")
Back to Journals » Open Access Emergency Medicine » Volume 15
Diagnostic Impact of Hs-CRP and IL-6 for Acute Coronary Syndrome in Patients Admitted to the ED with Chest Pain: Added Value to the HEART Score?
Authors Rafiqi K , Hoeks CB, Løfgren B , Mortensen MB, Bruun JM
Received 4 July 2023
Accepted for publication 18 September 2023
Published 21 September 2023 Volume 2023:15 Pages 333—342
DOI https://doi.org/10.2147/OAEM.S425319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Khalil Rafiqi,1,2 Camilla Bang Hoeks,3 Bo Løfgren,3,4 Martin Bødtker Mortensen,5,6 Jens M Bruun1,4
1Steno Diabetes Center Aarhus, Aarhus University Hospital, Aarhus, Denmark; 2Emergency Department, Aarhus University Hospital, Aarhus, Denmark; 3Department of Internal Medicine, Randers Regional Hospital, Randers, Denmark; 4Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 5Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark; 6Ciccarone Center for Prevention of Heart Disease, Johns Hopkins, Baltimore, MD, USA
Correspondence: Khalil Rafiqi, Steno Diabetes Center Aarhus, Aarhus University Hospital, Palle Juul-Jensens Blvd. 11, Indgang A, Aarhus, 8200, Denmark, Email [email protected]
Objective: To investigate whether hs-CRP and IL-6 provide additional diagnostic value beyond that achieved by the HEART score in patients with chest pain suggestive of acute coronary syndrome (ACS) admitted to the emergency department (ED).
Methods: This was a post hoc analysis using data from the RACING-MI study. Baseline data, including hs-CRP and IL-6 levels, were analyzed using the plasma from the biobank. A total of 818 patients with chest pain suggestive of ACS were included in this analysis. Of these, 98 were diagnosed with ACS (12%). Logistic regression was used to identify the independent predictors of ACS development in patients with chest pain.
Results: hs-CRP levels > 2 mg/L were observed in 50% of all ACS cases. IL-6 levels > 1.3 pg/mL were observed in 71% of all ACS cases. hs-CRP had a sensitivity of 50% and specificity of 51% for the diagnosis of ACS, whereas IL-6 had a sensitivity of 71% and specificity of 29%. The diagnostic likelihood ratios for ACS was 1.0 for hs-CRP> 2 mg/L and IL-6 > 1.3 pg/mL, respectively. Logistic regression analysis revealed that age, male gender, and ongoing smoking were associated with ACS in patients with acute chest pain. No association was found between IL-6 or hs-CRP level and ACS. This was observed for both IL-6 and hs-CRP, whether assessed on a continuous scale or using prespecified cut-off values.
Conclusion: Among the 818 patients admitted to the ED with chest pain suggestive of ACS, neither hs-CRP nor IL-6 provided an independent added diagnostic value. Our results suggest that inflammatory markers have limited diagnostic value in detecting patients with ACS in the ED.
Keywords: admission hs-CRP and IL-6 values, HEART-score, acute coronary syndrome, diagnosis
Introduction
Chest pain is one of the most common reasons for emergency department (ED) visits. In the United States alone, more than six million patients with chest pain are evaluated in EDs each year.1 The potential etiologies vary from harmless to life-threatening manifestations of acute coronary syndrome (ACS). Any delay in the diagnosis and treatment of ACS can have a negative impact on the prognosis.2,3 Risk stratification to safely identify patients at low risk of ACS has the potential to reduce the length of stay in the ED, thereby reducing the patient burden, frequency of hospitalization, and costs.4,5
