Back to Journals » Patient Preference and Adherence » Volume 19
Development of the PRACTIC Goal Setting Interview (PGSI) for Frail Community-Dwelling Patients. Feasibility, Interrater Reliability and Content validity—a Mixed Methods Study
Authors Væringstad A ![]() , Kirkevold Ø
, Kirkevold Ø ![]() , Dalbak ETG
, Dalbak ETG ![]() , Myhre J, Feiring IH
, Myhre J, Feiring IH ![]() , Bergh S
, Bergh S ![]() , Lichtwarck B
, Lichtwarck B ![]()
Received 30 July 2025
Accepted for publication 1 December 2025
Published 12 December 2025 Volume 2025:19 Pages 4033—4050
DOI https://doi.org/10.2147/PPA.S557233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Anette Væringstad,1,2 Øyvind Kirkevold,1– 3 Ellen Thea Gjelseth Dalbak,1,2 Janne Myhre,4,5 Ingvild Hjorth Feiring,1 Sverre Bergh,1,3 Bjørn Lichtwarck1
1The Research Centre for Age-Related Functional Decline and Disease, Innlandet Hospital Trust, Ottestad, Norway; 2Faculty of Medicine NTNU, Department of Health, Care and Nursing, Norwegian University of Science and Technology, Gjovik, Norway; 3The Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust, Vestfold, Norway; 4Faculty of Social and Health Sciences, Inland Norway University of Applied Sciences (INN University), Elverum, Norway; 5Norwegian Centre for Violence and Traumatic Stress Studies (NKVTS), Oslo, Norway
Correspondence: Anette Væringstad, The Research Centre for Age-related Functional Decline and Disease, Innlandet Hospital Trust, Ottestad, Norway, Tel +47 995 40 470, Email [email protected]; [email protected]
Introduction: Goal-setting interviews in randomised controlled trials (RCTs), such as the Bangor Goal-Setting Interview (BGSI), provide personalised, measurable outcomes that are meaningful to participants because they reflect their unique needs. The PRACTIC (PReventing and Approaching Crises for frail community-dwelling patients Through Innovative Care) RCT (2023– 2024) evaluates a biopsychosocial intervention to approach and prevent crises for frail community-dwelling patients. The PRACTIC Goal Setting Interview (PGSI), adapted from the BGSI, focuses on individual goal attainment and readiness to change and was chosen as the primary outcome in the PRACTIC RCT. This study aimed to translate and develop the PGSI, exploring its feasibility, content validity and interrater reliability.
Design and Methods: This study used a convergent mixed-method design; quantitative and qualitative data were collected with equal priority, analysed separately, and compiled for the results and discussion. Two substudies are included: 1) translation and development of the BGSI towards the PGSI and 2) feasibility, content validity and interrater reliability of the PGSI. Substudy 1 comprised field notes from meetings with municipal staff (n=7) across two municipalities. Substudy 2 included data from 28 municipalities participating in the PRACTIC RCT; patient (n=126), next of kin (n=72), and data from focus groups with staff members (n=13) and data collectors (n=5), as well as individual interviews; patients (n=8) and next of kin (n=4).
Results: The PGSI was well received in the home care services and helped strengthen patient involvement. However, there were challenges in using the PGSI, such as time pressure and workload for the staff. After 12 weeks, participants with high motivation showed a significant increase in PGSI compared with those with low motivation (p = 0.010). Analyses also revealed strong positive correlations between participants and staff members assessments of goal attainment at 12 weeks (Spearman’s ρ = 0.87– 0.92, p < 0.001). The results indicate that the PGSI is a valid and reliable tool for improving patient care through structured goal setting and the active involvement of patients and their next of kin.
Conclusion: The PGSI appears to be a useful and feasible tool for goal setting in home care services. The tool strengthens patient engagement and goal attainment with high content validity and interrater reliability.
Trial Registration: ClinicalTrials.gov identifier: NCT05651659. Registration date: 07.12.22.
Keywords: frailty, crises, home care services, health services for the aged, goal setting, PRACTIC goal setting interview, PGSI
Introduction
The number of older people over the age of 65 is expected to double by 2050, according to the UN report on ageing from 2020.1 Increasing life expectancy contributes to the growing population of individuals over 65 years of age.2 It is important that older people are involved in decisions that affect their own health and care and that they are supported in taking care of their own health through information and guidance.3 Patient participation ensures tailored care that matches individual needs and preferences, resulting in more effective and satisfying health experiences.4 People who receive home care services are a heterogeneous group with variations in their level of functioning, age, life situation, number of diseases and severity, and many have several chronic diseases (multimorbidity).5–7 The number of older people with multimorbidity is estimated to double over the next 20 years, and one-third of this group will suffer from cognitive impairment, dementia, or depression.8 Many older people also experience major life changes and losses, and their health conditions may deteriorate. In addition, many older people are frail.7,9 Frailty is a complex phenomenon influenced by biological, psychological, and social factors.10 Frailty can be defined as a condition of physiological vulnerability characterized by a decreased ability to respond to and manage both internal and external stressors.11 The estimated prevalence of frailty is 11% among people over 65 years of age, increasing to 50% in those over 80 years of age.11–13 People who are frail and receive home care services face a considerable risk of being in an unstable situation, that is, a crisis, which can result in undesirable incidents, coercive measures, and urgent hospitalisation.14–16 Coercive measures in the context of crises refer to care practices carried out without the person’s consent, often to protect the individual or others.14 According to a study by Clare et al,17 patients who want to improve aspects of their daily functioning may experience the ability to set individual goals. The authors stated that the personalised approach can be applied flexibly to accommodate different types of needs and unstable situations.17,18
In 2019, the Early Detection and Timely INTERvention in DEMentia network (INTERDEM) presented a manifesto describing how research should be planned and conducted so that it considers the heterogeneity of the people who are the subject of the research.19 The authors described that individualised interventions provide the opportunity to develop person-centred approaches to individual patients. They also emphasised that outcome measures for assessing the effects of such interventions should be coordinated across biomedical and psychosocial approaches. INTERDEM highlights the importance of an approach that focuses on individual goal attainment to ensure that the results of the research are both relevant and applicable in practice.19 The Bangor Goal-Setting Interview Manual, by Clare et al,20 indicates that goal-setting interviews can be used both in clinical practice and research. The manual provides a structured approach to setting and achieving personal goals, especially for people with cognitive challenges or other health problems. The manual emphasizes the importance of setting specific, measurable, attainable, relevant/reasonable, and time-bound (SMART) goals to improve daily functioning, well-being, and self-activity. The process consists of four main steps: identifying areas to work on, setting goals, assessing current goal attainment and motivation to achieve the goal, and evaluation progress and evaluating progress. The manual includes various types of questions to facilitate the identification and setting of goals, emphasizing a collaborative process between the interviewer and the interviewee, often with the involvement of next of kin.20 According to Clare et al,17 goal-setting interviews are a key component in ensuring holistic and person-centred care for elderly people living at home. It promotes their participation, improves the quality of care, and contributes to a better quality of life. When goals are person-centred and relevant, the patient may experience a sense of control and patient involvement. The next of kin plays a crucial role in implementing and sustaining changes in daily life for this group of patients.17 This is a patient group that often has complex needs and limited ability to handle these themselves, which makes support from close relationships extra important. A systematic review by Nordaunet et al21 revealed that family members experienced a gap between the basic care provided and their perceived need for support. The perspective and participation of family members can enrich goal-setting conversations by adding unique insights and emotional depth.17 For frail older people, who often have disabilities and reduced cognitive capacity, the efforts of next of kin are crucial for continuity of care and quality of life. Their participation adds goal-setting interviews both insight and depth and contributes to realistic and sustainable follow-up plans. Next of kin should therefore be seen as an integral part of the care – not just a supplement.
