Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Development of an Evidence-Based and Theory-Informed Self-Management Intervention for People with Lipoedema: An Intervention Mapping Study
Authors Kloosterman LM ![]() , Hendrickx A
, Hendrickx A ![]() , Schneider F, Dekker R
, Schneider F, Dekker R ![]() , Jager-Wittenaar H
, Jager-Wittenaar H ![]() , Scafoglieri A
, Scafoglieri A ![]()
Received 23 April 2025
Accepted for publication 2 September 2025
Published 26 September 2025 Volume 2025:18 Pages 6151—6165
DOI https://doi.org/10.2147/JMDH.S536084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jagdish Khubchandani
Lise Maren Kloosterman,1– 4 Ad Hendrickx,1,3 Francine Schneider,5 Rienk Dekker,6 Harriët Jager-Wittenaar,1,2,4,7 Aldo Scafoglieri4,8
1Research Group Healthy Ageing, Allied Health Care and Nursing, Hanze University of Applied Sciences, Groningen, 9714 CA, the Netherlands; 2FAITH research, Groningen, 9714 CA, the Netherlands; 3Center of Expertise for Lymphovascular Medicine, Nij Smellinghe Hospital, Drachten, 9202 NN, the Netherlands; 4Experimental Anatomy Research Group, Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Physical Education and Physiotherapy, Vrije Universiteit Brussel, Jette, Brussels, 1090, Belgium; 5Department of Health Promotion, Care and Public Health Research Institute CAPHRI, Maastricht University, Maastricht, 6200 MD, the Netherlands; 6Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, Groningen, 9700 RB, the Netherlands; 7Department of Gastroenterology and Hepatology, Dietetics, Radboud university medical center, Nijmegen, HB, 6500, the Netherlands; 8Frailty in Aging Research Group, Faculty of Medicine and Pharmacy, Vrije Universiteit Brussel, Jette, Brussels, 1090, Belgium
Correspondence: Lise Maren Kloosterman, Research Group Healthy Ageing, Allied Health Care and Nursing, Hanze University of Applied Sciences, Groningen, 9714 CA, the Netherlands, Email [email protected]
Background: The etiology of lipoedema remains unclear, making diagnosis and treatment challenging. Current treatment primarily consists of general lifestyle recommendations, with effective self-management being essential for integrating these recommendations into daily life. However, no self-management interventions currently address the unique needs of people with lipoedema. This study aimed to develop an evidence-based, theory-informed intervention to enhance self-management in people with lipoedema using the Intervention Mapping (IM) approach.
Methods: Following the first four steps of the IM approach, this study used a participatory methodology involving stakeholders, empirical data, and theory. Steps included: 1) needs assessment; 2) identification of outcomes, performance objectives, and change objectives; 3) selection of behavioural change methods; and 4) development of program components.
Results: The resulting intervention includes a program for people with lipoedema and a training program for healthcare professionals (HCPs). The intervention aims to empower patients to engage in self-management and equip HCPs to provide effective support. Key determinants targeted include self-efficacy, self-regulation skills, knowledge, attitudes, and social facilitation. The program for people with lipoedema consists of seven themes aligned with self-management behaviours and is delivered through 19 sessions: seven one-on-one sessions, one session involving supportive individuals, and 11 group sessions. The program for HCPs is delivered through six group sessions, each focusing on the core skills HCPs need to effectively deliver self-management support to their patients.
Conclusion: The IM approach effectively guided a systematic, transparent, and reproducible development process. Grounded in established theories and behavioural change methods, the intervention provides a strong foundation for implementation and evaluation among people with lipoedema. The fifth and sixth steps of IM are considered future priorities.
Keywords: lipoedema, self-management, support, intervention mapping
Introduction
Lipoedema is a chronic condition that predominantly affects women, characterised by an abnormal, painful, and symmetrical accumulation of adipose tissue, primarily in the legs and sometimes in the arms.1,2 People with lipoedema commonly experience fatigue, heaviness in the affected limbs, psychological distress, physical limitations, and reduced physical capacity, all negatively impacting their functioning and quality of life.3–6 The exact etiology of lipoedema remains unclear, and the absence of a clear pathophysiological explanation complicates both diagnosis and treatment.7 Current treatment primarily consists of general lifestyle recommendations, such as weight management and maintaining an active lifestyle.1,8
Effective self-management is essential for incorporating lifestyle recommendations into daily life. The most recent guideline on lipoedema highlights the critical role of self-management in managing the condition.9 Self-management is defined as ‘an individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with a disorder’.10 A key factor in improving patient self-management is the provision of adequate self-management support by healthcare professionals (HCPs). Self-management support is ‘the systematic provision of education and supportive interventions by HPCs to increase patients’ skills and confidence in managing their health problems, including regular assessment of progress and problems, goal setting, and problem-solving support’.11
Self-management interventions for people with chronic conditions have shown positive results, including improved functioning, quality of life, health behaviours and communication with HCPs.12–14 While chronic conditions share challenges in managing the condition, condition-specific factors must also be addressed.13 A recent needs assessment among people with lipoedema identified several key requirements for people with lipoedema, including tailored lifestyle plans, progress monitoring, supportive networks, skill-building, and access to role models.15 However, no self-management interventions currently address the unique needs of people with lipoedema.
This study aimed to develop an evidence-based, theory-informed intervention to enhance self-management in people with lipoedema, using the Intervention Mapping (IM) approach. This intervention, delivered by an interprofessional team, aims to provide people with lipoedema and their HCPs with a structured, evidence- and theory-based framework to effectively enhance self-management and self-management support. This improvement is expected to lead to better functioning and, ultimately, an enhanced quality of life for people with lipoedema. Furthermore, this theoretically grounded development process lays a solid foundation for future empirical studies that address the critical gap in care for people with lipoedema.
