Back to Journals » Clinical Optometry » Volume 17
Diabetic Eye Screening: Evaluation and Comparison of the Grading Results Between Community and Hospital Eye Services
Authors Stewart C ![]() , Al-duhaimi M, Singh Bhangu J
, Al-duhaimi M, Singh Bhangu J ![]() , John R
, John R ![]() , Williams GS, Awad MH
, Williams GS, Awad MH ![]()
Received 11 April 2025
Accepted for publication 28 October 2025
Published 15 December 2025 Volume 2025:17 Pages 399—407
DOI https://doi.org/10.2147/OPTO.S533954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Christopher Stewart,1 Mokhalad Al-duhaimi,2 Jaskaran Singh Bhangu,1 Rebecca John,3 Gwyn Samuel Williams,2 Mahmoud Husseiny Awad2
1Faculty of Medicine, Health and Life Science, Swansea University, Swansea, UK; 2Department of Ophthalmology, Singleton Hospital, Swansea, UK; 3Primary Care Services, NHS Wales Shared Services Partnership, Cardiff, UK
Correspondence: Rebecca John, Email [email protected]
Background: Diabetes is a significant global health crisis, affecting approximately 828 million individuals worldwide, including 5.6 million in the UK and an estimated 212,000 in Wales. Diabetic Retinopathy (DR) is a leading cause of blindness in the UK and severely impacts the working-age population. Effective screening programs are vital for early detection and intervention, as prolonged diabetes increases the risk of developing DR. Since 2003, Diabetic Eye Screening Wales (DESW) has coordinated DR screening in Wales, but no studies have assessed grading agreement across the screening pathway.
Methods: This retrospective study analysed data from January 2021 to December 2023, involving 762 eyes from 486 patients referred across different grading levels. The RxMx system was used to classify retinopathy and maculopathy. The agreement between primary graders (DESW) and secondary graders (community optometrists) was compared, along with that between secondary and tertiary graders (hospital eye services). Percentage agreement and weighted Cohen’s Kappa were calculated to assess interobserver reliability.
Results: The percentage agreement was 60.4% (weighted Cohen’s Kappa of 0.423, indicating moderate agreement) between primary and secondary graders for retinopathy. For maculopathy, the agreement was 69.6% (weighted Cohen’s Kappa of 0.42). Between secondary and tertiary graders, the percentage agreement for retinopathy was 61.5% (Kappa of 0.634, indicating substantial agreement), while for maculopathy, it was 75.0% (Kappa of 0.618).
Conclusion: The findings show fair agreement between primary and secondary graders and a substantial agreement between secondary and tertiary graders. These results highlight concerns regarding the reliability of current screening practices and suggest incorporating optical coherence tomography (OCT) to enhance grading accuracy. Additionally, implementation of personalised risk-based screening may help reduce the burden of DR on healthcare services, although consideration is necessary to prevent exacerbating existing health inequalities. An electronic system for shared imaging data could further improve screening reliability and grader competency assessment.
Keywords: diabetic retinopathy, diabetic maculopathy, diabetic eye disease, screening, shared care, public health
Introduction
Globally, about 828 million people have diabetes, with approximately 5.6 million affected in the UK, accounting for around 8% of the population.1,2 There is estimated to be 212,000 diabetics who live in Wales.2 The impact of diabetes on the National Health Service (NHS) in the UK is significant, costing around £10 billion per annum.2
Diabetes has many systemic complications, one of which is diabetic retinopathy (DR), which is one of most common causes of blindness in the UK.3 It affects vision through two main forms: active proliferative retinopathy, that leads to new blood vessel growth and potential haemorrhage, and diabetic maculopathy, which disrupts central vision.4 DR poses significant economic costs as it impacts working-age individuals.5 It stems from hyperglycaemia-induced damage to retinal blood vessels, involving pericyte loss and barrier impairment, and is complicated by chronic inflammation and retinal neurodegeneration.4,6
DR affects 30–40% of those with diabetes, for all types of diabetes.3 Early detection and intervention can prevent irreversible damage.7,8 A robust screening program is essential to identify and refer at-risk individuals, aligning with the Wilson and Junger criteria adopted by the WHO and the UK National Screening Committee.9–12 Continuous screening is crucial, as the duration of diabetes is the primary risk factor for developing DR.13
Since 2003, DR screening in Wales has been centralised at Diabetic Eye Screening Wales (DESW), an NHS provision for eligible individuals.14 Clinics are offered throughout Wales, ensuring services for patients are close to home.15 Eligibility includes anyone over 12 years old with a diabetes diagnosis registered with a General Practitioner in Wales.15 Patients are automatically invited for screening upon diagnosis from secondary or primary care.15
To date, there has been no research evaluating grading agreement across the screening pathway for DR in Wales. The primary aim of this study was to identify the agreement between primary graders (DESW) and secondary graders (community optometrists with a specialist qualification in diabetic eye disease). A secondary aim was to compare the agreement between the secondary graders and the tertiary graders (hospital eye services).