Goal-setting interviews, as the primary outcome measure in randomised controlled trials (RCTs), can provide specific, personalised, and measurable outcomes that are meaningful to participants.20 A systematic review by Budgett et al22 in 2024 of goal-setting tools, including the Bangor Goal-Setting Interview (BGSI), revealed that these tools have good validity and reliability and are effective in capturing goals that are relevant to participants’ quality of life. Although the systematic review by Budgett et al reviewed studies including people living with dementia, the results may also be applicable to other patient groups. Using such goal-setting interviews ensures that research results, when they are statistically significant, also have the potential to be clinically relevant.22 Furthermore, this systematic review demonstrated that the BGSI is useful as a goal-setting tool for RCTs. The BGSI was also found to be reliable in one RCT.22,23 One advantage of using the BGSI is that the goal-setting interview provides good guidance for identifying personal goals, and the adaptability of the questionnaire makes it possible to use it in different contexts and with different populations.20 This can be particularly useful in populations with a large variation in individual needs.22 However, it is recommended that the reliability and validity of a scale be re-examined to evaluate the tool’s psychometric properties when adapted to and used in a new context and when translated into a new language.24 The COSMIN framework (COnsensus-based Standards for the selection of health Measurement INinstruments) emphasizes the importance of adapting the assessment of measurement properties to the purpose and context of the instrument. This supports our choice to investigate selected properties of PGSI (see Additional file 8), in particular content validity and interrater reliability, which represent two key measurement properties within COSMIN’s domains of validity and reliability.25
The Need for a Goal-Setting Interview Adapted to Norwegian Home Care Services
Starting in 2022, our research group designed a cluster RCT with 28 municipalities as clusters to evaluate the effectiveness of a biopsychosocial intervention to prevent and approach crises in a heterogeneous population of frail community-dwelling patients, the PReventing and Approaching Crises for frail community-dwelling patients Through Innovative Care (PRACTIC) study.26 The intervention in the PRACTIC RCT involves testing the effectiveness of an adapted version of a biopsychosocial person-centred model, the Targeted Interdisciplinary Model for Evaluation and Treatment of Neuropsychiatric Symptoms (TIME),27 to prevent and approach crises for frail patients who receive home care services in Norway. In this RCT, an adapted version of the TIME was tested, which included interdisciplinary case conferences and tailored treatment methods. The participants in the RCT represent a heterogeneous group with considerable variation in functional ability, age and living conditions. This includes both physical and psychosocial aspects. The inclusion criteria for the RCT were deliberately broad to include a diverse group of participants, making the study more pragmatic and representative of the real population receiving home care services. The inclusion criteria are the same in substudies 1 and 2 in this current study as in the PRACTIC RCT and are described under the method section.26 In this RCT, there was a need for a goal-oriented effectiveness outcome that embraced the variation in the challenges among the participants. In addition, there is a lack of studies investigating the use of goal-setting interviews where goal attainment can be assessed, in home care services in Norway. The goal of the intervention and the goal of the individual participant in the RCT, considering the heterogeneity of the population, necessarily vary from participant to participant.19 Thus, we translated and adapted a recently developed individual goal-setting interview, the BGSI,18,20 to measure the primary outcome in the PRACTIC. The translation and adaptation were performed in accordance with the research group that has developed the BGSI. We called our modified interview the PRACTIC Goal Setting Interview (PGSI). The PGSI identifies individual goals and assesses goal attainment, which expose changes and helps to find common goals set by the patient, next of kin and the home care services. Like the BGSI, the PGSI consists of four main steps to identify areas to work on, setting SMART goals, and scoring readiness to change and goal attainment. Readiness to change is scored from 0 (not ready to work with the goal) to 10 (very ready to work with the goal), while goal attainment is scored from 0 (cannot perform or does not perform satisfactorily) to 10 (can perform and performs very satisfactorily). This provides a structured approach to evaluating progress and developing realistic goals.
This study is guided by the Medical Research Council’s framework for complex interventions updated by Skivington et al in 2021, which provides a structured approach to designing and evaluating interventions in real-world settings.28 In this publication, we describe the translation and development of the BGSI towards the PGSI.
Methods
Aims of the Study
The study consisted of two substudies. First, the aim of substudy 1 was to describe the translation of the BGSI and the development of the BGSI towards the PGSI. Second, the aim of substudy 2 was to explore the feasibility, content validity and interrater reliability of the PGSI.
Design
This study has a convergent mixed method design, where quantitative and qualitative data are collected with equal priority and analysed separately but compiled for the results and discussion.
Methods Substudy 1: The Translation and Development of the BGSI Towards the PGSI
The BGSI was translated into Norwegian in line with the principles for translation and cultural adaptation of patient-reported outcome measures.29,30 Pilot testing of the translated BGSI was carried out in home care services in two municipalities (see Figure 1 for an overview of participants in the study). The purpose was to collect feedback on the clarity and relevance of the questions in the BGSI to develop an adapted goal interview for the home care services in Norway. Based on feedback from the pilot, the BGSI was revised, changed and adapted to become the PGSI. The core element of the BGSI is identifying individual personal goals, which was continued in the PGSI.18 Like the BGSI, the PGSI uses a scale from 0 to 10 to measure both the patient’s readiness for change and goal attainment. A higher score indicates a greater degree of readiness for change and goal attainment. For the development of the BGSI towards the PGSI, a qualitative method based on field notes was used.31
 |
Figure 1 Settings, participants and types of data in substudies 1 and 2. Notes: PGSI, PRACTIC Goal Setting Interview; PRACTIC, PReventing and Approaching Crises for frail community-dwelling patients Through Innovative Care. |
Settings and Participants in Substudy 1
In substudy 1 on the development of the BGSI towards the PGSI, a convenience sample of two municipalities located in southeastern Norway, close to our research centre, included seven members of the healthcare staff selected by their leaders from six different geographical zones in the municipalities. The healthcare staff from the municipality received training in how to carry out BGSI, and they then tested the BGSI with the patients in the municipalities. The included municipalities were, like other home care services in Norway, organized with healthcare staff who travelled out to the patients’ homes to provide the necessary help and support. A smaller sample made piloting the BGSI practical and manageable in terms of time and resources. We focused on going in-depth and getting detailed feedback from the staff who tested the BGSI. The healthcare staff and the municipalities in substudy 1 were only involved in the pilot study and did not participate in the PRACTIC RCT. See Figure 1 for an overview of the settings and participants in substudy 1. The BGSI was tested for four frail patients, ie, a Clinical Frailty Scale (CFS) score of 5 or higher.32 The recruitment of patients to test the BGSI was carried out by the staff in the home care services in the municipalities. It proved to be challenging to get frail elderly people to consent to participation. This difficulty can be due to several factors, including patients’ health status, concerns about strain, and lack of motivation to participate in research studies. The heterogeneity was reflected in the depth and detailsThe inclusion criteria for the patients on whom the questionnaire was to be tested were as follows: 1) recipients of home care services; 2) a score of 5 or higher on the CFS, corresponding to a mild to severe degree of frailty;32 and 3) an assessment by home care services of being in an unstable situation. The exclusion criteria were 1) expected short life expectancy (<4 weeks) and 2) decision-making for a long-term place in an institution. Other demographic or health data for these four patients were not collected in substudy 1.
A score of 5 or more on the Clinical Frailty Scale (CFS) indicates moderate to severe frailty, which can also comprise the impact of reduced cognition. People with a score of 5 may be cognitively intact and able to make decisions on their own but may need support in complex situations. At a score of 6 or higher, participants may have significant cognitive problems, but not necessarily, since there can be other reasons for their frailty. However, several patients with a high CSF score need significant support from the next of kin or home care services to make decisions.32
Data Collection Substudy 1
Qualitative Data
In substudy 1, AV (the first author) conducted three online meetings during the period, lasting approximately 1 hour, with the staff regarding the testing and the feasibility of BGSI and took field notes from these meetings. AV had a close dialogue with the staff by phone and e-mail and noted feedback about the testing of BGSI during the pilot study. The testing was conducted over six months. The staff provided feedback on the actual use of the BGSI. The topics that were evaluated/assessed included recruitment, who participated in the goal-setting interview, and the completion of steps 1–4 in the BGSI,20 at both baseline and follow-up assessments after 12 and 24 weeks. Additionally, the discussion covered factors that promoted and inhibited implementation.
Analyses in Substudy 1
Qualitative Analyses
The field notes in substudy 1 were analysed separately with thematic analysis and with a mainly deductive approach emphasising the feasibility of the translated version of the BGSI and possible promoting and inhibiting factors for conducting the BGSI.33,34 AV performed these analyses.