Methods
This study adhered the steps and tasks of the IM approach, which was chosen for its systematic and stakeholder-driven methodology. IM enabled a predominantly participatory process that actively engaged relevant stakeholders, empirical data, and theory throughout the development of the intervention. IM is an iterative process for addressing complex problems, consisting of six steps designed to create a blueprint for developing, implementing, and evaluating interventions (Figure 1).16 Each step involves specific tasks that build on the previous one, with six core processes supporting task completion at every stage.17 This study included step 1 through 4 of IM. A glossary of used key terms is provided in Appendix I. All steps were led and coordinated by the first author. At the conclusion of each step, the results (eg, the Logic Model of the Problem or Change) were presented to the co-authors to achieve consensus. All participants in this study provided informed consent. The study was conducted between May 2024 and June 2025.
 |
Figure 1 The six steps, its tasks and core processes of the Intervention Mapping approach. Data from Eldredge et al, 201616 and Ruiter & Crutzen, 202017. |
The first step was to conduct a needs assessment (outlined in a previously published paper) to explore the needs, barriers, and facilitators of self-management, focusing on patients and HCPs.15 Determinants of self-management were identified through a narrative review and focus groups involving people with lipoedema and their HCPs. Subsequently, a planning group was formed using a purposive sampling approach, consisting of at least nine participants representing the following disciplines: physiotherapy, physician assistants, dietetics, nursing, dermatology, psychology, skin therapy, program development management, and patient advocacy. The same disciplines were represented at each meeting, ensuring continuity of expertise, although individual participants could vary. The purpose of establishing the planning group was to engage stakeholders in order to support well-informed decision-making and to ensure that these decisions were contextually appropriate and grounded in real-world practice. The findings from the needs assessment and subsequent planning group discussions informed the development of the Logic Model of the Problem, which identified the root causes of suboptimal self-management in people with lipoedema.16
In step two, the behavioural outcomes, performance objectives, and change objectives of the self-management intervention were identified. The targeted outcomes were further refined using the Theory of Self-Regulation, which emphasises key processes such as self-monitoring, recognizing patterns and triggers, and developing self-reflective and reactive capabilities.18 These elements enable individuals to regulate their responses, set goals, and adjust behaviours accordingly. Environmental outcomes for HCPs were based not only on the Theory of Self-Regulation but also on the Five A’s Model.19 This model includes five stages: assess, advise, agree, assist, and arrange. It is widely used to support behavioural change and improve health outcomes, self-management skills, self-efficacy, social support, and quality of life.20–24 Using the outlined behaviours, performance objectives were developed to specify the actions required by people with lipoedema and their HCPs to achieve the desired changes in self-management behaviours.16 Subsequently, change objectives were formulated by integrating the performance objectives with the identified determinants from the needs assessment and using the framework provided by the Individual and Family Self-Management Theory (IFSMT). The IFSMT offers a foundation for understanding and promoting self-management.25 These efforts resulted in a matrix of change objectives that showed how changes in determinants can lead to the achievement of performance objectives.16 This matrix guided the development of the Logic Model of Change, which identified the behavioural determinants for people with lipoedema and their HCPs, along with the corresponding performance objectives.
In step three, to achieve the change objectives, relevant behaviour change methods were selected from the taxonomy of behaviour change methods,16,26 based on previously conducted self-management intervention development studies,27–31 and a comprehensive study on behaviour change techniques and their mechanisms of action.32 Methods were selected when they directly addressed and affected the determinant. The selected behaviour change methods were translated into practical applications, informed by the needs assessment, theoretical frameworks and empirical research. Additionally, the selection process considered the feasibility of each method and incorporated insights from the planning group.
In step four, the program content for each intervention session was developed based on the change objectives and selected behaviour change methods. Additionally, the needs assessment and planning group contributed to the program’s development. At the end of the development phase, the authors, the planning group, and people with lipoedema were invited to review the content and provide feedback. Their input was used to enhance clarity, improve content, and refine the suitability and visuals of the program materials.
Results
Step 1 Needs Assessment
The needs assessment, as outlined in a previously published paper, identified a set of determinants that were presented to the planning group.15 Drawing on their expertise, the group categorised modifiable determinants as essential, optional, or unnecessary for inclusion in the intervention. This process led to the development of a Logic Model of the Problem (Figure 2). The identified determinants represent modifiable factors that are causally linked to self-management in people with lipoedema and their HCPs. These factors can be targeted through a self-management intervention to promote positive behaviour change.16 Additionally, the behaviours exhibited by people with lipoedema contribute to the risk of suboptimal self-management, which may result in functional impairments and reduced quality of life. The environmental factors refer to external conditions that directly or indirectly influence inadequate self-management.
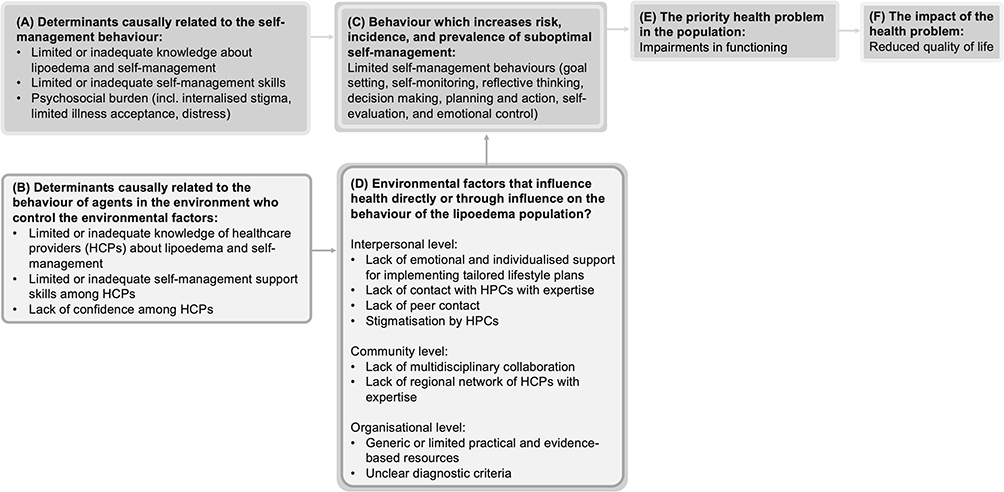 |
Figure 2 Logic Model of the Problem. (A) Determinants causally related to the self-management behaviour of people living with lipoedema; (B) determinants causally related to the self-management support provided by healthcare professionals (HCPs); (C) behaviours displayed by people with lipoedema that contribute to suboptimal self-management; (D) external conditions that directly or indirectly influence inadequate self-management of people with lipoedema; (E) impairments in functioning that represent the primary health problem for people with lipoedema; (F) the impact of impairments in functioning is a reduced quality of life. |
Step 2 Identification of Outcomes, Performance Objectives and Change Objectives
Outcomes and Determinants for Self-Management Behaviour
The intervention aims to empower people with lipoedema to actively engage in self-management behaviours such as goal setting, self-monitoring, reflective thinking, decision making, planning, taking action, self-evaluation, and emotional control.18,25 These skills collectively promote effective health management and help achieve desired outcomes and goals.33–38
The intervention targets the determinants of self-efficacy, self-regulation skills, knowledge about lipoedema and self-management, and attitude. Additionally, it addresses social facilitation, which refers to how relationships influence performance through support, cooperation, and social influence.39 The selection of determinants was based on the needs assessment, which highlighted that effective self-management requires adequate competencies, knowledge, and access to practical, evidence-based resources. Unhelpful attitudes towards self-management were identified as barriers, while supportive social networks and peer experience-sharing were key facilitators. HCPs emphasised the importance of addressing patients’ confidence and enhancing knowledge about the effects of personal behaviours and expectations. Research has emphasised the effectiveness of targeting these determinants to promote healthy behaviours25,40–45 and their positive associations with self-management behaviours.46–48
Outcomes and Determinants for Self-Management Support
The intervention aims to empower HCPs involved in the care of people with lipoedema to provide effective self-management support, enabling patients to successfully adopt and maintain self-management behaviours using the 5 A’s model.19
The key determinants for achieving environmental outcomes include knowledge, skills, and self-efficacy. The needs assessment among HCPs highlighted their need for these determinants, along with greater confidence in providing effective self-management support. Furthermore, a holistic understanding of their patients’ issues was identified as essential. Research has shown positive associations between self-efficacy and self-management support, with higher qualifications and greater experience among HCPs linked to improved outcomes.49,50 Although the direct impact of support skills on self-management has not been studied, their inclusion is informed by the needs assessment findings, as they likely play a critical role in translating knowledge and self-efficacy into effective interventions.