Ethics
This study adhered to the tenets outlined in the Declaration of Helsinki. The study was discussed with Swansea Bay University Health Board Research and Development department. It was deemed that no further ethical approval was required, and patients were not required to provide informed consent as the data was collected during normal service delivery. Data accessed complied with relevant data protection and privacy regulations.
Methods
Study Design and Subjects
This retrospective study assessed data collected between January 2021 and December 2023, identifying a total of 762 eyes from 486 patients. The data was obtained from referrals sent from the primary graders. In Swansea Bay Health board, all referrals are received by tertiary graders who then determine based on the grade whether they are to be seen by secondary or tertiary graders. The data obtained adhered to the RxMx grade (Table 1) which was used by all three groups: primary graders, secondary graders, and tertiary graders.16 It should be noted that maculopathy was further subdivided into active and stable maculopathy by the secondary and tertiary graders due to the ability to perform fundoscopy and acquire OCT (Optical Coherence Tomography) which are investigations not available to the primary graders. Given this, maculopathy between primary and secondary graders was only based on absence or presence of macular disease.
 |
Table 1 The RxMx Grading System Used in England, Wales, and Northern Ireland Which is a Feature-Based Grading System |
The standard procedure for patients after grading in Wales follows a three-tier system based on severity (see supplementary material 1). Primary graders from DESW initially screen all patients. Those classified as R0M0/R1M0 are re-invited biannually, due to their low risk of progression over a two-year period. Patients showing R2M0, R0M1, R1M1, or ungradable images are seen by secondary graders—qualified community optometrists, who perform further imaging and examinations. Ungradable images typically prompt a second attempt before being referred onwards. Patients classified as R3M0/R3M1 are seen directly by tertiary services for treatment and monitoring. The screening pathway is illustrated in Supplementary Material 1.
Inclusion and Exclusion Criteria
Retinal images that were excluded from this study were those deemed ungradable by DESW due to either poor picture quality, lack of a complete fundal image or abnormalities that lie outside the remit of the graders. This was because there would be no grading in place from the primary graders and thus an inability to look for interobserver agreement. Referrals received from primary and secondary graders, alongside clinic letters from tertiary graders that did not contain a complete grading score in line with the RxMx system were removed as to ensure completeness.
Training
The primary graders were non-clinical trained technicians specialising in assessing retinal images. They completed in-house training developed by a lead ophthalmologist and are required to evaluate a specific number of retinal images under supervision prior to independently grading retinal images. According to DESW guidance, any abnormalities outside of the RxMx grading system are referred to directly to Hospital Eye Services (HES).
The secondary graders were community optometrists listed with the General Optical Council who hold the College of Optometrists Professional Certificate in medical retina.17
The tertiary graders were the hospital eye service, this was composed primarily of ophthalmologists and qualified allied health professionals under direct consultant ophthalmologist supervision.
Clinical Assessment
Table 2 outlines the range of retinal imaging and clinical examinations performed by primary, secondary, and tertiary graders. Retinal imaging in the form of a two-field photograph were taken at each point of contact. The DESW cameras capture two 45-degree retinal images for each eye: one centred on the macula and the other focused on the nasal field, using a non-mydriatic Canon DGi camera equipped with either a 30D or 40D camera back. Secondary graders use various imaging machines based on the equipment available at the community optometrist’s practice.