Methods Substudy 2: Feasibility, Content Validity and Interrater Reliability of the PGSI
For substudy 2, a mixed methods approach was used. Mixed methods, which combine quantitative and qualitative approaches, provide a more comprehensive exploration of the research questions.35 The quantitative part of the study provides a broad overview and ensures generalizability, whereas the qualitative part provides deeper insight into the participants’ experiences and contexts.35
Settings and Participants in Substudy 2
The participants in substudy 2 were the same as those in the control municipalities in the PRACTIC RCT. The RCT included 126 participants. There were 15 municipalities with 67 participants randomly assigned to the intervention condition and 13 municipalities with 59 participants to the control condition. The RCT included 28 randomly selected municipalities from different health regions in Norway, representing various sizes and offering diverse home care services. The patients who participated in substudy 2 had the same inclusion criteria as those in substudy 1. The participants in substudy 2 were a heterogeneous group, based on variations in age, gender, functional status, and overall health condition, reflecting the diversity within the broader frail population included in the study. See Figure 1 for an overview of the settings and participants in both substudies 1 and 2. The qualitative parts of substudy 2 included the following:
Individual Interviews
All 59 patients who completed the control group in the PRACTIC RCT from April 2023 to April 2024 were invited to participate in an individual interview about using the PGSI. Eight patients and four of their next of kin who agreed to participate in an individual interview were included in this substudy. Only patients in the control group were invited to individual interviews, in order to minimize potential bias in subsequent surveys to the staff conducted as part of the process evaluation of the PRACTIC RCT.36 This process evaluation was carried out after completion of the intervention in the RCT trial and primarily focused on the intervention group.
Three Focus Groups
Data collectors from our research centre were invited to participate in a focus group about the use of the PGSI. Five of a total of thirteen data collectors who had the opportunity and agreed to participate are included in this substudy. The five data collectors were a group of health care professionals (nurses and social educators) who had undergone one-day training in the use of PGSI and were responsible for carrying out PGSI for patients, next of kin and staff from home care services in the PRACTIC RCT. The data collectors had no prior relationship with the participants and were not involved in their care or treatment. All the staff members who were resource persons (called project nurses) from the control municipalities in the PRACTIC RCT were invited to participate in a focus group interview on the use of the PGSI. Of these, 13 project nurses at home care services in six of the 13 control municipalities agreed to participate. Two focus groups were conducted, with five project nurses in one group and seven project nurses in the other. The project nurses at the home care services had received one day’s training in inclusion criteria for the study, assessment of competence to consent and in the use of the PGSI. In the PRACTIC RCT, the project nurses played a crucial role in the implementation and management of the trial. Their responsibilities include recruitment and consent of the participants, facilitating training and education and facilitating data assessment for the data collectors. Data collectors, on the other hand, were specifically trained nurses from the project’s research center who were not affiliated with the municipalities.
In the quantitative part of substudy 2, baseline data from all 126 patients in the PRACTIC RCT, both the control and intervention groups, were included.26
Data Collection in Substudy 2
Qualitative Data
In substudy 2, individual in-depth interviews with patients and their next of kin were performed by AV (the first author). They were interviewed about their experiences with using PGSI after completing the first phase of the PGSI, ie, determination of individual goals, goal attainment and readiness to change/motivation. The interview also covered the second phase of the PGSI, which focused on goal attainment after 12 weeks. If the patient preferred (two patients), the next of kin and the patient were interviewed separately. Otherwise (two dyads), they were interviewed together. Four patients were interviewed without a next of kin. Six interviews were conducted by telephone at the patient’s request, and two were conducted physically in their homes. Each interview was based on a semistructured interview guide (see Additional file 5) and took approximately 30 minutes. If the patient or the next of kin raised other comments about the PGSI, additional time was allocated to explore the topics further. After each interview, AV provided a summary of the main explicit points and key findings, requesting that participants confirm or revise the summary as needed. The interviews were recorded as a digital audio file and transcribed verbatim prior to analysis.
The two focus groups for the project nurses were conducted as online interviews, whereas the focus group with the data collectors was conducted in person. AV was the moderator, and BL (last author) was the interview facilitator. The focus group interviews followed a semistructured interview guide (see Additional files 6 and 7) and took approximately one hour. At the end of each interview, the facilitator summarised the main points and asked the participants to confirm or amend the summary. All interviews were recorded as a digital audio file and transcribed verbatim prior to analysis.
Quantitative Data
In substudy 2, interrater reliability and content validity data were collected at baseline and at the 12-week follow-up for the 126 participants included in the PRACTIC RCT, including both the control and intervention groups. These data include 1) the descriptions of goals when using the PGSI, ie, the goals for the participants as stated at baseline; 2) the scores on the PGSI for the readiness to change/motivation of the patient (from 0–10) at baseline; and 3) goal attainments (from 0–10) assessed by the patient together with next of kin and goal attainments assessed by the service at baseline and the 12-week follow-up.
Analyses in Substudy 2
Qualitative Analyses
The transcripts of the interviews in substudy 2 were initially analysed separately by AV and BL, two researchers with different backgrounds. AV and BL then met several times to compare and summarise the analysis results at different stages of the analysis process. We used a cross-cutting thematic analysis in which patterns and themes in the interviews were searched to answer the question of the content validity and feasibility of the PGSI.34 The analysis method, therefore, involved a combined deductive approach based on the interview guide and an inductive approach rooted in the data. Thematic analysis is well suited for this purpose.34 Data collection was considered to have reached saturation when no new themes or concepts emerged during the analysis of the final interviews. Data management and coding were carried out in NVivo (software for qualitative data analysis). An example that illustrates how the main themes from the qualitative data were developed through coding and then evolved into subthemes and the final evolution of the themes is shown in Table 1.
 |
Table 1 Excerpts from the Development of the Themes in Substudy 2 |
Statistical Analyses
All the statistical analyses in substudy 2 were performed with the Statistical Program IBM SPSS Version 29.0. The scores for readiness to change/motivation among the patients using the PGSI are presented descriptively with means and standard deviations (SDs). A high score for readiness to change/motivation indicates a higher degree of content validity for the PGSI as a goal-setting interview. Concordance for stating goal attainment in the PGSI between the dyad’s patient/next of kin and staff was tested with Spearman correlation. The Mann‒Whitney U-test was used to compare dependent groups (staff and patient/next of kin). Wilcoxon’s rank test was used to compare independent groups (low and high motivation). In this study, p values lower than 0.05 were considered statistically significant.
Results
In this results section, the findings from substudy 1, with qualitative results from the analyses of the field documents on the development of PGSI, are presented first. This is followed by the results from substudy 2. In substudy 2, the results concerning the feasibility of the PGSI from the analyses of the interviews and focus groups are first presented. Next, the results on content validity as assessed through qualitative and quantitative analyses are presented. Finally, the results of the interrater reliability of the PGSI from the quantitative analyses are presented.
Substudy 1: Development of the PGSI
The feedback from the staff in the home care services was mostly positive regarding the feasibility of the translated BGSI. When the goal-setting interviews were conducted as natural dialogues, the conversations between staff and patients were conducted, which is in line with how the staff in home care services works as usual but now more systematically. The BGSI was experienced by the staff as clear and was followed systematically. The staff considered that the BGSI was well received by both patients and next of kin. To set goals, the visual scoring for assessing the readiness to change and goal attainment were perceived as rather straightforward tasks to perform. However, the staff in the home care services found it somewhat challenging to describe goal attainment as a percentage (identify the extent of goal attainment as 0%, 25%, 50%, 75% or 100%). The goal-setting interview was considered time-consuming, easily lasting an hour. It was deemed necessary to restructure the service’s work plan after lunch to carry out the PGSI. Table 2 provides an overview of the promoting and inhibiting factors for conducting the BGSI as conveyed by the staff in the home care services.