The Global Registry of Acute Coronary Events (GRACE) score6 and Thrombolysis in Myocardial Infarction (TIMI) score7 are widely used risk evaluation scores that were initially developed for a large number of patients with confirmed ACS and have later been validated for use in patients admitted to the ED with suspected ACS.8–10 The HEART score is another validated risk score that consists of five elements: History, ECG, Age, Risk factors, and Troponin (Table 1). It can stratify patients with chest pain into low-, moderate-, and high-risk groups based on the development of major adverse cardiac events.11 Comparisons among the three risk scores demonstrated that the HEART score outperformed both GRACE and TIMI in safely identifying low-risk patients admitted to the ED with suspected ACS.11–14 However, other important biochemical parameters such as inflammatory biomarkers were not incorporated into the HEART score. Inflammation is thought to be an important factor in ACS through its role in the initiation and progression of coronary plaque disruption and is reflected by an increase in multiple inflammatory markers such as C-reactive protein (CRP) and Interleukin-6 (IL-6).15–20 As an example, the CANTOS study found that Canakinumab, a specific human monoclonal anti-human IL-1β antibody, significantly reduced IL-6 fibrinogen, CRP, and led to a significantly lower rate of recurrent cardiovascular events than placebo.21
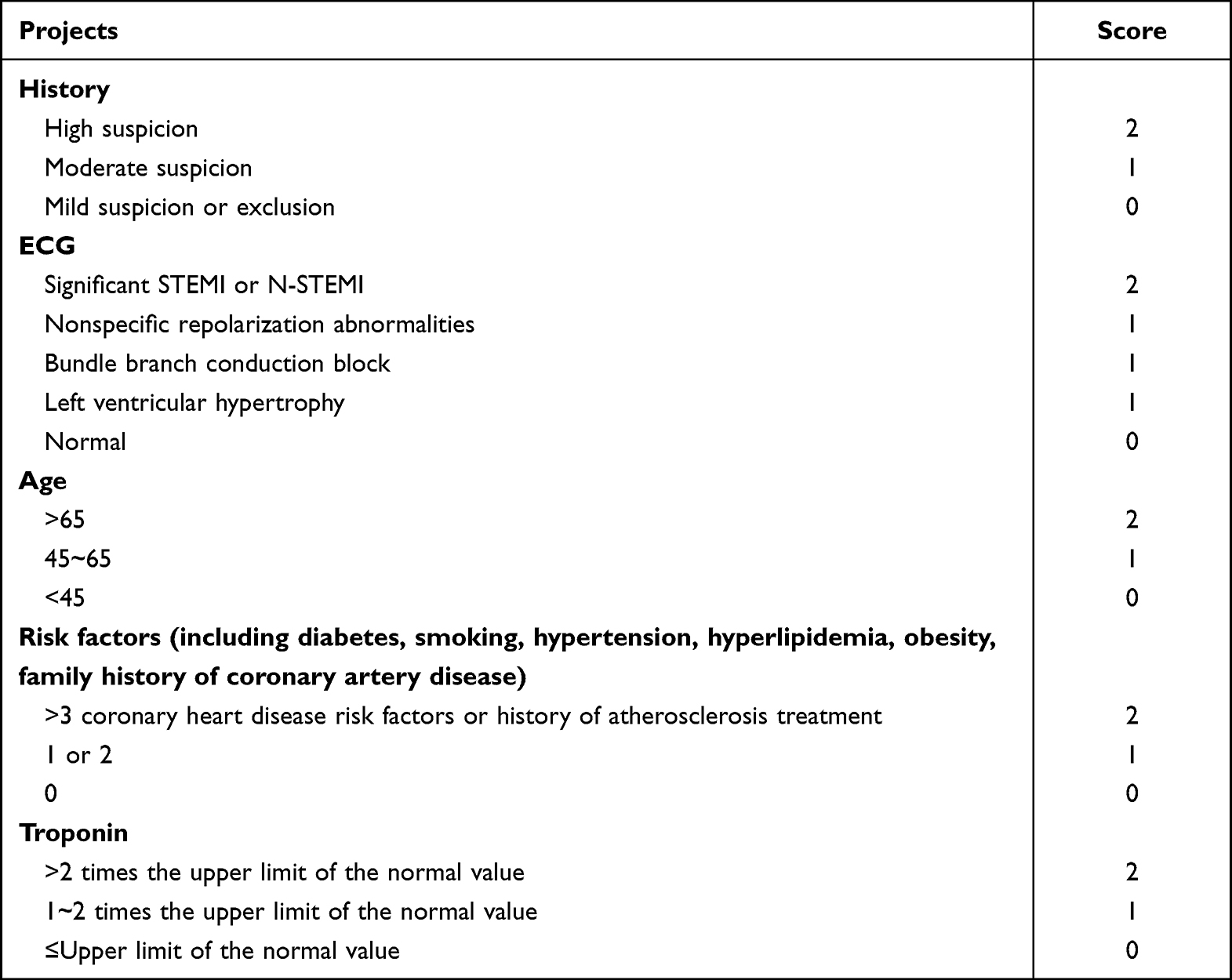 |
Table 1 HEART Score |
The present study aimed to investigate whether the ACS-related inflammatory markers hs-CRP and IL-6 add diagnostic value to the HEART score in patients with chest pain suggestive of ACS admitted to the ED.
Methods
Study Design
This study was a post-hoc analysis based on a single-center clinical cohort study, the Rapid Use of High-Sensitive Cardiac Troponin I for Ruling-in and Ruling-out of Acute Myocardial Infarction: the RACING-MI cohort study.22,23 The RACING-MI cohort study was conducted between November 2016 and February 2019 and included patients with chest pain indicative of ACS who were admitted to the ED at a Danish regional hospital. The study design and methods have been previously described and published.22 The RACING-MI protocol was approved by The Regional Committee on Health Research Ethics (no.1-10-72-213-16). The investigation conforms with the principles outlined in the Declaration of Helsinki and the Danish Health Act. Written and oral informed consent was obtained from all subjects, including permission to store and use blood in a biobank for future research (no. 1-16-02-530-16). Approval to perform post-hoc analysis of hs-CRP and IL-6 for this specific study was also obtained (no.1-10-72-206-22).
Patients
All patients admitted to the ED with chest pain suggestive of ACS were eligible for inclusion in the study, see Figure 1. As part of the standard procedure, a prehospital examination was performed on all patients, including ECG and point-of-care cardiac Troponin T in the ambulance. Patients with ST-segment elevation myocardial infarction (STEMI) or significant troponin elevation were transferred directly to a University Hospital with an invasive heart center.24 Patients with non-STEMI or unstable angina pectoris were transferred to regional hospitals (ie Randers Regional Hospital) for further diagnostic investigation and clarification.24
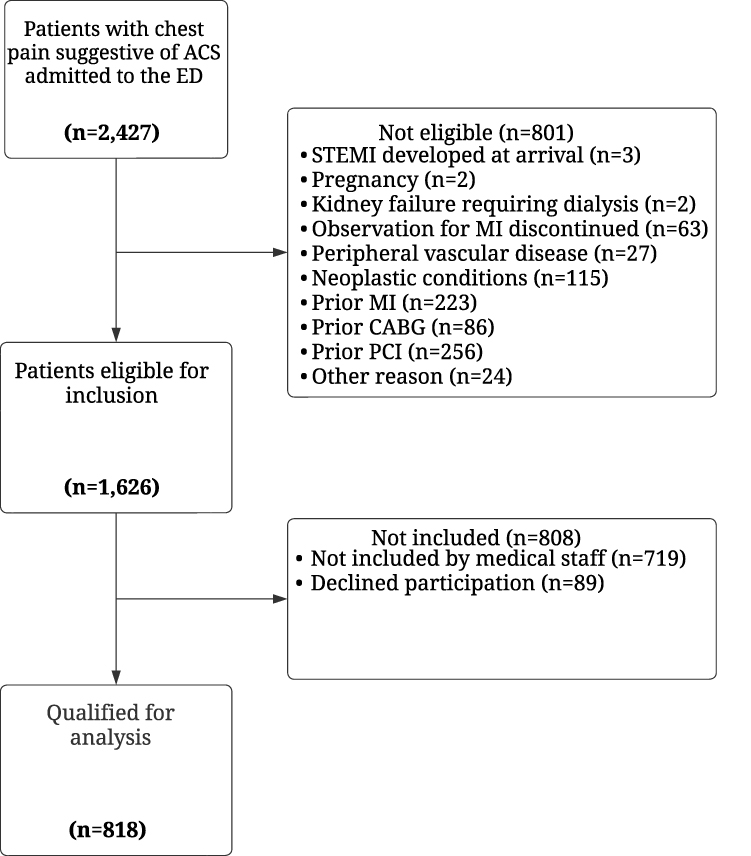 |
Figure 1 Patient flow-chart. Abbreviations: ACS, Acute Coronary syndrome; ED, Emergency department; STEMI; ST-elevation myocardial infarction; MI, Acute myocardial infarction; CABG, Coronary artery bypass graft; PCI, percutaneous coronary intervention. |
Excluded from the study were patients with STEMI at admission, age ≤18, pregnancy, kidney failure requiring dialysis, prior MI, treatment with percutaneous coronary intervention (PCI), and/or coronary artery bypass graft. Due to potentially high levels of inflammatory biomarkers, patients with signs of infectious disease, cerebral hemorrhage or stroke, peripheral vascular disease, neoplastic conditions, known thrombotic disorders, dilated cardiomyopathy, surgery, or major trauma in the last month were also excluded.25
Study Procedures
