferred to the microbiology laboratory in ambient air. According to the manufacturer's instructions, plates were incubated aerobically for 24–48 h at 35–37°C. Plates were checked daily for turquoise- to sky blue-colored colonies. Confirmation of GBS identification was done by using a Gram stain, a catalase test and serological identification.6 According to GBS colony forming unit (CFU) count, growth density was classified into the following categories: high (>100 CFU per swab), moderate (50–100 CFU per swab), and low (<50 CFU per swab).
Enrichment broth: immediately following collection the second swab was inoculated into a sterile screw-capped tube containing 3 mL of Lim broth (Todd-Hewitt broth supplemented with 15 µg/mL nalidixic acid and 10 µg/mL colistin). Tubes were transferred to the laboratory; tube caps were loosened, and tubes were incubated at 35–37°C in 5% CO2. After 5 h incubation, 1 mL inoculated enrichment broth was used for GBS antigen detection by latex agglutination (in ithe mmunological test). The remaining broth (2 mL) was incubated for an additional 13–19 h. After a total of 18–24 h enrichment, GBS growth was retested both bacteriologically (subcultured on SBS media) and immunologically (GBS antigen detection).
Immunological test (GBS antigen detection)
GBS antigen was detected both directly in the third vaginal swab by direct latex agglutination (DLA) test (and in the enrichment broth after 5 h incubation as well as after 18–24 h incubation. Latex agglutination was performed using PASTOREXTM STREP (Bio-Rad, Marnes-la-Coquette, France). DLA was performed after enzymatic extraction of GBS antigen from the third vaginal swab. Antigen detection was performed with some modification to the manufacturer's instructions. One drop of the latex particle was added to 4 drops of antigen extract. This allowed dilution of the latex-coated antibody concentration to be proportional to the antigen extract concentration and helped visualization of the antigen antibody reaction. Every test involved one negative control and one positive control.
According to the Lim broth manufacturer's instructions (Becton Dickinson, USA), GBS antigen can be detected after 5 h incubation. In this study this was done by vortexing enrichment broth and then 1 ml was transferred by an automatic pipette to a sterile microcentrifuge tube and centrifuged at 1000 x g for 10 min. Broth supernatant was carefully decanted and GBS antigen was enzymatically extracted from the bacterial pellet. Antigen extraction and latex agglutination were done by the same steps as for enrichment broth after 18–24 h incubation.
Antibiotic susceptibility testing
Antibiotic susceptibility testing was performed for all isolated GBS using the disk diffusion method according to CLSI guidelines.7 The tested antibiotics included penicillin G (10 units) (resistant ≥24 mm), clindamycin (2 µg) (resistant ≥19 mm), erythromycin (15 µg) (resistant ≥21 mm), ceftriaxone (10 µg) (resistant ≥24 mm), ampicillin (10 µg) (resistant ≥24 mm) and vancomycin (30 µg) (resistant ≥17 mm). The D-zone test was done to detect inducible clindamycin resistance in erythromycin-resistant strains.8 GBS strain ATCC 12403 was used as the quality control strain (American Type Culture Collection Global Bioresource Center, Manassas, VA, USA).
Ethical approvals
The study was approved by Institutional Review Board (IRB) no. 5442, Faculty of Medicine, Zagazig University. All participants provided their written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
Data were analyzed by Statistical Package of Social Science (SPSS) version 20. Quantitative data were defined using mean and standard deviation and qualitative data were defined using number and percent. Chi-square test was used to analyze the categorical variables. P-values less than 0.05 were considered significant. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPP) were calculated.
Results
Patient characteristics
The mean age of pregnant women carriers for GBS was 27.9±4.03 years with no statistically significant difference (P>0.05) either for maternal age, gestational age (weeks), or even parity Table 1.