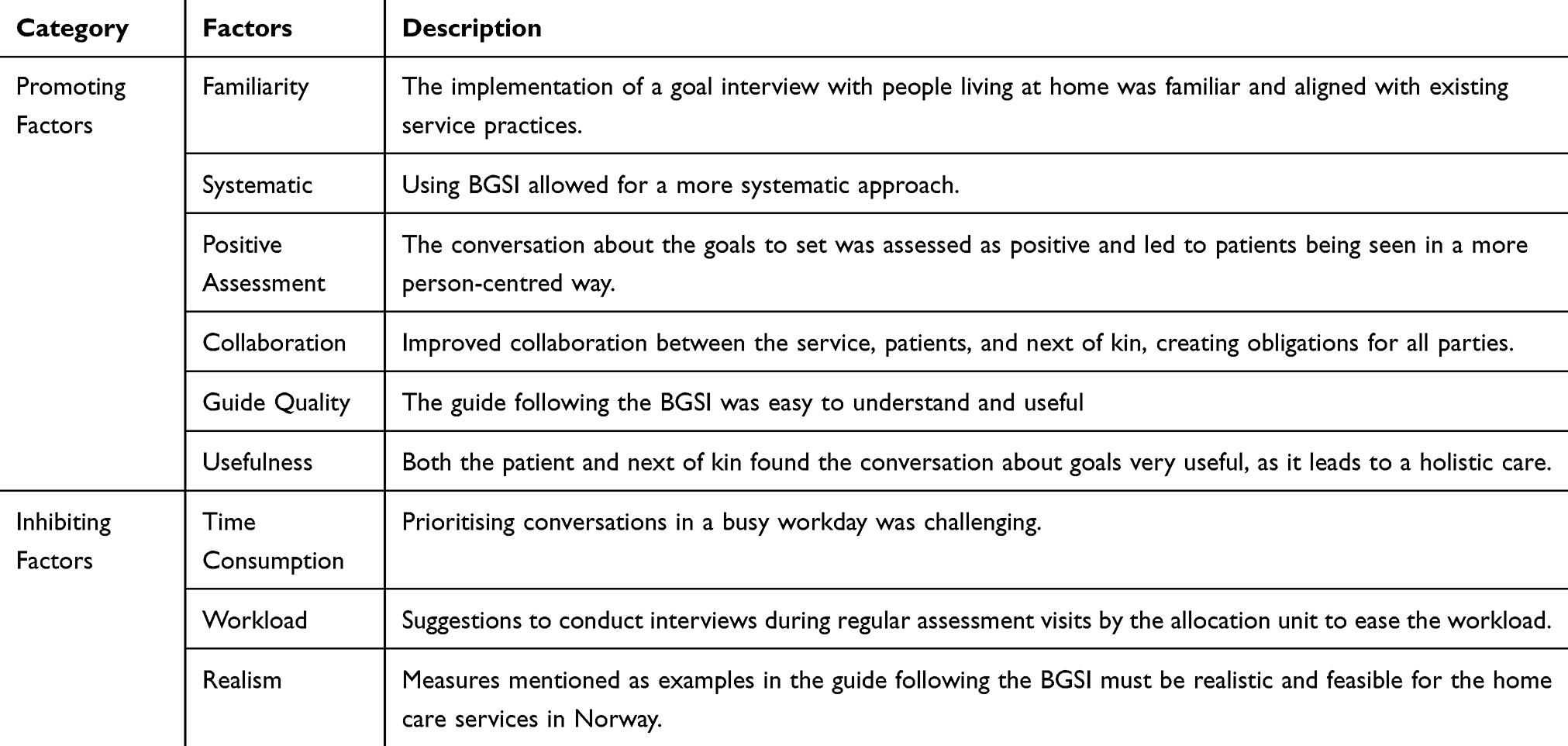 |
Table 2 Overview of Promoting Factors and Inhibiting Factors for Conducting the BGSI |
The pilot study entailed three specific changes from the original form of the BGSI to the final PGSI (see Table 3 for an overview of the differences between the BGSI and the PGSI):
- The BGSI guide was shortened and simplified to be more practical and easier to understand for those who work in home care services.
- In the BGSI, each goal is given a percentage value from 0–100% on the basis of the percentage of progress towards the set goals. This was removed in the design of the PGSI since it was challenging for home care services to score.
- Several examples of possible treatment measures and actions in the guide following the BGSI were not applicable to home care services in Norway. To further improve the ease of use of the form, they were changed to examples of more appropriate measures.
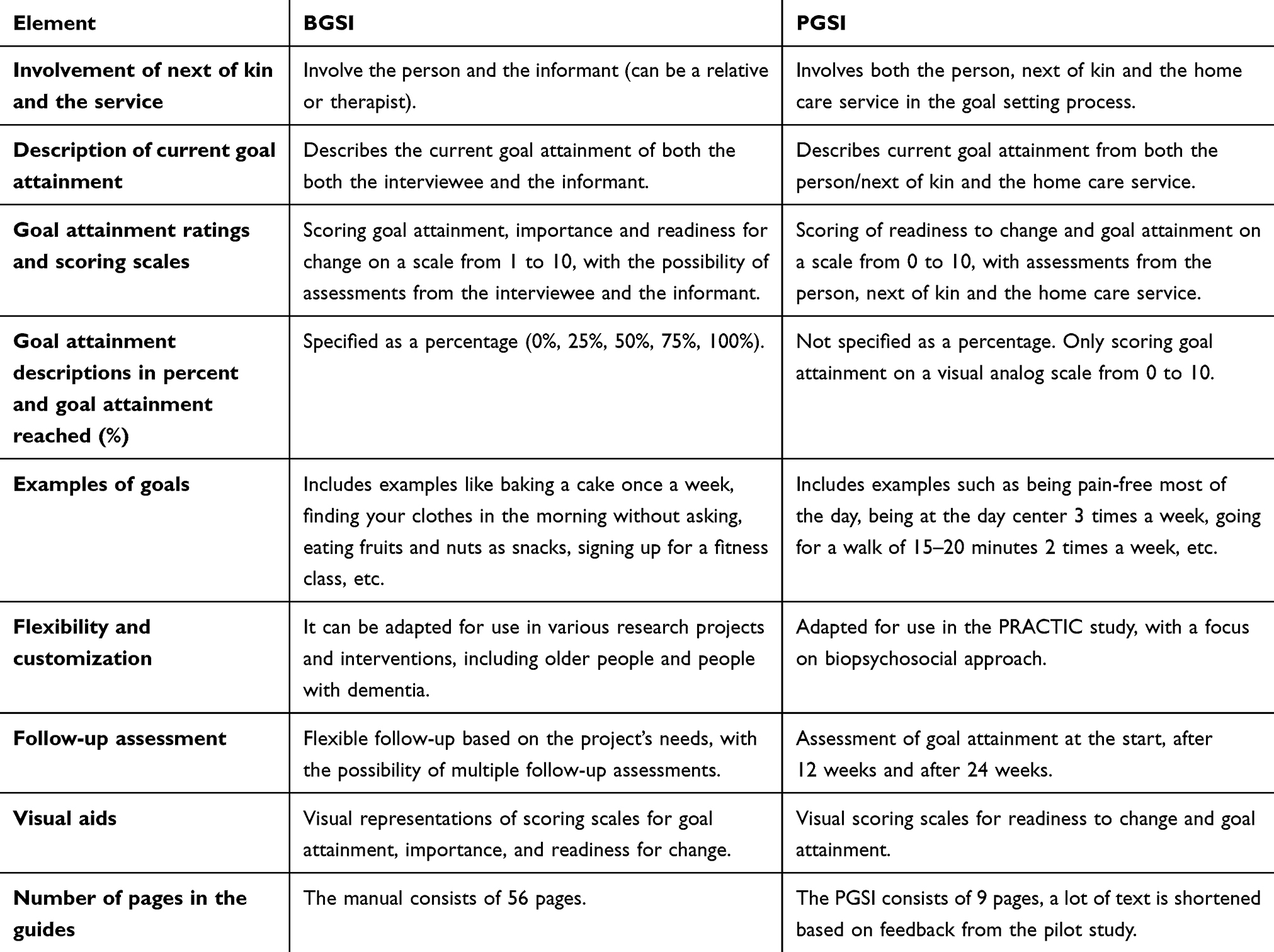 |
Table 3 Overview of the Differences Between the BGSI and the PGSI |
Substudy 2: Feasibility, Content Validity and Interrater Reliability of the PGSI
Feasibility
Based on the analysis of the goals set in the PGSI by the patients/next of kin and the home care services, a wide range of individual goals were observed. Table 4 presents a categorised presentation of patients’ goals, grouped according to relevant topics that emerged during the analysis. All the participants managed to set at least one goal.