All patients underwent standard protocol care for chest pain suggestive of ACS. After oral and written consent were obtained, a research assistant registered all baseline parameters, including vital parameters, admission blood samples, serial troponin measurements, concomitant disease, medication upon admission to the ED, and patient demographics. In addition, all patients completed a 19-item questionnaire focusing on chest pain characteristics and cardiovascular risk profiles. Additional blood from each patient was stored in a biobank for future research, and hs-CRP and IL-6 levels were analyzed in the frozen plasma samples.
Determination of Hs-CRP and IL-6 Assays and HEART Score
Measurements of hs-CRP and IL-6 levels were performed using the plasma from the biobank. Siemens ADVIA Chemistry CardioPhase™ High Sensitivity C‑Reactive Protein Reagents (Siemens Healthcare GmbH, Erlangen, Germany) were used to analyze hs-CRP levels. IL-6 levels were analyzed using Siemens Advia Centaur® IL-6 (Siemens Healthcare GmbH, Erlangen, Germany). The methods were accredited according to Danish, European and International standards for medical laboratories (DS/EN ISO 15189). The Limit of Detection (LoD) was provided by the manufacturer to be 0.1 mg/L for the hs-CPR assay and 2.7 pg/mL for the IL-6 assay. The 97.5th percentile cut-off point for both sexes were 7.6 mg/L for the hs-CRP assay and 4.4 pg/mL for the IL-6 assay. The cut-off point for hs-CRP ≥ 2 mg/L has been used in large clinical trials26 while the mean value of IL-6 in healthy individuals has previously been found to be 1.3 pg/mL.27
Variables included in the HEART score were readily available after patients underwent examination in the ED. The total score was 10 points and was calculated using the software affiliated with the database. The patients were stratified into low group (0–3 points), moderate group (4–6 points), and high-risk groups (7–10 points) groups. The HEART scoring system is presented In Table 1.
Endpoints
The primary endpoint was whether hs-CRP and IL-6 levels provided additional diagnostic value when combined with the HEART score in patients with chest pain who were admitted to the ED with a low risk of ACS.
Adjudication of Final Diagnosis
The 4th universal definition of MI, which includes relative troponin changes, was used to diagnose patients with ACS.28 All patients underwent a 30-day follow-up for major adverse cardiac events after discharge from the hospital. Adjudication was made independently by two physicians and was based on available clinical data from admission to the ED until 30 days after discharge. In the event of a discrepancy, consensus was achieved by consulting a senior attending Cardiologist.23
Statistical Analysis
Quantile–quantile plots and histograms were used to analyze data with a normal distribution. Continuous variables are presented as mean ±standard deviation (SD) and categorical variables are presented as counts and percentages. Variables with non-normal distributions are displayed as medians (lower quartile (Q1)] to upper quartile (Q3)). In accordance with the Wilson score method, endpoint measures were calculated using 95% confidence intervals (CI). Logistic regression was used to calculate the odds ratios (ORs) and 95% Cis for development ACS. The models were adjusted for age, sex, smoking status, and diabetes status. Two logistic regression models were constructed: one with Hs-CRP and IL-6 as continuous variables and another with HS-CRP and IL-6 with the chosen cut-off points (Hs-CRP > 2 mg/L and IL-6 >1.3 pg/mL). Statistical analyses were performed using the R version 6.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
During the original study period, 2427 consecutive patients were admitted to the ED with chest pain suggestive of ACS. A total of 818 patients were included in the current analysis according to the exclusion criteria. The patient flowchart is shown in Figure 1 and patient characteristics are listed in Table 2. The baseline values of the inflammatory and lipid markers stratified by ACS as the final diagnosis are presented in Table 3.
