Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Development of an Early Activation Hip Fracture Care Bundle and Implementation Strategy to Improve Adherence to the National Hip Fracture Clinical Care Standard
Authors Curtis K, Moules P, McKenzie J, Weidl L, Selak T ![]() , Binks S, Hernandez D, Rijsdijk J, Risi D, Wright J, O'Rourke L, Knapman M, Ristevski M, Stephens T, Harris I, Close JCT
, Binks S, Hernandez D, Rijsdijk J, Risi D, Wright J, O'Rourke L, Knapman M, Ristevski M, Stephens T, Harris I, Close JCT
Received 18 June 2021
Accepted for publication 27 September 2021
Published 14 October 2021 Volume 2021:14 Pages 2891—2903
DOI https://doi.org/10.2147/JMDH.S323678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of "eHIP to improve adherence to ACSQHC standards" [ID 323678].
Views: 147
Kate Curtis,1– 4 Peter Moules,2 John McKenzie,2,3 Lauren Weidl,2 Tanya Selak,2 Simon Binks,2 Daniel Hernandez,2 Joshua Rijsdijk,2 Dante Risi,2 James Wright,5 Lauren O’Rourke,2 Myles Knapman,6 Meagan Ristevski,2 Teala Stephens,2 Ian Harris,7 Jacqueline CT Close8,9
1Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia; 2Illawarra Shoalhaven LHD, Emergency Department, Wollongong, NSW, Australia; 3Illawarra Health and Medical Research Institute, Wollongong, NSW, Australia; 4George Institute for Global Health, Newtown, NSW, Australia; 5Agency for Clinical Innovation, St Leonards, NSW, Australia; 6Western NSW LHD, Department of Surgery, Dubbo, NSW, Australia; 7Ingham Institute of Applied Medical Research, South Western Sydney Clinical School, UNSW, Sydney, NSW, Australia; 8Prince Wales Clinical School, UNSW, Sydney, NSW, Australia; 9Neuroscience Research Australia, UNSW, Sydney, NSW, Australia
Correspondence: Kate Curtis Email [email protected]
Objective: To develop and implement a multidisciplinary early activation mechanism and bundle of care (eHIP) to improve adherence to ACSQHC standards in a regional trauma centre.
Methods: Barriers to implementation were categorised using the Theoretical Domains Framework, then linked to specific strategies guided by the Behaviour Change Wheel and Behaviour Change Technique Taxonomy (BCTT). The resulting implementation strategies were assessed using Affordable, Practical, Effective, Acceptable, had Side-effects (APEASE) criteria.
Results: Eighty-three barriers to implementation of the hip fracture care bundle were identified. The behaviour change wheel process resulted in the identification of 41 techniques to address these barriers. The predominant mechanisms to achieve this were development and implementation of 1) formal policy that outlines eHIP roles; 2) video promotion; 3) pager group; 4) fascia iliaca block enabling; 5) eMR modifications; 6) face-to-face reinforcement and modelling; 7) communication and prompts; 8) environmental restructuring.
Conclusion: We applied behaviour change theory through a pragmatic evidence-based process. This resulted in a codesigned strategy to overcome staff and organisational barriers to the implementation of a multidisciplinary early activation mechanism and bundle of care (eHIP). Future work will include evaluation of the uptake and clinical impact of the care bundle.
Keywords: hip fracture, implementation, clinical pathway, emergency, behaviour change, injury, older persons, orthopaedic
Introduction
Hip fracture is the most serious and costly fall-related injury suffered by frail older people and numbers are on the rise. The human cost of a hip fracture is high;1 25% of patients are dead at one year, 50% do not regain their previous level of function, and for 11% of patients, the fracture heralds the end of independent living.2,3 Hip fractures are one of the top three causes of emergency admissions involving surgery in Australia,4 with nearly 17,000 treated in Australian hospitals each year at a cost of nearly AU$1Billion.5 An acute hip fracture results in pain, bleeding and immobility. These factors initiate inflammatory, hypercoagulable, catabolic and stress states that precipitate complications.6
Several countries have national guidelines and monitoring of outcomes for Hip Fracture management.7–10 In Australia, the Australian Commission on Safety and Quality in Health Care (ACSQHC) produced the Hip Fracture Care Clinical Care Standard in 2016,11 consolidating the best available evidence for managing this patient group. However, there is mounting evidence of variation in the quality and safety of care of patients with hip fractures across jurisdictions and hospitals in Australia including a large amount of variation in mortality that may be explained by different approaches to delivery of care12 For example, 61% of Australian patients and 58% of New Zealand patients with hip fractures underwent pain assessment within 30 minutes of ED arrival;12 79% of Australian patients and 67% of New Zealand patients received the gold standard femoral nerve block; 80% of Australian patients and 84% of New Zealand patients received operative intervention within 48 hours; and only 26% of Australian patients and 23% of New Zealand patients were routinely provided individualised written information on prevention of future falls and fractures. These variances are reflected around the globe7,13–18
Healthcare organizations are complex social entities.19 There is a need for effective and sustainable interventions to support sustained Hip Fracture guideline uptake,12 in particular, to ensure staff have the capability, opportunity and motivation to comply. Numerous studies have implemented best practice pathways, some demonstrating no improvement to patient outcomes7 and their uptake poor. Despite this, most published intervention studies have led to some improved outcomes for patients in targeted areas. For example, the “Hip Attack” model which, through early medical clearance, reduced time to operative intervention and post-operative complications,6 including a significant reduction in the incidence of delirium, as did that of Chuan et al.13 The implementation of a hip fracture coordination service in Israel resulted in improved osteoporotic medical treatment9 The majority of the guideline implementation evaluation reports do not comment in detail in the design and method of implementation of the pathways, compliance or uptake. Further, evidence-based clinician enabling strategies that activate the necessary referrals and care throughout the entire course of hip fracture care are required.