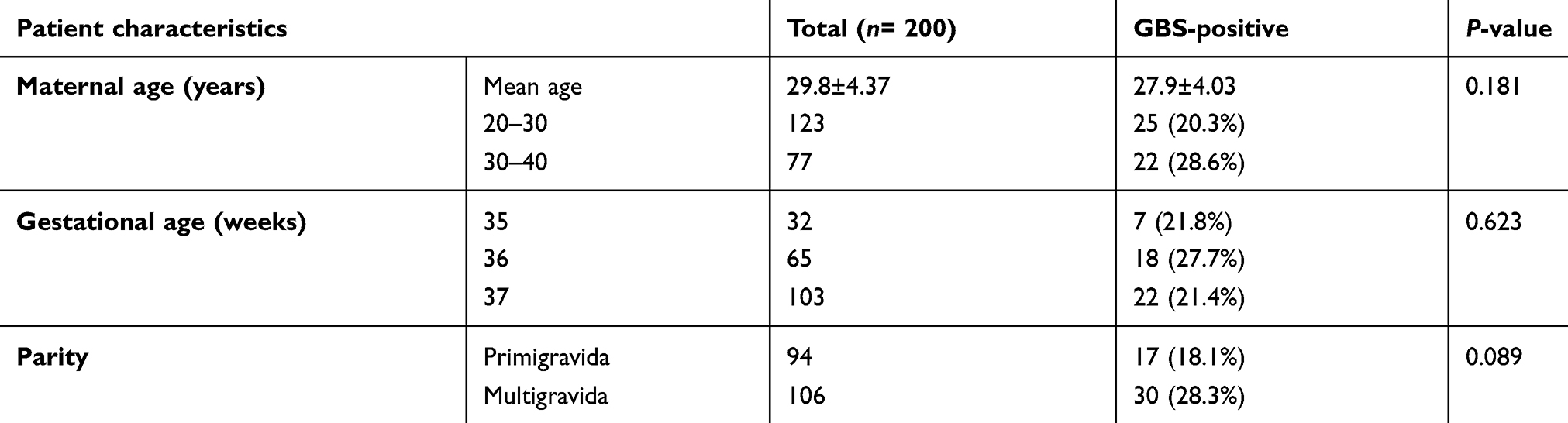 |
Table 1 Clinical characteristics of studying population |
GBS carriage detection by different methods
In this study, 47 of 200 (23.5%) pregnant women were GBS carriers using post-enrichment subculture on SBS medium recommended by the CDC. Table 2 summarizes the diagnostic performance of four methods used to screen GBS carriers. Post-enrichment 24 h LA showed the highest sensitivity (95.7%), while DLA was the least-sensitive method (4.3%). Table 3 shows that DLA sensitivity in samples of heavy growth density was 13.3%. The sensitivity of the 5 h post-enrichment LA test for heavy and moderate growth density on SBS culture was 100% and 88.8%, respectively.
 |
Table 2 Performance of direct SBS inoculation, DLA test, post-enrichment 5 h LA and post-enrichment 24 h LA results as compared with conventional post-enrichment CDC-recommended culture method results |
 |
Table 3 DLA test and post-enrichment 5 h LA results as compared with different density levels of GBS on SBS |
Antibiotic susceptibility pattern of isolated GBS
All isolated GBS strains were 100% sensitive to penicillin, ampicillin, ceftriaxone, and vancomycin., while resistance to erythromycin and clindamycin was detected in 21.3% and 12.8%, respectively. We noted that 10 (21.3%) of the GBS isolates were resistant to erythromycin; two (4.3%) of these were constitutively resistant to clindamycin. The eight (17.02%) erythromycin-resistant GBS isolates that were sensitive to clindamycinwere submitted to the D-zone test. One (2.1%) of the eight erythromycin-resistant GBS isolates had inducible clindamycin resistance.
Discussion
In this study, there was no statistically significant difference (p>0.05) in GBS carriers regarding maternal age, gestational age (weeks) and parity. This was in line with many reasonable studies.4,9 In contrast, other studies have found most GBS were isolated from pregnant females at the 37th week of gestation and whose age range was 20–30 years.10
The maternal carriage rate of GBS was (23.5%) is in agreement with results obtained by two other studies in Egypt; in Alexandria the rate was found to be 26.5%10 and in Ismalia 25.3%.5 Also, the international prevalence rate of GBS carriage was found to be 24%, 20.7%, 18.4% in Kuwait, Lebanon, and Saudi Arabia, respectively.1,11 Much lower prevalences were noticed in China (7.1%), India (7.6%), and Korea (8%).12–14 A higher colonization rate was reported in Zimbabwe as 60.3%.15 This wide variation can be linked to differences in geographic, ethnic, socioeconomic, hygiene, nutritional factors, sexual practice as well as sampling and methodological issues.
