Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Diabetes Related Knowledge, Attitudes and Practice – A Survey Among Oral Health Professionals in Victoria, Australia
Authors Chinnasamy A ![]() , Moodie M
, Moodie M ![]()
Received 27 November 2019
Accepted for publication 29 January 2020
Published 3 April 2020 Volume 2020:12 Pages 111—121
DOI https://doi.org/10.2147/CCIDE.S240212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Alagesan Chinnasamy,1 Marjory Moodie2
1Melbourne Dental School, The University of Melbourne, Melbourne, VIC, Australia; 2Deakin Health Economics, Deakin University, Geelong, VIC, Australia
Correspondence: Alagesan Chinnasamy
Melbourne Dental School, 720 Swanston Street, Carlton, Melbourne, VIC 3053, Australia
Tel + 61 426931940
Email [email protected]
Purpose: Until now, little is known as to how well the evidence supporting the link between periodontal disease and diabetes is incorporated in the dental practice, in Australia. This study aims to explore Oral health Professionals (OHP) knowledge, attitudes, and practice (KAP) towards diabetes screening in the dental setting.
Methods: The survey questionnaire consisted of sociodemographic, practice characteristics and Likert scaled questions categorised in different domains of KAP and one additional domain as barriers. A Mann–Whitney and Kruskal–Wallis test was performed to determine differences in the OHP response. To predict if practice behavior was influenced by knowledge and attitudes, a multiple linear regression was conducted.
Results: A total of 197 respondents were included in the analysis of the results. General dentists constituted 64.6% of the response. For chairside screening of diabetes, 58% felt it was essential and 70% felt it was appropriate. More public sector OHP (79%) felt it is important to conduct chairside screening for T2DM. Patient willingness was identified as the most important and insurance coverage as the least important (43%) consideration for T2DM screening.
Conclusion: Overall, knowledge, attitude and practice towards DM were positive, but a significant proportion of the OHP felt chairside screening may not be appropriate or important.
Keywords: diabetes, oral health professional, screening, periodontal disease
Introduction
Diabetes Mellitus (DM) is the fastest growing chronic condition in Australia. Its prevalence is higher than in nearly all Western European nations.1 It is estimated that 1.7 million people are known to have DM and three million will develop DM by the year 2025.2,3 Approximately 30% of Australians with type 2 DM (T2DM) are undiagnosed and unaware of their DM status.4
DM affects nearly every organ in the body, causing disability and life-threatening health problems. This can lead to a substantial economic loss to the individual, families and the national health-care system. In the Western Pacific region, Australia has the highest per-person spending on DM5 with an annual direct cost of AUD 4390.6 One-third of preventable hospital admissions were directly or indirectly linked to DM, and the economic cost is estimated to be at A$ 14.6 billion in the year 2010.6
The starting point for living well with T2DM is an early diagnosis. Early identification of at-risk individuals can delay or prevent the onset of T2DM with minimal microvascular complications.7–9 The Ely cohort study identified that screening could bring forward the diagnosis of T2DM on average by 3.3 years.10 However, the challenges with early diagnosis are that many individuals with pre-DM and some with undiagnosed DM are asymptomatic, leading to late presentation to the health-care provider.
DM is an established risk factor for periodontal disease, and periodontal disease is one of the leading causes of tooth loss among adults. Dental patients with poorly controlled DM experience far greater periodontal problems and poorer treatment outcomes compared to those who keep their blood glucose within normal limits.11,12 With this close link between DM and periodontal disease, the dental practice offers a good setting for the opportunistic screening of patients’ medical problems as Oral Health Professionals (OHPs) are extremely likely to encounter asymptomatic patients with undiagnosed DM and pre-DM.13–15
A survey among the United States’ (U.S) dentists identified that an overwhelming majority (68−85%) were willing to undertake chairside screening of a medical condition. However, only 56% of the respondents were comfortable drawing blood with a finger stick for blood glucose measurement.16 Some of the important barriers identified in screening for medical conditions in the dental setting include lack of training, knowledge, fear of being judgemental or fear of offending the patient.17–20 Furthermore, Barasch and colleagues in 2009 identified that many dental practitioners regarded blood glucose investigation as outside their scope of practice, and only a few dental offices owned and use a glucometer.21
In Australia, little is known about the OHP knowledge, attitudes and practice (KAP) around identification of patients with diagnosed and undiagnosed DM. To explore OHPs’ knowledge on DM, referral, and pathway of care, an understanding of risk factors for DM, opinions about and perceived barriers to screening is important. As such, the aim of this study is to determine Victorian OHPs’ 1. knowledge and opinions on DM and periodontal disease. 2. attitudes and practice behaviours towards T2DM screening in the dental setting.
Materials & Methods
This is a cross-sectional survey of Victorian OHPs. The study was supported by the eviDent Foundation and the Victorian Research Network (VicReN) two key practice-based research networks in the dental and the primary care disciplines, respectively. Ethical approval was obtained from the Human Ethics Advisory Group of the Melbourne Dental School (Ethics ID: 1647537).
A KAP questionnaire was drafted from previous studies in the literature.16,22-24 Further, it was pilot tested with a convenience representative sample of 40 postgraduate dental students, teaching staff and those who attended a workshop at the Melbourne Dental School to check reliability, clarity, and user-friendliness, before rolling out to dental practitioners more widely. The response from the pilot survey was used to determine the Cronbach’s alpha or internal construct of the scale in measuring the underlying dimension of the knowledge (0.56; 0.81 and 0.81), attitude (0.87) and practice (0.76;0.88;0.86) domain scales.
The final e-questionnaire consisted of 53 items. Sociodemographic and practice characteristics included gender, practice location (regional, rural, suburban and inner-city), dental practice sector (private, public or others), type of OHP (specialist dentist, general dentist, dental hygienist, dental therapist and oral health therapist), place of primary dental qualification (Australia or overseas) and years in practice. The remainder of the questions were Likert scales, categorized into KAP domain and one additional domain as “barriers” for incorporating T2DM screening in the dental setting. The five-point Likert scales consisted of different ratings where 1 = “least important” to 5 = “most important” or “strongly disagree/never” to “strongly agree/always.” In the four-point Likert scale, the choices were 1 = negligible, 2 = low, 3 = moderate and 4 = significant.16,22-24
Population and Sample Size
As of March 2017, there were 5113 registered OHPs in Victoria, which represents 23% of all the OHPs in Australia and includes 3921 (76.6%) dentists, 346 (6.7%) oral health therapists, 218 (4.2%) dental hygienists, and 148 (2.8%) dental therapists. Excluding dental prosthetists, there were 4633 OHPs in Victoria.25
The sample size for the multiple regression analysis with two predictor variables and Mann–Whitney test was conducted using GPower with the alpha set at 0.05 and power at 0.80. The moderate effect size (f2= 0.15) was used for the regression analysis.26 A medium effect size (d = 0.05) and two tails for the Mann–Whitney U-test.26 Based on these assumptions the minimum number of participants required for the analysis was determined to be 68 and 134.