To improve compliance with the ACSQHC Hip Fracture Care Clinical Care Standard in our hospital, in October 2018, the Wollongong Hospital hip fracture committee designed eHIP – a multidisciplinary early activation mechanism and bundle of care. This paper describes the development and implementation of eHIP.
Methods
This project was conducted at Wollongong Hospital (WH), which manages around 350 patients with hip fractures annually. WH is consistently one of the worst performing hospitals in Australia and New Zealand for emergency department (ED) length of stay (LOS)12,20,21 and had previously been among the worst performing regarding time to hip fracture surgery.20,21 The process of developing of eHIP for effective implementation and maximum uptake is described, followed by the steps taken to develop an implementation plan using behaviour change theory. As this is a description of the development of an intervention, rather than an evaluation of an intervention, no ethical approval was required.
Behaviour Change Theory
The implementation plan for eHIP focuses on clinician behaviour change, with particular consideration to organisational barriers to change. Although healthcare disciplines share the same goal of improving patient outcomes, they often have differing priorities, roles, and expectations about how care should be delivered.22 Central to sustained compliance with any intervention is individual and collective human behaviour.22 As such, part of the implementation plan development, a behavioural analysis was conducted at the study sites that considered all disciplines using the following steps recommended by French et al which are known to be effective, practical and pragmatic:23 1. Who needs to do what, differently? 2. Using a theoretical framework, which barriers and enablers need to be addressed? 3. Which intervention components (behaviour change techniques and mode(s) of delivery) could overcome the modifiable barriers and enhance the enablers? 4. How can behaviour change be measured and understood?
Step 1: Development of eHIP
eHIP is an implementation strategy that contains mechanisms to embed the ACSQHC Hip Fracture Care Clinical Care Standard in everyday clinical practice. This was a collaborative endeavour, which involved key stakeholder groups (clinicians, managers, NSW Agency for Clinical Innovation [ACI] and consumers), including the Local Health District Executive. The success of implementing practice change is heavily reliant on senior clinician support,24 those that will be impacted by the intervention, and those that will be required to act on the intervention (the end users). As such, a working group was formed to review each component of the ACSQHC Hip Fracture Care Clinical Standard to determine a mechanism to action each component. The multidisciplinary working group represented the key stakeholders for each discipline within the hospital that was required to contribute to ensure all components of the ACSQHC Hip Fracture Care Clinical Standard were addressed. The group was chaired by the Clinical Nurse Consultant for Surgery and comprised an emergency nurse, orthopaedic nurse manager, orthopaedic clinical educator, health service manager, geriatrician, anaesthetist, pain service (anaesthetics/nurse), orthopaedic physiotherapist, dietitian and orthopaedic surgeon and met monthly for 12 months.
Step 2: Identification of Barriers to Implementation
Throughout the 12 months, local barriers to compliance with each of the ACSQHC Hip Fracture Care Clinical Care Standard were regularly collected through a series of departmental meetings. The representative from each discipline discussed the role of their department in eHIP with their frontline clinicians and managers and assembled the feedback. Throughout this iterative consultation process, they specifically asked their colleagues about what they thought would and would not be feasible, practical, or effective. The feedback from each department was tabled at each meeting and collated in a list.
Step 3: Categorising Barriers to the Theoretical Domains Framework
The collated list of identified barriers to the implementation of eHIP was then categorised using the Theoretical Domains Framework (TDF).22 The TDF is a robustly developed tool informed by 33 theories of behaviour and behaviour change.22 These have been clustered into 14 domains, which provide a theoretical lens to view the impact of cognitive, social and environmental influences on behaviour (Table 1).