Performance, Change Objectives, and Logic Model of Change
The performance objectives developed to address the behavioural outcomes related to self-management, as detailed in the Logic Model of Change, are presented in Figure 3. The mapping of the selected determinants to the performance objectives, to create change objectives for the intervention are presented in Table 1 and Supplementary Tables 1 and 2.
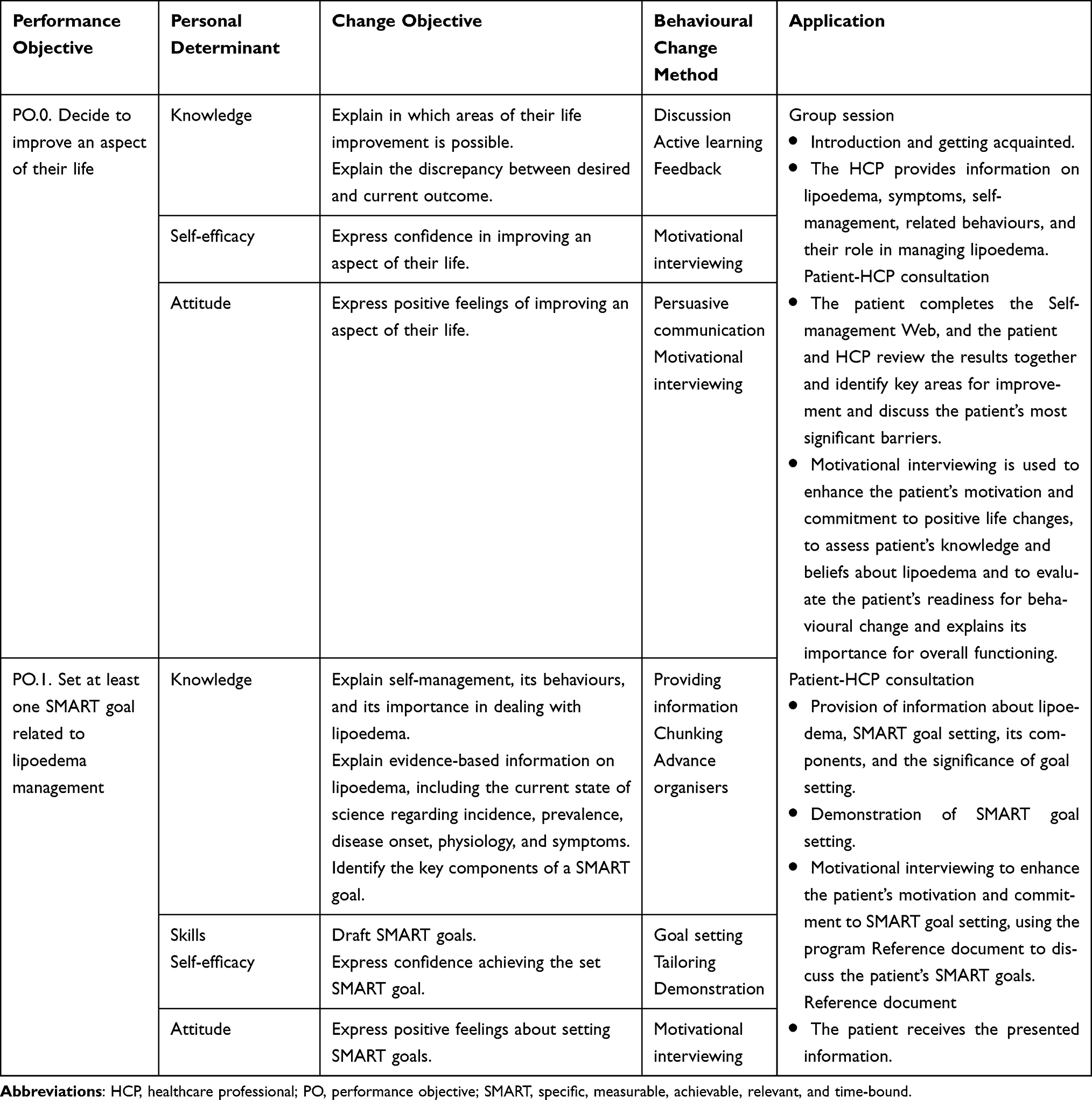 |
Table 1 Examples of Performance Objectives, Personal Determinants, Change Objectives, Behaviour Change Methods and Their Application for People with Lipoedema |
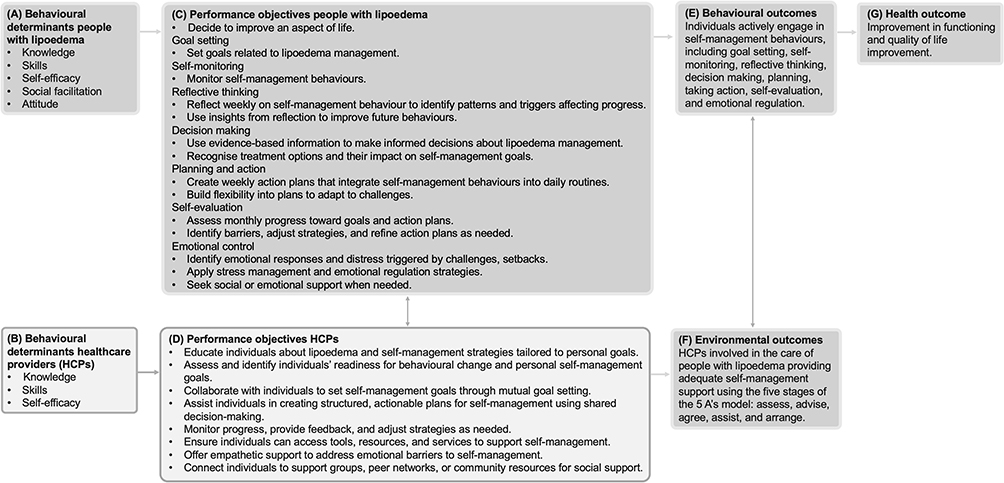 |
Figure 3 Logic Model of Change. (A) determinants causally related to the self-management behaviour of people living with lipoedema; (B) determinants causally related to the self-management support provided by healthcare professionals (HCPs); (C) performance objectives for people with lipoedema; (D) performance objectives for HCPs; (E) behavioural outcomes of the intervention; (F) environmental outcomes of the intervention; (G) health outcomes of the intervention. |
Step 3 Theory- and Evidence-Based Change Methods
Several behavioural change methods were selected to enhance knowledge as a determinant (Supplementary Tables 3 and 4). Firstly, discussion was included to aid information processing by prompting individuals to analyse the information, consider the pros and cons, and exchange their viewpoints with others.51 Secondly, active learning was employed as an interactive process that involves learners in exploring, processing, and applying information, fostering learning through goal-oriented experiences.16 Thirdly, chunking was selected to facilitate memory retention and recall by organizing smaller bits of information into larger, meaningful chunks, making retrieval and application easier.52 Fourthly, advance organisers was used to improve comprehension and knowledge retention by activating prior knowledge and providing a structured overview of the intervention’s content in a graphic format.53 Fifthly, feedback was given throughout the intervention by both peers and HCPs, assisting patients in evaluating their progress toward achieving their goals and adjusting their behaviour as needed. Sixthly, tailoring was selected as a behavioural change method to personalise information, skill-building activities, and self-efficacy training according to each patient’s unique needs and characteristics, thereby improving the intervention’s effectiveness.16 Furthermore, the needs assessment revealed that people with lipoedema emphasised the importance of tailored care and the need for informative, practical, and evidence-based resources.15
To enhance skills and self-efficacy, methods primarily rooted in theories of self-regulation were used, including guided practice, self-monitoring of behaviour, cue altering, goal setting, planning coping responses, and motivational interviewing.18 Demonstrations followed by guided practice were selected as behavioural change methods. A task is first demonstrated to individuals, followed by practicing and repeating the task under guidance, reinforcing learning through active engagement.16 Furthermore, self-monitoring of behaviour was used to encourage individuals to keep a record of their feelings or behaviours, helping them become more aware of their actions and influence their own behaviour.18 Goal setting was included to encourage individuals to plan specific actions with a clear definition of desired behaviours, while cue altering was chosen to help them adjust triggers of undesired behaviours, fostering the development of more positive behavioural patterns.16 Additionally, planning coping responses was selected to assist individuals in creating strategies to overcome potential obstacles, ensuring they are prepared for challenging situations.