A request was submitted to the Australian Dental Association-Victoria Branch (ADAVB) and Australian Dental and Oral Health Therapists Association (ADOHTA) to assist with the distribution of the survey to all the currently registered OHPs in Victoria. The professional association represents approximately 70–80% of the OHPs in Victoria. The final survey was conducted online using SurveyMonkey platform, www.surveymonkey.com (SurveyMonkey Inc, San Mateo, California, USA). The SurveyMonkey web link was sent by email to 2722 registered dentists and 176 registered dental hygienists, oral health therapists and dental therapists. In addition, the study was advertised in the ADAVB, and eviDent Foundation e-News, website and social media to maximise participation. SurveyMonkey allowed invitations to be sent and responses to be obtained securely. Data were collected from May 2017 to the end of February 2018. A written informed consent was obtained and all the participants were informed that the results of the study were to be published. No monetary benefits or gifts as incentives were offered.
Statistical Analysis
Descriptive statistics with frequencies and percentages were used to summarize sociodemographic and dependent variables. All the five and four-point Likert scales were transformed into a three-point Likert scale. This was done to maintain uniform scores across all the KAP variables for the purpose of analysis. For the sociodemographic independent variable with two categories, a Mann–Whitney U-test was used and a Kruskal–Wallis test for variables with more than two groups to determine if there were differences in response to the KAP and barriers dependent variables.
The transformed three-point Likert response for individual questions was averaged to give a single knowledge score, an attitude score and a practice behaviour score for each participant using the compute variable function in SPSS to form a scale variable. To predict if practice was influenced by knowledge and attitudes, a multiple linear regression was conducted. All the analyses were performed using Statistical Package for the Social Sciences software (SPSS for Windows, Version 24, Chicago, IL).
Results
One hundred and seventy-five OHPs responded to the e-survey. With the inclusion of the pilot data, the number of responses was 215. Respondents who did not complete any answer (n = 6) were excluded from the analysis. Listwise deletion was used to eliminate a further 12 participants with large amounts of missing data. A total of 197 OHPs were included in the final analysis of the results.