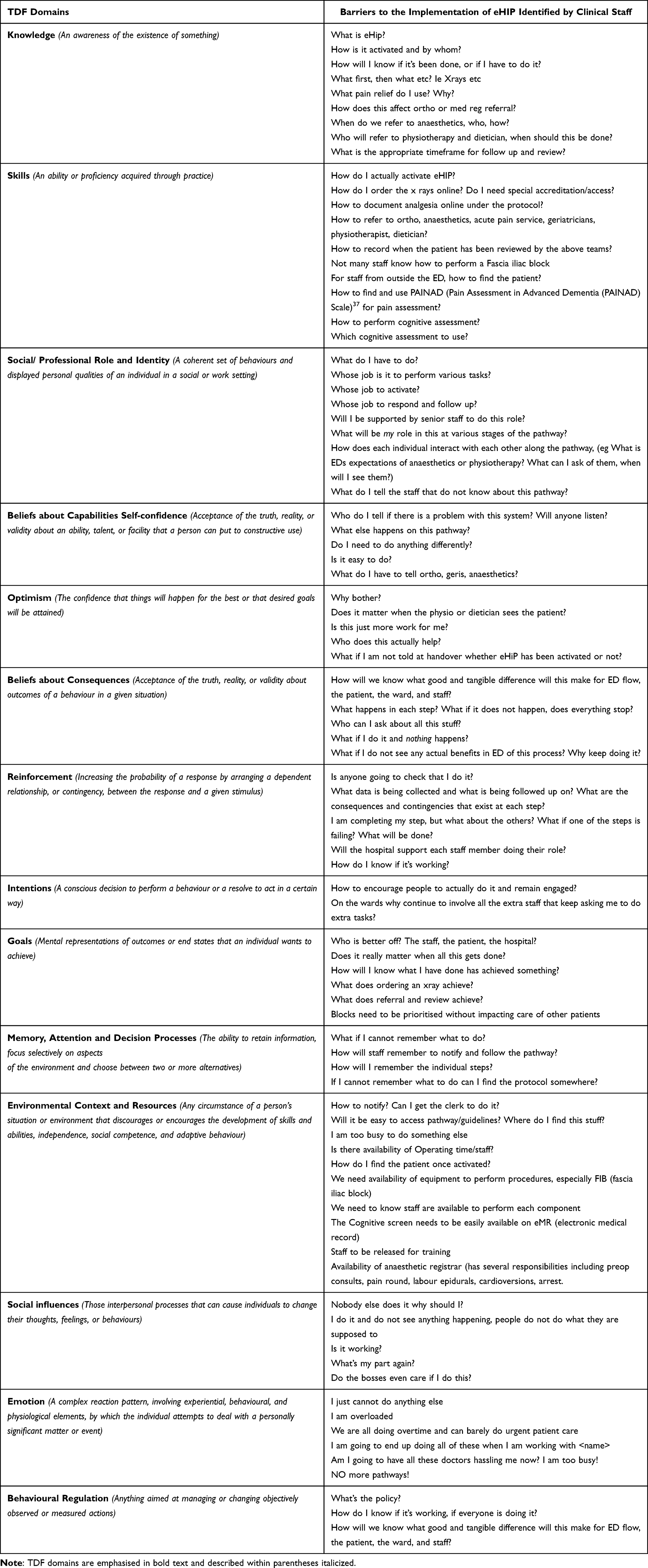 |
Table 1 Barriers to Implementation of eHIP Categorised to the Theoretical Domains Framework |
Step 4: Development of Implementation Strategies
Firstly, the barriers were mapped to intervention functions and behaviour change techniques known to be effective and guided by the Behaviour Change Wheel.25 Intervention functions are “broad categories by means of which an intervention can change behaviour”.25 Each intervention function was assessed to see if they were Affordable, Practical, Effective, Acceptable, had Side-effects and were safe and Equitable (APEASE criteria),25 and prioritised.26 Stakeholders (front line and management level nursing, medical and allied health staff) were involved in the assessment of intervention functions during the monthly committee meetings, and a series of meetings where the eHIP concept was tabled at various departmental meetings to garner support for the intervention. Secondly, the authors chose behaviour change techniques (BCTs) from the Behaviour Change Technique Taxonomy (BCTTv1) based on the intervention functions. A BCT is a component of an intervention that will alter behaviour.25 The taxonomy includes 93 techniques for behaviour change linked to the Behaviour Change Wheel. Each intervention function is associated with a list of BCTs that are relevant to that intervention function, which can be assessed for relevancy to the local context. For example, if the barriers differed between emergency physicians and surgeons, the intervention function and supporting BCTs were refined to that group. Each BCT was also assessed using the APEASE criteria for inclusion. The resulting BCTs were collated and integrated into an implementation plan approved by the committee and hospital executive.