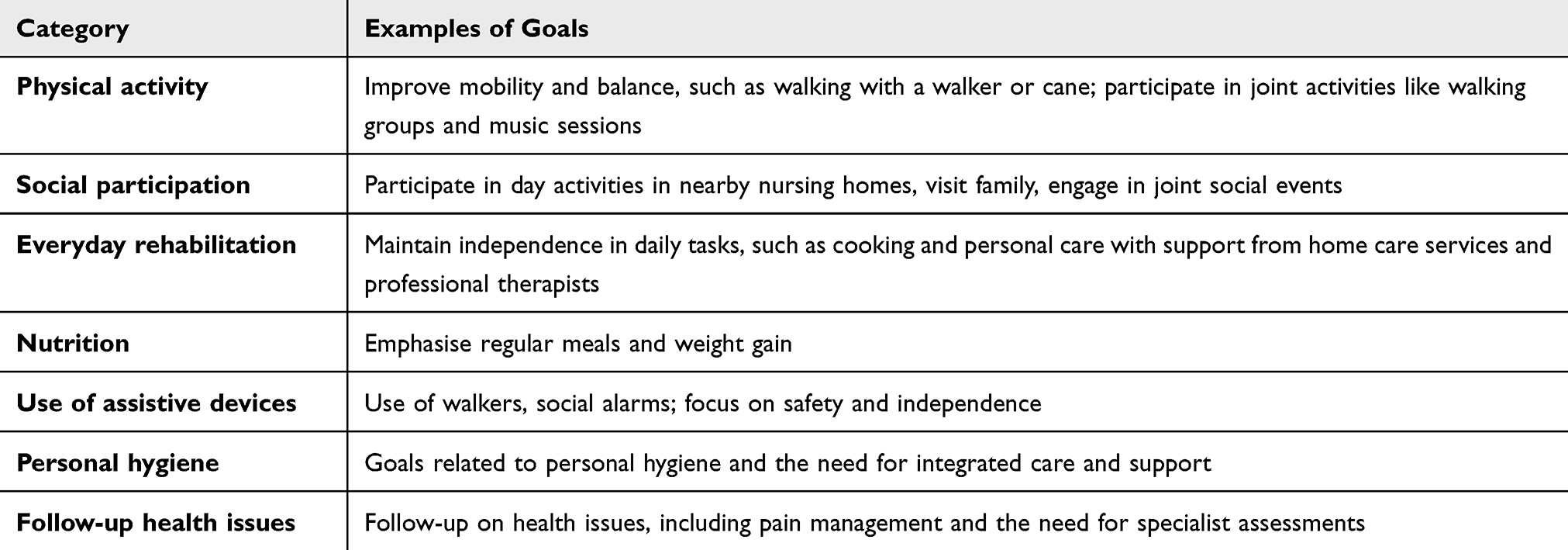 |
Table 4 Overview of the Various Goals Set by Patients and Their Next of Kin in the RCT |
Patient Engagement and Next-of-Kin Involvement Increased When the Goal-Setting Interview Was Used
The involvement of next of kin played an essential role in supporting patients both in identifying and setting concrete goals through goal-setting interviews. By actively participating in these processes, the next of kin helped increase patients’ motivation and goal attainment. Their presence and support also helped create a more coherent and effective treatment plan. One of the data collectors expressed the importance of involving next of kin in this way:
Overall, it is very positive that the next of kin are more involved, and I think it is very good for the next of kin to be involved. (Data collector 2)
Conversations about goals also led to increased patient engagement and participation in the conversation. One of the staff noted that the PGSI is a useful tool and that goal setting increased patient engagement:
I think it was a really good mapping tool. We map the patients when they enter our services, and the PGSI provided a deeper level of mapping. I felt that the care improved when we gained more insights, and the patients became more engaged. It made the care feel less like just a standard offer from the municipality and more tailored to individual needs. Although we had known these patients for a few years before starting the project, we got to know them in a completely new way with this approach. (Staff 1)
Despite the initial goal discussion between health care staff, the next of kin and patients worked well and provided a good foundation for further goal attainment. PGSI contributed to a person-centred approach.
Conducting Goal Interviews with People Living at Home is Complex
The home care services were characterised by different cultures and resources, which affected how goal-setting interviews were conducted. One of the data collectors stated:
I really noticed the difference between the municipalities; they were not very far apart, but the culture was completely different. In one municipality, it was like: we can’t help with that, or we can’t contribute anything. In the other municipality, it was yes; of course, we will help with that; we can fix that. (Data collector 3)
Time constraints and resource limitations in home care services were the greatest obstacles to effective implementation. For the frailest patients, setting goals was particularly challenging, and quantifying goal attainment was also difficult. One of the patients described the obstacles in this way:
No – it’s a bit difficult to talk about goals when you’re as old as I am now. (Patient 1)
One of the next of kin illustrated obstacles such as time use and lack of resources in home care services in this way:
But you see that they [staff in home care services] are on pins and needles; they have to move on. They have so much to do that I feel sorry for them. I was driving behind a car from the home care service yesterday when we came from the doctor; she drove like she had stolen both the car and the petrol. (Next of kin of patient 2)
The PGSI is a Useful and Feasible Tool
PGSI was perceived as a structured conversation that made it easier for patients to express their wishes and needs while providing staff from home care services with a clear understanding of patients’ goals. As noted by one patient:
I think that there are a lot of people who have perceived it very well. A lot of them, both patients and the staff from the home care services, because they have got a different, a completely different attitude. (Patient 2)
Even though a few patients were unfamiliar with setting goals, they conveyed that they had achieved it with the help of their next of kin and home care services. The optimal effect was achieved when all parties involved worked together to formulate the goals. The questionnaire also proved to be particularly valuable for people with cognitive impairment or dementia, who seemed to benefit from a structured approach. Additionally, the simplicity and straightforwardness of PGSI were often noted by the staff, as conveyed in this statement:
That’s exactly what I thought, and it was very straightforward in a way; it (the PGSI) was easy to understand. Perhaps the simplest form of them all. (Staff 3)
This simplicity was perceived as particularly valuable for the tool’s effectiveness in providing a structured and easily comprehensible approach to goal setting.
The tool’s usability improved with experience for both the data collector and staff in home care services. As one staff member noted in the statement:
I found that the PGSI was very helpful after I used it a few times. As I became more familiar with it, I found it easier to use. (Staff 2)
This suggests that while initial implementation may be challenging, repeated use enhances its effectiveness, supporting the notion that PGSI becomes more accessible over time.
Content Validity of the PGSI
PGSI Reveals the Needs and Goals of Patients
The PGSI helps improve patient care through targeted communication and mapping. Using a goal-setting interview created more time for the service with the patient. Time was set aside to sit down and talk together, and the staff had the opportunity to get to know the patient more thoroughly. By focusing on conversations about what was important for the patient, the patient’s voice became stronger. This helped patients achieve goal attainment, which also provided better documentation about the patient’s wishes and needs. One of the patients in the study described the importance of identifying and taking care of needs in this way:
I think it’s useful in the way that they see that I have some needs that are not satisfied. So, I think that in the long run, they must be able to see that more measures are needed somewhere. (Patient 3)
The goal conversations changed both the patient’s and the service’s attitudes towards sitting down and talking together, and they also saw the benefits of these conversations. These conversations meant that the service, the next of kin, and the patient better understood the patient’s needs and could more quickly implement measures in unstable situations. Simple measures could bring about large changes, and through this process, the need for more help was often revealed. With the help of the goal conversation, the services obtained a better understanding of the patient’s needs and wishes and the value of prevention factors. This was expressed by one of the staff members in this way:
I think it was a very nice tool – what I’m left with is a bit of a different way of doing mapping – you may see slightly different things, and that you can take very simple measures that actually have a very big – make very big changes. A very small measure can mean a lot. Also, this value of prevention – it is much easier to prevent than to have to repair something that has gone wrong. (Staff 1)
Readiness to Change and Goal Attainment
The distribution of the PGSI score (scale from 0–10) for readiness to change (motivation) at baseline did not follow a normal distribution, with a median of 8 and a mean of 7.76 (SD 2.17), N= 123 (a drop-out rate of three patients due to missing data for two patients and errors in the measurement for the third patient. Missing data were excluded from the analyses). Readiness to change was therefore dichotomised into low and high scores, by using the median as cut-off value. A low readiness to change was defined as a score of 1–7 on the PGSI (n=48), whereas a high readiness to change was defined as a score of 8–10 (n=75).