Motivational interviewing was used as a behavioural change technique to explore and address patient ambivalence about self-management, while also improving skills and self-efficacy through patient-centered, collaborative, and goal-driven communication.54 Additionally, tailoring was selected to ensure that intervention components align with an individual’s characteristics, while individualisation was applied to allow participants to ask personal questions and receive instructions matched to their specific progress.16 The behavioural change method enhancing network linkages was used to improve social support. The need for a supportive network and the opportunity to share experiences with peers were identified as key facilitators for effective self-management.15 Furthermore, in the needs assessment, HCPs emphasised the importance of setting and planning small, achievable goals and steps, creating a personalised fallback plan, and ensuring understanding of information through follow-up to facilitate patient reflection.
To promote attitude change, persuasive communication and argumentation were used to help individuals develop a desired attitude by offering information and rationale to motivate specific behaviours.16 Additionally, motivational interviewing was used to reduce patient ambivalence regarding self-management, while belief selection helped individuals identify, strengthen, or weaken their current beliefs to facilitate positive behavioural change.16,54 Reinforcement was applied by connecting patients’ behaviours to their experienced consequences, while consciousness raising aimed to improve awareness and attitude by providing information, feedback, or confrontation about specific behaviours.16
Step 4 Producing Program Components
Program for People with Lipoedema
Several practical applications of behavioural change methods were implemented to target behavioural determinants (Supplementary Table 3). Knowledge transfer was primarily facilitated through patient-HCP consultations, a reference document containing relevant information that also serves as a diary, as well as group sessions and group discussions. To enhance skills, self-efficacy, and attitude, interactive group workshops and patient-HCP consultations were used. Social facilitation in patients was primarily addressed through groups discussion, but also included a session involving patients’ supportive individuals. Both one-on-one sessions and group sessions are part of the intervention as the needs assessment among people with lipoedema showed the need for tailored, individualised and emotional support as well as sharing experiences with peers.15 Components of the program are predominantly interactive.
The theme of the program for people with lipoedema is: “SELF-MANAGING your lipoedema”. This title reflects the self-management behaviours and determinants targeted in the intervention: self-efficacy, self-evaluation, and self-monitoring (SEL); social facilitation (F); making decisions (M); action planning (A); kNowledge (N); attitude (A); goal setting (G); skIlls (I); and reflective thinkiNG (NG). The program consists of seven program themes that align with seven self-management behaviours. It includes 19 sessions of approximately one hour each: seven one-on-one sessions, one session with supportive individuals, and 11 group sessions, organised into three phases (Figure 4). The program warm-up begins with a group session that includes introductions and getting acquainted. Patients are also informed about lipoedema and self-management. Additionally, a one-on-one consultation between the patient and HCP addresses the patient’s openness and readiness for self-management. The 19-session format was pragmatically derived from the IIM process, based on the scope and complexity of the identified needs, change objectives, and behavioural determinants. The Self-Management Web, a conversation tool developed to explore how people with chronic conditions manage self-management55 is used, as HCPs in the needs assessment emphasised the importance of ensuring that patients are receptive to self-management and can be effectively supported.15 The intervention then progresses to phase two, which consists of core program sessions covering themes such as emotional regulation, goal setting, self-monitoring, reflective thinking, decision making, planning and taking action, and self-evaluation. Each session follows a structured