Results
Each ACSQHC Hip Fracture Care Clinical Care Standard was mapped to specific actions along with expected outcomes. For example, to operationalise ACSQHC Hip Fracture Care Clinical Care Standard 1: Care at presentation: The triage nurse will identify potential hip fracture patients, order an x-ray and analgesia. “eHIP” page will be activated on confirmation of a hip fracture and activate a series of mandated assessments and treatments (Table 2). These mechanisms were developed into a formal eHIP policy outlining the roles and responsibilities of each team member and a one page flow chart for easy reference (Figure 1).
 |
Table 2 eHIP Mechanism to Meet Each ACSQHC Hip Fracture Care Clinical Care Standard |
 |
Figure 1 Flow chart summarising the eHIP policy and process. Red, green, and blue sections represent the notify, assess and treat, and plan and prevent stages of eHIP, respectively. Abbreviations: #NOF, neck of femur fracture; SDMH, Shoalhaven District Memorial Hospital; WH, Wollongong Hospital; MRN, medical record number; eMR, electronic medical record; HIRAD, history, red flags, assessment, intervention, diagnostics; IDC, indwelling catheter; ECG, electrocardiograph; FBC, full blood count; UEC, urea, electrolytes, creatinine; CMP, calcium, magnesium, phosphate; LFT, liver function tests; Vit D, vitamin (D); G + H, group and hold; BTF, vital signs between the flags; GP, general practitioner. |