After 12 weeks, participants with high motivation showed a statistically significant increase in PGSI compared with those with low motivation (p value = 0.010). An overview of these results is shown in Table 5.
 |
Table 5 Readiness to Change at Baseline and Change in Goal Attainment from Baseline at 12 weeks |
Interrater Reliability of the PGSI
The assessment of goal attainment of the PGSI was conducted separately by the patients and the next of kin as a dyad and by the staff from the home care services. At baseline, analyses revealed a strong positive correlation between the two groups (Figure 2). The strength of the correlation appears moderate to strong, as indicated by the distribution of points trending upwards across the scatter plot, with a Spearman correlation coefficient of 0.92 (p<0.001; n=113 patients). Analyses also revealed a strong positive correlation between the two groups at 12 weeks, with a Spearman correlation coefficient of 0.87 (p < 0.001; n=96 patients).
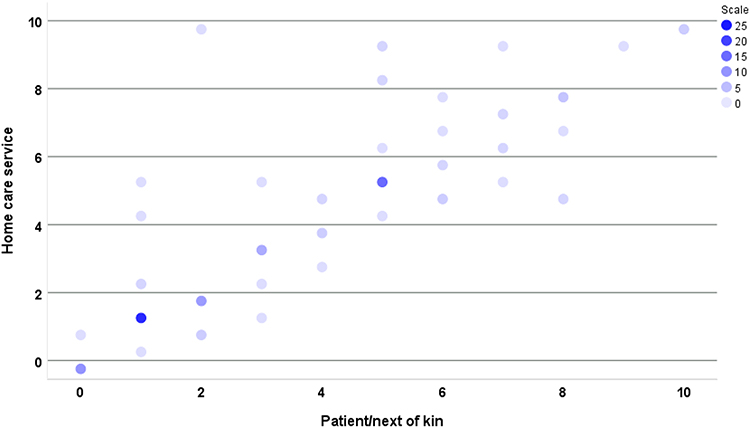 |
Figure 2 Correlations between PGSI goal attainment scores from patients/next of kin and home care service at baseline. Note: The varying colour intensity of the points, represented by the scale, represents the number of cases with these scores, with darker circles indicating more cases. At baseline, the Spearman correlation coefficient was 0.92 (p < 0.001; n = 113), and at 12 weeks 0.87 (p < 0.001; n = 96), indicating a strong positive correlation. |
With respect to the perception of goal attainment at baseline, there were no statistically significant differences between staff and the dyads patient/next of kin. Staff scored at the PGSI with a mean of 3.64 (SD 2.84) median=3 and 25th quartile=1 and 75th quartile=5, and the dyads scored at the PGSI with a mean of 3.47 (SD 2.68) with the same median and quartile scores as the staff. The Wilcoxon rank test was used because of non-normally distributed data, and the nonsignificant p value was 0.30, suggesting there is no statistically significant difference in perception between the dyad patients/next of kin and the staff for goal attainment.
Discussion
Substudy 1
The findings from substudy 1 demonstrate that the staff in home care services provided predominantly positive feedback on using a goal-setting interview. When new methods align with established routines, resistance can be reduced, and adaptation becomes easier. For new tools to be effective, they must be adapted to local conditions to ensure that they function well across different contexts and needs.5 The Norwegian Directorate of Health supports the need for practical and adapted frameworks in home care services.3 In substudy 1, goal conversations were conducted as natural dialogues, consistent with the service’s existing practices, but with added systematisation.
Our patient group for the BGSI was frailer and often exhibited multimorbidity compared with those in routine rehabilitation teams, where the BGSI has usually been tested.17 The increasing complexity of multimorbidity in the elderly underscores the need for effective goal-setting and individualised care strategies.8 While this can increase the usefulness of such tools, it may also affect feasibility when participants are frail and vulnerable.9 Adapting goals on the basis of the patient’s condition can lead to better goal attainment for frail and multimorbid individuals.6 Additionally, substudy 1 highlighted that time-consuming goal interviews posed a challenge on busy workdays, reflecting practical issues in the Norwegian health care system. Balancing time pressure with quality of care is essential, and the tool should be flexible enough to adapt to various organisational and practical conditions in home care services.5,6
The BGSI was considered effective in setting relevant and achievable goals, providing more targeted treatment tailored to the needs of participants.17 This finding is consistent with that of Tavemark et al,7 who reported that goal setting strengthens patient collaboration and follow-up. The findings of substudy 1 show that collaboration is key to achieving common goals and creating positive outcomes for all parties involved. However, findings from substudy 1 show that even though a lack of time and resources can challenge goal-setting collaboration, flexible tools, when adapted to the context, can improve collaboration and perceptions of services.5,7
The quality of the tool guide is crucial for the staff in home care services who use goal-setting interviews. Male et al24 emphasised that forms must be psychometrically valid, easy to understand, short, and adapted to both patients and health care personnel for effective use. The findings of substudy 1 led to a simplification of the guide for the PGSI, adapted from the BGSI, to a frailer and more heterogeneous population, making it more practical and easier to understand for home care services and patients. Clare et al17 reported that the BGSI was useful for setting realistic goals but that its effectiveness depends on proper implementation. Substudy 1 concludes that training, effective guidance, and support during implementation are necessary to maximise the feasibility and effectiveness of goal-setting interviews.
Substudy 2
Feasibility
The findings from the data in substudy 2 indicate that patients living at home set a wide range of goals (see Table 3). Their priorities, such as improving mobility and balance or participating in social activities, align with the goals described in other studies and national guidelines.2,3 Emphasis is placed on the importance of social participation and daily rehabilitation, which reflects a need to maintain a level of functioning, social attachment, and quality of life.5,7 This diversity in patient needs requires a flexible approach from healthcare professionals, who must have sufficient resources, time and expertise to manage and adapt to various objectives effectively.
Involving next of kin in goal-setting interviews increased patient engagement in our study. This finding is consistent with the findings in the literature, which emphasise the importance of the next of kin in patients’ goal setting.4 The participation of family members helps to strengthen the patient’s motivation and create a more coherent treatment plan, which is consistent with the recommendations in studies on patient and family involvement.6,16 If family members actively participate, this can improve the patient’s motivation and ensure continuity in follow-up. However, this can also challenge the feasibility of the PGSI if the next of kin are unavailable or cannot contribute to the extent needed.
The findings also revealed challenges related to resource and time constraints in home care services, which can affect the effectiveness of goal-setting interviews. This is similar to the literature highlighting that time constraints and a lack of resources are often barriers to home care services, as are the implementation of new assessment instruments in the healthcare system.6,7,22 Time constraints and a lack of resources in the healthcare system can significantly reduce the feasibility of goal-setting interviews, as these barriers often lead to rushed processes and inadequate adaptation of goals to the patient’s individual needs.5,6 This highlights the need for a realistic approach to what is possible to achieve within the existing framework. Cultural differences can also affect feasibility, as different care cultures may have different expectations of the care and follow-up of patients. Wild et al29 noted the importance of good practice in the cultural adaptation of patient reporting tools, which can contribute to increased feasibility.
PGSI appears to be a useful and feasible tool for goal setting, which is consistent with the literature showing that structured tools can improve both patients’ and healthcare professionals’ experience with goal setting.12,17,20 The simple and easy-to-understand approach of the PGSI makes it particularly useful for people with dementia or cognitive impairments, which is supported by previous research by Clare et al.17 Feasibility in this context depends on the ability of healthcare professionals to adapt to patients’ individual goals and needs, the availability of resources in home care services, and the effectiveness of tools such as the PGSI.