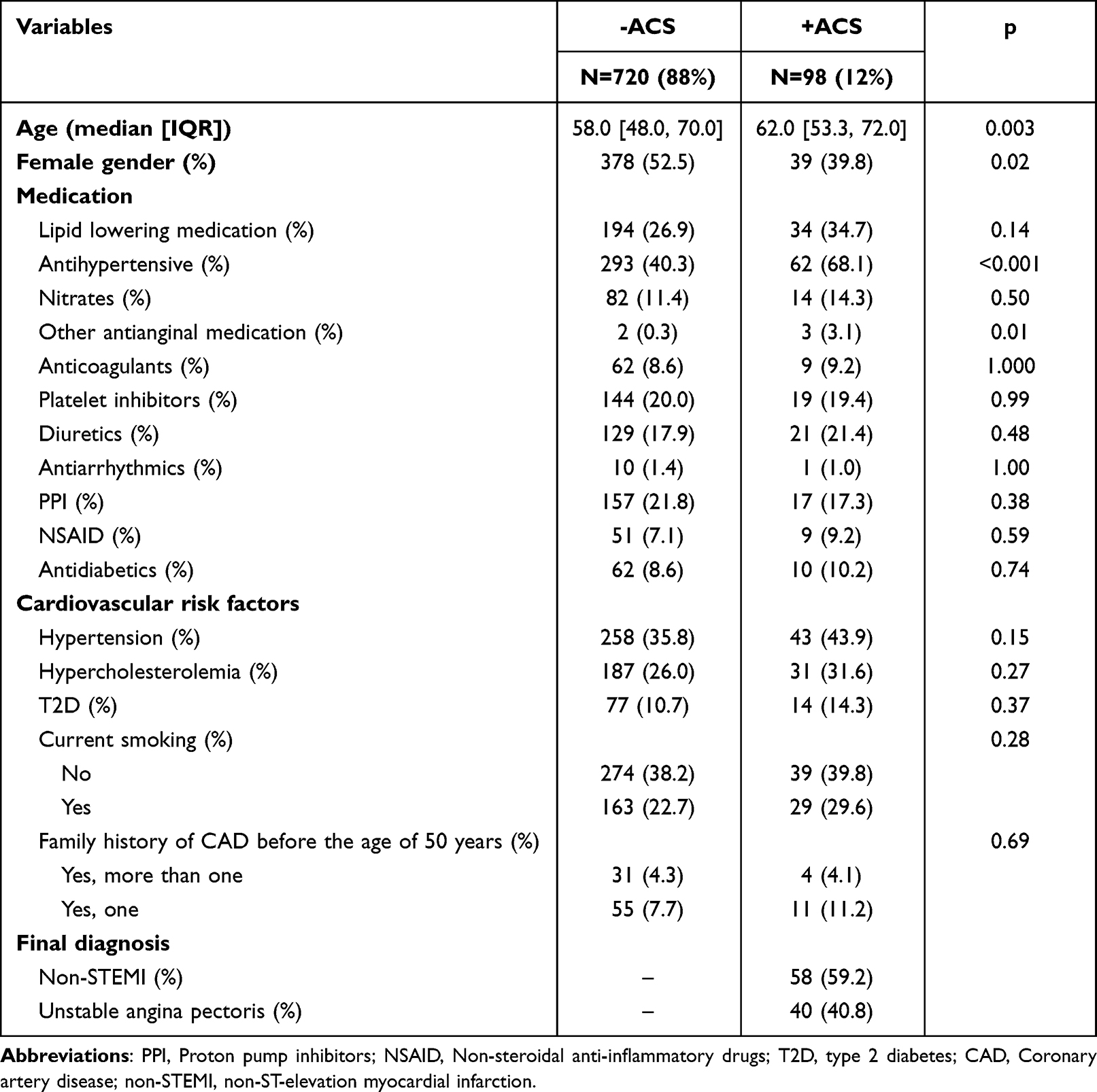 |
Table 2 Baseline Characteristics of Patients Without (-ACS) and with (+ACS) |
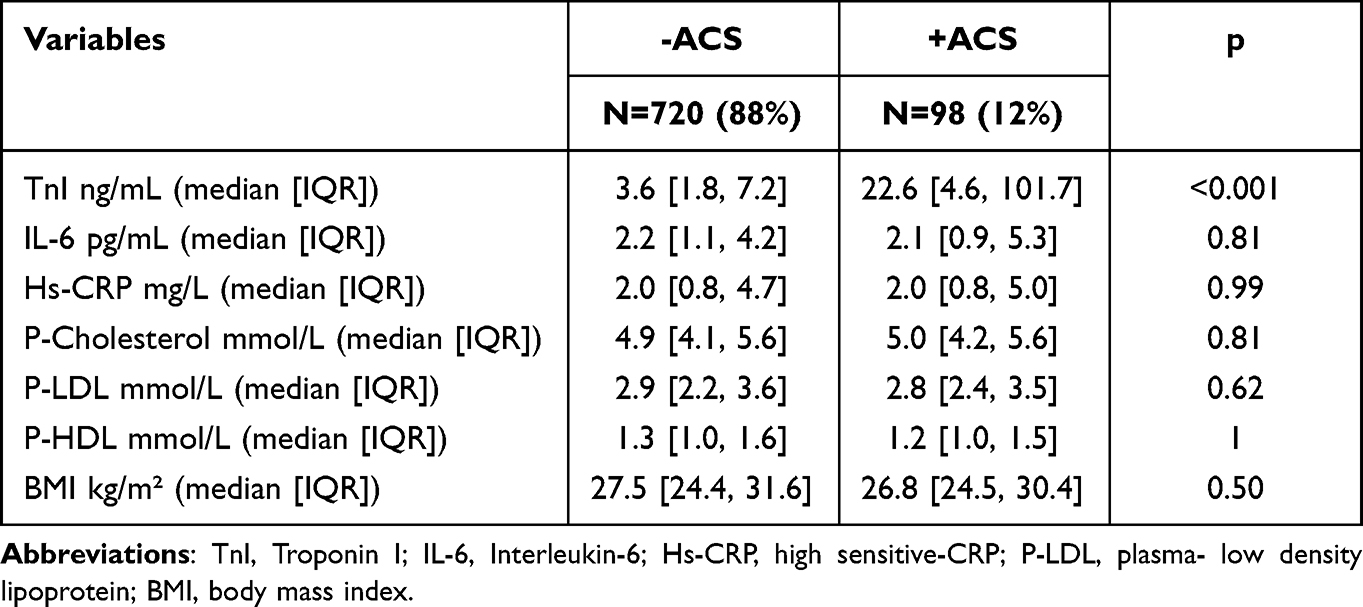 |
Table 3 Baseline Values Based on Patients with and without ACS |
Occurrence of ACS
Of the 818 patients included in this study, 98 patients were diagnosed with ACS (12%). Of the 98 patients, 58 (59%) were diagnosed with non-STEMI, and 40 (41%) with unstable angina pectoris. Of the 98 patients diagnosed with ACS, 14 (14.3%) had type 2 diabetes (T2D). Other cardiovascular diseases (eg, heart failure, aortic dissection, and arrhythmia) accounted for 10% of the study group. Patients diagnosed with a non-cardiovascular disease (eg, infection, dyspepsia, gastric ulcers) constituted of 238 (29%) patients, and in total 432 (53%) were discharged after evaluation in the ED without any diagnosis requiring treatment (eg, musculoskeletal pain). During the 30-day adjudication period, none of the 720 patients who were not diagnosed with ACS at admission experienced major adverse cardiac events.