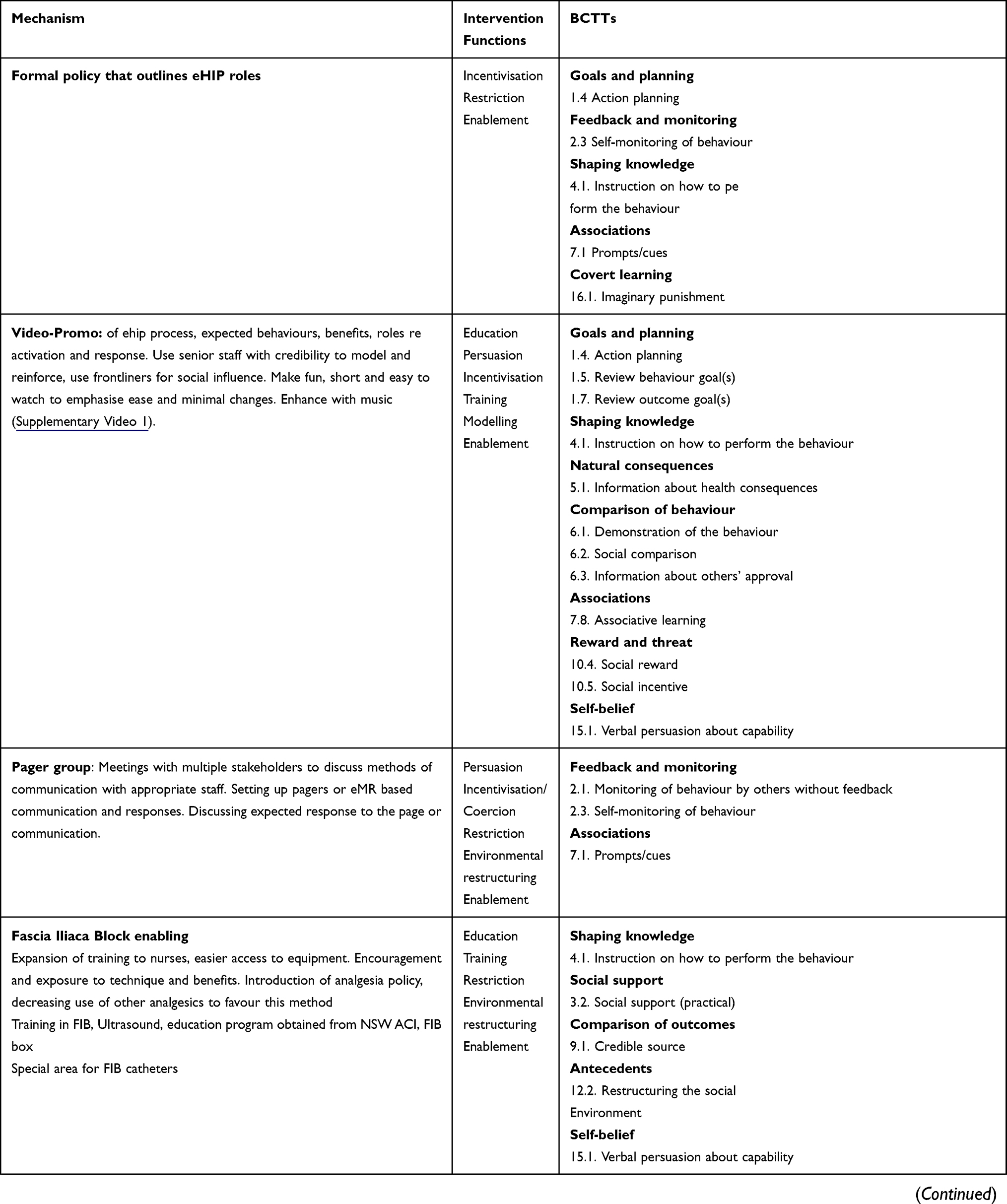
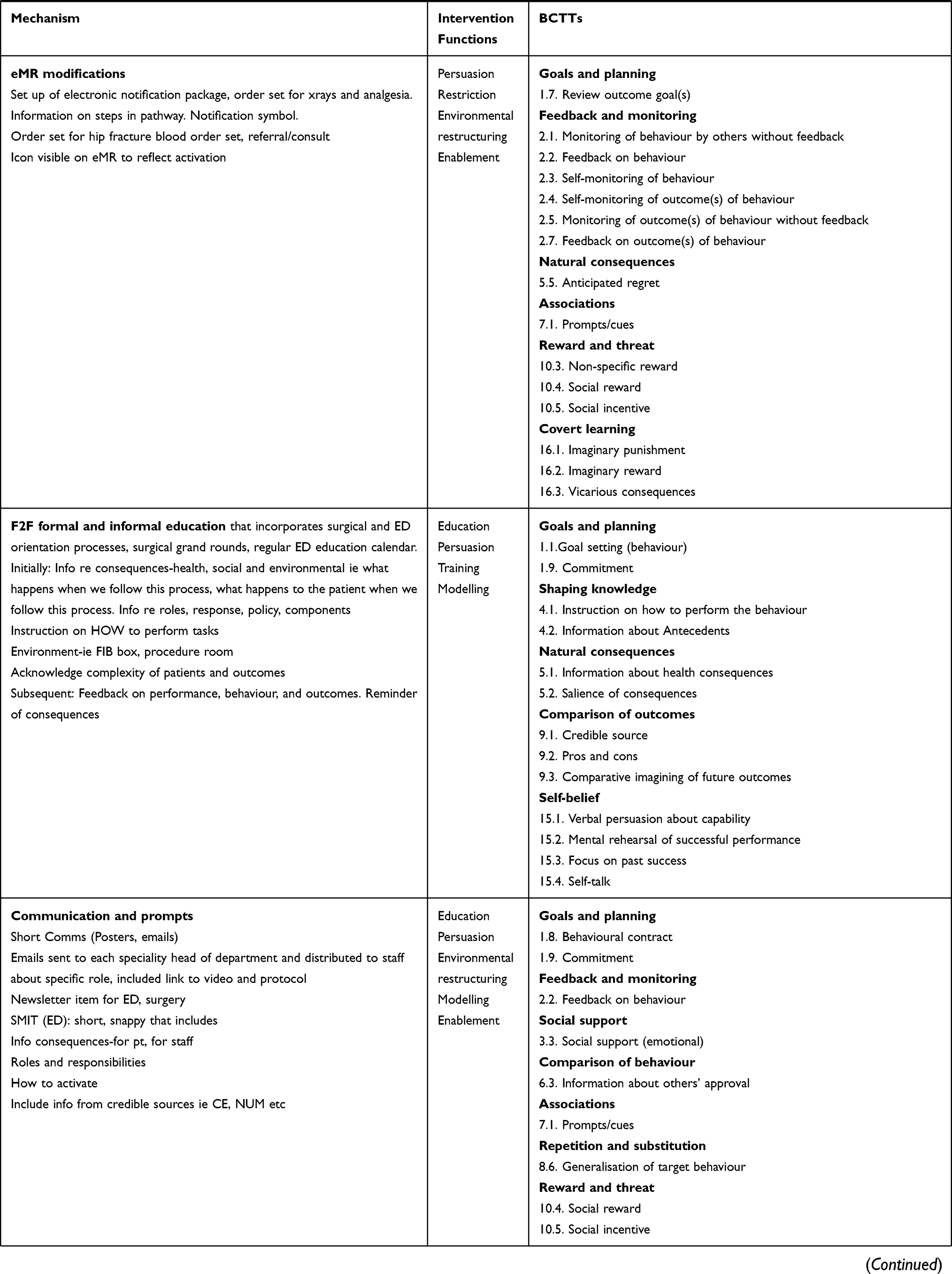
We identified 83 barriers to the implementation of eHIP in all 14 domains of the TDF. Barriers included concerns about other team members “I’m completing my step, but what about the others? What if one of the steps is failing? What will be done?” a lack of skills to complete a fascia iliaca block and other assessments not commonly performed by staff. These are all listed in Table 2. These barriers were mapped to nine intervention functions and assessed using the APEASE criteria. The selected intervention functions were mapped to BCTTs. The 41 BCTTs selected by the committee and stakeholders during the consultation process were mechanised through operational changes to electronic medical records (eMR), a communication plan, an informative and instructional video (Supplementary Video 1, Figure 2), monitoring by clinical champions, additional training in procedures and assessment skills, and clear delineation in expectations of individual staff members (Table 3). eHIP went live on 22nd of June, 2020.