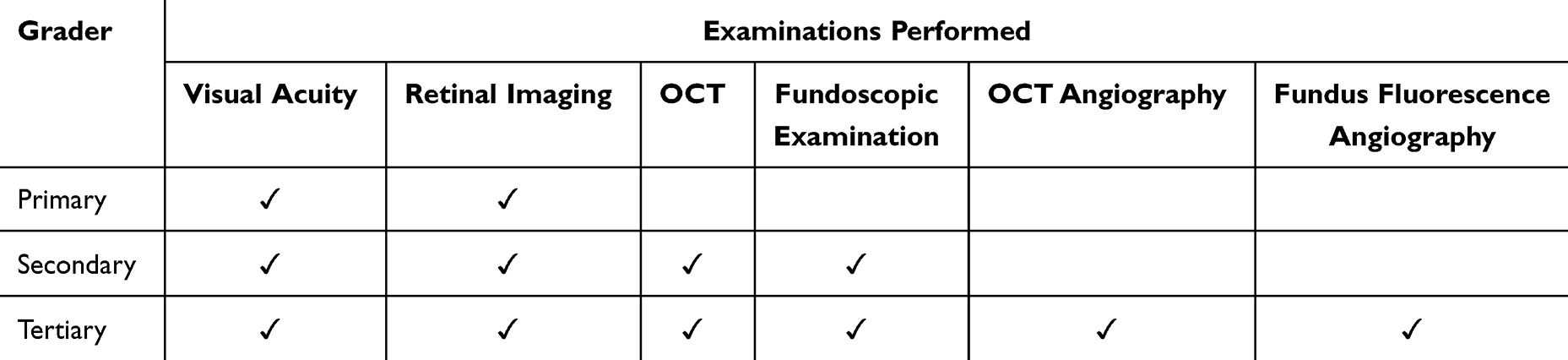 |
Table 2 Clinical Examinations Performed by Primary, Secondary, and Tertiary Graders |
There is currently no centralised database in Wales allowing images taken by one group to be seen by the others. The imaging modality for DESW consisted solely of retinal photographs, while secondary and tertiary graders also utilised OCT and fundoscopic examination (Table 2). The tertiary graders had the greatest range of imaging modalities including OCT-angiography, fundus fluorescence angiography (FFA), and ultra-wide field imaging in the form of Optos.18
Patients under DESW routine follow-up would adhere to the strict criteria of being seen biannually unless they met criteria meaning they were referred to the secondary or tertiary graders. Those under of the secondary and tertiary graders would be seen according to clinical need as determined by the clinician’s judgement.
Measures
Statistical Analysis
The percentage agreement was calculated by comparing the number of times both groups assign the same Rx value to an eye, divided by the total number of cases assessed by the first group. For example, between primary and secondary graders for R0, as illustrated below.

Weighted Cohen’s Kappa was performed to measure the reliability of the agreement between the secondary graders using SPSS Version 14. The weighted Cohen’s Kappa test looks at the interobserver reliability using a scale of 0 to 1.19–21 At its extremes, the scale implies that a value of 0 is when there is no agreement, whilst between 0.81 and 1 there is almost perfect agreement. In between this range there is 0.01 to 0.2 as none to slight, 0.21–0.4 as fair, 0.41–0.6 as moderate, and 0.61 to 0.8 as substantial. The use of weighted Cohen’s Kappa was chosen as it is more sensitive to the degree of disagreement, providing a more accurate reflection of agreement in ranked categories.22,23
Percentage agreement and weighted Cohen’s Kappa is reported for retinopathy (R1, R2, R3) and maculopathy (M0, M1) between primary and secondary graders, and secondary and tertiary graders.
Public and Patient Involvement
The study’s design incorporated input from patients and the public through collaboration with the Royal College of Ophthalmologists in Wales, as well as consultations with national organisations and local Eye Clinic Liaison Officers. Upon publication, the study’s findings will be disseminated to members of the Wales Vision Forum and Wales Council for the Blind.
Results
In accordance with the inclusion and exclusion criteria, a total of 1,030 eyes were analysed between primary and secondary graders (n=268 excluded) and 134 eyes were analysed between secondary and tertiary graders (n=38 excluded).
Agreement Between Primary and Secondary Graders Retinopathy
Percentage agreement between the retinopathy grading of the primary and secondary graders was 87.9%, 58.5%, and 45.6% for R0, R1, and R2, respectively. The R3 were not compared as patients were seen directly by tertiary graders and so no interobserver agreement would be seen. These agreement levels are illustrated in Table 3 and results in an overall percentage agreement of 60.4% (460/762). The weighted Cohen’s Kappa was 0.423 (Standard error [SE] 0.029) indicating moderate agreement.