Comparison between different detection methods showed that post-enrichment 24 h LA was the best because its sensitivity was 95.7%, which was slightly lower than the sensitivity reported by Konikkara et al.,16 which was 100%. In the current study two samples were GBS-positive on subculture after Lim broth enrichment for 24 h but negative by post-enrichment 24 h LA. These samples showed scant growth of GBS with a predominance of enterococci in post-enrichment subculture, indicating a low antigenic mass of GBS in enrichment broth due to enterococci interference with its growth. Conversely, Rallu et al.1 declared that the post-enrichment antigen detection method was more sensitive and easier than standard GBS culture methods (enrichment in Lim broth for 20 h followed by subculture on blood agar) used in their study.
Direct inoculation of swabs on selective chromogenic media had 83% sensitivity when compared with subculture following enrichment; this result differs from Dunne and Holland-Staley,17 who reported that direct inoculation of a vaginal swab on selective solid media was equally sensitive to post-enrichment subculture on blood agar. Additionally, other authors reported discrepancies between direct inoculation and subculture post-enrichment using Granada medium and chromogenic medium as shown in Table 4.18–22 This difference could be explained mostly due to variations in the different preparations of the GBS-selective media, tested strains, which differ in their biochemical activities in chromogenic media, and the gold standard in each study.
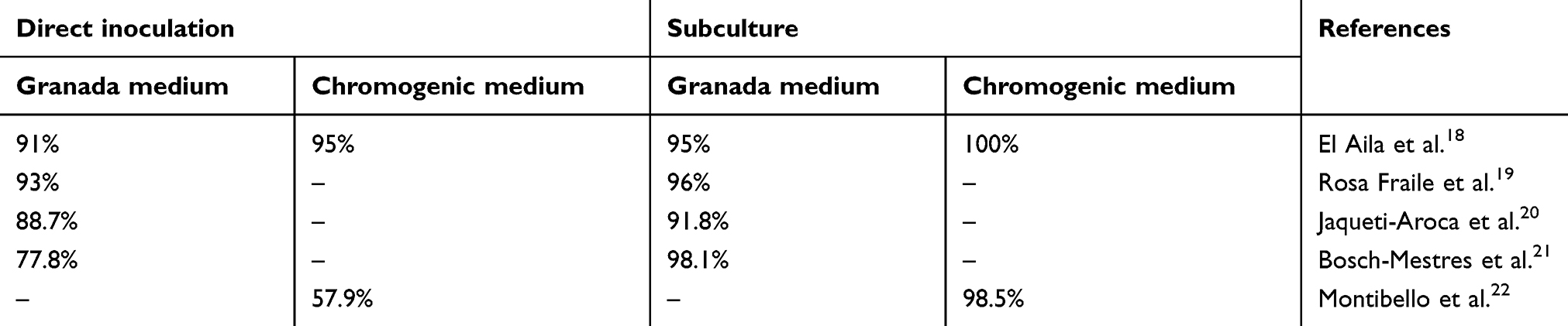 |
Table 4 Sensitivity of direct inoculation and subculture using group B streptococcus-selective medium in different studies |
This work revealed that the sensitivity of DLA was only 4.3%. Of 15 heavy-growth GBS carriage samples detected by direct plating on SBS culture, only two (13.3% sensitivity) were positive by DLA. This result is lower than that reported by Kontnick and Edberg, who reported the overall sensitivity of direct GBS antigen analysis in vaginal swabs to be 19% and much increased to reach 63% of heavily colonized females.23 In their study they classified bacterial density quantitatively in contrast to the semiquantitative method in the current study; there may also differences due to LA kit sensitivity and the GBS antigen extraction method between the two studies. Results in the current study are also much lower than those reported by Ghaddar and coworkers.24 On the other hand, many studies proved poor sensitivity and inadequacy of direct GBS antigen detection in vaginal swabs.25
In a trial to shorten the detection duration of GBS carriage, the enrichment broth was tested after 5-h incubation for GBS antigen by the LA test. The sensitivity of this method was 66%, which was slightly less sensitive than direct plating on SBS media. This difference in sensitivity was due to failure of the post-enrichment 5 h LA to identify all low-density vaginal carriage, reflecting the failure of a short incubation duration to induce increases of GBS count to reach the critical point needed for detection by the latex agglutination test.