sequence: it begins with enhancing knowledge, followed by skills and self-efficacy training, and concludes with social facilitation. To further support people with lipoedema in adopting a healthy lifestyle, four interactive group workshops have been designed. These workshops focus on muscle strength and cardiovascular training, as well as the role of nutrition and nutritional status. The fourth workshop addresses the impact of self-image, illness acceptance, and stigma on self-management. This workshop was added to the intervention based on a prior study that identified patient acceptance and (perceived) stigma as important factors influencing functioning and effective self-management.4,15
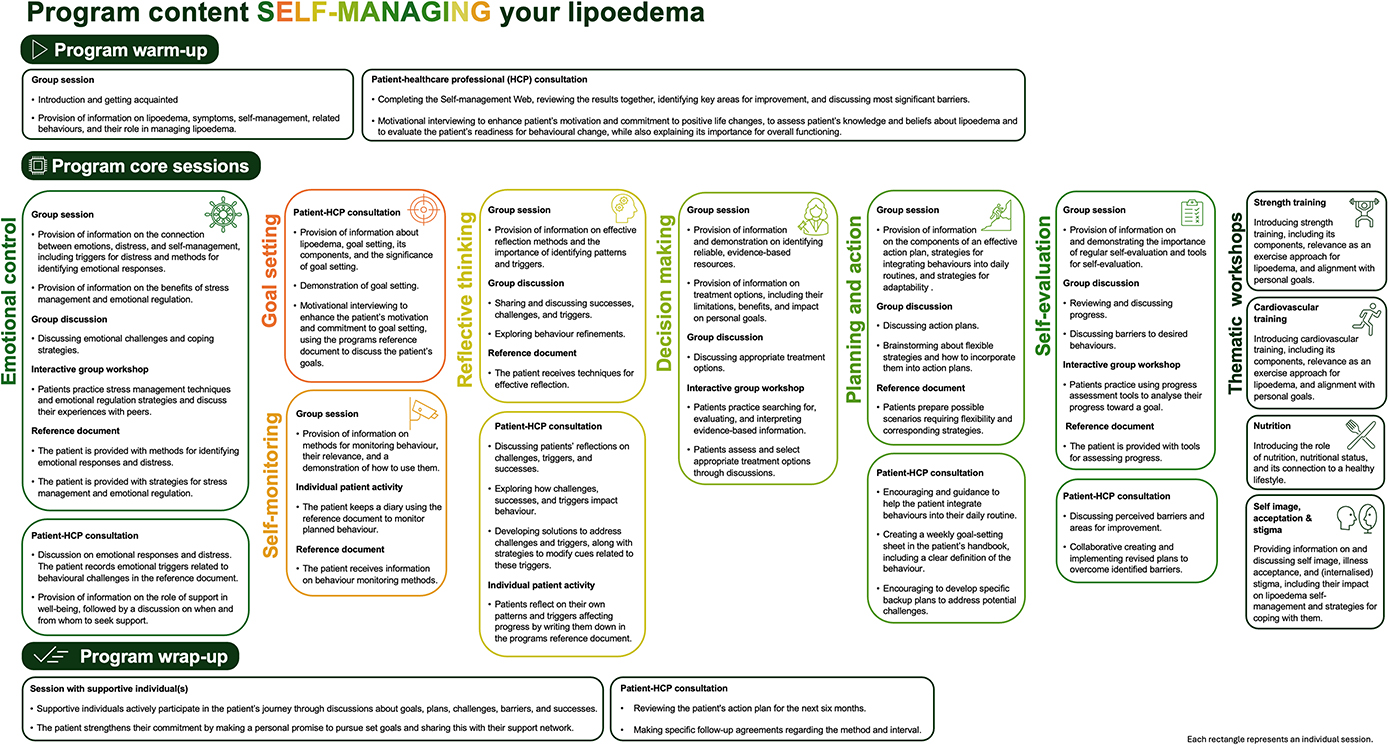 |
Figure 4 Program content “SELF-MANAGING your lipoedema”. |
Program for HCP
The HCP program consists of six group sessions, each lasting between one hour and one-and-a-half hours (Figure 5). Each session begins with a group session focused on providing information to enhance knowledge. In the second part, interactive workshops are used to develop skills and self-efficacy (Supplementary table 4).
 |
Figure 5 Program content for healthcare professional training. |
The program themes for HCP training are: assess, advise, agree, assist, and arrange, representing the core skills HCPs need to effectively support their patients in the self-management of lipoedema.19 HCPs begin by assessing a patient’s readiness for behavioural change, their knowledge, beliefs, and current behaviours. They also evaluate the patient’s progress and perception of how their behaviour relates to barriers, goal attainment, and other influencing factors. This stage helps HCPs develop a holistic understanding of patients’ challenges and encourages openness to education and self-management strategies which is important for adequate self-management support according to the needs assessment.15 It also enables HCPs to identify and address patient-related barriers for self-management support, such as low self-esteem, limited self-awareness of behaviours, and unrealistic expectations. The advise stage involves providing specific information about lipoedema, tailored self-management strategies, and the benefits of improving self-management.19 This aligns with the needs expressed by people with lipoedema, who emphasise the importance of gaining knowledge about both self-management and lipoedema.15 They also noted that experiencing tangible benefits from health-related behaviours would help them manage their condition more effectively. During this stage, HCPs provide personalised feedback based on questionnaire results and other assessments. The agree stage focuses on shared decision-making, where HCPs and patients collaboratively set behaviour change goals that align with the patient’s needs, priorities, and assessment outcomes. In the needs assessment, HCPs highlight active patient engagement under the guidance of an HCP as a key facilitator for self-management support. In the assist stage, HCPs help patients develop a structured, actionable self-management plan using a problem-solving approach. People with lipoedema have also highlighted the need for support in developing and implementing tailored lifestyle plans.15 HCPs acknowledge that setting small, achievable goals and taking incremental steps enhances the effectiveness of self-management support. Finally, the arrange stage involves jointly establishing a follow-up plan to monitor progress and ensure ongoing support. This aligns with the needs of people with lipoedema, who emphasise the importance of regular contact with HCPs for monitoring, guidance, and counselling.15
Discussion
This study describes the development of an evidence-based, theory-informed self-management intervention aimed at improving the functioning and quality of life of people with lipoedema. The first four steps of the IM methodology guided the process in a systematic, transparent, and reproducible manner. Grounded in widely accepted theories and incorporating proven behavioural change methods, the intervention provides a solid foundation for its implementation and evaluation.