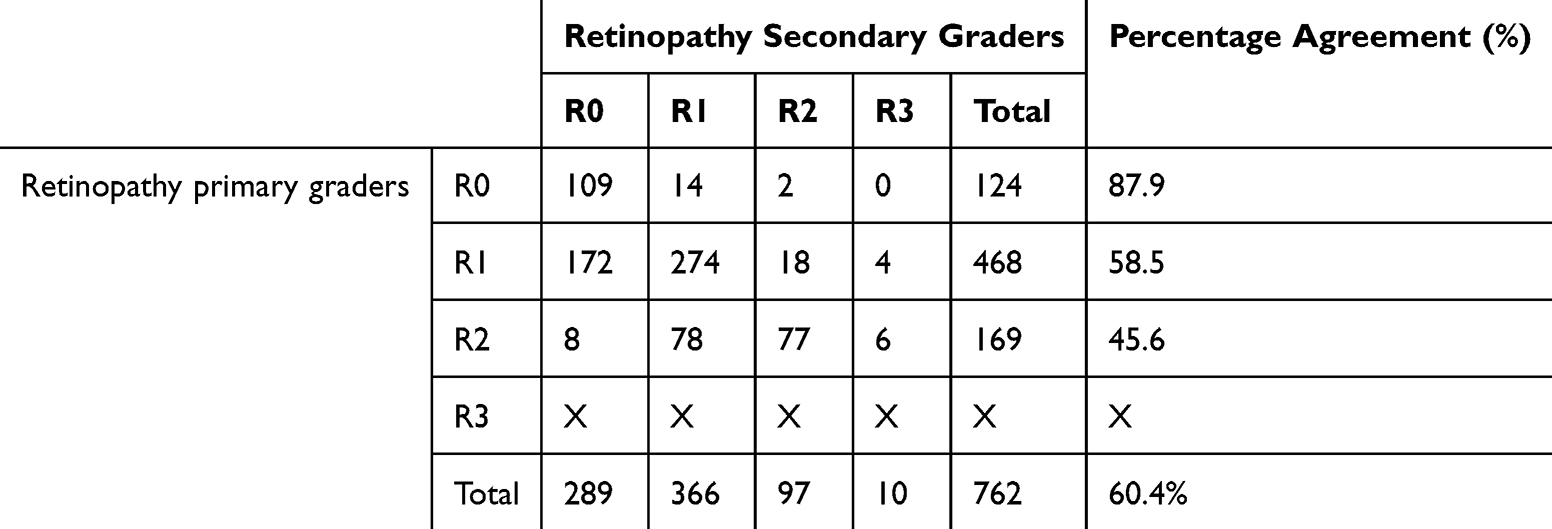 |
Table 3 Grading Scores for Retinopathy Given by the Primary (DESW) and Secondary Graders (Community Optometrists) Illustrating Percentage Agreement for R0, R1, R2, R3, and Overall |
Agreement Between Primary and Secondary Graders Maculopathy
Percentage agreement between primary and secondary graders was 71.7% (294/410) and 67.0% (236/352) for M0 and M1, respectively (Table 4), resulting in an overall percentage agreement of 69.6%. The weighted Cohens Kappa was 0.42 (SE, 0.017), demonstrating moderate agreement.
 |
Table 4 Grading Scores for Maculopathy Given by the Primary (DESW) and Secondary (Community Optometrists) Graders Illustrating Percentage Agreement for M0, M1, and Overall |
Agreement Between Secondary and Tertiary Graders Retinopathy
Percentage agreement between the retinopathy grading of the secondary and tertiary graders was 55.0% (11/20), 75.0% (21/28), 48.3% (14/29), and 68.4% (13/19) for R0, R1, R2, and R3, respectively. This is illustrated in Table 5 and results in an overall percentage agreement of 61.50% (59/96). The weighted Cohen’s Kappa was 0.634 (SE, 0.068) and tertiary graders illustrating percentage agreement for R0, R1, R2, R3, and overall.