 |
 |
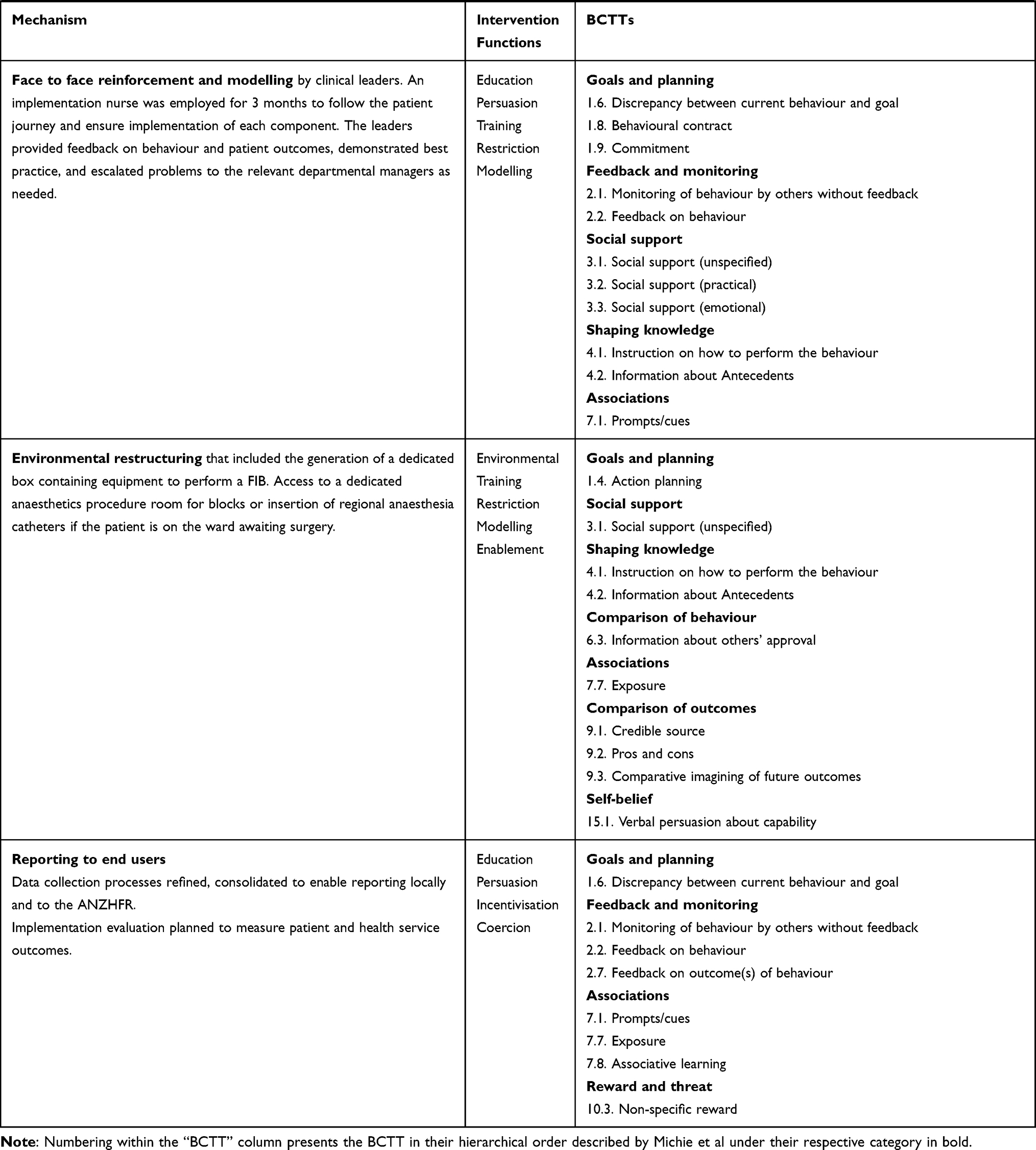 |
Table 3 Mechanism, Intervention Functions, and Behavioural Change Technique Taxonomy (BCTT) as Identified Using the Behaviour Change Wheel |
 |
Figure 2 Screen shots from eHIP implementation video. |
Discussion
This paper describes the development and implementation of a care bundle called eHIP to operationalise the ACSQHC Hip Fracture Care Clinical Care Standard. The development of eHIP and its supporting policy was relatively straightforward, due to existing national guidelines and the support of clinicians with the opportunity and motivation to initiate and coordinate change. However, navigating the organisational barriers for the vulnerable hip fracture patient group was complex.