Diagnostic Value of Admission Hs-CRP and IL-6 for ACS
In total, 403 patients had hs-CRP levels >2 mg/L, which amounted to 50% (49 patients) of all the patients. Similarly, IL-6 levels > 1.3 pg/mL were found in 574 patients, and they constituting 71.4% (70 patients) of all ACS patients. Diagnostic value of hs-CRP and IL-6 for the diagnosis of ACS is presented in Table 4 and was 1.0 for hs-CRP>2 mg/L and IL-6 > 1.3 pg/mL, respectively.
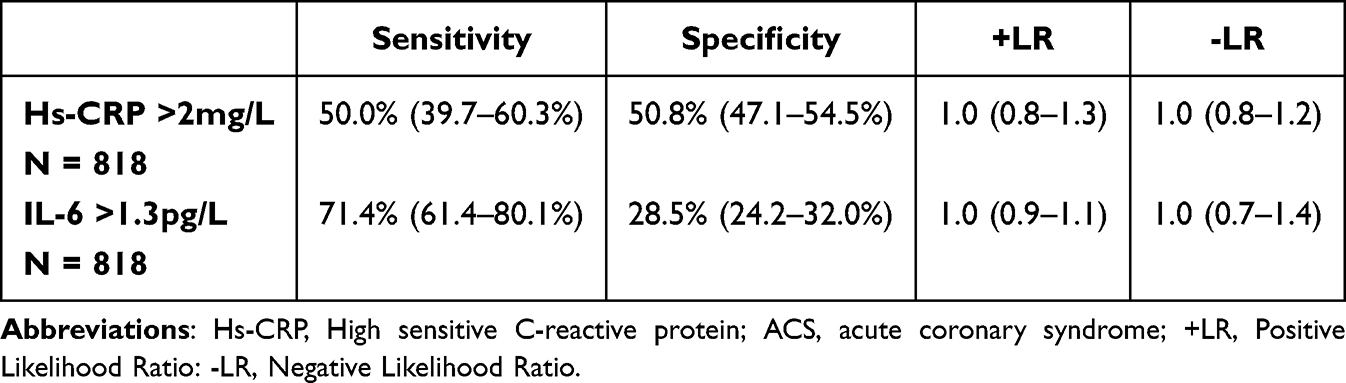 |
Table 4 Diagnostic Value of Hs-CRP > 2mg/L and IL-6 >1.3 Pg/L for the Diagnosis of ACS |
Independent Association Between Inflammatory Markers and ACS in Patients with Acute Chest Pain
Table 5 and Table 6 summarize the results of the logistic regression analyses of the factors associated with ACS in patients with acute chest pain. The logistic regression analyses were adjusted for age, sex, smoking status, and diabetes. Age, male sex, and ongoing smoking are associated with ACS in patients with acute chest pain. In contrast, there was no association between IL-6 or hs-CRP level and ACS. This was true for IL-6 and hs-CRP at both continuous and prespecified cut-off values.