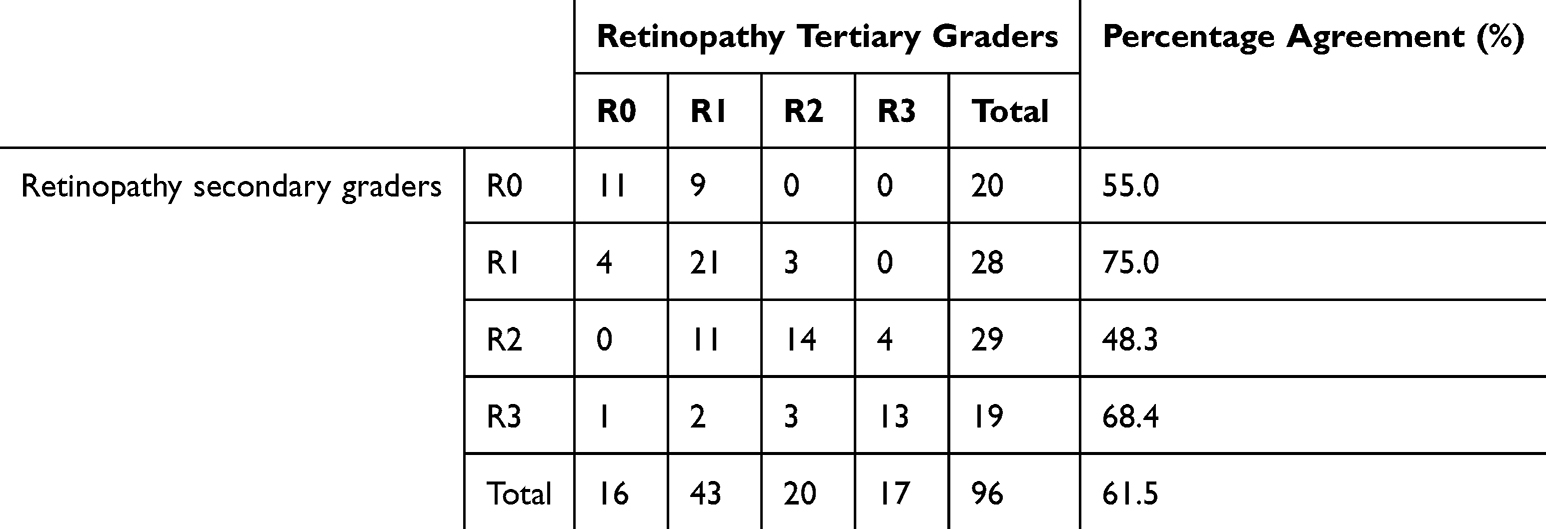 |
Table 5 Grading Scores for Retinopathy Given by the Secondary (Community Optometrists) Graders Illustrating Percentage Agreement for R0, R1, R2, R3, and Overall |
Agreement Between Secondary and Tertiary Graders Maculopathy
Percentage agreement between secondary and tertiary graders was 89.7% (26/37), 65.9% (29/44), and 68.0% (17/25) for M0, M1a, and M1s, respectively (Table 5). Overall percentage agreement was 75.0%, as shown in Table 6. The weighted Cohen’s Kappa of 0.618 (SE, 0.062) indicating substantial agreement.
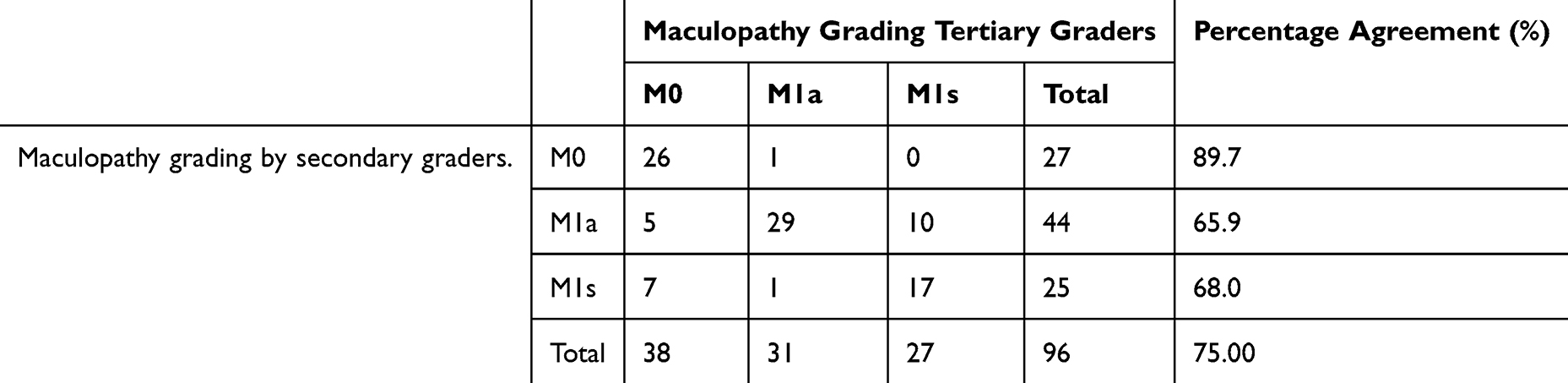 |
Table 6 Grading Scores for Maculopathy Given by the Primary and Secondary Graders Illustrating Percentage Agreement for M0, M1a, M1s, and Overall |
The weighted Cohen’s Kappa values are shown in Figure 1, for each interobserver agreement analysed with the benchmark highlighted.