For eHIP to have a high chance of sustainable success, our strategy needed to consider clinician behavior change, organizational resources and culture.29 This is not a unique finding.18,30 Implementing change in health care is an inherently political process influenced by prevailing power structures, clinician behavior,19 lack of time, individual motivation and the culture of specific healthcare discipline.27,28 Implementation needs planning and strategies that address the complexity of healthcare systems, individual practitioners, managers, as well as strong organizational support and patronage which is influential to normalize a new practice among staff.19,31,32 We achieved this through application of the behavior change wheel,25 as have colleagues elsewhere.30,33
Despite a robust implementation plan and strategy to address all the well-known barriers to change, our implementation was not immune, particularly amid a global pandemic and the subsequent competing priorities among various crucial stakeholders, such as the electronic medical record team. This impacted crucial aspects of the implementation (changes to the electronic notification and referral processes) and made regular well-attended committee meetings challenging, given many staff had leadership roles within our organization’s response to COVID-19.
Implementation of a new process involves many processes, systems and interactions.34 In our complex and multidisciplinary healthcare system, aside from our patients, who are at the center of care, those impacted by eHIP included multiple services and medical specialties from outside of the instigating departments, such as the hospital switchboard, radiology, allied health and hospital executive. We managed to reach agreement among diverse and multiple stakeholders with differing priorities by considering valuing the skills and knowledge of each discipline in the micropolitical context of the health service.19 We also gained support across multiple levels of leadership.19 It is critical to involve end users throughout the process, which we did by establishing a working party of key stakeholders to develop a consensus plan to streamline implementation.
The next stages of our eHIP project will include evaluation of the clinical efficacy of eHIP, as well as measurement of “reach”, “fidelity”, and “dose”.35 Reach assesses whether the intended recipients came into contact with an intervention, this is, how many hip fracture patients received an eHIP activation and if it was appropriate.35 Fidelity will assess if eHIP was delivered as intended and if adaptations were made. Dose will evaluate the quantity of the intervention implemented, that is, each component of the ACSQHC Hip Fracture Care Clinical Care Standard.35,36
Conclusion
The implementation of any intervention in the complex acute care environment requires consideration of local micropolitics and influencers on individual and collective human behaviour. We applied behaviour change theory through a pragmatic evidence-based process. This resulted in a codesigned strategy to overcome staff and organisational barriers to the implementation of a multidisciplinary early activation mechanism and bundle of care (eHIP). Future work will include evaluation of the uptake and clinical impact of the care bundle.
Acknowledgments
NSW Agency for Clinical Innovation and Illawarra Health and Medical Research Institute for funding.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Goh EL, Lerner RG, Achten J, Parsons N, Griffin XL, Costa PML. Complications following hip fracture: results from the World Hip Trauma Evaluation cohort study. Injury. 2020;51(6):1331–1336. doi:10.1016/j.injury.2020.03.031
2. Dixon T. The Problem of Osteoporotic Hip Fracture in Australia. Canberra: AIHW; 2010.
3. Health AIo, Welfare. Estimating the Prevalence of Osteoporosis in Australia. Canberra: AIHW; 2014.
4. Health AIo, Welfare. Australia’s Hospitals at a Glance 2016–17. Canberra: AIHW; 2018.
5. Watts JJ, Abimanyi-Ochom J, Sanders KM. Osteoporosis Costing All Australians: A New Burden of Disease Analysis – 2012 to 2022. Sydney: Osteoporosis Australia; 2013.
6. Buse GL, Mohit B, Sancheti P, et al. Accelerated care versus standard care among patients with hip fracture: the HIP ATTACK pilot trial. Can Med Assoc J. 2014;186(1):E52.
7. Panella M, Seys D, Sermeus W, et al. Minimal impact of a care pathway for geriatric hip fracture patients. Injury. 2018;49(8):1581–1586. doi:10.1016/j.injury.2018.06.005
8. National Institute for Health and Care Excellence. Hip fracture: management clinical guideline [CG124]; 2017.
9. Or O, Fisher Negev T, Hadad V, et al. Fracture liaison service for hip fractures: is it a game changer? IMAJ. 2021;23(8):490–493.
10. Costa ML, Griffin XL, Achten J, et al. World Hip Trauma Evaluation (WHiTE): framework for embedded comprehensive cohort studies. BMJ Open. 2016;6(10):e011679. doi:10.1136/bmjopen-2016-011679