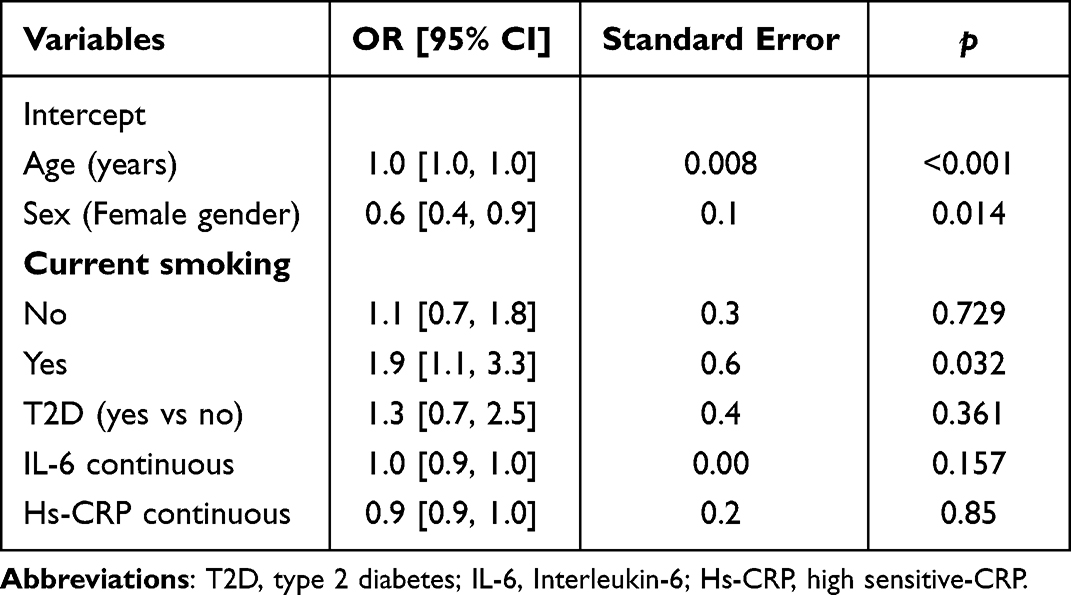 |
Table 5 Logistic Regression Analysis with Continuous Values of IL-6 and Hs-CRP, Outcome: ACS (n=98) |
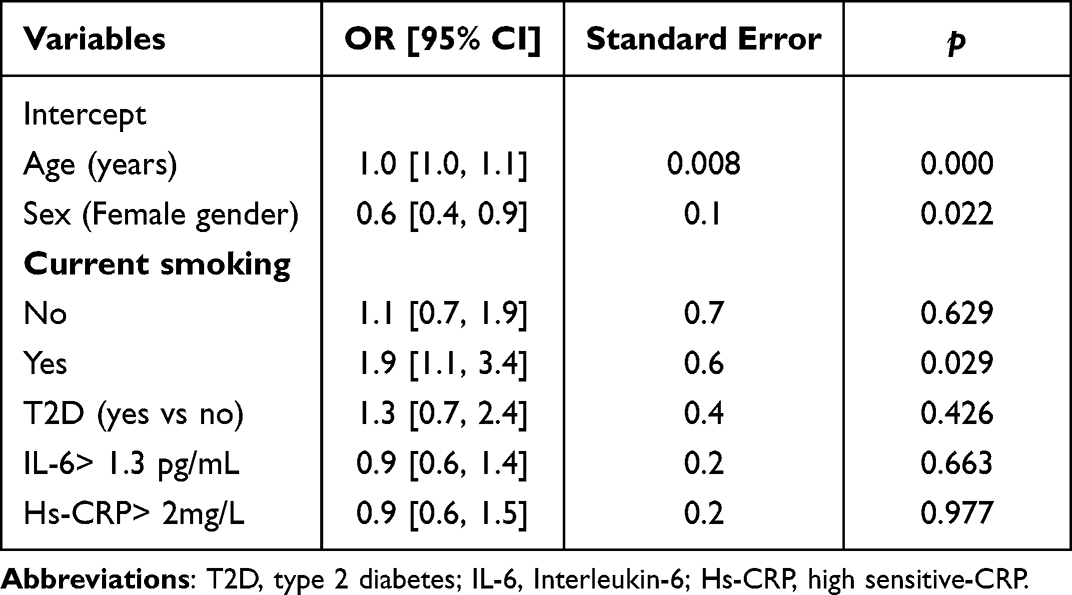 |
Table 6 Logistic Regression Analysis with Prespecified Cut-off Values of IL-6 and Hs-CRP, Outcome: ACS (n=98) |
Discussion
Summary
The present study investigated whether the cardiovascular inflammatory risk markers hs-CRP and IL-6 provide additional diagnostic value for ACS beyond that achieved using the HEART score. Among 818 patients admitted to the ED with chest pain suggestive of ACS, our results showed that neither hs-CRP nor IL-6 provided independent diagnostic value, as demonstrated by 1) similar levels of hs-CRP and IL-6 in patients with versus without ACS, 2) diagnostic likelihood ratios of 1.0 for both inflammatory markers, and 3) that hs-CRP and Il-6 are not independently associated with a higher risk of ACS.
Taken together, the present study adds to the available literature by demonstrating that inflammatory markers do not provide diagnostic value in the workup of patients with chest pain who are being evaluated for ACS.
Previous Literature
A diagnostic threshold of 25 mg/L for CRP showed sensitivity for the diagnosis of ACS of 93%, specificity of 65%, and negative predictive value of 96% in a setting with an invasive heart center [20]. In Another study using a population-based threshold for CRP level ≥3.16 mg/L showed sensitivity for the diagnosis of ACS of 70%) and specificity of 74%).20,29 These studies reported significantly higher levels of sensitivity and specificity than those in the present study.
However, previous studies have used conventional CRP measurements, whereas hs-CRP levels were measured in this study. This study is consistent with a previous study on low-risk chest pain patients by Diercks et al, which used a diagnostic threshold of hs-CRP ≥2 mg/L. The study reported a sensitivity for and diagnosis of ACS of 53.1% and specificity of 50.3%.30 In another study in which 1028 patients developed STEMI, the mean levels of IL-6 were found to be 18.7 pg/mL and mean CRP levels of 13.0 mg/L, and a significant correlation between peak troponins and IL-6 and CRP was also found.31 The levels of the inflammatory markers were significantly lower in the present study. As patients with STEMI were not included in the study, the results may underestimate the true values of hs-CRP and IL-6 in patients with ACS.