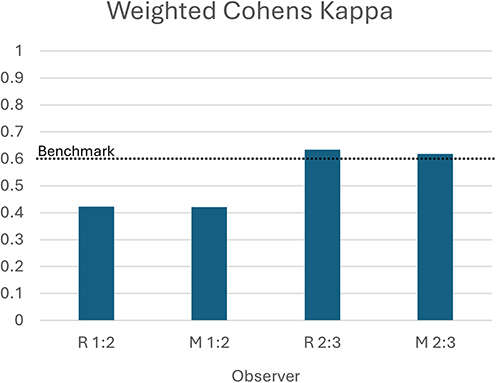 |
Figure 1 Weighted Cohen’s Kappa value for interobserver agreement for retinopathy (R) and maculopathy (M) by primary (1) and secondary (2) graders followed by agreement between secondary (2) and tertiary (3) graders. |
Discussion
Our results show a fair and substantial level of agreement according to weighted Cohen’s Kappa between primary/secondary and secondary/tertiary graders, respectively, for retinopathy grading. Evidence suggests that an agreement below 60% is inadequate for clinical reliability, while agreement of approximately 80% is generally accepted as the gold standard.20,21
Agreement between the primary and secondary graders was greatest for the lower grades of DR (R0 and M0), with agreement decreasing as the retinopathy grade increased. The results indicate that primary graders tend to over-grade, which is seen in previous literature.24–26This could be explained by the limited information available from fundus images alone as well as the role-specific nature of the primary grader, with over-grading being considered safer than under-grading. Furthermore, the 2013 Four Nations Diabetic Retinopathy Screening Intervals Project Study Group27 noted variations in grading practices across UK programs, affecting patient assessments and treatment for diabetic retinopathy. To address this, steps should be taken to enhance quality assurance and transparency in the screening program, with clear targets for internal and external reviews.
Despite the higher percentage of agreement in the maculopathy group, concerningly there were 116 out of the 410 patients graded by primary graders as M0 which were graded by the secondary graders as M1. Resemblances can be seen in a previous study,28 that highlighted the lack of OCT as fundamental to operating with retinal images alone as a screening tool for DM. The presence of DM increases the risk of sight loss between 30% and 50% after two years and thus it is imperative to have an effective screening tool.29 In comparison to DR, the higher agreement levels may be due to the high prevalence of M0 grades which could inflate the overall agreement as well as the simplified categorisation of DM as either present or absent.
Introducing optical coherence tomography (OCT) alongside fundal imaging could help address discrepancies in DR screening in Wales, potentially increasing grader agreement as currently, OCT is not part of the DESW programme. Recent research suggests that introducing OCT could streamline the screening process by reducing false positives and improving cost-effectiveness.30 This is supported by our results of increased agreement between secondary and tertiary graders where both OCT and fundoscopy was utilised.
With a projected increase in the number of people living with diabetes in Wales to 260,000 by 2035/2036 will come with an increase on burden of eyecare services.2,31 Recent studies32–34 suggest that personalised risk-based screening could be more effective than annual reviews. This challenges the current one-size-fits-all screening model, as over-grading may lead to unnecessary referrals, while under-grading increases the risk of delayed treatment, especially with capacity constraints in hospital. Changes to the service like the introduction of the extended screening interval in 2023, which allows low-risk patients to be screened biennially aims to reduce service demand.12,15 However, a blanket approach for the low-risk patients may lead to disparities among ethnic and higher-risk groups, as studies have shown that biennial reviews may not be adequate for all populations.35,36 For example, younger patients may present later to services and are more likely to fail to attend, compounding the issue by presenting with more advanced disease and having poorer outcomes.9
Strengths and Limitations
The key strength of this study is the use of real-world data without the typical synthetic environment created by studies that remove the human factors and environmental influences that can contribute to outcomes. However, in Wales, the lack of a centralised electronic patient records meant that retinas were assessed at different times using different modalities which may impact upon agreement. It is possible that some extent of the lower agreement could be attributed to the disease progression between grading sessions for both datasets. The average time between assessment by primary and secondary graders was 26 weeks. In contrast, the time between secondary and tertiary graders was 8 weeks.
Conclusion
Further analysis is required to ascertain whether these findings highlight deficiencies in current screening practices, reflect an impact of certain patient characteristics (eg severity of DR, image quality, presence of media opacity) on grading discrepancies or, are indicative of broader systemic factors. Implementing personalised risk-based screening could potentially mitigate the increasing burden of DR on healthcare services; however, it is crucial to approach this with caution to prevent the exacerbation of existing health inequalities. Additionally, the introduction of an electronic system that allows all graders to access the same images may facilitate enhanced monitoring of program reliability and the assessment of competency among graders at different levels.
Acknowledgments
The authors would like to thank Flora Lawton (Swansea medical student), Gowry Ganenthira (Swansea medical student), and Mohammed Rifat (foundation doctor) for their assistance in data collection.