Although this is the first study to describe the development of a lipoedema-specific intervention focused on enhancing self-management, the determinants targeted (ie, knowledge, skills, self-efficacy, and attitude) are commonly included in interventions aimed at improving self-management behaviour in individuals with chronic conditions.27–31 Differences between studies can be attributed to the use of the IM approach, which systematically guides developers to consider the end-users of an intervention in the needs assessment and involves end-user participation in the planning group.16,17 This results in variations in the needs addressed across different interventions.15 Additionally, the context in which interventions are delivered (eg, online vs face-to-face, or clinical vs non-clinical settings) influences the selection of feasible and modifiable determinants. Compared to previous studies, this is, to our knowledge, the first to incorporate specific programs targeting both people with lipoedema and HCPs to improve the support offered. The training program for HCPs, among other objectives, aims to enhance self-efficacy. Research has shown a positive association between self-efficacy and self-management support behaviour, suggesting that improving HCPs’ self-efficacy could enhance the overall effectiveness of the self-management intervention.49 Additionally, this study is one of the few to incorporate social facilitation, a component of the IFSMT, into the intervention, as research indicates that social facilitation is important for the successful self-management of chronic conditions.46
Strengths and Limitations
Firstly, this is the first study describing the development of a self-management intervention that considers the needs, barriers, and facilitators for self-management (support) of people with lipoedema and HCPs. This was achieved through a comprehensive needs assessment, incorporating a narrative review and focus groups.15 The needs assessment highlighted that people with lipoedema require tailored care and support, while HCPs emphasised the need for multidisciplinary teams. Key facilitators of self-management (support) include knowledge, skills, supportive networks, patient involvement, and setting achievable goals. Secondly, the participatory and iterative approach of the IM methodology ensured that the intervention not only aligns with the needs of people with lipoedema and their HCPs but also takes its feasibility into account. Frequent feedback from the planning group not only improved the feasibility of the intervention but also increased stakeholder acceptance of its practical application. Additionally, this member-checking process further enhanced the credibility of the study. Thirdly, the methodology used in this study is transparent, reproducible, and systematic, as it explicitly links behavioural change methods with performance and change objectives. Moreover, integrating various theoretical frameworks (ie, IFSMT, the Theory of Self-Regulation, Five A’s Model) further strengthened the scientific validity of the intervention.18,19,25 Finally, this study not only describes the intervention for people with lipoedema but also includes training for HCPs. This training is based on the needs assessment among HCPs and is designed to equip professionals with the skills to provide adequate self-management support to their patients. Furthermore, the dual patients-HCPs approach offers an innovative and transferable model for self-management support across chronic conditions.
This study also has some limitations that should be taken into account. Firstly, this study focuses only on steps 1 to 4 of IM. Steps 5 and 6, ie, implementation and evaluation, were not conducted, meaning that the effectiveness of the intervention has not yet been tested. However, the selection of proven and evidence-based methods from behavioural change science suggests that the intervention has good potential to be effective. Furthermore, the study makes a valuable contribution by addressing a critical gap in lipoedema care by providing a structured, theory-based intervention framework that lays the groundwork for future empirical research and practical application. Secondly, although the planning group and the iterative process of IM contributed to the continuous refinement of the intervention, feasibility or sustainability in the long term is not guaranteed. However, involving stakeholders throughout the development process is expected to reduce potential implementation barriers. Finally, although the IM approach is methodologically strong, proper implementation of the intervention is time-consuming and resource-intensive. The program consists of 19 patient sessions and requires HCPs to complete specific training. These requirements may present practical barriers in clinical settings. Furthermore, variations across healthcare systems may affect the feasibility of implementing the intervention as originally designed. This may pose challenges, especially in low-resource settings or healthcare systems with limited capacity. However, the transparency of the development process and the strong theoretical foundation of the intervention are intended to support flexible adaptation to diverse contexts. For example, implementers may tailor delivery methods, session formats, or intensity levels to fit local constraints, as long as the core components (eg, parameters for using behavioural change methods and the core sessions) are maintained. In addition, the intervention was designed with input from various stakeholders, which increases its relevance and cultural sensitivity. The training for HCPs, as described in this paper, is also expected to facilitate correct and efficient implementation across different settings.
Implications
The developed intervention has the potential to improve self-management behaviours in people with lipoedema by enhancing their knowledge, skills, self-efficacy, attitudes, and support. This is achieved through a tailored support program that combines one-on-one patient-HCP sessions with group sessions. HCPs play a crucial role in the intervention, and the training based on both Self-Regulation Theory and the Five A’s model provides them better insights into the challenges and needs of their patients, which could lead to more effective interventions.18,19 For the successful implementation of the intervention, it is essential for implementers to consider the parameters for using behavioural change methods.26 Additionally, while the core sessions of the intervention must be implemented correctly, implementers have flexibility in choosing the format of the intervention (such as the overall duration, intensity, pacing, session frequency and delivery methods). The holistic nature of the intervention is another key feature that should be incorporated into each setting. The intervention can be integrated into existing healthcare programs for people with lipoedema, such as primary care, rehabilitation centers, or specialised clinics. However, the training of HCPs is fundamental to the potential success of the intervention and should be provided to all professionals involved in the program.
Future research should focus on implementing the intervention and evaluating its long-term effectiveness in improving self-management behaviour, functioning, and quality of life among people with lipoedema. Ideally, this should be assessed using a randomised controlled trial or other appropriate designs, such as a single-case experimental design. Recommended outcome measures include the 36-Item Short Form Health Survey to assess quality of life and subjective functioning, and the Self-Management Web to evaluate self-management behaviour.56,57 Since establishing new behaviours as habits takes time, with an average of 66 days but a range from 18 to 254 days depending on the behaviour’s complexity and consistency, an appropriate follow-up period (eg, at three, six, and twelve months) should be adopted.58 Additionally, the impact of HCP training on patient outcomes should be investigated. Furthermore, the intervention should be evaluated qualitatively by interviewing both people with lipoedema and the HCPs involved in their care to assess its feasibility, acceptability, and perceived impact. Exploring the integration of eHealth components in future iterations could improve accessibility, scalability, and support more flexible delivery of the intervention.
Conclusion
This study described the development of an evidence-based and theory-informed self-management intervention aimed at improving the functioning and quality of life of people with lipoedema. The first four steps of the IM methodology guided the process in a systematic, transparent, and reproducible manner. Grounded in widely accepted theories and incorporating proven behavioural change methods, the intervention provides a theoretically grounded framework for its implementation and evaluation. The dual patients-HCPs approach offers an innovative and transferable model for self-management support across chronic conditions. Future research should focus on implementing the intervention and evaluating its effectiveness and feasibility in people with lipoedema considering self-management behaviour, functioning, and quality of life, using rigorous study designs, appropriate outcome measures, and suitable follow-up periods.
Ethics Approval and Consent to Participate
The study was conducted according to the principles of the Declaration of Helsinki.59 Recruitment and data collection started subject to approval of the study by the Hanze Ethics Advisory Committee (approval number: heac.T2024.026) and Nij Smellinghe hospital’s local feasibility committee (reference: 26906/JB/AB).
Acknowledgments
We thank all participants who took part in this study.