Sociodemographic characteristics of the respondents are presented in Table 1. Females constituted 60.7% of the respondents (n = 119). The majority of the OHPs were private practitioners, and little over half (n = 102) of the responding OHPs were from a suburban setting, with the least from a rural location (6.5%). Inner-city or regional practice accounted for approximately 20% of the responses. The most frequently observed category of OHPs was general dentists (65%), while specialist dentists constituted approximately 10% of the respondents. More than 95% of the specialist dentists were from the suburban and inner-city location. The average years in dental practice were 18.90 ± 13.86 (range, 1−51) with approximately 40% having had less than 10 years of work experience. Almost everyone with 10 years or less (93%) or 40 years or more (100%) of work experience had obtained their primary dental qualification in Australia.
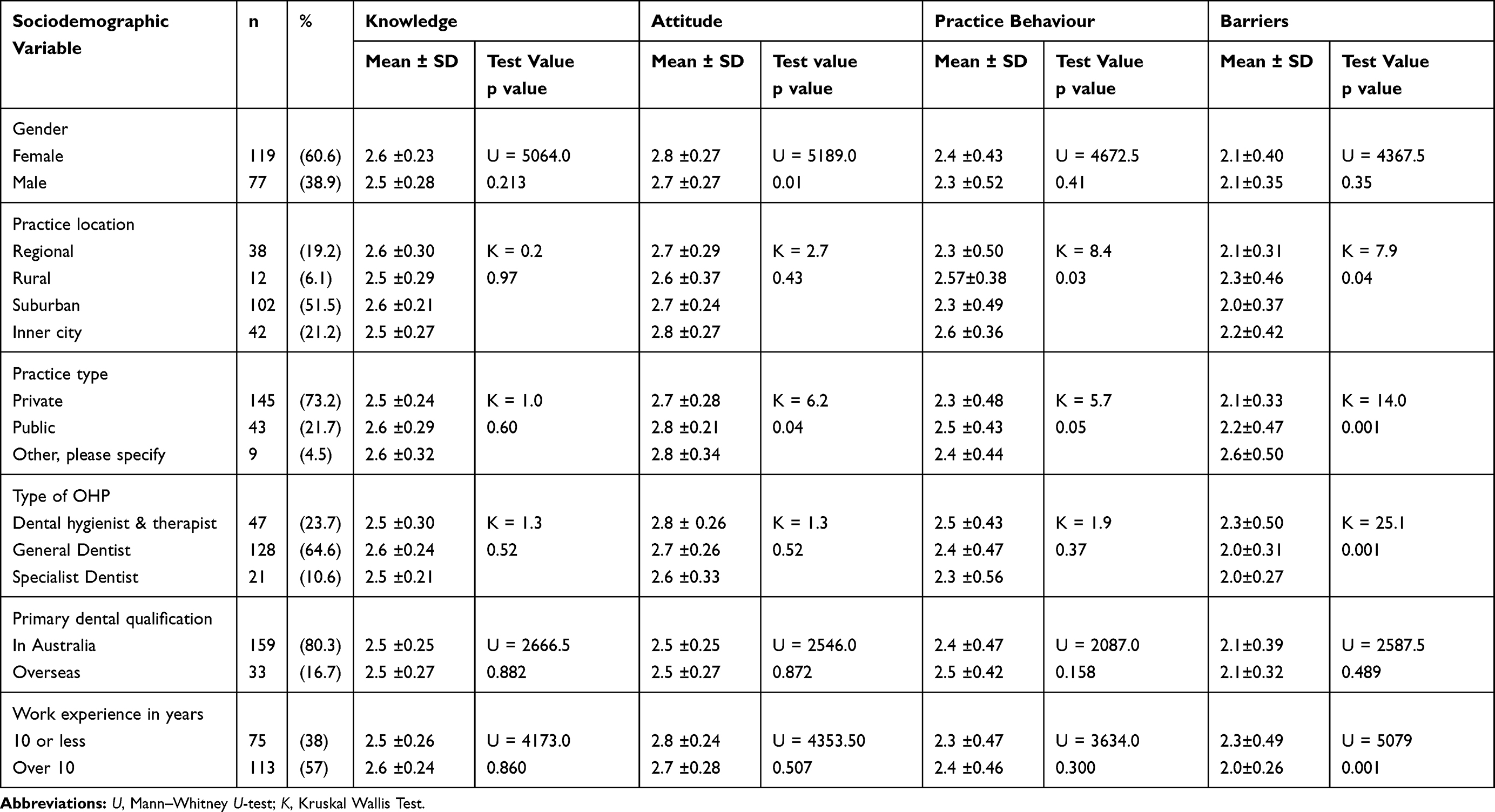 |
Table 1 Group Difference of Independent Variable to KAP Variables |
DM Related Knowledge Scores
Tables 1 and 2 present the results of the DM related knowledge scores There was no significant difference in the overall knowledge score with any of the categories within the sociodemographic variables. Few OHPs indicated that osteoporosis (n=23; 12%) and stroke (n =78; 39.6%) were a significant complication of DM compared to other questions in that scale. The lowest number of respondents (n = 110; 55.8%) among those who agreed/strongly agreed to the knowledge question was DM as a risk factor for “high blood pressure”. Compared to their Australian peers, overseas-qualified dentists in Australia were 20% less likely to agree that the Aboriginal and Torres Straits Islanders were at increased risk of DM. Among the knowledge variables, the question where more number of OHPs neither agreed nor disagreed was “Patients reporting a glycated haemoglobin level (HbA1c) of less than 5.7% is indicative of good glycaemic control” (n = 71; 36%). The mean knowledge score was 2.5 (SD = 0.25) with a range of 1.6 to 3.
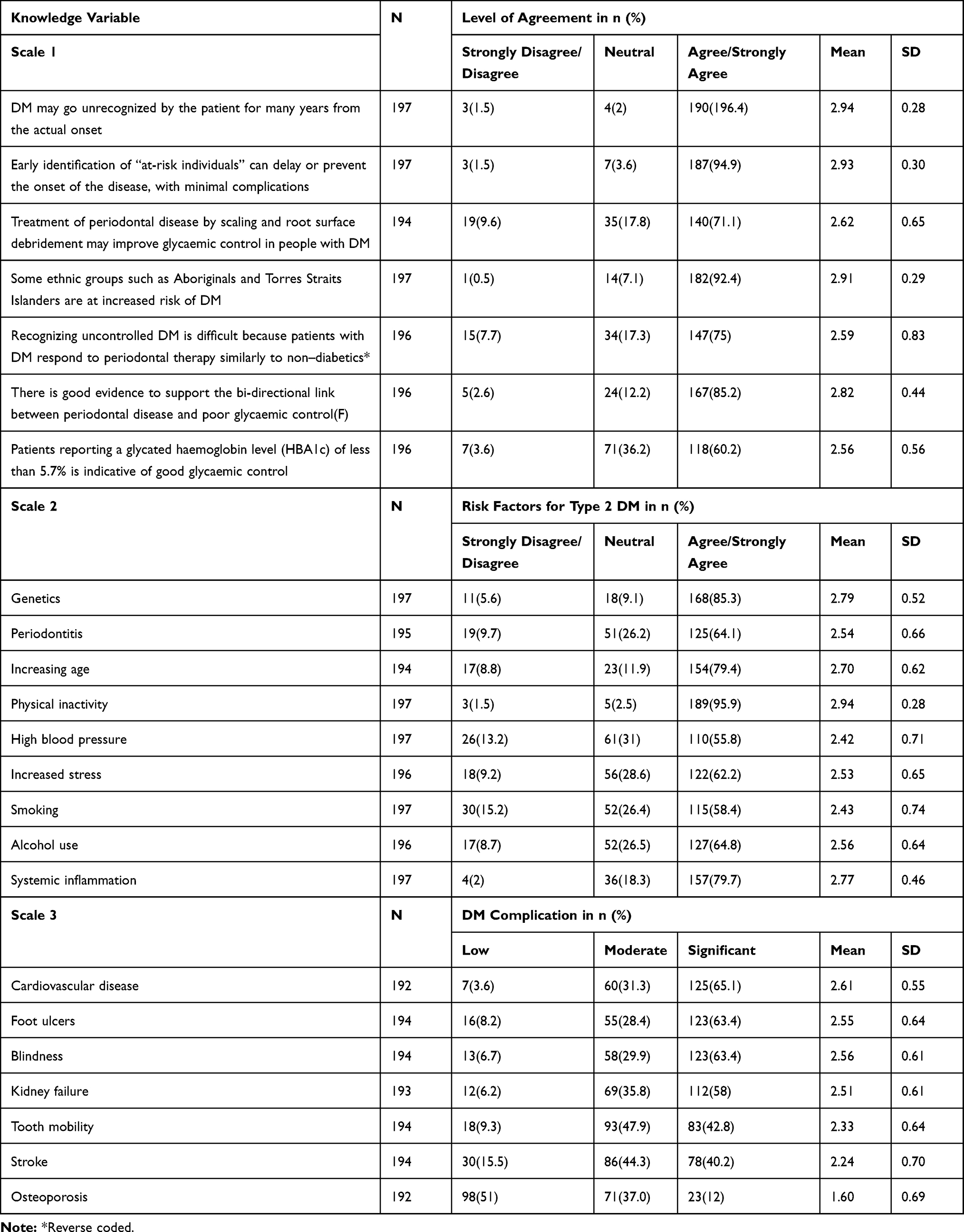 |
Table 2 OHP Response to Knowledge Variables |
DM Related Attitude Scores
Tables 1 and 3 present the DM related attitude scores. The mean attitude score was 2.78 (SD = 0.26) with a range of 1.7 to 3. Around 90% of the OHPs felt patient’s overall health is essential for better treatment outcomes and screening for T2DM would offer new opportunities to identify patients with undiagnosed T2DM or at risk of T2DM. However, fewer felt it is essential (58%) or appropriate (70%) for OHPs to perform or conduct chair side screening for DM.