Funding
Roche Products Ltd. supported with funding for the article submission charges by a hands-off grant. Roche Products Ltd. did not have any involvement in the preparation, drafting or editing of this paper or in the choice of authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou B, Rayner AW, Gregg EW, et al. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404(10467):2077–2093. doi:10.1016/S0140-6736(24)02317-1
2. Wales PRPH. 2023. Diabetes prevalence – trends, risk factors, and 10-year projection. Available from: https://phw.nhs.wales/services-and-teams/observatory/data-and-analysis/diabetes-prevalence-trends-risk-factors-and-10-year-projection/.
3. Lawrenson JG, Bourmpaki E, Bunce C, et al. Trends in diabetic retinopathy screening attendance and associations with vision impairment attributable to diabetes in a large nationwide cohort. Diabetic Med. 2021;38(4):e14425. doi:10.1111/dme.14425
4. Wang W, Lo ACY. Diabetic retinopathy: pathophysiology and treatments. Int J Mol Sci. 2018;19(6).
5. Kropp M, Golubnitschaja O, Mazurakova A, et al. Diabetic retinopathy as the leading cause of blindness and early predictor of cascading complications—risks and mitigation. EPMA Journal. 2023;14(1):21–42. doi:10.1007/s13167-023-00314-8
6. Cai J, Boulton M. The pathogenesis of diabetic retinopathy: old concepts and new questions. Eye. 2002;16(3):242–260. doi:10.1038/sj.eye.6700133
7. Scanlon Peter H. The contribution of the English NHS diabetic eye screening programme to reductions in diabetes-related blindness, comparisons within Europe, and future challenges. Acta Diabetol. 2021;58(4):521–530. doi:10.1007/s00592-021-01687-w
8. Kollias AN, Ulbig MW. Diabetic retinopathy: early diagnosis and effective treatment. Dtsch Arztebl Int. 2010;107(5):75–83. doi:10.3238/arztebl.2010.0075
9. Scanlon PH, Stratton IM, Leese GP, et al. Screening attendance, age group and diabetic retinopathy level at first screen. Diabetic Med. 2016;33(7):904–911. doi:10.1111/dme.12957
10. Dobrow MJ, Hagens V, Chafe R, Sullivan T, Rabeneck L. Consolidated principles for screening based on a systematic review and consensus process. Can Med Assoc J. 2018;190(14):E422. doi:10.1503/cmaj.171154
11. Europe WHOrganizationRO for. Screening programmes: a short guide. Increase effectiveness, maximize benefits and minimize harm. Copenhagen: World Health Organization. Regional Office for Europe; 2020. Available from: https://iris.who.int/handle/10665/330829.
12. UK National Screening Committee. Department of Health and Social Care. 2024. UK National Screening Committee: screening in healthcare. Available from: https://www.gov.uk/guidance/principles-of-population-screening/principles-of-screening.
13. Wong TY, Mwamburi M, Klein R, et al. Rates of progression in diabetic retinopathy during different time periods: a systematic review and meta-analysis. Diabetes Care. 2009;32(12):2307–2313. doi:10.2337/dc09-0615
14. Public Health Wales, Diabetic Eye Screening Wales. Diabetic eye screening wales annual statistical report 2019-20. Cardiff. 2021.
15. Public Health Wales. Cardiff. 2020. Diabetic eye screening wales: about diabetic eye screening. Available from: https://phw.nhs.wales/services-and-teams/screening/diabetic-eye-screening-wales/about-diabetic-eye-screening/.
16. NHS England. NHS diabetic eye screening programme: grading definitions for referable disease. Available from: https://www.gov.uk/government/publications/diabetic-eye-screening-retinal-image-grading-criteria/nhs-diabetic-eye-screening-programme-grading-definitions-for-referable-disease-start-date-october-01.
17. The College of Optometrists [UK]. Higher qualifications. 2024 Available from: https://www.college-optometrists.org/professional-development/further-qualifications/higher-qualifications.
18. Byberg S, Vistisen D, Diaz L, et al. Optos wide-field imaging versus conventional camera imaging in Danish patients with type 2 diabetes. Acta Ophthalmol. 2019;97(8):815–820. doi:10.1111/aos.14118
19. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther. 2005;85(3):257–268. doi:10.1093/ptj/85.3.257
20. McHugh M. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(1):276–282. doi:10.1016/j.jocd.2012.03.005
21. Fleiss JL, Levin B, Paik MC. statistical methods for rates and proportions. In: Fourth. Hoboken: John Wiley & Sons, Inc; 2003:598–622.