Content Validity of the PGSI
The content validity of the PGSI was supported by qualitative findings that show how the tool effectively uncovers patients’ diverse needs and goals. For example, one patient described how the PGSI helped shed light on needs that had not previously been met and emphasised the importance of preventive rather than restorative measures. These findings are consistent with the WHO’s framework for patient engagement, which highlights the importance of patients’ active participation in their own care.4 Furthermore, the findings reflect existing theories of ageing and multimorbidity, which emphasise the need for individualised care and preventive measures for older patients.8–10 By providing a structured approach to goal setting, the PGSI contributes to a more precise and holistic understanding of patient needs, which in turn can improve the quality of healthcare services. Focusing on patients’ goals through person-centred care and collaboration can improve health services and increase the quality of life of those who receive home care services.7
The results from substudy 2 demonstrate that having a high degree of readiness to change, as assessed in the PGSI, was associated with high goal attainment. These results confirm the validity of the PGSI as a useful tool for setting personal goals. Tavemark et al also suggested that patients who are actively engaged in the goal-setting process show greater readiness to change and adapt, which can lead to more successful attainment of goals.7 This is in line with findings from the GREAT study, in which Clare et al17 noted that individual goal setting can increase patients’ engagement in treatment. The INTERDEM manifesto written by Vernooij-Dassen et al19 highlighted the usefulness of having a person-centred focus in interventions. Furthermore, while they do not focus directly on setting specific goals, they do emphasise the need for a holistic approach by, for example, using a goal-setting interview such as the PGSI. The study by Tavemark et al7 highlighted the value that individual goal setting can lead to better goal attainment, as goals that are specific and personally relevant often motivate more and provide a clearer direction.
Interrater Reliability of the PGSI
Substudy 2 shows a high degree of interrater reliability in the assessments with the PGSI for goal attainment between the dyad of patients and next of kin and the staff members in the homecare services, with strong correlations for the measurements at baseline and 12 weeks in the PRACTIC RCT. This finding aligns with the findings of Budgett et al,22 who also reported high interrater reliability of goal-setting tools. One possible reason for the positive correlation between the assessments of patients/next of kin and home care services may be related to patient engagement. According to Genet et al,5 patient cooperation and participation in goal setting are essential for effective home care. When patients and the home care service agree on goals, this is reflected in reliable assessments. Tavemark et al7 confirmed that individual goal setting in municipal home care could promote a unified understanding of goals and expectations, contributing to high correlations in assessments of goal attainment. When both patients/next of kin and home care services report high goal attainment, PGSI effectively captures relevant information about goal attainment.
Strengths and Limitations
A strength of the study is the use of a mixed methods approach that combines quantitative and qualitative research methods. By using both methods together, we gained a deeper and more nuanced evaluation of the feasibility and the properties of the of the PGSI. A strength of substudy 1 was the continuous meetings between the first author (AV) and the staff in the home care services, which led to an in-depth follow-up of the participants and an iterative adaption of the goal-setting interview. In substudy 1, the sample is limited, as the purpose was to assess the feasibility of a simplified and modified version of an existing goal-setting interview, rather than to develop a new one. One strength of the substudy 2 was the heterogeneous group of participants, which provides a broader perspective and makes the findings more transferable to real world settings.
It should be noted that the transferability of the findings from substudy 1 is limited. The study was conducted in a Norwegian context with a small sample, and the findings therefore reflect specific organizational and cultural characteristics. The PGSI differs from traditional psychometric scales in that it is not designed to measure a wide range of psychometric properties in a standardised way. This is because goal-setting interviews are flexible tools for individual goal setting, and, therefore, there is often a lack of comprehensive quantitative data on such characteristics. A systematic review of goal-setting tools for people with dementia by Budgett et al22 confirmed that these tools have limited possibilities for measuring their psychometric properties. As noted by Budgett et al,22 interview-based goal-setting tools such as the BGSI tend to show moderate validity but limited reliability compared with more standardised measures (eg, GAS, COPM). Similarly, the PGSI is primarily a flexible, person-centred interview tool rather than a fully standardised psychometric scale, which limits direct comparison in terms of traditional psychometric robustness. However, our findings show that it is possible to investigate feasibility, content validity and interrater reliability, indicating the PGSI’s practical and research applicability despite the lack of traditional psychometric data.
Conclusions
Our study revealed that the newly developed PGSI was well received in home care services as a useful, systematic tool, despite some challenges with time use and a lack of resources. Improvements in the development of the PGSI from the original BGSI, such as simplifying the form and changes in the guide for the use of the PGSI, increased the tool’s usability. The PGSI is a feasible tool for individual goal setting in a heterogeneous patient population, improves patient engagement and goal attainment, and has high content validity and interrater reliability.
Implications for Practice and Research
Further research should investigate long-term effects, adaptation to different patient groups, implementation in practice, and possibly digitalisation of goal-setting interviews. In addition, future studies should explore how digital solutions can preserve patient engagement while improving efficiency and accessibility. Comparative research across different healthcare contexts will be important to assess whether the tool can be transferred beyond the Norwegian setting. Finally, cost-effectiveness and training requirements should be evaluated to ensure successful large-scale implementation.
Abbreviations
BGSI, Bangor Goal-Setting Interview; CFS, Clinical Frailty Scale; PGSI, PRACTIC Goal Setting Interview; PRACTIC, PReventing and Approaching Crises for frail community-dwelling patients Through Innovative Care; RCT, Randomised Controlled Trial; TIME, Targeted Interdisciplinary Model for Evaluation and Treatment of Neuropsychiatric Symptoms.
Data Sharing Statement
A list of the variables supporting the conclusions of this article are available on the website for the PRACTIC study (www.practic.no). The data collected in the study are not publicly available. Data are available upon reasonable request to the first author AV at the Research Centre for Age-related Functional Decline and Disease, Innlandet Hospital Trust (AFS).
The data are stored on a separate server for research at the Innlandet Hospital Trust. Only three of the researchers on the research team who analysed the data had access to these data.
Ethics Approval and Consent to Participate
The study was approved by the Data Protection Officer at Innlandet Hospital Trust in accordance with applicable ethical and data protection regulations (approval number: 23886962). The study has been conducted in accordance with the principles of the Declaration of Helsinki. In substudy 1, patients from home care services were not active study participants. Only the staff assessed the BGSI for these patients and participated in the meetings about the goal-setting form. Health information and other demographic details about the patients were not shared with the research group. In substudy 2, for the qualitative data, written consent to participate in the interviews was obtained from the data collectors, the staff in the home care services, the patients, and the next of kin. For patients with reduced or no capacity to consent to participate in the interviews, next-of-kin consented on behalf of the patient. A letter of consent with information about the study has been developed for patients, one for next of kin and one for the staff in home care services. In addition, a separate information letter has been developed for participants with a reduced capacity to consent. If a patient showed resistance to participate in an interview, the interview was not carried out, and the participant was withdrawn from the study. All participants provided informed consent prior to participation, and this consent included permission to publish anonymised responses and direct quotes. It is very unlikely that a participant could be injured due to participation in this study, as no new experimental treatments for patients were introduced to the participants. The researchers who conducted the interviews with the patient and next of kin were health personnel with experience from interview situations and from geriatric psychiatry. For the quantitative data, consent was previously collected in the RCT. This is described in a previously published article [26].
Consent for Publication
All participants consented to the publication of results from the study. The consent form for the dividual interviews with next of kin regarding participation is attached as Additional file 1. The consent form for the dividual interviews with patient regarding participation is attached as Additional file 2. The consent form for the focus group interviews with the staff members regarding participation is attached as Additional file 3. The consent form for the focus group interviews with the data collectors regarding participation is attached as Additional file 4.
Acknowledgments
We would like to thank all the patients, next of kin, staff members in homecare services and data collectors for their participation and cooperation in the study. We thank the staff at the Research Centre for Age-related Functional Decline and Disease, Innlandet Hospital Trust, for their support and valuable contributions throughout the study. We would also like to thank Bjørn Hoff, an external user contributor from the resource group of the PRACTIC study, for his collaboration. Hoff actively participated in the research process by providing valuable perspectives on the PGSI form and the qualitative findings of the study.