11. ACSQHC. Hip Fracture Care Clinical Care Standard. Sydney: ACSQHC; 2016.
12. ANZHFR. Bi-national annual report of hip fracture care; 2020.
13. Chuan A, Zhao L, Tillekeratne N, et al. The effect of a multidisciplinary care bundle on the incidence of delirium after hip fracture surgery: a quality improvement study. Anaesthesia. 2020;75(1):63–71. doi:10.1111/anae.14840
14. Cehic M, Lerner RG, Achten J, Griffin XL, Prieto-Alhambra D, Costa ML. Prescribing and adherence to bone protection medications following hip fracture in the United Kingdom. Bone Joint J. 2019;101–B(11):1402–1407. doi:10.1302/0301-620X.101B11.BJJ-2019-0387.R1
15. Lian T, Dybvik E, Gjertsen J-E, et al. Compliance with national guidelines for antibiotic prophylaxis in hip fracture patients: a quality assessment study of 13 329 patients in the Norwegian Hip Fracture Register. BMJ Open. 2020;10(5):e035598. doi:10.1136/bmjopen-2019-035598
16. Schulze Raestrup U, Grams A, Smektala R. Guideline compliance in hip fracture: results of an external quality-assurance program in North Rhine Westphalia: 2003–2005. Der Unfallchirurg. 2008;111(2):65–70. doi:10.1007/s00113-008-1405-0
17. Zielinski S, Meeuwis MA, Heetveld M, et al. Adherence to a femoral neck fracture treatment guideline. Int Orthop. 2013;37(7):1327–1334. doi:10.1007/s00264-013-1888-3
18. Rath S, Yadav L, Tewari A, et al. Management of older adults with hip fractures in India: a mixed methods study of current practice, barriers and facilitators, with recommendations to improve care pathways. Arch Osteoporos. 2017;12(1):55. doi:10.1007/s11657-017-0344-1
19. Rogers L, De Brún A, Birken SA, Davies C, McAuliffe E. The micropolitics of implementation; a qualitative study exploring the impact of power, authority, and influence when implementing change in healthcare teams. BMC Health Serv Res. 2020;20(1):1059. doi:10.1186/s12913-020-05905-z
20. ANZHFR. Bi-national annual report of hip fracture care; 2019.
21. ANZHFR. Bi-national annual report of hip fracture care; 2018.
22. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
23. French SD, Green SE, O’Connor DA, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implement Sci. 2012;7:38. doi:10.1186/1748-5908-7-38
24. Bennetts S, Campbell-Brophy E, Huckson S, Doherty S, National H. Medical research council’s national institute for clinical studies national emergency care pain management I. Pain management in Australian emergency departments: current practice, enablers, barriers and future directions. Emergency Med Australasia. 2012;24(2):136–143. doi:10.1111/j.1742-6723.2011.01499.x
25. Michie S, Atkins L, West R. The Behaviour Change Wheel: A Guide to Designing Interventions. Great Britain: Silverback Publishing; 2014.
26. Sinnott C, Mercer SW, Payne RA, Duerden M, Bradley CP, Byrne M. Improving medication management in multimorbidity: development of the MultimorbiditY COllaborative Medication Review And DEcision Making (MY COMRADE) intervention using the behaviour change wheel. Implementation Sci. 2015;10(1):132. doi:10.1186/s13012-015-0322-1
27. Handley MA, Gorukanti A, Cattamanchi A. Strategies for implementing implementation science: a methodological overview. Emergency Med J. 2016;33(9):660. doi:10.1136/emermed-2015-205461
28. Jabbour M, Newton AS, Johnson D, Curran JA. Defining barriers and enablers for clinical pathway implementation in complex clinical settings. Implement Sci. 2018;13(1):139. doi:10.1186/s13012-018-0832-8
29. Glisson C. The role of organizational culture and climate in innovation and effectiveness. Human Serv Organ. 2015;39(4):245–250.
30. Oberai T, Laver K, Killington M, Woodman R, Crotty M, Jaarsma R. No longer lost in translation: study protocol for preventing delirium post hip fracture. Eur J Pers Centered Healthcare. 2019;7:98–105.
31. Resnick LA. Paving clinical pathways: using a trusted change management model to establish standardized, evidence-based care across the continuum. ASQ’s Healthcare Update; 2014.
32. Seckler E, Regauer V, Rotter T, Bauer P, Müller M. Barriers to and facilitators of the implementation of multi-disciplinary care pathways in primary care: a systematic review. BMC Fam Pract. 2020;21(1):113. doi:10.1186/s12875-020-01179-w
33. Thomas S, Mackintosh S. Use of the theoretical domains framework to develop an intervention to improve physical therapist management of the risk of falls after discharge. Phys Ther. 2014;94(11):1660–1675. doi:10.2522/ptj.20130412
34. Curtis K, Fry M, Shaban RZ, Considine J. Translating research findings to clinical nursing practice. J Clin Nurs. 2017;26(5–6):862–872. doi:10.1111/jocn.13586
35. Moore GF, Audrey S, Barker M, et al. Process evaluation of complex interventions: medical Research Council guidance. BMJ. 2015;350:h1258. doi:10.1136/bmj.h1258
36. Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implementation Sci. 2007;2(1):40. doi:10.1186/1748-5908-2-40
37. Warden V, Hurley AC, Volicer L. Development and Psychometric Evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc. 2003;4(1):9–15. doi:10.1097/01.JAM.0000043422.31640.F7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.