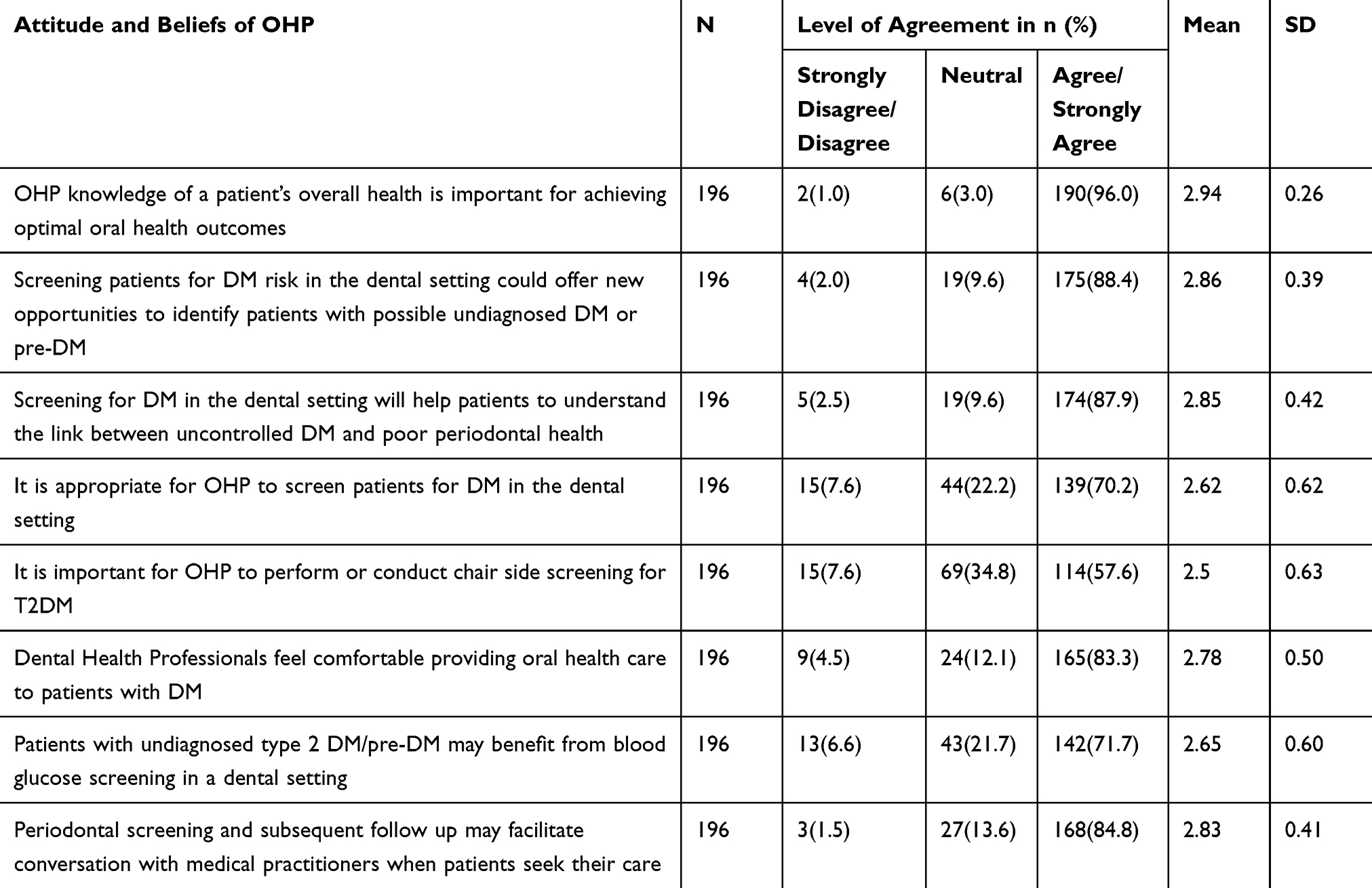 |
Table 3 OHP Response to Attitudes and Beliefs Variables |
Individual attitude item analysis identified more female (67%) OHPs agreed or strongly agreed that “It is important for OHPs to perform or conduct chair side screening for T2DM”. Public sector OHPs (n= 31, 79%) compared to private practitioners (n = 78, 55%) also responded that chairside screening for T2DM is important and this difference was statistically significant (χ2(2) = 8.03, p = 0.018).
There was a significant difference in the overall attitude score by gender, practice type and type of OHP. Female OHPs had a significantly higher DM related mean attitude score (p = 0.01) compared to the males. Since the overall test was significant for the practice type and type of OHP, post hoc pairwise multiple comparisons were performed to examine responses within each category, but no significant difference was observed between the private, public or other practice type. However, post hoc pairwise multiple comparisons identified significant difference where dental hygienists and therapists expressed more positive attitude towards screening compared to specialist dentists.
DM Related Practice Behaviour Scores
Tables 1 and 4 present DM related practice behaviour scores. The mean practice score was 2.43 (SD = 0.46) with a range of 1.1 to 3. There was a significant difference in the overall practice behaviour scores and practice location (P = 0.03). Even though the overall test was significant, none of the individual pairwise comparisons identified significant differences within the group.