Funding
This research was funded by Hanze University of Applied Sciences, Groningen, The Netherlands and the Center of Expertise for Lymphovascular Medicine, Nij Smellinghe Hospital, Drachten, The Netherlands.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Halk AB, Damstra RJ. First Dutch guidelines on lipedema using the international classification of functioning, disability and health. Phlebology. 2017;32(3):152–159. doi:10.1177/0268355516639421
2. Wold LE, Hines EA, Allen EV. Lipedema of the legs; a syndrome characterized by fat legs and edema. Ann Intern Med. 1951;34(5):1243. doi:10.7326/0003-4819-34-5-1243
3. Dudek JE, Białaszek W, Ostaszewski P. Quality of life in women with lipoedema: a contextual behavioral approach. Qual Life Res. 2016;25(2):401–408. doi:10.1007/s11136-015-1080-x
4. Kloosterman LM, Eilers R, Scafoglieri A, Hendrickx A, Dekker R, Jager-Wittenaar H. More than meets the eye: phenomenological insights into the functioning of people with lipoedema. Int J Qual Stud Health Well-Being. 2025;20(1):2463157. doi:10.1080/17482631.2025.2463157
5. Kloosterman LM, Hendrickx A, Scafoglieri A, Jager-Wittenaar H, Dekker R. Functioning of people with lipoedema according to all domains of the international classification of functioning, disability and health: a scoping review. IJERPH. 2023;20(3):1989. doi:10.3390/ijerph20031989
6. van Esch-Smeenge J, Damstra RJ, Hendrickx AA. Muscle strength and functional exercise capacity in patients with lipoedema and obesity: a comparative study. J Lymphoedema. 2017;12(1):5.
7. Bertsch T, Erbacher G, Elwell R, Partsch H. Lipoedema: a paradigm shift and consensus. J Wound Care. 2020;29(11):1–52. doi:10.12968/jowc.2020.29.Sup11b.1
8. Amato ACM, Peclat APRM, Kikuchi R, et al. Brazilian consensus statement on lipedema using the delphi methodology. J Vasc Bras. 2025;24:e20230183.
9. Faerber G, Cornely M, Daubert C, et al. S2k guideline lipedema. J Deutsche Derma Gesell. 2024;22(9):1303–1315.
10. Barlow J. How to use education as an intervention in osteoarthritis. Best Pract Res. 2001;15(4):545–558. doi:10.1053/berh.2001.0172
11. Institute of Medicine (US). Committee on identifying priority areas for quality improvement. priority areas for national action: Transforming Health Care Quality [Internet]. Washington, D.C.: National Academies Press; 2003 [cited January 17, 2025]. Available from: http://www.nap.edu/catalog/10593.
12. Cramm JM, Hartgerink JM, Steyerberg EW, Bakker TJ, Mackenbach JP, Nieboer AP. Understanding older patients’ self-management abilities: functional loss, self-management, and well-being. Qual Life Res. 2013;22(1):85–92. doi:10.1007/s11136-012-0131-9
13. Lorig KR, Holman HR. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
14. Musekamp G, Bengel J, Schuler M, Faller H. Improved self-management skills predict improvements in quality of life and depression in patients with chronic disorders. Patient Educ Couns. 2016;99(8):1355–1361. doi:10.1016/j.pec.2016.03.022
15. Kloosterman LM, Jager-Wittenaar H, Schneider F, Hendrickx A, Dekker R, Scafoglieri A. Comprehensive needs assessment for enhancing self-management in people with lipoedema and the support provided by their healthcare professionals. JMDH. 2025;18:1217–1230. doi:10.2147/JMDH.S508816
16. Eldredge LKB, Markham CM, Ruiter RA, Fernández ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. John Wiley & Sons.; 2016.
17. Ruiter RAC, Crutzen R. Core processes: how to use evidence, theories, and research in planning behavior change interventions. Front Public Health. 2020;8:247. doi:10.3389/fpubh.2020.00247
18. Bandura A. Social cognitive theory of self-regulation. Organizational Beha Human Decis Processes. 1991;50(2):248–287. doi:10.1016/0749-5978(91)90022-L
19. Glasgow RE, Davis CL, Funnell MM, Beck A. Implementing practical interventions to support chronic illness self-management. Jt Comm J Qual Saf Jt Comm J Qual Patient Saf. 2003;29(11):563–574. doi:10.1016/S1549-3741(03)29067-5
20. Keivan S, Shariati A, Miladinia M, Haghighizadeh MH. Role of self-management program based on 5A nursing model in quality of life among patients undergoing hemodialysis: a randomized clinical trial. BMC Nephrol. 2023;24(1):58. doi:10.1186/s12882-023-03108-2
21. Mirian Z, AbdiShahshahani M, Noroozi M, Mostafavi F, Beigi M. Effect of intervention based on the 5A self-management model on the improvement of behaviors related to women’s reproductive health after legal abortion. Sci Rep. 2023;13(1):11316. doi:10.1038/s41598-023-38521-y
22. Moosavimoghadam SF, Dehghani A, Akbar RE. The effect of 5A self-management program on medication adherence of epileptic patients during the COVID - 19 pandemic: a randomized controlled trial. Acta Neurol Taiwan. 2024;33(4):165–174. doi:10.4103/ANT.33-4_112_0072
23. Moradi M, Nasiri M, Jahanshahi M, Hajiahmadi M. The effects of a self-management program based on the 5 A’s model on self-efficacy among older men with hypertension. Nurs Midwifery Stud. 2019;8(1):21. doi:10.4103/nms.nms_97_17
24. Shojaee D, Mohammadi Shahboulaghi F, Fallahi-Khoshknab M, Vahedi M, Bakhtiari A, Zabolypour S. Effect of a 5A model-based self-management program on self-management ability and dyspnea severity in the elderly with chronic heart failure: a randomized clinical trial. Salmand. 2024;18(04):488–501. doi:10.32598/sija.2023.3512.1
25. Ryan P, Sawin KJ. The individual and family self-management theory: background and perspectives on context, process, and outcomes. Nurs Outlook. 2009;57(4):217–225.e6. doi:10.1016/j.outlook.2008.10.004
26. Kok G, Gottlieb NH, Peters GJY, et al. A taxonomy of behaviour change methods: an intervention mapping approach. Health Psychol Rev. 2016;10(3):297–312. doi:10.1080/17437199.2015.1077155
27. Detaille SI, Van Der Gulden JW, Engels JA, Heerkens YF, Van Dijk FJ. Using intervention mapping (IM) to develop a self-management programme for employees with a chronic disease in the Netherlands. BMC Public Health. 2010;10(1):353. doi:10.1186/1471-2458-10-353
28. Hurley DA, Murphy LC, Hayes D, et al. Using intervention mapping to develop a theory-driven, group-based complex intervention to support self-management of osteoarthritis and low back pain (SOLAS). Implementation Sci. 2015;11(1):56. doi:10.1186/s13012-016-0418-2
29. Janssen AM, Dam J, Prins J, Buffart LM, De Bruin M. Systematic adaptation of the adherence improving self‐management strategy to support breast cancer survivors’ adherence to adjuvant endocrine therapy: an intervention mapping approach. European J Cancer Care. 2022;31(6).
30. Shegog R, Begley CE. Clinic-based mobile health decision support to enhance adult epilepsy self-management: an intervention mapping approach. Front Public Health. 2017;5:256. doi:10.3389/fpubh.2017.00256
31. Zuidema RM, van Gaal BG, van Dulmen S, Repping-Wuts H, Schoonhoven L. An online tailored self-management program for patients with rheumatoid arthritis: a developmental study. JMIR Res Protoc. 2015;4(4):e140. doi:10.2196/resprot.4571
32. Carey RN, Connell LE, Johnston M, et al. Behavior change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med. 2019;53(8):693–707.