Author Contributions
BL is the principal investigator of the study. ØK, ETGD, JM, DH, and SB assisted with the preparation of the manuscript. AV and BL drafted the manuscript. All authors made a significant contribution to the study design, the acquisition of data, analysis and interpretation. All authors took part in drafting, revising, reviewing the article and gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted; and have agreed to be accountable for all aspects of the work. SB is responsible for data management.
Funding
The study is part of Anette Væringstad’s Ph.D. study, which is funded in total by a grant from the Innlandet Hospital Trust (project number: 150667).
Disclosure
The authors declare that they have no competing interests.
References
1. United Nations Department of Economic Social Affairs. World Population Ageing 2019. New York, NY: United Nations; 2020.
2. Suzman R, Beard J. Global health and aging; 2011. Available from: https://www.nia.nih.gov/sites/default/files/2017-06/global_health_aging.pdf.
3. Helsedirektoratet. En aldrende befolkning; 2023. Available from: https://www.helsedirektoratet.no/rapporter/folkehelse-i-et-livslopsperspektiv-helsedirektoratets-innspill-til-ny-folkehelsemelding/folkehelse-gjennom-livslopet-eldre/en-aldrende-befolkning#fotnoter.
4. World Health Organization. Patient engagement; 2016. Available from: https://iris.who.int/handle/10665/252269.
5. Genet N, Boerma W, Kroneman M, Hutchinson A, Saltman RB. Home Care Across Europe: Current Structure and Future Challenges. Geneva, Switzerland: World Health Organization and Regional Office for Europe; 2012.
6. Nylenna M. Helsetjenesten I Norge. Et Overblikk [Healthcare Services in Norway. An Overview]. Oslo, Norway: Gyldendal Akademisk; 2024.
7. Tavemark S, Kihlgren A, Norell Pejner M, James I. Individual goal-setting in municipal homecare: a participatory appreciative action and reflection study. J Public Health Res. 2023;12:22799036231181198. doi:10.1177/22799036231181198
8. Kingston A, Robinson L, Booth H, Knapp M, Jagger C; MODEM Project. Projections of multi-morbidity in the older population in England to 2035: estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing. 2018;47:374–380. doi:10.1093/ageing/afx201
9. Vetrano DL, Palmer K, Marengoni A, et al. Frailty and multimorbidity: a systematic review and meta-analysis. J Gerontol a Biol Sci Med Sci. 2019;74:659–666. doi:10.1093/gerona/gly110
10. Teo N, Yeo PS, Gao Q, et al. A bio-psycho-social approach for frailty amongst Singaporean Chinese community-dwelling older adults – evidence from the Singapore longitudinal aging study. BMC Geriatr. 2019;19:350. doi:10.1186/s12877-019-1367-9
11. Collard RM, Boter H, Schoevers RA, Voshaar RCO. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60:1487–1492. doi:10.1111/j.1532-5415.2012.04054.x
12. Travers J, Romero-Ortuno R, Bailey J, Cooney MT. Delaying and reversing frailty: a systematic review of primary care interventions. Br J Gen Pract. 2019;69:e61–9. doi:10.3399/bjgp18X700241
13. Kyrdalen IL, Strand BH, Selbæk G, et al. Prevalence and future estimates of frailty and pre-frailty in a population-based sample of people 70 years and older in Norway: the HUNT study. Aging Clin Exp Res. 2024;36:188. doi:10.1007/s40520-024-02839-y
14. Ledgerd R, Hoe J, Hoare Z, et al. Identifying the causes, prevention and management of crises in dementia. An online survey of stakeholders. Int J Geriatr Psychiatry. 2016;31:638–647.
15. Myhre J, Bergh S, Kirkevold Ø, Lichtwarck B. An organisation working mainly reactively instead of proactively: a qualitative study of how frail users of home care services and their next of kin experience crises. BMC Health Serv Res. 2024;24:1102.
16. Vroomen JM, Bosmans JE, van Hout HP, de Rooij SE. Reviewing the definition of crisis in dementia care. BMC Geriatr. 2013;13:10.
17. Clare L, Kudlicka A, Oyebode JR, et al. Goal-oriented cognitive rehabilitation for early-stage Alzheimer’s and related dementias: the GREAT RCT. Health Technol Assess. 2019;23:1–242.
18. Clare L, Kudlicka A, Oyebode JR, et al. Individual goal-oriented cognitive rehabilitation to improve everyday functioning for people with early-stage dementia: a multicentre randomised controlled trial (the GREAT trial). Int J Geriatr Psychiatry. 2019;34:709–721.
19. Vernooij-Dassen M, Moniz-Cook E, Verhey F, et al. Bridging the divide between biomedical and psychosocial approaches in dementia research: the 2019 INTERDEM manifesto. Aging Mental Health. 2019;25:206–212.
20. Clare L, Nelis SM, Kudlicka A. Bangor Goal-Setting Interview Manual. Exeter, United Kingdom: The University of Exeter; 2016.
21. Nordaunet OM, Gjevjon ER, Olsson C, Aagaard H, Borglin G. What about the fundamentals of nursing—its interventions and its continuity among older people in need of home- or facility-based care: a scoping review. BMC Nurs. 2024;23:59. doi:10.1186/s12912-023-01675-1
22. Budgett J, Sommerlad A, Kupeli N, Zabihi S, Olsen A, Cooper C. Setting individualised goals for people living with dementia and their family carers: a systematic review of goal-setting outcome measures and their psychometric properties. Dementia. 2024;23:312–340. doi:10.1177/14713012231222309
23. Hindle JV, Watermeyer TJ, Roberts J, et al. Goal-orientated cognitive rehabilitation for dementias associated with Parkinson’s disease―a pilot randomised controlled trial. Int J Geriatr Psychiatry. 2018;33:718–728. doi:10.1002/gps.4845
24. Male L, Noble A, Atkinson J, Marson T. Measuring patient experience: a systematic review to evaluate psychometric properties of patient reported experience measures (PREMs) for emergency care service provision. Int J Qual Health Care. 2017;29:314–326. doi:10.1093/intqhc/mzx027
25. Mokkink LB, Terwee CB, Knol DL, et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC Med Res Method. 2010;10:1–8. doi:10.1186/1471-2288-10-22
26. Væringstad A, Dalbak ETG, Holle D, et al. PReventing and Approaching Crises for frail community-dwelling patients Through Innovative Care (PRACTIC): protocol for an effectiveness cluster randomised controlled trial. Trials. 2024;25:304.
27. Lichtwarck B, Selbaek G, Kirkevold Ø, et al. Targeted interdisciplinary model for evaluation and treatment of neuropsychiatric symptoms: a cluster randomized controlled trial. Am J Geriatr Psychiatry. 2018;26:25–38. doi:10.1016/j.jagp.2017.05.015
28. Skivington K, Matthews L, Simpson SA, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess. 2021;25(57):1–132. doi:10.3310/hta25570
29. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8:94–104. doi:10.1111/j.1524-4733.2005.04054.x
30. Fenn J, Tan C-S, George S. Development, validation and translation of psychological tests. BJPsych Adv. 2020;26:306–315. doi:10.1192/bja.2020.33
31. Patton M. Designing qualitative studies. In: Patton M, editor. Qualitative Research and Evaluation Methods. United States of America: Sage Publications, Inc.; 2015:209–431.
32. Rockwood K, Theou O. Using the clinical frailty scale in allocating scarce health care resources. Can Geriatr J. 2020;23:210–215. doi:10.5770/cgj.23.463
33. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15:398–405. doi:10.1111/nhs.12048
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
35. Creswell JW, Clark VLP. Designing and Conducting Mixed Methods Research. Thousand Oaks, CA: Sage Publications; 2017.
36. Dalbak ETG, Væringstad A, Lichtwarck B, et al. Preventing and approaching crises for frail community-dwelling patients through innovative care (PRACTIC): study protocol for a process evaluation of a complex intervention in home care service. Trials. 2025;26:178. doi:10.1186/s13063-025-08876-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.