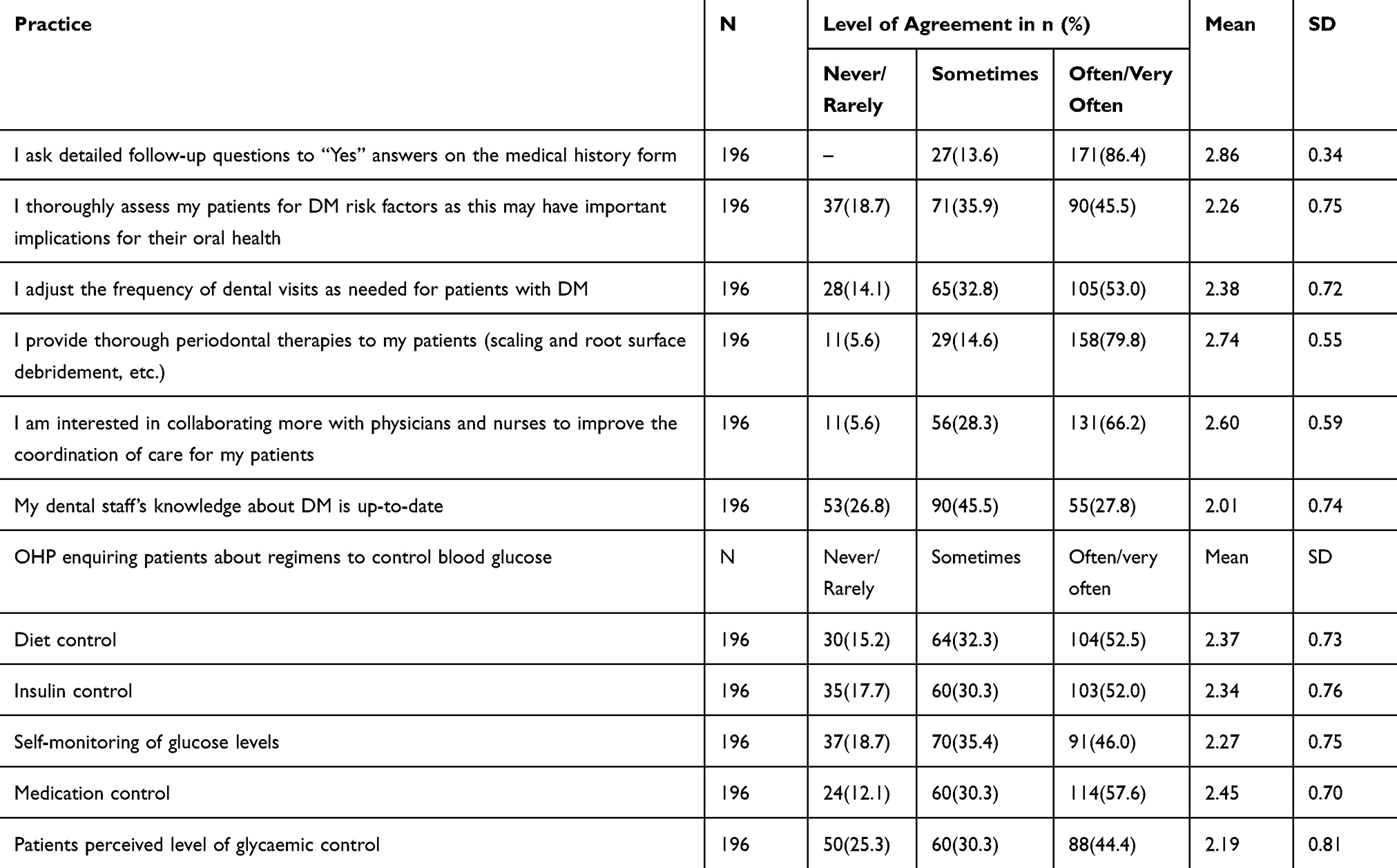 |
Table 4 Frequency Table for Practice Behaviour Variable |
Individual item analysis of practice variables identified approximately 80% or more of the respondents indicated (very often/always) that they make a detailed inquiry of the patient’s medical history and provide thorough periodontal therapies. Around half the responding OHPs cited (very often/always) that they thoroughly assess their patients’ DM risk or adjust the frequency of dental visits based on DM risk. Around 65% indicated their willingness to collaborate more with physicians and nurses to improve patient care behaviour. Only 29% responded (as very often/always) that their staffs’ knowledge about DM was up-to-date.
Important Consideration for Implementing T2DM Screening
Tables 1 and 5 present the potential barriers to implement T2DM screening in the dental setting. The mean barriers score was 2.1 (SD = 0.38) with a range of 1 to 3. Significant differences were observed within categories of location, type of practice, OHPs and work experience. However, pairwise comparison failed to identify that this difference existed within the categories of practice location. Overall, OHPs with more than 10 years of work experience rated as of lower importance, patient willingness, legal liability, time and insurance coverage for implementing T2DM screening. Pairwise comparison of the type of practice and OHPs identified significant differences in the response of dental hygienists, dental therapists and general dentists and between private practitioners and others. Individual item analysis identified patient willingness as the most important consideration (mean = 2.3), insurance coverage the least important (mean = 1.9) and no significant difference within groups was observed.
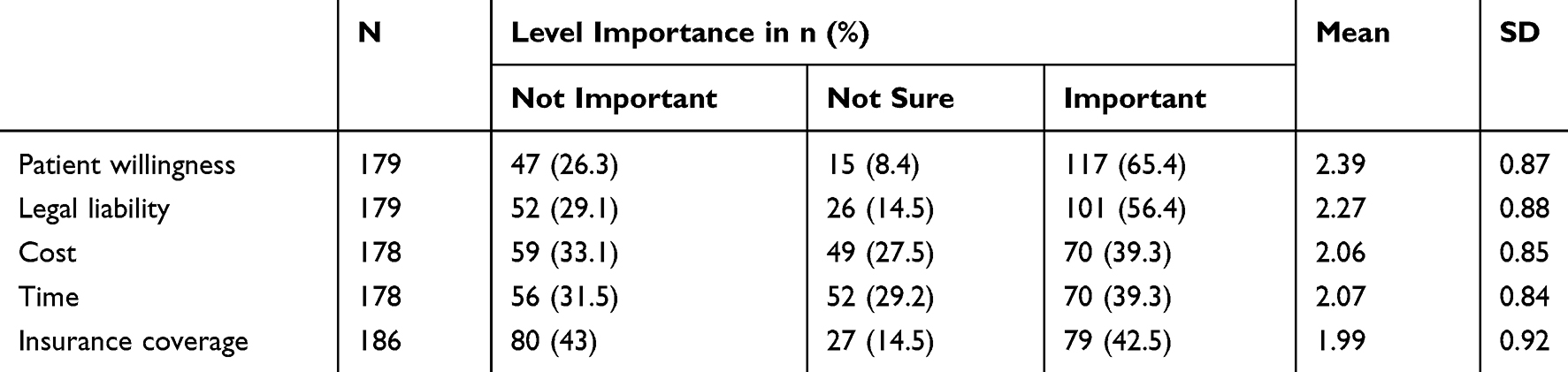 |
Table 5 Level of Importance OHP Foresee for Incorporating DM Screening |
Table 6 summarizes the results of the regression model. Results of the linear regression analysis were significant, F (2184) = 12.87, p < 0.001, R2 = 0.12, indicating that approximately 12% of the variance in practice behavior was explainable by knowledge and attitude values. Knowledge and attitude significantly predict practice behavior, B = 0.33, t(184) = 2.38, p = 0.018; B = 0.42, t(184) = 3.28, p = 0.001. This indicates that on average a one-unit increase in knowledge will increase the practice behavior score by 0.33 units and further a unit increase of attitude will increase the value of practice behavior by 0.42 units.