33. Epton T, Currie S, Armitage CJ. Unique effects of setting goals on behavior change: systematic review and meta-analysis. J Consult Clin Psychol. 2017;85(12):1182–1198. doi:10.1037/ccp0000260
34. Howell D, Harth T, Brown J, Bennett C, Boyko S. Self-management education interventions for patients with cancer: a systematic review. Support Care Cancer. 2017;25(4):1323–1355. doi:10.1007/s00520-016-3500-z
35. Kassavou A, Wang M, Mirzaei V, Shpendi S, Hasan R. The association between smartphone app–based self-monitoring of hypertension-related behaviors and reductions in high blood pressure: systematic review and meta-analysis. JMIR mHealth uHealth. 2022;10(7):e34767. doi:10.2196/34767
36. Liao Y, Gao G, Peng Y. The effect of goal setting in asthma self-management education: a systematic review. Int J Nurs Sci. 2019;6(3):334–342. doi:10.1016/j.ijnss.2019.04.003
37. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4(6):256–262.
38. McBain H, Shipley M, Newman S. The impact of self-monitoring in chronic illness on healthcare utilisation: a systematic review of reviews. BMC Health Serv Res. 2015;15(1):565. doi:10.1186/s12913-015-1221-5
39. Zajonc RB. Social Facilitation: a solution is suggested for an old unresolved social psychological problem. Science. 1965;149(3681):269–274. doi:10.1126/science.149.3681.269
40. Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health. 2013;103(5):813–821. doi:10.2105/AJPH.2012.301069
41. Hennessy EA, Johnson BT, Acabchuk RL, McCloskey K, Stewart-James J. Self-regulation mechanisms in health behavior change: a systematic meta-review of meta-analyses, 2006–2017. Health Psychol Rev. 2020;14(1):6–42. doi:10.1080/17437199.2019.1679654
42. Janssen V, Gucht VD, Dusseldorp E, Maes S. Lifestyle modification programmes for patients with coronary heart disease: a systematic review and meta-analysis of randomized controlled trials. Eur J Prev Cardiolog. 2013;20(4):620–640. doi:10.1177/2047487312462824
43. Kwan YH, Cheng TY, Yoon S, et al. A systematic review of nudge theories and strategies used to influence adult health behaviour and outcome in diabetes management. Diabetes Metabolism. 2020;46(6):450–460. doi:10.1016/j.diabet.2020.04.002
44. Ruddock HK, Brunstrom JM, Vartanian LR, Higgs S. A systematic review and meta-analysis of the social facilitation of eating. Am J Clin Nutr. 2019;110(4):842–861. doi:10.1093/ajcn/nqz155
45. Sheeran P, Maki A, Montanaro E, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. 2016;35(11):1178–1188. doi:10.1037/hea0000387
46. Alexandre K, Campbell J, Bugnon M, et al. Factors influencing diabetes self-management in adults: an umbrella review of systematic reviews. JBI Evidence Synth. 2021;19(5):1003–1118. doi:10.11124/JBIES-20-00020
47. Breland JY, Wong JJ, McAndrew LM. Are Common Sense Model constructs and self-efficacy simultaneously correlated with self-management behaviors and health outcomes: a systematic review. Health Psychol Open. 2020;7(1):2055102919898846. doi:10.1177/2055102919898846
48. Heisler M. Overview of peer support models to improve diabetes self-management and clinical outcomes. Diabetes Spectr. 2007;20(4):214–221. doi:10.2337/diaspect.20.4.214
49. Arslan M, Van Dongen SI, Witkamp E, et al. Nurse practitioners’ self-efficacy and behavior in supporting self-management of patients with a progressive, life-threatening illness and their relatives: a nationwide, cross-sectional online survey. J Hosp Palliat Nurs. 2022;24(4):E126–34. doi:10.1097/NJH.0000000000000863
50. Landu ZK, Crowley T. Primary health care nurses’ knowledge, self-efficacy and performance of diabetes self-management support. African J Primary Health Care Family Med. 2023;15(1). doi:10.4102/phcfm.v15i1.3713
51. Petty RE, Barden J, Wheeler SC. The elaboration likelihood model of persuasion: developing health promotions for sustained behavioral change. In: Emerging Theories in Health Promotion Practice and Research 2. 2009;185–214.
52. Bodie GD, Powers WG, Fitch-Hauser M. Chunking, priming and active learning: toward an innovative and blended approach to teaching communication-related skills. Interactive Learning Environ. 2006;14(2):119–135. doi:10.1080/10494820600800182
53. Kools M, Van De Wiel MWJ, Ruiter RAC, Crüts A, Kok G. The effect of graphic organizers on subjective and objective comprehension of a health education text. Health Educ Behav. 2006;33(6):760–772. doi:10.1177/1090198106288950
54. Song D, Xu TZ, Sun QH. Effect of motivational interviewing on self-management in patients with type 2 diabetes mellitus: a meta-analysis. Int J Nurs Sci. 2014;1(3):291–297. doi:10.1016/j.ijnss.2014.06.002
55. Van Staa AL, Beck D, Been-Dahmen JMJ, Massey EK. Ondersteuning bij zelfmanagement: een nieuwe verpleegkundige interventie. Dé Verpleegkundig Specialist. 2017;12(1):8–14.
56. Angst F, Lehmann S, Aeschlimann A, Sandòr PS, Wagner S. Cross-sectional validity and specificity of comprehensive measurement in lymphedema and lipedema of the lower extremity: a comparison of five outcome instruments. Health Qual Life Outcomes. 2020;18(1):. doi:10.1186/s12955-020-01488-9
57. Zorg voor Beter. 2018 [cited February 26, 2025]. Zelfmanagement Web. Available from: https://www.zorgvoorbeter.nl/tips-tools/tools/zelfmanagement-web.
58. Lally P, Van Jaarsveld CHM, Potts HWW, Wardle J. How are habits formed: modelling habit formation in the real world. Euro J Social Psych. 2010;40(6):998–1009. doi:10.1002/ejsp.674
59. World Medical Association. 2022 [cited March 23, 2023]. Wma declaration of helsinki – ethical principles for medical research involving human subjects. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Needs Assessment for Enhancing Self-Management in People with Lipoedema and the Support Provided by Their Healthcare Professionals
Kloosterman LM, Jager-Wittenaar H, Schneider F, Hendrickx A, Dekker R, Scafoglieri A
Journal of Multidisciplinary Healthcare 2025, 18:1217-1230
Published Date: 27 February 2025