22. Viera A, Garrett J. Understanding Interobserver agreement: the kappa statistic. Fam Med. 2005;37:360–363.
23. Cohen J. Weighted kappa: nominal scale agreement provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4). doi:10.1037/h0026256
24. Oke JL, Stratton IM, Aldington SJ, Stevens RJ, Scanlon PH. The use of statistical methodology to determine the accuracy of grading within a diabetic retinopathy screening programme. Diabetic Med. 2016;33(7):896–903. doi:10.1111/dme.13053
25. Patra S, Gomm EMW, Macipe M, Bailey C. Interobserver agreement between primary graders and an expert grader in the Bristol and Weston diabetic retinopathy screening programme: a quality assurance audit. Diabetic Med. 2009;26(8):820–823. doi:10.1111/j.1464-5491.2009.02767.x
26. Sellahewa L, Simpson C, Maharajan P, Duffy J, Idris I. Grader agreement, and sensitivity and specificity of digital photography in a community optometry-based diabetic eye screening program. Clin Ophthalmol. 2014;8(1):1345–1349. doi:10.2147/OPTH.S61483
27. UK National Screening Comittee. Four Nations Diabetic Retinopathy Screening Intervals Project Study Group. 2013.
28. Kousha O, Fave MMD, Cozzi M, Carini E, Pagliarini S. Diabetic maculopathy: multicolour and SD-OCT versus fundus photography. BMJ Open Ophthalmol. 2021;6(1):e000514. doi:10.1136/bmjophth-2020-000514
29. Virgili G, Menchini F, Casazza G, et al. Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy. Cochrane Database Syst Rev.
30. Leal J, Luengo-Fernandez R, Stratton IM, Dale A, Ivanova K, Scanlon PH. Cost-effectiveness of digital surveillance clinics with optical coherence tomography versus hospital eye service follow-up for patients with screen-positive maculopathy. Eye. 2019;33(4):640–647. doi:10.1038/s41433-018-0297-7
31. Thomas RL, John R, Bunce C, et al. Trends in certifications of overall vision impairment and that due to diabetic retinopathy/maculopathy in England and Wales, 2009/2010 to 2019/2020: a retrospective database analysis. BMJ Open. 2025;15(1):e090597. doi:10.1136/bmjopen-2024-090597
32. Lund SH, Aspelund T, Kirby P, et al. Individualised risk assessment for diabetic retinopathy and optimisation of screening intervals: a scientific approach to reducing healthcare costs. Br J Ophthalmol. 2016;100(5):683. doi:10.1136/bjophthalmol-2015-307341
33. Broadbent DM, Wang A, Cheyne CP, et al. Safety and cost-effectiveness of individualised screening for diabetic retinopathy: the ISDR open-label, equivalence RCT. Diabetologia. 2021;64(1):56–69. doi:10.1007/s00125-020-05313-2
34. Dai L, Sheng B, Chen T, et al. A deep learning system for predicting time to progression of diabetic retinopathy. Nat Med. 2024;30(2):584–594. doi:10.1038/s41591-023-02702-z
35. Olvera-Barrios A, Rudnicka AR, John A, et al. Two-year recall for people with no diabetic retinopathy: a multi-ethnic population-based retrospective cohort study using real-world data to quantify the effect. Br J Ophthalmol. 2023;107(12):1839–1845. doi:10.1136/bjo-2023-324097
36. Kliner M, Fell G, Gibbons C, Dhothar M, Mookhtiar M, Cassels-Brown A. Diabetic retinopathy equity profile in a multi-ethnic, deprived population in Northern England. Eye. 2012;26(5):671–677. doi:10.1038/eye.2012.3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Towards a Device Agnostic AI for Diabetic Retinopathy Screening: An External Validation Study
Rao DP, Sindal MD, Sengupta S, Baskaran P, Venkatesh R, Sivaraman A, Savoy FM
Clinical Ophthalmology 2022, 16:2659-2667
Published Date: 17 August 2022
Psychometric Impact of Diabetic Retinopathy-Induced Visual Impairment: A Hospital-Based Study, Al Buraimi, Sultanate of Oman
Vankudre GS, Mohamed ZD, Ayyappan JP, Alrasheed SH
Clinical Optometry 2025, 17:3-10
Published Date: 13 January 2025
Comparison of the Aireen System with Telemedicine Evaluation by an Ophthalmologist – A Real-World Study
Šín M, Ženíšková R, Slíva M, Dvořák K, Vaľková J, Bayer J, Karasová B, Tesař J, Fillová D, Prázný M
Clinical Ophthalmology 2025, 19:957-964
Published Date: 19 March 2025
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025