Latex agglutination after short-term 5-h enrichment helped to identify 15 of 15 (100% sensitivity) heavily and 16 of 18 (88.8% sensitivity) moderately GBS-colonized women as classified by semiquantitative direct streaking of swabs on SBS media. Post-enrichment 5-h latex agglutination is a relatively rapid, simple test with fair overall sensitivity (66%) for GBS carriage detection and high sensitivity for heavy and moderate carriage (100% and 88.8%, respectively), which is directly related with risk of serious neonatal disease.26 However, fair sensitivity (34% false negative) and 5 h time-lapsed post-enrichment suggested that this test is not suitable for screening pregnant female in labor. Despite this limitation in sensitivity, post-enrichment 5 h latex agglutination has the advantage of providing a result after 5 h as compared to 48 h in the conventional post-enrichment culture method.
Regarding antimicrobial sensitivity testing, 100% of isolated GBS were susceptible to penicillin G, ampicillin, ceftriaxone, and vancomycin. Resistance to erythromycin was 21.3% and to clindamycin 12.8%. This was similar to the results declared by Sadeka et al.10 in Egypt, where all isolates (100%) were susceptible to penicillin, ampicillin, ceftriaxone, cefotaxime, cefepime, vancomycin, and linezolid while 22.6%, and 15% of isolated GBS were resistant to erythromycin and clindamycin, respectively. In Ethiopia, all isolated GBS were sensitive to penicillin, ampicillin, vancomycin, and gentamicin. Resistance was observed against erythromycin (6.9%) and ceftriaxone (10.3%) by Mohammed and coworkers.9
Unfortunately, Onipede et al.27 in Nigeria found high and multiple resistance patterns of GBS isolates to different antibiotics in their study, where 100% of isolates were resistant to penicillin G, ampicillin, and clindamycin and 64.7% and 70.6% were resistant to erythromycin and vancomycin, respectively. In Brazil, a lower degree of resistance was detected by Melo et al.,28 where all of the GBS isolates were susceptible to penicillin and vancomycin. They also reported that 8.1% of isolates was resistant to erythromycin and 5.9% resistant to clindamycin.28
Conclusion
Group B streptococcal antigen detection by latex agglutination after 5 h enrichment is a reliable, easy, and relatively rapid method for the screening of GBS carriage in pregnant woman not in labor. Latex agglutination after 18–24 h enrichment can be used as an alternative to the standard subculture method for screening GBS carriage.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rallu F, Barriga P, Scrivo C, Martel-Laferriere V, Laferriere C. Sensitivities of antigen detection and PCR assays greatly increased compared to that of the standard culture method for screening for group B streptococcus carriage in pregnant women. J Clin Microbiol. 2006;44:725–728. doi:10.1128/JCM.44.3.725-728.2006
2. Spellerberg B. Brandt C Streptococcus. In: Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA, editors. Manual of Clinical Microbiology.
3. Centers for Disease Control and Prevention. Prevention of perinatal Group B streptococcal disease. Revised guidelines from CDC. MMWR. 2010;59(RR–10):1–32.
4. Alp F, Findik D, Dagi HT, Arslan U, Pekin AT, Yilmaz SA. Screening and genotyping of group B streptococcus in pregnant and non-pregnant women in Turkey. J Infect Dev Ctries. 2016;10(3):222–226. doi:10.3855/jidc.6190
5. Shabayek SA, Abdalla SM, Abouzeid AM. Vaginal carriage and antibiotic susceptibility profile of group B Streptococcus during late pregnancy in Ismailia. Egypt J Infect Public Health. 2009;2(2):86–90. doi:10.1016/j.jiph.2009.03.004
6. Verani JR, McGee L, Schrag SJ. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease – revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010;59(RR–10):1–36.
7. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
8. Yusuf E, Bel A, Bouasse J, Pie´rard D. D-Zone test for detection of inducible clindamycin resistance using SirScan paper disks and Rosco Neo-Sensitabs at 25- and 15-mm distances. J Med Microbiol. 2014;63:1052–1054. doi:10.1099/jmm.0.074641-0
9. Mohammed M, Asrat D, Woldeamanuel Y, Demissie A. Prevalence of group B streptococcus colonization among pregnant women attending antenatal clinic of Hawassa Health Center, Hawassa, Ethiopia. Ethiop J Health Dev. 2012;26:36–42.