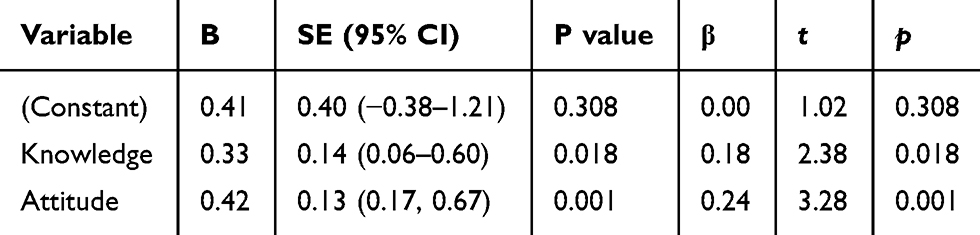 |
Table 6 Level of Importance OHP Foresee Incorporating DM Screening |
Discussion
To our knowledge, this study is the first to examine Victorian OHPs’ knowledge on DM attitudes towards screening and management of patients with DM. The results of this study show that around 86% of the OHPs had adequate knowledge of DM. There was very little difference in the average knowledge scores among the different type of OHPs or those with less or more than 10 years of work experience with a mean correct answer of 17 out of 22 questions.
Among the knowledge variable, only 12% of the OHPs identified osteoporosis as a significant complication of DM. This may be due to the fact that evidence relating T2DM and Bone Mineral Density (BMD) is inconsistent and equivocal.27–32 Having said that, several studies have demonstrated higher incidence of fracture among T2DM being linked to glycaemic control, retinopathy, peripheral neuralgia and stroke, thus increasing the risk of fall.33–36
When we compared our results with a similar survey on U.S general dentists24 and dental hygienists37 on selected (DM risk factors) knowledge items with the same wording, we observed Victorian OHPs with 7–8% higher knowledge scores. However, the number of survey respondents in our study was small and may not be representative of the entire Victorian OHPs. As such, results need to be interpreted with caution.
The overall attitude of OHPs towards screening for T2DM appears positive, with an average 93% agreement. The results were encouraging as the willingness to address this important issue seems to exist. Although 70% of the OHPs acknowledged that it is appropriate to screen patients for T2DM in the dental setting, only 58% felt it is important to perform chairside screening for T2DM. Among the respondents, twice as many (77%) dental hygienists and therapists felt it is essential to perform chairside screening compared to specialist dentists. This difference in opinion may be due to the fact that a quarter of the specialist dentists were Orthodontists and Paedodontists who would primarily treat children and young adults. Having said that, it is not easy to ascertain plausible reasons for the difference in opinion when the responding specialist dentist, dental hygienist and dental therapist number in this survey is small.
When we compared our findings (Figure 1) against the first nationwide survey of U.S dental professionals,16,38 Victorian OHPs exhibited 18.6% and 11.8% lower importance to chairside screening of T2DM. However, when compared against the New Zealand dentists,39 Victorian dentists expressed 28% higher importance to chairside screening of T2DM. The reduced willingness among the New Zealand dentists may be due to the wording “finger stick test” used in the survey.39 Again, the results need to be interpreted with caution because of the disproportionate participant numbers in all these studies.
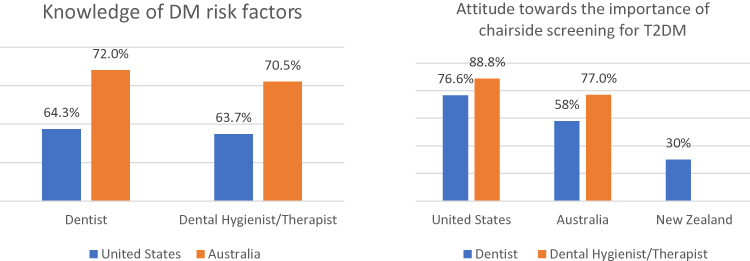 |
Figure 1 Comparison of OHP Knowledge and attitude with other countries. |
Knowledge, attitudes and beliefs are strong predictors of intentions and behaviour.40–42 Studies among a variety of health-care providers, including dentists, show clear evidence of psychological theory translating into practice.16,41-43 Our analysis identified that knowledge and attitudes significantly predicted practice behaviour. OHPs acknowledged that only 29% of their staff knowledge on DM was up-to-date. With a significant number of patients with DM accessing oral health services, the need for updating staff knowledge with formal training is important. This will help improve their confidence, effectiveness in patient management by asking the right questions and improving on the referral process for medical attention.
Diabetes Australia, in partnership with the International Diabetes Federation (IDF) provides a free online course on DM for health professionals with a certificate on completion of the training module.44 Findings from this study will help to inform OHPs of the need to discuss risk factors for DM if we expect to see any change in the disease level or associated complication of this prevalent yet preventable condition. OHPs can also play an important role in creating awareness about DM amongst patients, and promoting healthy lifestyles, attitudes and habits by enhancing patients’ understanding of the potential oral health consequences associated with their behaviours.
The survey identified patient willingness as the most important consideration among the OHPs for implementing T2DM screening in the dental setting. A study conducted in Thailand identified 80–85% of the dental patients in university, hospital, and private clinics were willing to be screened for T2DM in the dental setting.45 However, patient compliance for physician referral was identified a significant concern in a study conducted in the US46 with only 21.5% of the dental patients from private dental clinics following up with their physician despite an HbA1c value of 5.7 or more and being informed prior of the possibility of being referred to the physician. The reasons for non-adherence are not clear but resistance to comply is a significant barrier and strategies to overcome this need to be explored. The author further recommended a formal contract with the patient to follow up with referral or involve more OHPs to monitor the entire process with the referral and follow-up.46 Such concerns need to be explored and addressed to establish and streamline this extended service in the dental setting. It is important for OHPs to appreciate the value, willingness to screen and patient compliance.