In this study, cut-off values of 2 mg/L for hs-CRP and 1.3 pg/mL for IL-6 were used, as these values have been used in large-scale clinical trials to define the increased risk of cardiovascular events.26,32 Nevertheless, uniform cutoff points for inflammatory markers eg, such as hs-CRP and IL-6, may be challenging because BMI, diabetes mellitus, hypertension, physical activity, alcohol consumption, smoking, and other factors cause baseline variation.25,27
Clinical Perspective
Patients admitted to the ED with acute chest pain suggestive of ACS may find it challenging to obtain a quick and accurate diagnosis. It is necessary to quickly and safely stratify patients to offer optimal treatment for cardiovascular events. The HEART score has been found to be an effective tool for identifying patients with low risk of cardiac ischemia who can be safely discharged early after hospitalization.13,33,34
This study investigated whether hs-CRP and IL-6 levels could provide diagnostic value in combination with the HEART score. Prior studies have used TIMI and GRACE scores in combination with hs-CRP and other serum biomarkers to investigate whether they provide improved risk stratification for patients with ACS.35,36 Klingenberg et al found that combinations of biomarkers, including hsTnT, NT-proBNP, and hs-CRP, with GRACE scores enhanced risk discrimination in patients with ACS.35 The current HEART score includes only the laboratory-based biomarker troponin. Variables that reflect the other pathophysiological characteristics of ACS may provide additional diagnostic information. Despite the important role of inflammation in the pathogenesis of atherothrombosis, including myocardial infarction, our findings do not support the notion that inflammatory markers such as hs-CRP and IL-6 provide diagnostic value for detecting ACS among patients with chest pain in combination with the HEART score.
One major strength of the HEART score is that it is a readily available diagnostic tool that requires only information available shortly after admission, together with the troponin level, and can be used in both large hospitals with a coronary catheterization facility and in smaller hospitals with no invasive capabilities. The HEART score summarizes the descriptions and reflections of patients with chest pain. This could have major effects on minimizing unnecessary and expensive bed allocation, which could further increase patient safety as overcrowded ED’s have been linked to increased mortality.37 Furthermore, faster diagnosis of patients with cardiovascular events may reduce the time to thrombolysis and/or revascularization, although its effect on morbidity and mortality is still unknown. IL-6 and hs-CRP levels have limited diagnostic value as independent markers in patients with chest pain admitted to the ED with a low risk of ACS. Therefore, we do not recommend that Il-6 and hs-CRP be implemented in clinical practice in the ED because they will most likely not help with a faster diagnosis of patients with cardiovascular events. Larger prospective studies are necessary to confirm the findings of the present study.
Limitations
This study was based on data obtained from a single center. The study relied on the medical staff for patient inclusion and blood sampling. Therefore, not all patients admitted to the ED with chest pain were included in the study, and blood samples were unavailable for IL-6 and hs-CRP measurements. This could have increased the risk of unintended lack of inclusion, resulting in selection bias. However, there is no reason to suspect that patients who were not included in the study by the medical staff were different from the included patients. This was a post hoc analysis of blood samples from a biobank, which means that we did not have multiple blood test samples from each patient. The concentration of inflammatory markers may peak later, which may have impeded the hs-CRP and IL-6 results.38 However, in patients with chest pain, the focus is on myocardial necrosis markers; therefore, it is difficult to take serial hs-CRP and IL-6 measurements.
Conclusion
Among the 818 patients admitted to the ED with chest pain suggestive of ACS, neither hs-CRP nor IL-6 provided an independent added diagnostic value. Our results suggest that inflammatory markers have limited diagnostic value in detecting patients with ACS in the ED.
Abbreviations
ACS, Acute coronary syndrome; ECG, Electrocardiogram; ED, Emergency Department; GRACE, The Global Registry of Acute Coronary Events; HEART-score, History, ECG, Age, Risk factors, Troponin-score; Hs-CRP, High sensitive C-reactive protein; IL-6, Interleukin-6; MI, Myocardial Infarction; PCI, Percutaneous coronary intervention; RACING-MRACING-MI, Rapid Use of High-Sensitive Cardiac Troponin I for Ruling-in and Ruling- out of myocardial infarction; STEMI, ST-segment elevation MI; SD, Standard deviation; TIMI, Thrombolysis in Myocardial Infarction score; T2D, Type 2 diabetes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ko DT, Dattani ND, Austin PC, et al. Emergency department volume and outcomes for patients after chest pain assessment. Circ Cardiovasc Qual Outcomes. 2018;11(11):e004683. doi:10.1161/circoutcomes.118.004683
2. Maroko PR, Kjekshus JK, Sobel BE, et al. Factors influencing infarct size following experimental coronary artery occlusions. Circulation. 1971;43(1):67–82. doi:10.1161/01.cir.43.1.67
3. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–2619. doi:10.1093/eurheartj/ehu278
4. Six AJ, Backus BE, Kingma A, Kaandorp SI. Consumption of diagnostic procedures and other cardiology care in chest pain patients after presentation at the emergency department. Neth Heart J. 2012;20(12):499–504. doi:10.1007/s12471-012-0322-6
5. Hoffmann U, Truong QA, Schoenfeld DA, et al. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012;367(4):299–308. doi:10.1056/NEJMoa1201161
6. Grace Investigators. Rationale and design of the GRACE (Global Registry of Acute Coronary Events) Project: a multinational registry of patients hospitalized with acute coronary syndromes. Am Heart J. 2001;141(2):190–199. doi:10.1067/mhj.2001.112404
7. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284(7):835–842. doi:10.1001/jama.284.7.835
8. Than M, Cullen L, Reid CM, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet. 2011;377(9771):1077–1084. doi:10.1016/s0140-6736(11)60310-3
9. Than M, Flaws D, Sanders S, et al. Development and validation of the emergency department assessment of chest pain score and 2 h accelerated diagnostic protocol. Emerg Med Australas. 2014;26(1):34–44. doi:10.1111/1742-6723.12164
10. Reaney PDW, Elliott HI, Noman A, Cooper JG. Risk stratifying chest pain patients in the emergency department using HEART, GRACE and TIMI scores, with a single contemporary troponin result, to predict major adverse cardiac events. Emerg Med J. 2018;35(7):420–427. doi:10.1136/emermed-2017-207172
11. Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART score. Neth Heart J. 2008;16(6):191–196. doi:10.1007/bf03086144
12. Poldervaart JM, Langedijk M, Backus BE, et al. Comparison of the GRACE, HEART and TIMI score to predict major adverse cardiac events in chest pain patients at the emergency department. Int J Cardiol. 2017;227:656–661. doi:10.1016/j.ijcard.2016.10.080
13. Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol. 2013;168(3):2153–2158. doi:10.1016/j.ijcard.2013.01.255
14. Six AJ, Cullen L, Backus BE, et al. The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study. Crit Pathw Cardiol. 2013;12(3):121–126. doi:10.1097/HPC.0b013e31828b327e
15. Vigushin DM, Pepys MB, Hawkins PN. Metabolic and scintigraphic studies of radioiodinated human C-reactive protein in health and disease. J Clin Invest. 1993;91(4):1351–1357. doi:10.1172/jci116336
16. Gauldie J, Richards C, Harnish D, Lansdorp P, Baumann H. Interferon beta 2/B-cell stimulatory factor type 2 shares identity with monocyte-derived hepatocyte-stimulating factor and regulates the major acute phase protein response in liver cells. Proc Natl Acad Sci USA. 1987;84(20):7251–7255. doi:10.1073/pnas.84.20.7251
17. Cainzos-Achirica M, Miedema MD, McEvoy JW, et al. The prognostic value of high sensitivity C-reactive protein in a multi-ethnic population after >10 years of follow-up: the Multi-Ethnic Study of Atherosclerosis (Mesa). Int J Cardiol. 2018;264:158–164. doi:10.1016/j.ijcard.2018.02.027
18. Nakachi T, Kosuge M, Hibi K, et al. C-reactive protein elevation and rapid angiographic progression of nonculprit lesion in patients with non-ST-segment elevation acute coronary syndrome. Circ J. 2008;72(12):1953–1959. doi:10.1253/circj.cj-08-0185
19. Mitchell AM, Garvey JL, Kline JA. Multimarker panel to rule out acute coronary syndromes in low-risk patients. Acad Emerg Med. 2006;13(7):803–806. doi:10.1197/j.aem.2006.03.553
20. Magadle R, Weiner P, Beckerman M, Berar-Yanay N. C-reactive protein as a marker for active coronary artery disease in patients with chest pain in the emergency room. Clin Cardiol. 2002;25(10):456–460. doi:10.1002/clc.4960251004
21. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
22. Bang C, Hansen C, Lauridsen KG, et al. Rapid use of high-sensitive cardiac troponin I for ruling-in and ruling-out of acute myocardial infarction (RACING-MI): study protocol. Open Heart. 2019;6(1):e000995. doi:10.1136/openhrt-2018-000995
23. Bang C, Lauridsen KG, Frederiksen CA, et al. Rapid rule-out of myocardial infarction after 30 minutes as an alternative to 1 hour: the RACING-MI cohort study. Ann Emerg Med. 2021;79:102–112. doi:10.1016/j.annemergmed.2021.08.024
24. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/clep.S179083
25. Kones R. Rosuvastatin, inflammation, C-reactive protein, Jupiter, and primary prevention of cardiovascular disease--a perspective. Drug Des Devel Ther. 2010;4:383–413. doi:10.2147/DDDT.S10812
26. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359(21):2195–2207. doi:10.1056/NEJMoa0807646
27. Knudsen LS, Christensen IJ, Lottenburger T, et al. Pre-analytical and biological variability in circulating interleukin 6 in healthy subjects and patients with rheumatoid arthritis. Biomarkers. 2008;13(1):59–78. doi:10.1080/13547500701615017
28. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20):e618–e651. doi:10.1161/cir.0000000000000617
29. Liyan C, Jie Z, Yonghua W, Xiaozhou H. Assay of ischemia-modified albumin and C-reactive protein for early diagnosis of acute coronary syndromes. J Clin Lab Anal. 2008;22(1):45–49. doi:10.1002/jcla.20223
30. Diercks DB, Kirk JD, Naser S, Turnipseed S, Amsterdam EA. Value of high-sensitivity C-reactive protein in low risk chest pain observation unit patients. Int J Emerg Med. 2011;4:37. doi:10.1186/1865-1380-4-37
31. Ritschel VN, Seljeflot I, Arnesen H, et al. IL-6 signalling in patients with acute ST-elevation myocardial infarction. Results Immunol. 2014;4:8–13. doi:10.1016/j.rinim.2013.11.002
32. Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005;352(1):20–28. doi:10.1056/NEJMoa042378
33. Mahler SA, Miller CD, Hollander JE, et al. Identifying patients for early discharge: performance of decision rules among patients with acute chest pain. Int J Cardiol. 2013;168(2):795–802. doi:10.1016/j.ijcard.2012.10.010
34. Oliver JJ, Streitz MJ, Hyams JM, et al. An external validation of the HEART pathway among emergency department patients with chest pain. Intern Emerg Med. 2018;13(8):1249–1255. doi:10.1007/s11739-018-1809-y
35. Klingenberg R, Aghlmandi S, Räber L, et al. Improved risk stratification of patients with acute coronary syndromes using a combination of hsTnT, NT-proBNP and hsCRP with the GRACE score. Eur Heart J Acute Cardiovasc Care. 2018;7(2):129–138. doi:10.1177/2048872616684678
36. Manenti ER, Bodanese LC, Camey SA, Polanczyk CA. Prognostic value of serum biomarkers in association with TIMI risk score for acute coronary syndromes. Clin Cardiol. 2006;29(9):405–410. doi:10.1002/clc.4960290907
37. Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006;184(5):208–212. doi:10.5694/j.1326-5377.2006.tb00416.x
38. Young B, Gleeson M, Cripps AW. C-reactive protein: a critical review. Pathology. 1991;23(2):118–124. doi:10.3109/00313029109060809
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.