10. Sadaka SA, Aly HA, Meheissen MA, Orief YA, Arafa BM. Group B streptococcal carriage, antimicrobial susceptibility, and virulence related genes among pregnant women in Alexandria, Egypt. Alexandria Med J. 2018;54:69–76. doi:10.1016/j.ajme.2017.01.003
11. Arain FR, Al-Bezrah NA, Al-Aali KY. Prevalence of maternal genital tract colonization by group B streptococcus from Western Province, Taif, Saudi Arabia. J Clin Gynecol Obstet. 2015;4(3):258–264. doi:10.14740/jcgo341w
12. Lu B, Li D, Cui Y, Sui W, Huang L, Lu X. Epidemiology of Group B streptococcus isolated from pregnant women in Beijing, China. Clin Microbiol Infect. 2014;20:O370–O373. doi:10.1111/1469-0691.12416
13. Santhanam S, Jose R, Sahni RD, Thomas N, Beck MM. Prevalence of Group B streptococcal colonization among pregnant women and neonates in a tertiary hospital in India. J Turk Ger Gynecol Assoc. 2017;18(4):181–184. doi:10.4274/jtgga.2017.0032
14. Lee BK, Song YR, Kim MY, et al. Epidemiology of group B streptococcus in Korean pregnant women. Epidemiol Infect. 2010;138:292–298. doi:10.1017/S0950268809990859
15. Mavenyengwa RT, Afset JE, Schei B, et al. Group B streptococcus colonization during pregnancy and maternal-fetal transmission in Zimbabwe. Acta Obstet Gynecol Scand. 2010;89:250–255. doi:10.3109/00016340903398029
16. Konikkara KP, Baliga S, Shenoy S, Bharati B. Evaluation of culture, antigen detection and polymerase chain reaction for detection of vaginal colonization of Group B Streptococcus (GBS) in pregnant women. Clin Diagn Res. 2014;8(2):47–49.
17. Dunne WM, Holland-Staley CA. Comparison of NNA agar culture and selective broth culture for detection of group B streptococcal colonization in women. J Clin Microbiol. 1998;36(8):2298–2300.
18. El Aila NA, Tency I, Claeys G, et al. Comparison of different sampling techniques and of different culture methods for detection of group B streptococcus carriage in pregnant women. BMC Infect Dis. 2010;10:285. doi:10.1186/1471-2334-10-285
19. Rosa-Fraile M, Rodriguez-Granger J, Cueto-Lopez M, et al. Use of Granada medium to detect group B streptococcal colonization in pregnant women. J Clin Microbiol. 1999;37(8):2674–2677.
20. Jaqueti-Aroca J, Molina-Esteban L, García-Arata I. Comparison of 2 guidelines for detecting Streptococcus agalactiae using Granada medium. Rev Esp Quimioter. 2017;30(3):239–240.
21. Bosch-Mestres J, Martín-Fernández RM, Jiménez de Anta-Losada MT. Comparative study of three culture media for detecting Group B streptococcus colonization in pregnant women. Enferm Infecc Microbiol Clin. 2003;21(7):346–349.
22. Montibello Silvia E, Guelfand Liliana I, Machaín Mónica G, et al. Optimización de metodologías de cribaje para la búsqueda de Streptococcus agalactiae en embarazadas. Rev Argent Microbiol. 2011;43(1):4–8. doi:10.1590/S0325-75412011000100002
23. Kontnick CM, Edberg SC. Direct detection of group B streptococci from vaginal specimens compared with quantitative culture. J Clin Microbiol. 1990;28:336–339.
24. Ghaddar N, Alfouzan W, Anastasiadis E, et al. Evaluation of chromogenic medium and direct latex agglutination test for detection of group B streptococcus in vaginal specimens from pregnant women in Lebanon and Kuwait. J Med Microbiol. 2014;63:1395–1399. doi:10.1099/jmm.0.066738-0
25. Baker CJ. Inadequacy of rapid immunoassays for intrapartum detection of group B streptococcal carriers. Obstet Gynecol. 1996;88(1):51–55. doi:10.1016/0029-7844(96)00111-1
26. Melin P. Neonatal group B streptococcal disease: from pathogenesis to preventive strategies. Clin Microbiol Infect. 2011;17(9):1294–1303. doi:10.1111/j.1469-0691.2011.03576.x
27. Onipede A, Adefusi O, Adeyemi A, Adejuyigbe E, Oyelese A, Ogunniyi T. Group B streptococcus carriage during late pregnancy in ile-ife, Nigeria. Afr J Clin Exp Microbiol. 2012;13:135–143.
28. Melo SC, Santos NC, Oliveira M, et al. Antimicrobial susceptibility of Streptococcus agalactiae isolated from pregnant women. Rev Inst Med Trop Sao Paulo. 2016;58:83. doi:10.1590/S1678-9946201658025
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.