Australians generally have favourable dental visiting patterns, and dental practice visits offer a largely untapped opportunity for DM screening. Most patients visit their OHPs when they perceive themselves as not unhealthy, but visit the physician only when they are sick.47 Such findings give OHPs an opportunity to screen asymptomatic patients with underlying medical conditions in the dental setting. By stretching the number of contact points between health-care providers and individuals seeking care, there is plenty of opportunity for early detection of asymptomatic individuals at risk of T2DM. Shared responsibility for early identification will also lessen some of the load imposed on the medical community. Routine oral health screenings can be extended to systematically screen for particular diseases, such as DM.48 Several studies have shown that health professionals from different specialities have contributed in the identification of DM.46,49-51
Conclusion
Overall, knowledge, attitude and practice towards DM was positive. There is increasing interest towards medical screening in the dental setting, but a significant proportion of the OHPs felt chairside screening may not be appropriate or important. To implement T2DM screening in the dental setting, it is important for OHPs to appreciate the value, willingness to screen and compliance of the patient. Currently, there are no evidence-based guidelines for medical screening from the state dental regulating bodies in Australia. As such, a positional statement is vital in motivating OHP and determine the scope of medical screening in the dental setting.
Acknowledgment
This study was supported by Colgate Palmolive Limited. We thank Rodrigo Marino, Meredith Temple Smith, Jennifer O’Connor, Meaghan Quinn and Michele King for their support in carrying out this survey.
Disclosure
The authors declare that they have no competing interests.
References
1. Whiting DR, Guariguata L, Weil C, et al. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–321. doi:10.1016/j.diabres.2011.10.029
2. Shaw JTS. Diabetes: The Silent Pandemic and Its Impact on Australia. Melbourne: Baker IDI Heart and Diabetes Institute;2012. Available from: https://www.baker.edu.au/-/media/Documents/impact/diabetes-the-silent-pandemic.ashx?la=en.
3. Diabetes Australia. Diabetes in Australia. 2018. Available from: https://www.diabetesaustralia.com.au/diabetes-in-australia.
4. Sainsbury E, Shi Y, Flack J, et al. Burden of diabetes in Australia: its time for more action. 2018. Available from: https://sydney.edu.au/content/dam/corporate/documents/faculty-of-medicine-and-health/research/centres-institutes-groups/burden-of-diabetes-its-time-for-more-action-report.pdf.
5. International Diabetes Federation. IDF diabetes atlas. 2015. Available from: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas.
6. Lee CM, Colagiuri R, Magliano DJ, et al. The cost of diabetes in adults in Australia. Diabetes Res Clin Pract. 2013;99(3):385–390. doi:10.1016/j.diabres.2012.12.002
7. Bansal N. Prediabetes diagnosis and treatment: a review. World J Diabetes. 2015;6(2):296. doi:10.4239/wjd.v6.i2.296
8. Buysschaert M, Medina JL, Bergman M, et al. Prediabetes and associated disorders. Endocrine. 2015;48(2):371–393. doi:10.1007/s12020-014-0436-2
9. Li G, Zhang P, Wang J, et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing diabetes prevention study: a 20-year follow-up study. Lancet. 2008;371(9626):1783–1789. doi:10.1016/S0140-6736(08)60766-7
10. Rahman M, Simmons RK, Hennings SH, et al. How much does screening bring forward the diagnosis of type 2 diabetes and reduce complications? Twelve year follow-up of the Ely cohort. Diabetologia. 2012;55(6):1651–1659. doi:10.1007/s00125-011-2441-9
11. Lamster I, Lalla E, Borgnakke W, et al. The relationship between oral health and diabetes mellitus. J Am Dent Assoc. 2008;139(Suppl):19S–24S. doi:10.14219/jada.archive.2008.0363
12. Mealey BL, Rose LF. Diabetes mellitus and inflammatory periodontal diseases. Curr Opin Endocrinol Diabetes Obes. 2008;15(2):135–141. doi:10.1097/MED.0b013e3282f824b7
13. Beikler T, Kuczek A, Petersilka G, et al. In-dental-office screening for diabetes mellitus using gingival crevicular blood. J Clin Periodontol. 2002;29(3):216–218. doi:10.1034/j.1600-051x.2002.290306.x
14. Lalla E, Cheng B, Kunzel C, et al. Dental findings and identification of undiagnosed hyperglycemia. J Dent Res. 2013;92(10):888–892. doi:10.1177/0022034513502791
15. Lalla E, Kunzel C, Burkett S, et al. Identification of unrecognized diabetes and pre-diabetes in a dental setting. J Dent Res. 2011;90(7):855–860. doi:10.1177/0022034511407069
16. Greenberg BL, Glick M, Frantsve-Hawley J, et al. Dentists’ attitudes toward chairside screening for medical conditions. J. Am Dent Assoc. 2010;141(1):52–62. doi:10.14219/jada.archive.2010.0021
17. Albert DA, Severson H, Gordon J, et al. Tobacco attitudes, practices, and behaviors: a survey of dentists participating in managed care. Nicotine Tob Res. 2005;7(Suppl 2):S9–S18. doi:10.1080/14622200500078014
18. Patton LL, Ashe TE, Elter JR, et al. Adequacy of training in oral cancer prevention and screening as self-assessed by physicians, nurse practitioners, and dental health professionals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(6):758–764. doi:10.1016/j.tripleo.2005.10.072
19. Curran AE, Caplan DJ, Lee JY, et al. Dentists’ attitudes about their role in addressing obesity in patients: a national survey. J Am Dent Assoc. 2010;141(11):1307–1316. doi:10.14219/jada.archive.2010.0075
20. Lee JY, Caplan DJ, Gizlice Z, et al. US pediatric dentists’ counseling practices in addressing childhood obesity. Pediatr Dent. 2012;34(3):245–250.
21. Barasch A, Safford MM, Qvist V, et al. Random blood glucose testing in dental practice: a community-based feasibility study from the dental practice-based research network. J Am Dent Assoc. 2012;143(3):262–269. doi:10.14219/jada.archive.2012.0151
22. Greenberg BL, Kantor ML, Bednarsh H. American dental hygienists’ attitudes towards chairside medical screening in a dental setting. Int J Dent Hyg. 2017;15(4):e61–e68.
23. Owens JB, Wilder RS, Southerland JH, et al. North Carolina internists’ and endocrinologists’ knowledge, opinions, and behaviors regarding periodontal disease and diabetes: need and opportunity for interprofessional education. J Dent Educ. 2011;75(3):329–338.
24. Paquette DW, Bell KP, Phillips C, et al. Dentists’ knowledge and opinions of oral-systemic disease relationships: relevance to patient care and education. J Dent Educ. 2015;79(6):626–635.
25. Dental Board of Australia. Statistics - Registrant Data. 2017. Available from: http://www.dentalboard.gov.au/About-the-Board/Statistics.aspx.
26. Faul F, Erdfelder E, Buchner A, Lang A-G. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
27. Ma L, Oei L, Jiang L, et al. Association between bone mineral density and type 2 diabetes mellitus: a meta-analysis of observational studies. Eur J Epidemiol. 2012;27(5):319–332. doi:10.1007/s10654-012-9674-x
28. Sundararaghavan V, Mazur MM, Evans B, et al. Diabetes and bone health: latest evidence and clinical implications. Ther Adv Musculoskelet Dis. 2017;9(3):67–74. doi:10.1177/1759720X16687480
29. De Liefde I, Van der Klift M, De Laet C, et al. Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. Osteoporosis Int. 2005;16(12):1713–1720. doi:10.1007/s00198-005-1909-1
30. Akin O, Göl K, Aktürk M, et al. Evaluation of bone turnover in postmenopausal patients with type 2 diabetes mellitus using biochemical markers and bone mineral density measurements. Gynecol Endocrinol. 2003;17(1):19–29. doi:10.1080/gye.17.1.19.29
31. Starup-Linde J. Diabetes, biochemical markers of bone turnover, diabetes control, and bone. Front Endocrinol (Lausanne). 2013;4:21. doi:10.3389/fendo.2013.00021
32. Migliaccio S, Greco EA, Fornari R, et al. Is obesity in women protective against osteoporosis? Diabetes Metab Syndr Obes. 2011;4:273–282. doi:10.2147/DMSO.S11920
33. Dede AD, Tournis S, Dontas I, et al. Type 2 diabetes mellitus and fracture risk. Metabolism. 2014;63(12):1480–1490. doi:10.1016/j.metabol.2014.09.002
34. Schwartz AV, Hillier TA, Sellmeyer DE, et al. Older women with diabetes have a higher risk of falls: a prospective study. Diabetes Care. 2002;25(10):1749–1754. doi:10.2337/diacare.25.10.1749
35. Maurer MS, Burcham J, Cheng H. Diabetes mellitus is associated with an increased risk of falls in elderly residents of a long-term care facility. J Gerontol a Biol Sci Med Sci. 2005;60(9):1157–1162. doi:10.1093/gerona/60.9.1157
36. Strotmeyer ES, Cauley JA, Schwartz AV, et al. Nontraumatic fracture risk with diabetes mellitus and impaired fasting glucose in older white and black adults: the health, aging, and body composition study. Arch Intern Med. 2005;165(14):1612–1617. doi:10.1001/archinte.165.14.1612
37. Bell KP, Phillips C, Paquette DW, et al. Dental hygienists’ knowledge and opinions of oral-systemic connections: implications for education. J Dent Educ. 2012;76(6):682–694.
38. Greenberg BL, Kantor ML, Bednarsh H. American dental hygienists’ attitudes towards chairside medical screening in a dental setting. Int J Dent Hyg. 2017;15(4):e61–e8. doi:10.1111/idh.2017.15.issue-4
39. Forbes K, Thomson WM, Kunzel C, et al. Management of patients with diabetes by general dentists in New Zealand. J Periodontol. 2008;79(8):1401–1408. doi:10.1902/jop.2008.070640
40. Perkins M, Jensen P, Jaccard J, et al. Applying theory-driven approaches to understanding and modifying clinicians’ behavior: what do we know? Psychiatr Serv. 2007;58(3):342–348. doi:10.1176/ps.2007.58.3.342
41. Limbert C, Lamb R. Doctors’ use of clinical guidelines: two applications of the theory of planned behaviour. Psychol Health Med. 2002;7(3):301–310. doi:10.1080/13548500220139377
42. Walker AE, Grimshaw JM, Armstrong EM. Salient beliefs and intentions to prescribe antibiotics for patients with a sore throat. Br J Health Psychol. 2001;6(Part 4):347–360. doi:10.1348/135910701169250
43. Edwards HE, Nash RE, Najman JM, et al. Determinants of nurses’ intention to administer opioids for pain relief. Nurs Health Sci. 2001;3(3):149–159. doi:10.1046/j.1442-2018.2001.00080.x
44. D-NET The International Diabetes Federation - Diabetes Network for Health Professionals. Connecting Diabetes Professionals Worldwide. Available from: https://d-net.idf.org/en.
45. Tantipoj C, Hiransuthikul N, Supa-amornkul S, et al. Patients’ attitude toward diabetes mellitus screening in Thai dental clinics. J Health Res. 2018;32(1):2–11. doi:10.1108/JHR-11-2017-001
46. Genco RJ, Schifferle RE, Dunford R, et al. Screening for diabetes mellitus in dental practices: a field trial. J Am Dent Assoc. 2014;145(1):57–64. doi:10.14219/jada.2013.7
47. Glick M, Greenberg BL. The potential role of dentists in identifying patients’ risk of experiencing coronary heart disease events. J Am Dent Assoc. 2005;136(11):1541–1546. doi:10.14219/jada.archive.2005.0084
48. Sultan A, Warreth A, Fleming P, et al. Does the dentist have a role in identifying patients with undiagnosed diabetes mellitus? J Ir Dent Assoc. 2014;60(6):298–303.
49. Martinell M, Dorkhan M, Stalhammar J, et al. Prevalence and risk factors for diabetic retinopathy at diagnosis (DRAD) in patients recently diagnosed with type 2 diabetes (T2D) or latent autoimmune diabetes in the adult (LADA). J Diabetes Complications. 2016;30(8):1456–1461. doi:10.1016/j.jdiacomp.2016.08.009
50. AlGhamdi AST, Bukhari SMN, Elias WY, et al. Dental clinics as potent sources for screening undiagnosed diabetes and prediabetes. Am J Med Sci. 2013;345(4):331–334. doi:10.1097/MAJ.0b013e318287c96c
51. Willis A, Rivers P, Gray LJ, et al. The effectiveness of screening for diabetes and cardiovascular disease risk factors in a community pharmacy setting. PLoS One. 2014;9(4):e91157. doi:10.1371/journal.pone.0091157
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.